Summary
Malabsorption is the impaired absorption of nutrients caused by functional or structural alterations of the intestinal mucosa or inadequate breakdown of food in the intestinal lumen (i.e., maldigestion). Malabsorption can lead to malnutrition, which, in children, can manifest with delayed and inadequate physical development. Adults typically present with chronic diarrhea, weight loss, steatorrhea, and signs of nutritional deficiencies. Diagnosis is primarily based on clinical evaluation. Diagnostic testing, including laboratory studies, is aimed at identifying the underlying cause, which is the focus of management, e.g., adherence to a gluten-free diet for patients with celiac disease.

© AMBOSS
Definitions
-
Malabsorption
- Impaired absorption of nutrients due to functional or structural alterations of the intestinal mucosa
- Often used as an umbrella term for both malabsorption and maldigestion in clinical practice
- Maldigestion: impaired breakdown of food in the intestinal lumen
Malabsorption is commonly used as an umbrella term for both malabsorption and maldigestion, despite distinct underlying pathological mechanisms.
Etiology
Disorders can cause malabsorption through multiple pathways simultaneously. [1]
-
Mucosal damage [1][2]
- Celiac disease [2]
- Infections, e.g., tropical sprue, Whipple disease, giardiasis [2]
- Inflammatory bowel disease, e.g., Crohn disease [1]
- Lactase deficiency
- Chronic radiation enteritis
- Chronic mesenteric ischemia
- Intestinal lymphangiectasia [1]
- HIV enteropathy [1]
- Small intestinal bacterial overgrowth (SIBO) [1][2]
- Short bowel syndrome [2]
- Hormonally active tumors (e.g., gastrinoma, VIPoma)
-
Maldigestion
- Exocrine pancreatic insufficiency [2]
-
Bile acid deficiency, due to: [1]
- Hepatobiliary disorders, e.g., cholestasis, cirrhosis, primary sclerosing cholangitis
- Bile acid malabsorption, e.g., after ileum resection or due to Crohn disease [2]
- Medications, e.g., orlistat, acarbose [3]
- Gastric resection [1]
Malabsorption can be caused by insufficient nutrient absorption and/or insufficient breakdown of nutrients.
Subtypes and variants
"Short bowel syndrome" is described in detail in a separate article.
Carbohydrate malabsorption [4]
- Definition: the inability to efficiently absorb nutritional carbohydrates (e.g., lactose, fructose, sorbitol) in the small intestine, either due to primary (e.g., lactase deficiency) or secondary causes (e.g., SIBO, Crohn disease)
- Symptoms can often be managed by removing the specific type of carbohydrate from the diet.
- See also:
- Lactose intolerance (common)
- Fructose malabsorption, including hereditary fructose intolerance
Exocrine pancreatic insufficiency [5][6]
- Definition: the inability of the pancreas to release pancreatic enzymes necessary for digestion, including amylase, lipases, and proteases (e.g., trypsinogen, chymotrypsinogen, elastase), which can lead to malabsorption of fats, fat-soluble vitamins (A, D, E, K), vitamin B12, carbohydrates, proteins, folate, thiamine, zinc, calcium, and magnesium
-
Etiology
- Chronic pancreatitis
- Cystic fibrosis
- Obstruction, e.g., due to pancreatic cancer
- Pancreatic resection
- Severe necrotizing pancreatitis
- Shwachman-Diamond syndrome: a rare autosomal recessive condition and the second most common cause of exocrine pancreatic insufficiency in children, after cystic fibrosis
-
Clinical features of exocrine pancreatic insufficiency
- Steatorrhea (with or without diarrhea)
- Weight loss
- Secondary protein-energy malnutrition
- Signs of nutritional deficiencies
-
Diagnostics [6]
- Stool elastase test (preferred initial test): ↓ fecal elastase-1 (< 100 mcg/g) [6]
- Consider abdominal imaging (CT, MRI, or endoscopic ultrasound) to evaluate for pancreatic disease.
- Additional supportive findings include:
- ↓ Bicarbonate and ↓ pH in the duodenum
- If performed, normal D-xylose absorption test
-
Management [5][6]
- Prescribe pancreatic enzyme replacement therapy with food, e.g., pancrelipase ; adjust as needed. [6]
- H2 receptor blocker or PPI for patients receiving non-enteric-coated pancreatic enzyme replacement therapy [6]
- Fat-soluble vitamin supplementation [6]
- Dietary modifications (e.g., high-protein diet) under specialist guidance [6]
- Monitoring for nutritional deficiencies and complications of deficiencies
Clinical features
General symptoms
Symptoms vary based on the cause and severity of the condition but are often mild and nonspecific.
- Chronic diarrhea (most common)
- Steatorrhea
- Weight loss
- Fatigue
- Abdominal distention, flatulence
- Additional symptoms in children include delayed and inadequate physical development.
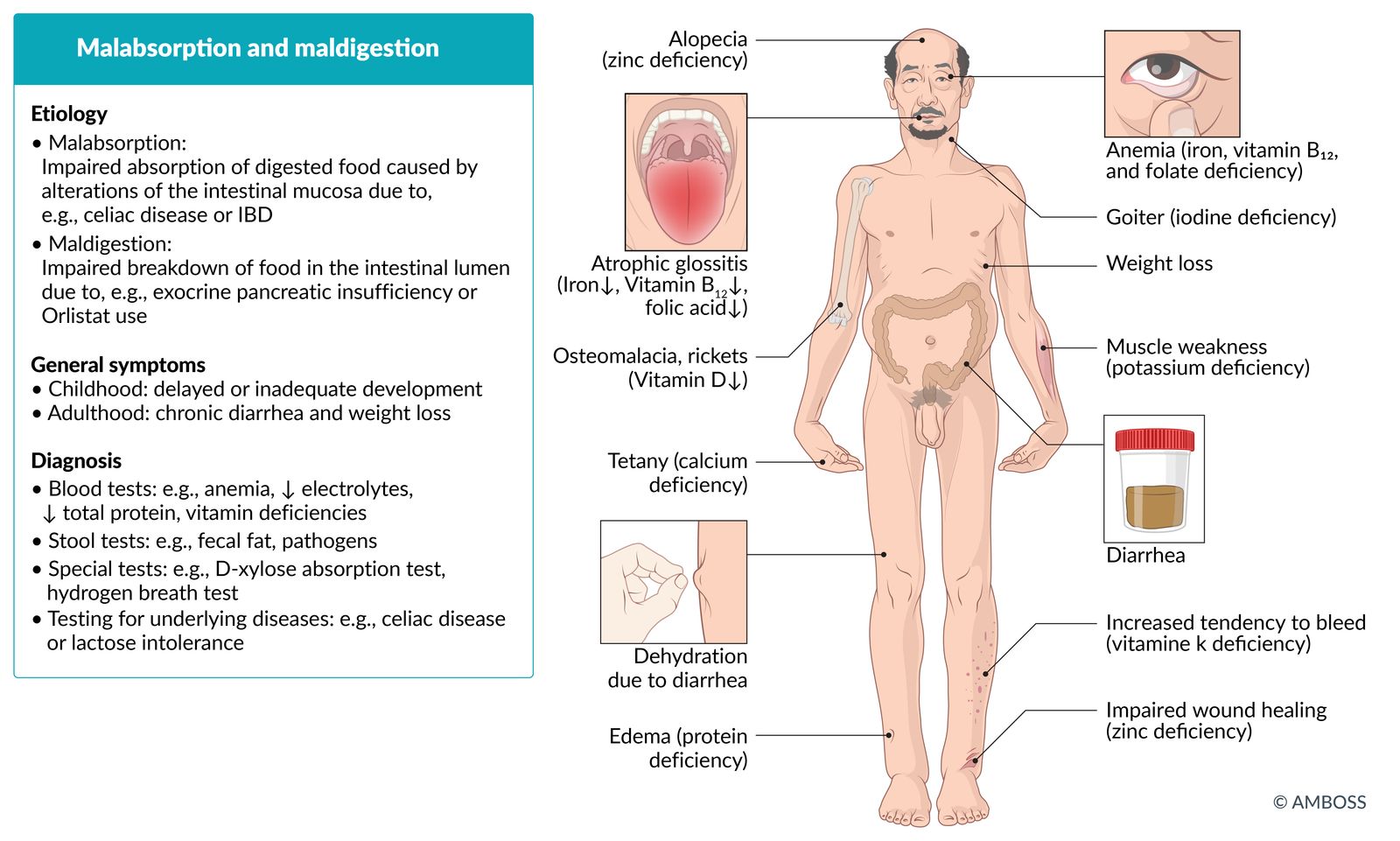
Signs of nutritional deficiencies
-
Vitamin deficiency, e.g.:
- Clinical features of vitamin D deficiency, e.g., osteoporosis
- Clinical features of vitamin B12 deficiency, e.g., fatigue, pallor, peripheral neuropathy
- See “Water-soluble vitamins” and “Fat-soluble vitamins” for an overview of symptoms of other vitamin deficiencies.
-
Trace element deficiency, e.g.:
- Zinc deficiency: alopecia, diarrhea, periorificial and/or acral dermatitis
- Iron deficiency anemia: fatigue, pallor
- Protein deficiency: edema, cachexia
-
Electrolyte deficiency, e.g.:
- Clinical features of hypokalemia
- Clinical features of hypocalcemia
Diagnosis
Approach [7]
Suspect malabsorption in patients with chronic diarrhea, steatorrhea, and/or nutritional deficiencies.
- Obtain a focused patient history, including:
- Symptom duration and triggers, e.g., specific foods
- Risk factors for potentially causative diseases, e.g., alcohol consumption
- History of abdominal surgery (including bariatric surgery)
- Consider routine laboratory studies to assess for diagnostic clues for nutritional deficiencies.
- Obtain focused testing based on clinical suspicion.
Diarrhea can have various causes, but the presence of nutritional deficiencies should raise suspicion for malabsorption, as nutrients are almost exclusively absorbed in the small bowel. [7]
Laboratory studies
Broad diagnostic testing is not routinely necessary, as the differential diagnosis can usually be narrowed based on patient history.
-
Routine studies: may indicate certain deficiencies
-
CBC
- Macrocytic anemia in vitamin B12 deficiency and/or folate deficiency [7]
- Microcytic anemia in iron deficiency [7]
-
CMP
- ↓ Electrolytes
- ↓ Total protein, ↓ albumin
- Abnormal cholesterol levels
- ↑ ALP and ↓ calcium in vitamin D deficiency [7]
- Coagulation panel: ↑ PT in vitamin K deficiency [7]
-
CBC
-
Testing for specific deficiencies (based on previous findings), e.g.:
- Fat-soluble vitamins, including vitamin D, vitamin K, β-carotene (indirect marker of vitamin A deficiency)
- Vitamin B12, folate
- Iron
Stool studies
-
Evaluation for steatorrhea [7][8]
- Screening test: Sudan III stain
- Gold standard test: 72-hour fecal fat test
-
Evaluation for specific causes of malabsorption
- Stool culture ± microscopy: to assess for pathogens, e.g., Giardia duodenalis, Escherichia coli
- Fecal elastase-1: to evaluate for exocrine pancreatic insufficiency
- Stool pH: pH < 6 supports carbohydrate malabsorption. [8]
Small bowel evaluation
Diagnostic testing in the absence of a clear clinical suspicion focuses on the small bowel. [7]
Endoscopy
-
Small bowel biopsy [7]
- Indications include:
- Steatorrhea
- Chronic diarrhea
- Abnormalities on small bowel follow-through
- Can be used to diagnose mucosal diseases, e.g., Whipple disease, amyloidosis, Crohn disease, celiac disease
- See “Differential diagnosis of malabsorption” for specific findings.
- Indications include:
- Small bowel aspirate: to evaluate for SIBO [8]
Other
These tests have limited clinical relevance because of widespread access to endoscopy.
-
Small bowel follow-through [7]
- Findings may be nonspecific, e.g., dilation, diverticula, strictures
- Rarely, findings may be specific, e.g., string sign in Crohn disease
- Cannot be used to rule out diseases
-
D-xylose absorption test: may be used to assess the absorptive function of the upper small intestine
- Physiological background [7]
- Intestinal absorption of D-xylose requires intact mucosa in the proximal small intestine, but not digestive enzymes. [7]
- Most of the absorbed D-xylose is eliminated by the kidneys without being metabolized.
- Method
- After overnight fasting, 25 g of D-xylose is administered orally. [7]
- Urine is collected over 5 hours, and a venous blood sample is collected after 1 hour. [7]
-
↓ D-xylose levels (in urine and serum) indicates either: ; [7]
- Damage to the duodenal and/or jejunal mucosa (e.g., celiac disease, Whipple disease)
- Small intestine bacterial overgrowth
- Adequately elevated D-xylose levels suggest a different cause of malabsorption.
- Physiological background [7]
Further testing for underlying diseases
Obtain further testing based on clinical suspicion.
-
Hydrogen breath tests: to assess for malabsorption of individual carbohydrates (e.g., lactose malabsorption; , fructose malabsorption) or SIBO, e.g.:
- Glucose hydrogen breath test
- Lactulose breath test
- Serologic studies: : e.g., tTG IgA to assess for celiac disease
- Mesenteric angiography: if chronic mesenteric ischemia is suspected
Differential diagnoses
Differential diagnoses of malabsorption
| Common causes of malabsorption | ||||
|---|---|---|---|---|
| Condition | Epidemiology/risk factors | Characteristic clinical features | Diagnostics | |
| Intestinal | Extraintestinal | |||
| Ulcerative colitis |
|
|
|
|
| Crohn disease |
|
|
||
| Lactose intolerance |
|
|
|
|
| Celiac disease |
|
|
|
|
| Tropical sprue |
|
|
|
|
| Exocrine pancreatic insufficiency |
|
|
|
|
| Whipple disease |
|
|
|
|
The differential diagnoses listed here are not exhaustive.
Treatment
- Identify and treat the underlying disease.
- Optimize diet under specialist guidance based on the underlying disease, e.g.:
- Calorie- and protein-enriched diet
- Supplementation of fluid and nutrients, including vitamins and trace elements
- Specific dietary restrictions, e.g., gluten in celiac disease, dairy in lactose intolerance
- Total parenteral nutrition may be temporarily necessary in severe cases, e.g., after extensive intestinal resection or in intestinal failure
- Symptomatic treatment as needed, e.g., antidiarrheal agents
- Follow-up includes:
- Monitoring for nutritional deficiencies
- Monitoring for complications, e.g., intestinal failure, osteoporosis
Complications
- Intestinal failure
- Dehydration
- Complications of severe deficiencies, e.g.:
- Protein-energy malnutrition
- Osteoporosis
- Coagulopathy
- Peripheral neuropathy
- In children: failure to thrive
Protein-losing enteropathy [15]
- Definition: a condition characterized by massive loss of protein that can occur as a complication of several gastrointestinal disorders
-
Etiology
- Erosive or ulcerative conditions (e.g., Crohn disease, Clostridioides difficile infection)
- Increased intestinal permeability to proteins (e.g., celiac disease, SIBO)
- Impaired lymphatic circulation (e.g., intestinal lymphangiectasia, Whipple disease)
-
Clinical features
- Peripheral edema and effusions
- Nutritional deficiencies
- Infections
- Gastrointestinal symptoms (e.g., diarrhea, steatorrhea, abdominal pain, vomiting)
- Symptoms of the underlying disease
-
Diagnostics
- Nonselective hypoproteinemia: hypoalbuminemia and ↓ immunoglobulins
- Exclusion of alternative causes of hypoproteinemia, diarrhea, and/or malabsorption
- Diagnostic confirmation: ↑ 24-hour fecal alpha-1 antitrypsin [15]
- Additional diagnostics: Obtain as needed to determine the underlying cause and assess for complications.
-
Treatment
- Treatment of the underlying disease
-
Supportive care, e.g.:
- Correction of electrolyte abnormalities
- Vitamin and trace element supplementation
- Nutritional support
- Management of peripheral edema (e.g., with compression stockings)
- IVIg and antibiotic prophylaxis for patients with immunodeficiency and recurrent infections
We list the most important complications. The selection is not exhaustive.
References
- Owens SR, Greenson JK. "The pathology of malabsorption: current concepts". Histopathology. 50(1). :64-82. (2006)
- Schiller LR. "Evaluation of chronic diarrhea and irritable bowel syndrome with diarrhea in adults in the era of precision medicine". Am J Gastroenterol. 113(5). :660-669. (2018)
- Burgers K, Lindberg B, Bevis ZJ. "Chronic Diarrhea in Adults: Evaluation and Differential Diagnosis.". Am Fam Physician. 101(8). :472-480. (2020)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Sweetser S. "Evaluating the Patient With Diarrhea: A Case-Based Approach". Mayo Clinic Proceedings. 87(6). :596-602. (2012)
- Feuerstein JD, Cheifetz AS. "Crohn Disease: Epidemiology, Diagnosis, and Management". Mayo Clinic Proceedings. 92(7). :1088-1103. (2017)
- Rubin et al. "ACG Clinical Guideline: Ulcerative Colitis in Adults". Am J Gastroenterol. 114(3). :384-413. (2019)
- Dahlhamer JM, Zammitti EP, Ward BJ, Wheaton AG, Croft JB. "Prevalence of Inflammatory Bowel Disease Among Adults Aged ≥18 Years — United States, 2015". MMWR Morb Mortal Wkly Rep. 65(42). :1166–1169. (2016)
- Szilagyi A, Ishayek N. "Lactose Intolerance, Dairy Avoidance, and Treatment Options". Nutrients. 10(12). :1994. (2018)
- Catassi C, Gatti S, Lionetti E. "World Perspective and Celiac Disease Epidemiology". Dig Dis. 33(2). :141-146. (2015)
- Tack GJ, Verbeek WHM, Schreurs MWJ, Mulder CJJ. "The spectrum of celiac disease: epidemiology, clinical aspects and treatment". Nat Rev Gastroenterol Hepatol. 7(4). :204-213. (2010)
- Omer A, Quigley EMM. "Carbohydrate Maldigestion and Malabsorption". Clin Gastroenterol Hepatol. 16(8). :1197-1199. (2018)
- Forsmark CE. "Diagnosis and Management of Exocrine Pancreatic Insufficiency". Curr Treat Options Gastroenterol. 16(3). :306-315. (2018)
- Whitcomb DC, Buchner AM, Forsmark CE. "AGA Clinical Practice Update on the Epidemiology, Evaluation, and Management of Exocrine Pancreatic Insufficiency: Expert Review". Gastroenterology. 165(5). :1292-1301. (2023)
- Ozen A, Lenardo MJ. "Protein-Losing Enteropathy". N Engl J Med. 389(8). :733-748. (2023)
- Pazirandeh S, Burns DL. "Overview of vitamin A". UpToDate. UpToDate. https://www.uptodate.com/contents/overview-of-vitamin-a#H10. [2016-10-26]
- Ansstas G. "Vitamin A Deficiency". WebMD. http://emedicine.medscape.com/article/126004-clinical#b5. [2016-10-12]
- Drezner MK. "Patient education: Vitamin D deficiency (Beyond the Basics)". UpToDate. UpToDate. https://www.uptodate.com/contents/vitamin-d-deficiency-beyond-the-basics#H9. [2015-06-09]
- Pazirandeh S, Burns DL. "Overview of vitamin D". UpToDate. UpToDate. https://www.uptodate.com/contents/overview-of-vitamin-d?source=see_link#H9. [2016-01-15]
- Pazirandeh S, Burns DL. "Overview of vitamin E". UpToDate. UpToDate. https://www.uptodate.com/contents/overview-of-vitamin-e#H7. [2016-10-03]
- Pazirandeh S, Burns DL, Lipman TO, Motil KJ, Hoppin AG. "Overview of Vitamin K". UpToDate. UpToDate. https://www.uptodate.com/contents/overview-of-vitamin-k. [2016-04-13]
- Nguyen-Khoa D-T. "Beriberi (Thiamine Deficiency)". WebMD. http://emedicine.medscape.com/article/116930-overview#showall. [2016-07-01]
- Xiong GL. "Wernicke-Korsakoff Syndrome". WebMD. http://emedicine.medscape.com/article/288379-overview#showall. [2016-04-18]
- Gill RS. "Riboflavin Deficiency". WebMD. http://emedicine.medscape.com/article/125193-overview. [2016-08-09]
- Pazirandeh S, Burns DL. "Overview of water-soluble vitamins". UpToDate. UpToDate. https://www.uptodate.com/contents/overview-of-water-soluble-vitamins?source=search_result&search=niacin%20deficiency&selectedTitle=1~32. [2016-11-09]
- "Vitamin B5 (Pantothenic acid)". http://umm.edu/health/medical/altmed/supplement/vitamin-b5-pantothenic-acid. [2013-07-16]
- Frye RE. "Pyridoxine Deficiency". WebMD. http://emedicine.medscape.com/article/124947-overview#a4. [2016-09-15]
- Schick P. "Megaloblastic Anemia". WebMD. http://emedicine.medscape.com/article/204066-overview#a1. [2016-10-29]
- Schrier SL. "Clinical Manifestations and Diagnosis of Vitamin B12 and Folate Deficiency". UpToDate. UpToDate. https://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-vitamin-b12-and-folate-deficiency. [2016-07-15]