Summary
The lymphatic system is part of the adaptive immune system as well as the circulatory system and comprises the thymus and bone marrow (primary lymph organs); mucosa-associated lymphatic tissue (MALT), the spleen, and the lymph nodes (secondary lymphatic organs); the lymphatic vessels and capillaries; and the lymph fluid. The primary function of the lymphatic system is to return excess interstitial fluid and waste products, such as proteins and cellular debris, to the bloodstream. The interstitial fluid is absorbed by lymphatic capillaries throughout the body via diffusion. The lymph fluid is then transported through the network of lymphatic vessels and lymph nodes to the right lymphatic duct, which drains into the right subclavian vein, and the thoracic duct, which drains into the left subclavian vein. Its secondary function is immune defense, which mainly involves the transport of leukocytes (esp. lymphocytes) between the bone marrow and the lymph nodes and the stimulation of immune response through the transport of antigen-presenting cells to the lymph nodes. Another function is the transport of fats as chyle from the digestive system to the bloodstream. Accordingly, lymph fluid is transparent when initially formed from the interstitial fluid but adopts a milky appearance as it accumulates proteins, fats, cellular debris, and leukocytes.
The lymph nodes are the main sites for lymph filtration and the storage of lymphocytes, including B cells, which mature and differentiate in the bone marrow, and T cells, which likewise form in the bone marrow but migrate to the thymus for maturation. Antigen presentation induces the differentiation and proliferation of B lymphocytes and the activation of T lymphocytes. Following antigen presentation, mature lymphocytes differentiate into effector cells in the secondary lymph organs. Lymph node clusters exist throughout the body, some of which are palpable (e.g., cervical lymph nodes) while others are not (e.g., mediastinal lymph nodes). They may become enlarged in response to inflammatory processes due to local infection, malignancy, or granulomatous disease.
Primary lymphatic organs
Lymphocytes form and mature in the primary lymphatic organs (the bone marrow and thymus). Both B lymphocytes and T lymphocytes arise from hematopoietic stem cells in the bone marrow. While B lymphocytes remain within the bone marrow during the process of maturation, T lymphocytes migrate to the thymus to mature and differentiate.
Bone marrow
-
B lymphocytes and T lymphocytes originate from pluripotent stem cells in the bone marrow.
- T lymphocytes migrate to the thymus to mature and differentiate.
- B lymphocytes mature in the marrow and migrate to secondary lymphatic organs to form follicles and proliferate.
Bone marrow: B cell maturation; Thymus: T cell maturation

Thymus
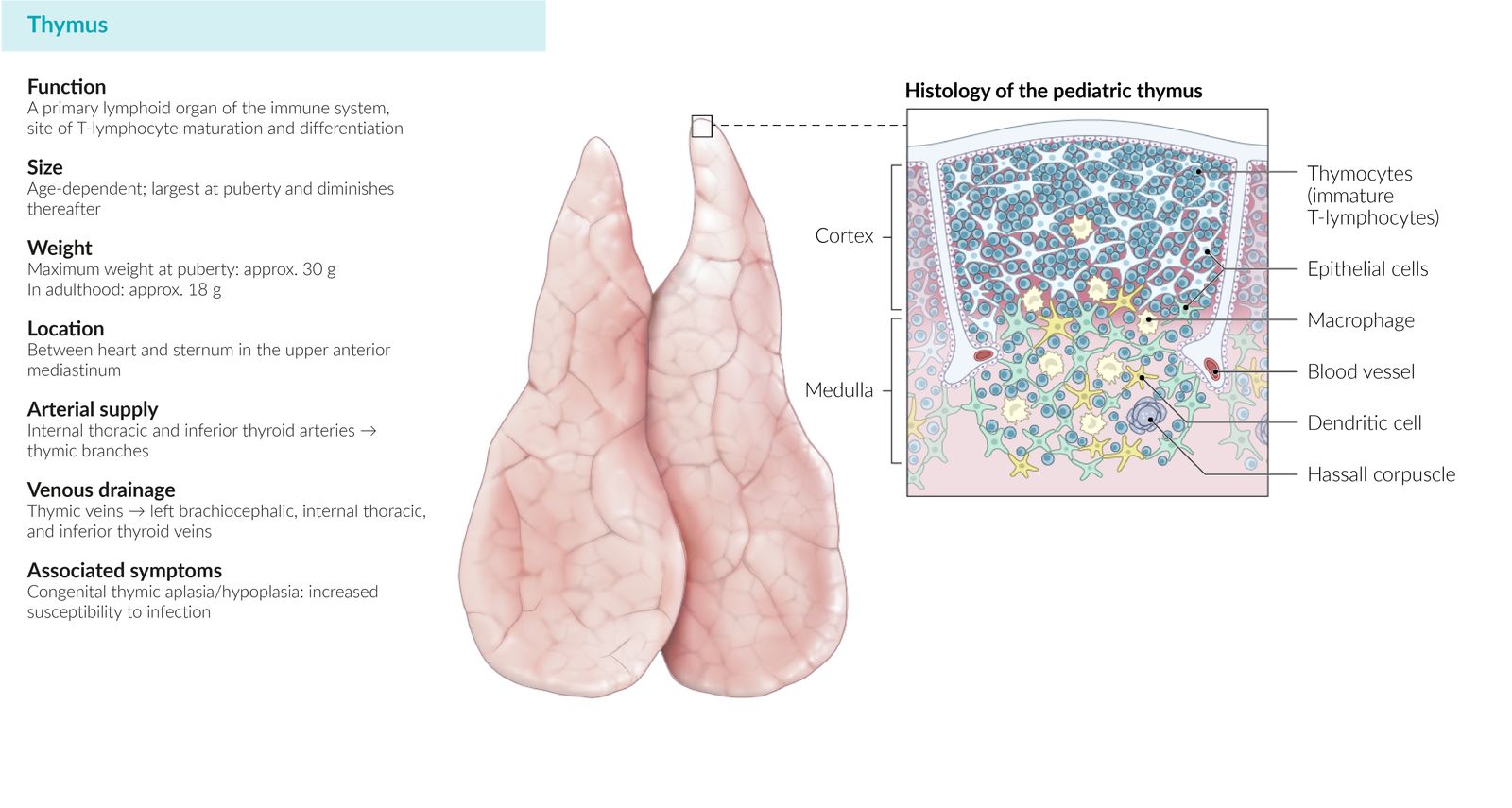
- Function: maturation and differentiation of T lymphocytes
-
Location
- Superior anterior mediastinum
- Retrosternal, precordial
-
Structure: bilobar organ surrounded by a fibrous capsule
-
Neonates and infants
- The largest and most active thymus
- A prominent thymic shadow can be seen on chest x-ray (thymic sail sign).
- Involution begins at 1 year of age. [1]
-
Adults
- Atrophic, mostly replaced by fatty tissue
- Thymus undergoes age-related thymic involution.
-
Neonates and infants
-
Histology
- Thymic epithelial cells, dendritic cells, and macrophages
-
Thymic cortex
- Peripheral region
- Dark
- Densely packed, immature T lymphocytes (thymocytes)
-
Thymic medulla
- Central region
- Light
- Fewer cells: mature T lymphocytes and Hassall corpuscles that consist of concentrically arranged eosinophilic reticular cells (onion-like appearance)
-
Embryology
- Thymus epithelium arises from the 3rd pharyngeal pouch (endoderm).
- Thymic lymphocytes originate from the mesoderm.
-
Clinical significance
- Thymic hypoplasia or aplasia: DiGeorge syndrome, SCID
- True thymic hyperplasia : secondary to steroid therapy, chemotherapy
- Thymic lymphoid hyperplasia : certain autoimmune diseases (e.g., myasthenia gravis, SLE, and rheumatoid arthritis)
-
Thymoma: tumor of thymic epithelial cells
- Seen in the context of myasthenia gravis, pure red cell aplasia, immunodeficiency with thymoma
- An asymptomatic thymoma is usually detected as an incidental finding on a chest x-ray, where it appears as an anterior mediastinal mass.
- Symptomatic thymomas typically manifest in individuals 40–60 years of age with thoracic symptoms (e.g., chest pain, cough, dyspnea, SVC syndrome) or paraneoplastic syndromes.
- Treatment: options include surgery, chemotherapy, and/or radiotherapy.
- Thymic carcinoma: more aggressive than thymoma (mediastinal invasion and extrathoracic metastasis)
The Thymus arises from the Third pharyngeal pouch.
DiGeorge syndrome is caused by abnormal development of the 3rd and 4th pharyngeal pouches, which prevents the formation of thymus and parathyroid glands. As a result, patients with DiGeorge syndrome have an increased susceptibility to hypocalcemia and viral and fungal infections.
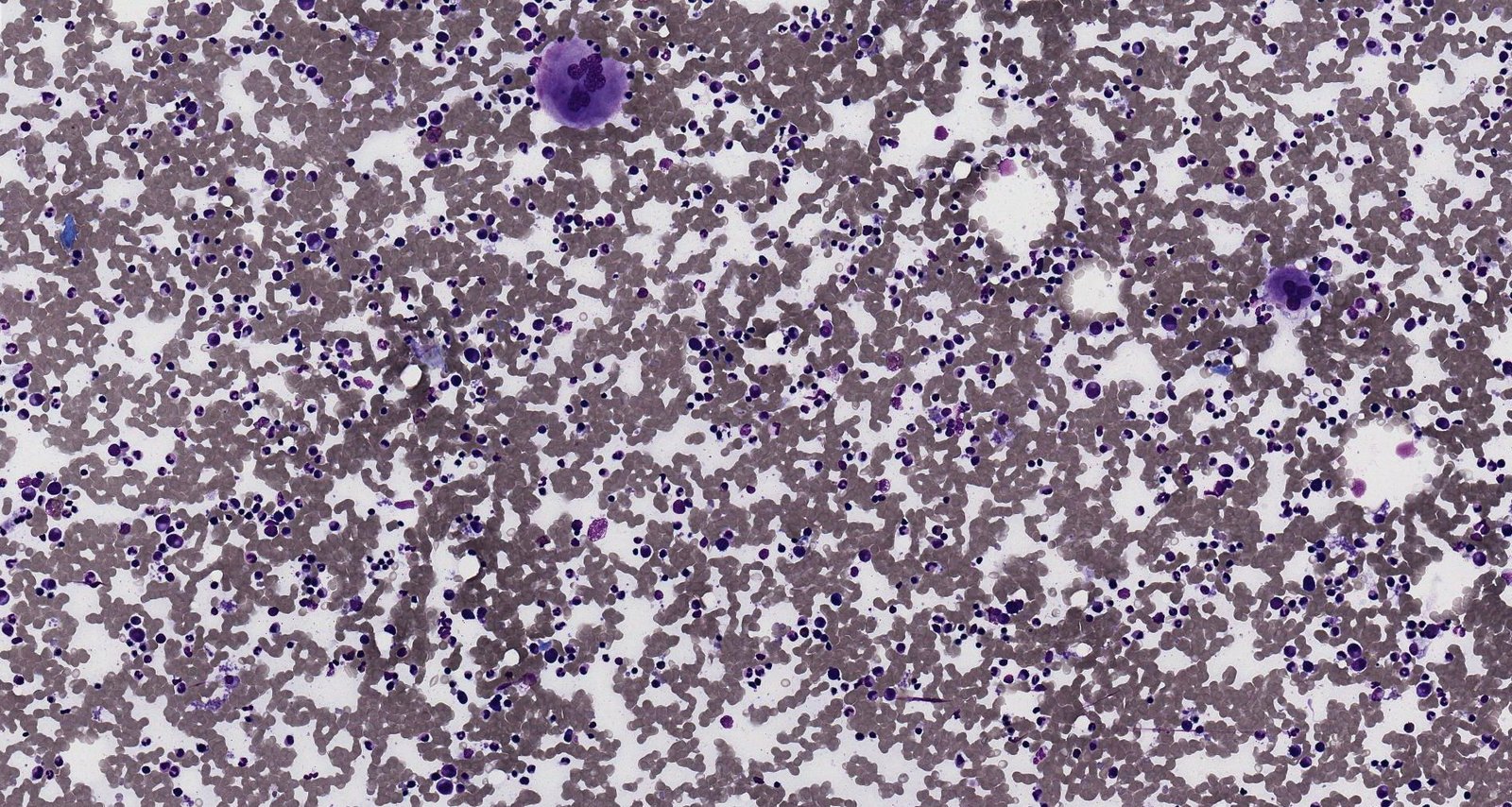
Photomicrograph of a bone marrow smear (H&E stain; high magnification)
Numerous, darkly stained granulocytes can be seen within a sea of red blood cells at various stages of development. Several eosinophils (red-stained cells), basophils (dark blue-stained cells), and two large megakaryocyte cells are also visible (center right; center left).
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: Prof. Dr. Karl-Anton Kreuzer, Facharzt für Innere Medizin, Hämatologie und Onkologie
© AMBOSS
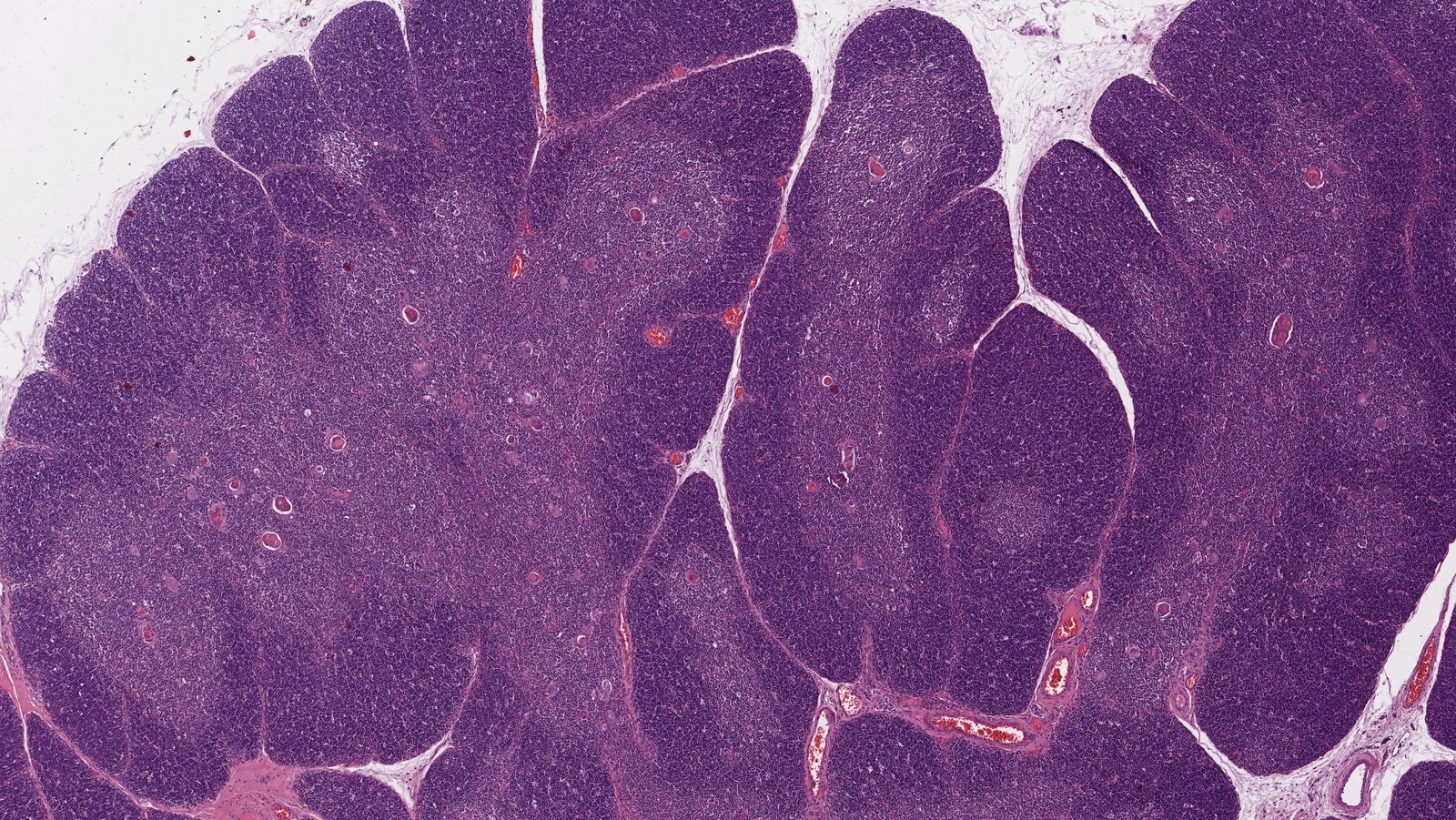
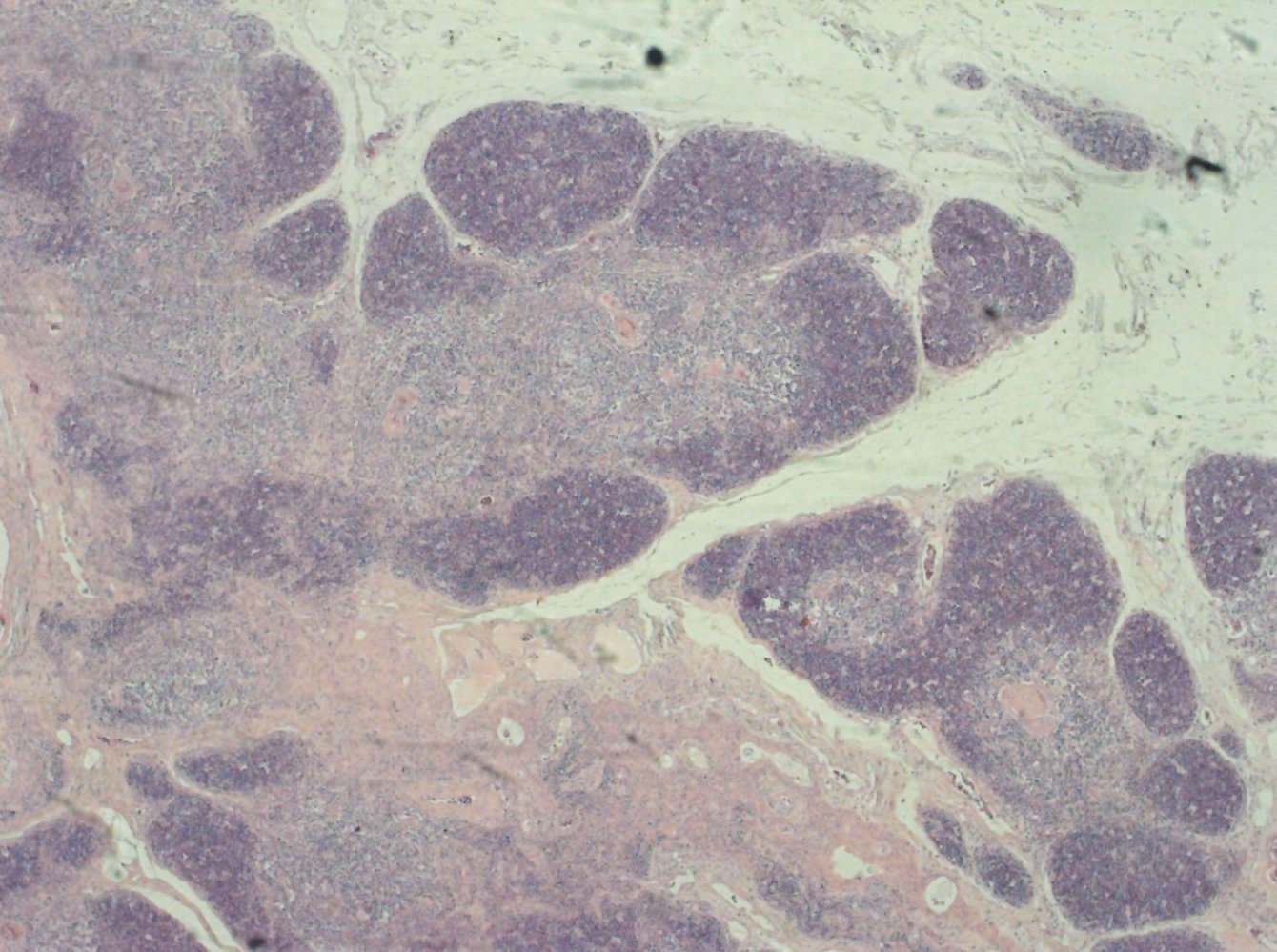
Microscopic image of the thymus (H&E stain, 25x magnification)
The thymus retains its characteristic two-layered structure until puberty. The lymphocyte-rich cortex (dark purple) is clearly distinguishable from medulla with its lower density of lymphocytes and presence of thymic corpuscles (red).
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
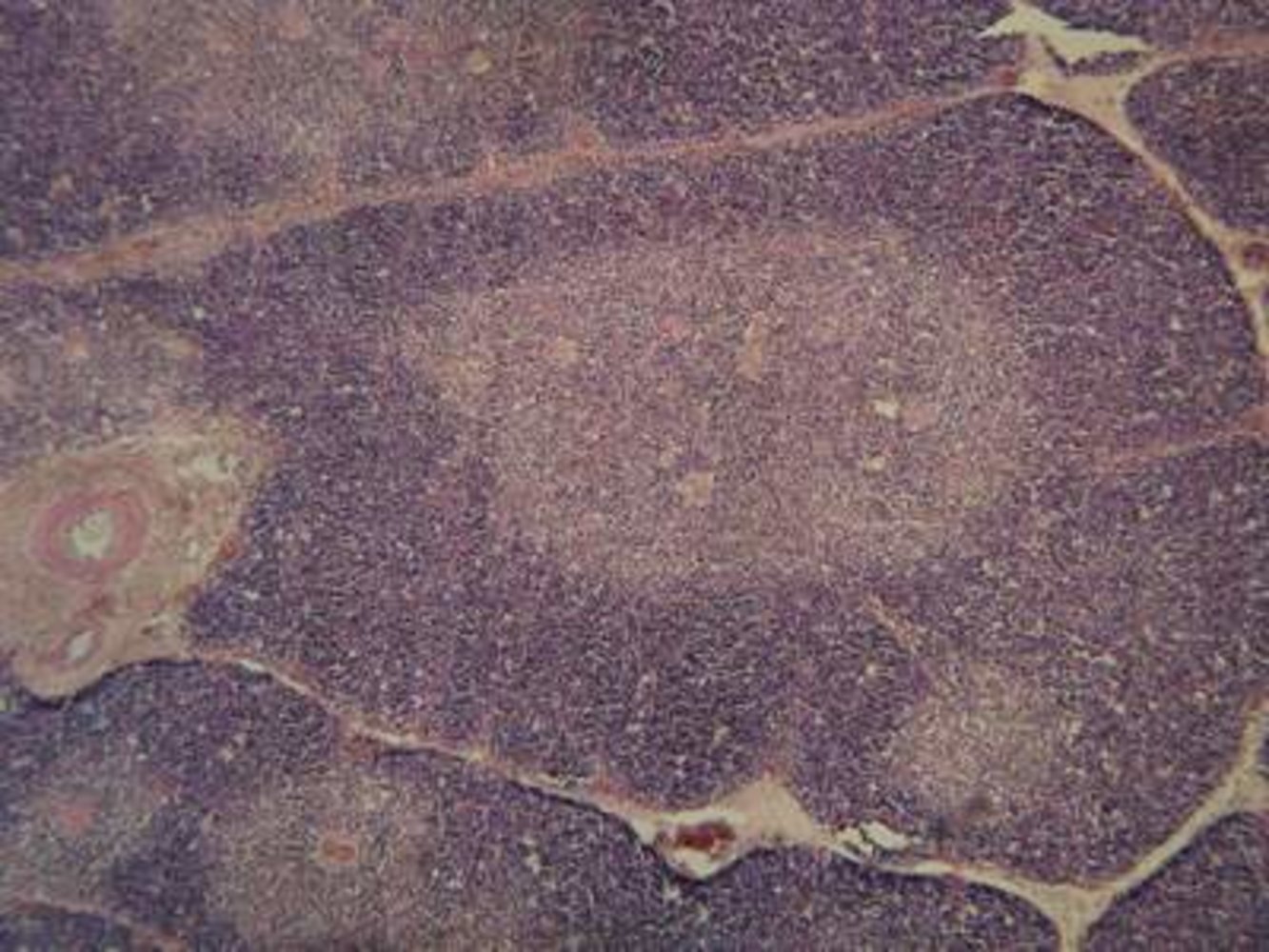
Photomicrograph of a child's thymus (H&E stain)
The cortex (rich in lymphocytes, resulting in a dark purple color) and the medulla (fewer lymphocytes, lighter color) can be clearly distinguished.
Thymic corpuscles (red) are visible in the medulla.
Source: “Thymuslobje 50 x vergroot” by Tourbulence, Wikipedia Commons, licensed under CC BY-SA 3.0.

X-ray chest (AP view) of an infant
A homogeneous soft tissue opacity representing normal thymic tissue extends laterally from the right side of the superior mediastinum into the right upper hemithorax. Its lateral border is convex while its inferior border is straight (green overlay) producing a sail-like appearance (illustration) that has been termed the thymic sail sign.
Source: “Radiology 1300566 Nevit” by Nevit Dilmen, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
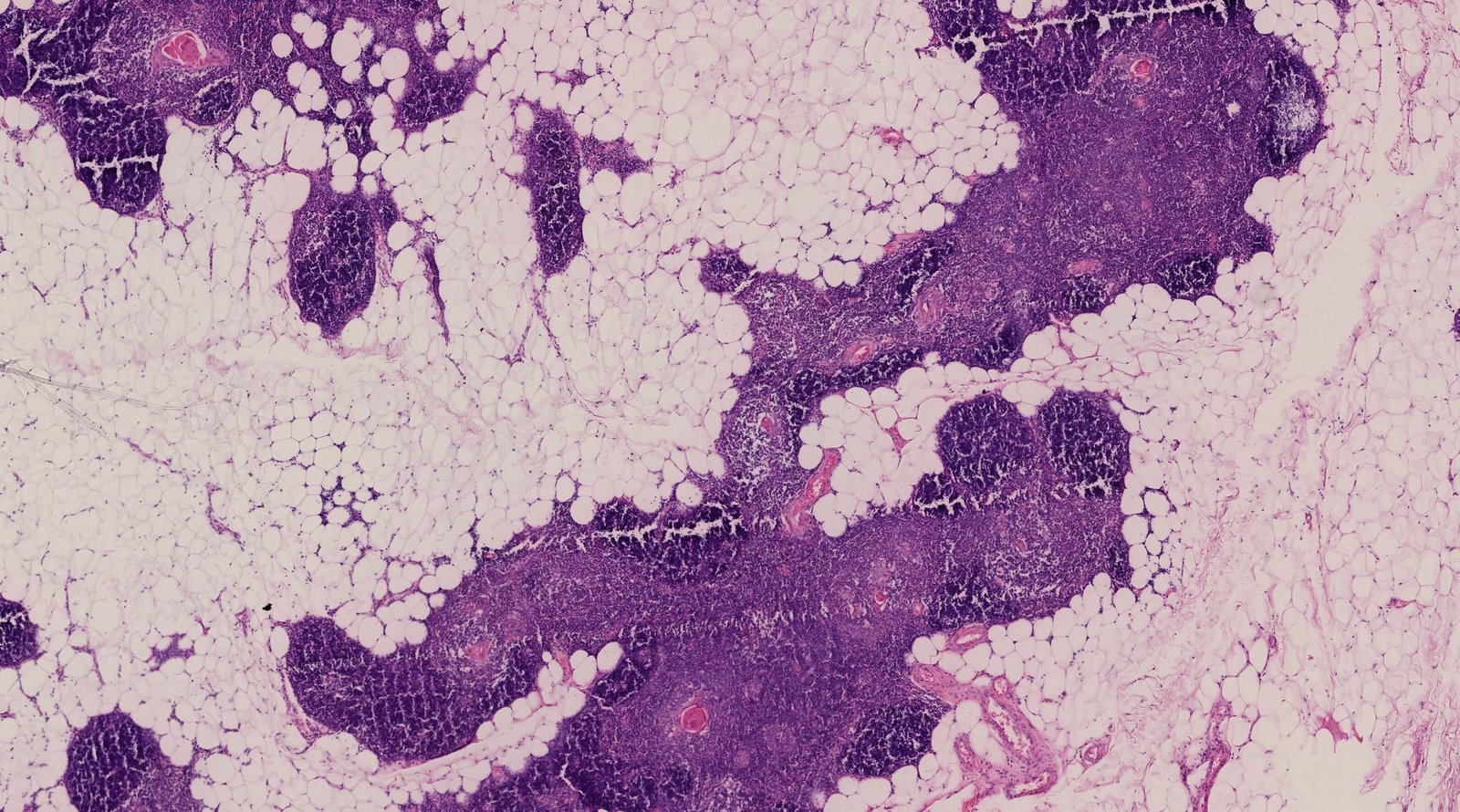
Microscopic image of the thymus (H&E stain, 25x magnification)
Age-related thymic involution occurs after puberty. The parenchyma of the thymus (purple) loses mass and is replaced by adipose tissue (pale pink). The thymic cortex (dark purple) is affected to a greater degree by this process than the medulla (light purple), which contains thymic corpuscles (red) are visible.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
Photomicrograph of thymus tissue
The cortex (e.g., red overlay) is rich in lymphocytes and divided into lobules by strands of connective tissue (e.g., yellow overlay).
The medulla (green overlay) contains the eosinophilic Hassall corpuscles (white arrowheads), which are composed of epithelial reticular cells (the cells in the center of those corpuscles are degenerated and keratinized). Hassall corpuscules are characteristic of thymus tissue.
Source: © IMPP

Photomicrograph of thymic biopsy depicting the thymic medulla (H&E stain)
Concentric eosinophilic whorls (green overlay) composed of elongated eosinophilic epithelial cells (blue overlay) of the thymus with pale nuclei are seen in the center of the image.
This is the characteristic appearance of Hassal corpuscles that are normally present in the thymic medulla.
Numerous mature T lymphocytes (black arrowhead) and thymic epithelial cells (yellow overlay) surround the corpuscles.
Source: “Thymic corpuscle” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Secondary lymphatic organs
The secondary lymphatic organs are the spleen, lymph nodes, and mucosa-associated lymphatic tissue (e.g., the Peyer patches and tonsils). It is in the secondary lymphatic organs that antigen presentation occurs. They are also the site of differentiation of mature, naive lymphocytes into effector cells.
Spleen
-
Function
- Filtration of old or misshapen RBCs and platelets
- Vital role in forming and initiating a humoral immune response through B and T lymphocytes
- See “Spleen” for more information.
-
Location
- Underneath the left part of the diaphragm
- Close to the left kidney (anterolateral)
- Behind the ninth, tenth, and eleventh ribs
-
Structure
-
White pulp is responsible for antigen filtration and presentation, and contains the following structures:
- Lymphoid follicles: house large numbers of B lymphocytes
- Periarteriolar lymphatic sheath: contains T lymphocytes
- Red pulp: responsible for blood filtration
-
White pulp is responsible for antigen filtration and presentation, and contains the following structures:
Lymph nodes
Function
- Nonspecific lymph filtration: macrophages within lymph node
- Storage and circulation of B cells and T cells
- Immune system activation: Antigen presentation induces differentiation and proliferation of B lymphocytes and activation of T lymphocytes.
Location
- Throughout the body in close proximity to organs and large vessels
- See “Lymph nodes clusters” below.
Structure
- Bean-shaped organ; surrounded by fibrous capsule with trabeculae
- The trabecular sinus leads lymph from the subcapsular sinus to the medullary sinus.
- The hilus
- Allows blood vessels and efferent lymphatic vessels to enter or leave the lymph node
- Typically, only one or a small number of efferent lymphatic vessels leave the lymph node, compared to the larger number of afferent lymphatic vessels that enter the lymph node through the cortex.
- The entering artery and vein branch into a large capillary network, which forms the post-capillary high endothelial venules.

Histology
-
Cortex (B-cell zone): contains lymphoid follicles, which is the site of B lymphocyte storage, differentiation, and proliferation
- Secondary lymphoid follicle (active): dense mantle zone; surrounding a pale germinal center
- Primary lymphoid follicle (inactive): dense aggregates of naive B lymphocytes
-
Paracortex (T-cell zone)
- Region between the cortex and medulla
- Contains T lymphocytes and high endothelial venules, which allows circulating B and T lymphocytes to enter or leave the bloodstream
- Site of T-cell activation
-
Medulla
- Medullary cords: tightly packed with plasma cells and lymphocytes
-
Medullary sinus of the lymph node
- Composed of macrophages, reticular cells
- Connected to the efferent lymphatic structures




Clinical significance
- Inflammatory or immune reactions (e.g., due to EBV infection) → reactive paracortical hyperplasia → clinically apparent lymphadenopathy (see “Lymphadenopathy”)
- Depletion of paracortical lymphocytes: DiGeorge syndrome


Mucosa-associated lymphoid tissues (MALT)
MALT include the tonsils, Peyer patches, and solitary lymphoid follicles of the mucosa; . The structure of MALT resembles that of other secondary lymphatic organs but it is also composed of a specialized reticular epithelium (follicle-associated epithelium) with a humoral defense mechanism . The follicle-associated epithelium of the gut-associated lymphatic tissue (GALT) contains M cells, which allow transcytosis of antigens into the lamina propria.
Peyer patches
-
Function
- Immune system activation in response to ingested pathogens
- M cells transport antigens from the intestinal lumen to antigen-presenting cells (e.g., macrophages) → B cells within the germinal center detect antigens and differentiate to plasma cells that secrete IgA → IgA acquires a secretory component and becomes secretory IgA → secretory IgA is transported across the intestinal epithelium and secreted on the luminal surface of the gut
- Location: ileum (lamina propria and submucosa)
-
Histology
- Aggregates of lymphoid follicles: contain numerous lymphocytes and dendritic cells
- Follicle-associated epithelium : site of specialized M cells

Tonsils
- Function: Waldeyer tonsillar ring (first line of defense against inhaled or ingested pathogens)
- Structure: similar to other secondary lymphatic organs
- Location and histology
| Characteristics of tonsils | ||||
|---|---|---|---|---|
| Characteristic | Pharyngeal tonsils (adenoids) | Palatine tonsils | Lingual tonsils | Tubal tonsils |
| Location |
|
|
|
|
| Histology |
|
|
|
|






Inducible bronchus associated lymphoid tissue (iBALT) [2][3][4]
- Location: walls of the upper and lower respiratory tracts (in the perivascular spaces)
- Function: immune system activation in response to antigens encountered in the upper and lower respiratory tracts following inflammation or infection
-
Structure and histology
- Central, large B-cell follicles with or without adjacent T-cell areas
- Numerous follicular dendritic cells
- Contains specialized stromal cells, lymphatics, and high endothelial venules
- Lacks an M cell-containing dome epithelium
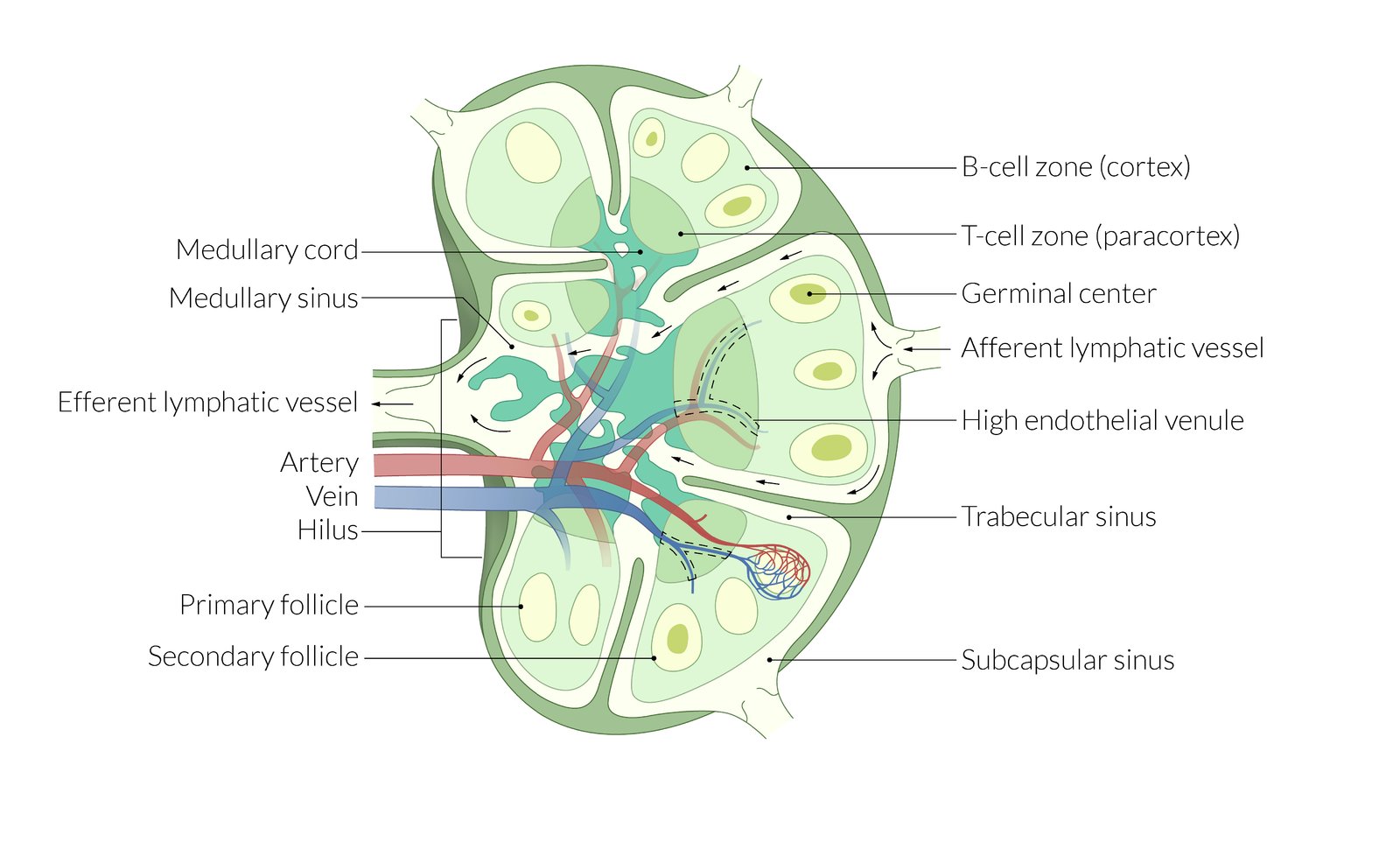
The parenchyma of the lymph node is divided into a B-cell zone (cortex), a T-cell zone (paracortex), and the marrow. The cortex contains primary and secondary lymph follicles with germinal centers, which allow affinity maturation of B cells. At the hilum (concave side), blood vessels enter and efferent lymphatic vessels leave the node. The entering artery and vein branch into a large capillary network. Special high endothelial venules in the paracortex allow for lymphocyte extravasation.
Afferent lymphatic vessels enter through the capsule at many points in the periphery and open into the subcapsular sinus. The cortical sinus runs from the cortex via the paracortex to the medullary sinus, which then drains into the efferent lymphatic vessel.
© AMBOSS
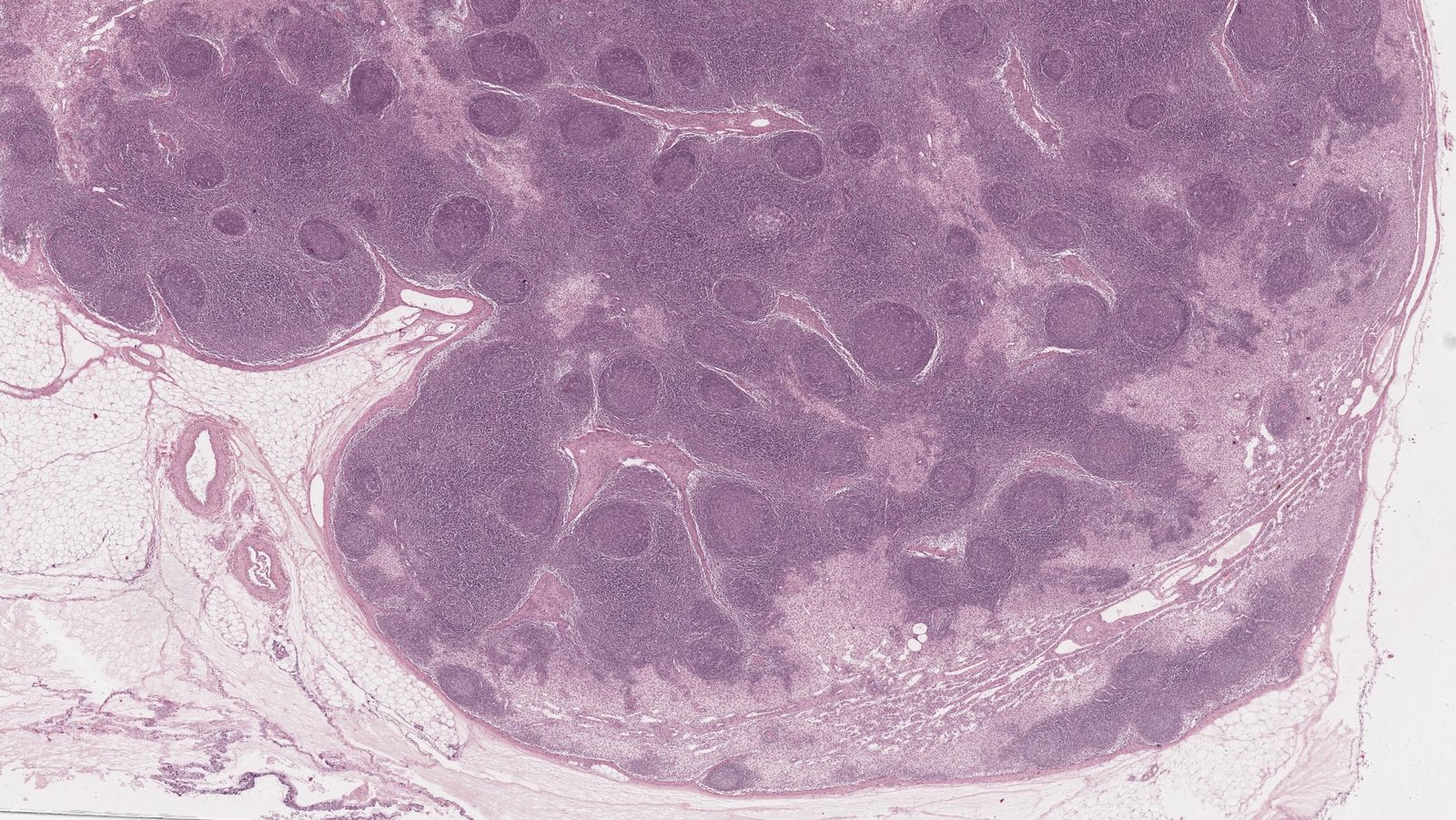
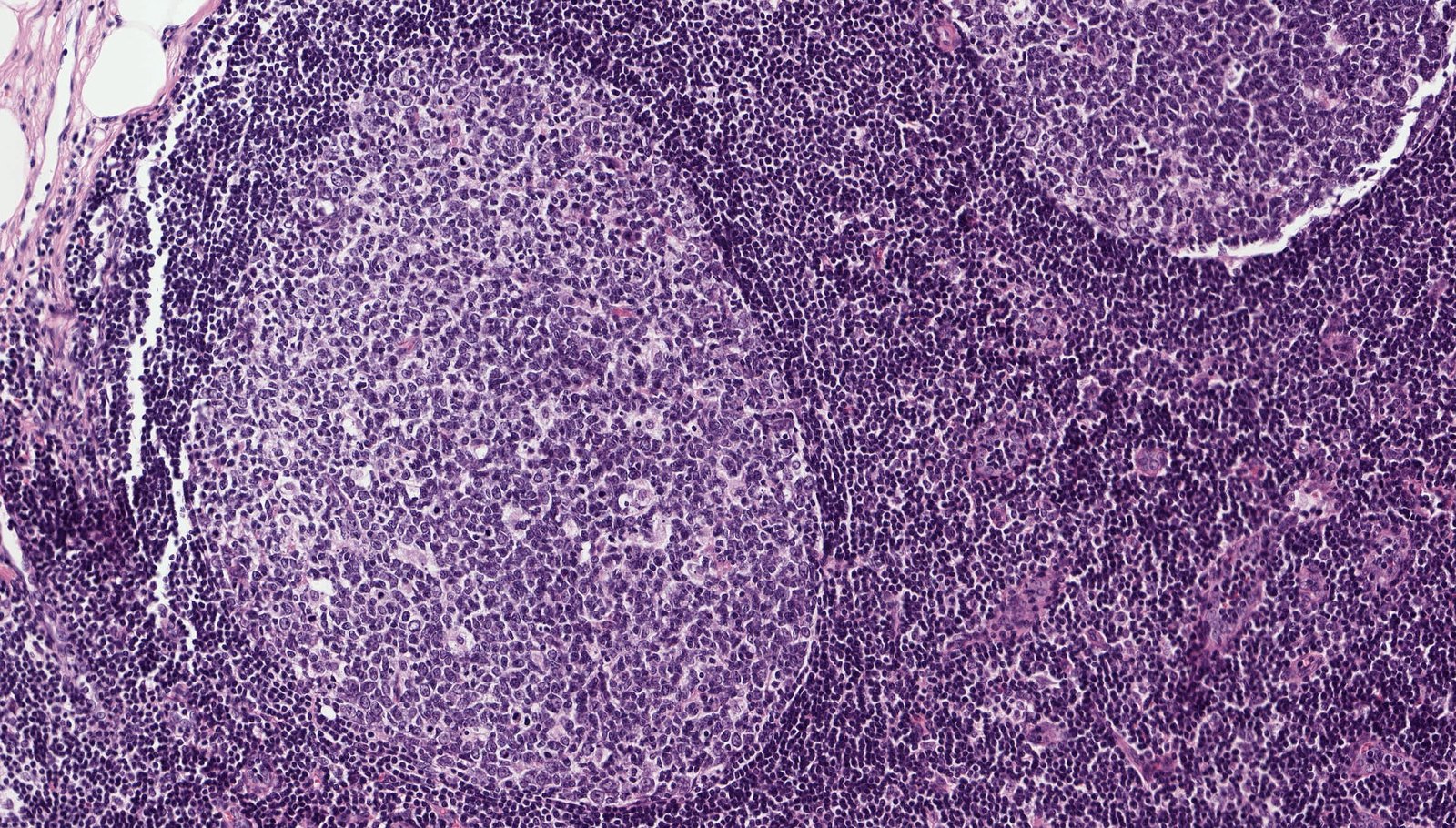
Photomicrograph of a lymph node tissue specimen (H&E stain, low magnification)
The cortex of a lymph node consists of numerous round lymph follicles (examples indicated by green overlay), in whose pale germinal centers B cells differentiate. The interfollicular areas are rich in T cells. The light areas represent the lymph sinuses (examples indicated by yellow overlay), which are rich in histiocytes.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
Microscopic image of a lymph node (H&E stain, 200x magnification)
The pale germinal center contains centroblasts and centrocytes. The darker mantle zone is composed of mature, naive B cells.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
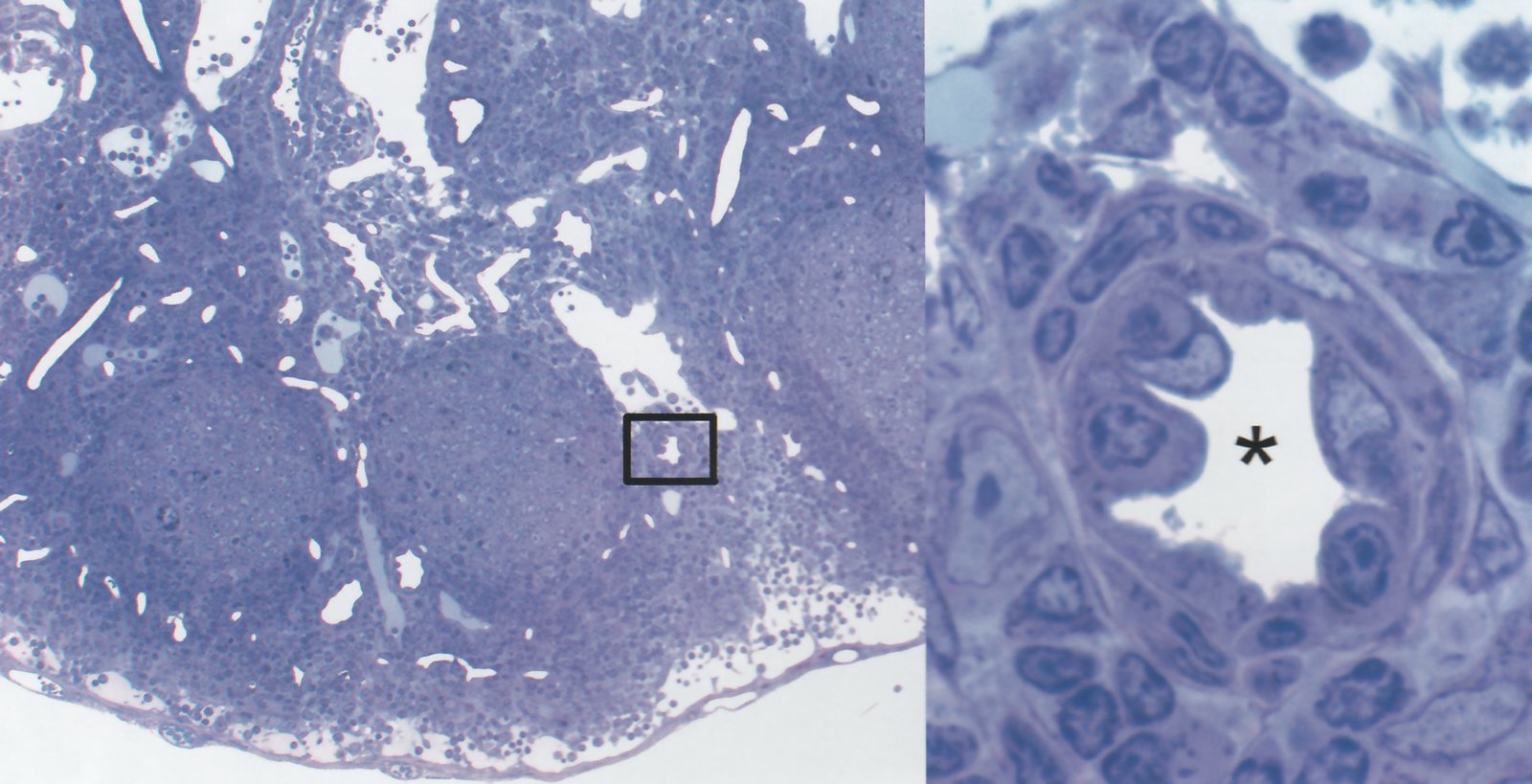
Photomicrograph of lymph node tissue (toluidine blue stain)
Left image (overview, low magnification): The B-cell zone (B) consists of several lymphoid follicles (here, three secondary follicles can be seen) with a light germinal center (yellow overlay) and a darker margin (red overlay).
The T-cell zone (T) is homogeneous and mainly contains naive T lymphocytes and high endothelial venules (HEV; black box).
Right image (cross section of an HEV; high magnification detail of black box): HEV (lumen: asterisk) enable lymphocytes in the circulation to enter lymph nodes. The endothelium of HEV is characteristically cobble-shaped with round cell nuclei.
Source: © IMPP
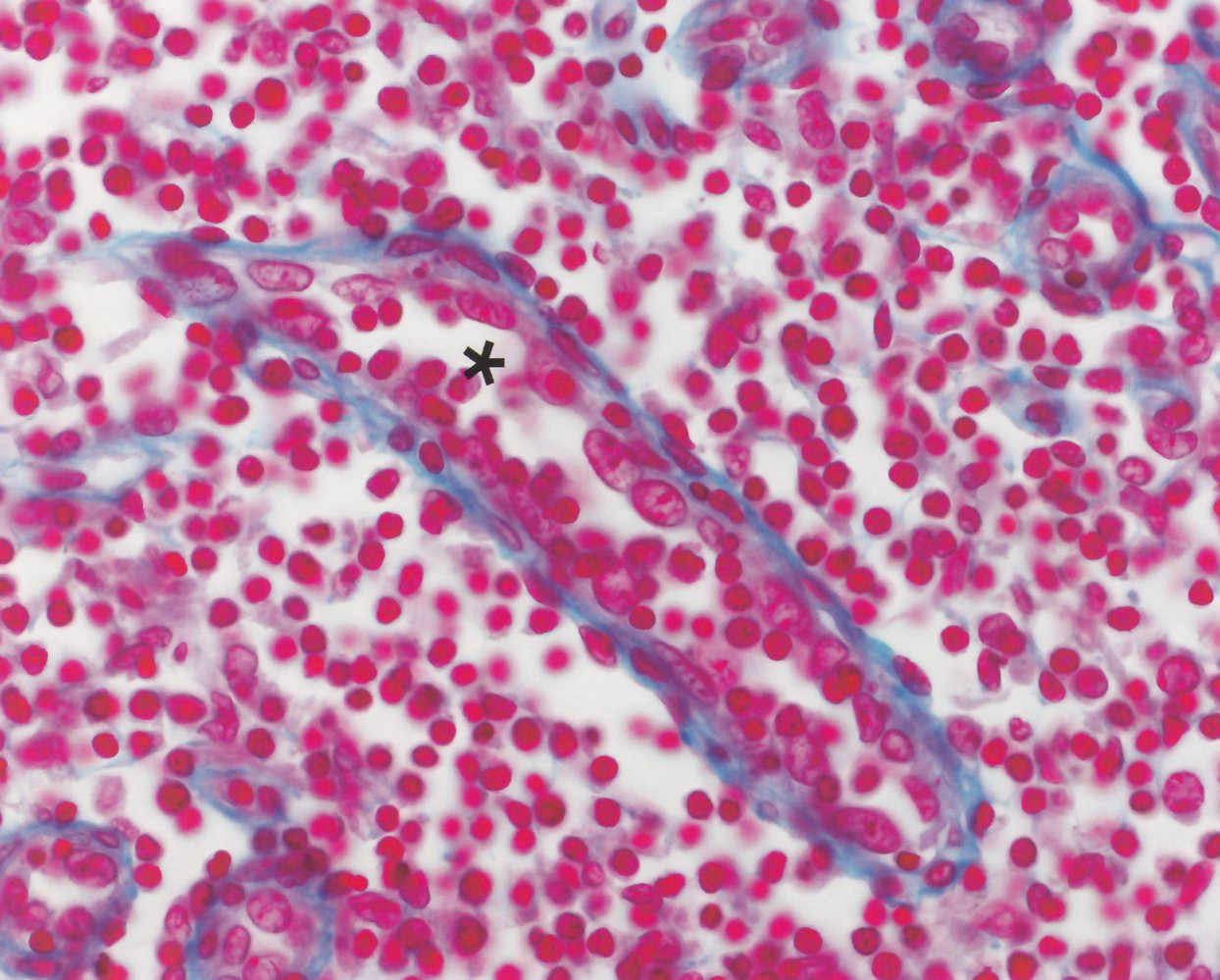
Microscopic image of a lymph node (azan stain, 550x magnification)
The asterisk indicates a high endothelial venule (HEV), sectioned longitudinally. HEVs are lined by cuboidal endothelium with prominent nuclei (black outlines). Additional transverse sections of HEV are marked by arrowheads.
The endothelium is situated on a blue-stained, discontinuous basement membrane. HEVs are located in the parafollicular T zone (green overlay highlights numerous round T cell nuclei) in secondary lymphatic organs (apart from the spleen) and permit recirculation of lymphocytes (white outline).
Source: © IMPP

© AMBOSS

© AMBOSS
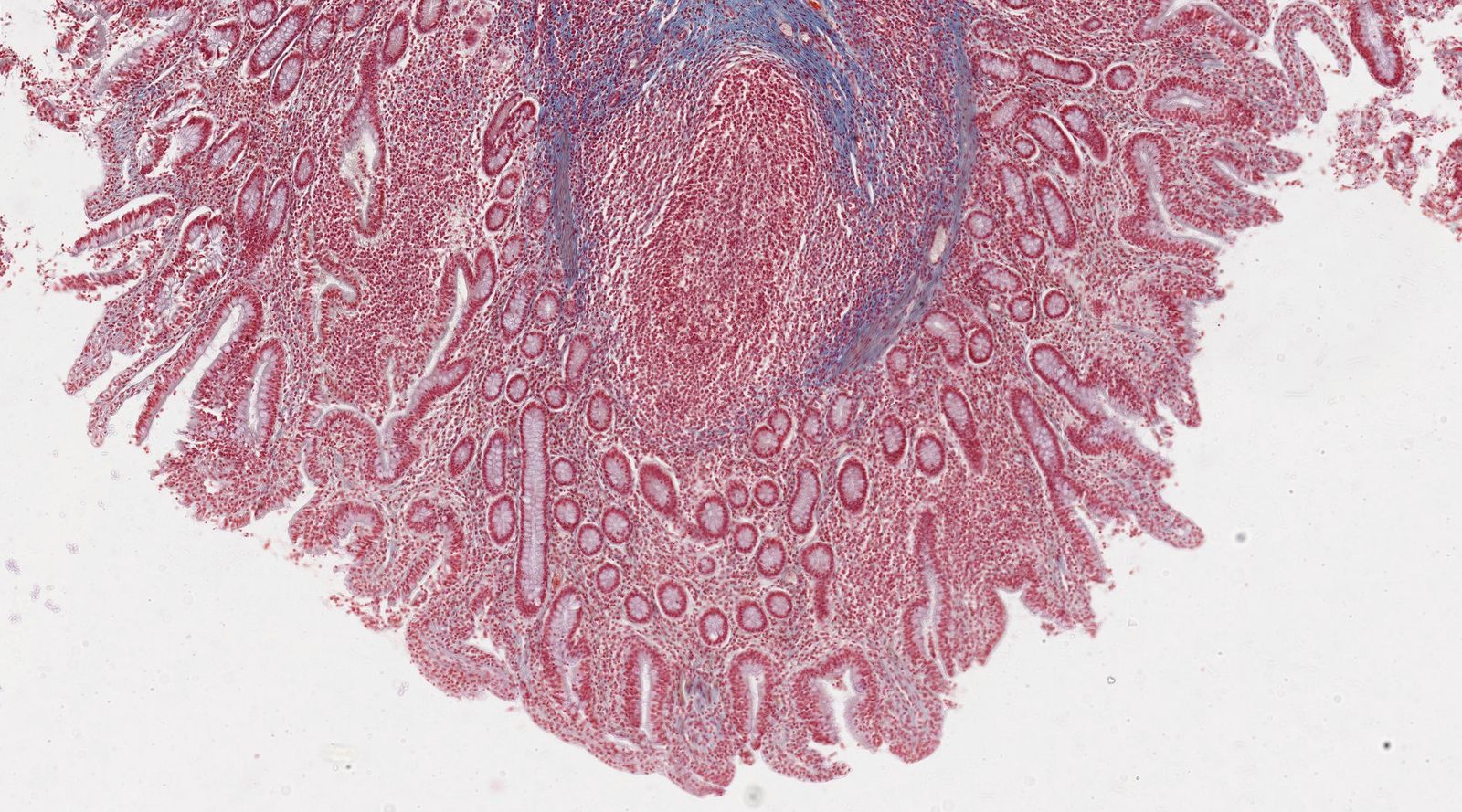
Photomicrograph of ileal tissue (Masson trichrome stain; low magnification)
Peyer patches (example indicated by green overlay) are large, secondary lymphoid follicles within the ileal mucosa and submucosa. They are covered by the ileal epithelium, which is composed of villi and crypts.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
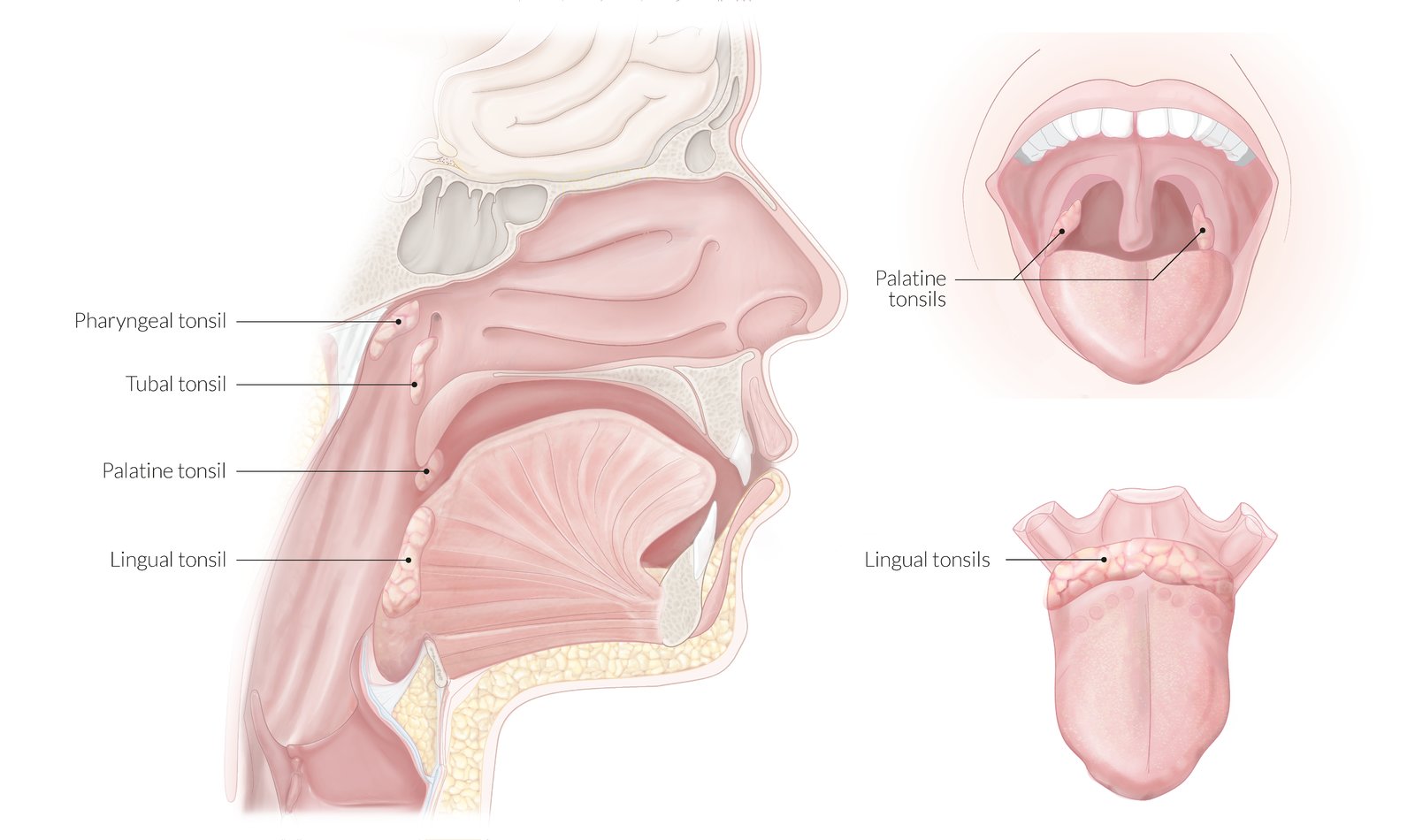
The tonsils are lymphatic organs located between the oral and nasal cavity and the pharynx. The tonsils are part of the immune system's mucosa-associated lymphoid tissue (MALT).
The pharyngeal tonsil is located at the roof of the nasopharynx. The paired tubal tonsils are located in proximity of the opening of the eustachian tube. In the oropharynx, the paired palatine tonsils are based in the tonsillar fossa, and the unpaired lingual tonsil is situated at the root of the tongue.
© AMBOSS
Microscopic image of adenoid tissue (H&E stain, 50x magnification)
The surface of the adenoid is lined with a pseudostratified ciliated columnar epithelium that allows for clear distinction from the tonsils, which are lined with a nonkeratinized stratified squamous epithelium. Beneath the epithelial lining, lymphatic nodules (purple, round) with germinal centers and seromucous glands with ducts extending to the surface (pink, left of center) are visible.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
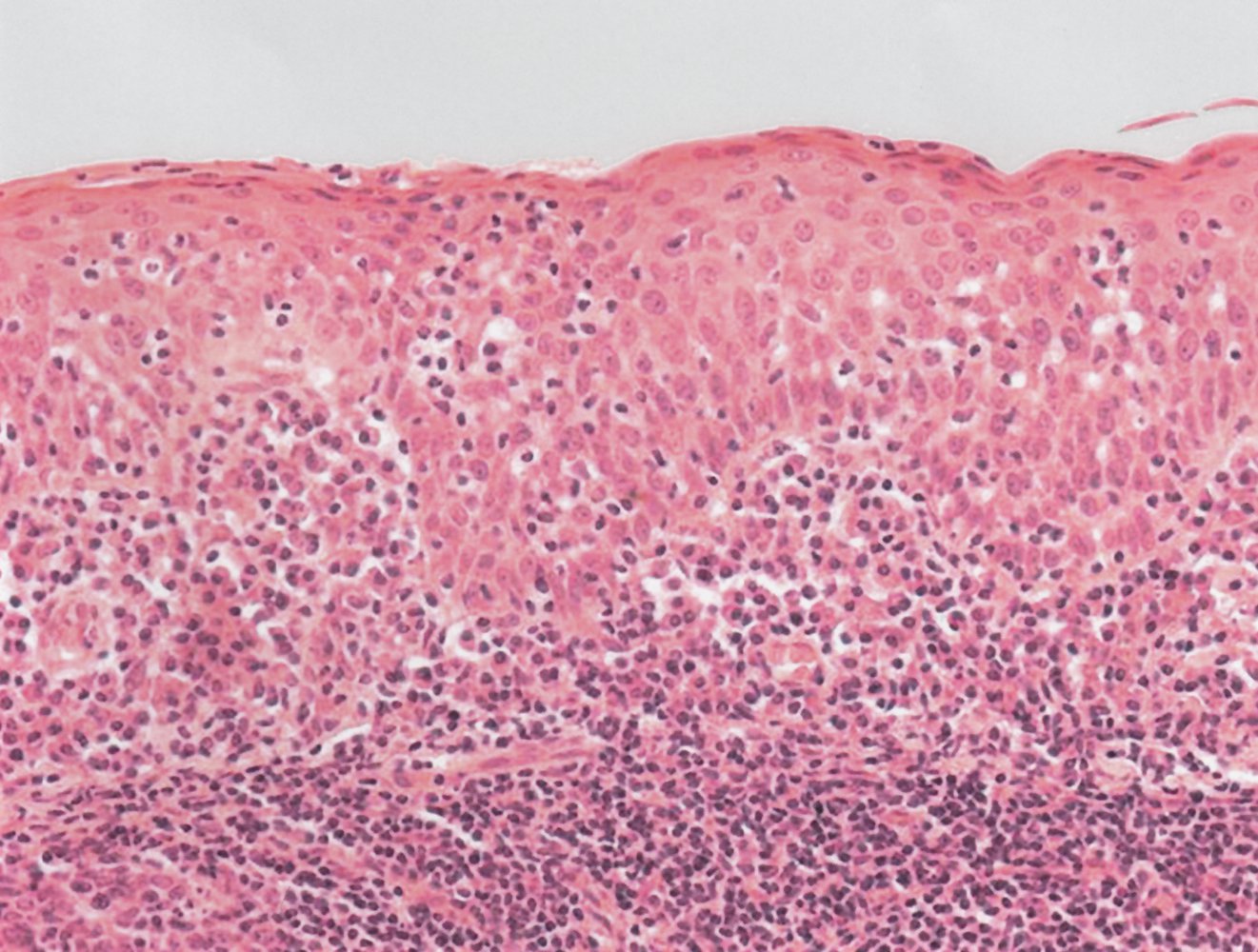
Photomicrograph of a palatine tonsil tissue sample (H&E stain; 400x magnification)
The characteristic stratified nonkeratinized squamous epithelium lining the palatine tonsil can be seen at the top. There are single lymphocytes infiltrating the epithelium between the keratinocytes (examples indicated by arrows; white arrowheads indicate examples of keratinocyte nuclei), features that are physiological in the tonsils and other lymphoepithelial tissues. Mucosa-associated lymphatic tissue can be seen in the underlying tissue in the lower part of the image.
Source: © IMPP
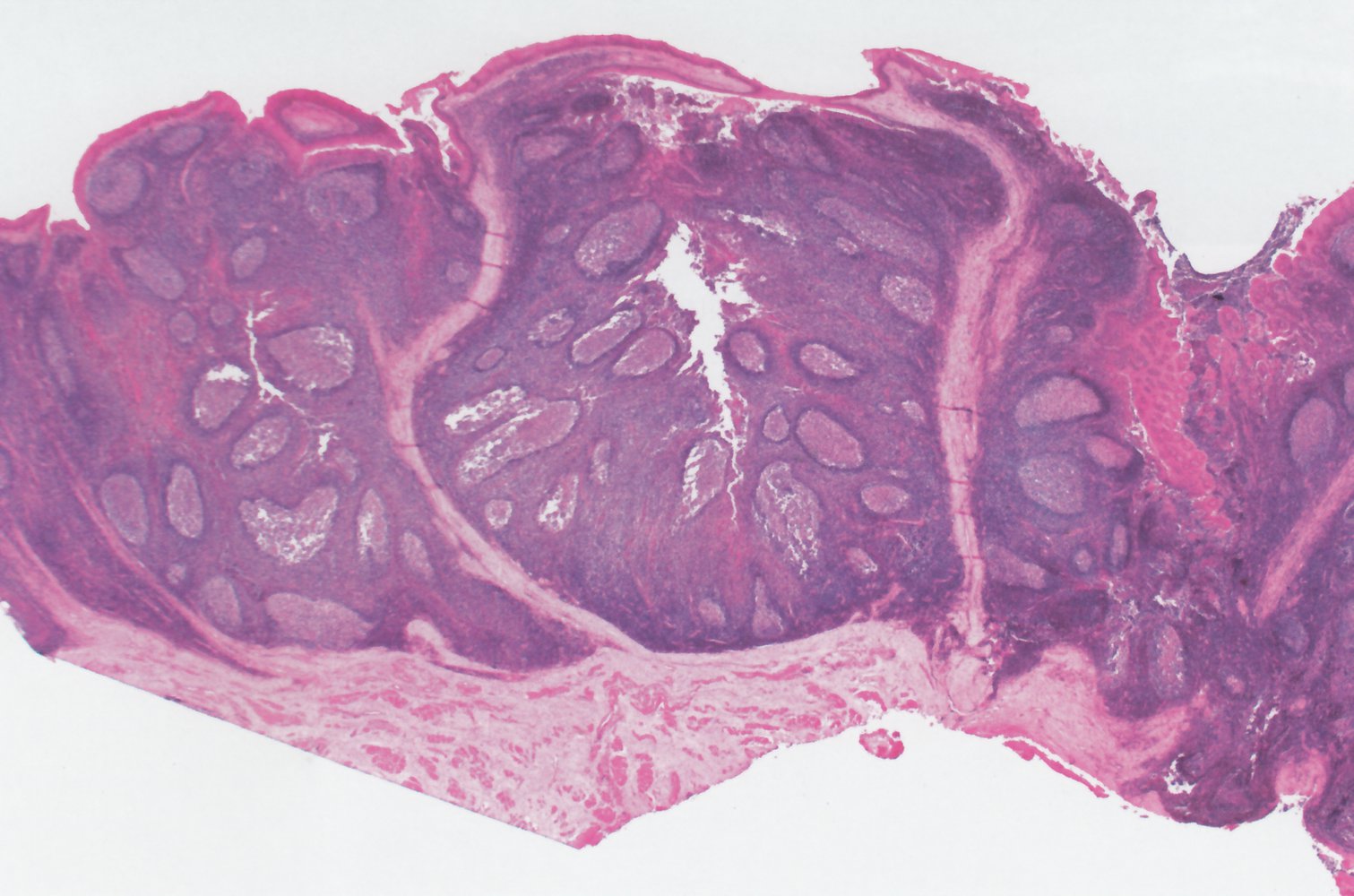
Photomicrograph of a palatine tonsil tissue sample (H&E-stain, 40x magnification)
The palatine tonsil is covered by stratified squamous, nonkeratinizing epithelium (example region highlighted by green overlay) and contains numerous lymph follicles (examples indicated by hatched green overlay). Detritus collecting in the tonsillar crypts (example indicated by red arrow) can cause tonsillitis.
Source: © IMPP

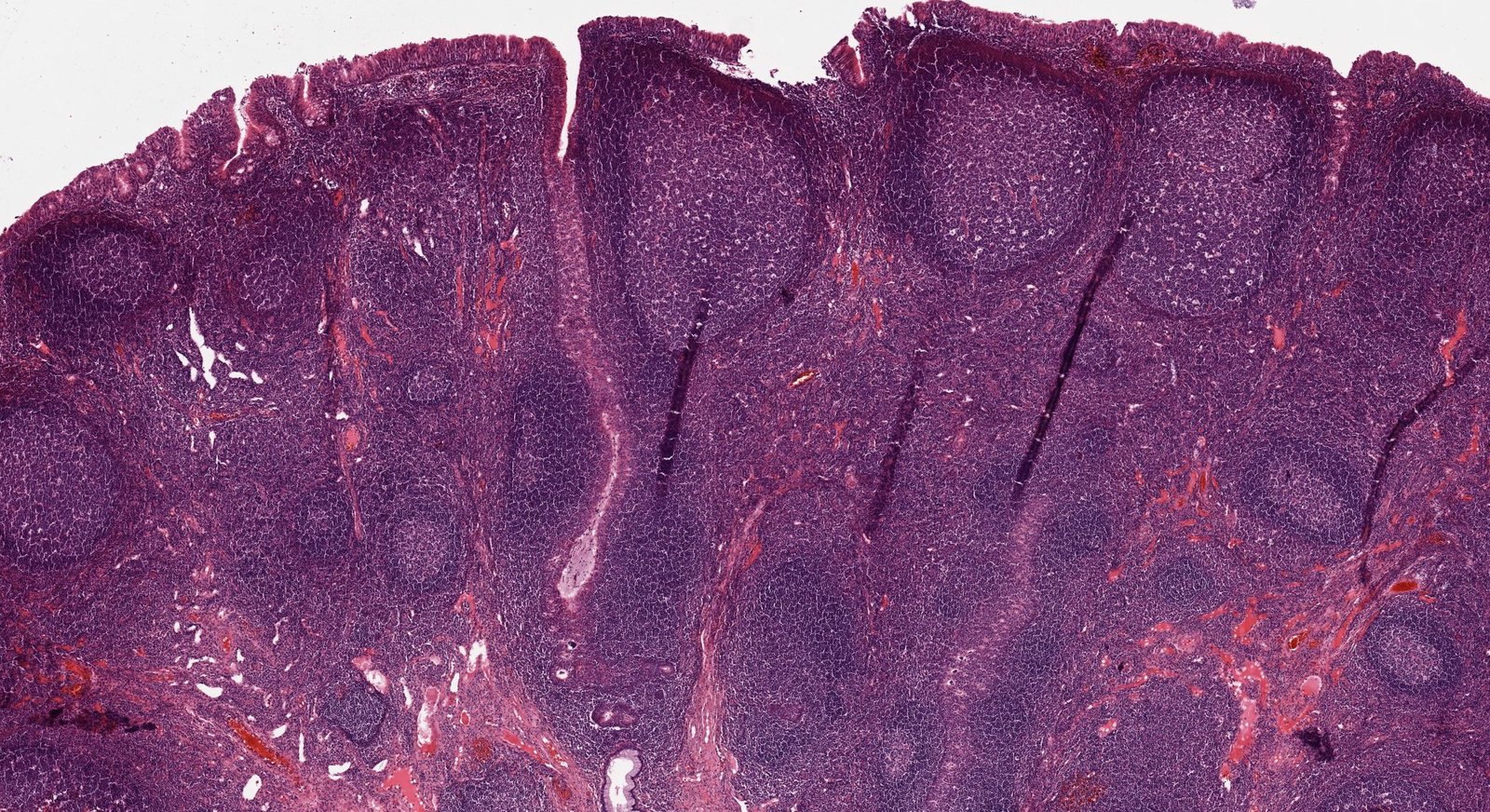
Microscopic image of palatine tonsillar tissue (H&E stain, 25x magnification)
The palatine tonsil is lined with nonkeratinized stratified squamous epithelium and is characterized by the round lymphoid follicles (light purple lined with dark purple) and deep branched tonsillar crypts (white, top center of image).
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
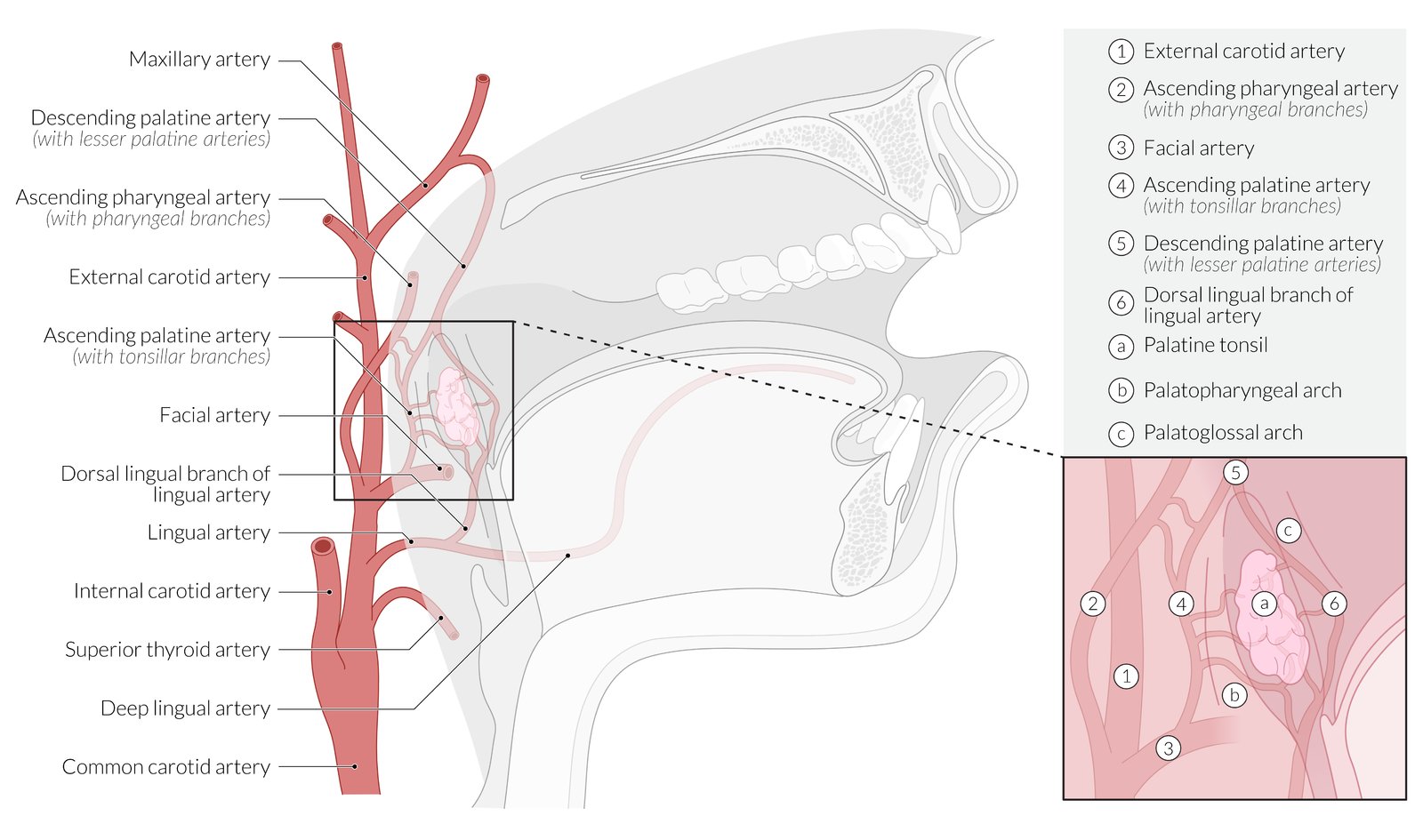
Sagittal section of the mouth, larynx, and pharynx
The palatine tonsils are supplied by branches of the lingual artery, ascending palatine artery, ascending pharyngeal artery, and descending palatine artery, all of which arise from the external carotid artery.
© AMBOSS
Lymphatic drainage
Overview
-
Lymph
- Drained by the lymph capillaries from body tissues, then circulates through lymphatic vessels and secondary lymphatic organs
- Lymph reenters blood circulation via the thoracic duct and right lymphatic duct.
-
Chyle (lymph and triglycerides) is taken up from the intestine during digestion and conveyed by the thoracic duct to empty into the venous system.
-
Thoracic duct
- Drains lymph fluid from all body sections except for the right arm, the right side of the thorax, and the right head and neck region (including the left side of the thorax and upper limb)
- Cisterna chyli; : a dilated lymphatic sac that lies near the left crus of the diaphragm, from which the thoracic duct arises [5]
- The thoracic duct continues from the cisterna chyli, ascends the posterior mediastinum (thoracic aorta to its left), and empties into the left venous arch (junction of the left subclavian vein and left internal jugular vein).
- Drains up to 4 liters of lymph per day
- Injury to the thoracic duct may result in chylothorax.
-
Right lymphatic duct
- Drains lymph fluid from the right arm, the right side of the thorax, and the right head and neck region.
- Originates from the junction of the right subclavian trunk, the right bronchomediastinal trunk, and the right jugular trunk
- Empties into the right venous arch (junction of the right subclavian vein and right internal jugular vein)
-
Thoracic duct
Lymph node clusters
Palpable lymph nodes

Head and neck
| Lymph nodes of the head and neck | |||
|---|---|---|---|
| Cluster | Location | Drainage area | Differential diagnoses |
| Parotid lymph nodes |
|
|
|
| Preauricular lymph nodes |
|
|
|
| Retroauricular lymph nodes |
|
|
|
| Submandibular lymph nodes |
|
|
|
| Submental lymph nodes |
|
|
|
| Occipital lymph nodes |
|
|
|
| Deep cervical lymph nodes |
|
|
|
| Posterior triangle lymph nodes |
|
|
|
| Supraclavicular lymph nodes |
|
|
|




Upper extremity
| Lymph nodes of the upper extremity | ||||
|---|---|---|---|---|
| Cluster | Location | Drainage area | Differential diagnoses | |
| Axillary lymph nodes | Central lymph nodes |
|
|
|
| Anterior (pectoral) lymph nodes |
|
|
||
| Posterior (subscapular) lymph nodes |
|
|
|
|
| Lateral (brachial) lymph nodes |
|
|
|
|
| Apical (subclavicular) lymph nodes |
|
|
|
|
| Supratrochlear/epitrochlear lymph nodes |
|
|
|
|



Abdomen and lower extremity
| Lymph nodes of the lower extremity | ||||
|---|---|---|---|---|
| Cluster | Location | Drainage area | Differential diagnoses | |
| Periumbilical [6] |
|
|
|
|
| Inguinal lymph nodes | Superficial inguinal lymph nodes |
|
|
|
| Deep inguinal lymph nodes |
|
|
|
|
| Popliteal lymph nodes |
|
|
|
|
The testicles, epididymis, and seminal ducts are drained by the deep, iliac, and lumbar lymph nodes.
Nonpalpable lymph nodes [7][8]

Thoracic
| Thoracic lymph nodes | ||||
|---|---|---|---|---|
| Cluster | Location | Drainage area | Drain into | Differential diagnoses |
| Mediastinal lymph nodes (paratracheal) |
|
|
|
|
| Hilar lymph nodes |
|
|
|
|


Abdominal
| Abdominal lymph nodes | |||||
|---|---|---|---|---|---|
| Cluster | Location | Drainage area | Drain into | Differential diagnoses | |
| Pre-aortic lymph nodes | Celiac lymph nodes |
|
|
|
|
| Superior mesenteric lymph nodes |
|
|
|||
| Inferior mesenteric lymph nodes |
|
|
|||
| Paraaortic lymph nodes (lumbar) |
|
|
|
|
|
Pelvic
| Pelvic lymph nodes | ||||
|---|---|---|---|---|
| Cluster | Location | Drainage area | Drain into | Differential diagnoses |
| Internal iliac lymph nodes |
|
|
|
|
| External iliac lymph nodes |
|
|
|
|
| Common iliac lymph nodes |
|
|
|
|

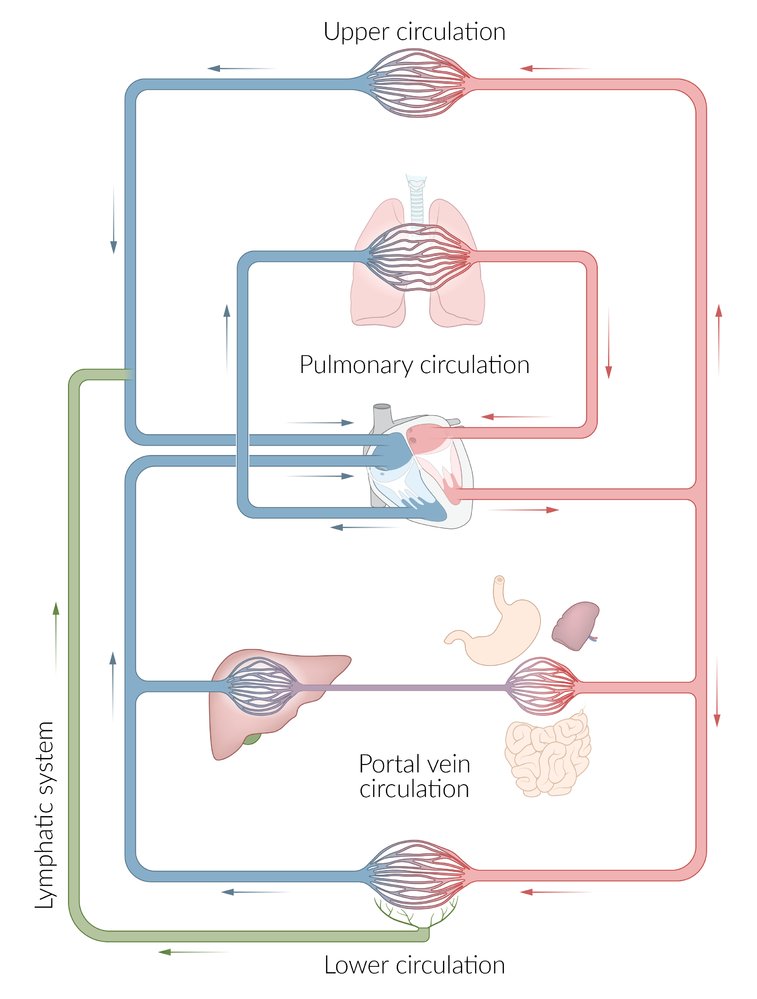
The systemic circulation carries blood from the left ventricle via the upper and lower circulation to the capillaries of the organs, and back to the right atrium of the heart. From there, the pulmonary circulation carries blood to the lungs and back to the left atrium of the heart.
The lymphatic system, shown in green, starts with blind-ended tubes in tissues that collect interstitial fluid. It drains into the upper circulation of the systemic circulation near the junction of internal jugular vein and subclavian vein.
Portal circulation is particular to the systemic circulation and is present in the liver and pituitary gland; there, the blood passes through the consecutive capillary beds of two different structures before returning to the heart.
© AMBOSS
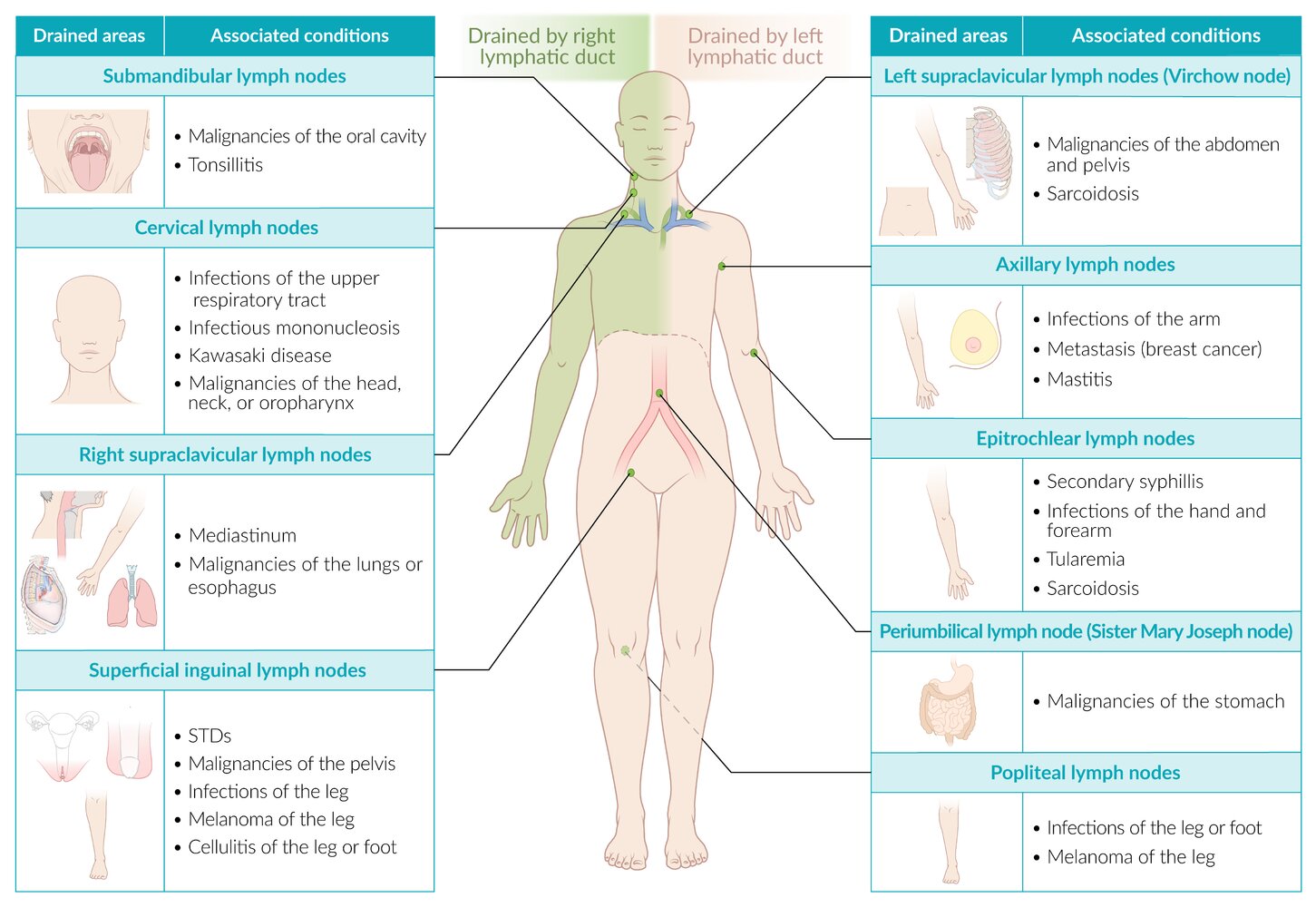
Lymph is drained into the systemic circulation via the subclavian veins. The right lymphatic duct primarily drains the upper right side of the body (green overlay). The thoracic duct is responsible for draining the rest of the body.
Testicular tumors do not typically disseminate to scrotal lymph nodes, because the two organs have separate lymphatic systems: testes drain to the para-aortic nodes and the scrotum drains to superficial inguinal nodes.
© AMBOSS
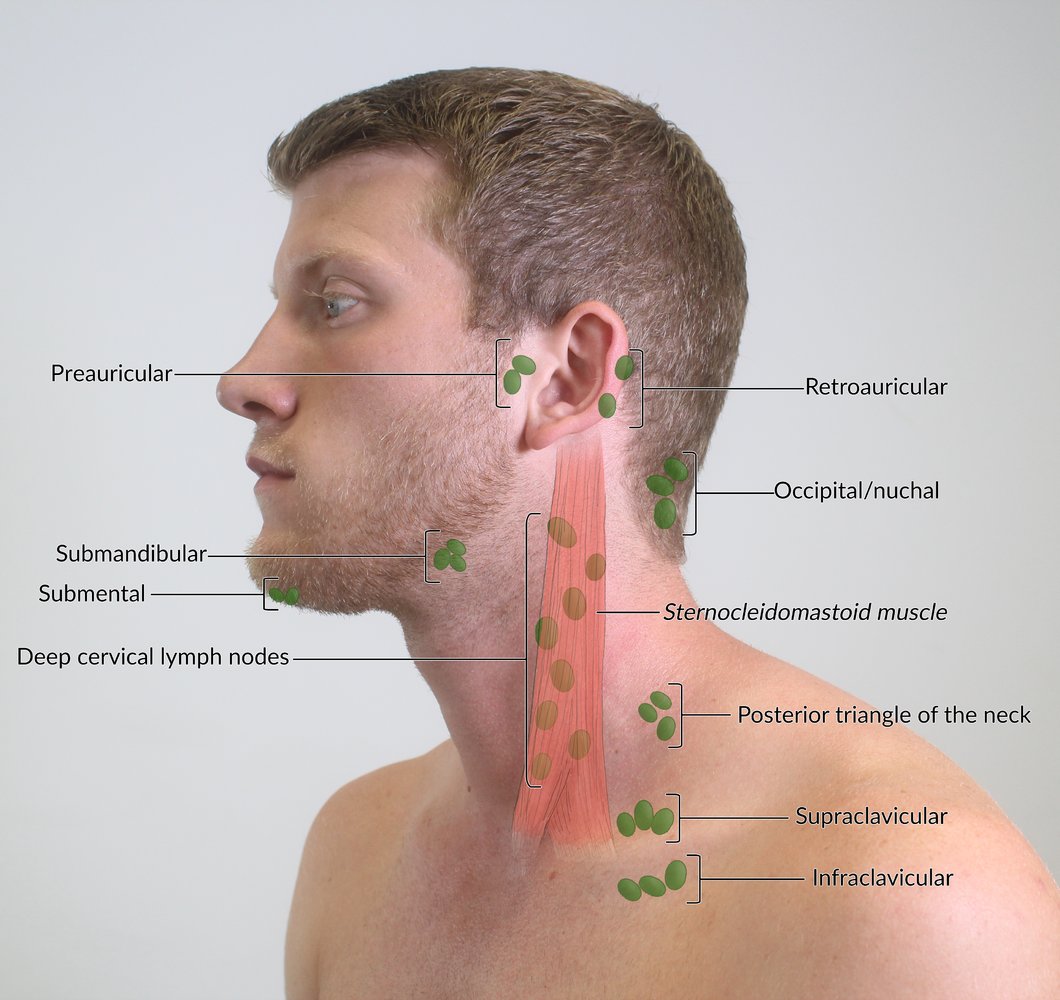
Palpable superficial and deep lymph nodes.
© AMBOSS
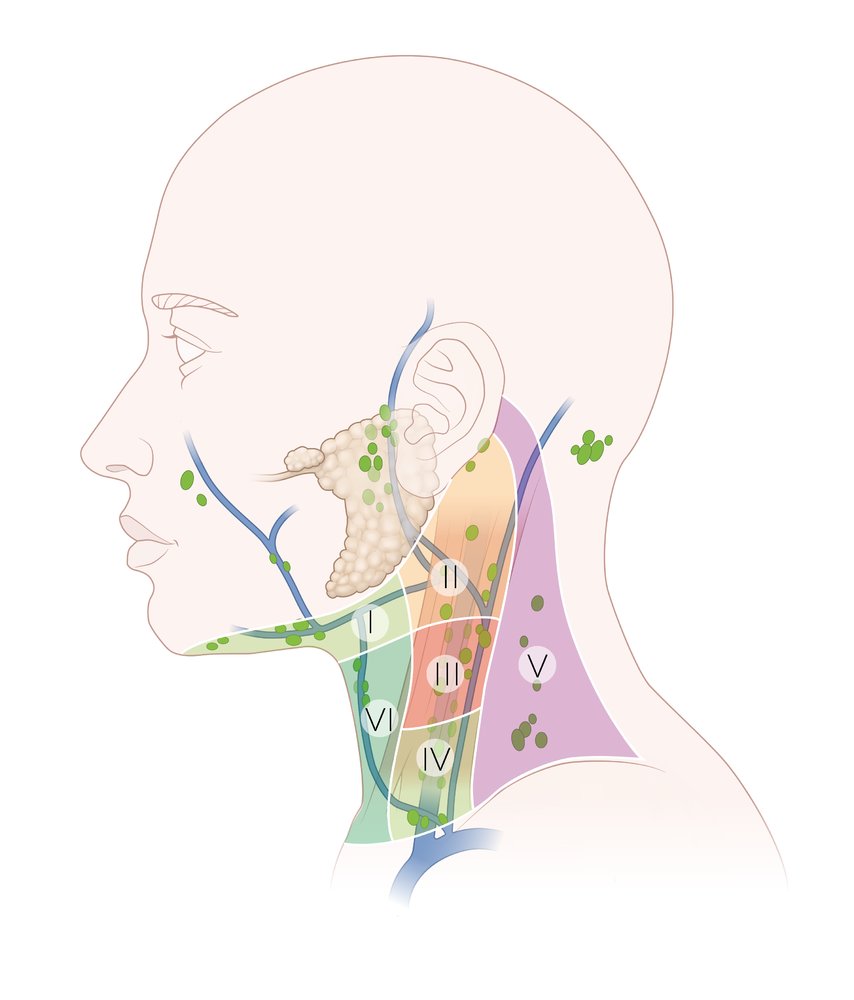
– Level I (submental and submandibular lymph nodes): extends from the inferior border of the mandible to the upper border of the hyoid
– Level II (upper jugular lymph nodes): extends from the base of the skull to the hyoid
– Level III (middle jugular lymph nodes): extends from the hyoid to the cricoid
– Level IV (lower jugular lymph nodes): extends from the cricoid to the clavicle
– Level V (posterior triangle): posterior to the posterior edge of the sternocleidomastoid muscle and anterior to the anterior border of the trapezius muscle
– Level VI (prelaryngeal, pretracheal, and paratracheal lymph nodes): extends from the suprasternal notch to the innominate artery
© AMBOSS

Bilaterally enlarged cervical lymph nodes (black arrows) and submandibular lymph nodes are seen in the neck region of a patient with infectious mononucleosis.
Additionally, there is a pale, macular rash on the neck and upper chest. A rash seen in infectious mononucleosis may be caused by the infection itself but is more commonly due to antibiotic use.
Source: “Lymphadenopathy” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

There is significant symmetrical neck swelling due to swelling of the salivary glands and lymph nodes.
Source: "ID#: 3168", CDC/ Heinz F. Eichenwald, MD, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
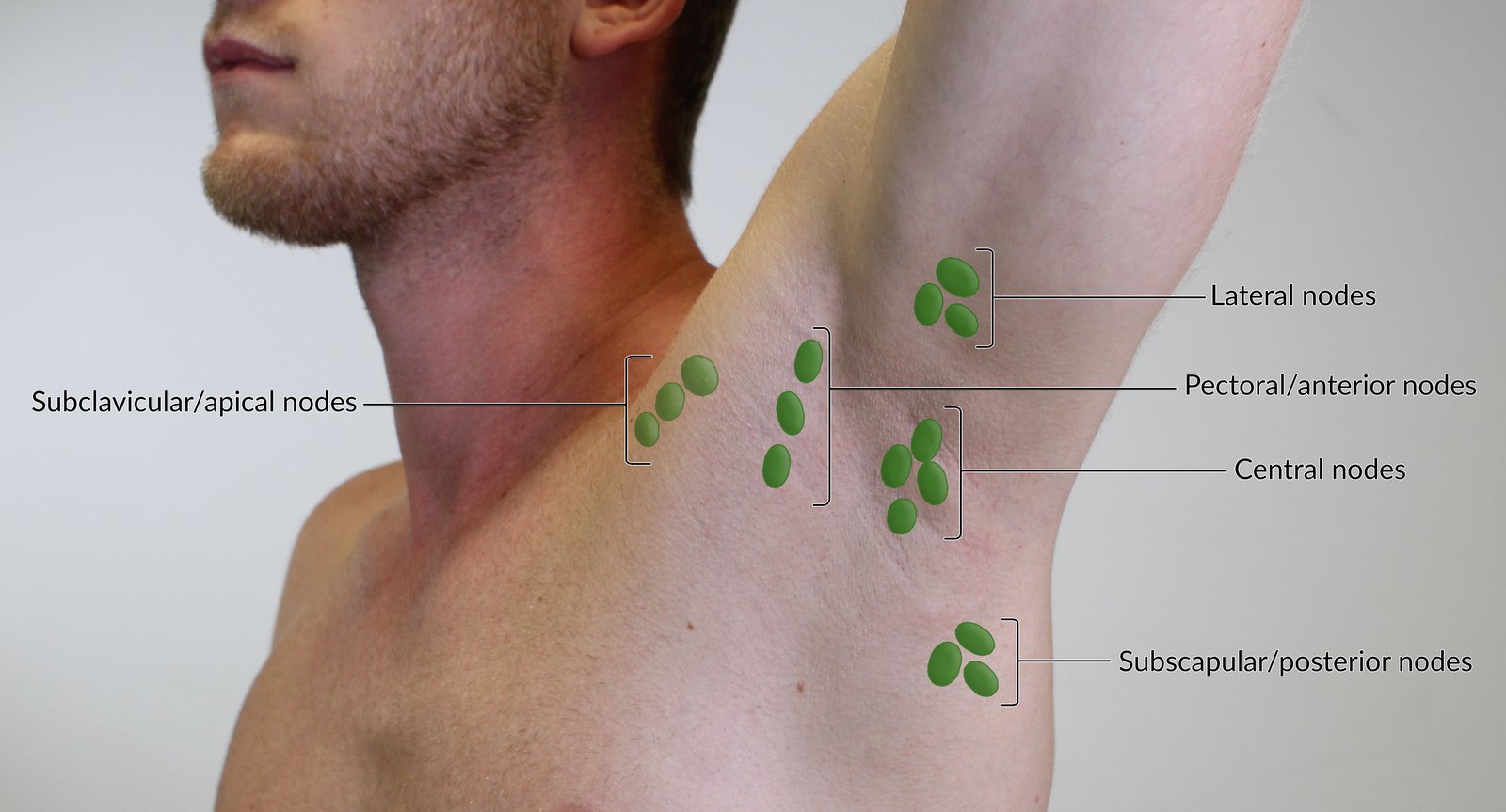
The lateral nodes drain most of the arm and shoulder and are palpable near the proximal humerus. The pectoral or anterior nodes drain the thoracic wall and parts of the thorax and are palpable in the anterior axillary line. The subscapular or posterior nodes drain the posterior thoracic wall and parts of the arm and are palpable in the posterior axillary line.
All these lymph nodes drain into the central nodes, which are palpable at the base of the axilla. Before entering the venous system, lymph from the central nodes passes through the subclavicular or apical nodes before entering the venous system. Therefore, these nodes should also be palpated in the examination.
For educational purposes, the lymph nodes are depicted enlarged.
© AMBOSS
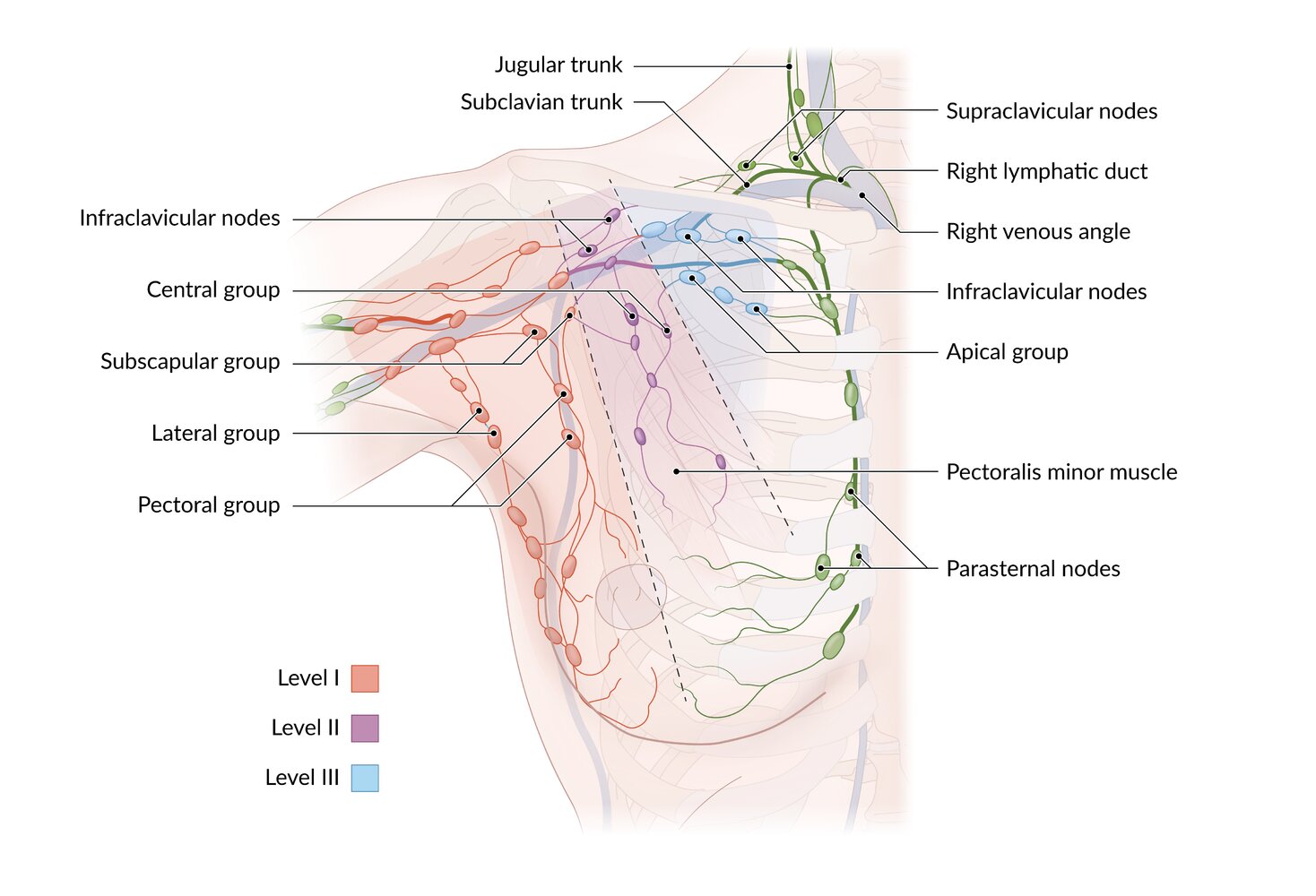
Lymphatics of the breast drain into three groups:
1. Axillary group, further divided into three levels
– Level I: lateral to the lateral border of the pectoralis minor
– Level II: behind the pectoralis minor
– Level III: medial to the medial border of the pectoralis minor
2. Parasternal (internal thoracic) group
3. Posterior intercostal group (not shown here)
Efferent lymphatics travel to the supraclavicular nodes and terminate in the thoracic duct (on the left; not shown here) or the right lymphatic duct.
© AMBOSS

Right axilla of a male patient diagnosed with plague
The axilla appears swollen secondary to underlying lymph node enlargement due to infection with Yersinia pestis.
This disease is rare but if diagnosed requires immediate antibiotic treatment.
Source: "ID #2045", CDC, Centers for Disease Control and Prevention, Atlanta, USA licensed under Public Domain
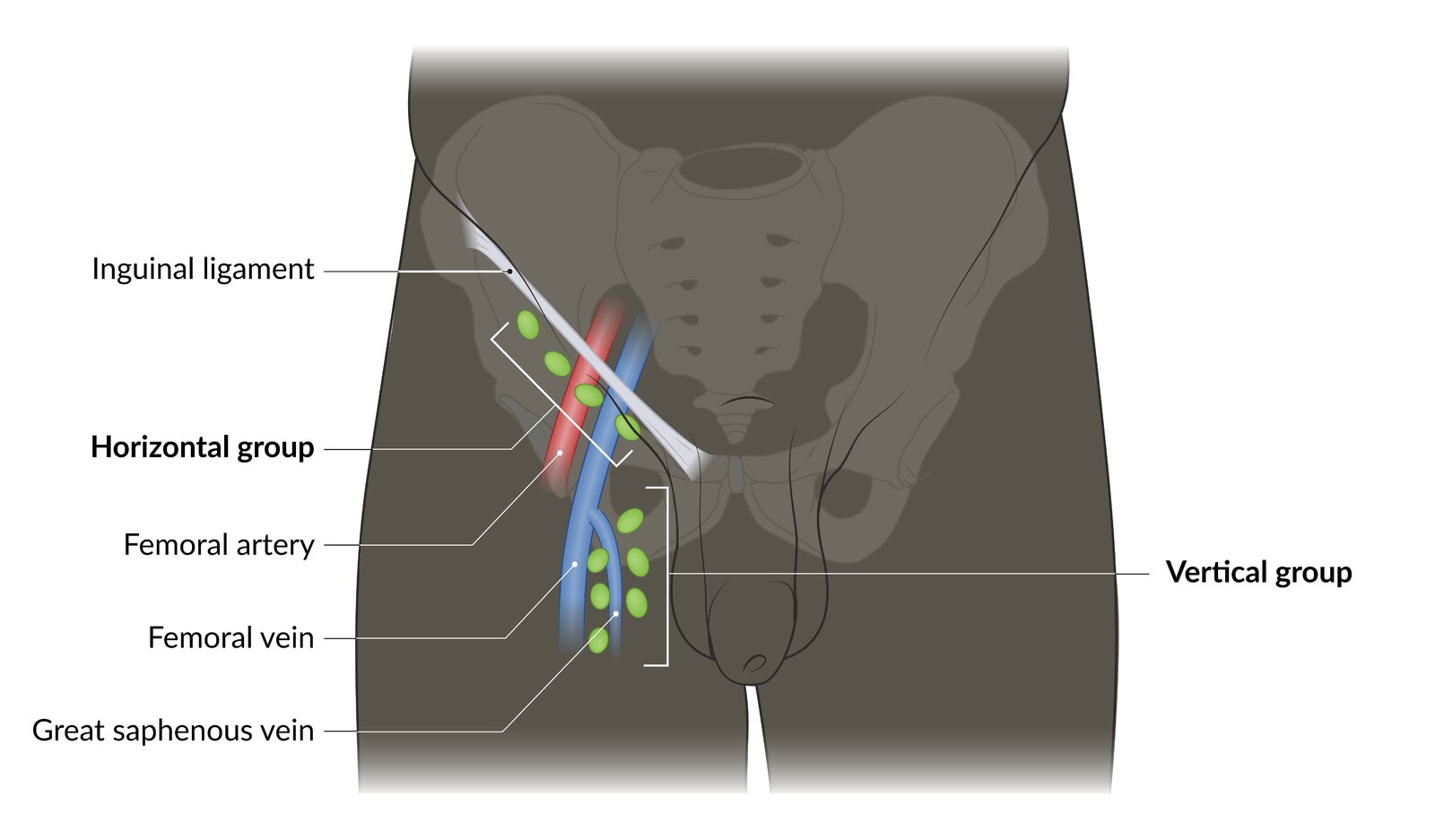
The superficial inguinal lymph nodes are divided into a horizontal group, which can be palpated directly underneath the inguinal ligament, and a vertical group, which can be palpated in the region where the great saphenous vein drains into the femoral vein.
© AMBOSS
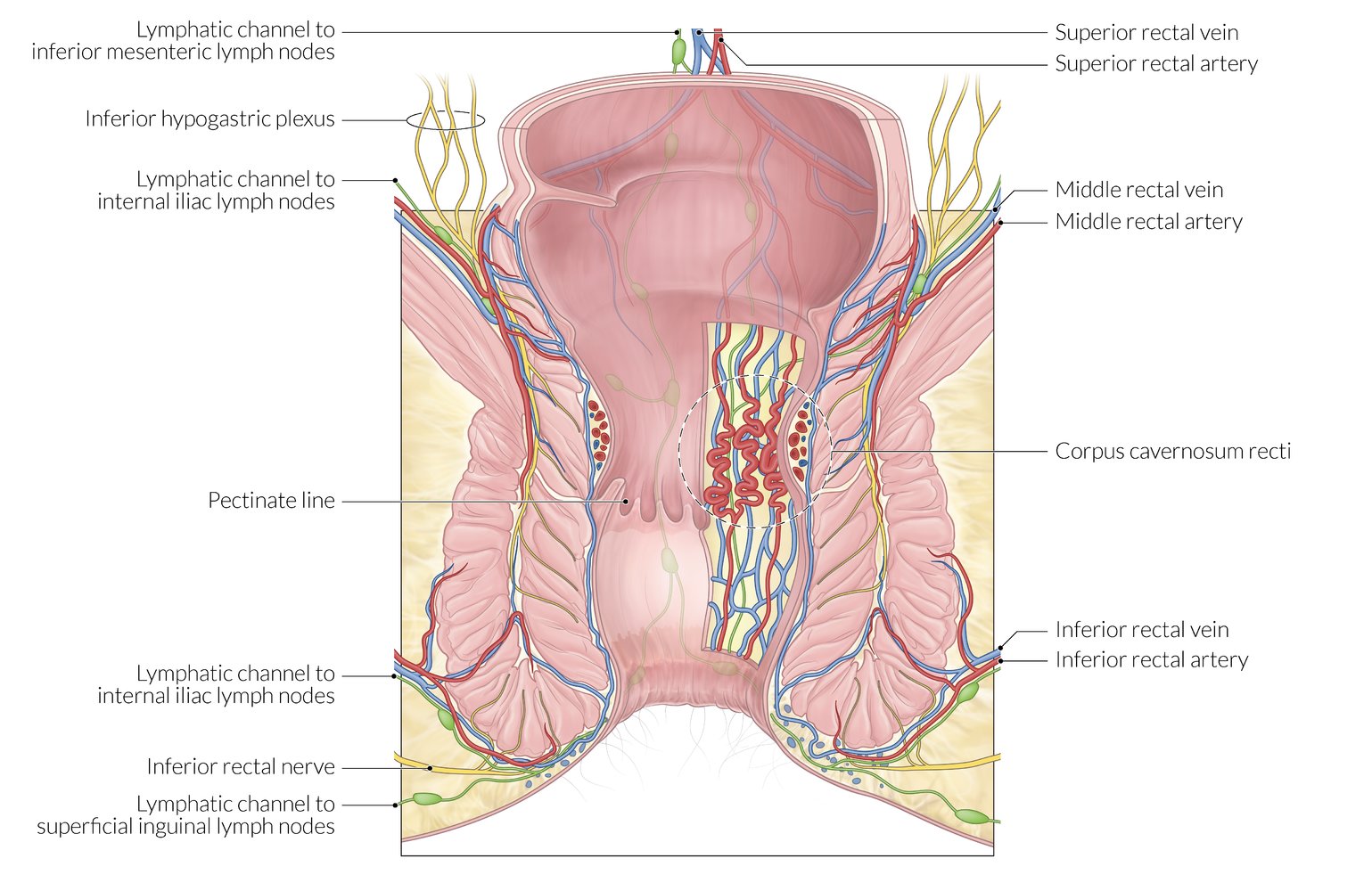
Illustration depicting the dual lymphovascular supply of the anal canal
The anal valves form the pectinate line (seen as a longitudinal scalloped line), which divides the anal canal into upper and lower parts.
Arterial supply
Above the pectinate line:
- Superior rectal artery (a branch of the inferior mesenteric artery)
- Middle rectal artery (a branch of the internal iliac artery)
Below the pectinate line: inferior rectal artery (a branch of the internal pudendal artery)
Venous drainage (site of porto-systemic anastomosis)
Above the pectinate line:
- Superior rectal vein (drains into the inferior mesenteric vein, which drains into the portal vein)
- Middle rectal vein (drains into the internal iliac vein, a systemic vein)
Below the pectinate line: inferior rectal vein (drains into the internal pudendal vein, a systemic vein)
Lymphatic drainage
Above the pectinate line: into the internal iliac and inferior mesenteric lymph nodes
Below the pectinate line: into the superficial inguinal lymph nodes
© AMBOSS

Photograph of the right upper leg of a patient diagnosed with plague
Enlarged lymph nodes secondary to an infection with Yersinia pestis, the causative bacterium for plague, are visible.
Source: "ID #2047", CDC, Centers for Disease Control and Prevention, Atlanta, USA licensed under Public Domain
Lymph is ultimately drained into the systemic circulation via the subclavian veins. The right lymphatic duct only drains roughly the upper right area of the body (green), whereas the thoracic duct is responsible for the rest of the body. The deep lymph nodes are not palpable.
© AMBOSS
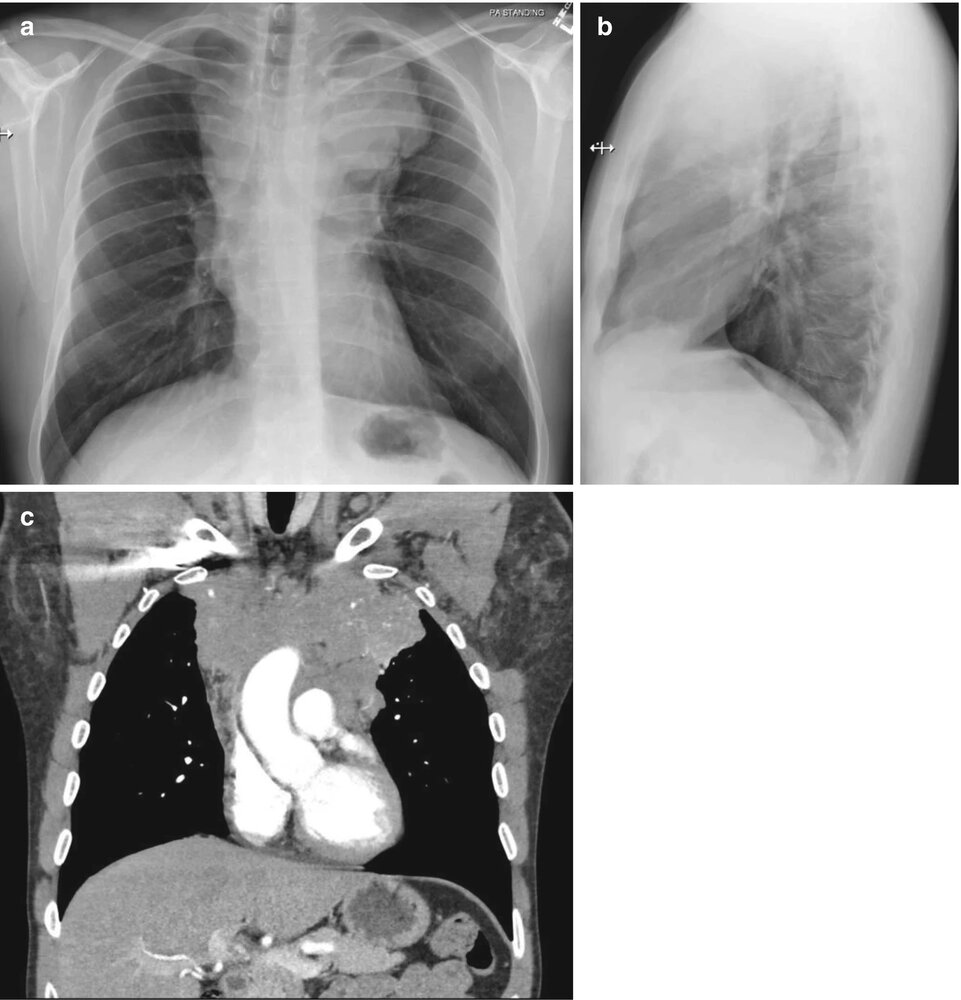
X-ray chest (a: PA view; b: left lateral view) and CT chest (c: with contrast; coronal plane) of a patient with nodular sclerosing Hodgkin lymphoma
The PA radiograph shows an abnormal superior mediastinum that is dense, markedly widened, and lobulated (green overlay). On the lateral radiograph, there is opacification of the retrosternal space, which should normally be a clear area. CT confirms the presence of a large anterior locally invasive mediastinal soft tissue mass (arrows).
Li: liver; LV: left ventricle
Source: “Fig. 1.3, in: A Systematic Approach to Chest Radiographic Analysis” by Jeffrey S. Klein, Melissa L. Rosado-de-Christenson, Springer Link, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
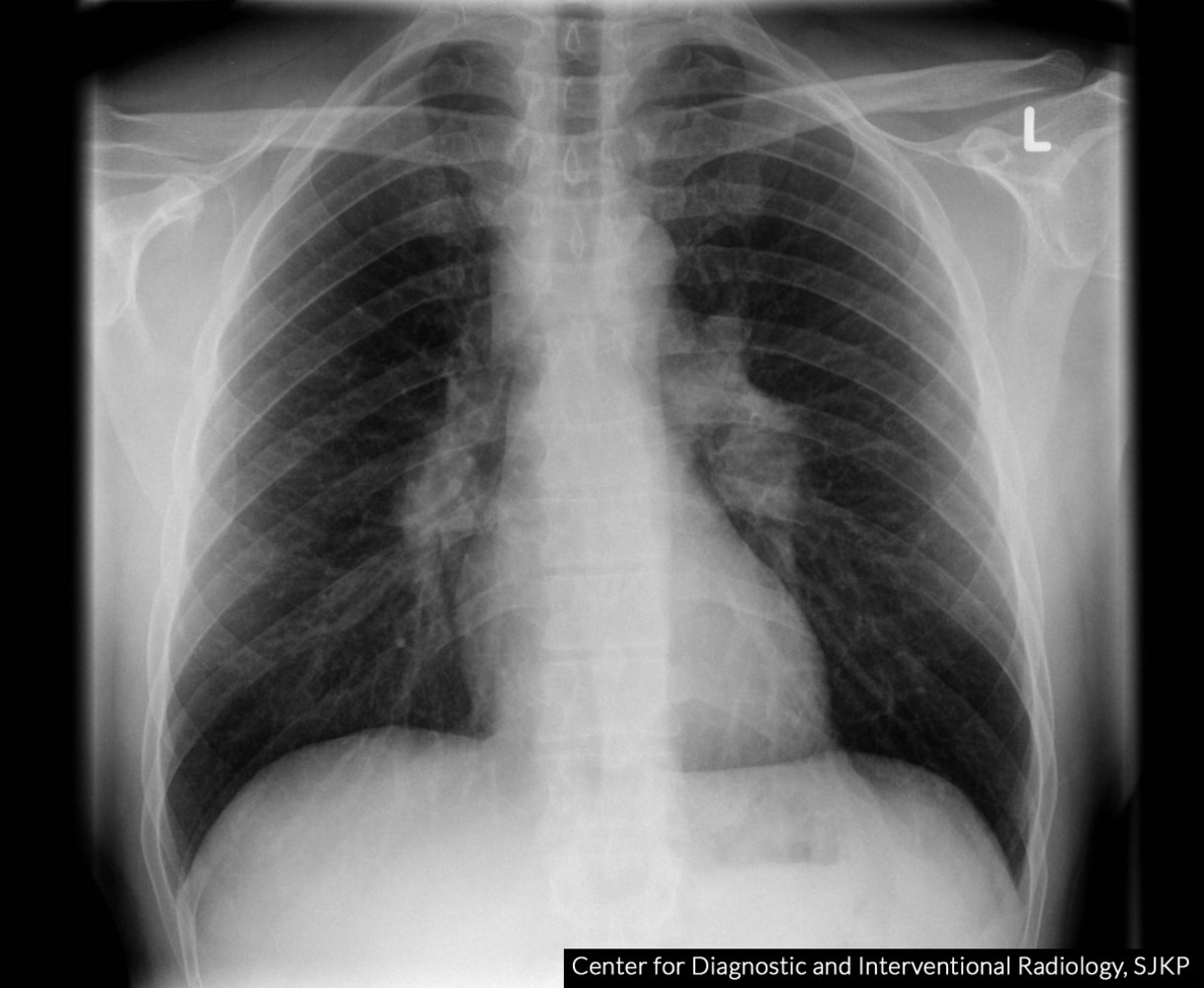
Chest x-ray (PA view) of a patient with sarcoidosis
The pulmonary hila (green overlay) are enlarged and lobulated. Additionally, the right superior mediastinum (red overlay) is widened and dense. A normal thin right paratracheal stripe is not seen.
Relatively symmetric bilateral hilar and right paratracheal lymph node enlargement on a chest radiograph in sarcoidosis is termed the “1-2-3 sign” or “Garland triad.” Examples of other causes of hilar and mediastinal lymphadenopathy include lymphoma, metastatic disease, granulomatous infections, and inorganic dust disease.
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.
References
- Shanley DP, Aw D, Manley NR, Palmer DB. "An evolutionary perspective on the mechanisms of immunosenescence". Trends Immunol. 30(7). :374-381. (2009)
- Randall TD, Mebius RE. "The development and function of mucosal lymphoid tissues: a balancing act with micro-organisms". Mucosal Immunology. 7(3). :455-466. (2014)
- Silva-Sanchez A, Randall TD. "Anatomical Uniqueness of the Mucosal Immune System (GALT, NALT, iBALT) for the Induction and Regulation of Mucosal Immunity and Tolerance". Elsevier. :21-54. (2020). ISBN: 9780128119242
- Hwang JY, Silva-Sanchez A, Carragher DM, et al. "Inducible Bronchus–Associated Lymphoid Tissue (iBALT) Attenuates Pulmonary Pathology in a Mouse Model of Allergic Airway Disease". Frontiers in Immunology. 11. (2020)
- Taneja SS. "Complications of Urologic Surgery". Saunders. (2010). ISBN: 9781416045724
- Gibbs TS. "Sister Mary Joseph Nodule". Journal of Diagnostic Medical Sonography. 28(3). :107-117. (2012)
- Ferrer R. "Lymphadenopathy: differential diagnosis and evaluation.". Am Fam Physician. 58(6). :1313-20. (1998)
- Lucey BC, Stuhlfaut JW, Soto JA. "Mesenteric lymph nodes seen at imaging: causes and significance". Radiographics. 25(2). :351-365. (2005)
- Murphy K, Weaver C. "Janeway's Immunobiology". Garland Science. (2016). ISBN: 9780815345503