Summary
Juvenile idiopathic arthritis (JIA; formerly called juvenile rheumatoid arthritis) is a broad term for childhood rheumatic diseases that begin before the age of 16 and are characterized by joint inflammation that lasts more than 6 weeks. It is classified into various types based on the pattern of joint involvement, the presence of extra-articular manifestations (e.g., uveitis, rash, nail changes, lymphadenopathy, hepatosplenomegaly), laboratory findings, and disease prognosis. Oligoarticular JIA, which is the most common type, presents with asymmetric involvement of up to four joints (with the knee joint most often affected). Nearly half of all cases of oligoarticular JIA are associated with anterior uveitis, which may be diagnosed by slit-lamp examination. Laboratory tests such as ESR, rheumatoid factor (RF), antinuclear antibodies (ANA), and the HLA-B27 antigen test are used to classify and determine the prognosis of JIA. Treatment of JIA is similar to that of adult rheumatoid arthritis and involves the use of NSAIDs, intra-articular steroid injections, and disease-modifying antirheumatic drugs (DMARDs) such as methotrexate. Systemic glucocorticoid therapy should be avoided because of the risk of growth impairment.
Epidemiology
- Prevalence: 1:1000 children [1]
- Sex: ♀ > ♂
- Age of onset: : < 16 years of age
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Idiopathic
-
Immunological predisposition: different HLA associations [2][3]
- Oligoarticular JIA: HLA-DR8, HLA-DR5
- Polyarticular JIA: HLA-DR4
- Enthesis associated and psoriatic JIA: HLA-B27
- Possibly triggered by a viral or bacterial infection
- Exposure to antibiotics during childhood may increase the risk of JIA.
Pathophysiology
Autoimmune and/or autoinflammatory disease → chronic synovial inflammation with infiltration of plasma cells, B lymphocytes, and T lymphocytes → joint capsule hyperplasia → growth of fibrovascular connective tissue (pannus) → invasion of the articular surface → loss of joint function [4]
Clinical features
For the exact pattern of joint involvement and specific extra-articular symptoms, see “Subtypes and variants” below.
-
Arthritic symptoms
- Swollen joints, rarely erythema
- Early morning stiffness
- Limited or painful joint movement
-
Extra-articular manifestations [1]
- Fever (for ≥ 2 weeks)
- Uveitis
- Rash
- Nail changes
- Lymphadenopathy
- Hepatosplenomegaly
-
Nonspecific features
- Excessive crying
- Lethargy
- Decreased scholastic performance
The affected joints are often stiff in the morning or after longer periods of inactivity (e.g., sitting). Joint stiffness improves with movement and decreases later in the day.
Subtypes and variants
| Classification of juvenile idiopathic arthritis [4][5] | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Type of JIA | Relative frequency | Peak incidence | Sex | Definition | Pattern of joint involvement | Extra-articular manifestations | Laboratory findings | Treatment | Prognosis |
| Oligoarticular JIA |
|
|
|
|
|
|
|
|
|
| Seronegative polyarticular JIA [7] |
|
|
|
|
|
|
|
|
|
| Seropositive polyarticular JIA [7] |
|
|
|
|
|
|
|
||
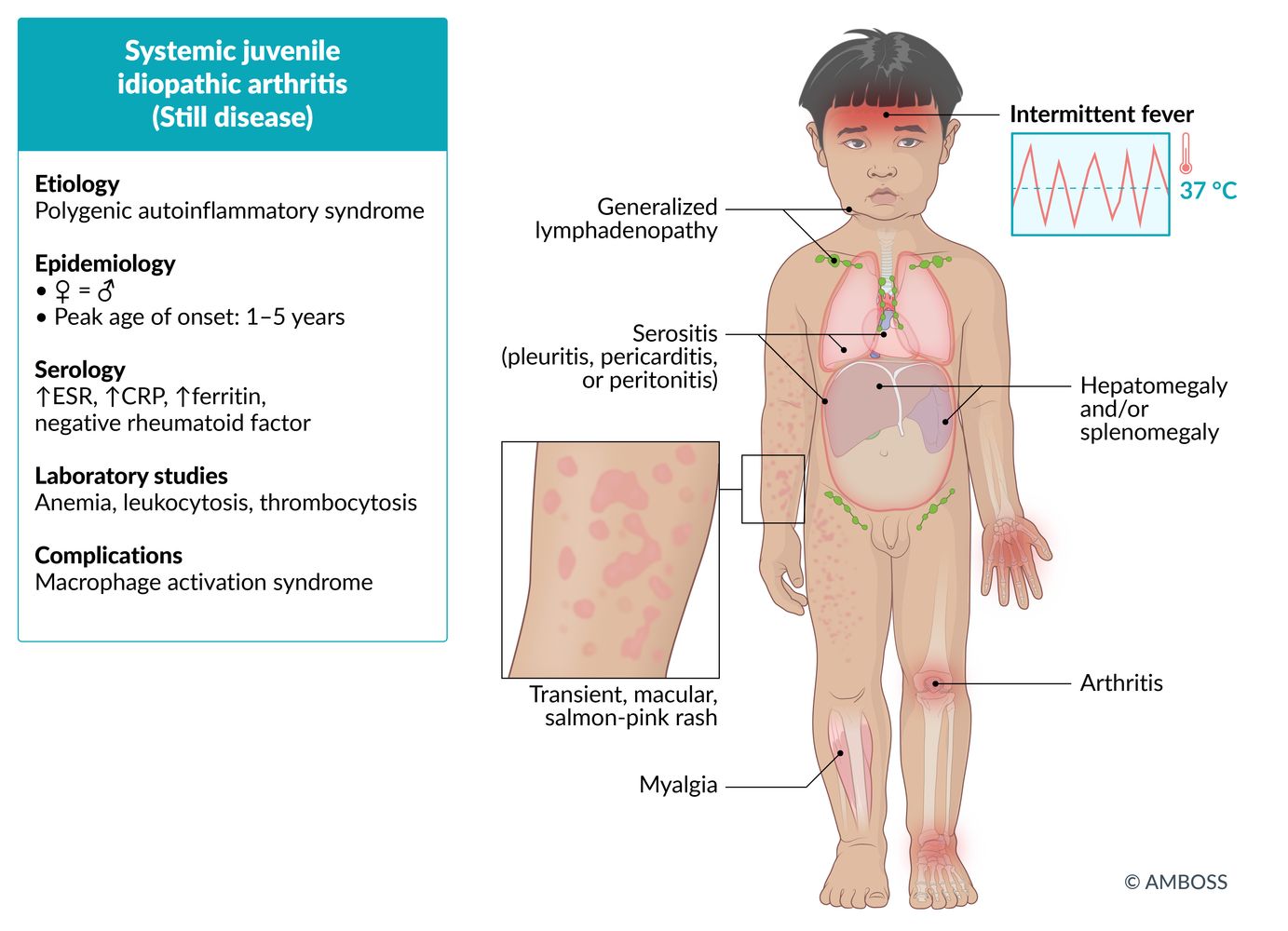
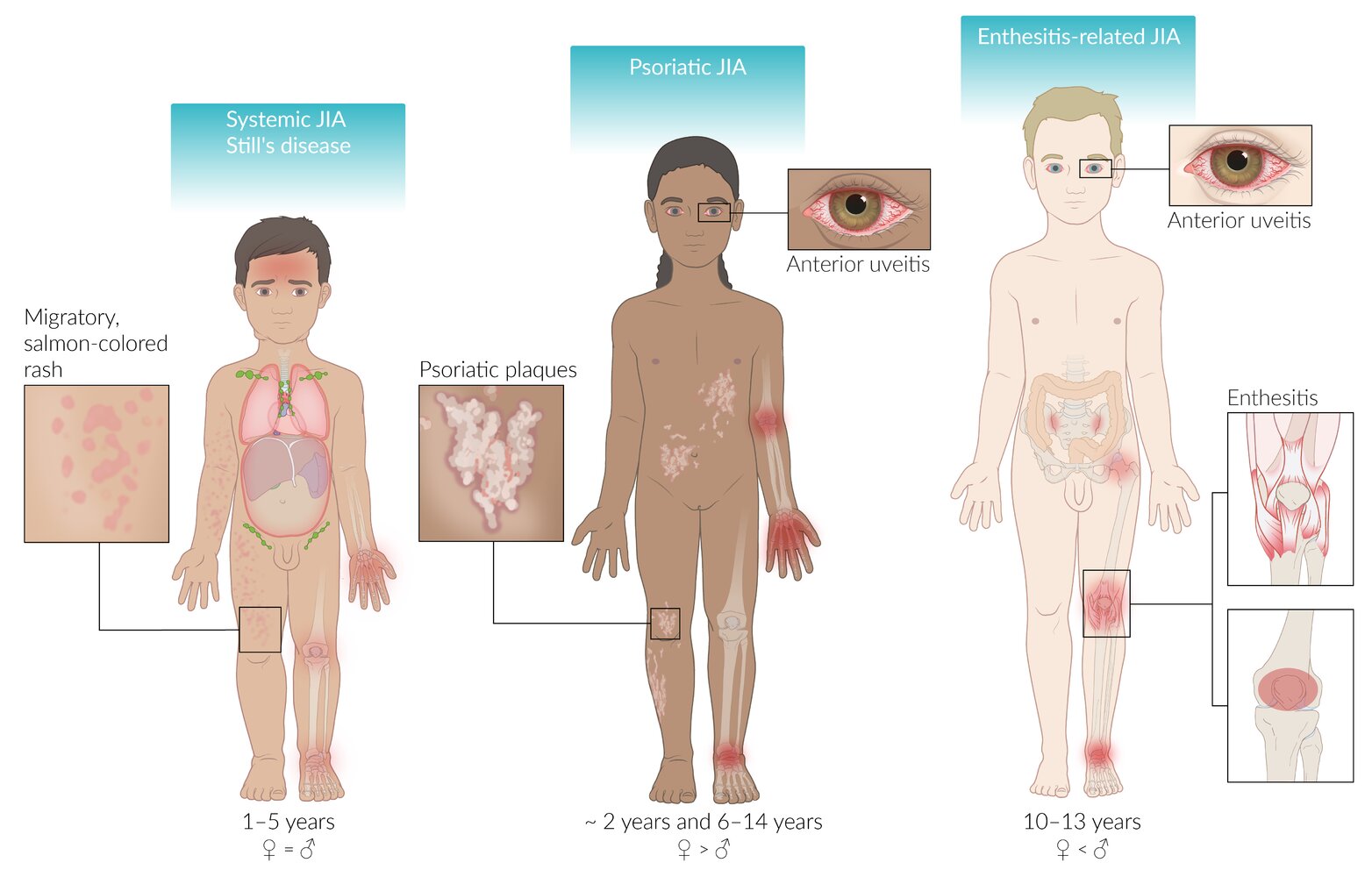
| Systemic JIA (Still disease) |
|
|
|
|
|
|
|
|
|
| Psoriatic JIA |
|
|
|
|
|
|
|
|
|
| Enthesitis-related JIA |
|
|
|
|
|
|
|
|
|
A prerequisite for the diagnosis of all forms of JIA is that arthritic symptoms begin before the age of 16 and last ≥ 6 weeks.
© AMBOSS
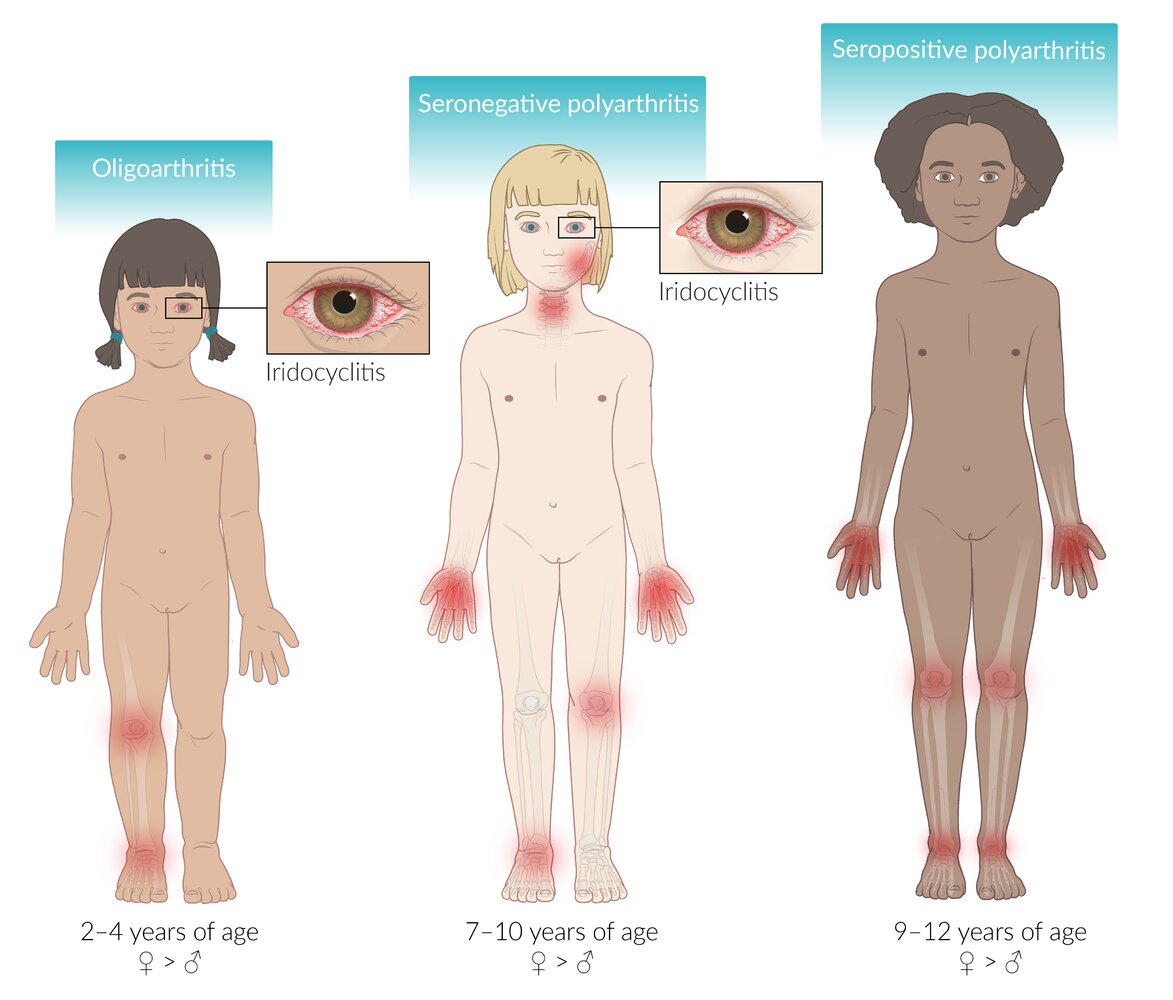
– Oligoarthritis: asymmetrical oligoarthritis involving ≤ 4 joints (within 6 months of onset); associated with iridocyclitis
– Seronegative polyarthritis: asymmetrical or symmetrical oligoarthritis; associated with iridocyclitis
– Seropositive polyarthritis: symmetrical polyarthritis involving ≥ 5 joints (within 6 months of onset)
© AMBOSS
Commonly involved joints for each subtype are highlighted in red.
Also illustrated in systemic JIA are pyrexia, and the extra-articular manifestations of lymphadenopathy, serositis (pleuritis, peritonitis, and/or pericarditis), and hepatosplenomegaly
Note: Anterior uveitis in psoriatic JIA is commonly bilateral and chronic, while in enthesitis-related JIA it more commonly manifests as unilateral flare-ups.
© AMBOSS
Diagnosis
The clinical diagnosis of JIA can be supported by a number of diagnostic tests.
Laboratory tests
Blood tests are used to classify JIA, assess the prognosis, and rule out other similar conditions (see “Subtypes and variants” above).
-
Autoantibodies levels [10]
-
Rheumatoid factor (RF)
- Absent in most cases of JIA (except seropositive polyarticular JIA)
- Associated with poor prognosis
-
↑ ANA
- Most commonly associated with oligoarticular JIA (∼ 70%)
- Incidence of anterior uveitis increases when antinuclear antibodies (ANA) are present.
- Anti-CCP antibodies: indicate a poor prognosis [11]
-
Rheumatoid factor (RF)
-
Acute phase reactants
- ↑ ESR: usually seen with all forms of JIA
- ↑ CRP, ferritin: usually associated with systemic JIA
-
CBC
- Anemia
- Leukocytosis
- Thrombocytosis: denotes a more severe inflammatory response in polyarticular and systemic JIA
Imaging tests
-
Ultrasound [12]
- Used to detect synovial hypertrophy and intraarticular fluid collections
- Best imagistic tool for the detection of early bone erosions
-
X-ray [13]
- May be used for the identification of JIA complications
- Should not be performed routinely
Other diagnostic tests
-
Synovial biopsy
- Can provide a definitive diagnosis of JIA [14]
- Shows infiltration of plasma cells, B lymphocytes, and T lymphocytes
- Slit lamp examination: : should be performed for regular ophthalmological screening in patients with anterior uveitis [10]
-
Slit lamp examination [10][15]
- Patients with a high risk of developing anterior uveitis (ANA positive; , age of onset ≤ 7 years, and disease duration ≤ 4 years) should undergo ophthalmic screening every 3 months.
- All other patients should undergo ophthalmic screening every 12 months.
- Patients with anterior uveitis should be monitored every 1–3 months, depending on the choice of therapy and response to treatment.
Anterior uveitis that occurs with JIA may be asymptomatic (especially in the case of chronic anterior uveitis). However, untreated anterior uveitis is associated with a high risk of developing glaucoma, cataracts, and optic nerve damage. Therefore, early detection via slit lamp examination and swift initiation of treatment are of paramount importance.
Differential diagnoses
The differential diagnosis of JIA includes other causes of nonsuppurative arthritis in children: [16]
- Acute lymphocytic leukemia
- Reactive arthritis
- Acute rheumatic fever
- Juvenile ankylosing spondylitis
- Connective tissue disease (e.g., SLE, Sjögren syndrome)
- Trauma
- Hemophilia
- Growing pains
The differential diagnoses listed here are not exhaustive.
Treatment
Definitive therapy
First-line therapy [17]
-
NSAIDs
-
Indomethacin
- Commonly used; highly effective in the treatment of JIA
- Has severe side effects: headaches, renal failure, and bone marrow depression
- Other commonly used NSAIDs: naproxen, ibuprofen, meloxicam, celecoxib, and tolmetin
-
Indomethacin
- Local intra-articular steroids (e.g., triamcinolone): indicated in the case of active arthritis
Second-line therapy
-
Disease-modifying antirheumatic drugs (DMARDs) [18]
- Therapy with DMARDs should be started as early as possible in the case of high disease activity.
- The DMARD of choice is determined on an individual basis with methotrexate being used in most cases.
-
Biologic agents
- Indicated if the response to DMARDs is poor.
- Examples: etanercept, adalimumab, tocilizumab, anakinra
-
Systemic glucocorticoid therapy (oral, IV) [19]
- Rarely used in children because of the risk of catabolic side effects (e.g., osteoporosis, growth impairment)
- A short course of systemic glucocorticoid therapy may be prescribed in the following situations:
- Severe systemic involvement (e.g., severe serositis; see “Still disease”)
- As bridge therapy when DMARDs are initiated
- Acute anterior uveitis
- Macrophage activation syndrome
Supportive therapy
- Physiotherapy: to prevent joint deformities
- Surgery, splints, and/or orthotics: to correct limb length discrepancy and/or joint deformities
Most drugs that are used to treat adult rheumatoid arthritis may be used to treat JIA as well (see “Therapy” in “Rheumatoid arthritis”). However, certain forms of therapy (e.g., systemic glucocorticoid therapy) should, as a rule, be avoided in children.
Complications
-
Articular complications
- Joint destruction → joint subluxation and/or deformities (e.g., swan-neck deformity, boutonniere deformity)
- Limb length discrepancy
- Growth retardation
-
Extra-articular complications
- Chronic anterior uveitis → blindness
- Pericarditis, pleuritis
-
Macrophage activation syndrome (MAS) [4]
- A rare complication of JIA (most commonly systemic JIA) characterized by thrombocytopenia, elevated transaminases, low fibrinogen, and markedly increased ferritin levels
- In a patient with systemic JIA, the presence of a normal or decreased WBC count, falling ESR, and/or increased triglyceride levels should raise the suspicion of MAS.
We list the most important complications. The selection is not exhaustive.
Prognosis
The clinical course and prognosis are highly variable (see “Subtypes and variants” above) . Most cases (∼ 95%) resolve by puberty.
-
Factors associated with a poor prognosis [17]
- Early onset
- Prolonged active systemic disease
- Hip and/or wrist involvement
- Polyarticular involvement
- Symmetrical disease
- Presence of RF
- Presence of anti-CCP antibodies
Early disease onset is associated with a greater degree of growth impairment and deformity.
References
- "Juvenile idiopathic arthritis". https://ghr.nlm.nih.gov/condition/juvenile-idiopathic-arthritis#statistics. [2020-08-17]
- Ellis JA, Munro JE, Ponsonby A-L. "Possible environmental determinants of juvenile idiopathic arthritis". Rheumatology. 49(3). :411-425. (2009)
- Petty RE, Laxer RM, Lindsley CB, Wedderburn L. "Textbook of Pediatric Rheumatology". Elsevier. (2015). ISBN: 9780323241458
- "Juvenile Idiopathic Arthritis". http://www.pathophys.org/jia/. [2017-02-19]
- Mahmud SA, Binstadt BA. "Autoantibodies in the Pathogenesis, Diagnosis, and Prognosis of Juvenile Idiopathic Arthritis". Frontiers in Immunology. 9. (2019)
- Hamooda M, Fouad H, Galal N, Sewelam N, Megahed D. "Anti-cyclic citrullinated peptide antibodies in children with Juvenile Idiopathic Arthritis". Electronic physician. 8(9). :2897-2903. (2016)
- Wakefield RJ, Gibbon WW, Conaghan PG, et al. "The value of sonography in the detection of bone erosions in patients with rheumatoid arthritis: a comparison with conventional radiography". Arthritis Rheum. 43(12). :2762-2770. (2000)
- Sheybani EF, Khanna G, White AJ, Demertzis JL. "Imaging of juvenile idiopathic arthritis: a multimodality approach.". Radiographics. 33(5). :1253-73. (2013)
- Singhal O, Kaur V, Singhal M, et al. "Arthroscopic synovial biopsy in definitive diagnosis of joint diseases: An evaluation of efficacy and precision". International Journal of Applied and Basic Medical Research. 2(2). :102. (2012)
- Angeles‐Han ST, Ringold S, Beukelman T, et al. "2019 American College of Rheumatology/Arthritis Foundation Guideline for the Screening, Monitoring, and Treatment of Juvenile Idiopathic Arthritis–Associated Uveitis". Arthritis Care Res. 71(6). :703-716. (2019)
- Kim KH, Kim DS. "Juvenile idiopathic arthritis: Diagnosis and differential diagnosis". Korean Journal of Pediatrics. 53(11). :931. (2010)
- Beukelman T, Patkar NM, Saag KG, et al. "2011 American College of Rheumatology recommendations for the treatment of juvenile idiopathic arthritis: initiation and safety monitoring of therapeutic agents for the treatment of arthritis and systemic features". Arthritis Care Res. 63(4). :465-482. (2011)
- Ringold S, Weiss PF, Beukelman T, et al. "2013 Update of the 2011 American College of Rheumatology recommendations for the treatment of juvenile idiopathic arthritis". Arthritis Rheum. 65(10). :2499-2512. (2013)
- Schiappapietra B, Varnier G, Rosina S, et al. "Glucocorticoids in juvenile idiopathic arthritis.". Neuroimmunomodulation. 22(1-2). :112-8. (2015)
- Klein-Gitelman M. "Classification of Juvenile Arthritis". UpToDate. UpToDate. https://www.uptodate.com/contents/classification-of-juvenile-arthritis. [2017-09-21]
- Al-Matar MJ, Petty RE, Tucker LB, et al. "The early pattern of joint involvement predicts disease progression in children with oligoarticular (pauciarticular) juvenile rheumatoid arthritis.". Arthritis Rheum. 46(10). :2708-15. (2002)
- Verbsky J, Oberle E, Harris J. "Polyarticular juvenile idiopathic arthritis – epidemiology and management approaches". Clin Epidemiol. :379. (2014)
- Mullin AH, Nataraj D, Ren JJ, Mullin DA. "Inhaled benzene increases the frequency and length of lacI deletion mutations in lung tissues of mice.". Carcinogenesis. 19(10). :1723-33. (1998)
- "Systemic onset juvenile idiopathic arthritis". https://rarediseases.info.nih.gov/diseases/10966/systemic-onset-juvenile-idiopathic-arthritis. [2007-01-01]
- "Questions and Answers about Juvenile Arthritis". https://www.niams.nih.gov/health_info/juv_arthritis/. [2015-06-01]
- Cunha BA. "Fever of unknown origin caused by adult juvenile rheumatoid arthritis: The diagnostic significance of double quotidian fevers and elevated serum ferritin levels". Heart Lung. 33(6). :417-421. (2004)