Summary
Ischemic stroke is an acute neurological condition caused by impaired cerebral blood flow (e.g., vascular occlusion or systemic hypoperfusion). The most important risk factors are chronic systemic hypertension and cardiovascular disease. Modifiable risk factors should be managed (e.g., primary prevention of ASCVD, anticoagulation for patients with atrial fibrillation) for primary prevention of stroke. Clinically, ischemic stroke is characterized by the acute onset of focal neurological deficits, which are dependent on the cerebral territory covered by the relevant vessel. If ischemic stroke is suspected, a noncontrast head CT should immediately be performed to rule out intracranial hemorrhage and blood glucose should be measured as it is a stroke mimic. Revascularization of the vessels affected in ischemic stroke, e.g., via tissue plasminogen activator (tPA) or thrombectomy, can preserve brain tissue and improve outcomes if given early. Further treatment consists of supportive care, neuroprotective measures, management of underlying causes, and reducing subsequent stroke risk with antiplatelet therapy and other management of ASCVD.
Central retinal artery occlusion, transient ischemic attack, intracerebral hemorrhage, and subarachnoid hemorrhage are covered in separate articles. See also “Overview of stroke.”
Definitions
- Acute neurological dysfunction caused by brain, spinal cord, or retinal infarction [1]
- See “Overview of stroke” for related conditions.
Epidemiology
Ischemic strokes account for ∼ 85% of all strokes.
Risk factors for ischemic stroke
-
Nonmodifiable risk factors [2][3][4]
- Age ≥ 65 years
- Sex ♂ > ♀
- African Americans, Native Americans, Alaska Natives, and Hispanics are at higher risk.
- Family history of cardiovascular or cerebrovascular disease
- Genetic disorders (e.g., sickle cell disease)
- History of TIA
- Migraine with aura
- Low birth weight
-
Modifiable risk factors [2][4]
- Systemic hypertension
- Hyperlipidemia
- Diabetes mellitus
- Atherosclerosis
-
Cardiovascular disease
- Carotid artery stenosis
- Atrial fibrillation
- Obesity
- Coagulopathy (e.g., protein C or S deficiency), hyperhomocysteinemia
- Heavy alcohol use
- Tobacco use
- Recreational drug use (e.g., cocaine can cause cerebral vasospasm)
- Oral contraceptive use
- Hormone replacement therapy
- Sedentary lifestyle
- Suboptimal diet (e.g., high salt intake, inadequate fruit and vegetable intake)
For both ischemic and hemorrhagic strokes, age is the most important nonmodifiable risk factor and arterial hypertension is the most important modifiable risk factor.
Epidemiological data refers to the US, unless otherwise specified.
Etiology

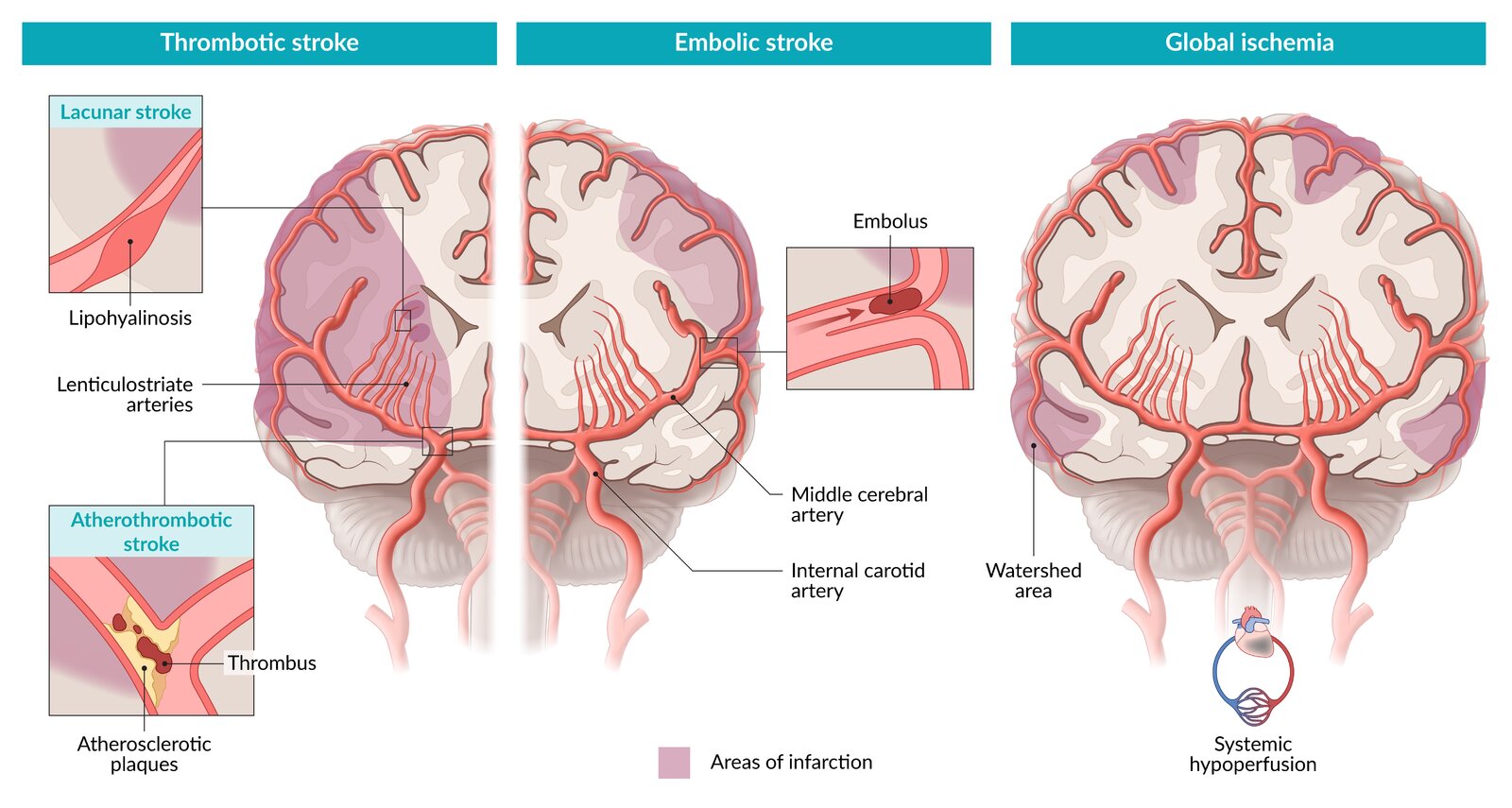
Embolic strokes (∼ 20% of all strokes)
- Most commonly affect the middle cerebral artery (MCA)
- Dislodged emboli can affect multiple cerebral vascular territories simultaneously.
-
Cardiac emboli
- Atrial fibrillation
- Atrial or ventricular thrombi
- Rheumatic heart disease
- Ventricular aneurysms
-
Atheroemboli
- Internal carotid artery
- Aortic arch (less common)
- Infectious emboli: bacterial endocarditis
- Paradoxical embolism: venous thromboembolism (especially due to deep vein thrombosis) in patients with right-to-left cardiac shunt (e.g., persistent foramen ovale or atrial septal defect)
- Spectacular shrinking deficit: distal migration of the embolus leads to recanalization of the affected vessel and rapid clinical improvement after symptom onset

Thrombotic strokes (∼ 40%)
-
Large vessel atherosclerosis (∼ 20%)
- Rupture of an atherosclerotic plaque and exposure of subendothelial collagen → formation of a thrombus
- Thrombus formation most commonly occurs at branch points in arteries (e.g., ; internal carotid artery bifurcation or where the MCA branches from the circle of Willis).
- Small vessel occlusion (e.g., lacunar infarct) (∼ 20%): see “Subtypes and variants” below.
Global cerebral ischemia
-
Systemic hypoperfusion
- Shock or bilateral large artery atherosclerosis (e.g., of carotid arteries) → decreased effective oxygen delivery to the whole brain
- Common during cardiac surgeries
- Can result in watershed infarct
- Hypoglycemia: Repeated episodes of hypoglycemia (e.g., due to insulinoma) increase the risk of cerebral ischemia.
- Severe and/or chronic hypoxia: hypoxemia (e.g., due to respiratory arrest) → global tissue hypoxia in the brain
Other causes
-
Hypercoagulable states
- Inherited thrombophilia (e.g., factor V Leiden mutation, protein C deficiency)
- Polycythemia
- Hormonal contraceptive use
- Hormone replacement therapy
- Sickle cell disease
- Vasculitis (e.g., giant cell arteritis)
- Arterial dissection (e.g., due to trauma or fibromuscular dysplasia)
References:[5][6][7][8][9][10][11]
© AMBOSS
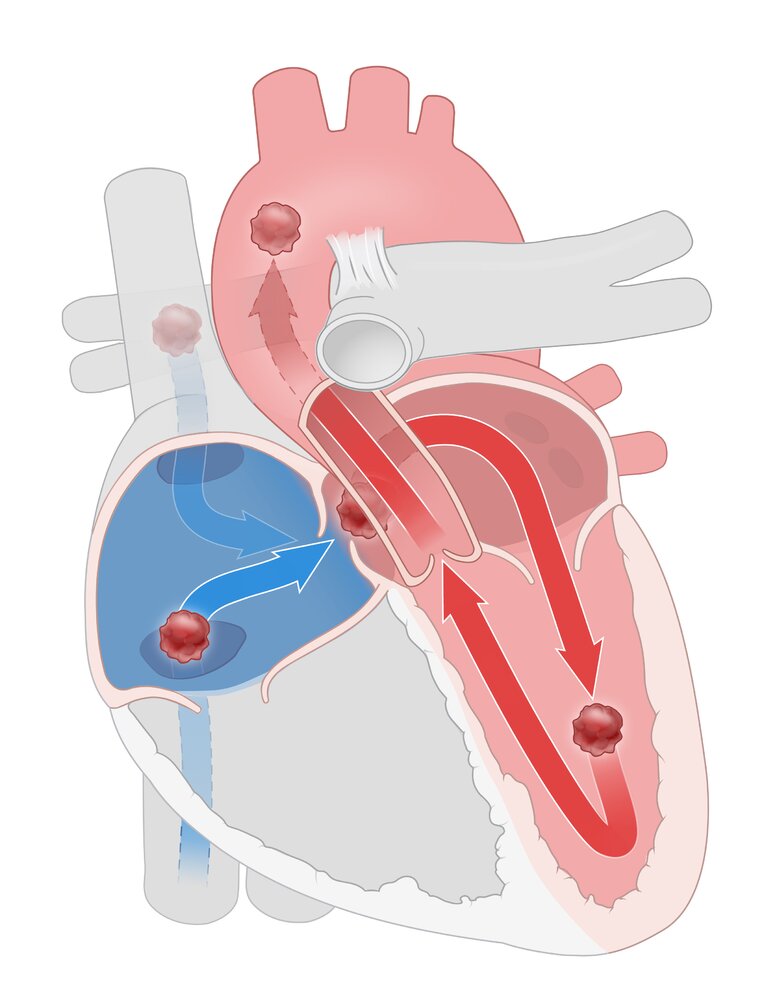
In the presence of a patent foramen ovale, transient increases in right atrial pressure (e.g., when coughing) can allow emboli from the venous system to pass from the right atrium to the left atrium. From there, they can enter systemic arterial circulation and cause arterial embolism (e.g., stroke).
© AMBOSS
Clinical features
- Sudden onset of focal neurological deficits (e.g., weakness/paralysis, paresthesias, aphasia, dysarthria)
- Nonspecific symptoms (e.g., impaired consciousness, nausea, vomiting, headache, seizures)
- Symptoms depend on the location of the stroke (see “Stroke symptoms by affected vessel” and “Stroke symptoms by affected region”)
- Symptoms suggesting a specific etiology:
- Aortic dissection: chest pain, hypotension, dyspnea
- Endocarditis: fever, heart murmur
- ICH/SAH: sudden, severe headache
Stroke should be ruled out in patients presenting with first-time epileptic seizures and subsequent neurological deficits, as the seizure may have been caused by an acute cerebral pathology.
Subtypes and variants
Lacunar infarct [7][12]
- Definition: noncortical infarcts characterized by the absence of cortical signs (e.g., no aphasia, hemianopsia, agnosia, apraxia)
-
Etiology
- Most common: chronic hypertensive vasculopathy → lipohyalinosis of the small vessels → occlusion of small, penetrating arteries (e.g., lenticulostriate artery); → lacunar stroke resulting in specific lacunar syndromes (see “Lacunar syndromes”)
- Less common
- Cardioembolic event
- Microatheroma formation
- Microbleed (rare)
-
Risk factors
- Hypertension
- Diabetes mellitus
-
Clinical features
- Acute transient focal neurological symptoms that often have a stuttering course
- Symptoms depend on the affected territory.
- See “Lacunar syndromes.”
-
Commonly affected areas
- Internal capsule, corona radiata
- Pons
- Basal ganglia (striatum, putamen, globus pallidus, thalamus, caudate)
- Diagnosis: diffusion-weighted MRI
- Pathology: results in a pale infarction at the periphery of the cortex
- Treatment: same as for other ischemic strokes (see “Treatment”)
Infarction of the posterior limb of the internal capsule is the most common type of lacunar stroke and may manifest clinically with pure motor stroke, pure sensory stroke (rare), sensorimotor stroke, dysarthria-clumsy hand syndrome, and/or ataxic hemiparesis.
Watershed infarct [6][13]
- Definition: border-zone infarct in the region between the territory of two major arteries that supply the brain (watershed area)
-
Etiology: sudden decrease in blood pressure or cessation of blood flow through both vessels → ischemia in the susceptible region between two vascular territories
- Cortical border zones: territories between the anterior and middle cerebral arteries and between the middle and posterior cerebral arteries
- Internal border zones: territories between the superficial and deep branches of the MCA
-
Clinical features
- Signs of systemic hypoperfusion (e.g., tachycardia, low blood pressure, pallor, sweating)
- Diffuse neurological deterioration
- PCA-MCA watershed region: bilateral visual loss (cortical blindness)
- ACA-MCA watershed region: proximal limb weakness with sparing of the face, hands, and feet (“man-in-the-barrel syndrome”)

© AMBOSS
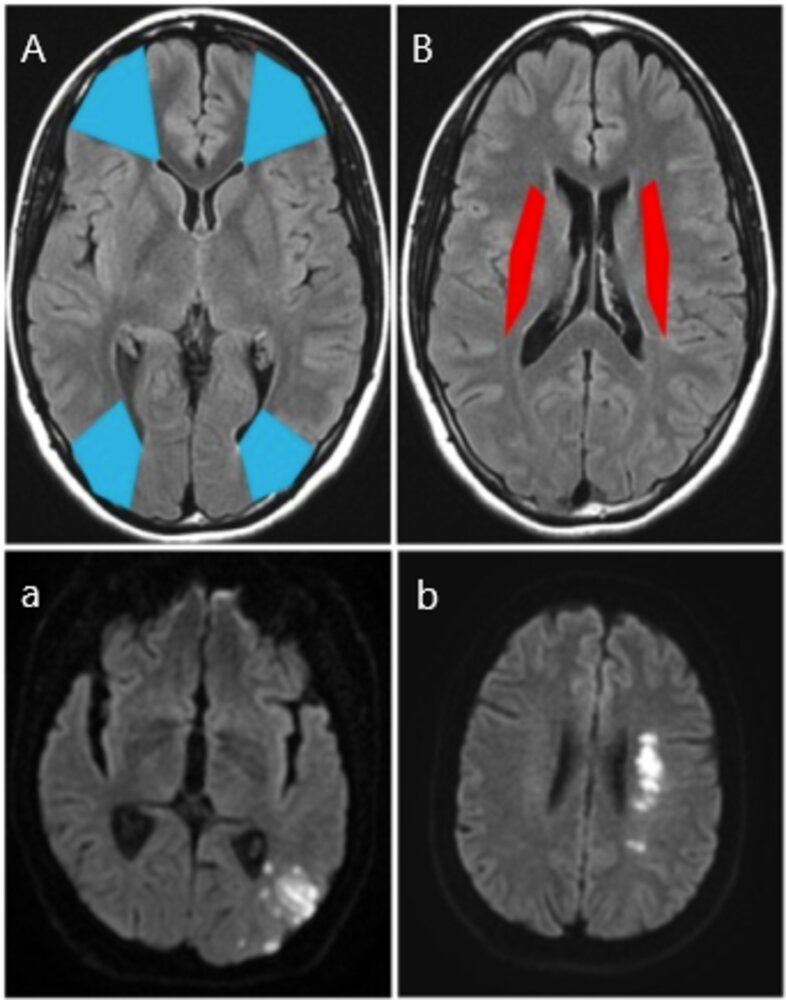
MRI head (A and B: FLAIR; a.and b.; DWI)
Cortical border zones, or watershed areas (A; blue), are located between the ACA and MCA territories and the PCA and MCA territories. A left occipital infarct (a; white) is shown at the boundary between the middle and posterior cerebral territories.
Internal border zones (B; red) are located between the superficial and deep branches of the MCA. A left internal watershed infarct (b; white) is shown.
FLAIR: fluid-attenuated inversion recovery; DWI: diffusion-weighted imaging; ACA: anterior cerebral artery; MCA: middle cerebral artery; PCA: posterior cerebral artery
Source: “Figure 1, in: Relationship between Watershed Infarcts and Recent Intra Plaque Haemorrhage in Carotid Atherosclerotic Plaque” by Isabel C et al., Plos One, licensed under CC BY 4.0. Modifications: Image cropped, labels changed.
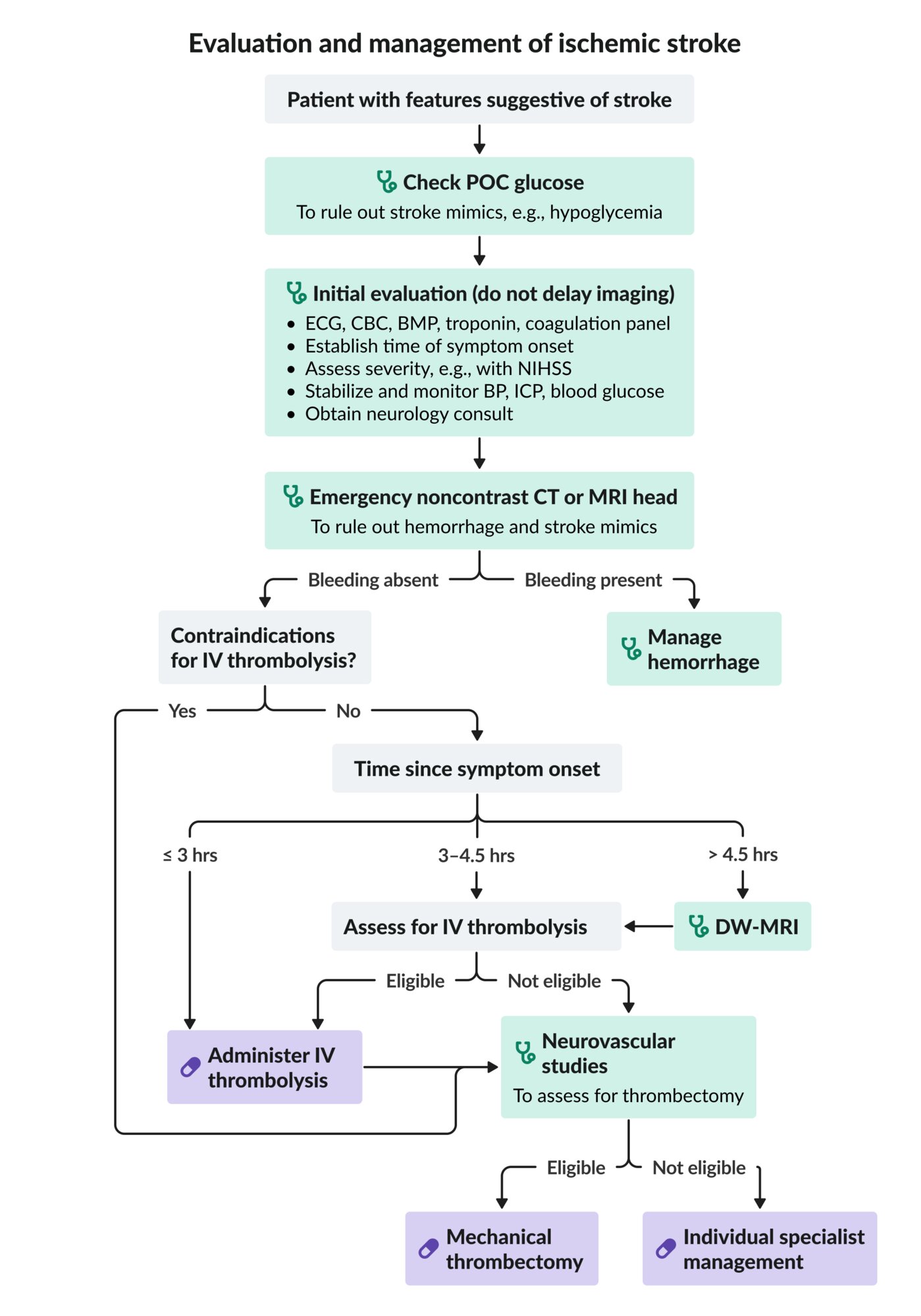
Initial evaluation and acute stabilization
Primary survey
Clinical assessment and management should occur simultaneously with the goals of stabilizing the patient, keeping the door-to-neuroimaging time to a minimum, and identifying candidates for reperfusion therapy as soon as possible. [14][15][16]
- Airway management: Secure airway if airway protective reflexes are impaired, e.g., due to depressed level of consciousness or bulbar dysfunction.
-
Respiratory support
- Provide oxygen therapy to keep SpO2 > 94%.
- Consider mechanical ventilation for respiratory failure.
- Hemodynamic support: See “Blood pressure management in ischemic stroke.”
-
Rapid focused neurological assessment
- Determine the time of symptom onset or, if this is unknown, the time the patient was last seen well or at neurological baseline.
- Identify risk factors for ischemic stroke and risk factors for hemorrhagic stroke.
- Minimum neurological examination
- GCS score
- Pupillary examination
- Identification of lateralizing signs, e.g., hemiparesis, facial droop, pronator drift
- Screening for signs of cerebral herniation
- Focused neurological examination
- Attempt to localize lesion by identifying stroke symptoms by affected vessel.
- Perform severity assessment: e.g., NIHSS
- Assess for a central cause in patients presenting with vertigo (e.g., using HINTS examination). [17]
-
Critical management steps [14][18]
- Check POC glucose and treat immediately if < 60 mg/dL or > 400 mg/dL to rule out stroke mimic.
- Arrange emergency neuroimaging, e.g., noncontrast CT head, to rule out intracranial hemorrhage.
-
Treat eligible patients with reperfusion therapy for acute ischemic stroke (e.g., IV thrombolytics, mechanical thrombectomy)
- Identify inclusion and exclusion criteria.
- Lower BP to < 185/110 mm Hg prior to initiation.
- Initiate neuroprotective measures and supportive care for ischemic stroke.
- Start ICP management if needed: Avoid steroids, hypothermia, and barbiturates.
-
Consults and disposition
- Consult neurology immediately if acute ischemic stroke is identified.
- Consult neurosurgery for any hemorrhagic transformation or if there are indications for ventriculostomy or decompressive craniectomy: e.g., cerebral edema with refractory ↑ ICP, large cerebellar infarction with obstructing hydrocephalus.
- Admit the patient to a dedicated stroke unit (or ICU) for at least 24 hours .
- Arrange immediate transfer to a stroke center if specialized care is unavailable locally. [17]
- Next steps: See “Diagnostics of ischemic stroke” and “Treatment of ischemic stroke.”
Only POC glucose and noncontrast neuroimaging (e.g., CT head or MR brain) are required prior to thrombolytic therapy. Do not delay treatment to complete the remainder of the diagnostic evaluation. A classic clinical presentation without evidence of a stroke mimic or intracranial bleeding on initial neuroimaging is typically enough to diagnose acute ischemic stroke in time-limited settings. [14]
Malignant infarctions in the MCA territory or large PICA infarctions may require surgical intervention before edema reaches its maximum extent to prevent brain herniation. [14]

Blood pressure management in acute ischemic stroke [14]
- Provide immediate hemodynamic support for hypotension and hypovolemia (see “Neurogenic shock”).
-
Treatment of hypertension in patients not undergoing reperfusion therapy
- BP < 220/120 mm Hg
- Permissive hypertension: Moderate hypertension is tolerated within the first 48–72 hours with the goal of maintaining cerebral perfusion.
- Earlier BP reduction is indicated in patients with certain comorbidities, e.g., concomitant heart failure or aortic dissection, and after thrombolysis.
- BP ≥ 220/120 mm Hg: Careful BP reduction, e.g., by ∼ 15% within the first 24 hours of stroke onset may be considered.
- BP < 220/120 mm Hg
- Patients undergoing reperfusion therapy: Reduce BP to < 185/110 mmHg beforehand and keep BP < 180/105 mm Hg for the first 24 hours after treatment.
- Recommended agents: labetalol , clevidipine , or nicardipine
- Once the patient is neurologically stable, start (or restart) oral antihypertensive therapy if BP > 140/90 mm Hg.
BMP: basic metabolic panel
BP: blood pressure
CBC: complete blood count
CT: computed tomography
DW-MRI: diffusion-weighted magnetic resonance imaging
ECG: electrocardiogram
ICP: intracranial pressure
IV: intravenous
MRI: magnetic resonance imaging
NIHSS: National Institutes of Health Stroke Scale
POC: point-of-care
© AMBOSS
Severity assessment
The following scales can be calculated at initial presentation to guide treatment decisions and estimate prognosis, or repeated to monitor progression and response to therapy during admission, rehabilitation, and follow-up. They are also used as outcome measures in clinical trials.
National Institutes of Health Stroke Scale (NIHSS) [19]
- A severity score that quantifies neurological impairment for specific categories within the following broad domains:
- Level of consciousness, orientation, and ability to follow commands
- Cranial nerve palsies: e.g., visual impairment, facial droop
- Motor and sensory deficits or neglect
- Language impairment
- Coordination
- Scores between are assigned for each category are combined and totals can range from 0 (no impairment) to 42 (most severe).
The NIHSS is weighted towards anterior circulation strokes and underestimates stroke severity in the posterior circulation. [20]
| National Institute of Health Stroke Scale (NIHSS) [14][19] | ||
|---|---|---|
| Category | Task | Score |
| 1a: Level of consciousness | Assess alertness. |
|
| 1b: Orientation questions | Ask month and age. |
|
| 1c: Commands | Patient opens/closes eyes and makes a fist. |
|
| 2: Gaze | Patient follows examiner's finger in horizontal movements. |
|
| 3: Visual fields | Present visual stimuli in the patient's visual field quadrants. |
|
| 4: Facial palsy | Patient shows teeth, raises eyebrows, squeezes eyes shut. |
|
| 5a: Motor: left arm 5b: Motor: right arm | Patient elevates each arm to 45° from a supine position or 90° if sitting with open palms facing downwards. |
|
| 6a: Motor: left leg 6b: Motor: right leg | Patient elevates each leg to 30° from a supine position. |
|
| 7: Limb ataxia | Patient performs finger-to-nose and heel-shin tests on both sides. |
|
| 8: Sensory | Test sensation of face, arms, and legs. |
|
| 9: Language | Patient names items, describes a picture, or reads a sentence. |
|
| 10: Dysarthria | Ask patient to read or repeat words. |
|
| 11: Sensory extinction or inattention | Offer simultaneous tactile and visual stimuli. |
|
| ||
")
Modified Rankin scale [26][27]
- A scale used to quantify the degree of disability and dependence in daily activities before and after cerebral stroke.
- The scale ranges from 0 (no symptoms) to 6 (death).
| Modified Rankin scale | ||
|---|---|---|
| Disability | Symptoms | Score |
| None | Absent | 0 |
| Insignificant | Present, but not affecting usual activities | 1 |
| Slight | Affecting some activities, but not affecting independence | 2 |
| Moderate | Necessitating assistance for some ADLs, but not for walking | 3 |
| Moderately severe | Necessitating assistance for walking and most ADLs | 4 |
| Severe | Necessitating full-time care for all ADLs (e.g., bedbound, incontinent) | 5 |
| Death | 6 | |
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Diagnosis
Diagnostic approach [28][29][30][31]
- Prioritize neuroimaging for ischemic stroke as soon as possible.
- Obtain initial noncontrast imaging without delay. [14]
- CT head is usually the initial imaging modality
- MRI brain is more sensitive for early stroke detection than CT , however, it is less commonly available and takes longer.
- Consider advanced neuroimaging in consultation with a neurologist, but do not delay reperfusion therapy if indicated. [28][32]
- Identify any stroke mimics on neuroimaging: e.g., brain tumor, brain abscess
- Consider follow-up neuroimaging for patients with high clinical suspicion and equivocal initial CT and MRI.
- Obtain initial noncontrast imaging without delay. [14]
- Order additional studies within the first 48 hours of symptom onset to determine the underlying etiology.
- Laboratory studies
- ECG and further cardiac evaluation (e.g., to identify atrial fibrillation)
- Neurovascular studies: to identify stenosis or dissection of the carotid or vertebral arteries
-
Anterior circulation infarct
- Obtain noninvasive carotid imaging: e.g., CTA, MRA, or carotid artery duplex
- Consider noninvasive intracranial arterial imaging: e.g., CTA, MRA, transcranial doppler
- See also “Carotid artery stenosis diagnostics.”
- Posterior circulation infarct: Consider noninvasive imaging of intracranial and extracranial arteries (including vertebrobasilar circulation)
-
Anterior circulation infarct
- If etiology remains uncertain (i.e., cryptogenic stroke): Consider advanced studies, e.g., prolonged ambulatory ECG monitoring, evaluation for patent foramen ovale, screening for genetic diseases or vasculitides
Obtain noncontrast neuroimaging as soon as possible.
The decision to obtain advanced imaging should not delay the administration of thrombolytic therapy in appropriate candidates. [14]
Immediate laboratory studies [11][14][31][33]
- Glucose
- Serum troponin [11]
- Coagulation panel
- BMP
- CBC
Cardiac evaluation [14][31]
All patients with a suspected ischemic stroke should receive an initial ECG and cardiac monitoring.
- All patients
- ECG: to evaluate for atrial fibrillation, atrial flutter, or other cardiac conditions (e.g., acute myocardial infarction)
- Cardiac monitoring: indicated for a minimum of 24 hours to detect occult atrial fibrillation
- Select patients
- Consider prolonged cardiac monitoring (i.e., 30 days) for suspected intermittent atrial fibrillation or atrial flutter. [33][34]
-
Echocardiography: Consider in patients with suspected embolic stroke or symptoms of heart disease.
- TTE is the preferred initial modality.
- TEE may be added if the identification of a PFO , valvular disease, or aortic arch atherosclerosis will change management. [34][35]
- Possible findings include left atrial or ventricular thrombus, dilated or restrictive cardiomyopathy, patent foramen ovale (PFO), and cardiac tumor.
- Consider cardiac CT or cardiac MRI if embolic stroke of undetermined source (ESUS) is suspected.
Additional investigations [11][14][33]
Consider these in select patients, e.g., to identify the underlying cause, assess the risk of recurrence, and evaluate comorbidities or complications.
- Guiding treatment and reducing subsequent stroke risk
- Lipid profile
- Fasting glucose or OGTT
- Hemoglobin A1C
- Pregnancy test
- Liver chemistries
- TSH [36][37]
- Evaluating underlying cause
- Thrombophilia screening: consider if patient is < 50 years of age and/or has a history of thrombosis [33]
- CNS infection screening: e.g., blood culture, CSF culture, HIV test, VDRL, RPR
- Toxicology screen: e.g., blood alcohol level, urine screen for cocaine or amphetamines [11]
- ESR/CRP
- Others
- Electroencephalogram (EEG): Consider if there is a concern for seizures.
- Chest x-ray: Consider if cardiac or respiratory diseases are suspected.
BMP: basic metabolic panel
BP: blood pressure
CBC: complete blood count
CT: computed tomography
DW-MRI: diffusion-weighted magnetic resonance imaging
ECG: electrocardiogram
ICP: intracranial pressure
IV: intravenous
MRI: magnetic resonance imaging
NIHSS: National Institutes of Health Stroke Scale
POC: point-of-care
© AMBOSS
Neuroimaging
Noncontrast CT head [29][30][38][39][40]
- Indication: all patients with a suspected acute stroke to rule out intracerebral hemorrhage and potential stroke mimics (e.g., tumors) and detect early signs of stroke [14]
- Stroke protocols: can be paired with CTA head and neck in some centers.
-
Findings: may be normal or show evolving ischemic changes over time [28][41]
-
< 2 hours after event
- Usually, no signs of infarction are visible.
- In a large artery occlusion, there may be hyperdense occluded vessels (e.g., hyperdense MCA sign, which indicates an acute thromboembolic occlusion of the MCA ).
-
< 6 hours after the event: in some cases, early signs of cytotoxic edema
- Hypodense parenchyma of infarcted region
- Loss of corticomedullary (i.e., gray-white matter) differentiation, especially in the basal ganglia and insula
- Effacement of the sulci: e.g., obscuring of the lateral sulcus (also known as Sylvian fissure) due to cortical swelling
- 12–24 hours after event; : Hypodense parenchyma starts becoming more clearly demarcated.
- 3–5 days after event: maximum extent of edema and mass effect [42]
- 2–3 weeks after event: Infarcted region appears isodense. [43]
- Chronic infarcts appear hypodense (isodense to cerebral spinal fluid) and well-demarcated, with negative mass effect.
-
< 2 hours after event
Infarctions in the cerebellum and brainstem may be harder to detect with noncontrast head CT than infarctions in other regions. [44]
 sign")






MRI brain [14][38][45]
-
Indications
- If readily available, brain MRI may be performed instead of noncontrast head CT. [46]
- Unclear time of onset or wake-up stroke: to determine eligibility for thrombolysis
- Signs or symptoms of a posterior circulation infarct
- Stroke protocols: includes T1-weighted, T2-weighted, fluid-attenuated inversion recovery (FLAIR), and diffusion-weighted imaging (DWI).
-
Findings: The appearance of early ischemic lesions depends on the time and imaging sequence [30][47]
- Early acute (< 6 hours after event)
- Arterial enhancement or a hyperdense media sign may be visible.
- DWI: Ischemic lesion appears hyperintense within a few minutes (most sensitive modality).
- Late acute (6–24 hours after event)
- T1-weighted: Ischemic lesion appears hypointense.
- T2-weighted and FLAIR: Ischemic lesion appears hyperintense.
- Chronic infarcts can show variable signal intensity.
- Typical signal patterns can suggest an underlying etiology [48]
- Cardioembolic: multiple lesions in different vascular territories
- Large artery atherosclerosis: scattered lesions in one vascular territory
- Early acute (< 6 hours after event)
DWI-FLAIR mismatch indicates hyperacute ischemic stroke that occurred within the past 6 hours. [47]
Neurovascular studies [11][14][17][31]
- Goal: visualize intracranial and/or extracranial vascular occlusions and collateral vessels [14][38]
-
Indications
- Confirming the diagnosis in patients with high clinical suspicion for ischemic stroke and equivocal noncontrast neuroimaging
- Identify candidates for vascular recanalization
- Large vessel revascularization (e.g., carotid endarterectomy): e.g., patients with nondisabling stroke (modified Rankin scale < 2) in the territory of the carotid arteries
- Mechanical thrombectomy: patients with acute ischemic stroke presenting in a late time window (6–24 hours since time last seen normal)
- Timing: within 24 hours if not already done at admission
-
Options: Choose modality based on individual patient risks and resource availability.
- Advanced neuroimaging
- CTA head and neck (most common): often directly follows noncontrast CT head in many stroke neuroimaging protocols
- MR angiography head and neck
- Perfusion-weighted imaging: to assess the presence and size of the ischemic penumbra [17][30][49][50]
-
Ultrasound studies
- Carotid artery duplex: to evaluate extracranial vasculature
- Transcranial doppler: to evaluate intracranial vasculature [51]
- Digital subtraction angiography (DSA): Invasive, catheter-based gold standard for cerebral vessel assessment [52]
- Advanced neuroimaging
-
Findings
-
CTA/MR angiography [38]
- Large vessel occlusion(s)
- Vascular dissection (e.g., dissection of the carotid or vertebral artery)
- Carotid artery stenosis
- CT perfusion
- Ischemic penumbra: reduced cerebral blood flow and blood volume
- Ischemic core: severely reduced cerebral blood flow and blood volume PLUS increased mean transit time
- MR perfusion: A perfusion-diffusion mismatch indicates the presence of a potentially salvageable penumbra.
-
CTA/MR angiography [38]
In potential candidates for mechanical thrombectomy, perform CTA immediately following noncontrast CT. If indicated, thrombolysis can be performed simultaneously. [14]
If indicated, do not delay CTA to wait for creatinine or TSH levels, as the risk of iodine-induced hyperthyroidism and contrast-induced nephropathy is relatively low, especially in patients with no known history of thyroid or renal abnormalities. [36][40][53][54]


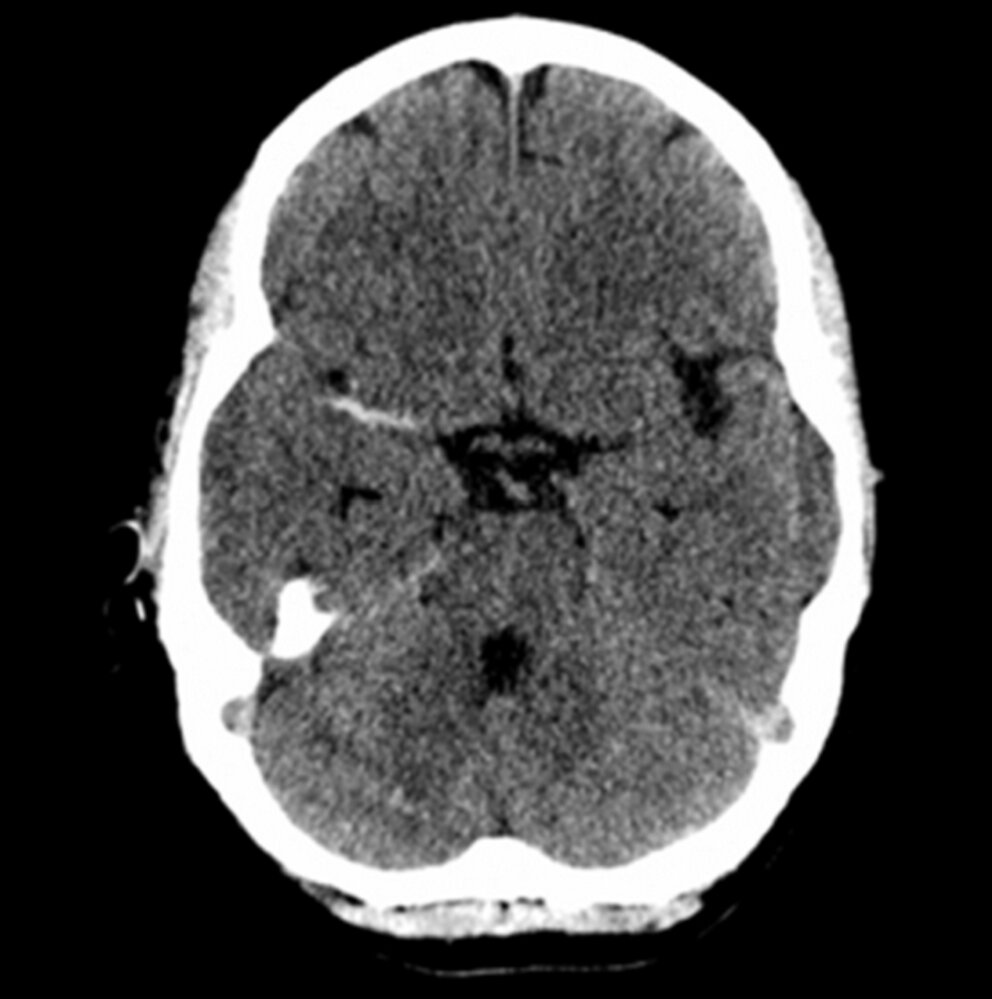
CT head (without contrast; axial plane)
The right middle cerebral artery (MCA; green overlay) is hyperdense compared to the regions of the left MCA (arrow) and tip of the basilar artery (red overlay).
The hyperdense MCA sign is a marker of middle cerebral artery thrombosis. This sign is visible before parenchymal changes of ischemia.
Source: “Figure 1a, in: Therapeutic Decision Making in Acute Stroke due to Carotid Artery Dissection: A Potential Role for Percutaneous Vascular Intervention following Intravenous Thrombolysis” by J. B. Lewis, Á. Merwick, R. Ó. Laoide et al., Hindawi - Case Reports in Vascular Medicine, licensed under CC BY 3.0. Modifications: removed white border and "a". The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
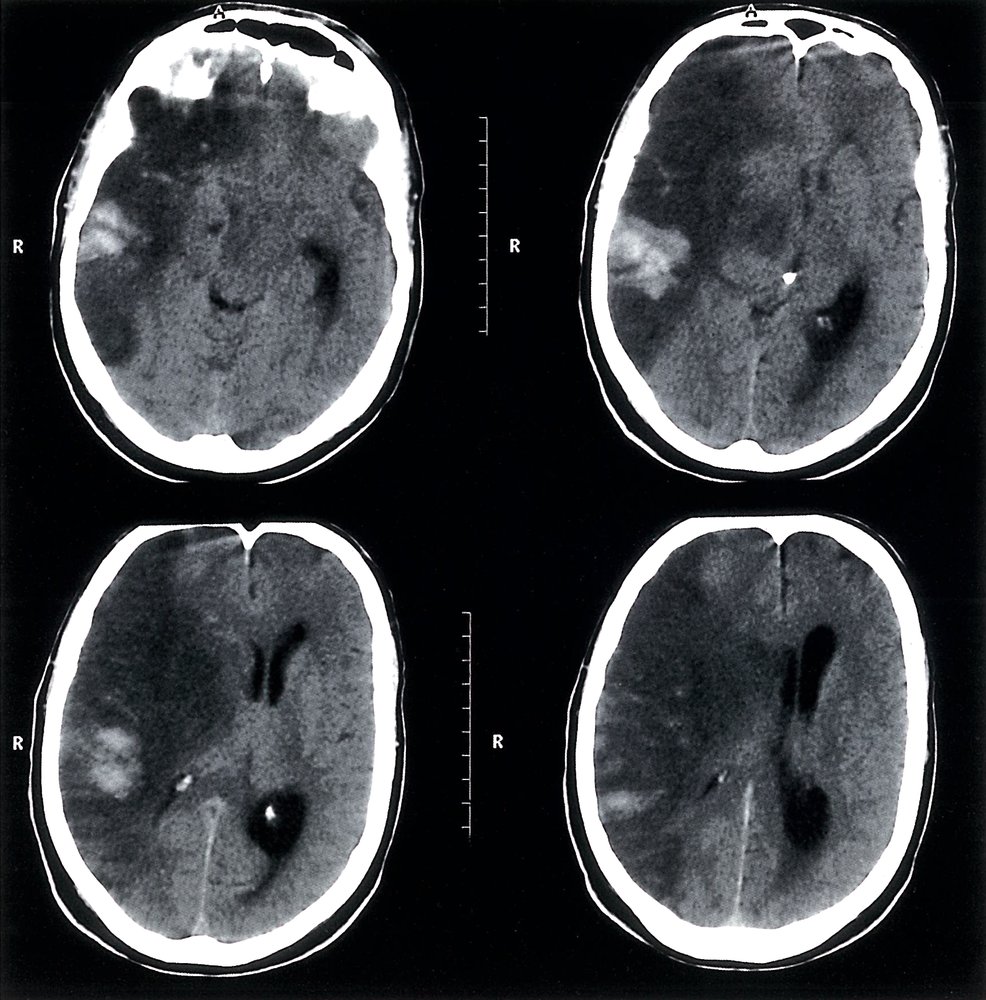
CT head (without contrast; axial plane)
The right cerebral hemisphere is hypodense (green overlay) in the distributions of the middle and anterior cerebral arteries. The presence of thromboembolic material has caused the right middle cerebral artery (MCA) to appear hyperdense (hyperdense-MCA sign; white arrowhead). Cerebral edema has resulted in effacement of the sulci and the loss of differentiation between the medulla and cortex. Accompanying mass effect has compressed the right lateral ventricle (red overlay) and caused slight contralateral shift of the midline (indicated by white arrow and dashed line).
Created by: Nándor Faluhelyi. Organization providing image: University of Pécs, Medical School. Further notes: Our great thanks to Nándor Faluhelyi (University of Pécs, Medical School) for kindly providing this case.
CT head (without contrast; axial plane)
Diffuse hypodensity (green overlay) involving the left anterior, middle, and posterior cerebral artery distributions is accompanied by sulcal effacement and a loss of gray-white matter differentiation. There is mild mass effect on the falx cerebri (blue line) and left lateral ventricle (red overlay).
Source: © IMPP
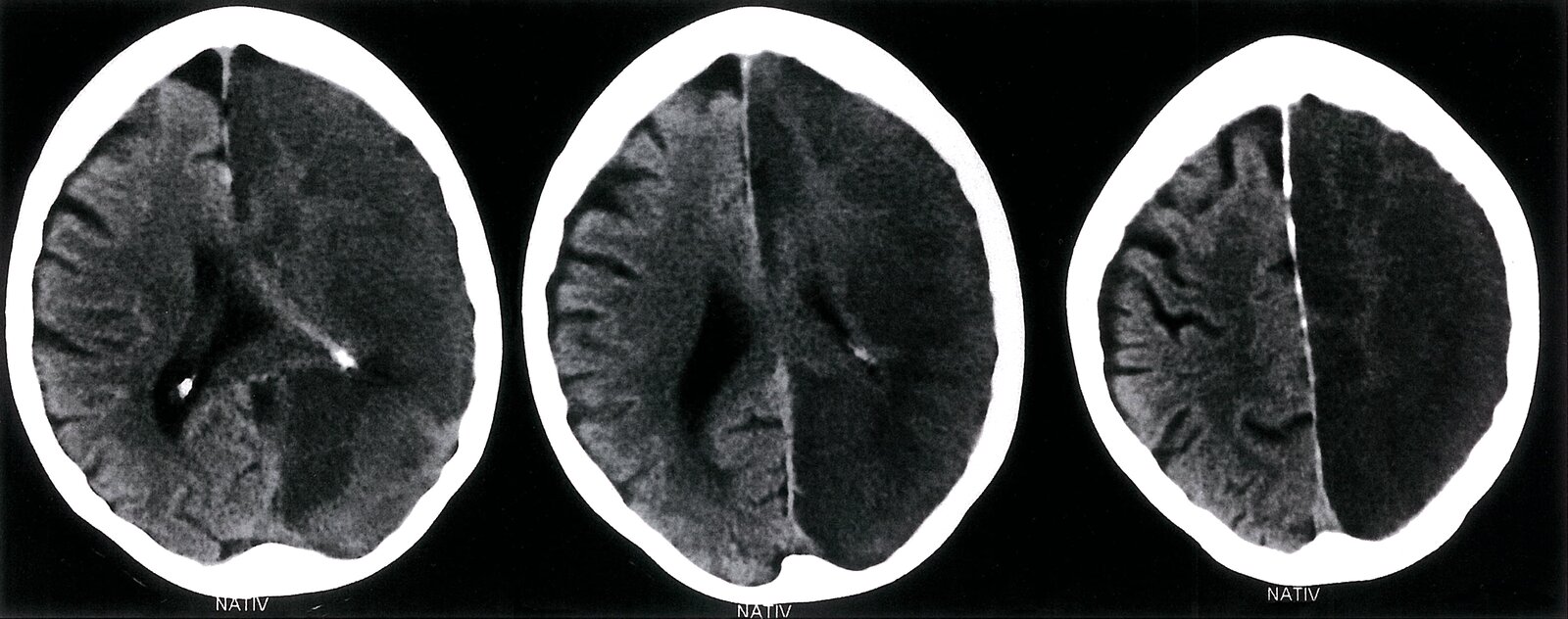
CT head (without contrast; axial plane)
Extensive hypodensity (green overlay) in the right middle cerebral artery distribution is accompanied by sulcal effacement and midline shift (dashed line and arrows) from edema. The right ventricle is compressed (red arrowheads), and the left ventricle is trapped and dilated (white arrowheads). Multiple hyperdense foci within the infarct represent areas of intraparenchymal hemorrhage (red overlay).
Source: © IMPP
CT head (without contrast; axial plane)
The left middle cerebral artery (green overlay) is hyperdense as a result of thromboembolic occlusion. Hypodensity with loss of gray-white matter differentiation in the left frontal, temporal, and parietal regions (red-dashed overlay) corresponds to an acute infarct in the middle cerebral artery distribution.
Source: “Dens media sign mit Mediainfarkt” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
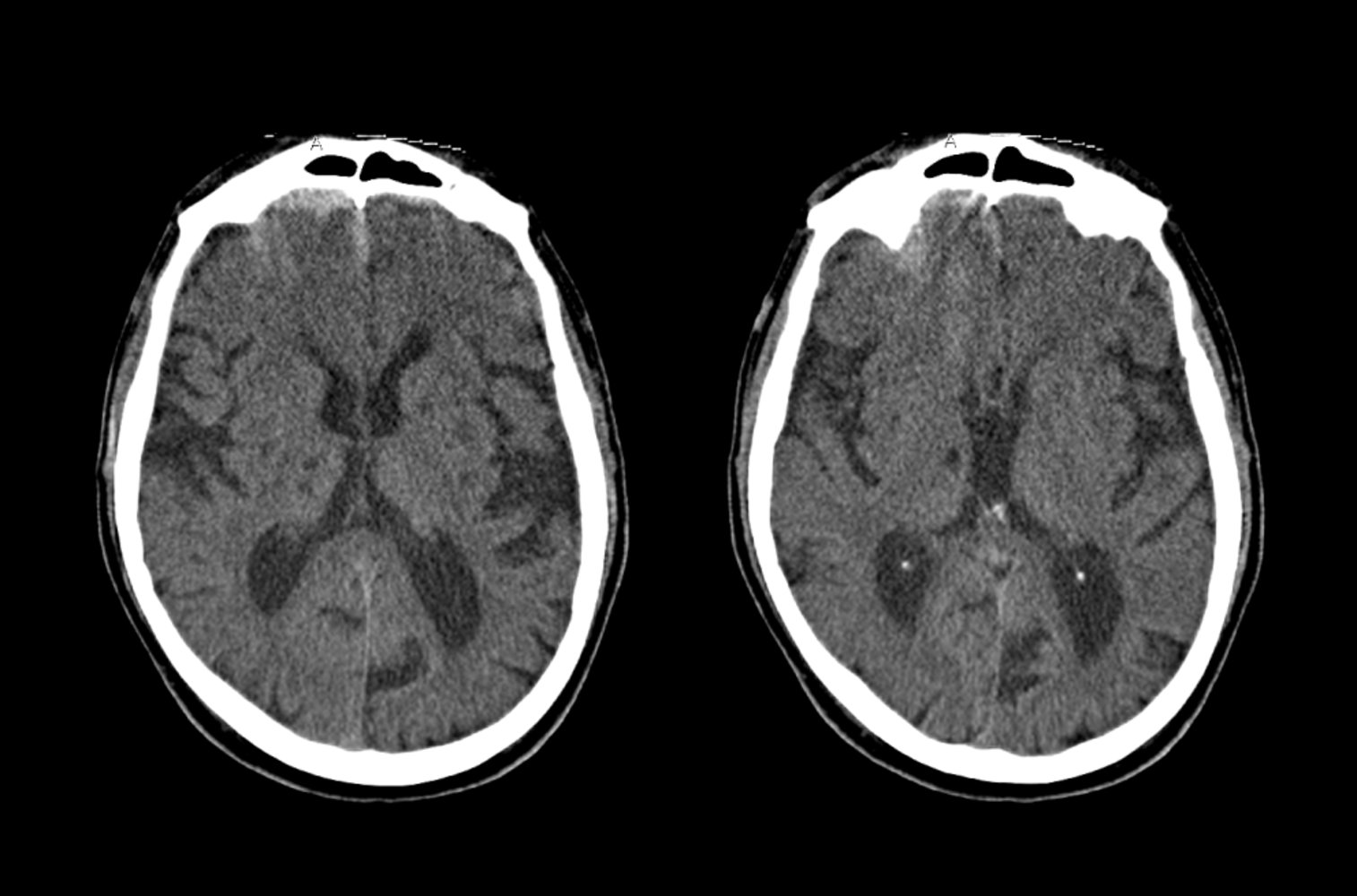
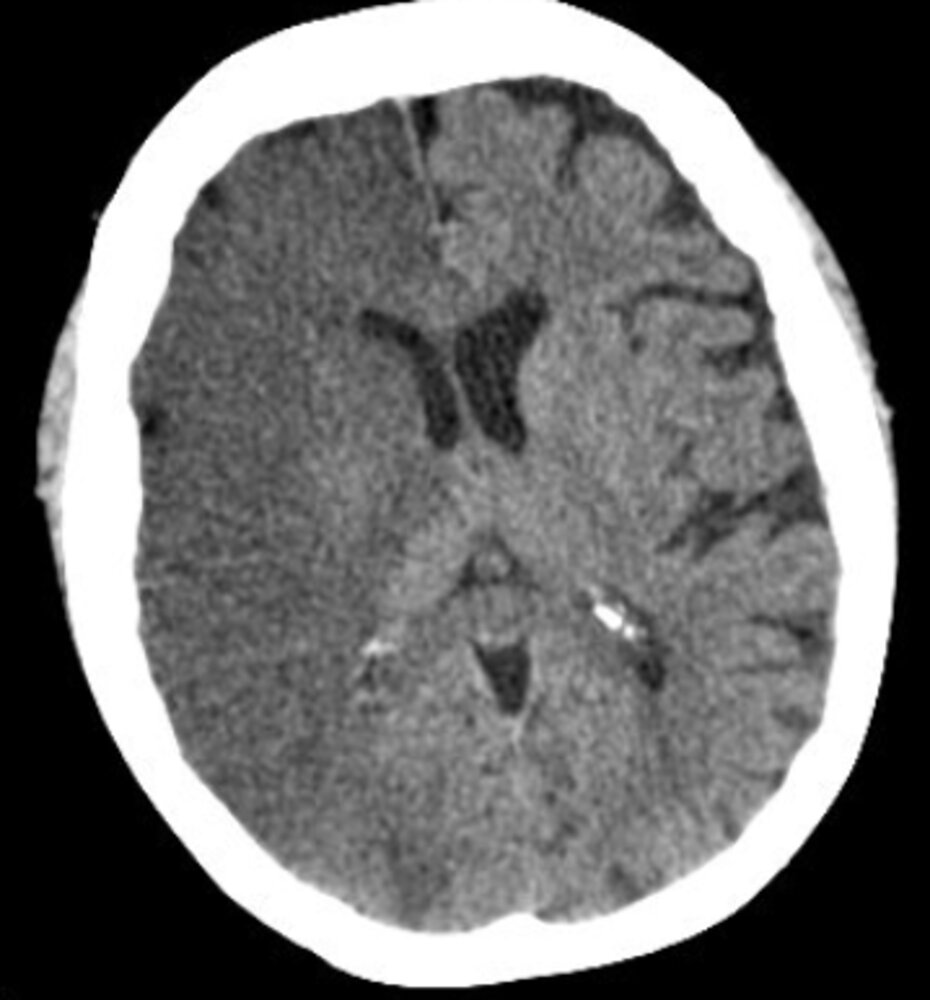
CT head (without contrast; axial plane)
Multiple, very small, sharply-demarcated hypodense lesions are present in the basal ganglia (green overlay), left internal capsule (blue overlay), and right thalamus (red overlay). Additionally, there is diffuse cerebral atrophy with prominence of the sulci and ventricles.
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.
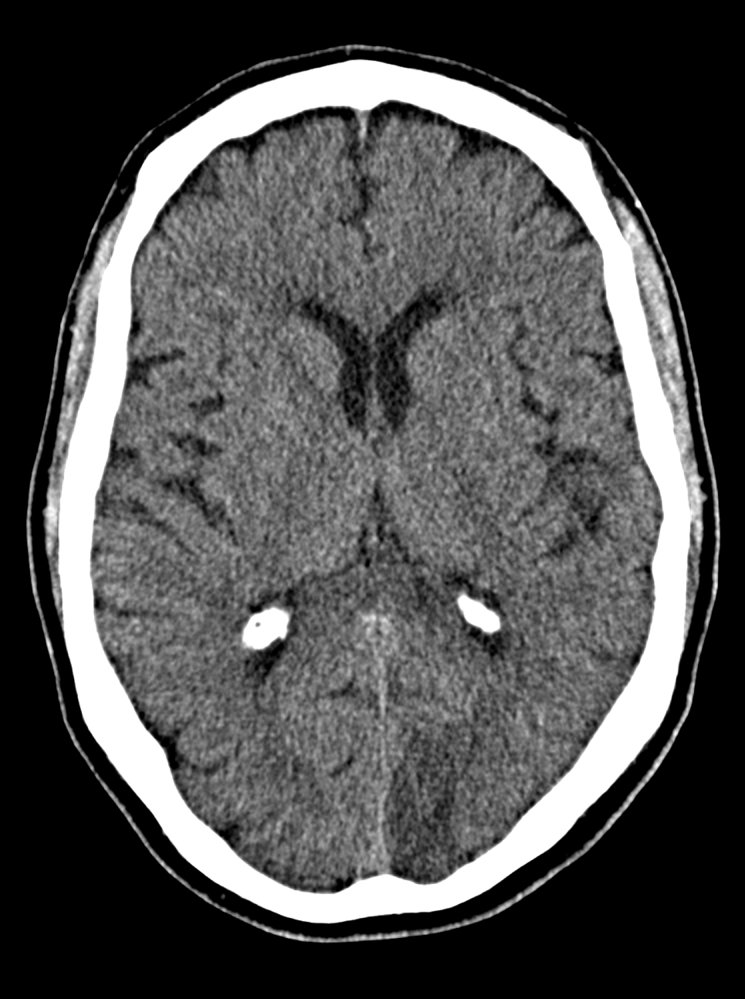
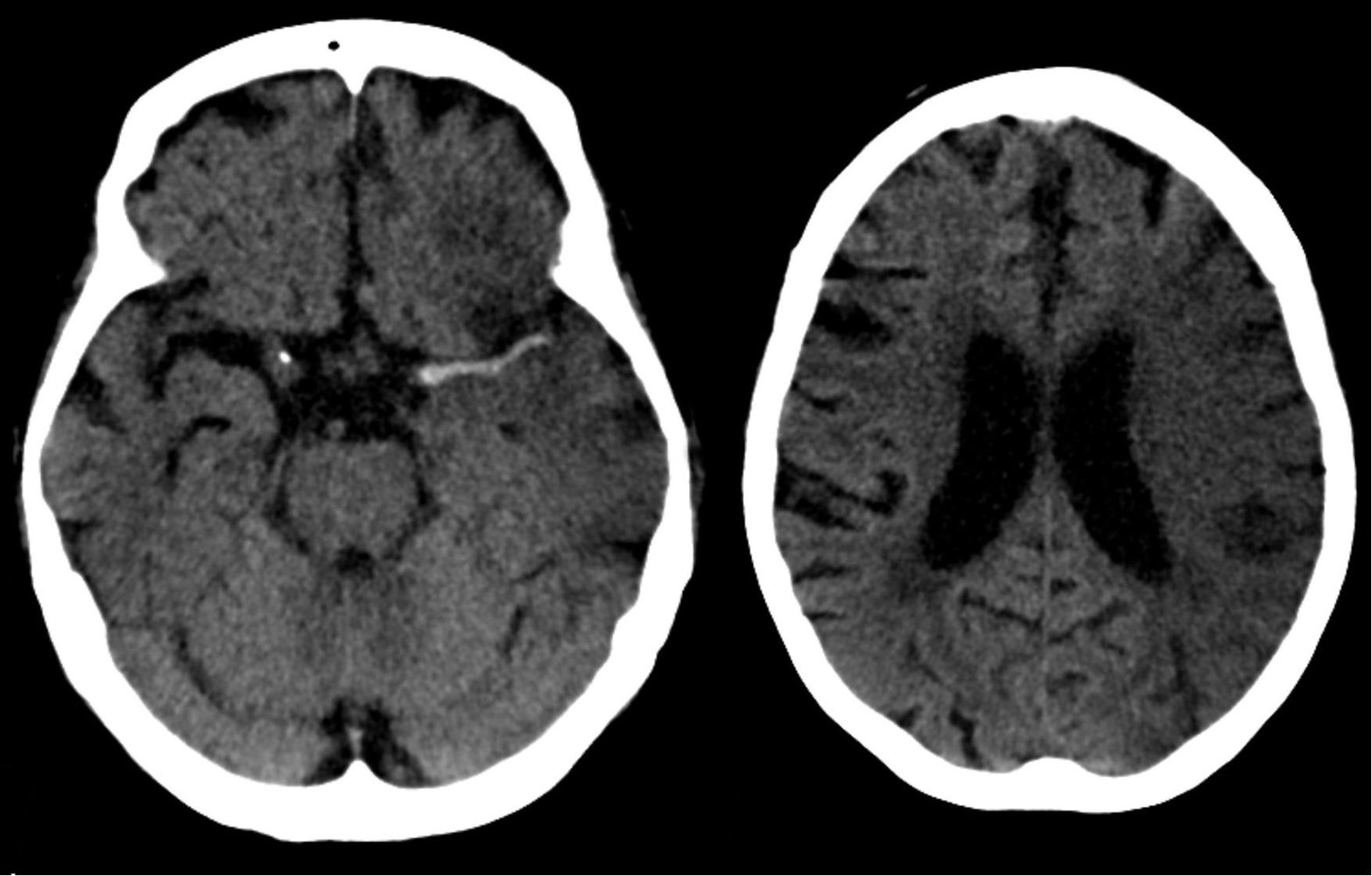
CT head (without contrast; axial plane)
A hypodense occipital infarct (green) in the distribution of the left posterior cerebral artery is accompanied by a loss of normal gray-white matter differentiation. The density of the lesion is greater than that of CSF. There is no mass effect or hemorrhage. Choroid plexus calcifications in the lateral ventricles are physiologic.
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.
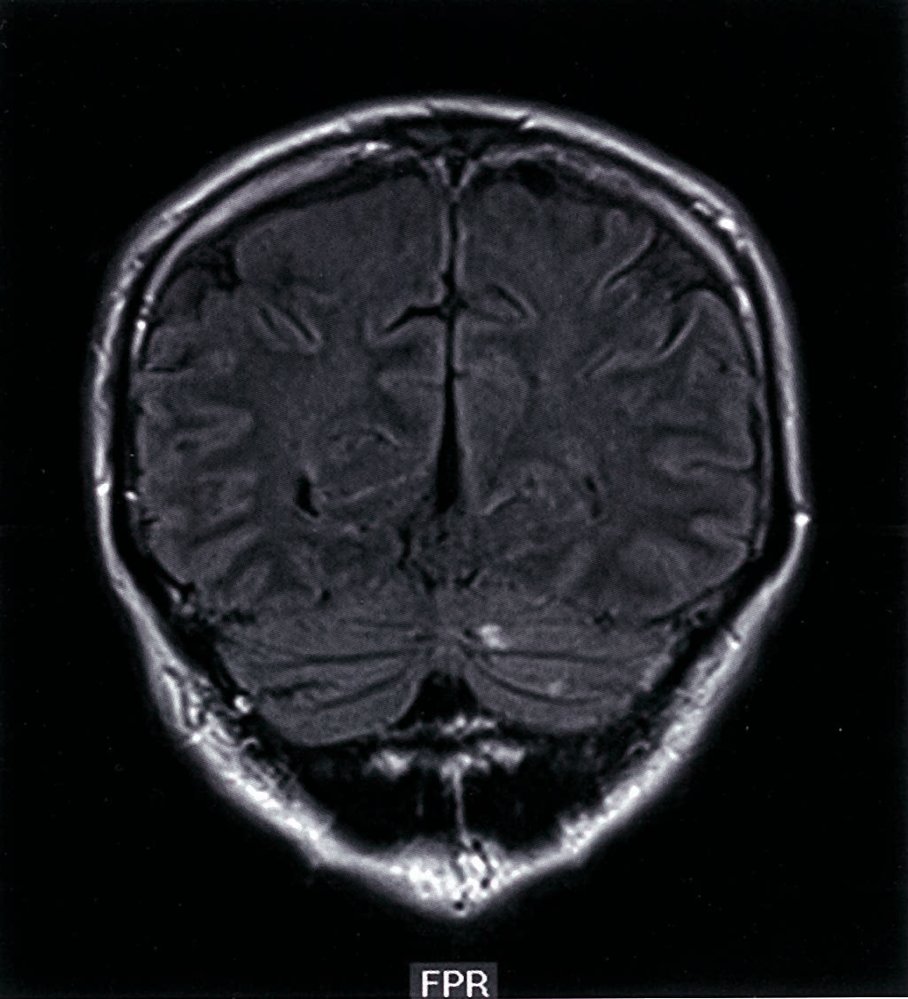
MRI head (T2-weighted FLAIR; coronal plane) of a patient with polycythemia vera
Small hyperintense lesions (green overlays) in the left cerebellum (Ce; green outline) not associated with mass effect are compatible with infarction.
Source: © IMPP
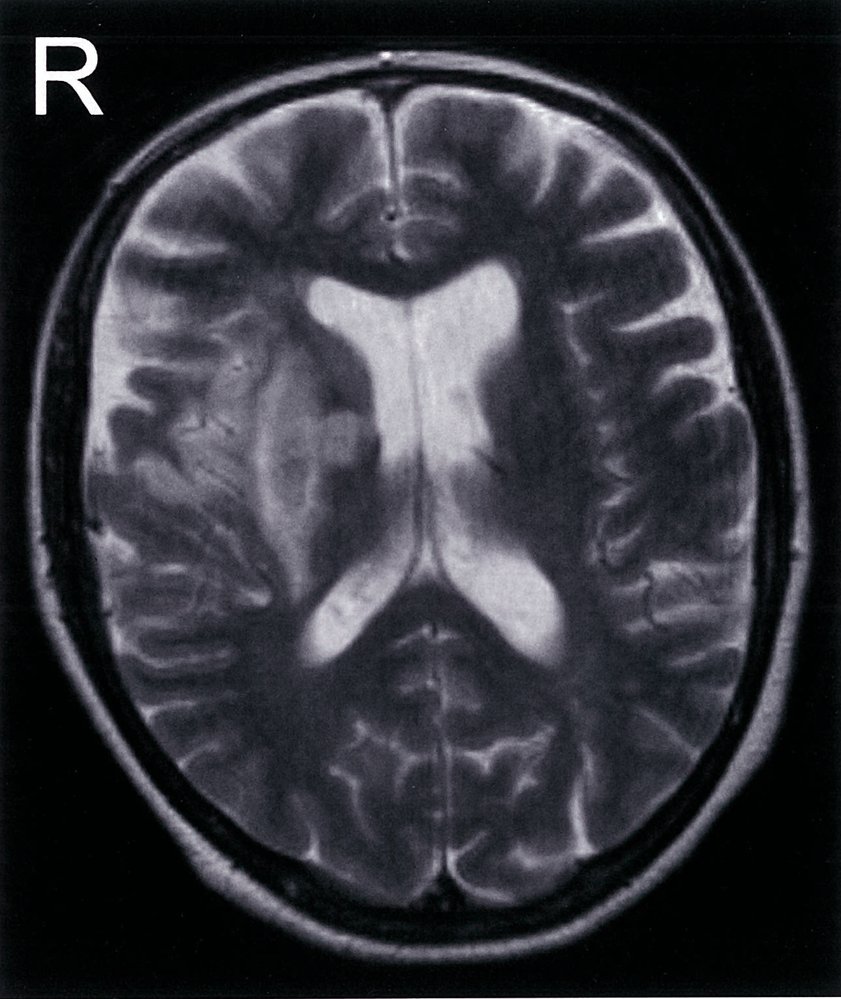
MRI head (T2-weighted; axial plane)
The lentiform nucleus, insular cortex, and genu of the internal capsule of the right cerebral hemisphere are hyperintense (green overlay), with a central hypointense area within the lentiform nucleus (red overlay). The findings are consistent with a right middle cerebral artery infarction with hemorrhagic transformation when the clinical findings are also compatible with this diagnosis.
Source: © IMPP
Pathology
Patterns of necrosis in ischemic stroke [55]
- General: infarction → liquefactive necrosis; → cystic cavity formation
- Two main responses to brain tissue ischemia
- Selective neuronal necrosis: more likely to occur with transient ischemia
- Pannecrosis: more likely to occur with irreversible ischemia (e.g., infarction)
- Irreversible neuronal injury begins ∼ 5 minutes after tissue hypoxia.
- See “Cellular changes and adaptive responses.”
Infarction of brain tissue is typically followed by liquefactive necrosis, in contrast to the coagulative necrosis seen after infarction in other organs.
Selective neuronal necrosis
- Definition: selective destruction of nerve cells with sparing of glial cells
-
Mechanism
- Transient ischemia → subsequent reperfusion (e.g., resuscitation following cardiac arrest) → increased metabolic demand, release of toxic excitatory neurotransmitters → ischemic injury
-
Certain neurons are more susceptible to ischemic injury.
- Pyramidal cells of the hippocampus: Damage causes anterograde amnesia.
- Purkinje cells of the cerebellum: Damage causes intention tremor, nystagmus, and ataxia.
- Pyramidal cells of neocortex: Symptoms depend on the affected brain region.
- Histology: neuronal necrosis with viable glial cells (which can proliferate and cause a laminar or pseudolaminar tissue architecture)

Pannecrosis
- Definition: the death of all cell types in a given region of the brain, including neurons, glial cells, and vascular cells
- Mechanism: permanent ischemia
- Histology: cystic lesions and loss of tissue architecture
Histologic changes in the infarcted region [55][56]
| Time from start of ischemia | Histologic features |
|---|---|
| 12–24 hours |
|
| 1–3 days |
|
| 3–5 days |
|
| 5–15 days |
|
| > 15 days |
|
-
Areas and cells most vulnerable to hypoxia
- Neocortex
- Hippocampus
- Purkinje cells (cerebellum)
- Watershed areas
The hippocampus, neocortex, Purkinje cells, and watershed areas are the areas most vulnerable to hypoxia: Vulnerable hippos Need PURe water.


References:[55][56]

Photograph of a section of a brain slice (coronal section)
The grey/white matter border can no longer be seen in some areas of the cortex (white arrows).
Source: © IMPP
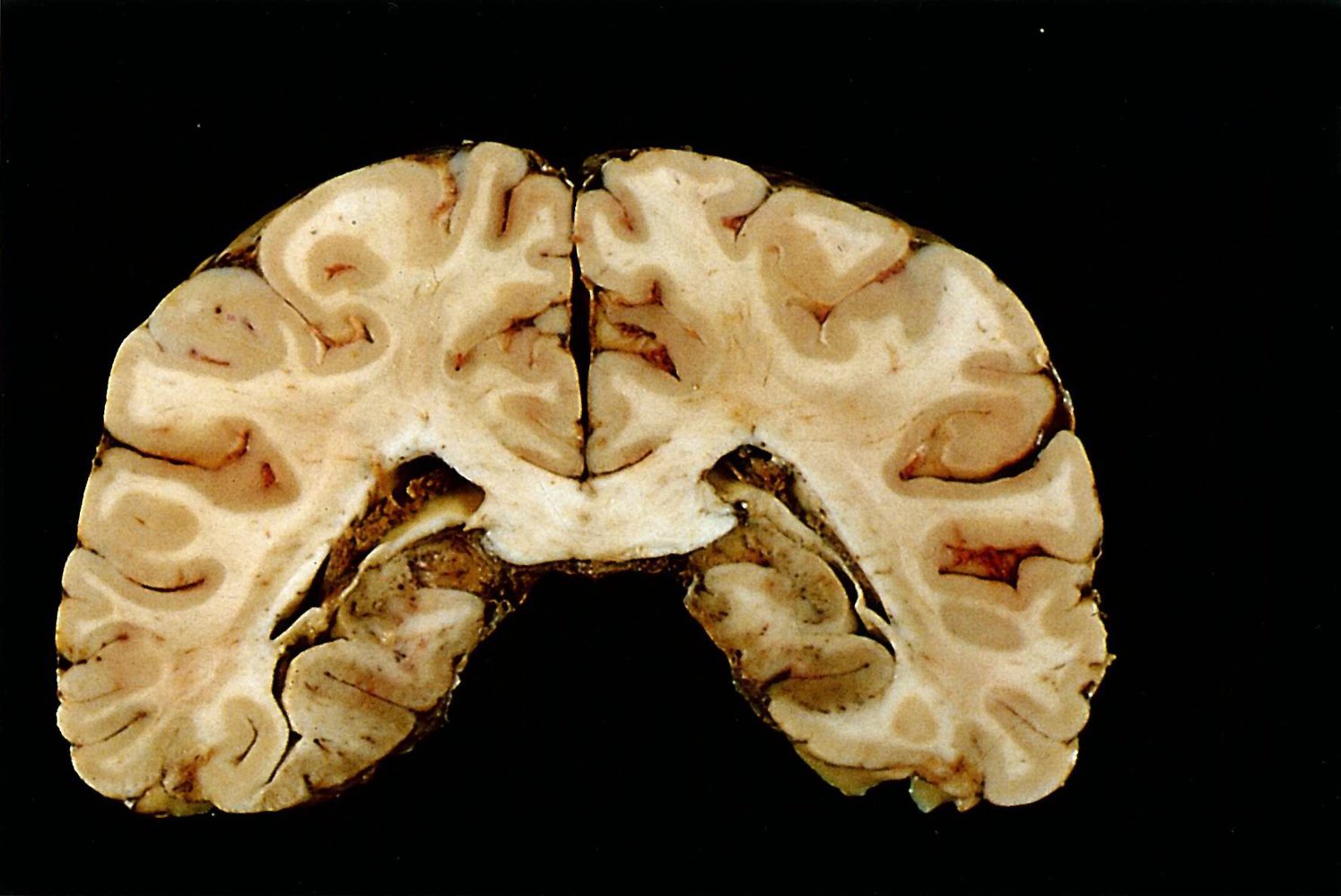
Coronal brain section
There is bilateral brown discoloration of the tissue below the posterior horn of the lateral ventricle and blurring of the cortex-medulla margin in the calcarine sulcus (red lines).
These findings are the result of thromboembolic infarcts of the posterior cerebral arteries (outlined in green).
A1: vascular territory of the anterior cerebral artery (green overlay); A2: middle cerebral artery (yellow overlay); A3: posterior cerebral artery (red overlay); 1: hippocampus; 3: corpus callosum; 4: lateral ventricle; 5: cingulate sulcus
Source: © IMPP
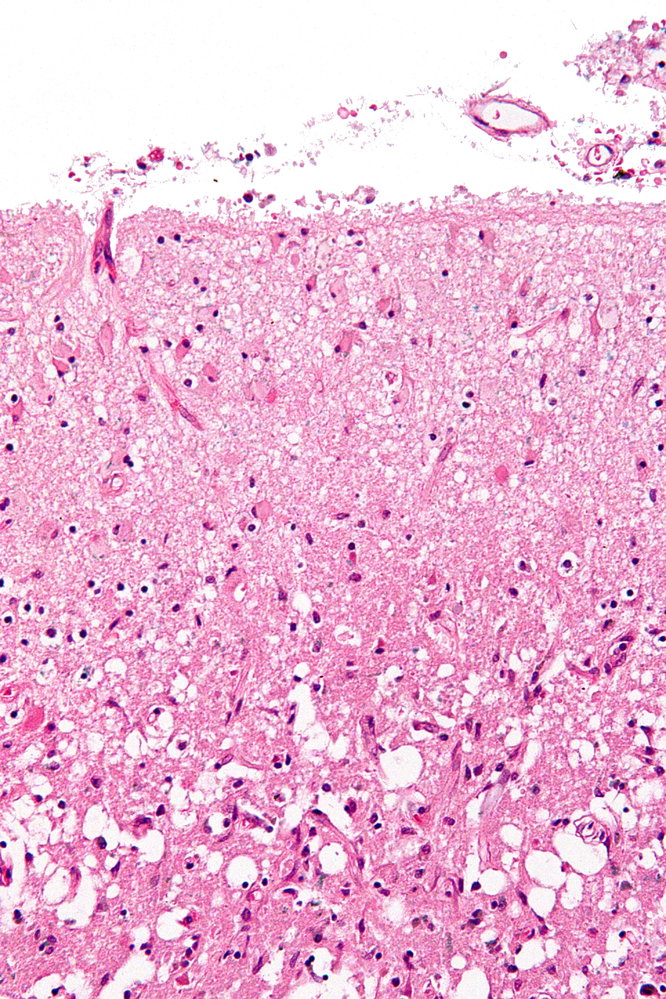
Photomicrograph of a brain biopsy sample (H&E stain)
Numerous deeply staining nuclei surrounded by unstained areas are visible throughout the microscopic field. This “naked nuclei” appearance is characteristic of astrocytes on an H&E stain.
Astrocytic proliferation and hypertrophy (astrocytosis) indicate reactive gliosis (or CNS scarring), which occurs secondary to CNS injury.
Source: “Reactive astrocytes - lfb - high mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
Treatment
Therapeutic approach [14]
- Treat all eligible patients with reperfusion therapy for acute ischemic stroke within recommended time frames.
- Continue supportive care for ischemic stroke including neuroprotective measures.
-
Initiate measures for reducing subsequent stroke risk.
- Start antiplatelet treatment with aspirin or clopidogrel within 24–48 hours after symptom onset.
- Treat underlying conditions: e.g., atrial fibrillation, carotid artery stenosis, carotid or vertebral artery dissection
- Reduce modifiable risk factors: e.g., smoking, hypertension, hyperlipidemia, diabetes
- Monitor and treat any complications.
- Provide early rehabilitation and mobilization.
Reperfusion therapy
General principles [14]
- Identify eligible candidates and initiate treatment as soon as possible.
- Goal: to prevent further tissue ischemia and irreversible infarction
- Commonly used treatment options include intravenous thrombolytic therapy and mechanical thrombectomy.
- The effectiveness of intraarterial thrombolysis is unclear.
Time is brain! Reperfusion therapy should not be delayed. However, intracranial hemorrhage is a contraindication for reperfusion therapy and must be ruled out first.
Intravenous thrombolysis [14]
Inclusion and exclusion criteria for thrombolysis are not strict and treatment decisions should be made in consultation with a neurologist taking into account multiple individual patient factors.
-
Agents: intravenous recombinant tissue plasminogen activator (tPA)
- Alteplase
- OR tenecteplase [14][17][57]
-
Inclusion criteria
- No evidence of stroke mimic or intracranial hemorrhage
- Acute disabling neurological symptoms
-
Time from onset of symptoms or last seen normal (or at baseline)
- < 3 hours: patients ≥ 18 years old with any disabling stroke (including mild disabling or severe stroke) [14]
- 3–4.5 hours: select patients (consult neurology)
- Unclear symptom onset > 4.5 hours from last known baseline state (e.g., wake-up stroke): MRI findings determine whether thrombolysis is indicated.
If a patient is unable to consent to treatment (e.g., altered mental status, aphasia) and a legal representative is not immediately present, IV alteplase can still be administered in eligible patients with disabling stroke symptoms. [14]
Do not wait on coagulation parameters before administering tPA in patients with no known history of coagulopathy or thrombocytopenia. Discontinue treatment if platelets are < 100,000/mm3, INR > 1.7 or PT is abnormally elevated. [14]
| Exclusion criteria for thrombolysis in acute ischemic stroke [14] | ||
|---|---|---|
| Absolute contraindications | Relative contraindications | |
| Preexisting conditions |
|
|
| Acute findings |
|
|
Some conditions commonly misconceived as contraindications for thrombolysis therapy include antiplatelet therapy, end-stage renal disease, and concurrent MI. In patients with preexisting disability or dementia, treatment decisions should be based on prestroke functionality and quality of life. [14][59]
Severe hypo- or hyperglycemia (glucose < 50 mg/dL or > 400 mg/dL) and severe hypertension > 185/110 mm Hg should be treated before tPA administration. [14]
Complications of IV thrombolytic therapy [14]
-
Angioedema: can compromise airway
- Stop tPA infusion and any ACE inhibitors.
- Secure difficult airway: See “Management of angioedema.”
- Medication protocol: differs from standard treatment of bradykinin-mediated angioedema.
- Administer in rapid sequence.
- Methylprednisolone
- Diphenhydramine
- Famotidine
- If edema progresses despite initial treatment: Administer epinephrine OR icatibant . [14]
- Administer in rapid sequence.
-
Intracranial hemorrhage: suspect if sudden neurological deterioration or headache
- Stop tPA infusion and obtain immediate noncontrast head CT.
- Order urgent CBC, coagulation panel, fibrinogen level, blood type and screen, crossmatching.
- Consult neurosurgery and hematology.
- Administer cryoprecipitate .
- Administer tranexamic acid OR ε-aminocaproic acid .
- Maintain neuroprotective measures.
- See also “Intracerebral hemorrhage.”
- Extracranial hemorrhage: Specific management depends on the site and severity of bleeding.
Additional measures after thrombolysis
- Check blood pressure and neurological status frequently.
- Avoid invasive procedures, if possible.
- Obtain a follow-up head CT (without IV contrast) or brain MRI 24 hours after thrombolysis, prior to starting anticoagulants or antiplatelet agents.
Mechanical thrombectomy [14]
-
Description
- Physical retrieval or aspiration of the occluding thrombus via the femoral artery using a stent retriever and/or an aspiration catheter
- Must be performed at a dedicated stroke center
-
Inclusion criteria [14]
- Age ≥ 18 years
- Acute large artery occlusion; causing a stroke: e.g., proximal artery occlusion in anterior cerebral circulation (M1) or occlusion of the internal carotid artery [17]
- Disabling stroke symptoms (NIHSS ≥ 6)
- Limited affected area on CT (Alberta Stroke Program Early CT Score ≥ 6)
- Previously independent in ADLs (prestroke modified Rankin scale (mRS) ≤ 1)
- Patients with symptom onset within the past 6 hours or selected patients with symptom onset between 6 and 24 hours ago
Patients who are eligible for tPA should receive thrombolysis immediately, while mechanical thrombectomy is being considered. If indicated, mechanical thrombectomy should be performed without delay to assess the response to thrombolysis. [14][60]
Supportive care and neuroprotective measures
Neuroprotective measures
Follow standard measures, including the following specific targets for acute ischemic stroke: [14]
-
Targeted temperature management: treat any temperature > 38°C
- Goals: Maintain normothermia and avoid neurogenic fever.
- Hypothermia is not recommended in acute ischemic stroke.
-
Glucose management for secondary brain injury prevention
- Hypoglycemia: Treat if blood glucose is < 60 mg/dL.
- Hyperglycemia; : Treat to maintain blood glucose levels in a range of 140 to 180 mg/dL [14]
- Blood pressure: see “Blood pressure management in acute ischemic stroke” for details.
Supportive care
-
Dysphagia screening
- Keep patient NPO until the risk of aspiration has been assessed.
- See “Dysphagia” for further information on diagnostics and management.
-
VTE prophylaxis: in addition to antiplatelet therapy and hydration [14]
- Mechanical VTE prophylaxis is preferred: intermittent pneumatic compression (IPCs).
- Benefits of pharmacological VTE prophylaxis are unclear.
-
Early rehabilitation and mobilization
- Start normal enteral diet within 7 days if possible.
- Order physiotherapy, occupational therapy, and speech therapy. [61]
- Screen for depression. [14]
Reducing subsequent stroke risk
Further therapeutic goals consist of identifying and treating risk factors and underlying conditions to prevent recurrent stroke. [14][33]
Antiplatelet therapy [14][31][33]
-
Starting within first 24–48 hours after symptom onset
- Aspirin
- OR clopidogrel
- Dual antiplatelet therapy (DAPT): Consider starting 21-day course in patients with minor stroke symptoms (e.g., NIHSS ≤ 3–5), aspirin AND clopidogrel [22]
-
Long-term antiplatelet therapy
- Indicated in patients with noncardioembolic stroke to reduce the risk of recurrence
- Choose an agent based on individual risk factors, e.g., aspirin , clopidogrel , or combination therapy. [62][63]
- Consult neurology for indication in patients with cardioembolic stroke and significant atherosclerosis. [14]
Wait at least 24 hours before initiating antiplatelet treatment after thrombolysis.
Management of underlying causes [14][31][33]
Large vessel disease
- All patients: Optimize medical management.
-
Extracranial artery stenosis
- Carotid artery stenosis: Consider carotid endarterectomy or carotid artery stenting patients with relevant ipsilateral stenosis within 2–7 days of the event.
- Vertebral artery stenosis: intensive medical therapy advised (see “Treatment of modifiable risk factors”)
-
Intracranial artery stenosis
- 50–99%
- Aspirin is preferred over warfarin.
- Target BP < 140/90 mm Hg, start high-intensity statin, and advise at least moderate physical activity
- 70–99%: Consider adding clopidogrel to aspirin for up to 90 days
- Routine angioplasty, stenting, and bypass surgery are discouraged.
- 50–99%
- Arterial dissection: treatment with antithrombotic agents for 3–6 months
Cardioembolic sources
-
Atrial fibrillation or atrial flutter: anticoagulation with warfarin or direct oral anticoagulant is indicated regardless of frequency or persistence.
- Agents and dosages: See “Anticoagulation regimens in atrial fibrillation.”
- Timing: depends on risk of hemorrhagic conversion (specialist consultation advised)
- High risk (e.g., large infarct territory): Consider delaying > 14 days.
- Low risk: can start in 2–14 days
- Avoid concurrent oral anticoagulation and antiplatelet therapy, except in specific circumstances.
- Patent foramen ovale: Initiate antiplatelet therapy and refer to neurologist and cardiologist to consider PFO closure.
- LV thrombus or cardiomyopathy with left atrial thrombus: anticoagulation for 3 months
-
Valvular heart disease and/or prosthetic valve
- Valvular AF: anticoagulation with warfarin
- Mechanical valve (mitral) and stroke prior to surgery: aspirin PLUS warfarin
- Other valvular diseases without another indication for anticoagulation: antiplatelet therapy typically preferred.
- Patients already on anticoagulation for stroke prevention: Consult neurology regarding management in the immediate post-stroke period. [64][65]
- Hypercoagulable states: See “Thrombophilia therapy.”
Consult neurology for patients who experience breakthrough stroke while on antithrombotic therapy.
Treatment of modifiable risk factors [31]
Management of ASCVD
-
Lifestyle modifications for ASCVD prevention
-
Smoking: Offer counseling on smoking cessation.
- Advise smoking cessation or reduction for those who cannot discontinue tobacco.
- Avoid second-hand smoke exposure.
- Consider pharmacotherapy: e.g., nicotine replacement (gums, patches), varenicline, bupropion
- Diet and exercise
- A heart-healthy diet, e.g., a Mediterranean diet, is preferred over a low-fat diet.
- Patients who can exercise
- Moderate intensity: minimum 10 minutes 4 times/week
- High intensity: minimum 20 minutes 2 times/week
- Patients who cannot exercise: Refer to physical therapy and rehabilitation.
-
Smoking: Offer counseling on smoking cessation.
-
Lipid-lowering therapy for ASCVD
- No coronary artery disease or cardioembolic source and LDL cholesterol > 100 mg/dL: Start atorvastatin .
- Other ASVCD present: lipid-lowering therapy with statin ± ezetimibe to a target LDL cholesterol < 70 mg/dL
-
Management of comorbidities
-
Management of hypertension
- Recommend lifestyle changes for managing hypertension, e.g., reducing sodium intake.
-
Antihypertensives: for patients with known hypertension or sustained average BP ≥ 130/80 mm Hg
- Target BP < 130/80 mm Hg [31]
- Preferred agents: thiazide diuretics, ACE-Is, ARBs
- Optimize agent and dosage on an individual basis.
- Management of diabetes mellitus: glycemic control with antihyperglycemics as needed to maintain HbA1c < 7%
-
Management of hypertension
The single most important treatable risk factor for preventing recurrent stroke is hypertension.
Other modifiable risk factors
-
Management of obesity: Weight loss is recommended.
- Screen BMI of all patients.
- Provide directed counseling on weight and diet changes and referral to comprehensive weight loss program.
- Obstructive sleep apnea (OSA): Consider screening in patients with risk factors for OSA, and CPAP therapy for established OSA.
-
Substance use
- Alcohol consumption: Eliminate OR reduce to ≤ 2 drinks/day for men and ≤ 1 drink/day for women.
- Provide counseling on substance use disorders and rehabilitation referrals for the following:
- Patients using CNS stimulants
- Patients with infectious endocarditis due to IV substance use
Acute management checklist
Initial evaluation
- Perform primary survey.
- Determine the time of onset of symptoms and assess severity with NIHSS.
- Call for immediate neurology consult or activate stroke team.
- Establish IV access.
- Continuous cardiac monitoring
- Start supplemental O2 to keep SpO2 > 94%.
- Obtain POC glucose and treat immediately if < 60 mg/dL or > 400 mg/dL.
- Order immediate head CT (without contrast).
- Stabilize patient prior to neuroimaging as needed.
- Intubation and mechanical ventilation for airway protection or respiratory failure
- Blood pressure management for acute ischemic stroke for shock or hypertensive emergency
- Begin ICP management for cerebral herniation syndromes.
- Consider further imaging (e.g., MRI or CTA with or without perfusion protocol) without delaying reperfusion therapy.
- Evaluate inclusion and exclusion criteria for thrombolysis in consultation with neurology.
- If thrombolysis is indicated:
- Lower blood pressure to < 185/110 mm Hg.
- Administer thrombolytic therapy (per neurologist).
- Evaluate indications for mechanical thrombectomy in discussions with stroke specialists.
After stabilization
- Admit preferentially to stroke unit (medicine or neurology) or ICU for first 24 hours.
- Continue blood pressure management and other neuroprotective measures (e.g., euglycemia, normothermia).
- Perform serial neurological assessments.
- Identify and treat the underlying cause: ECG, laboratory studies, neurovascular studies.
- Ensure supportive care: e.g., NPO and dysphagia screening, VTE prophylaxis, physical and occupational therapy.
- Identify and treat any complications (e.g., seizures, neurogenic fever).
- Start measures for reducing subsequent stroke risk (e.g., antiplatelet therapy, statins).
- Obtain 24-hour follow-up imaging, if indicated (post thrombolysis).
Differential diagnoses
- Transient ischemic attack
- See “Stroke mimics.”
- See “Weakness and paralysis.”
- See “Vertigo.”
The differential diagnoses listed here are not exhaustive.
Complications
- See “Complications” in “Overview of stroke.”
- Embolic strokes are more likely to undergo hemorrhagic conversion than thrombotic strokes.
We list the most important complications. The selection is not exhaustive.
Prevention
See “Primary prevention of stroke.”
Related One-Minute Telegram
- One-Minute Telegram 140-2026-2/3: Playing the long game: lipoprotein(a) predicts 30-year cardiovascular risk in women
- One-Minute Telegram 103-2024-3/3: A missed CHANCE: colchicine does not prevent early recurrent stroke
- One-Minute Telegram 100-2024-3/3: Blood pressure management in undifferentiated stroke: one size does not fit all
- One-Minute Telegram 83-2023-2/3: The OPTIMAL-BP after endovascular thrombectomy for stroke
- One-Minute Telegram 59-2022-1/3: Sugar free is not risk free
- One-Minute Telegram 59-2022-2/3: Asporvapril? Ramaspastatin? Single polypill for secondary ASCVD prevention better than usual care
- One-Minute Telegram 35-2021-1/3: Time is brain: mobile stroke units and patient outcomes in early stroke
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- Sacco RL, Kasner SE, Broderick JP, et al. "An Updated Definition of Stroke for the 21st Century". Stroke. 44(7). :2064-2089. (2013)
- "Stroke Facts". https://web.archive.org/web/20170519160313/https://www.cdc.gov/stroke/facts.htm. [2016-12-30]
- Appelros P, Stegmayr B, Terént A. "Sex differences in stroke epidemiology: a systematic review". Stroke. 40(4). (2009)
- Meschia JF, Bushnell C, Boden-Albala B, et al. "Guidelines for the Primary Prevention of Stroke". Stroke. 45(12). :3754-3832. (2014)
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161
- Caplan LR, Kasner SE, Dashe JF. "Etiology, Classification, and Epidemiology of Stroke". UpToDate. UpToDate. https://www.uptodate.com/contents/etiology-classification-and-epidemiology-of-stroke. [2017-03-14]
- Oliveira Filho J. "Lacunar infarcts". UpToDate. UpToDate. https://www.uptodate.com/contents/lacunar-infarcts. [2017-03-09]
- Furie KL, Rost NS. "Overview of secondary prevention of ischemic stroke". UpToDate. UpToDate. http://www.uptodate.com/contents/overview-of-secondary-prevention-of-ischemic-stroke. [2016-09-01]
- Oliveira Filho J, Mullen MT. "Initial assessment and management of acute stroke". UpToDate. UpToDate. http://www.uptodate.com/contents/initial-assessment-and-management-of-acute-stroke. [2016-08-15]
- Yew KS, Cheng EM. "Diagnosis of Acute Stroke". Am Fam Physician. 91(8). :528-536. (2015)
- EC J, JL S, Jr AH, et al. "Guidelines for the Early Management of Patients With Acute Ischemic Stroke". Stroke. 44(3). :870-947. (2013)
- De Lucas EM, Sánchez E, Gutiérrez A, et al. "CT Protocol for Acute Stroke: Tips and Tricks for General Radiologists". RadioGraphics. 28(6). :1673-1687. (2008)
- Tomandl BF, Klotz E, Handschu R, et al. "Comprehensive Imaging of Ischemic Stroke with Multisection CT". RadioGraphics. 23(3). :565-592. (2003)
- Srinivasan A, Goyal M, Azri FA, Lum C. "State-of-the-Art Imaging of Acute Stroke". RadioGraphics. 26. :S75-S95. (2006)
- Kleindorfer DO, Towfighi A, Chaturvedi S, et al. "2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association". Stroke. (2021)
- Powers WJ, Rabinstein AA, Ackerson T, et al. "Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association". Stroke. 50(12). (2019)
- Mayer SA, Viarasilpa T, Panyavachiraporn N, et al. "CTA-for-All". Stroke. 51(1). :331-334. (2020)
- Kernan WN, Ovbiagele B, Black HR et al. "Guidelines for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack". Stroke. 45(7). :2160-2236. (2014)
- Morris JG, Duffis EJ, Fisher M. "Cardiac Workup of Ischemic Stroke". Stroke. 40(8). :2893-2898. (2009)
- Easton JD, Saver JL, Albers GW, et al. "Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease.". Stroke. 40(6). :2276-93. (2009)
- Davenport M, Wang C, Asch D. "ACR Manual on Contrast Media". American College of Radiology. (2021). ISBN: 9781559030120
- Curry NS, Davenport R, Pavord S, et al. "The use of viscoelastic haemostatic assays in the management of major bleeding". Br J Haematol. 182(6). :789-806. (2018)
- Venkataraman P, Lui F. "Lacunar Syndromes". StatPearls. (2018)
- Standring S. "Gray's Anatomy: The Anatomical Basis of Clinical Practice". Elsevier Health Sciences. (2016). ISBN: 9780702052309
- Goljan EF. "Rapid Review Pathology". Elsevier Saunders. (2018). ISBN: 9780323476683
- Mena H, Cadavid D, Rushing EJ. "Human cerebral infarct: a proposed histopathologic classification based on 137 cases". Acta Neuropathol. 108(6). :524-530. (2004)
- Brott T, Adams HP, Olinger CP, et al. "Measurements of acute cerebral infarction: a clinical examination scale.". Stroke. 20(7). :864-870. (1989)
- Adams HP, Davis PH, Leira EC, et al. "Baseline NIH Stroke Scale score strongly predicts outcome after stroke: A report of the Trial of Org 10172 in Acute Stroke Treatment (TOAST)". Neurology. 53(1). :126-126. (1999)
- Lo BM, Carpenter CR, Ducey S, et al. "Clinical Policy: Critical Issues in the Management of Adult Patients Presenting to the Emergency Department With Acute Ischemic Stroke". Ann Emerg Med. 82(2). :e17-e64. (2023)
- Shah S, Luby M, Poole K, et al. "Screening with MRI for Accurate and Rapid Stroke Treatment: SMART". Neurology. 84(24). :2438-2444. (2015)
- Prasad K, Siemieniuk R, Hao Q, et al. "Dual antiplatelet therapy with aspirin and clopidogrel for acute high risk transient ischaemic attack and minor ischaemic stroke: a clinical practice guideline". BMJ. 363. :k5130. (2018)
- Hackam DG, Spence JD. "Antiplatelet Therapy in Ischemic Stroke and Transient Ischemic Attack". Stroke. 50(3). :773-778. (2019)
- Lansberg MG, O’Donnell MJ, Khatri P, et al. "Antithrombotic and Thrombolytic Therapy for Ischemic Stroke: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines". Chest. 141(2). :e601S-e636S. (2012)
- Rigual R, Rodríguez-Pardo J, Lorenzo-Diéguez M, et al. "Keeping prior anticoagulation treatment in the acute phase of ischaemic stroke: the REKOALA study". J Neurol. 271(7). :4086-4094. (2024)
- Groot AE, Vermeij JDM, Westendorp WF, et al. "Continuation or Discontinuation of Anticoagulation in the Early Phase After Acute Ischemic Stroke". Stroke. 49(7). :1762-1765. (2018)
- Winstein CJ, Stein J, Arena R, et al. "Guidelines for Adult Stroke Rehabilitation and Recovery". Stroke. 47(6). (2016)
- "NIH Stroke Scale". https://www.stroke.nih.gov/resources/scale.htm
- Meyer BC, Lyden PD. "The Modified National Institutes of Health Stroke Scale: its Time has Come". International Journal of Stroke. 4(4). :267-273. (2009)
- Fischer U, Baumgartner A, Arnold M, et al. "What Is a Minor Stroke?". Stroke. 41(4). :661-666. (2010)
- Haydel MJ, Garmel GM. "An Introduction to Clinical Emergency Medicine". Cambridge University Press. (2012)
- Frankel MR, Morgenstern LB, Kwiatkowski T, et al. "Predicting prognosis after stroke: A placebo group analysis from the National Institute of Neurological Disorders and Stroke rt-PA Stroke Trial". Neurology. 55(7). :952-959. (2000)
- Wouters A, Nysten C, Thijs V, Lemmens R. "Prediction of Outcome in Patients With Acute Ischemic Stroke Based on Initial Severity and Improvement in the First 24 h". Frontiers in Neurology. 9. (2018)
- Van Swieten JC, Koudstaal PJ, Visser MC, Schouten HJ, van Gijn J. "Interobserver agreement for the assessment of handicap in stroke patients.". Stroke. 19(5). :604-607. (1988)
- Fearon P, McArthur KS, Garrity K, et al. "Prestroke Modified Rankin Stroke Scale Has Moderate Interobserver Reliability and Validity in an Acute Stroke Setting". Stroke. 43(12). :3184-3188. (2012)
- Catanese L, Tarsia J, Fisher M. "Acute Ischemic Stroke Therapy Overview". Circ Res. 120(3). :541-558. (2017)
- González RG, Hirsch JA, Lev MH, Schaefer PW, Schwamm LH. "Acute Ischemic Stroke". Springer Science & Business Media. (2010). ISBN: 9783642127519
- Potter CA, Vagal AS, Goyal M, et al. "CT for Treatment Selection in Acute Ischemic Stroke: A Code Stroke Primer". RadioGraphics. 39(6). :1717-1738. (2019)
- Geyer JD, Gomez CR. "Stroke". Lippincott Williams & Wilkins. :263. (2009). ISBN: 9780781766142
- Dostovic Z, Dostovic E, Smajlovic D, Avdic O. "Brain Edema After Ischaemic Stroke". Medical Archives. 70(5). :339. (2016)
- Wardlaw JM. "RADIOLOGY OF STROKE". Journal of Neurology, Neurosurgery & Psychiatry. 70(90001). :7i-11. (2001)
- Hwang DY, Silva GS, Furie KL, Greer DM. "Comparative sensitivity of computed tomography vs. magnetic resonance imaging for detecting acute posterior fossa infarct.". J Emerg Med. 42(5). :559-65. (2012)
- Mandell J. "Core Radiology". Cambridge University Press. (2013). ISBN: 9781107679689
- Chalela JA, Kidwell CS, Nentwich LM, et al. "Magnetic resonance imaging and computed tomography in emergency assessment of patients with suspected acute stroke: a prospective comparison". The Lancet. 369(9558). :293-298. (2007)
- Allen LM, Hasso AN, Handwerker J, Farid H. "Sequence-specific MR Imaging Findings That Are Useful in Dating Ischemic Stroke". RadioGraphics. 32(5). :1285-1297. (2012)
- Kang D-W, Chalela JA, Ezzeddine MA, Warach S. "Association of Ischemic Lesion Patterns on Early Diffusion-Weighted Imaging With TOAST Stroke Subtypes". Arch Neurol. 60(12). :1730. (2003)
- Copen WA, Schaefer PW, Wu O. "MR Perfusion Imaging in Acute Ischemic Stroke". Neuroimaging Clin N Am. 21(2). :259-283. (2011)
- Vagal A, Wintermark M, Nael K, et al. "Automated CT perfusion imaging for acute ischemic stroke". Neurology. :10.1212/WNL.0000000000008481. (2019)
- Mazya MV, Ahmed N, Azevedo E, et al. "Impact of Transcranial Doppler Ultrasound on Logistics and Outcomes in Stroke Thrombolysis". Stroke. 49(7). :1695-1700. (2018)
- Latchaw RE, Alberts MJ, Lev MH, et al. "Recommendations for Imaging of Acute Ischemic Stroke". Stroke. 40(11). :3646-3678. (2009)
- Ross DS, Burch HB, Cooper DS, et al. "2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis". Thyroid. 26(10). :1343-1421. (2016)
- Brinjikji W, Demchuk AM, Murad MH, et al. "Neurons Over Nephrons". Stroke. 48(7). :1862-1868. (2017)
- Burgos AM, Saver JL. "Evidence that Tenecteplase Is Noninferior to Alteplase for Acute Ischemic Stroke". Stroke. 50(8). :2156-2162. (2019)
- Demaerschalk BM, Kleindorfer DO, Adeoye OM, et al. "Scientific Rationale for the Inclusion and Exclusion Criteria for Intravenous Alteplase in Acute Ischemic Stroke". Stroke. 47(2). :581-641. (2016)
- Ganesh A, Fraser JF, Gordon Perue GL, et al. "Endovascular Treatment and Thrombolysis for Acute Ischemic Stroke in Patients With Premorbid Disability or Dementia: A Scientific Statement From the American Heart Association/American Stroke Association". Stroke. 53(5). (2022)
- Lo BM, Carpenter CR, Milne K, et al. "Clinical Policy: Use of Thrombolytics for the Management of Acute Ischemic Stroke in the Emergency Department". Ann Emerg Med. 84(6). :e57-e86. (2024)
- Sorensen AG, Ay H. "Transient ischemic attack: definition, diagnosis, and risk stratification.". Neuroimaging Clin N Am. 21(2). :303-13, x. (2011)
- Kearon C, Akl EA, Ornelas J, et al. "Antithrombotic Therapy for VTE Disease". Chest. 149(2). :315-352. (2016)
- Porth C, Matfin G. "Pathophysiology". Lippincott Williams & Wilkins. (2009). ISBN: 9781605473901
- Harbison J, Hossain O, Jenkinson D, et al. "Diagnostic Accuracy of Stroke Referrals From Primary Care, Emergency Room Physicians, and Ambulance Staff Using the Face Arm Speech Test". Stroke. 34(1). :71-76. (2003)
- Smith EE, Kent DM, Bulsara KR, et al. "Accuracy of Prediction Instruments for Diagnosing Large Vessel Occlusion in Individuals With Suspected Stroke: A Systematic Review for the 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke". Stroke. 49(3). (2018)
- "NIHSS MD Calc". https://www.mdcalc.com/nih-stroke-scale-score-nihss
- Thomalla G, Simonsen CZ, Boutitie F, et al. "MRI-Guided Thrombolysis for Stroke with Unknown Time of Onset". N Engl J Med. 379(7). :611-622. (2018)
- Nogueira RG, Jadhav AP, Haussen DC, et al. "Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct". N Engl J Med. 378(1). :11-21. (2018)
- Albers GW, Marks MP, Kemp S, et al. "Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging". N Engl J Med. 378(8). :708-718. (2018)
- Hirai T, Korogi Y, Ono K, et al. "Prospective evaluation of suspected stenoocclusive disease of the intracranial artery: combined MR angiography and CT angiography compared with digital subtraction angiography.". AJNR Am J Neuroradiol. 23(1). :93-101. (2002)
- Bash S, Villablanca JP, Jahan R, et al. "Intracranial vascular stenosis and occlusive disease: evaluation with CT angiography, MR angiography, and digital subtraction angiography.". AJNR Am J Neuroradiol. 26(5). :1012-21. (2005)
- Goyal M, Demchuk AM, Menon BK, et al. "Randomized Assessment of Rapid Endovascular Treatment of Ischemic Stroke". N Engl J Med. 372(11). :1019-1030. (2015)
- Jovin TG, Chamorro A, Cobo E, et al. "Thrombectomy within 8 Hours after Symptom Onset in Ischemic Stroke". N Engl J Med. 372(24). :2296-2306. (2015)
- Saver JL, Goyal M, Bonafe A, et al. "Stent-Retriever Thrombectomy after Intravenous t-PA vs. t-PA Alone in Stroke". N Engl J Med. 372(24). :2285-2295. (2015)
- Campbell BCV, Mitchell PJ, Kleinig TJ, et al. "Endovascular Therapy for Ischemic Stroke with Perfusion-Imaging Selection". N Engl J Med. 372(11). :1009-1018. (2015)
- Berkhemer OA, Fransen PSS, Beumer D, et al. "A Randomized Trial of Intraarterial Treatment for Acute Ischemic Stroke". N Engl J Med. 372(1). :11-20. (2015)
- Kasner SE. "Clinical interpretation and use of stroke scales". The Lancet Neurology. 5(7). :603-612. (2006)
- Barber PA, Demchuk AM, Zhang J, Buchan AM. "Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy". The Lancet. 355(9216). :1670-1674. (2000)
- Thomalla G, Cheng B, Ebinger M, et al. "DWI-FLAIR mismatch for the identification of patients with acute ischaemic stroke within 4·5 h of symptom onset (PRE-FLAIR): a multicentre observational study". The Lancet Neurology. 10(11). :978-986. (2011)
- Johnston SC, Easton JD, Farrant M, et al. "Clopidogrel and Aspirin in Acute Ischemic Stroke and High-Risk TIA". N Engl J Med. 379(3). :215-225. (2018)
- Parker S, Ali Y. "Changing contraindications for t-PA in acute stroke: review of 20 years since NINDS.". Curr Cardiol Rep. 17(10). :81. (2015)
- Fugate JE, Rabinstein AA. "Absolute and Relative Contraindications to IV rt-PA for Acute Ischemic Stroke". The Neurohospitalist. 5(3). :110-121. (2015)