Summary
Knee ligament injuries are often the result of rotational movement of the knee joint or direct trauma. Injuries to the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), and lateral collateral ligament (LCL) result in knee pain and instability. Various maneuvers can be used to evaluate the stability of the joint and usually suffice to diagnose collateral ligament tears. An MRI is the best confirmatory test for cruciate ligament tears. Isolated ligament injuries are usually treated conservatively, while surgery is recommended for complex injuries, severe knee instability, and patients with physically demanding occupations.
Tibiofemoral joint dislocation is usually caused by high-energy trauma and is considered an orthopedic emergency. Immediate reduction is indicated to prevent neurovascular damage. Following reduction, a full neurovascular assessment must be performed in all patients, which includes a detailed neurovascular exam, measurement of the ankle-brachial index, and, if vascular injury is suspected, a CT angiogram.
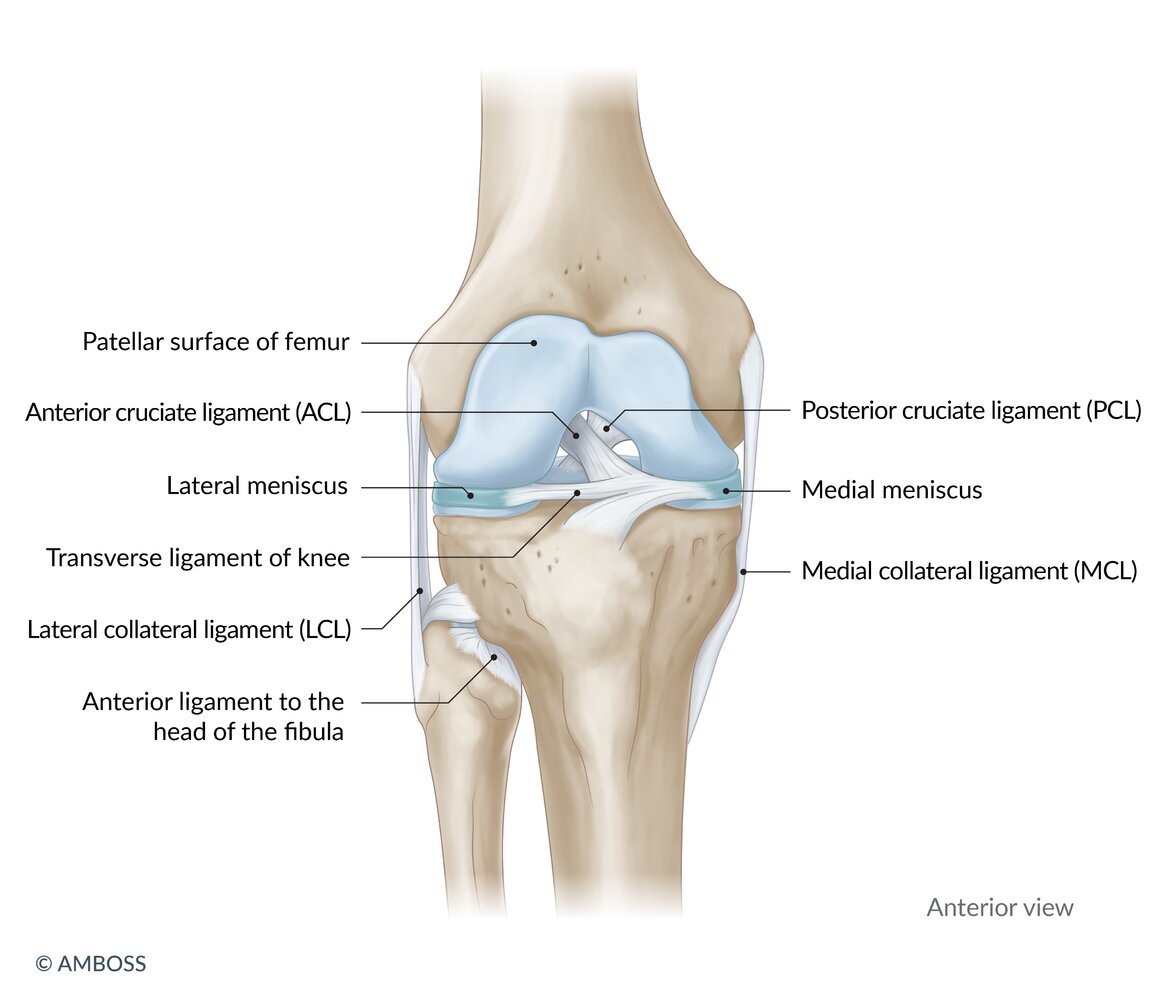
Anatomical overview
- The ACL and PCL connect the femur to the tibia.
- The MCL merges with the joint capsule of the knee.
- The LCL connects the femur and the fibula. It does not merge with the joint capsule of the knee.


© AMBOSS
© AMBOSS
Acute internal knee derangement
Description [1]
- An undifferentiated knee injury (e.g., fracture, ligamentous, or meniscus injury) for which diagnostic physical examination maneuvers are limited by acute pain and swelling.
- Clinical features include knee pain, knee effusion, and/or joint instability in the setting of acute injury.
Initial management [1][2][3]
Empiric management is often necessary as the clinical diagnosis of specific knee ligament injuries is limited acutely. The initial goal is to identify and treat potentially disabling or limb-threatening injuries.
All patients
- Provide acute pain management as necessary.
- Perform an initial knee examination, including skin and neurovascular examination.
- Examine pulses at the popliteal artery, dorsalis pedis, and posterior tibial artery.
- Identify signs of peroneal nerve injury and tibial nerve injury.
- If emergency knee imaging is indicated, obtain a full knee x-ray series (see “Ottawa knee rules”).
- Defer imaging until after urgent reduction if tibiofemoral dislocation is suspected.
- Diagnostic physical examination maneuvers (e.g., Lachman test, posterior drawer test, valgus stress test) are often deferred to a follow-up visit once pain and swelling have subsided.
Acute pain and swelling can make ligamentous and/or meniscus injury difficult to identify clinically. Repeat examination and confirmatory testing (e.g., MRI) in follow-up settings is typically appropriate. [3]
Specific injury suspected
- Tibiofemoral dislocation: immediate reduction followed by neurovascular assessment
- Isolated patellar dislocation: manual reduction of the patella
- Evidence of fracture, patellar and/or quadriceps tendon rupture, or neurovascular compromise: urgent specialist consult
-
Suspected isolated ligamentous (e.g., cruciate or collateral) or meniscus injury
- Consider joint aspiration for severe joint effusion (may show hemarthrosis).
- Place the patient in an unlocked hinged knee brace and provide crutches as needed.
- Allow weight-bearing as tolerated and arrange for orthopedic follow-up within one week.
- See “ACL injury,” “PCL injury,” “MCL injury,” “LCL injury,” and “Meniscus injury” for subsequent management and details.
Avoid knee immobilizers in isolated ligamentous injuries, as these can negatively affect treatment outcomes by decreasing quadriceps strength. Instead, use an unlocked hinged knee brace. [3]
Ottawa knee rules [4][5]
This clinical decision rule can be used to help determine when knee x-rays are indicated for emergency department (ED) patients with knee injuries. [3]
- Inclusion criteria: nonpregnant adults ≥ 18 years of age with acute knee pain ≤ 7 days after injury
-
Exclusion criteria
- Altered mental status
- Presence of additional injuries or multiple trauma
- Paraplegia
-
Risk features: Any of the following is an indication for a full knee x-ray series.
- Age ≥ 55 years
- Fibular head or isolated patellar tenderness
- Inability to flex knee to ≤ 90 degrees
- Inability to weight bear for 4 steps immediately after injury and in the ED

This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Cruciate ligament injuries
Overview [3]
Both ACL injury and PCL injury may present initially as acute internal knee derangement, reducing the yield of physical examination maneuvers. The diagnosis is typically confirmed via MRI, which can have variable findings depending on the mechanism and associated injuries.
| Comparison of ACL and PCL injury [3] | ||
|---|---|---|
| ACL injury | PCL injury | |
| Relative frequency |
|
|
| Classic mechanism |
|
|
| Distinguishing clinical features |
|
|
| Positive physical examination maneuvers |
|
|
| Definitive treatment |
|
|
Complications of cruciate ligament injuries [6][7]
- Chronic knee instability
- Meniscus degeneration
- Osteoarthritis
- Functional limitation
- Postoperatively: graft failure, graft impingement
Anterior cruciate ligament injury
Epidemiology
- Most commonly injured knee ligament [8][9]
- Higher incidence in female individuals
Mechanism of injury [3]
- Low-energy noncontact: sports injuries with a twisting mechanism, e.g., football, soccer, basketball, baseball, alpine skiing, and gymnastics [10]
- High-velocity contact injuries (less common): direct blows to the knee causing forced hyperextension or valgus deformity of the knee
Clinical features [3]
-
History
- Popping sound: commonly heard shortly before the onset of symptoms
- Knee buckling: episodic giving out and loss of ability to bear weight
- Difficulty getting up and moving
-
Physical examination findings
- Knee swelling (e.g., due to hemarthrosis), pain, and instability [3]
-
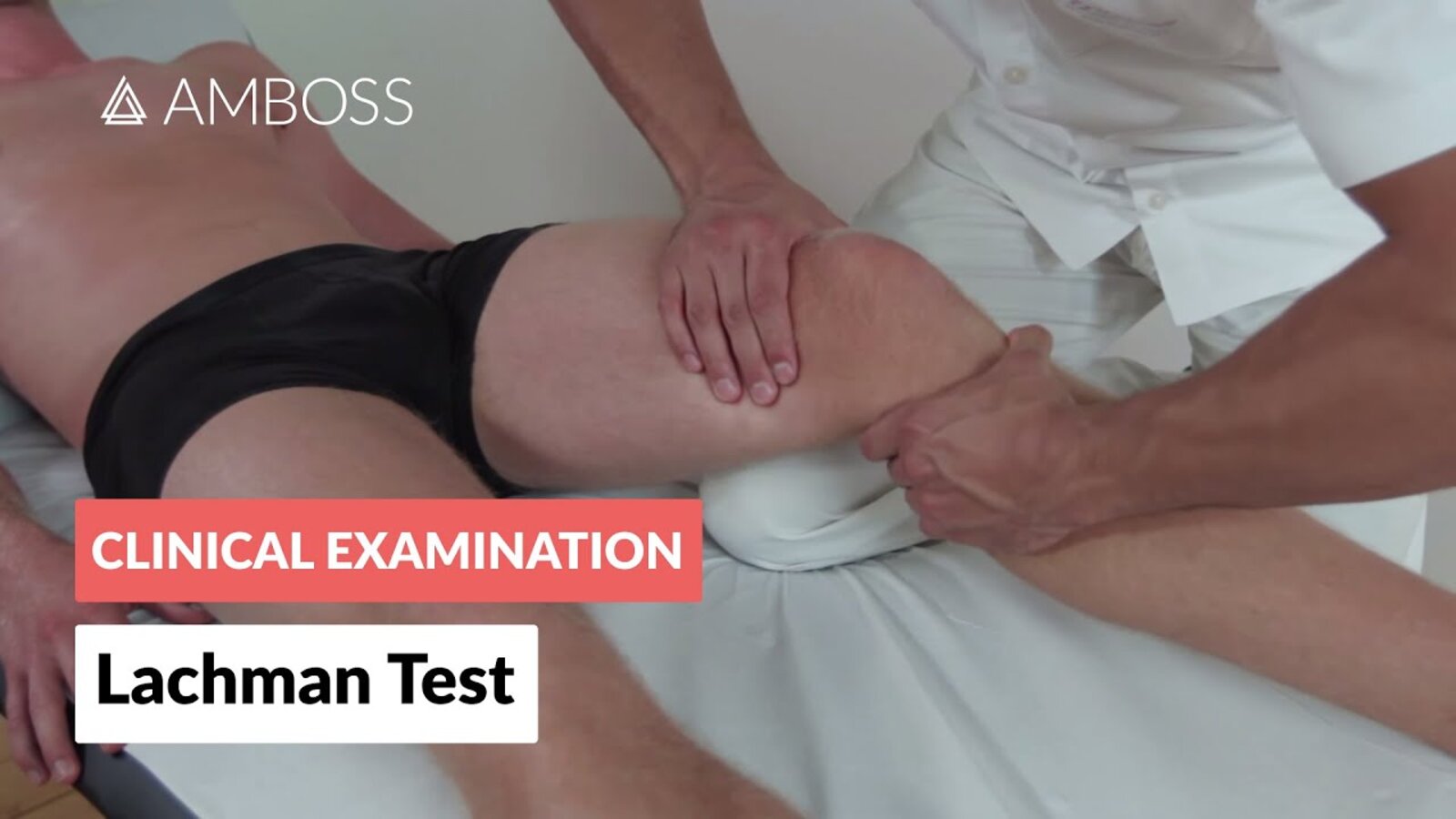
Positive Lachman test (most sensitive test)
- With the knee joint at 20–30° flexion, the examiner stabilizes the femur and pulls the tibia anteriorly.
- Increased tibial anterior gliding (compared to the opposite knee) and a soft endpoint indicate an ACL tear.
-
Positive anterior drawer test
- With the knee joint at 90° flexion, the examiner fixes the foot on the table and pulls the proximal tibia forward.
- Increased tibial anterior gliding (compared to the opposite knee) and a soft endpoint indicate an ACL tear.
-
Positive pivot shift test [11]
- With full extension of the knee joint, the examiner slowly flexes the knee while applying valgus stress with one hand and internally rotating the tibia with the other.
- If the ACL is torn, the anteriorly subluxed lateral tibial plateau jerks backward at 30° of knee flexion.
-
Commonly associated injuries
- Most commonly, lateral meniscus damage (often together with acute ACL and MCL injury)
-
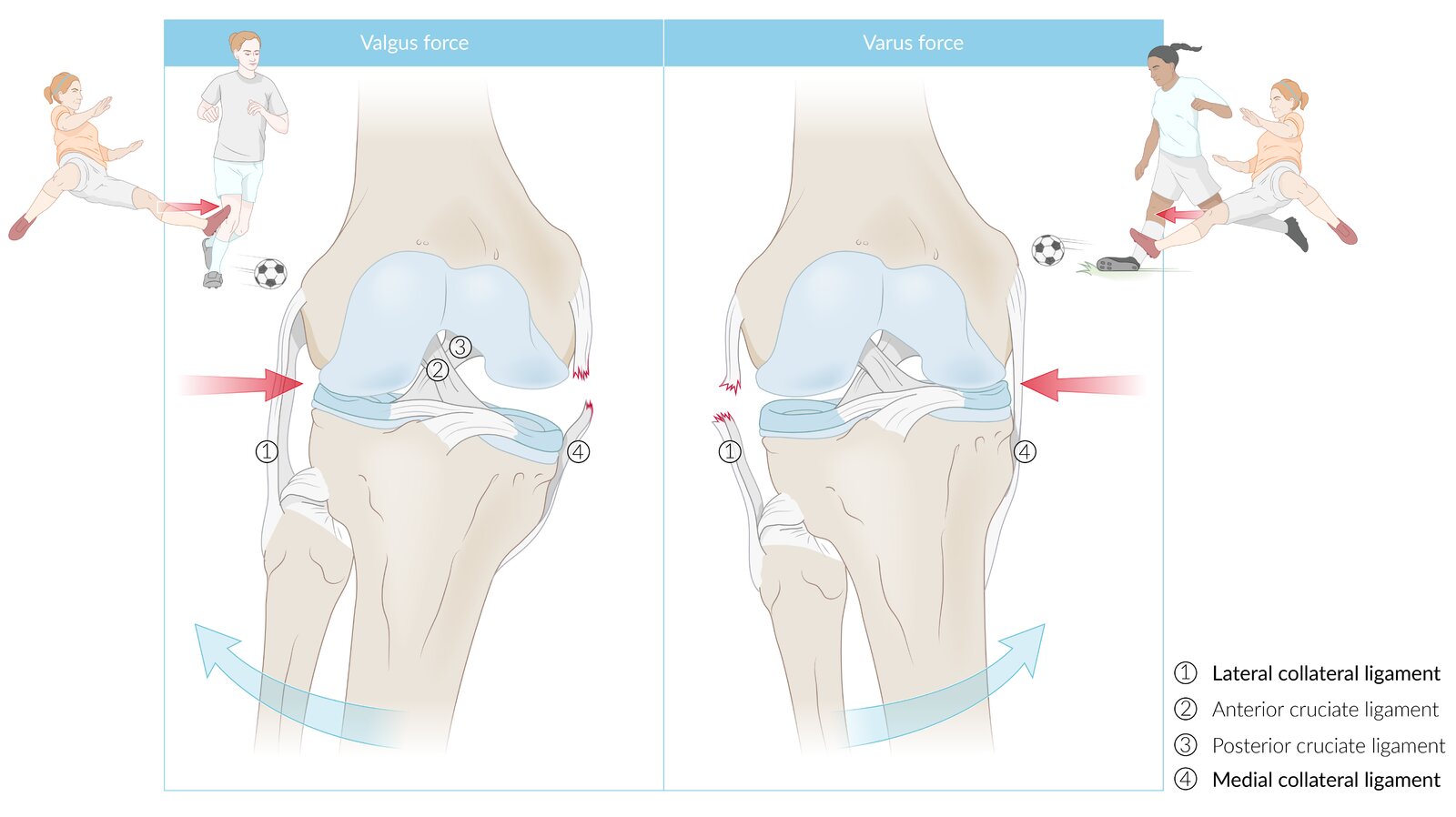
Unhappy triad: simultaneous injury of the ACL, MCL, and medial meniscus (the medial meniscus is attached to the MCL)
- Usually caused by valgus stress (lateral force) applied to the knee while the foot is fixed (e.g., during contact sports)
- Clinical features: pain, instability, tender medial joint line, poor knee extension
Consider deferring physical examination maneuvers in the acute setting as pain and swelling may limit their usefulness. [2]






Diagnostics [3][9]
If MRI is not readily available, a provisional clinical diagnosis of ACL injury can be made if physical examination maneuvers are feasible and reliable.
- Full knee x-ray series: to evaluate for associated fractures or avulsions
- MRI: confirmatory test [9]

Treatment [3][6][12]
For immediate management following injury, see “Acute internal knee derangement.”
-
Conservative treatment: suitable for patients with mild knee instability, older age, and a relatively sedentary lifestyle [6][12]
- Early referral to physiotherapy to maintain range of motion and strengthen quadriceps
- Offer crutches for a limited time and only to patients with significant difficulty with ambulation.
- Avoid knee immobilizers.
-
Arthroscopic surgery: typically pursued in competitive athletes and in patients with a relatively active lifestyle, concomitant meniscus or collateral ligament injury, or chronic knee instability [6][12]
- ACL reconstruction using allograft tissue
- Postoperative care: knee brace, crutches, physical therapy [13]
Complications
See “Complications of cruciate ligament injuries.”

With the patient in supine position, the knee to be examined is flexed at approximately 20°. The examiner grips the distal upper leg with one hand and the proximal lower leg with the second hand (thumb placed on the tibial tuberosity). The lower leg is then pulled ventrally. Increased movability in the ventral direction and/or a lax or nonexistent endpoint suggest injury of the anterior cruciate ligament, particularly if there is a significant difference to the other knee.
© AMBOSS

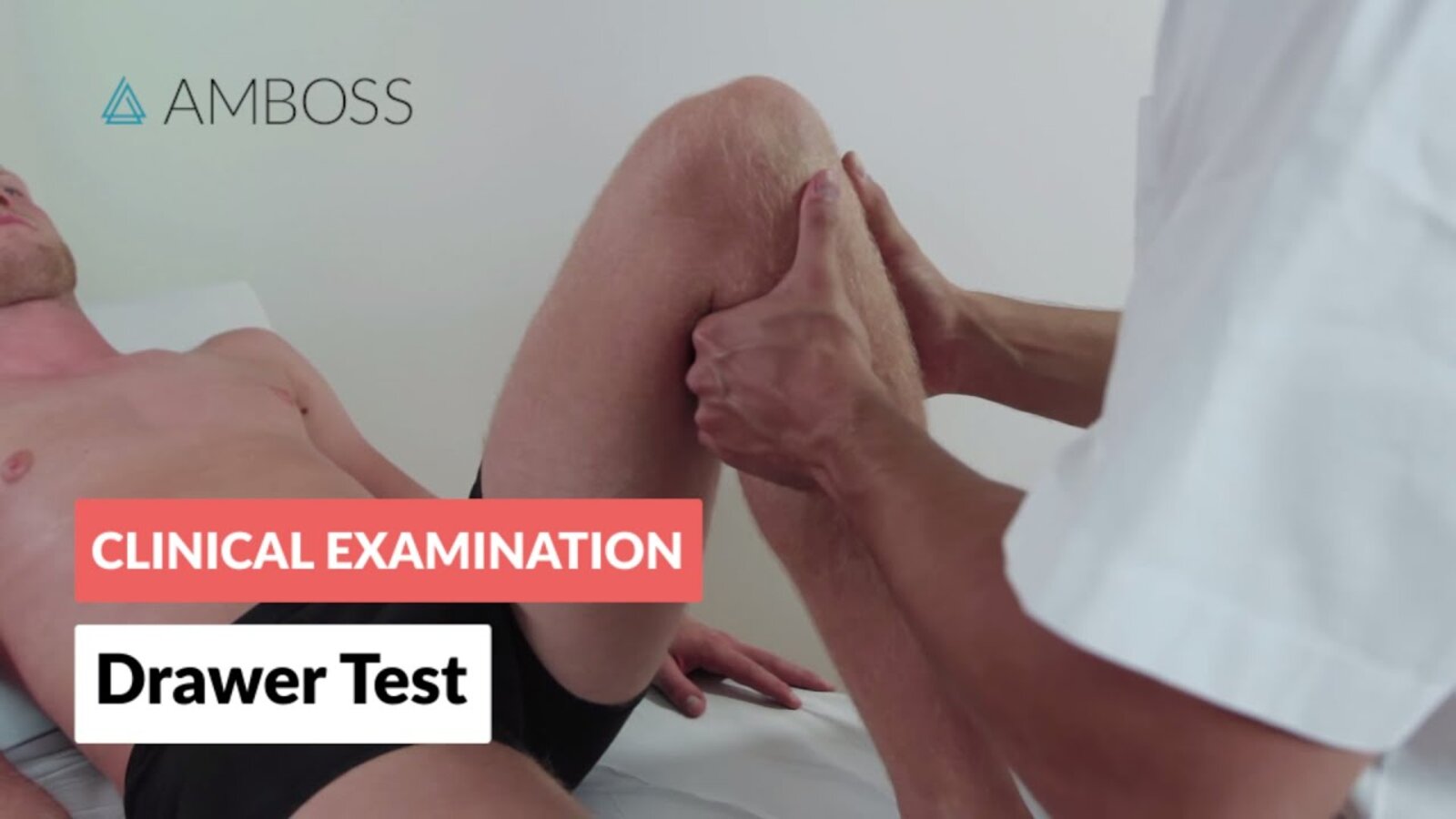
The patient is in supine position, the leg to be examined is erect, and the knee is flexed at approximately 90°. The examiner puts both hands around the lower leg (with the thumbs placed on the tibial tuberosity). To examine the anterior cruciate ligament, the tibia is pulled ventrally. To examine the posterior cruciate ligament, the tibia is pushed dorsally. If the movability of the tibia is increased (particularly compared to the other leg) or if there is a lax endpoint, the drawer test is said to be positive and may indicate an injury to the respective ligament.
© AMBOSS
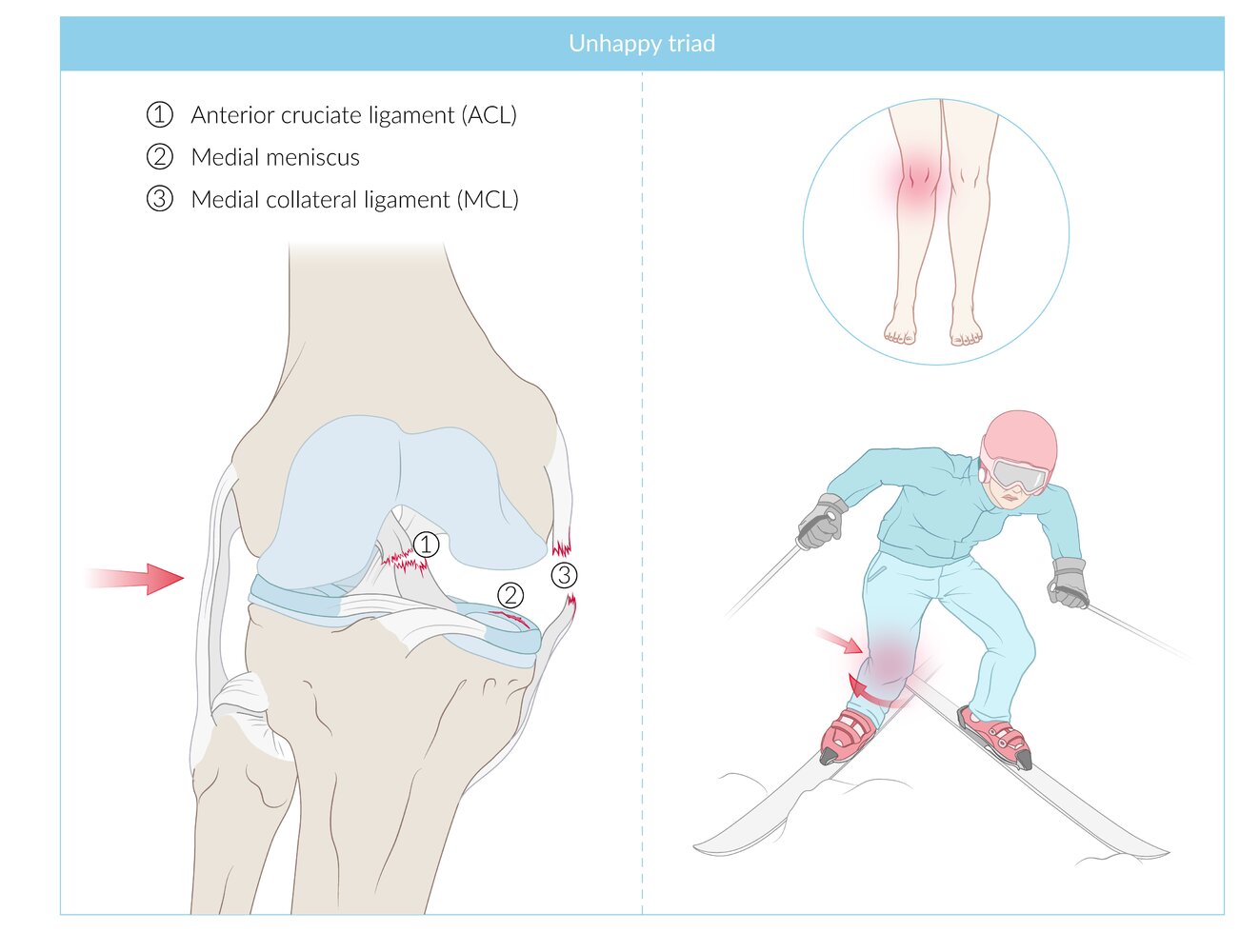
A triad of medial meniscus, anterior cruciate ligament, and medial collateral ligament tears. This injury typically occurs due to excessive valgus and external rotational stress with a fixed foot position.
© AMBOSS
© AMBOSS
© AMBOSS

© AMBOSS

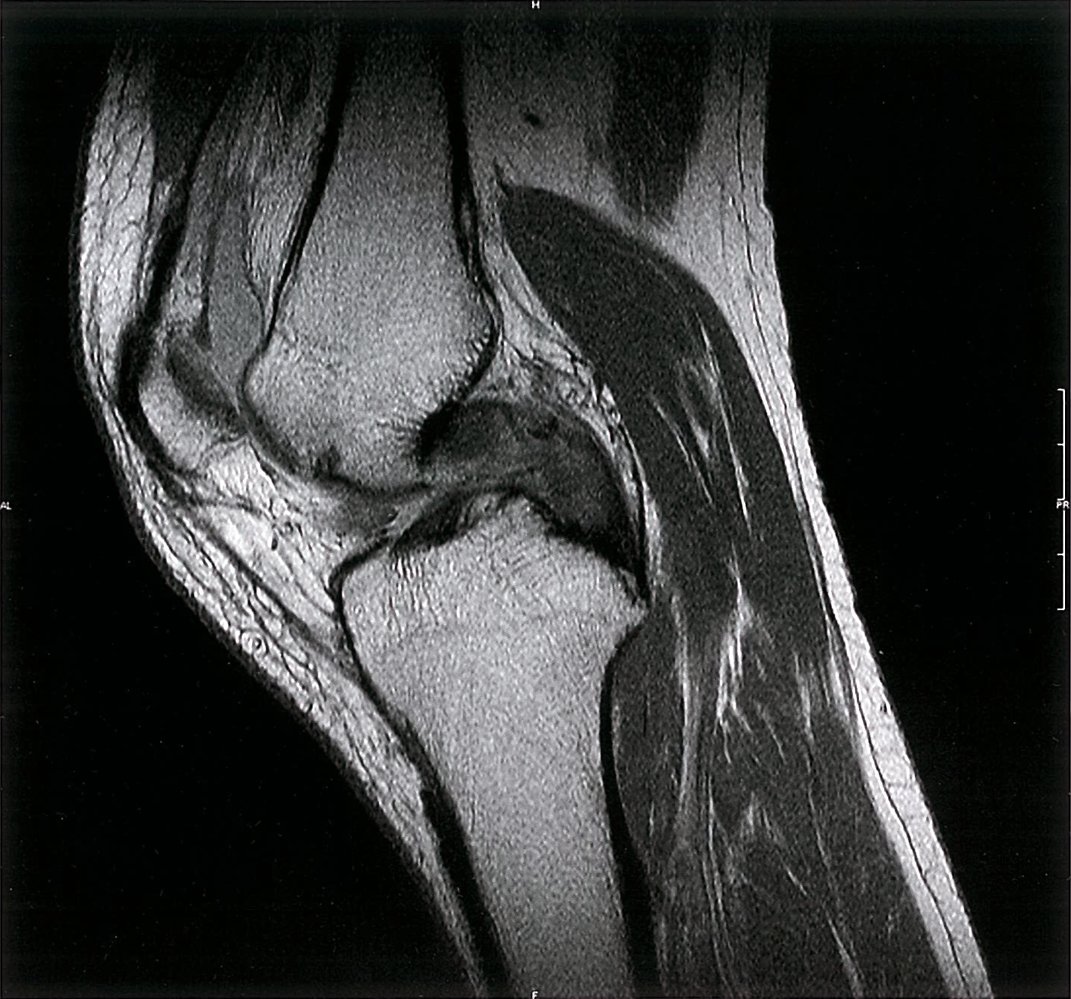
MRI knee (STIR; sagittal view)
The anterior cruciate ligament is discontinuous. The distal part of the ligament demonstrates normal hypointense signal (red overlay), but the proximal half ligament demonstrates heterogenous hyperintense signal (yellow overlay). There is a gap between these two areas. There is also a large suprapatellar joint effusion (demonstrated as a white area due to high signal intensity; blue overlay). The partially imaged posterior cruciate ligament (green overlay) appears intact.
This is an example of an anterior cruciate ligament rupture. The gap between the proximal and distal half of the ligament indicates it is a full-thickness tear. The heterogeneous hyperintense signal of the proximal half indicates partial thickness tearing of that component.
Source: © IMPP
Posterior cruciate ligament injury
Mechanism of injury [14]
- Noncontact injury involving hyperflexion of the knee with a plantarflexed foot (seen in athletes)
- Direct posterior blow to a flexed knee: seen in motor vehicle accidents (dashboard injury) or athletic contact injury
- Rotational injury involving hyperextension of the knee (rare)
Clinical features [3][14]
-
History
- Acute injury: vague or absent posterior knee pain, swelling, decreased functional range of motion
- Chronic injury: anterior knee pain and instability [3][14]
-
Physical examination findings
-
Positive posterior drawer test
- With the patient lying supine and the knee at 90° flexion, the examiner fixes the foot on the table and pushes the proximal tibia backward.
- Increased tibial posterior gliding (compared to the opposite knee) and a soft endpoint indicate PCL injury.
-
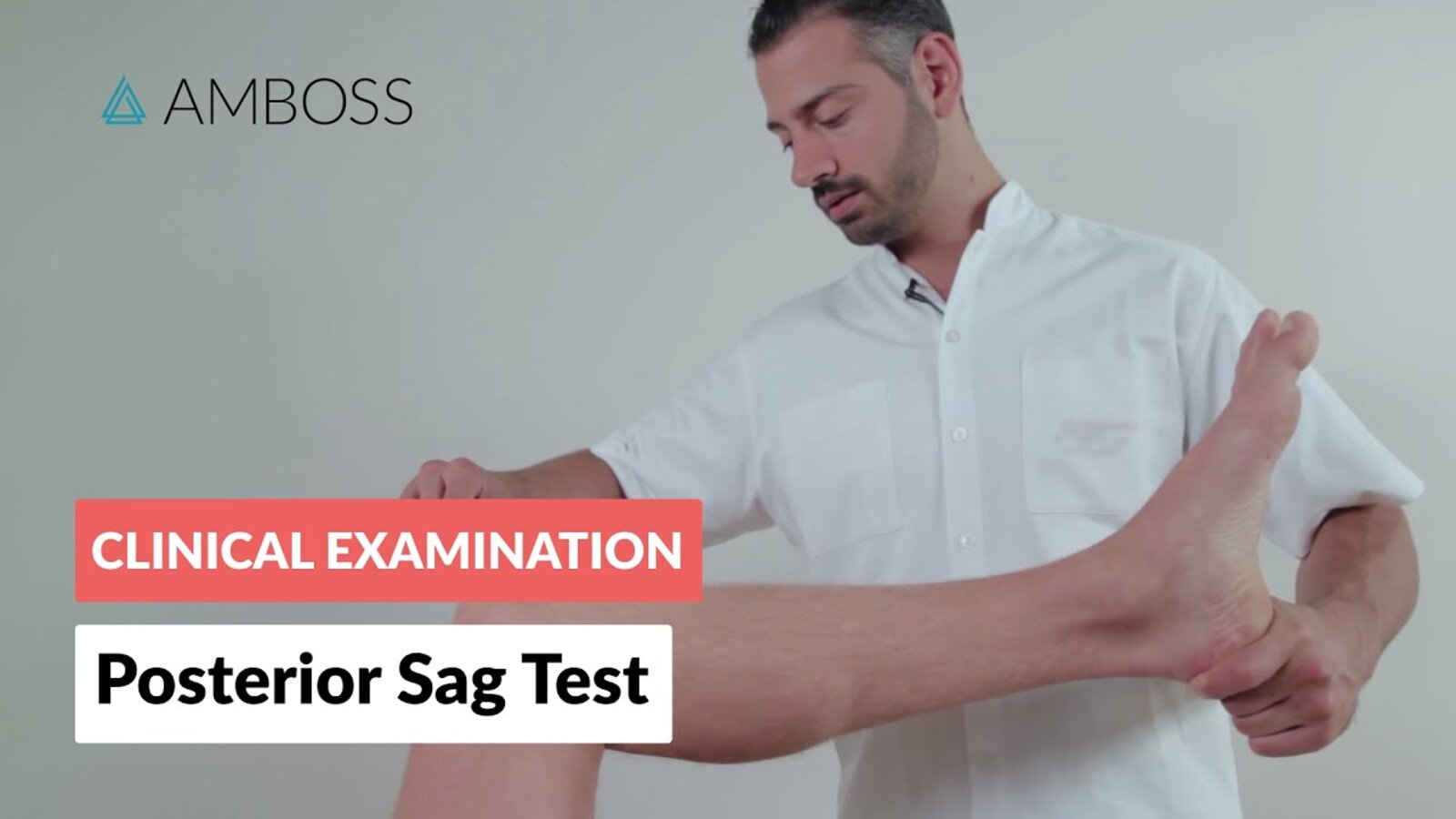
Positive posterior sag sign
- The patient lies down with both hips and knees flexed and aligned together.
- In this position, the tibia on the side of the torn PCL will appear to fall backwards under the influence of gravity.
- Positive quadriceps active test [14]
- The patient is placed in supine position with the knee flexed at 90° with the foot flat on the bed.
- Anterior translation of the tibia with isometric quadriceps contraction indicates PCL injury.
-
Positive posterior drawer test
Consider deferring physical examination maneuvers in the acute setting as pain and swelling may limit their usefulness. [2]
")

Diagnostics [3][14]
If MRI is not readily available, a provisional clinical diagnosis of PCL injury can be made if physical examination maneuvers are feasible and reliable.
- Full knee x-ray series: to evaluate for posterior sag of the tibia and associated fractures or avulsions
- MRI: (confirmatory test) [14]
")
")


Treatment [3][14]
For immediate treatment following injury, see “Acute internal knee derangement.”
- Conservative therapy for isolated injuries
- Surgery for multiligament injuries, chronic knee instability, and for highly competitive athletes
Complications
See “Complications of cruciate ligament injuries.”
The patient is in supine position, the leg to be examined is erect, and the knee is flexed at approximately 90°. The examiner puts both hands around the lower leg (with the thumbs placed on the tibial tuberosity). To examine the anterior cruciate ligament, the tibia is pulled ventrally. To examine the posterior cruciate ligament, the tibia is pushed dorsally. If the movability of the tibia is increased (particularly compared to the other leg) or if there is a lax endpoint, the drawer test is said to be positive and may indicate an injury to the respective ligament.
© AMBOSS
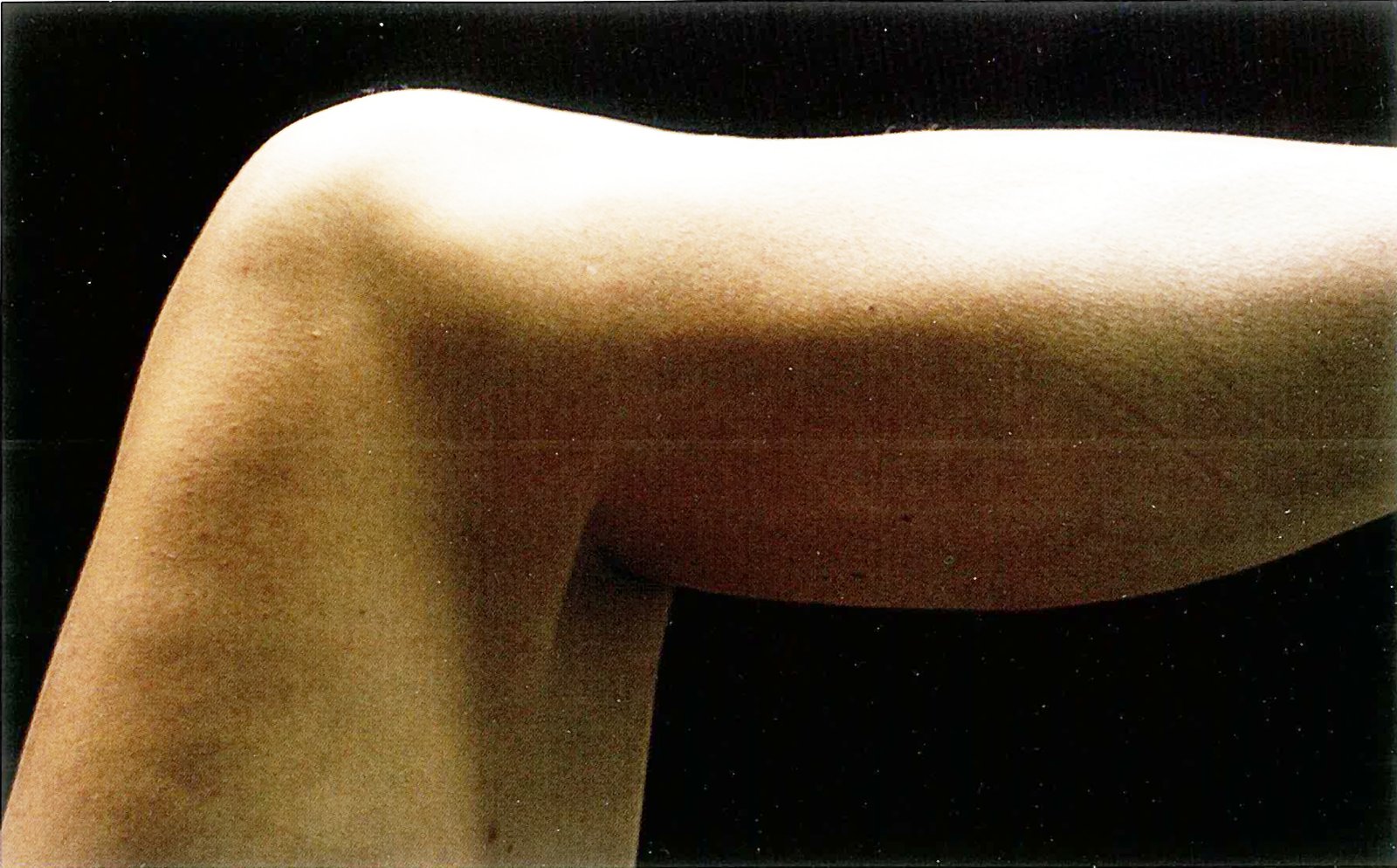
The knee is flexed to 90°: spontaneous posterior sag of the tibia as a result of gravity.
Source: © IMPP
© AMBOSS
© AMBOSS

X-ray knee (lateral view)
An avulsed fragment of bone (green overlay) projects over the posterior knee joint. A comminuted fracture (red overlay) of the patella is also seen, and increased soft tissue density in the suprapatellar recess (yellow overlay) indicates a joint effusion.
F: femur; T: tibia
Source: “Fig 1B, In: Modified Arthroscopic Suture Fixation of Posterior Cruciate Ligament Tibial Avulsion Fracture in the Setting of Multiligament Knee Injury in Teenager” by Quesado M, Esteves AS, da Silva NV et al., Hindawi, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

MRI knee (T2-weighted; fat saturated; sagittal plane)
An avulsed fragment of bone is seen at the posterior cruciate ligament tibial attachment site (green overlay). Also present are a comminuted patellar fracture with increased signal from marrow edema (green circle) and a hyperintense joint effusion (yellow overlay).
F: femur; T: tibia
Source: “Fig 3, In: Modified Arthroscopic Suture Fixation of Posterior Cruciate Ligament Tibial Avulsion Fracture in the Setting of Multiligament Knee Injury in Teenager” by Quesado M, Esteves AS, da Silva NV et al., Hindawi, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
MRI knee (T2-weighted; sagittal plane)
The posterior cruciate ligament (PCL) appears thickened and heterogeneous with an irregular and ill-defined contour (green overlay). It contains multiple areas of intermediate signal intensity, indicating tearing. A joint effusion is demonstrated by the hyperintense signal in the suprapatellar pouch (red overlay).
A ligament tear does not always appear as a discrete defect and may be demonstrated by the features in this example. A normal PCL should appear as hypointense on all conventional MRI sequences and have smooth margins.
Source: © IMPP

T2-weighted sagittal MRI image of the knee: suprapatellar joint effusion, intact posterior cruciate ligament (P=patella, F=femur, T=tibia)
Source: © IMPP
Collateral ligament injury
Overview
| Overview of collateral ligament injuries [3] | ||
|---|---|---|
| Medial collateral ligament injury | Lateral collateral ligament injury | |
| Mechanism of injury |
|
|
| Associated injuries |
|
|
| Distinguishing clinical features | ||
|
|
|
MCL injuries are more common than LCL injuries.

Clinical features [3]
- Knee swelling with ecchymosis, pain, deformity, and instability
- Increased joint laxity on varus stress test or valgus stress test
- Joint line tenderness
- Possible signs of associated cruciate ligament injury and/or meniscus injury
Classification
The degree of joint laxity is graded based on the estimated size of lateral joint space during the valgus stress test or varus stress test. [15]
- Grade I: 3–5 mm (mild instability)
- Grade II: 6–10 mm (moderate instability)
- Grade III: > 10 mm (severe instability; other knee ligaments may be injured)
Diagnostics [3]
- An isolated collateral ligament tear is a clinical diagnosis.
- X-rays and MRI may be used for confirmation and to rule out associated injuries.
Treatment [3]
For immediate management, see “Acute internal knee derangement.”
- Conservative treatment (functional brace and physical therapy) for isolated tears
- Surgery if associated injuries are present
© AMBOSS
Tibiofemoral joint dislocation
Mechanism of injury [3]
Usually caused by high-energy trauma (e.g., dashboard injury, fall from a height)
- Anterior dislocation (tibia is anterior to the femur): caused by hyperextension of the knee joint
- Posterior dislocation (tibia is posterior to the femur): caused by direct anterior impact to the proximal tibia
- Medial/lateral dislocation (tibia is medial or lateral to the femur): caused by varus or valgus force
- Rotary dislocation (anterolateral, posterolateral, anteromedial, or posteromedial tibial displacement): caused by twisting force


Clinical features [3]
-
Musculoskeletal findings
- Abnormal position of the knee joint (see “Mechanism of injury”)
- Swelling of the knee
- Ecchymosis
- Dimple sign (pathognomonic for posterolateral dislocation): indentation of the skin at the medial femoral condyle [16]
-
Neurovascular exam findings
- Signs of popliteal artery injury: weak or absent dorsalis pedis and posterior tibial artery pulses, 6 Ps of acute limb ischemia
- Signs of peroneal nerve injury and/or tibial nerve injury
Maintain a high level of suspicion for vascular injury, as popliteal artery injury may be present despite palpable pulses. [3]

Management [3]
See also “Acute internal knee derangement” for the approach to an undifferentiated knee injury.
-
Immediate dislocation reduction: Do not delay reduction to obtain imaging unless an alternate diagnosis is suspected.
- Isolated anterior or posterior dislocation: closed reduction under procedural sedation
- Posterolateral dislocation; : urgent orthopedic consult for open reduction (in most cases)
-
Neurovascular exam: : Document popliteal and distal pulses and distal lower extremity sensory and motor functions before and after reduction.
- Abnormalities detected: urgent vascular surgery consult
- No abnormalities detected: Proceed with further diagnostic evaluation.
-
Further evaluation
- Measure the ankle-brachial index (ABI).
- ABI < 0.9: Obtain CT angiogram of the lower extremity [17].
- ABI ≥ 0.9: Monitor with serial neurovascular exams every 2–3 hours.
- Obtain x-ray of the knee joint and the lower leg to evaluate for associated injury.
- Measure the ankle-brachial index (ABI).
-
Disposition
- Place patient in a posterior splint in 15–20° flexion and admit for 24–48 hours observation.
- Obtain vascular surgery consult if there are any clinical or imaging signs of neurovascular injury.
- Follow-up with orthopedics for surgical repair of ligamentous injury
Knee dislocation is an orthopedic emergency requiring immediate reduction to prevent limb-threatening neurovascular injury. [3]
Knee dislocations frequently reduce spontaneously before presentation to the emergency department. Neurovascular evaluation is mandatory in all patients with a relevant lower extremity injury mechanism (see “Mechanism of injury”). [3]
Complications [18]
- Injury of ACL, MCL, LCL, PCL, or PLC
- Popliteal artery injury
- Common peroneal or tibial nerve injury
- Periarticular fractures
- Compartment syndrome
- Deep vein thrombosis
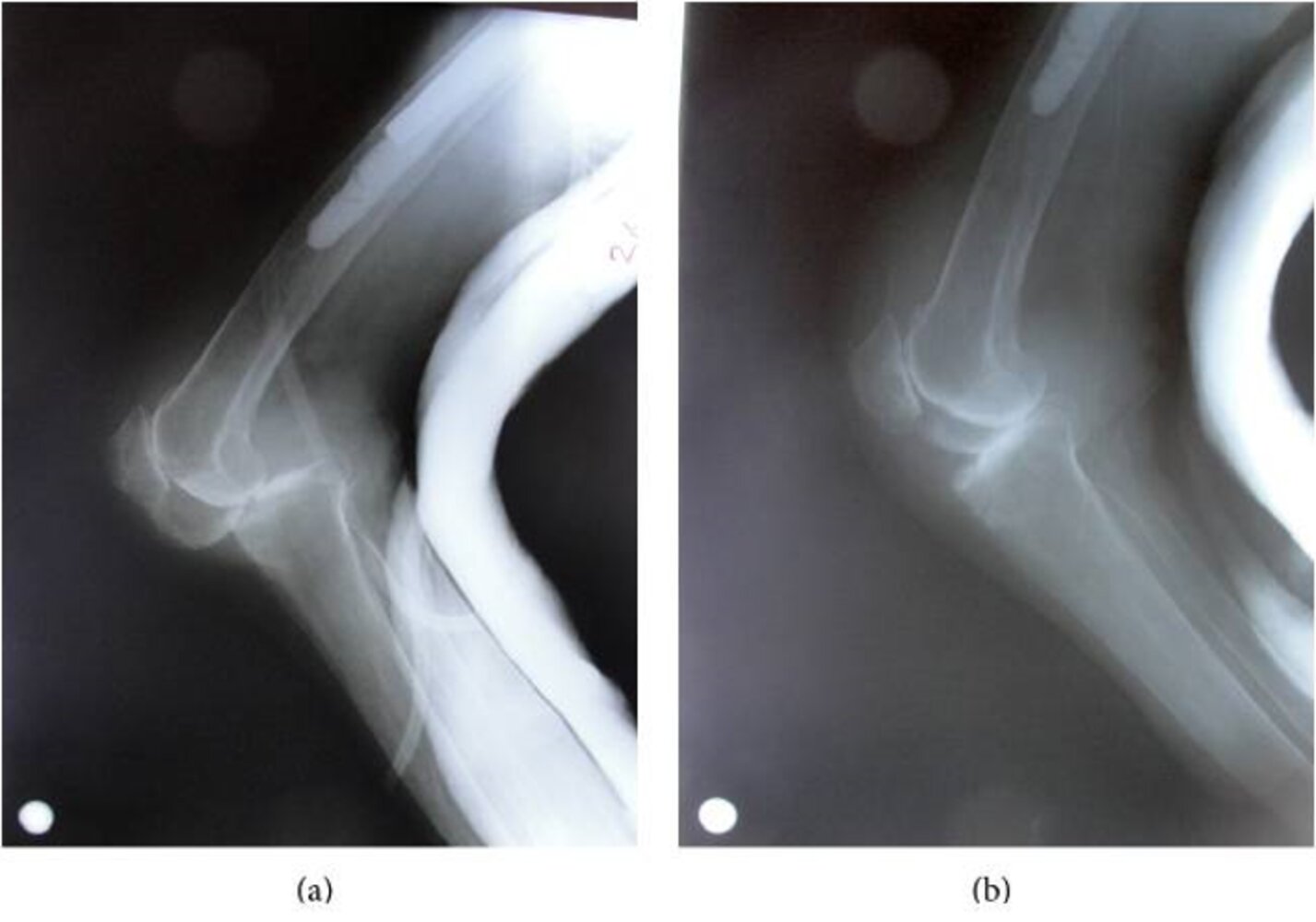
X-ray knee (lateral view; a: before reduction; b: after reduction)
Prior to reduction (a), the tibia is displaced posteriorly (indicated by red arrowheads) relative to the femur. After reduction (b), the tibia and femur are aligned. Degenerative changes (green arrowheads) are also seen along with a partially imaged cemented femoral rod (green overlay).
Knee dislocations are typically classified in terms of tibial displacement relative to the position of the femur. Dislocations may be described as anterior, posterior, medial, lateral, or rotary.
Source: “Fig 4, In: An Unexpected Complication of Hip Arthroplasty: Knee Dislocation” by Yilmaz S ,Cankaya D ,Deveci A,Ozdemir M,2 Bozkurt M, Hindawi, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

X-ray knee (left; a: AP view; b: lateral view)
The tibia is displaced anteriorly (indicated by arrows in b) and laterally (indicated by arrows and dashed lines in a) relative to the femur.
Knee dislocations are typically classified in terms of tibial displacement relative to the position of the femur. Dislocations may be described as anterior, posterior, medial, lateral, or rotary. Rotary dislocations can further be described as anterolateral, posterolateral, anteromedial, or posteromedial.
Source: “Fig 2, In: Knee Dislocation: A Case Report, Diagnostic Vascular Work-Up, and Literature Review” by Douma MR, Burg MD, Dijkstra BL, Hindawi, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

Left knee of a 22-year-old patient after a twisting sports-related injury
An abnormal left knee outline characterized by an anterolateral prominence below the knee can be seen. A discreet hematoma is visible in the area above the patella.
These findings result from a rotatory anterolateral knee dislocation.
Source: “Fig 1, In: Knee Dislocation: A Case Report, Diagnostic Vascular Work-Up, and Literature Review” by Douma MR, Burg MD, Dijkstra BL, Hindawi, licensed under CC BY 4.0.
References
- Pache S, Aman ZS, Kennedy M, et al. "Posterior Cruciate Ligament: Current Concepts Review.". The archives of bone and joint surgery. 6(1). :8-18. (2018)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Bunt CW, Jonas CE, Chang JG. "Knee Pain in Adults and Adolescents: The Initial Evaluation". Am Fam Physician. 98(9). :576-585. (2018)
- Mall NA, Chalmers PN, Moric M, et al. "Incidence and Trends of Anterior Cruciate Ligament Reconstruction in the United States". Am J Sports Med. 42(10). :2363-2370. (2014)
- Musahl V, Karlsson J. "Anterior Cruciate Ligament Tear". N Engl J Med. 380(24). :2341-2348. (2019)
- Dordevic M, Hirschmann MT. "Injury Mechanisms of ACL Tear". Springer Berlin Heidelberg. :49-53. (2014). ISBN: 9783642453489
- Benjaminse A, Gokeler A, van der Schans CP. "Clinical Diagnosis of an Anterior Cruciate Ligament Rupture: A Meta-analysis". Journal of Orthopaedic & Sports Physical Therapy. 36(5). :267-288. (2006)
- Cimino F, Volk BS, Setter D. "Anterior cruciate ligament injury: diagnosis, management, and prevention.". Am Fam Physician. 82(8). :917-22. (2010)
- Micheo W, Hernández L, Seda C. "Evaluation, Management, Rehabilitation, and Prevention of Anterior Cruciate Ligament Injury: Current Concepts". PM&R. 2(10). :935-944. (2010)
- Bousquet BA, O'Brien L, Singleton S, Beggs M. "POST-OPERATIVE CRITERION BASED REHABILITATION OF ACL REPAIRS: A CLINICAL COMMENTARY.". International journal of sports physical therapy. 13(2). :293-305. (2018)
- Phisitkul P, James SL, Wolf BR, Amendola A. "MCL injuries of the knee: current concepts review.". Iowa Orthop J. 26. :77-90. (2006)
- Reckling FW, Peltier LF. "Acute Knee Dislocations and Their Complications". Clin Orthop Relat Res. 422. :135-141. (2004)
- Walker REA, McDougall D, Patel S, et al. "Radiologic Review of Knee Dislocation: From Diagnosis to Repair". American Journal of Roentgenology. 201(3). :483-495. (2013)
- Peskun CJ, Levy BA, Fanelli GC, et al. "Diagnosis and Management of Knee Dislocations". Phys Sportsmed. 38(4). :101-111. (2010)
- Grover M. "Evaluating acutely injured patients for internal derangement of the knee.". Am Fam Physician. 85(3). :247-52. (2012)
- Stiell IG, Greenberg GH, Wells GA, et al. "Derivation of a Decision Rule for the Use of Radiography in Acute Knee Injuries". Ann Emerg Med. 26(4). :405-413. (1995)
- Sims JI, Chau MT, Davies JR. "Diagnostic accuracy of the Ottawa Knee Rule in adult acute knee injuries: a systematic review and meta-analysis". Eur Radiol. 30(8). :4438-4446. (2020)
- Sepúlveda F, Sánchez L, Amy E, Micheo W. "Anterior Cruciate Ligament Injury". Curr Sports Med Rep. 16(3). :172-178. (2017)