Summary
Major depressive disorder (MDD) is an episodic mood disorder primarily characterized by depressed mood and anhedonia lasting for at least two weeks. Women have a higher risk of developing MDD than men. The peak age of onset is the third decade. The etiology is multifactorial, including both biological and psychological factors. Reduced levels of neurotransmitters (serotonin, noradrenaline, dopamine) are believed to be the pathophysiological basis in most cases. Other symptoms of MDD include sleep disturbance, loss of appetite, and thoughts of suicide. Subtypes of MDD are characterized by additional symptoms. MDD with atypical features is additionally characterized by weight gain and increased appetite, while MDD with psychotic features is characterized by hallucinations and delusions. Presentations may also vary in special patient groups, e.g., pregnant patients, older patients, children and adolescents, and patients receiving palliative care. Treatment of all forms of MDD is multifaceted and often requires psychotherapy, pharmacotherapy (most commonly SSRIs), and lifestyle changes.
Epidemiology
- Sex: ♀ > ♂
- Lifetime prevalence: 10–20% [1]
- Age of onset: 3rd decade of life
References: [2]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Biological factors
- Monoamine hypothesis: Most antidepressants work by inhibiting the reuptake of monoamines (e.g., serotonin, noradrenaline, dopamine), indicating that a lack of monoamines plays a major role in the pathophysiology of depression (and other mood disorders).
- Genetic factors
- First-degree relatives of patients with depression are at increased risk of developing depression.
- The concordance rate in identical twins is ∼ 50%.
- Increased production of stress hormones (e.g., dysfunction of the hypothalamic-pituitary-adrenal axis)
- Psychological factors: traumatic and stressful experiences, behavioral factors (e.g., learned helplessness)
- Comorbidities: neurodegenerative diseases (e.g., Alzheimer disease), chronic inflammatory diseases (e.g., systemic lupus erythematosus or inflammatory bowel disease), and other psychiatric disorders (e.g., panic disorder)

References:[3][4]
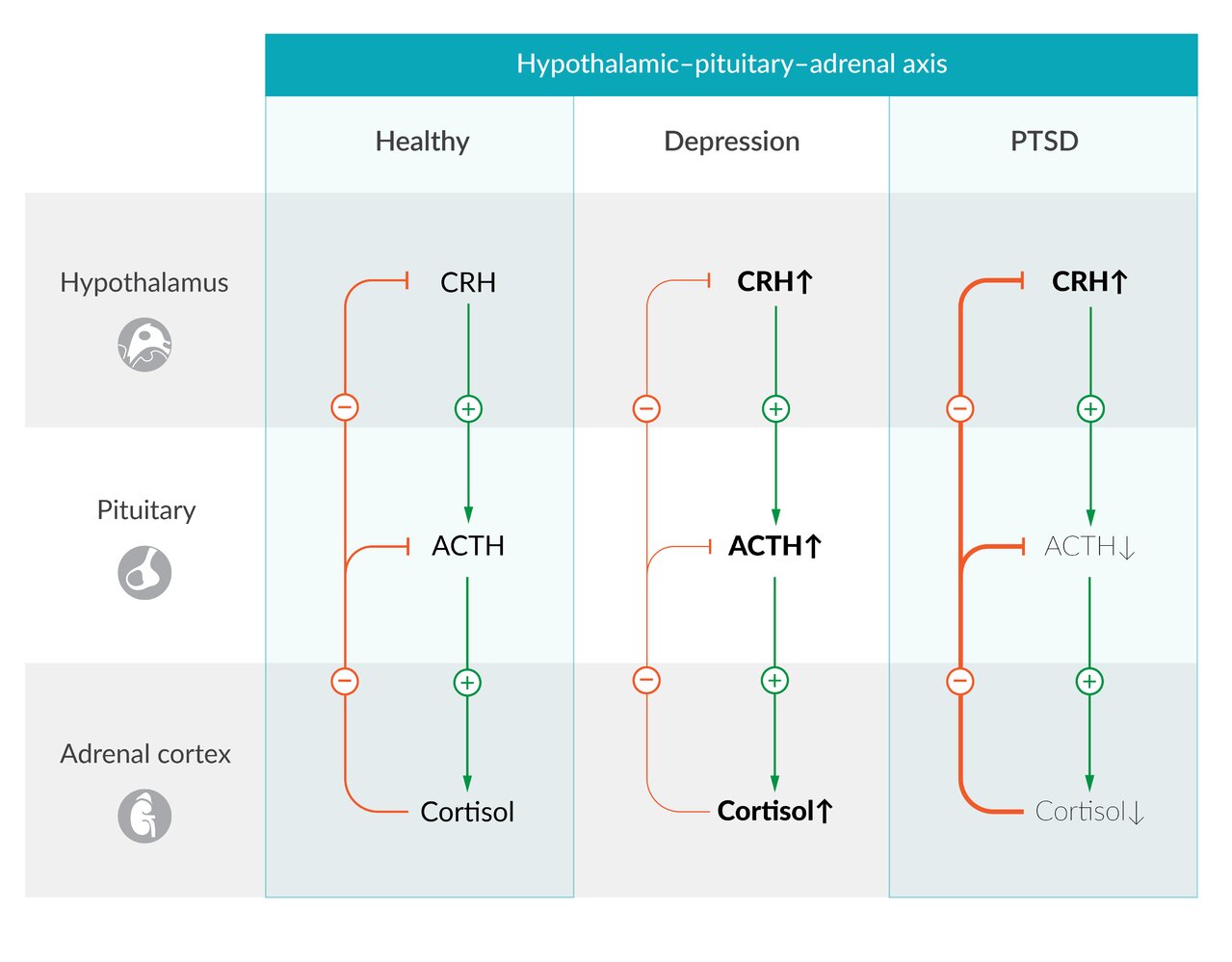
Hypothalamic-pituitary-adrenal (HPA) axis in the physiological state, in major depression, and in post-traumatic stress disorder (PTSD).
Left: Physiologically, further cortisol release is reduced via a negative feedback mechanism.
Center: In patients with major depression, the HPA axis is typically hyperactive, with increased cortisol levels at reduced feedback sensitivity. A potential underlying mechanism is a decreased function or number of glucocorticoid receptors.
Right: In patients with PTSD, cortisol levels are reduced, despite constantly elevated CRH levels. Persistently increased CRH stimulation in the pituitary gland leads to a downregulation of CRH receptors and thus to reduced ACTH production and cortisol release. Also, increased feedback sensitivity further leads to decreased ACTH production. In contrast to depression, the function or number of glucocorticoid receptors is increased.
© AMBOSS
Clinical features
- Depressed mood
- Anhedonia
- Feelings of guilt, worthlessness, or hopelessness
- Low energy levels
- Difficulty concentrating
- Changes in appetite and weight (increased or decreased)
- Sleep disorders (insomnia or hypersomnia)
- Psychomotor agitation or retardation
- Suicidal thoughts
-
May additionally manifest with:
- Somatic features, e.g., headaches, myalgia, gastrointestinal problems
- Aggression, substance use disorder, or increase in risk-taking behavior
Older adults with depression may be more likely than younger adults to present with physical symptoms than a low mood. [6]
Depression screening with “SIGECAPS”: Sleep (insomnia or hypersomnia), Interest loss (anhedonia), Guilt (low self-esteem), Energy (low energy or fatigue), Concentration (poor concentration or difficulty making decisions), Appetite (decreased appetite or overeating), Psychomotor agitation or retardation, and Suicidality.

© AMBOSS
Subtypes and variants
Major depressive disorder with seasonal pattern (seasonal affective disorder, winter depression)
- Definition: a subtype of major depressive disorder characterized by ≥ 2 depressive episodes associated with a seasonal pattern (e.g., the winter season) over ≥ 2 years
- Epidemiology: occurs in a yearly, season-specific pattern (commonly in fall or winter)
-
Clinical features
- Patients present with typical symptoms of MDD alongside atypical ones, such as weight gain and requiring more sleep.
- See “Major depressive episode” for details.
- Diagnostic criteria: Symptoms must be present for ≥ 2 consecutive years and for the majority of years in a lifetime.
- Treatment: Bright light therapy has been shown to improve symptoms.
Major depressive disorder with atypical features
- Epidemiology: most common variant of MDD
-
Clinical features
- Increased appetite or over-eating
- Hypersomnia
- Leaden paralysis (legs and arms feel heavy)
- Interpersonal rejection sensitivity that leads to social and occupational impairment
- Mood reactivity: brightening of mood in response to positive events, which is usually not the case in classical MDD
- Diagnostic criteria: two or more of the clinical features are present
-
Treatment
- 1st line: CBT with or without SSRIs
- MAO inhibitors can be effective although not commonly prescribed due to their side effects.
Major depressive disorder with psychotic features
- Definition: major depression accompanied by psychotic symptoms
- Etiology: overactivity of the hypothalamic-pituitary-adrenal axis (increased dopamine activity) is believed to play a major role.
- Clinical features: See “Major depressive episode” and “Psychotic features” for details.
-
Diagnostic criteria
- Features of MDD (see diagnostic criteria for major depressive disorder)
- Psychotic features, such as delusions and hallucinations, which are usually mood-congruent (delusions and hallucinations are often about worthlessness, guilt, death, and hopelessness)
- Psychotic features occur only alongside a major depressive episode.
-
Treatment
- Antidepressants together with atypical antipsychotics
- In severe cases, electroconvulsive therapy may be used.
References:[7][8]
Diagnosis
Approach [9]
- Screen all adults using a brief screening tool, e.g., Patient Health Questionnaire-2.
- If screening is positive, perform a full clinical assessment, including:
- Confirmation of diagnosis using DSM-5 criteria for MDD
- Determination of severity: Combined tools for screening and severity assessment can be used, e.g., Patient Health Questionnaire-9.
- Assessment of suicide risk
- Diagnostic studies for common differential diagnoses
- Identification of psychiatric and medical comorbidities
Screening for depression [5][10]
Overview
- Screen all adults aged ≥ 18 years and children aged ≥ 12 years.
- Recommended screening intervals [5]
- Adults: Optimum intervals are unclear; screen at least once and consider repeating either when risk factors arise or at routine health checks.
- Children aged ≥ 12 years: Screen annually until 18–21 years of age. [11]
Brief screening tool
- Use the Patient Health Questionnaire-2 (PHQ-2).
- A 2-item survey for assessing depressed mood and loss of interest or pleasure in activities over the last 2 weeks
- A score ≥ 3 is considered positive; follow up with a full clinical assessment.
")
Further screening tools
- Scores that also assess severity:
- Patient Health Questionnaire-9 (PHQ-9) [12]
- Major depression inventory
- Beck Depression Inventory (BDI) [13]
- Consider using specific screening scores when assessing for depression in special patient groups. [10]
Diagnostic criteria
| Diagnostic criteria for major depressive disorder(consistent with DSM-5) [8][14] | |
|---|---|
| A |
Five or more of the nine symptoms listed below, for at least 2 weeks, with at least one of the symptoms being depressed mood or anhedonia
|
| B | There is clinically significant distress or impaired functioning in important areas of life (e.g., work, school). |
| C | Symptoms are not due to the effects of psychoactive substances or organic disease. |
| D | Symptoms are not superimposed upon or due to schizoaffective disorder or another psychotic disorder. |
| E | There is no history of a manic or hypomanic episode. |
| |
Severity (according to DSM-5) [8]
Treatment recommendations are often categorized by severity:
- Mild: minimal number of symptoms to fulfill diagnostic requirements PLUS manageable symptom intensity PLUS minor impaired functioning
- Moderate: number of symptoms, symptom intensity, and impaired functioning greater than “mild” but less than “severe”
- Severe: number of symptoms more than fulfill diagnostic requirements PLUS unmanageable symptom intensity PLUS extremely impaired functioning
Depressive episodes are considered recurrent when there is a gap of at least two months between episodes during which the criteria for MDD are not met.
Further assessment [5]
Suicide risk [15][16]
- Screen all patients with MDD for suicidality. [15][16]
- Screening tools include the Ask Suicide-Screening Questions suicide risk screening tool and the Columbia-Suicide Severity Rating Scale.
- A comprehensive assessment includes consideration of risk factors for suicide and protective factors.
- See also “Suicide risk evaluation.”
Exclusion of organic causes of depression [5][15]
-
Comprehensive history and physical examination
- Assess patients for features of physical diseases that mimic depression, e.g., clinical features of hypothyroidism.
- Screen for drugs associated with medication-induced depressive disorder, e.g., beta blockers, glucocorticoids, oral contraceptives.
-
Laboratory studies [5][15]
- Thyroid function tests
- CBC
- CMP
- Vitamin B12
- Folate
- Consider the following based on clinical suspicion:
- Serum and urine toxicology [17][18]
- HIV testing
- Syphilis screening
- Diagnostic studies for Lyme disease
- Testosterone levels (♂)
- Neuroimaging: Consider evaluating for structural brain disease based on clinical presentation. [19]
- Cognitive testing: to assess for memory issues and dementia [6]
-
Polysomnography (PSG): not routinely performed but obtained if a concurrent primary sleep disorder is suspected [20]
- Sleep disturbances are associated with various psychiatric conditions, but most commonly occur in mood disorders.
- Results obtained during PSG can be helpful in differentiating mood-disorder-associated sleep abnormalities from primary sleep disorders.
-
PSG findings in depression include:
-
REM sleep abnormalities
- ↓ REM latency: associated with a number of depressive symptoms, including early morning awakening and anhedonia
- ↑ REM activity and density
- Sleep continuity disturbances
- Reduced slow-wave sleep
-
REM sleep abnormalities

Consideration of alternative diagnoses [5][15]
-
Bipolar disorder
- BD should be considered in patients with treatment-resistant depression or unexpected responses to antidepressants (e.g., manic or hypomanic symptoms)
- Screening tools include:
-
Mood disorder questionnaire (MDQ): self-report instrument used to assess and monitor for symptoms of bipolar disorder and other mood disorders
- Completion takes approx. 5 minutes.
- Consists of 13 yes-or-no questions
- Items include having more energy than usual and being more talkative or speaking more quickly than usual.
- Most sensitive for bipolar I disorder [21]
- Reported sensitivity is 0.28–0.73 and specificity is 0.67–0.97. [22]
-
Hypomania checklist (HCL-32): a self-report instrument used to identify hypomanic symptoms in the diagnosis of bipolar disorder; mostly used in patients with depression.
- Consists of 32 yes-or-no questions
- A score of > 13 is considered positive for hypomania.
- Reported overall sensitivity is 80% with a specificity of 65% in patients with a mood disorder. [23]
-
Mood disorder questionnaire (MDQ): self-report instrument used to assess and monitor for symptoms of bipolar disorder and other mood disorders
- Early diagnosis and treatment of BD is vital due to the high frequency of self-harm, suicide, and other complications associated with the condition.
- Studies report misdiagnosis rates for BD of up to 80%. [24]
- Reported estimates of unrecognized bipolar disorder in patients treated for depression range from 10–20%. [21][25]
- Schizophrenia: Negative symptoms of schizophrenia may be mistaken for depression.
- Other depressive disorders: e.g., adjustment disorder or persistent depressive disorder (see “Differential diagnoses of MDD”) [26]
Assess all patients presenting with depression for past episodes of mania and/or hypomania to rule out bipolar disorder. Patients with bipolar disorder who are treated with antidepressants without a mood stabilizer are at increased risk of manic symptoms. [15]
Identification of potential psychiatric comorbidities
Anxiety: most common comorbidity; screen using the GAD-7 scale. [12][15][27][28]
- Alcohol and substance use disorder
- Personality disorders
- ADHD [29]
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
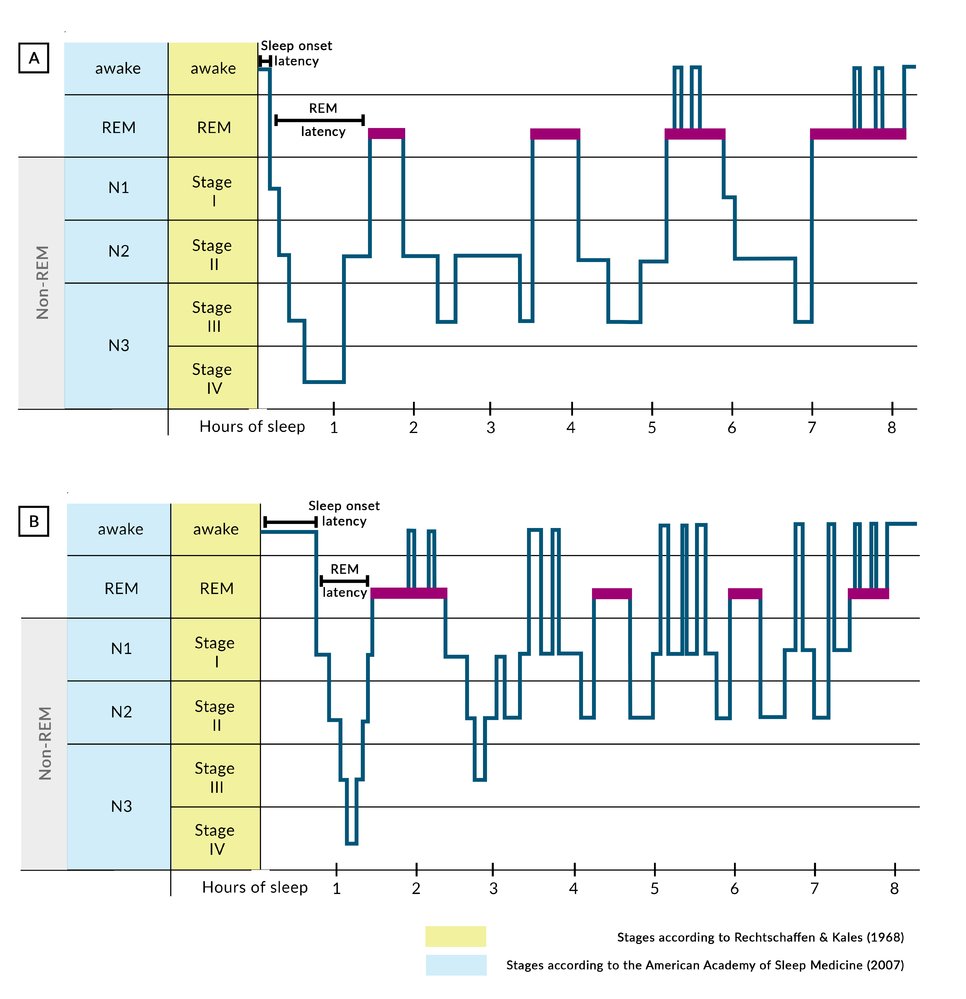
Compared to a healthy person (A), a person suffering from depression (B) has a longer latency of sleep onset, reduced REM latency, prolonged first REM sleep, an increased occurrence of REM sleep in the second part of the night, and an increasing duration of REM sleep throughout the night. In general, depressed people sleep less deeply and are awake more often during the night. Both representations are simplified for didactic purposes (i.e., common, brief periods of arousal during the REM sleep are not shown here).
© AMBOSS
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Differential diagnoses
See “Overview of depressive disorders.”
The differential diagnoses listed here are not exhaustive.
Treatment
The treatment advice in this section applies to the general adult population. For depression in other patient groups (e.g., older adults, children, patients with cancer), see “Depression in special patient groups.”
Approach [15][30][31]
- Advise patients on lifestyle modifications. [30]
- Start initial treatment based on severity.
- Mild depression: typically psychotherapy alone [15][32]
- Moderate and severe depression: psychotherapy and pharmacotherapy [31][32][33]
- Urgently refer patients with severe/complex depression or suicidality to psychiatry; admission may be required.
- Provide the patient and their family with information on depression (see “Managing chronic conditions”).
- Ensure patients receive treatment for:
- Psychiatric comorbidities, e.g., alcohol use disorder
- Contributing physical conditions [30]
- Review patients regularly; assess the efficacy of treatment at ∼ 6 weeks and consider modifications. [30]
Lifestyle modifications [34]
- Sleep hygiene [35][36]
- Reduction in substance use, e.g., alcohol, recreational drugs [37]
- Stress reduction
- Increasing social support
- Regular aerobic exercise [38][39]
- Relaxation/mindfulness [40]
- Improved nutrition [34][41]
Lifestyle modifications are more effective when individualized to the patient.
Psychotherapy [15][30][31]
- May be used alone or in combination with pharmacotherapy
- Options include:
- Cognitive behavioral therapy (CBT)
- Interpersonal therapy
- Behavioral activation
- Psychodynamic psychotherapy
- Supportive psychotherapy
There is no evidence to support the use of one modality of psychotherapy over another for the treatment of MDD. [31]
Initial pharmacotherapy [15][30][31]
Initiation
-
Choice of initial medication
- Most antidepressants have comparable efficacy but different adverse effects.
-
When choosing an antidepressant, consider:
- Psychiatric and medical comorbidities
- Current symptoms
- Previous treatment experiences
- Medication adverse effects
- Interactions with other medications
-
Initial medication trial
- Typically requires ≥ 4 weeks to take effect
- Start with the lowest dose and increase slowly (e.g., with dose adjustments every 2 weeks).
- Monitor for suicidal ideation, manic symptoms, psychotic symptoms, and agitation. [42]
First-line antidepressant medications
- Options include SSRIs (often trialed first), SNRIs, and the atypical antidepressants bupropion and mirtazapine.
- For further information on adverse effects and contraindications, see “Antidepressants.”
| First-line medications for the treatment of major depressive disorder [15][30] | |||
|---|---|---|---|
| Drug class | Examples | Important considerations | |
| SSRIs |
|
|
|
| SNRIs |
|
|
|
| Atypical antidepressants |
|
|
|
|
|
||
SSRIs and venlafaxine have been associated with an increased risk of suicidality in adults aged < 24 years. Monitor patients starting antidepressants carefully for side effects and worsening of depressive symptoms. [43]
Other antidepressant medications
- These medications cause more adverse effects than first-line therapies (e.g., SSRIs). [15]
- Options include:
- Trazodone: used primarily for insomnia; a higher dose is required when used as an antidepressant [44]
- Tricyclic antidepressants, e.g., amitriptyline, nortriptyline
- Monoamine oxidase inhibitors (MAOIs), e.g., phenelzine
MAOIs should not be combined with SSRIs/SNRIs or tricyclic antidepressants, because this may lead to serotonin syndrome. [15]
Ongoing management
Monitoring treatment efficacy
- Monitor treatment response using an objective score of symptom severity, e.g., PHQ-9. [45]
- Determine next steps after ∼ 6 weeks of good adherence to treatment. [30]
| Ongoing management of depression [15][30][31] | ||
|---|---|---|
| Treatment response | Recommended actions | |
| Minimal or no response |
|
|
| Partial response |
|
|
| Remission |
|
|
If an antidepressant has an insufficient effect, always assess the patient's medication adherence before adjusting the treatment plan. [30]
Switching or discontinuing antidepressants [30][31]
- When switching between antidepressants, consider medication class and the risk of serotonin syndrome. [46]
- From one SSRI (excluding fluoxetine) to another SSRI or SNRI: usually a direct switch [46][47]
- To or from non-MAOI classes: usually cross taper [46]
- To or from an MAOI: Taper completely, followed by a 2–6 week washout period. [30]
- When discontinuing medications:
- Consider tapering over 6–8 weeks to : [48][49][50]
- Decrease the risk of relapse
- Prevent antidepressant discontinuation syndrome
- Offer psychotherapy to prevent relapse.
- Consider tapering over 6–8 weeks to : [48][49][50]
When changing between antidepressants, monitor patients carefully for the development of serotonin syndrome. [44]
Symptoms of antidepressant discontinuation syndrome occur when treatment is FINISHed: Flu-like symptoms, Insomnia, Nausea, Imbalance, Sensory disturbances, Hyperarousal [51]
Treatment-resistant depression [30][52]
- Definition: MDD that persists despite trials of ≥ 2 antidepressants at optimal doses [52][53][54]
- Should not be diagnosed without assessing patients for:
- Comorbid psychiatric conditions (e.g., anxiety, substance use disorder)
- Adherence to antidepressant therapy
Management
- Refer all patients to a psychiatrist to determine further treatment.
-
Augmenting agents for depression [30][55]
- Lithium [30][55]
- Second-generation antipsychotics (e.g., aripiprazole)
- Thyroid hormones
- Ketamine [52][55][56]
- Anticonvulsant mood stabilizers (e.g., lamotrigine)
- Stimulants (e.g., methylphenidate)
- Neurostimulation therapy [30]
-
Electroconvulsive therapy (ECT)
- Highly effective treatment for treatment-resistant MDD and severe MDD [30][57]
- Accessibility and patient acceptance have limited its use. [52][57]
- Requires regular attendance for intensive therapy followed by a gradual taper [30][57]
- Vagal nerve stimulation
- Transcranial magnetic stimulation
-
Electroconvulsive therapy (ECT)
Consider ECT for patients with treatment-resistant depression, depression with psychotic features, catatonia, or a high risk of suicide. [58]
Additional therapies [30][31]
The following therapies are not recommended as first-line, have variable evidence to support their use, and should be performed under specialist guidance.
-
Complementary and alternative therapy [30][59]
- Used by some patients as an alternative to antidepressants and/or psychotherapy
- Exercise monotherapy can be considered for mild depression. [30][60]
- Herbal remedies, e.g., St. John's wort, are typically advised against because potential risks outweigh benefits. [30][59]
-
Bright-light therapy: daily exposure to a light intensity of 5000–10,000 lux [30][61]
- Used to treat seasonal affective disorder and may be used as an alternative or adjunctive treatment option in MDD
- Patients should be monitored for hypomania.
-
Sleep deprivation therapy [62][63][64]
- A structured regimen of sleep restriction used alone or in conjunction with bright-light therapy
- Thought to cause a rapid but transient improvement in depressive symptoms [64]
- Risk of inducing mania or seizures
Shared decision-making should be used to plan treatment, taking into consideration previous experience of MDD treatment. [31]
Patients with symptoms of psychosis or suicidal ideation should be urgently referred to a psychiatrist or evaluated in the emergency department; if patients at risk of suicide are deemed safe for outpatient management they should be given details of a suicide crisis line as part of a comprehensive suicide safety plan. [15][27]
Special patient groups
The diagnosis and treatment of depression in special patient groups is broadly the same as for the general adult population, with some modifications.
Depression in children and adolescents [31][65][66]
Overview
- ∼ 15% of adolescents (12–17 years of age) report major depression in the past 12 months. [66][67]
-
The presentation of depression in children may differ from adults. [11][31]
- Classical clinical features of MDD may be less marked.
-
Some symptoms may resemble those of attention deficit hyperactivity disorder, e.g.: [68]
- Irritability
- Difficulty concentrating or worsening performance at school
- Psychiatric comorbidities are common, e.g.: [31]
- Conduct disorder or oppositional defiant disorder
- Anxiety
- Attention deficit hyperactivity disorder
Diagnosis [66]
- See “Diagnosis of MDD.”
- Consider using the PHQ-9 modified for adolescents to screen for depression.
-
Diagnostic criteria for MDD are the same as for adults, with two exceptions: [8]
- Irritability can be noted in the assessment of mood.
- Failure to gain weight can be noted in the assessment of appetite.
Treatment of depression in children [11][65][66]
- Mild depression: Consider 6–8 weeks of active support and monitoring. [65]
- Moderate to severe depression or refractory mild depression
- Initiate treatment of MDD with psychotherapy and/or pharmacotherapy. [65]
- For psychotherapy, CBT and interpersonal therapy for adolescents are preferred.
- Patients requiring pharmacotherapy
- First-line: SSRIs [66]
- Monitor for adverse effects, including suicidality. [65]
- Continue treatment and monitoring for 6–12 months after the resolution of symptoms. [65]
Monitor all children starting on SSRIs for suicidality. [65]
Depression in older adults [6][30][31]
Overview
- MDD in older adults (late-life depression) is common. [69]
-
Risk factors include: [5]
- Social isolation
- Death of a spouse
- Low socioeconomic status
- Comorbid physical illness including uncontrolled pain
- Impairments to cognition and functioning
- Older patients may present atypically with irritability, anxiety, or physical symptoms as opposed to low mood. [6]
Diagnosis
- See “Diagnosis of MDD.”
- Consider using an adapted screening score, e.g., the Geriatric Depression Scale-15.
- Neurological disease and coexisting medical conditions are more common in this patient group; work up thoroughly to exclude physical causes.
- Older adults have an elevated suicide risk; screen carefully for suicidality. [5]
Treatment
- Lifestyle changes: Exercise may be particularly beneficial. [6]
- Pharmacotherapy: Older adults have an increased risk of adverse effects from medications (see “Pharmacology for older adults”). [6][70]
- SSRIs: preferred first-line treatment in individuals aged ≥ 60 years [6]
- Consider using reduced frequencies and/or lower doses than in the general adult population.
- Minimize polypharmacy whenever possible.
- Psychotherapy: Consider modifications in patients with cognitive impairment; problem-solving therapy may be effective. [6]
- ECT: highly effective; response rates are higher in adults aged > 65 years than in younger adults. [30]
- See “Treatment of MDD” for details.
Cognitive impairment should be considered as a possible underlying cause of depression in older adults. [6]
In older patients, monitor for hyponatremia after starting or adjusting the dosages of SSRIs, SNRIs, TCAs, or mirtazapine. [70]
Depression in patients receiving palliative care [71]
Overview
- Depressive symptoms or thoughts of suicide are common in patients with a limited life expectancy. [71][72]
-
Symptoms of depression (e.g., changes in appetite, low energy, impaired sleep) may overlap with : [71][73][74]
- Symptoms of an underlying medical condition
- Adverse effects of treatment
- Grief
Diagnosis [75]
- See “Diagnosis of MDD.”
- Screen for depression at diagnosis of a life-limiting illness and periodically thereafter. [75]
- Identify physical symptoms that may contribute to low mood (see “Principles of cancer care”).
Treatment [71][73]
- Psychotherapy is first-line treatment for mild to moderate depression.
- The choice of antidepressant is based on symptoms and comorbidities.
- SSRIs are typically used first-line because they have the lowest risk of adverse effects and interactions. [73][76]
-
Antidepressants may be selected because they have a dual function. [73]
- Consider a tricyclic or SNRI if the patient also has neuropathic pain.
- Use mirtazapine if patients have poor appetite or insomnia.
- Psychostimulants (e.g., methylphenidate) are sometimes used for patients with limited life expectancy. [71][77]
- See “Treatment of MDD” for details.
Consider life expectancy when selecting treatment for depression in patients near the end of life; many antidepressants can take several weeks to have an effect. [71]
Depression in patients with cancer [73][75]
MDD is more common in patients with cancer than in the general population. [78]
Diagnosis
- See “Diagnosis of MDD.”
- Clinical clues may include: [75]
- Poor adherence to treatment regimens
- Difficulty with referral follow-through
- Anhedonia that goes beyond the expected reaction of receiving a cancer diagnosis
- Screening [75]
- Actively screen for depression at time of original cancer diagnosis, regularly throughout cancer therapy, and when significant life events occur, e.g., in the case of cancer progression or recurrence, changes in therapy, entering into palliative care, or personal/social distress.
- The American Society of Clinical Oncology recommends the PHQ-2 and PHQ-9 screening tools for initial assessment.
- Assessment of MDD in patients with cancer can be complicated due to overlapping somatic symptoms like fatigue, insomnia or hypersomnia, weight loss, and cognitive impairment. [79]
- Insomnia or hypersomnia can be caused by poorly controlled pain or CNS malignancy.
- Fatigue can be due to malignancy, radiation, chemotherapy, or anemia (see cancer-related fatigue).
- Weight loss can be caused by cancer anorexia-cachexia syndrome, chemotherapy-induced nausea and vomiting, or chemotherapy-induced diarrhea.
- Cognitive impairment can be caused by CNS malignancy, chemotherapy, hormone therapy, or radiation.
Treatment [73][79]
- Treat cancer pain and other physical symptoms. [79]
-
The choice of antidepressants is based on symptoms and comorbidities. [73]
- SSRIs are typically used first-line because they have the lowest risk of adverse effects and interactions.
- Many antidepressants have a dual function that may benefit patients, e.g.:
- Consider a tricyclic or SNRI if the patient also has neuropathic pain.
- Use mirtazapine if the patient has poor appetite, nausea, or insomnia.
- See “Treatment of MDD” for details.
Depression post myocardial infarction [80]
Overview
- The risk of depression in individuals post MI is approx. three times that of the general population. [81]
- Depression post MI is associated with an increased risk of further adverse cardiovascular events.
Diagnosis
- See “Diagnosis of MDD.”
- Screening
- All patients with cardiovascular disease should be screened for depression.
- The American Heart Association recommends the PHQ-2 and PHQ-9 screening tools for initial assessment.
Treatment
- First-line treatment includes SSRIs, psychotherapy, and/or moderate exercise.
- SNRIs may increase the risk of hypertension and tachycardia.
- Avoid tricyclics due to their cardiotoxic effects.
- See “Treatment of MDD” for details.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Depression in the peripartum period
Peripartum depression
MDD that occurs during pregnancy or after delivery [8][82][83]
Epidemiology
- Affects up to 14% of pregnancies [84]
-
Risk factors for peripartum depression include: [82][85]
- Personal or family history of depression
- History of intimate partner violence
- Unplanned or undesired pregnancy
- Medical complications during pregnancy
- Poor support network
- Financial stress
- Patients with a previous history of depression are at increased risk of developing peripartum depression.
Diagnostics of peripartum depression
- See “Diagnosis of MDD.”
- Screening [10][86][87]
- Screen at least once in the peripartum period. [10][88][89]
- Consider using a modified screening tool, e.g., the Edinburgh postnatal depression scale.
- For patients with a positive screen: [89]
- Screen for bipolar disorder, e.g., using the MDQ.
- Screen for infanticidal thoughts as well as suicidality. [82][90]
Treatment of peripartum depression
Treatment of peripartum depression is broadly the same as for the general adult population (see “Treatment of MDD”), with some modifications.
Antenatal considerations
- Offer psychotherapy as an alternative to pharmacotherapy in mild to moderate depression.
- Discontinuation of pharmacotherapy can be considered in stable patients with a known diagnosis of MDD. [91]
- Patients starting or continuing antidepressants: Educate on the risks and benefits of antidepressants and monitor carefully. [91]
- Avoid paroxetine during pregnancy because of the potential risk of cardiac anomalies. [30]
- Use monotherapy whenever possible.
Postpartum considerations
- Patients already on SSRIs, SNRIs, TCAs, and mirtazapine can continue treatment while breastfeeding. [92]
- In patients starting antidepressants, begin with a medication that has few side effects and minimal transfer to breastmilk, e.g., sertraline. [30][82][92]
- Newer alternatives include :
- Brexanolone infusion [93]
- Zuranolone [94]
- Mother and baby units are preferred for patients requiring hospitalization. [95]
Depression has adverse effects on maternal and fetal health; the risks of pharmacotherapy should be balanced against the risks of leaving the condition untreated. [91]
ECT can be safely offered to pregnant and lactating patients who prefer to avoid pharmacotherapy. [30]
While SSRIs are generally compatible with breastfeeding, infants of breastfeeding mothers taking SSRIs should be monitored for signs of medication toxicity, such as excessive tiredness, irritability, and poor feeding. [82]
Complications
Untreated peripartum depression can have adverse consequences. [82][91]
- Maternal: suicide, impact on bonding
- Newborn: infanticide, failure to thrive, developmental delay [96]
Prevention
For patients at increased risk considering pregnancy :
- Consider psychiatry referral prior to conception. [91]
- Recommend psychotherapy. [84]
Differential diagnosis of postpartum low mood
| Overview of postpartum low mood [30][82][96] | |||
|---|---|---|---|
| Features | Postpartum blues | Postpartum depression | Postpartum psychosis [97] |
| Epidemiology |
|
|
|
| Timing |
|
|
|
| Clinical features [82][96][99] |
|
|
|
| Diagnosis |
|
|
|
| Management |
|
|
|
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Related One-Minute Telegram
- One-Minute Telegram 92-2024-1/3: Perinatal depression and risk of death
- One-Minute Telegram 87-2023-1/3: AI-guided treatment of depression: a byte-sized breakthrough?
- One-Minute Telegram 81-2023-1/3: Swift lift for postpartum depression
- One-Minute Telegram 78-2023-1/3: USPSTF recommends screening adults for major depressive disorder and anxiety disorders
- One-Minute Telegram 73-2023-2/3: Providing a boost for treatment-resistant depression
- One-Minute Telegram 62-2022-2/3: ECT more effective than ketamine in major depressive episode
- One-Minute Telegram 7-2020-3/3: Can Vitamin D3 supplementation prevent depression?
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- 2018 ACOG Committee Opinion: Screening for Perinatal Depression
- 2018 AAP Guidelines for Adolescent Depression in Primary Care: Identification, Assessment, and Initial Management
- 2018 AAP Guidelines for Adolescent Depression in Primary Care: Treatment and Ongoing Management
- 2016 ASCO Clinical Practice Guideline: Management of Depression in Patients With Cancer
- 2010 APA Practice Guideline: Treatment of Patients with Major Depressive Disorder
- One-Minute Telegram url:
References
- Hasin DS, Sarvet AL, Meyers JL, et al. "Epidemiology of Adult DSM-5 Major Depressive Disorder and Its Specifiers in the United States". JAMA Psychiatry. 75(4). :336. (2018)
- Kessler RC, Berglund P, Demler O. "Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication". Arch Gen Psychiatry. 62(6). :593-602. (2005)
- Hasler G. "Pathophysiology of depression: Do we have any solid evidence of interest to clinicans?". World Psychiatry. 9(3). :155-161. (2010)
- Siegel GJ, Agranoff BW, Albers RW et al. "Basic Neurochemistry: Molecular, Cellular and Medical Aspects". Lippincott-Raven. (1999). ISBN: 039751820x
- Maurer DM, Raymond TJ, Davis BN. "Depression: Screening and Diagnosis". Am Fam Physician. 98(8). :508-515. (2018)
- Taylor WD. "Depression in the Elderly". N Engl J Med. 371(13). :1228-1236. (2014)
- Association AP. "The American Psychiatric Association Practice Guidelines for the Psychiatric Evaluation of Adults, Third Edition". American Psychiatric Pub. (2015). ISBN: 9780890424650
- Barry MJ, Nicholson WK, et al. "Screening for Depression and Suicide Risk in Adults". JAMA. 329(23). :2057. (2023)
- Zuckerbrot RA, Cheung A, Jensen PS, et al. "Guidelines for Adolescent Depression in Primary Care (GLAD-PC): Part I. Practice Preparation, Identification, Assessment, and Initial Management". Pediatrics. 141(3). (2018)
- Hirschtritt ME, Kroenke K. "Screening for Depression". JAMA. 318(8). :745. (2017)
- Strauss E, Sherman EMS, Spreen O. "A Compendium of Neuropsychological Tests". American Chemical Society. (2006). ISBN: 9780195159578
- American Psychiatric Association. "Diagnostic and Statistical Manual of Mental Disorders". American Psychiatric Association. (2013). ISBN: 9780890425558
- "DSM-5-TR update to Major Depressive Disorder". https://web.archive.org/web/20220614223136/https://www.psychiatry.org/File%20Library/Psychiatrists/Practice/DSM/DSM-5-TR/APA-DSM5TR-MajorDepressiveDisorder.pdf
- Park LT, Zarate CA. "Depression in the Primary Care Setting". N Engl J Med. 380(6). :559-568. (2019)
- LeFevre ML. "Screening for Suicide Risk in Adolescents, Adults, and Older Adults in Primary Care: U.S. Preventive Services Task Force Recommendation Statement". Ann Intern Med. 160(10). :719. (2014)
- Longo LP, Johnson B. "Addiction: Part I. Benzodiazepines--side effects, abuse risk and alternatives". Am Fam Physician. 61(7). :2121-8. (2000)
- McGregor C, Srisurapanont M, Jittiwutikarn J, et al. "The nature, time course and severity of methamphetamine withdrawal". Addiction. 100(9). :1320-1329. (2005)
- Wilde EA, Kim HF, et al. "The American Psychiatric Publishing Textbook of Psychiatry, Sixth Edition". American Psychiatric Pub. (2014). ISBN: 9781585624447
- Sculthorpe LD, Douglass AB. "Sleep Pathologies in Depression and the Clinical Utility of Polysomnography". The Canadian Journal of Psychiatry. 55(7). :413-421. (2010)
- MILLER C. "Sensitivity and specificity of the Mood Disorder Questionnaire for detecting bipolar disorder". J Affect Disord. 81(2). :167-171. (2004)
- "The Mood Disorder Questionnaire (MDQ) - Overview". https://ibpf.org/wp-content/uploads/2016/11/MDQ.pdf
- Meyer TD, Schrader J, Ridley M, Lex C. "The Hypomania Checklist (HCL) — Systematic review of its properties to screen for bipolar disorders". Compr Psychiatry. 55(5). :1310-1321. (2014)
- Sasdelli A, Lia L, Luciano CC, et al. "Screening for Bipolar Disorder Symptoms in Depressed Primary Care Attenders: Comparison between Mood Disorder Questionnaire and Hypomania Checklist (HCL-32).". Psychiatry journal. 2013. :548349. (2013)
- Hughes T, Cardno A, West R, et al. "Unrecognised bipolar disorder among UK primary care patients prescribed antidepressants: an observational study". British Journal of General Practice. 66(643). :e71-e77. (2016)
- Maercker A, Lorenz L. "Adjustment disorder diagnosis: Improving clinical utility". World J Biol Psychiatry. 19(sup1). :S3-S13. (2018)
- McDowell AK, Lineberry TW, Bostwick JM. "Practical Suicide-Risk Management for the Busy Primary Care Physician". Mayo Clin Proc. 86(8). :792-800. (2011)
- Kessler RC, Sampson NA, Berglund P, et al. "Anxious and non-anxious major depressive disorder in the World Health Organization World Mental Health Surveys". Epidemiol Psychiatr Sci. 24(3). :210-226. (2015)
- Katzman MA, Bilkey TS, Chokka PR, Fallu A, Klassen LJ. "Adult ADHD and comorbid disorders: clinical implications of a dimensional approach". BMC Psychiatry. 17(1). (2017)
- "American Psychiatric Association Practice Guidelines for the Treatment of Patients With Major Depressive Disorder". https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/mdd.pdf. [2010-10-01]
- "American Psychological Association Clinical Practice Guideline for the Treatment of Depression Across Three Age Cohorts". https://www.apa.org/depression-guideline/guideline.pdf. [2019-02-16]
- Gabriel FC, de Melo DO, Fráguas R, et al. "Pharmacological treatment of depression: A systematic review comparing clinical practice guideline recommendations". PLoS ONE. 15(4). :e0231700. (2020)
- Craighead WE, Dunlop BW. "Combination Psychotherapy and Antidepressant Medication Treatment for Depression: For Whom, When, and How". Annu Rev Psychol. 65(1). :267-300. (2014)
- Sarris J, O’Neil A, Coulson CE, Schweitzer I, Berk M. "Lifestyle medicine for depression". BMC Psychiatry. 14(1). (2014)
- Li L, Wu C, Gan Y, Qu X, Lu Z. "Insomnia and the risk of depression: a meta-analysis of prospective cohort studies". BMC Psychiatry. 16(1). (2016)
- Alexander J. Scott, Thomas L. Webb, Marrissa Martyn-St James, Georgina Rowse, Scott Weich. "Improving sleep quality leads to better mental health: A meta-analysis of randomised controlled trials". Sleep Med Rev. 60. :101556. (2021)
- Lori Davis, Akihito Uezato, Jason M Newell, Elizabeth Frazier. "Major depression and comorbid substance use disorders". Curr Opin Psychiatry. 21(1). :14-18. (2008)
- Cooney GM, Dwan K, Greig CA, et al. "Exercise for depression". Cochrane Database Syst Rev. :CD004366. (2013)
- Morres ID, Hatzigeorgiadis A, Stathi A, et al. "Aerobic exercise for adult patients with major depressive disorder in mental health services: A systematic review and meta-analysis". Depress Anxiety. 36(1). :39-53. (2018)
- Blanck P, Perleth S, Heidenreich T, et al. "Effects of mindfulness exercises as stand-alone intervention on symptoms of anxiety and depression: Systematic review and meta-analysis". Behav Res Ther. 102. :25-35. (2018)
- Jacka FN, O’Neil A, Opie R, et al. "A randomised controlled trial of dietary improvement for adults with major depression (the ‘SMILES’ trial)". BMC Med. 15(1). (2017)
- Adams SM, Miller KE, Zylstra RG. "Pharmacologic management of adult depression". Am Fam Physician. 77(6). :785-92. (2008)
- Spielmans GI, Spence-Sing T, Parry P. "Duty to Warn: Antidepressant Black Box Suicidality Warning Is Empirically Justified". Front Psychiatry. 11. :18. (2020)
- Murphy MJ, Peterson MJ. "Sleep Disturbances in Depression". Sleep Medicine Clinics. 10(1). :17-23. (2015)
- Titov N, Dear BF, McMillan D, et al. "Psychometric Comparison of the PHQ-9 and BDI-II for Measuring Response during Treatment of Depression". Cogn Behav Ther. 40(2). :126-136. (2011)
- Procyshyn, M. R, Bezchlibnyk-Butler R, et al. "Clinical Handbook of Psychotropic Drugs". Hogrefe Publishing. (2021). ISBN: 9781616765934
- Zwiebel SJ, Viguera AC. "Discontinuing antidepressants: Pearls and pitfalls". Cleve Clin J Med. 89(1). :18-26. (2022)
- Sørensen A, Juhl Jørgensen K, Munkholm K. "Clinical practice guideline recommendations on tapering and discontinuing antidepressants for depression: a systematic review". Ther Adv Psychopharmacol. 12. :204512532110676. (2022)
- Jha MK. "Discontinuing Antidepressants". J Clin Psychiatry. 80(6). (2019)
- Jha MK, Rush AJ, Trivedi MH. "When Discontinuing SSRI Antidepressants Is a Challenge: Management Tips". Am J Psychiatry. 175(12). :1176-1184. (2018)
- Warner CH, Bobo W, Warner C, Reid S, Rachal J. "Antidepressant discontinuation syndrome". Am Fam Physician. 74(3). :449-56. (2006)
- Voineskos D, Daskalakis ZJ, Blumberger DM. "Management of Treatment-Resistant Depression: Challenges and Strategies". Neuropsychiatr Dis Treat. 16. :221-234. (2020)
- Little A. "Treatment-resistant depression". Am Fam Physician. 80(2). :167-72. (2009)
- Sforzini L, Worrell C, Kose M, et al. "A Delphi-method-based consensus guideline for definition of treatment-resistant depression for clinical trials". Mol Psychiatry. 27(3). :1286-1299. (2021)
- Taylor RW, Marwood L, Oprea E, et al. "Pharmacological Augmentation in Unipolar Depression: A Guide to the Guidelines". Int J Neuropsychopharmacol. 23(9). :587-625. (2020)
- Sanacora G, Frye MA, McDonald W, et al. "A Consensus Statement on the Use of Ketamine in the Treatment of Mood Disorders". JAMA Psychiatry. 74(4). :399. (2017)
- Espinoza RT, Kellner CH. "Electroconvulsive Therapy". N Engl J Med. 386(7). :667-672. (2022)
- Milev RV, Giacobbe P, Kennedy SH, et al. "Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder". Can J Psychiatry. 61(9). :561-575. (2016)
- Haller H, Anheyer D, Cramer H, Dobos G. "Complementary therapies for clinical depression: an overview of systematic reviews". BMJ open. 9(8). :e028527. (2019)
- Hoffman BM, Babyak MA, Craighead WE, et al. "Exercise and Pharmacotherapy in Patients With Major Depression: One-Year Follow-Up of the SMILE Study". Psychosom Med. 73(2). :127-133. (2011)
- Maruani J, Geoffroy PA. "Bright Light as a Personalized Precision Treatment of Mood Disorders". Front Psychiatry. 10. :85. (2019)
- Mitter P, De Crescenzo F, Loo Yong Kee K, et al. "Sleep deprivation as a treatment for major depressive episodes: a systematic review and meta-analysis". Sleep Med Rev. :101647. (2022)
- Ravindran AV, Balneaves LG, Faulkner G, et al. "Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder". Can J Psychiatry. 61(9). :576-587. (2016)
- Benedetti F, Colombo C. "Sleep Deprivation in Mood Disorders". Neuropsychobiology. 64(3). :141-151. (2011)
- Cheung AH, Zuckerbrot RA, Jensen PS, et al. "Guidelines for Adolescent Depression in Primary Care (GLAD-PC): Part II. Treatment and Ongoing Management". Pediatrics. 141(3). (2018)
- Selph SS, McDonagh MS. "Depression in Children and Adolescents: Evaluation and Treatment". Am Fam Physician. 100(10). :609-617. (2019)
- Bitsko RH, Claussen AH, Lichstein J, et al. "Mental Health Surveillance Among Children — United States". MMWR Supp. Suppl-2(71). :1-42. (2022)
- Fraser A, Cooper M, Agha SS, et al. "The presentation of depression symptoms in attention-deficit/hyperactivity disorder: comparing child and parent reports". Child Adolesc Ment Health. 23(3). :243-250. (2017)
- Aziz R, Steffens DC. "What Are the Causes of Late-Life Depression?". Psychiatr Clin North Am. 36(4). :497-516. (2013)
- 2023 American Geriatrics Society Beers Criteria® Update Expert Panel. "American Geriatrics Society 2023 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults". J Am Geriatr Soc. 71(7). :2052-2081. (2023)
- Widera EW, Block SD. "Managing grief and depression at the end of life". Am Fam Physician. 86(3). :259-64. (2012)
- Irwin SA. "Palliative Care". Am Psychiatr Publ. 11(1). :48-51. (2013)
- Li M, Kennedy EB, Byrne N, et al. "Management of Depression in Patients With Cancer: A Clinical Practice Guideline". J Oncol Pract. 12(8). :747-56. (2016)
- "The Management of Depression in Palliative Care: European Clinical Guidelines". https://www.kcl.ac.uk/cicelysaunders/attachments/depression-guidlines/the-management-of-depression-in-palliative-care.pdf
- Andersen BL, DeRubeis RJ, Berman BS, et al. "Screening, Assessment, and Care of Anxiety and Depressive Symptoms in Adults With Cancer: An American Society of Clinical Oncology Guideline Adaptation". J Clin Oncol. 32(15). :1605-1619. (2014)
- Alexander K, Goldberg J, Korc-Grodzicki B. "Palliative Care and Symptom Management in Older Patients with Cancer". Clin Geriatr Med. 32(1). :45-62. (2016)
- Howard P, Shuster J, Twycross R, Mihalyo M, Wilcock A. "Psychostimulants". J Pain Symptom Manage. 40(5). :789-795. (2010)
- Krebber AMH, Buffart LM, Kleijn G, et al. "Prevalence of depression in cancer patients: a meta‐analysis of diagnostic interviews and self‐report instruments". Psychooncology. 23(2). :121-130. (2013)
- Li M, Fitzgerald P, Rodin G. "Evidence-Based Treatment of Depression in Patients With Cancer". J Clin Oncol. 30(11). :1187-1196. (2012)
- Jha MK, Qamar A, Vaduganathan M, Charney DS, Murrough JW. "Screening and Management of Depression in Patients With Cardiovascular Disease: JACC State-of-the-Art Review". J Am Coll Cardiol. 73(14). :1827-1845. (2019)
- Thombs BD, Bass EB, Ford DE, et al. "Prevalence of depression in survivors of acute myocardial infarction". J Gen Intern Med. 21(1). :30-38. (2006)
- Duval F, Mokrani MC, Crocq MA et al. "Dopaminergic function and the cortisol response to dexamethasone in psychotic depression". Prog Neuropsychopharmacol Biol Psychiatry. 24(2). :207-225. (2000)
- Langan R, Goodbred AJ. "Identification and Management of Peripartum Depression". Am Fam Physician. 93(10). :852-8. (2016)
- Suri R, Altshuler L. "Postpartum Depression: Advances in Recognition and Treatment". Am Psychiatr Publ. 10(1). :15-21. (2012)
- Curry SJ, Krist AH, et al. "Interventions to Prevent Perinatal Depression". JAMA. 321(6). :580. (2019)
- Paladine HL, Blenning CE, Strangas Y. "Postpartum Care: An Approach to the Fourth Trimester". Am Fam Physician. 100(8). :485-491. (2019)
- "Screening for Perinatal Depression". https://www.acog.org/-/media/project/acog/acogorg/clinical/files/committee-opinion/articles/2018/11/screening-for-perinatal-depression.pdf. [2018-11-01]
- Presidential Task Force on Redefining the Postpartum Visit Committee on Obstetric Practice. "Optimizing Postpartum Care". Obstetrics & Gynecology. 131(5). :140-150. (2018)
- Earls MF, Yogman MW, Mattson G, et al. "Incorporating Recognition and Management of Perinatal Depression Into Pediatric Practice". Pediatrics. 143(1). (2019)
- "Screening and Diagnosis of Mental Health Conditions During Pregnancy and Postpartum Clinical Practice Guideline No. 4". http://dx.doi.org/10.1097/AOG.0000000000005200. [2023-06-01]
- Stewart DE. "Depression during Pregnancy". N Engl J Med. 365(17). :1605-1611. (2011)
- Yonkers K et al. "The management of depression during pregnancy: a report from the American Psychiatric Association and the American College of Obstetricians and Gynecologists". Obstet Gynecol. 114(3). :703-713. (2009)
- Sriraman NK, Melvin K, Meltzer-Brody S. "ABM Clinical Protocol #18: Use of Antidepressants in Breastfeeding Mothers". Breastfeed Med. 10(6). :290-9. (2015)
- Walton N, Maguire J. "Allopregnanolone-based treatments for postpartum depression: Why/how do they work?". Neurobiol Stress. 11. :100198. (2019)
- Deligiannidis KM, Meltzer-Brody S, Maximos B, et al. "Zuranolone for the Treatment of Postpartum Depression". Am J Psychiatry. (2023)
- Meltzer-Brody S, Howard LM, Bergink V, et al. "Postpartum psychiatric disorders". Nat Rev Dis Primers. 4(1). (2018)
- Stewart DE, Vigod S. "Postpartum Depression". N Engl J Med. 375(22). :2177-2186. (2016)
- Sit D, Rothschild AJ, Wisner KL. "A Review of Postpartum Psychosis". J Womens Health (Larchmt). 15(4). :352-368. (2006)
- Brenda L. Bauman, Jean Y. Ko, Shanna Cox, et al. "<i>Vital Signs:</i> Postpartum Depressive Symptoms and Provider Discussions About Perinatal Depression — United States, 2018". MMWR Morb Mortal Wkly Rep. 69(19). :575-581. (2020)
- Pearlstein T, Howard M, Salisbury A, Zlotnick C. "Postpartum depression". Am J Obstet Gynecol. 200(4). :357-364. (2009)