Summary
A late-term pregnancy is defined as 41 0/7 to 41 6/7 weeks' gestation; at 42 weeks' gestation, it becomes a postterm pregnancy. While the causes of postterm pregnancy are generally unknown, many supposed cases are likely due to a suboptimally dated gestational age. Risk factors may be maternal (e.g., age, previous postterm pregnancies, nulliparity) and fetal (e.g., male sex, disorders such as oligohydramnios). Patients with low-risk late-term pregnancies who have not had suboptimal gestational dating and who do not have indications for cesarean delivery or contraindications for induction of labor are usually offered the choice between expectant management with antepartum fetal surveillance and induction of labor. After 42 weeks' gestation, induction of labor is recommended regardless of cervical favorability in order to avoid associated complications. Membrane sweeping may be performed in well-dated pregnancies after 39 weeks' gestation to induce labor and prevent late-term or postterm pregnancy.
See also “Pregnancy” and “Prenatal care.”
Definitions
- Late-term pregnancy: a pregnancy between 41 0/7 and 41 6/7 weeks' gestation
- Postterm pregnancy: a pregnancy ≥ 42 0/7 weeks' gestation
- Postterm birth: live birth after the completion of 42 weeks of pregnancy (≥ 42 0/7 weeks' gestation)
Epidemiology
- Incidence is approximately 0.25%. [2]
- Postmaturity syndrome occurs in < 20% of postterm pregnancies. [1]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Etiology: usually unknown [3]
-
Risk factors for postterm pregnancy include:
- Maternal factors [4]
- Age > 30 years
- Maternal obesity [3]
- Genetic predisposition [3][4]
- Prior postterm pregnancies
- Nulliparity
- Fetal factors [4]
- Male fetus
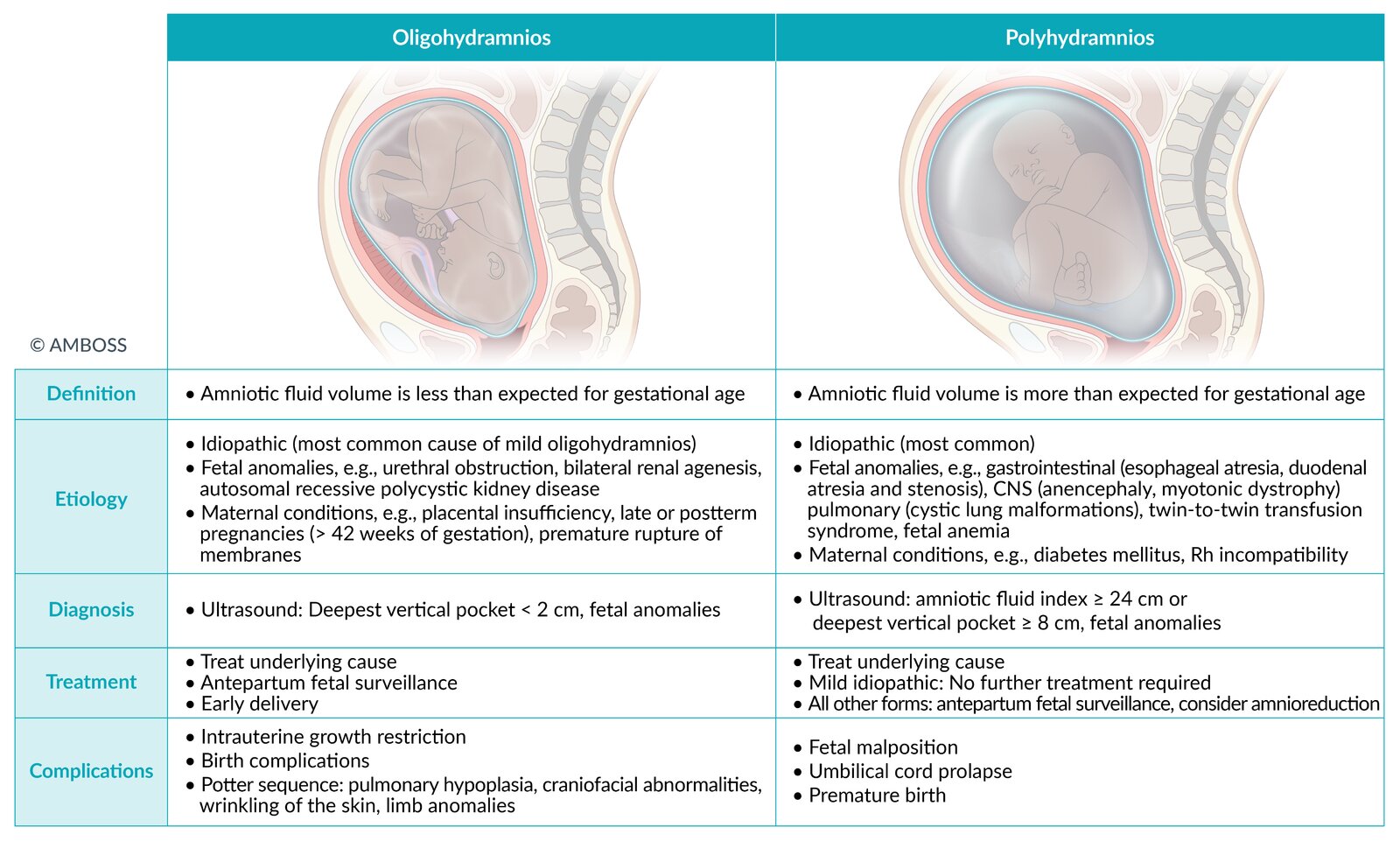
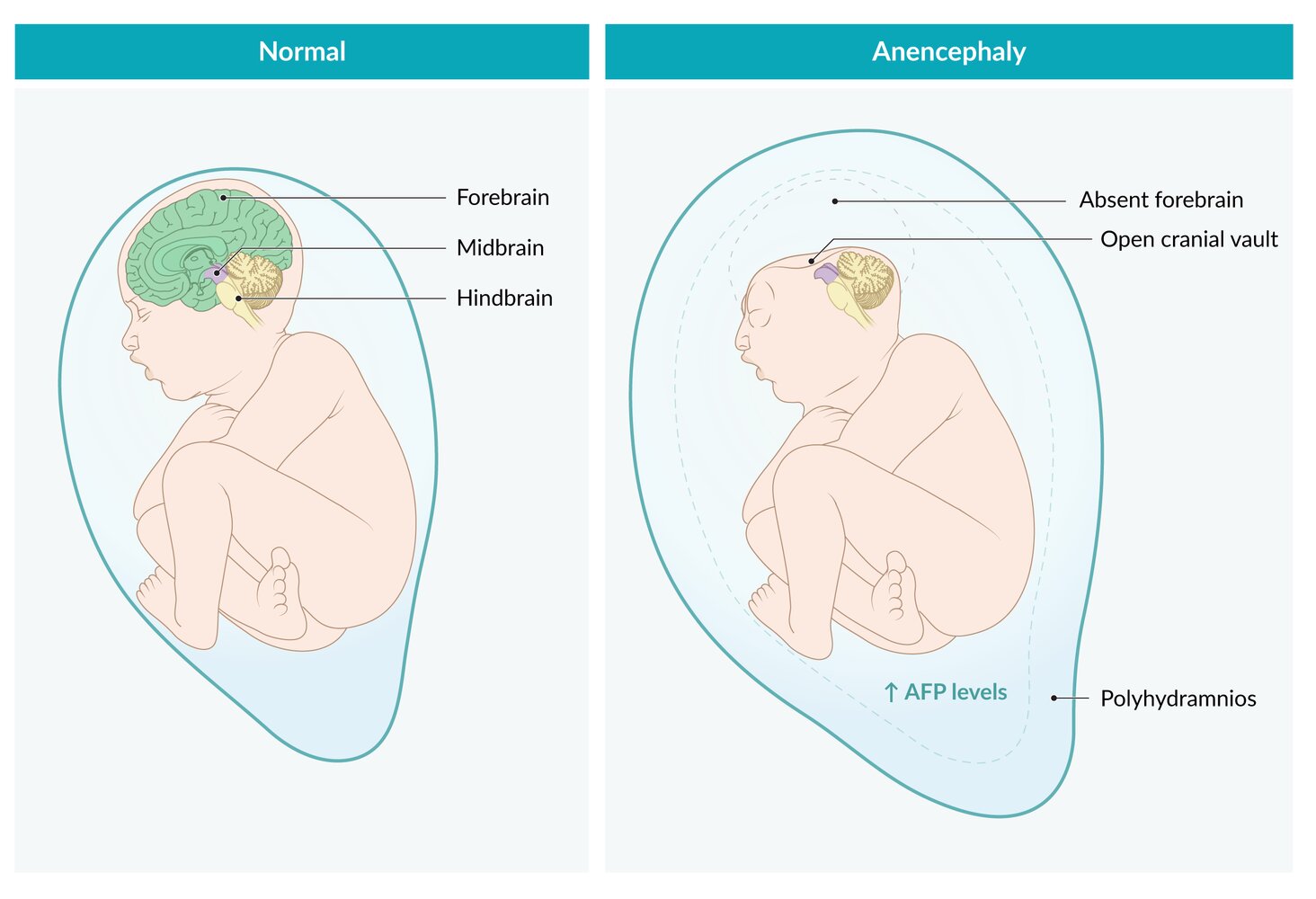
- Fetal disorders, e.g., oligohydramnios , anencephaly , steroid sulfatase deficiency [3]
- Maternal factors [4]
Many supposed cases of postterm pregnancy are likely due to suboptimal dating e.g., by using the LMP alone to calculate the EDD. [1][4]


© AMBOSS
© AMBOSS
Management
This applies to patients without high-risk pregnancy, indications for cesarean delivery, or contraindications for induction of labor.
Late-term pregnancy [1][4]
Begin by confirming whether the gestational age and estimated date of delivery for the pregnancy was accurately calculated.
First-trimester prenatal ultrasound is preferred over other methods of determining gestational age and estimated date of delivery. [1][3][5]

Suboptimally dated gestational age [6]
- Definition: a gestational age that was not confirmed or adjusted using ultrasound before 22 0/7 weeks gestation
- Perform induction of labor at 41 weeks' gestation (as determined by best clinical judgment).
Well-dated gestational age
Offer the following, using a shared decision-making approach:
- Membrane sweeping, if not previously done
- Choice of the following options:
- Induction of labor
- Expectant management with antepartum fetal surveillance
| Management options for low-risk, well-dated late-term pregnancies [1][4][7] | ||
|---|---|---|
| Induction of labor | Expectant management | |
| Key points for patient counseling |
|
|
| Management steps |
|
|
Postterm pregnancy [1][4]
- Perform induction of labor by 42 0/6 weeks' gestation. [1]
- Induction unsuccessful: Perform C-section.
After 42 weeks' gestation, induction is recommended regardless of cervical favorability in order to avoid complications of postterm pregnancy. [1]
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Complications
Postterm infant complications [1][3]
- Oligohydramnios
-
Increased birth weight and macrosomia, which can lead to birth trauma, e.g.:
- Neonatal brachial plexus palsy
- Birth-related clavicle fracture
- Stillbirth
- Low Apgar scores (i.e., ≤ 4 points) [1]
- Meconium aspiration syndrome
- Neonatal seizures [1][4]
- Admission to the NICU
- Cerebral palsy [4]
- Postmaturity syndrome: changes in appearance (i.e., weight loss, subcutaneous wasting, and dry, peeling skin) possibly caused by placental insufficiency and oligohydramnios [1][10]
Infants born postterm have an increased risk of meconium aspiration syndrome. [1][10]
")

Maternal complications [1][3]
- Associated with increased birth weight and fetal macrosomia:
- Prolonged stages of labor (see “Abnormal labor stages”)
- Obstructed labor
- Perineal lacerations
- Postpartum hemorrhage
- Infections: e.g., chorioamnionitis or endometritis [4]
We list the most important complications. The selection is not exhaustive.

The affected right arm is in adduction and internal rotation, with the forearm extended and pronated.
These features are characteristic of Erb palsy. The wrist and fingers are typically also flexed in this condition, but the child's clothing makes assessment of the degree of flexion difficult here.
Source: “Fig. 1, in: Oberlin partial ulnar nerve transfer for restoration in obstetric brachial plexus palsy of a newborn: case report” by Shigematsu K, Yajima H, Kobata Y, et al, Journal of Brachial Plexus and Peripheral Nerve Inury, licensed under CC BY 2.0.
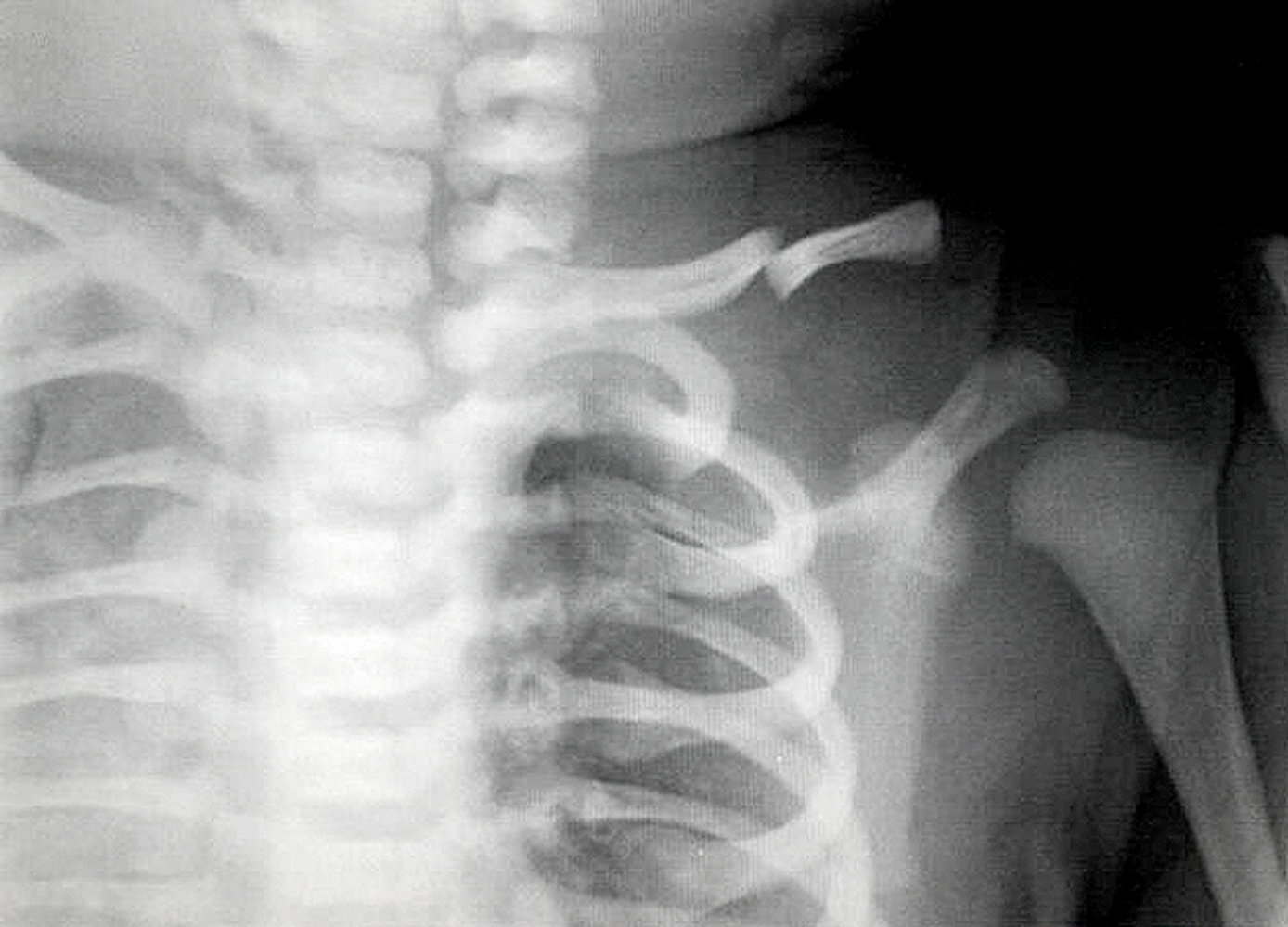
X-ray upper chest (AP view) of a newborn
A complete fracture of the mid-third of the left clavicle shows overriding of the fragments (green overlay).
Fractures of the clavicle are the most common birth trauma and may be complete or incomplete. Major causes include extended arms in breech presentation deliveries and shoulder dystocia in vertex presentation deliveries.
1: left first rib; white outlines: clavicle
Source: “Neonatal clavicle fracture” by ADMIN, http://www.anatomybox.com, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Prevention
Membrane sweeping [1][11][12]
- Definition: a procedure involving manually separating the amniotic membranes from the lower uterus wall during a pelvic examination
- Timing: may be performed at or after 39 0/7 weeks' gestation [11]
-
Goals
- Promote the onset of normal spontaneous labor [11]
- Decrease the risk of late-term and postterm pregnancy and need for induction
-
Risks include:
- Vaginal bleeding
- Pain
- Irregular contractions
- Contraindications: See “Contraindications for induction of labor.”
External Resources
References
- ACOG. "Practice Bulletin No. 146: ACOG Management of Late-Term and Postterm Pregnancies". Obstet Gynecol. 124(2). :390-396. (2014)
- Mandruzzato G, Alfirevic Z, Chervenak F, et al. "Guidelines for the management of postterm pregnancy". J Perinat Med. 38(2). (2010)
- Wang M, Fontaine P. "Common questions about late-term and postterm pregnancy". Am Fam Physician. 90(3). :160-5. (2014)
- Tinofeev, J.. "Postterm Pregnancy". Postgraduate Obstetrics & Gynecology. 31(18). :8. (2011)
- "Births: Final Data for 2020"
- Wheeler V, Hoffman A, Bybel M. "Cervical Ripening and Induction of Labor". Am Fam Physician. 105(2). :177-186. (2022)
- Adams R, Lichorad A, Simmons J. "Membrane Sweeping to Decrease Rates of Postdate Induction". Am Fam Physician. 95(1). :35-36. (2017)
- "Methods for estimating due date". https://www.acog.org/-/media/project/acog/acogorg/clinical/files/committee-opinion/articles/2017/05/methods-for-estimating-the-due-date.pdf. [2017-05-01]
- ACOG. "Committee Opinion No. 688: Management of Suboptimally Dated Pregnancies". Obstetrics & Gynecology. 129(3). :e29-e32. (2017)
- Philippa Middleton, Emily Shepherd, Jonathan Morris, Caroline A Crowther, Judith C Gomersall. "Induction of labour at or beyond 37 weeks' gestation". Cochrane Database Syst Rev. 2020(8). (2020)
- Caughey AB, Cahill AG, Guise JM, Rouse DJ. "Safe prevention of the primary cesarean delivery". Am J Obstet Gynecol. 210(3). :179-193. (2014)
- ACOG. "Indications for Outpatient Antenatal Fetal Surveillance (reaffirmed 2024)". Obstetrics & Gynecology. 137(6). :e177-e197. (2021)