Summary
Malaria is a potentially life‑threatening tropical infectious disease caused by Plasmodium parasites, which are transmitted through the bite of an infected female Anopheles mosquito. The disease is endemic in tropical and subtropical areas of Africa, Asia, and the Americas. Malaria has an incubation period of 7–30 days and may manifest with nonspecific symptoms like fever, nausea, and vomiting. Diagnosis can therefore be challenging. The gold standard for diagnosing malaria is identification of parasites in RBCs on a blood smear, although rapid diagnostic tests to identify Plasmodium antigens are used with increasing frequency. Malaria is classified as either severe or uncomplicated. Severe malaria is characterized by severe organ dysfunction; affected individuals should be admitted to the ICU and receive IV antimalarials immediately. Uncomplicated malaria can be treated with oral antimalarials. Preventative measures for malaria in travelers to endemic areas include chemoprophylaxis with antimalarial medications and efforts to prevent the bite of the Anopheles mosquito (e.g., mosquito nets, repellents, protective clothing). Malaria is a reportable disease and should be suspected in all patients with fever and a history of travel to an endemic region.
Epidemiology
-
Distribution [1]
- Most cases of malaria occur in tropical Africa (West and Central Africa).
- Transmission also occurs in other tropical and subtropical regions such as South and Southeast Asia, and Central and South America


Epidemiological data refers to the US, unless otherwise specified.

© AMBOSS
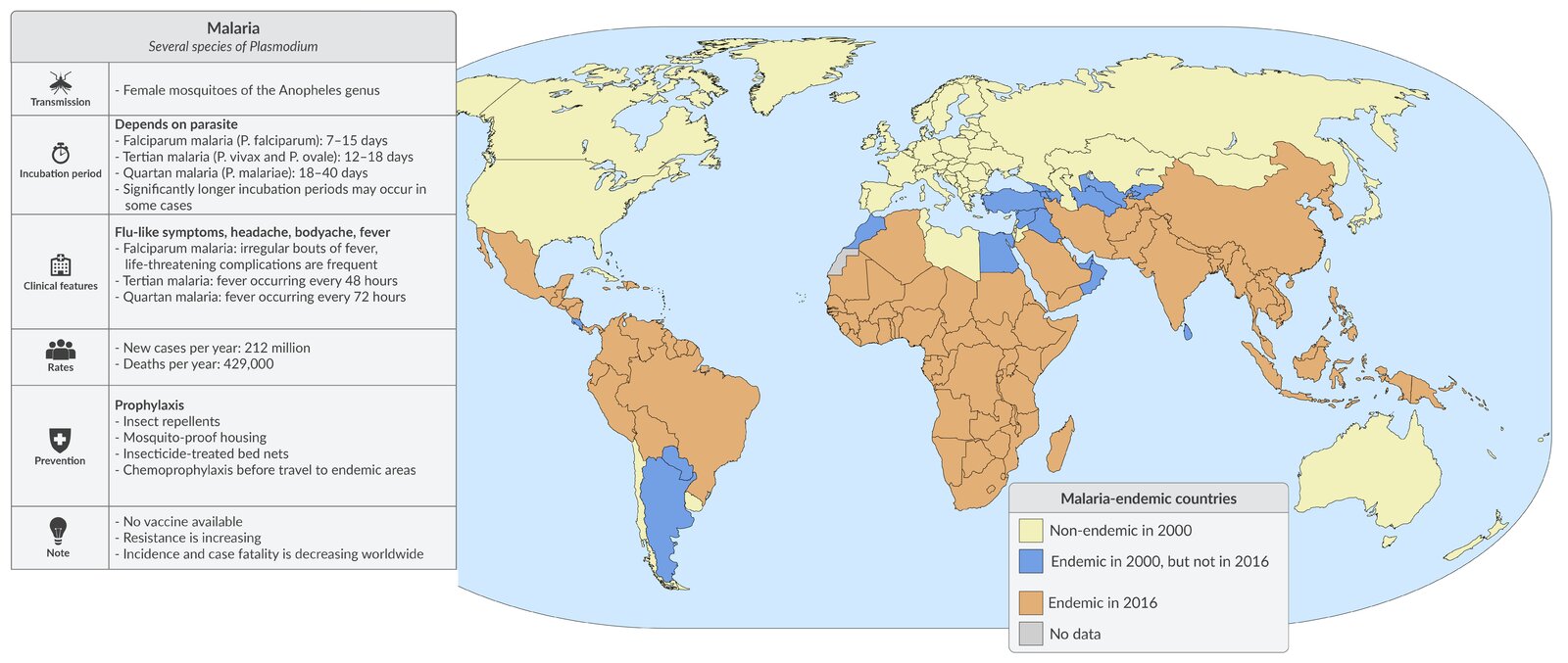
© AMBOSS. Data taken from WHO World Malaria Report 2016.
Etiology
-
Pathogen: Plasmodia
- Eukaryotic parasites (belonging to the Sporozoa group)
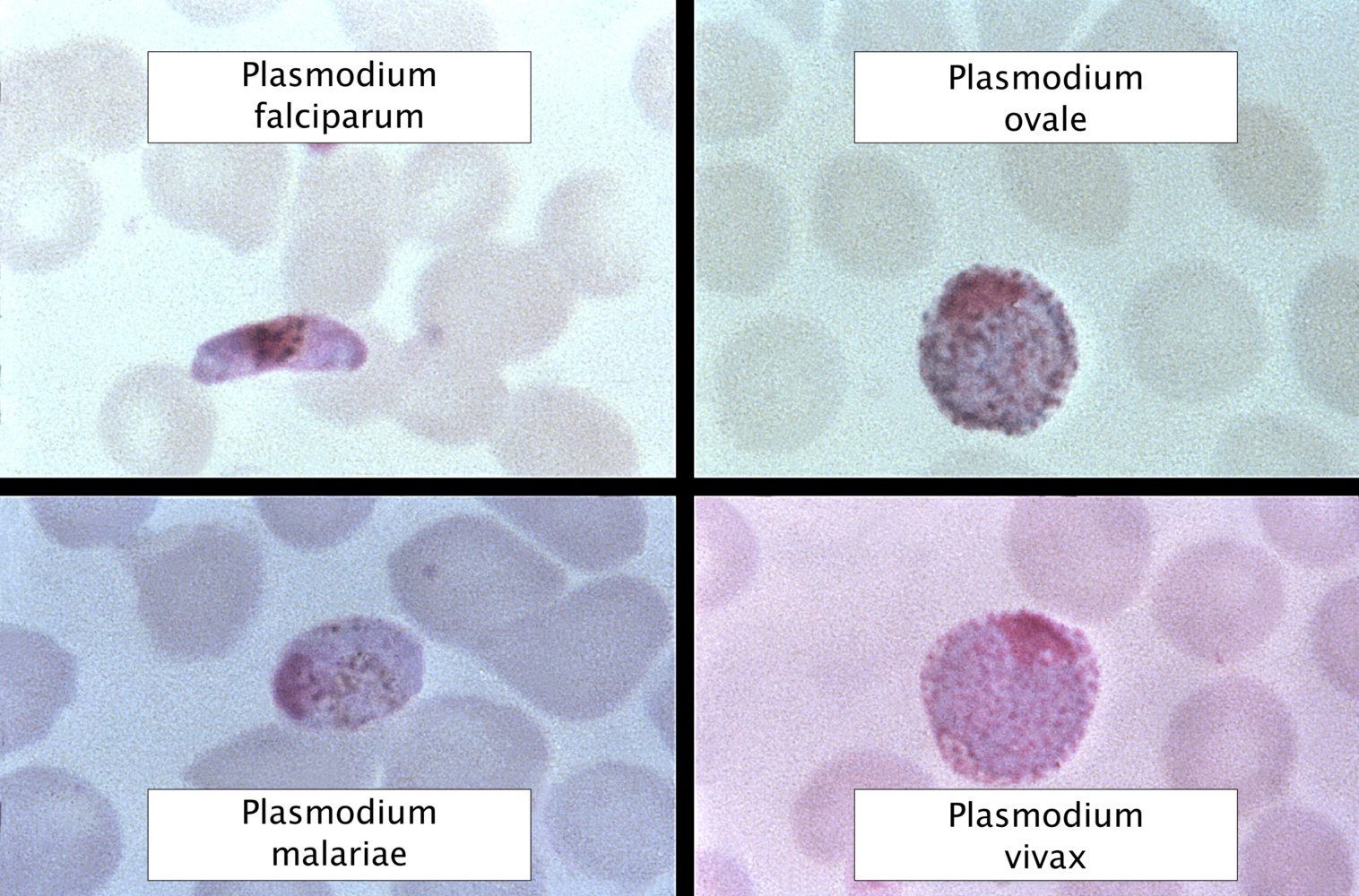
- Species that affect humans [2][3][4][5]
- Plasmodium falciparum; : most virulent and causes the most severe disease, i.e., falciparum malaria; dominant in Africa
- Plasmodium vivax: the most common of the less virulent species and causes milder disease; dominant in endemic areas outside Subsaharan Africa (e.g., Southeast Asia)
- Plasmodium ovale; and Plasmodium malariae: less common and cause milder disease [4]
- Plasmodium knowlesi: found in Southeast Asia and can cause severe malaria; possibly zoonotic and often misidentified as other species due to morphological similarities. [6]
- Vector: the female Anopheles mosquito
- Host: humans
-
Partial resistance against malaria [7]
- Carriers of sickle‑cell mutation
- Individuals with either certain Duffy antigens or no Duffy antigens are resistant to P. vivax and P. knowlesi [8]
- Other hemoglobinopathies (e.g., thalassemia, HbC)
- Infection with malaria subsequently leads to the development of specific Plasmodium antibodies that result in partial immunity for a limited amount of time (less than a year)
| Classic disease and fever patterns of different plasmodium species [9][10]. | ||
|---|---|---|
| Different species of plasmodium [11][12] | Disease | Fever spikes |
| P. vivax P. ovale |
|
|
| P. malariae |
|
|
| P. falciparum |
|
|
| P. knowlesi |
|
|


A female Anopheles mosquito (Anopheles gambiae) sucking blood from the photographer's hand using its proboscis. The mosquito's abdomen is already filled and expanded to the extent that one drop of blood is directly excreted. At the start of the blood meal, the mosquito injects saliva that contains anticoagulation agents and, in some cases, sporozoites (infectious form of the malaria parasite).
Source: "ID#: 17696", CDC/ James Gathany, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
Pathophysiology
Life cycle of Plasmodium (simplified) [13]
")
Asexual development in humans
- Transmission of Plasmodium sporozoites via Anopheles mosquito bite → sporozoites travel through the bloodstream to the liver of the host
- Liver: sporozoites enter hepatocytes → sporozoites multiply asexually → schizonts are formed containing thousands of merozoites → release of merozoites into the bloodstream
-
Circulatory system (two possible outcomes)
- Merozoites enter erythrocytes → maturation to trophozoites → red cell schizonts are formed containing thousands of merozoites → release of merozoites into the bloodstream (which causes fever and other manifestations of malaria) → penetration of erythrocytes recurs
- Merozoites enter erythrocytes → differentiation into gametocytes (male or female)
Sexual development in female Anopheles mosquito
- A mosquito bites an infected human and ingests gametocytes → gametocytes mature within the mosquito intestines → sporozoites are formed and these migrate to the salivary glands → transmission of sporozoites to humans via mosquito bite
- See also “Developmental stages of Plasmodium in RBCs.”
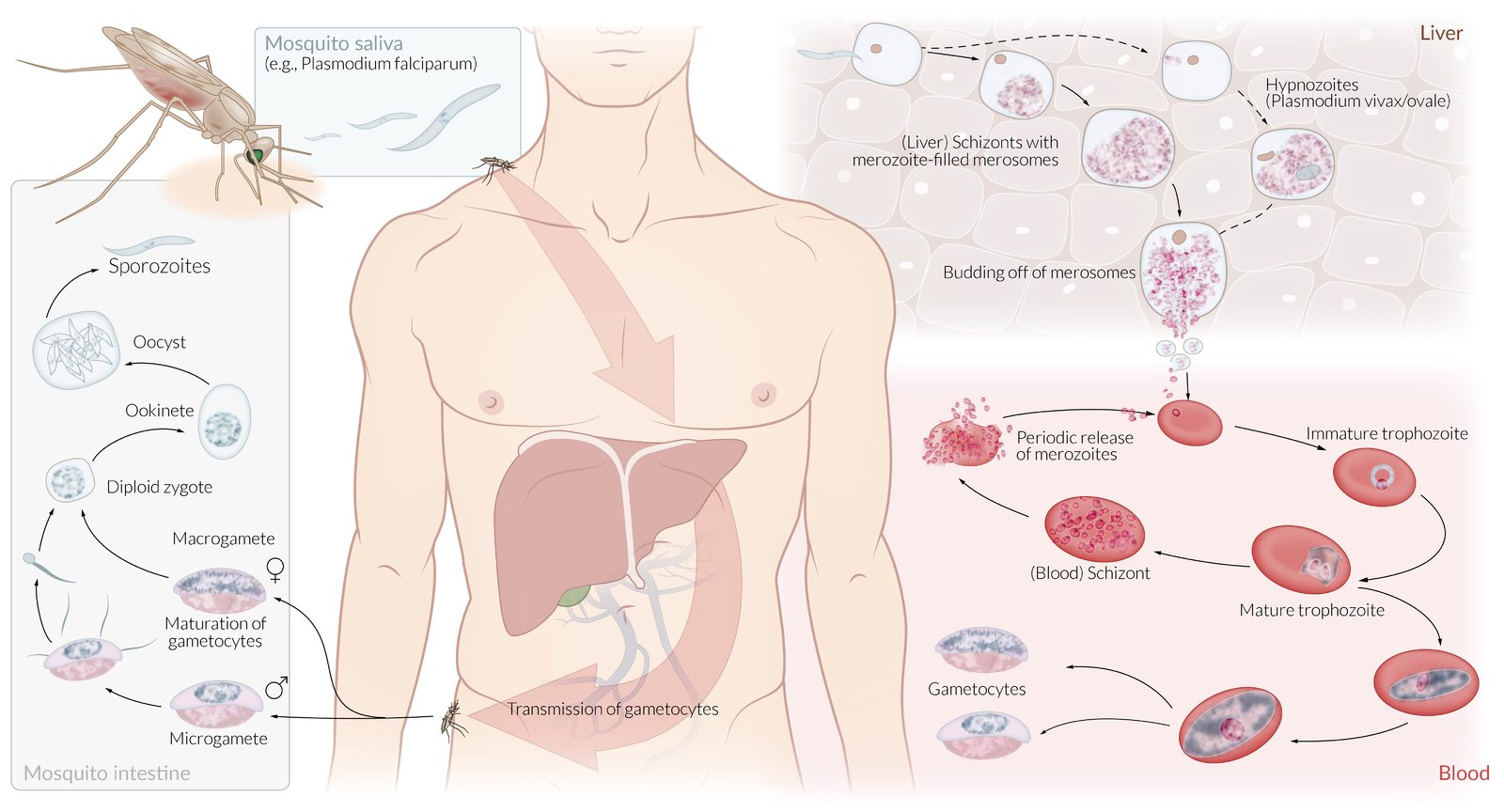
Malaria is caused by plasmodia transmitted via the saliva of female Anopheles mosquitoes. During development, there is a generational (asexual/sexual reproduction) and host change (between mosquito and human).
Human host
Liver (exoerythrocytic) stage: Following a bite from an infected mosquito, sporozoites (spindle-shaped, infective pathogen) reach the liver via the blood or lymphatic system and mature into schizonts within the hepatocyte. Asexual propagation produces thousands of daughter cells (merozoites), which are transmitted to the bloodstream via merosomes. Plasmodium Vivax and Ovale are associated with the development of dormant stages (hypnozoites) which persist for several years in hepatocytes and later develop into schizonts.
Blood (erythrocytic) stage: Merozoites infect erythrocytes and develop into trophozoites, which then mature into schizonts. Asexual propagation produces merozoites, which are then released into the bloodstream via merosomes. This cycle repeats itself over a course of 48-72 hours causing periodic decay of erythrocytes and the resulting pathognomic spiking fevers of malaria.
Mosquito host
Ingested gametocytes mature into flagellated microgametes (♂) or macrogametes (♀) within the gastrointestinal tract of the mosquito. The mature sexual forms merge into a mobile zygote, which in turn develops into a sporozoite-containing oocyst. The sporozoites are released, enter the salivary glands, and may eventually be transferred to a new host.
© AMBOSS
Clinical features
Incubation period
- 7–30 days [14]
The incubation period of malaria is a minimum of seven days; if fever occurs before the seventh day following exposure in an endemic region, it is most likely not due to malaria.
Course
-
Infection → asymptomatic parasitemia → uncomplicated illness → severe malaria → death
- Asymptomatic parasitemia: Especially in endemic regions, cases of asymptomatic plasmodia carriers are reported. [15]
- Infections with P. vivax, P. ovale, and P. malariae typically have milder symptoms; , involve fewer organs (CNS or gastrointestinal symptoms are rare), and have a markedly lower risk of causing severe malaria. [16]
- Following the successful treatment of tertian malaria, dormant P. ovale or P. vivax forms (hypnozoites) may remain in the liver and can cause relapse after months or even years. [16]
General symptoms [1][14]
- Flu‑like symptoms, headache
- Diaphoresis
-
High fever: Fever spikes occurring at regular intervals are no longer commonly observed. ; [9][10]
- Tertian malaria: periodic fever spikes every 48 hrs
- Quartan malaria: periodic fever spikes every 72 hrs
- Malignant tertian malaria (associated with falciparum malaria): irregular fever spikes without a noticeable rhythm
Organ-specific symptoms [1][14]
-
Blood
- Thrombocytopenia: increased bleeding risk
- Hemolytic anemia: weakness, paleness, dizziness
-
Gastrointestinal
- Nausea, vomiting
- Diarrhea, abdominal pain
- Liver: : hepatosplenomegaly, discrete jaundice
- Renal: flank pain, oliguria, hemoglobinuria
- Cardiac: heart failure
- CNS: hallucinations, confusion, impaired consciousness, seizures, coma
Impaired consciousness, shock, and abnormal bleeding are signs of severe malaria that requires immediate IV treatment. [17]


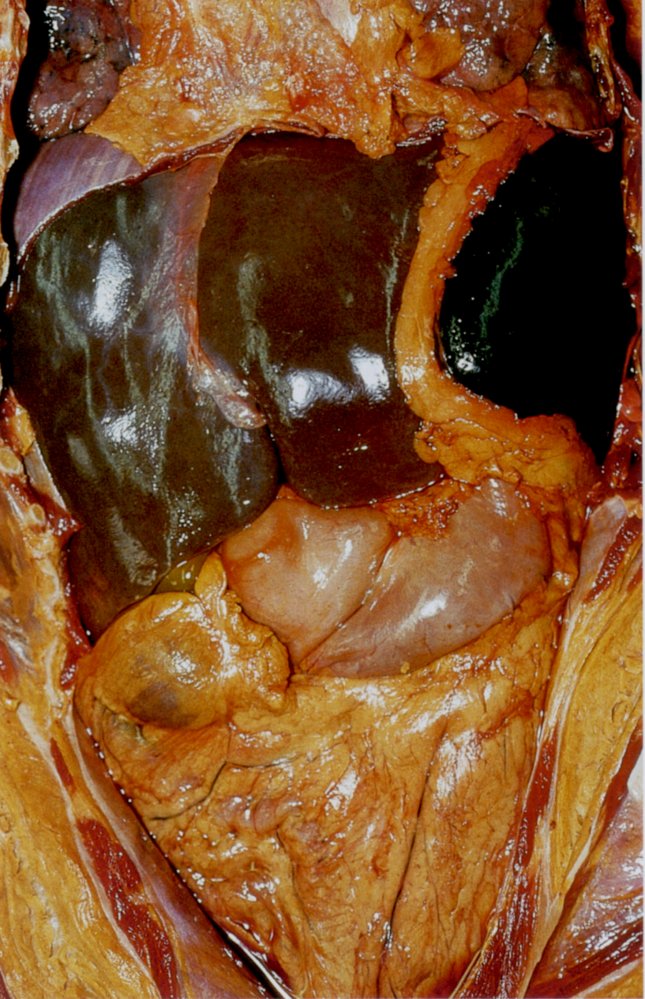
Malaria may lead to an enlarged liver and spleen (hepatosplenomegaly), as seen in the image.
Source: © IMPP

Pathological finding in the cerebrum of a patient with lethal malaria infection: The gray matter of the brain appears slightly pink, because infected erythrocytes clog small blood vessels, leading to stasis. In the area of the posterior horn, the white matter is dotted by petechiae (circles).
Source: © IMPP
Diagnosis
Approach
-
Focused clinical evaluation [18][19][20][21]
- Time of travel to regions where malaria is endemic and previous chemoprophylaxis
- Evaluate for signs of severe malaria.
- Routine laboratory studies: CBC, CMP, LFTs, and coagulation panel to evaluate for organ dysfunction [17]
-
Parasitological testing: confirms the presence and determines the species of Plasmodia
- Microscopic examination of thick and thin blood smears (gold standard) [19]
- Antigen detection test (more rapid but less sensitive) [19]
Malaria can present in many different ways and is therefore often misdiagnosed. In patients with fever who have recently traveled to endemic regions, malaria must always be considered. [22]
Routine laboratory studies [21]
Used to assess the severity of malaria and identify concurrent diseases, see also “Criteria for severe malaria.”
-
CBC: Changes in multiple parameters may occur. [23]
- Hemolytic anemia: ↓ Hb, ↓ haptoglobin, ↑ LDH, ↑ indirect bilirubin, ↑ reticulocytes
- Thrombocytopenia
- Leukocytosis or leukopenia are uncommon except in severe disease.
- CMP: Hypoglycemia and AKI can occur in severe malaria. [17]
- Urinalysis: Hemoglobinuria may occur with intravascular hemolysis. [16][17]
- Other (as clinically indicated): ABG , type and screen , blood and urine cultures CSF analysis [19][24]
Parasitological testing for malaria [16][19][25]
False-negative test results can occur with RDTs and blood smears, especially when malaria parasitemia is low. Repeat parasitological testing when clinical suspicion is high. [21][25][26]
Rapid diagnostic tests (RDTs)
- Detects specific malaria antigens (e.g., HRP2, pLDH, aldolase) [19][25]
- Allows for quick diagnosis if high‑quality microscopy is unavailable or delayed. [25]
- Confirm all RDT results via microscopy when available. [22][25]
RDTs can detect P. falciparum but typically cannot distinguish between other species of Plasmodium. [22]
Blood smear
Gold standard test: allows for visualization of parasites within RBCs via microscopy to confirm malaria diagnosis [22]
- Thick blood smear: high sensitivity; best initial test [10][19]
-
Thin blood smear: lower sensitivity, high specificity; confirmatory test [27]
- Allows identification of Plasmodium species [19]
- Enables calculation of malaria parasitemia: the percentage of RBCs containing a Plasmodium organism; used to classify severity and monitor response to therapy. [16][17]
- Findings include:
- Schuffner granules (fine, brick-red dots) within RBCs infected with P. vivax and P. ovale [10]
- Crescent-shaped gametocytes in individuals infected with P. falciparum
-
Evaluation of a negative blood smear [16]
- Patients may become symptomatic before parasites can be seen on the blood smear.
- If an initial test result is negative, blood smears should be repeated every 12–24 hours for a total of 3 tests.
- If all three sets are negative, malaria can be excluded as the diagnosis.
A single negative blood smear does not rule out malaria. Repeat three sets of blood smears (one set every 12–24 hours) before ruling out the diagnosis. [16][22]
| Developmental stages of Plasmodium in RBCs [13] | ||
|---|---|---|
| All Plasmodium spp. | Plasmodium falciparum | |
| Immature trophozoite |
|
|
| Mature trophozoite |
|
|
| Immature schizont |
|
|
| Mature schizont |
|
|
| Gametocytes |
|
|
")


")
")
")


Other studies
-
PCR [25][28]
- Identifies species of Plasmodium; useful for suspected P. knowlesi infection
- High sensitivity but expensive and usually only available at reference laboratories
-
Serological testing
- Positive serological results indicate prior exposure to Plasmodium. [16]
- Not recommended in acute malaria due to length of time for antibodies to reach detectable levels [25]
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: Prof. Dr. Karl-Anton Kreuzer, Facharzt für Innere Medizin, Hämatologie und Onkologie
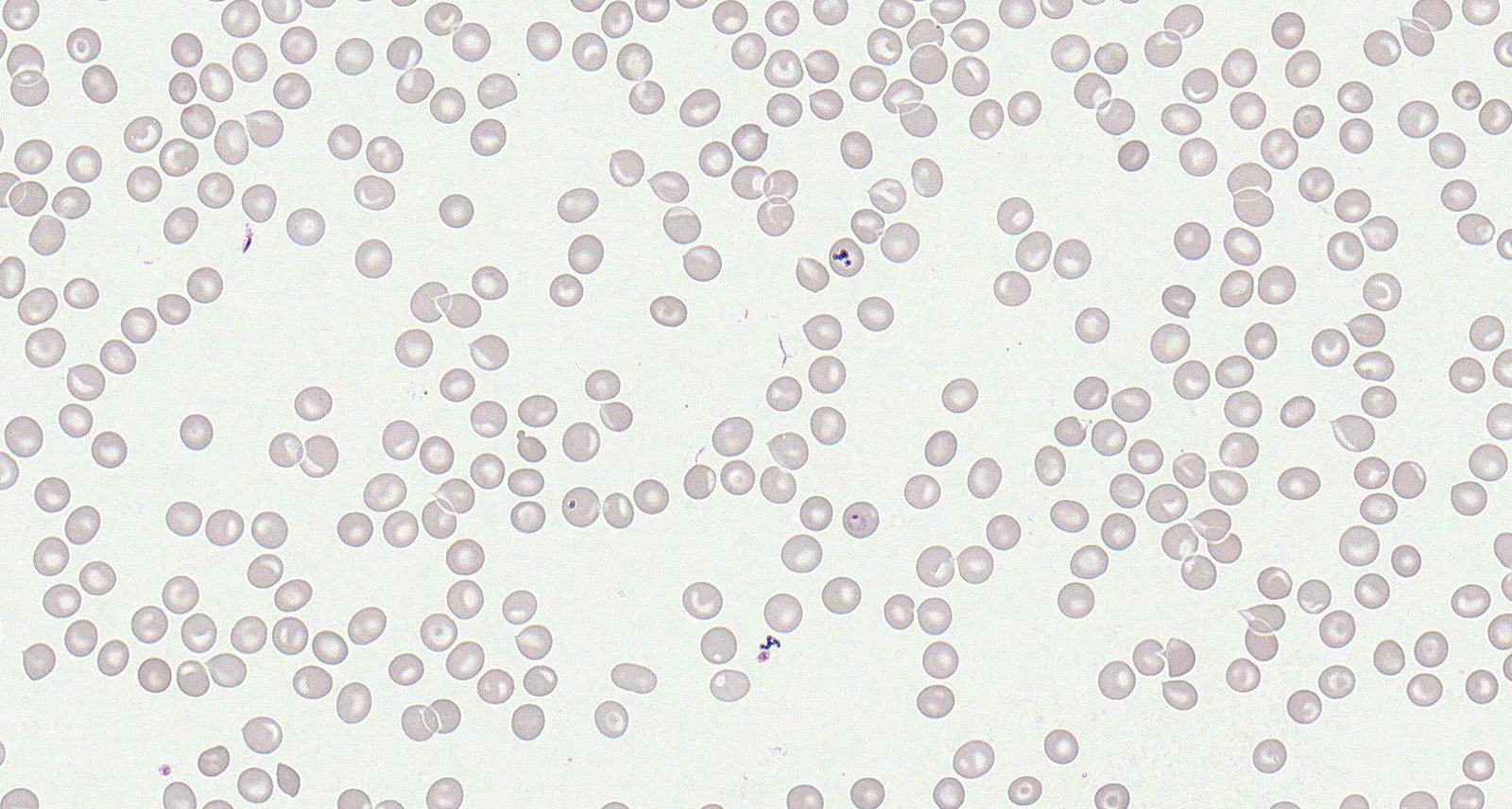
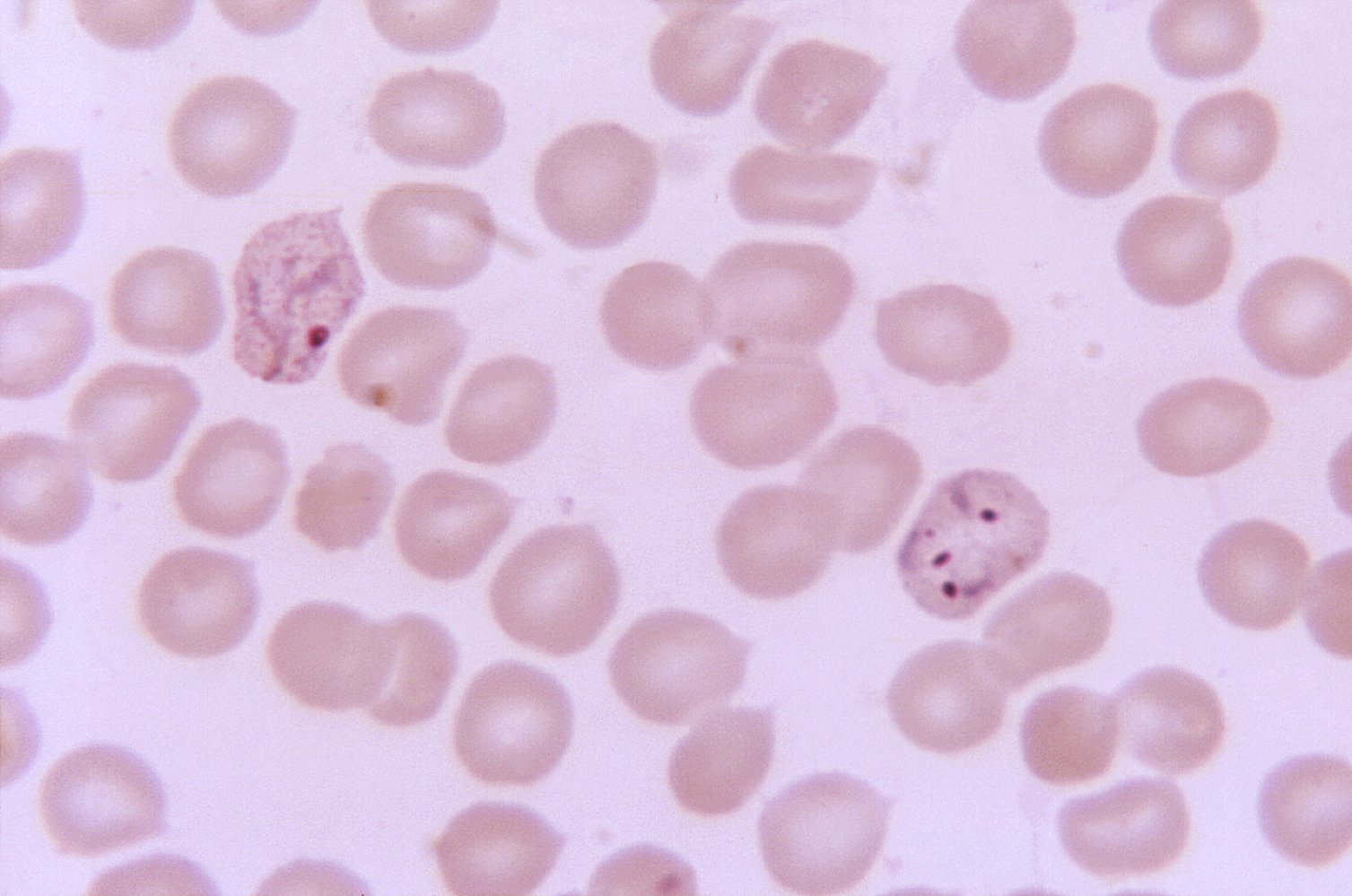
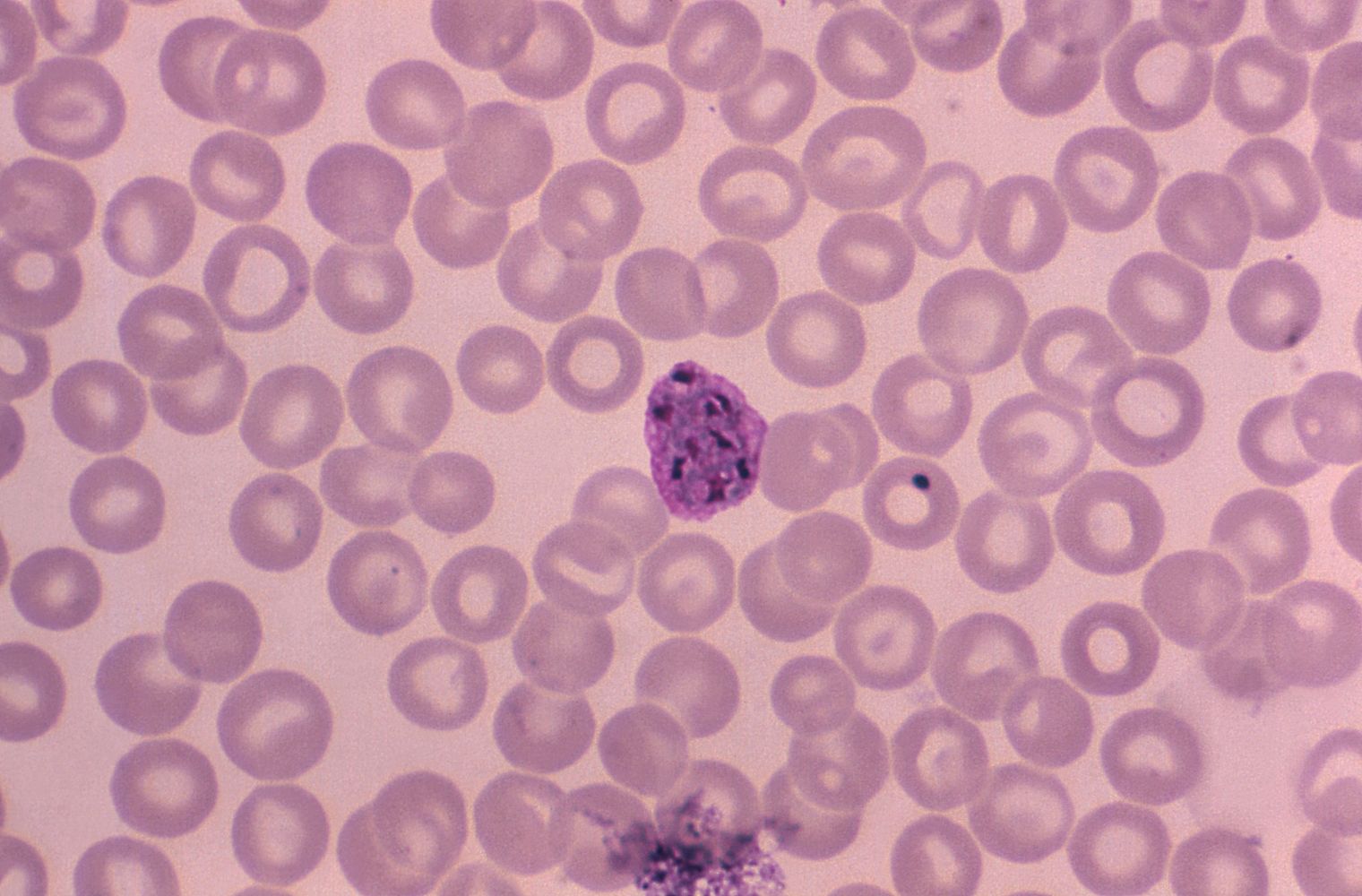
Red blood cell inclusions in a patient with malaria
A large ring-like inclusion within erythrocyte in the center of the slide is an immature trophozoite. Thick, dark purple, ring‑shaped inclusions and fine dotting within erythrocytes (i.e., "Schüffner granules") are characteristic of infection with Plasmodium vivax or P. ovale.
Source: © IMPP
Compared to other forms of malaria, trophozoites of falciparum malaria are characterized by smaller and finer ring-shaped inclusions (green overlay). Plasmodium falciparum invades many erythrocytes, and one erythrocyte is typically invaded by more than one plasmodium, which is not the case in other forms of malaria.
Source: © IMPP
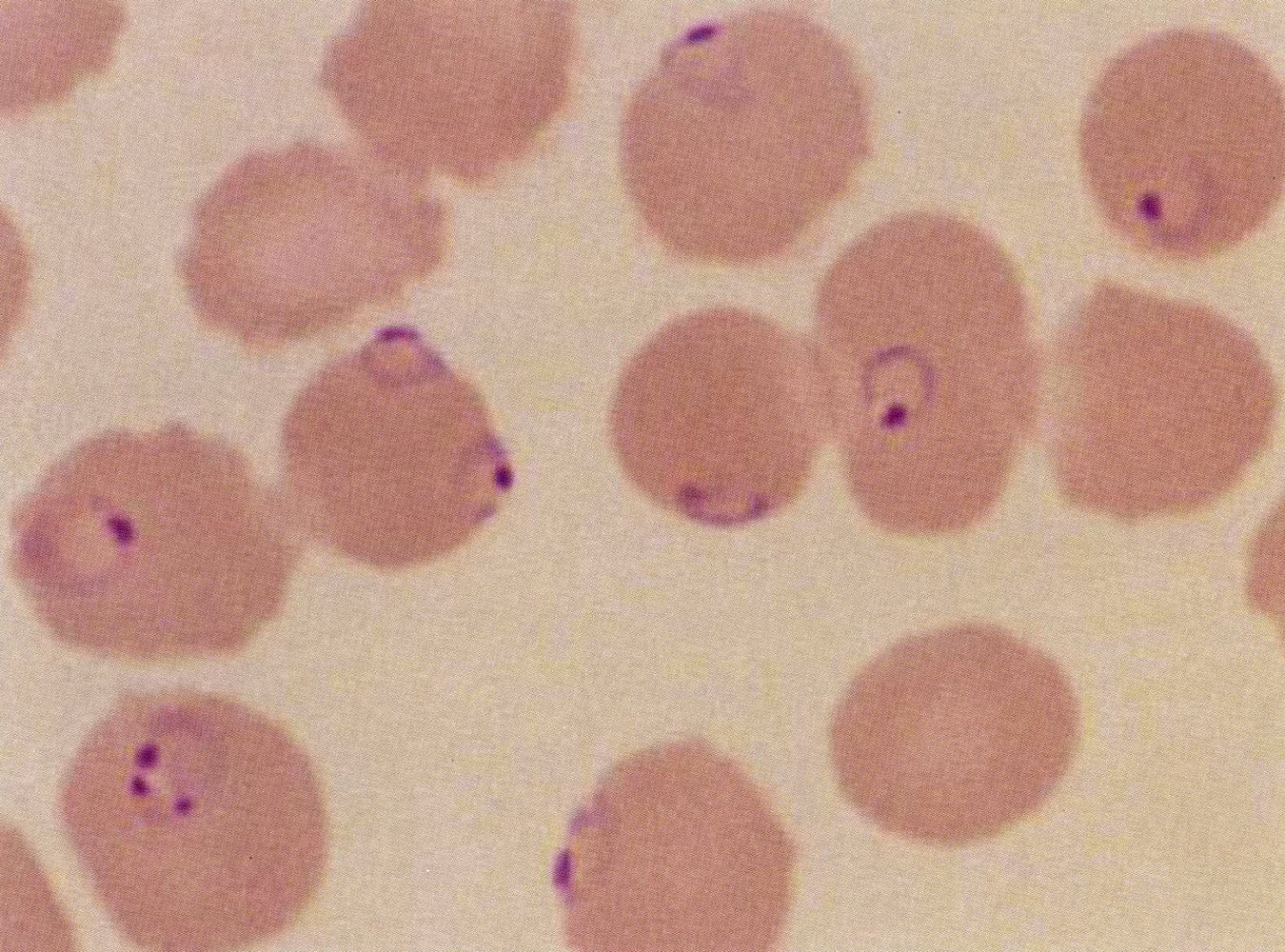
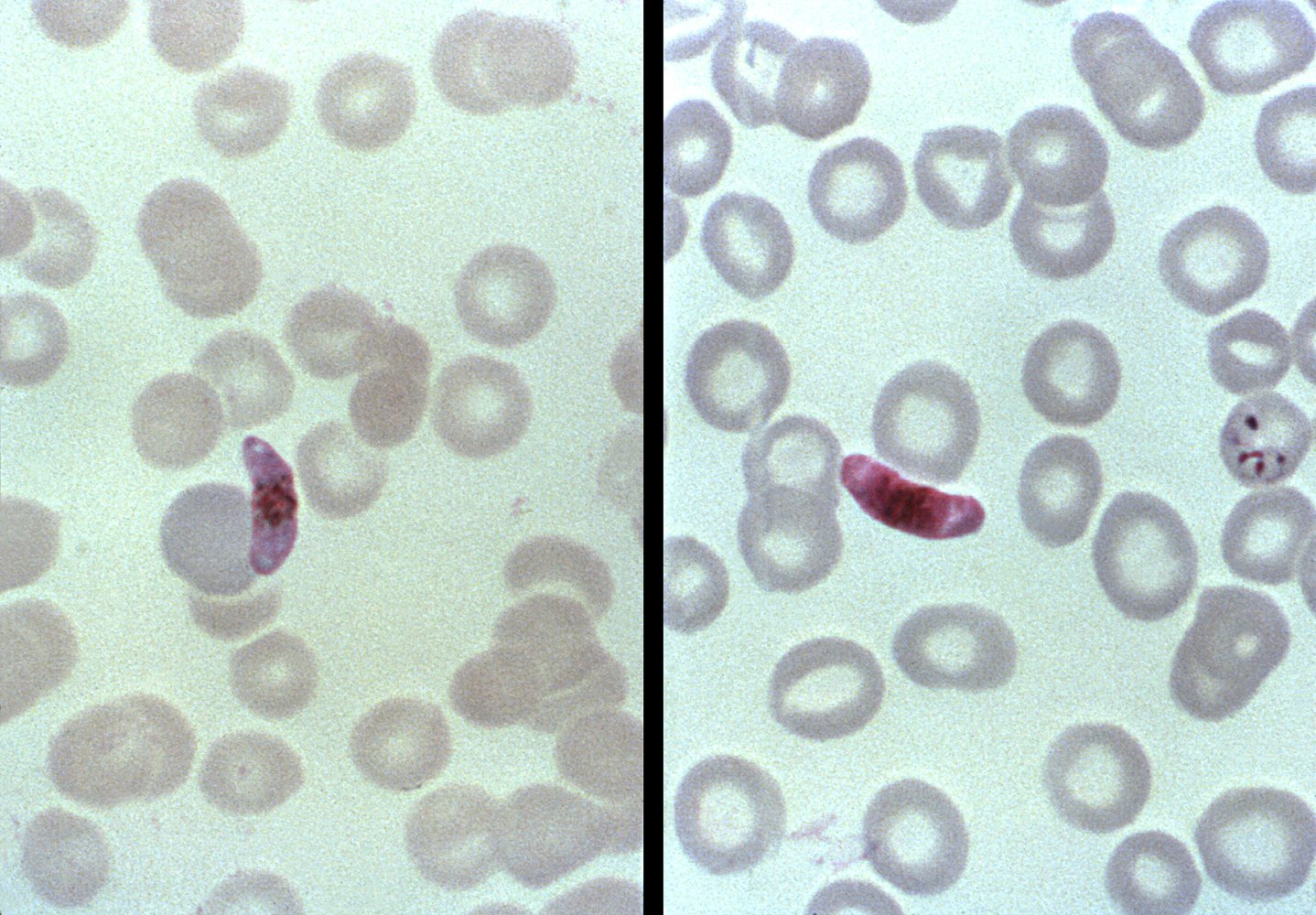
Blood smear showing two trophozoites of Plasmodium vivax. The left trophozoite contains ameboid rings (green overlay), which are a sign of maturity. In contrast, the right trophozoite has three smaller, irregular rings, a sign of immaturity.
Source: "ID#: 12088", CDC/ Dr. Mae Melvin, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
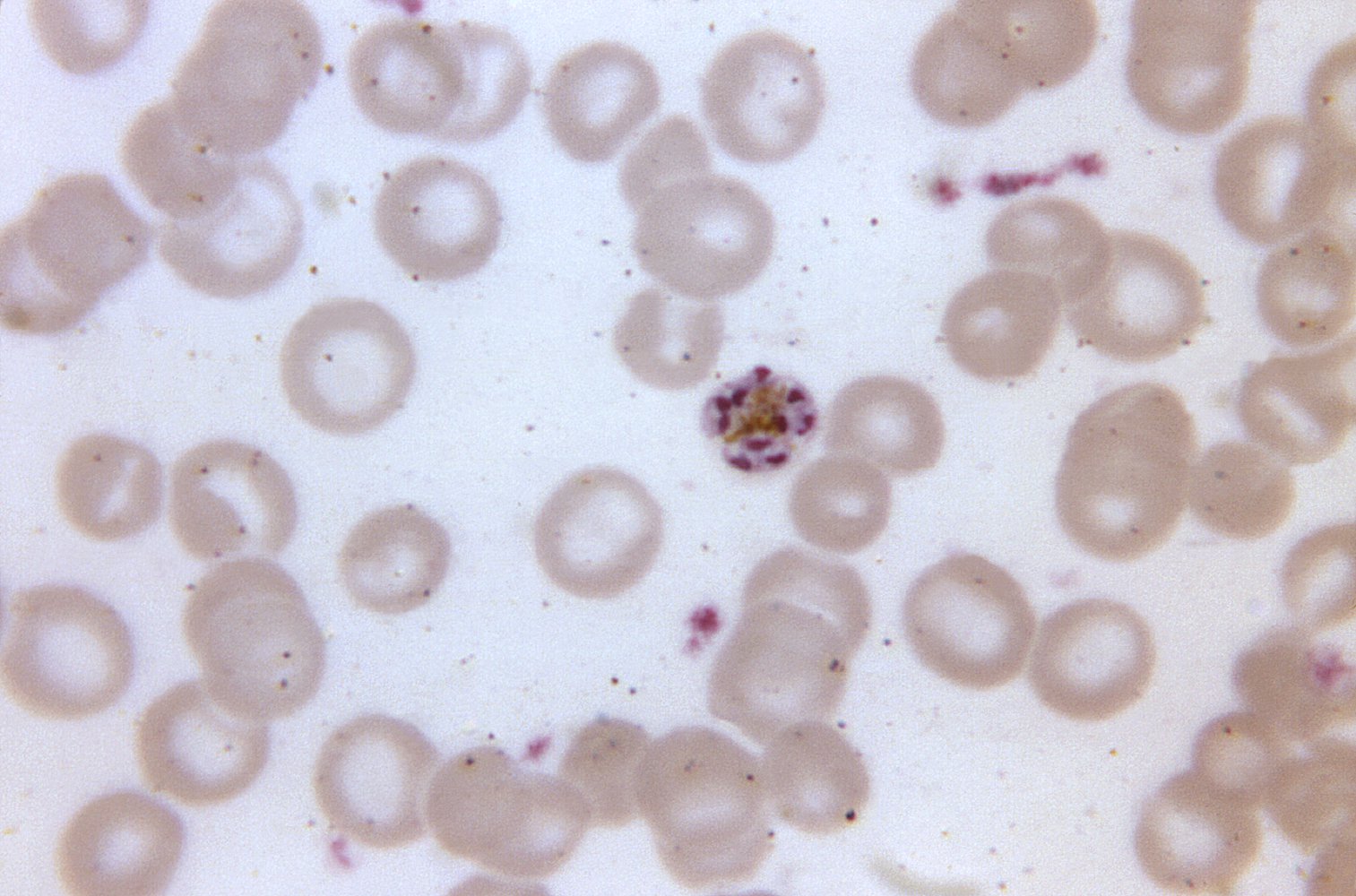
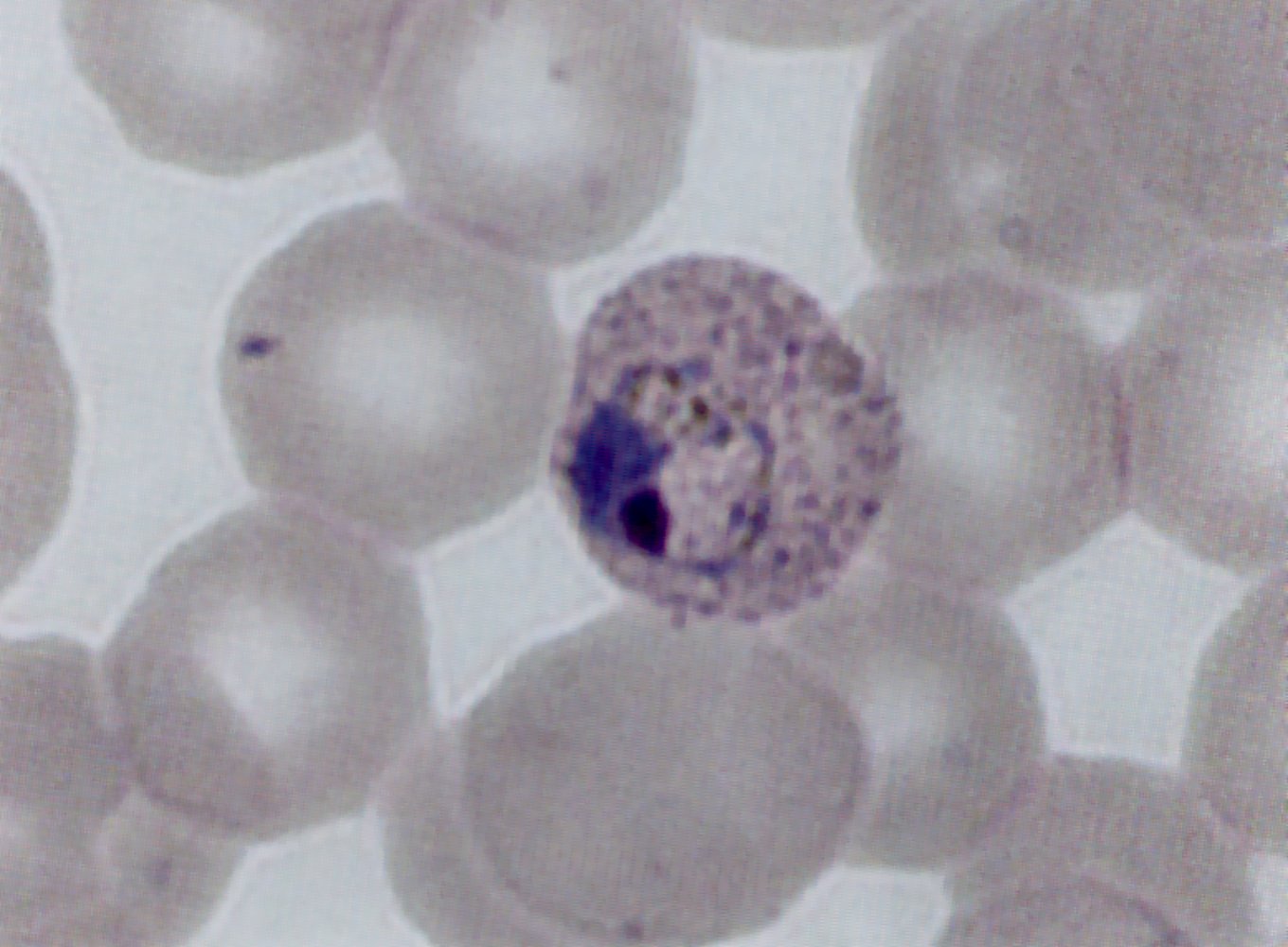
Thin blood smear showing a mature schizont of Plasmodium malariae. A conglomerate of merozoites (red overlay) is organized around the brownish pigment in the center, which is called the rosette. Within the red cell schizont, merozoites replicate asexually every 48–72 hours, depending on the type of Plasmodium. Increased parasite burden causes the infected erythrocytes to burst. A subsequent release of proinflammatory factors results in a fever spike. Merozoites, which have been set free from the erythrocyte, enter other erythrocytes to replicate again.
Source: "ID#: 12102", CDC/ Dr. Mae Melvin, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
Giemsa-stained blood smear showing erythrocytes of a patient infected with Plasmodium vivax. In the middle, there is a red cell schizont (green overlay), which is an erythrocyte containing many merozoites (yellow overlay). Within the red cell schizont, merozoites replicate asexually every 48–72 hours, depending on the type of Plasmodium. The increased parasite burden causes the infected erythrocytes to burst. A subsequent release of proinflammatory factors results in a fever spike. Merozoites, which have been set free from the erythrocyte, enter other erythrocytes in order to replicate again.
Source: "ID#: 14674", CDC/ Dr. Mae Melvin, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
Blood smears illustrating the morphological differences between the female sexual form (e.g., macrogametocytes) of different types of Plasmodium. Macrogametocytes of P. ovale, vivax, and malariae have an oval to round shape, eccentric, compact chromatin, and scattered brown pigment (hemozoin). However, macrogametocytes of P. falciparum are different: They have a crescent shape with a central nucleus surrounded by dark pigment.
Source: "ID#: 5942", CDC/ Steven Glenn, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
The Giemsa-stained left thin blood smear on the left shows a microgametocyte of P. falciparum. It exhibits the characteristic crescent shape. While shaped similarly, the macrogametocyte on the right is darker compared to the microgametocyte.
A gametocyte is the mature form of Plasmodium capable of sexual reproduction. To reproduce, the gametocytes must leave the human host and commence the sexual stage of their life cycle within the mosquito.
Source: "ID#: 5941", CDC/ Steven Glenn, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
Classification
Uncomplicated malaria
- Definition: symptomatic, diagnostically proven malaria without features of severe malaria [21][22]
- Etiology: can be caused by all Plasmodium species
- Treatment: See “Treatment of uncomplicated malaria.”
Severe malaria (complicated malaria) [14][17][19]
- Description: potentially fatal manifestation or complication of malaria
- Etiology: most commonly a result of falciparum malaria
- Pathophysiology: Infected erythrocytes occlude capillaries, which can lead to severe organ dysfunction.
-
Criteria for severe malaria: ≥ 1 of the following in a patient with proven malaria [16][29]
- Clinical findings
- General: prostration
- CNS: seizures (> 2 convulsions in 24 hours), impaired consciousness [29]
- Cardiovascular: shock (e.g., hypotension, capillary refill time ≥ 3 seconds)
- Pulmonary: respiratory distress, pulmonary edema
- Gastrointestinal: jaundice
- Hematologic: significant bleeding
- Laboratory findings
- Severe anemia: < 7 g/dL in adults, ≤ 5 g/dL in children [29]
- Hypoglycemia: < 40 mg/dL
- Acidosis: base deficit > 8 mEq/L, bicarbonate < 15 mEq/L, or lactate ≥ 5 mEq/L
- Acute kidney injury: creatinine > 3 mg/dL or urea > 56 mg/dL
- Hyperbilirubinemia: bilirubin > 3 mg/dL
- High malaria parasitemia [16][29]
- Clinical findings
- Treatment: See “Treatment of severe malaria.”
Treatment
See “Special patient groups” for management of malaria in children and pregnant individuals.
Approach [16][19][21][22]
- Consult infectious disease service early.
- Check for criteria for severe malaria.
- Treat severe malaria immediately with IV artesunate, following ABCDE approach.
- Treat uncomplicated malaria based on species, resistance patterns, and degree of chemoprophylaxis.
- Determine disposition
- Severe malaria: ICU admission and supportive care
- Uncomplicated malaria: Consider admission for observation and serial monitoring of parasite count.
- Report all confirmed malaria to public health authorities.
Treatment of severe malaria [16][19][21]
-
Pharmacotherapy
- Start IV artesunate immediately. [10][16][21]
- Repeat malaria parasite density after 3rd dose of artesunate.
- > 1%: Continue IV artesunate
-
≤ 1%: Switch to oral antimalarials under specialist guidance
- Artemether-lumefantrine (preferred)
- OR atovaquone-proguanil
- OR quinidine (in the US; quinine elsewhere)
-
Supportive care and monitoring
- Manage fever with acetaminophen, tepid sponging, and/or cooling blankets.
- Treat acute seizures, e.g., with IV or rectal diazepam
- Avoid aggressive fluid replacement and rapid fluid boluses.
- Rule out superadded bacterial infection: Perform fever workup, e.g., blood cultures. [21]
- Prevent hypoglycemia: Check blood glucose every 4 hours. [21]
- Monitor Hb every 6–12 hours and renal function daily. [9]
- Measure malaria parasitemia on days 7 and 28 to monitor response to therapy. [25]
- Disposition: Admit to ICU.
The CDC recommends contacting their Malaria Hotline for all patients with severe malaria. [16]
Severe malaria is a medical emergency; without appropriate treatment, mortality is nearly 100%. [21]
Treatment of uncomplicated malaria [16][19][21]
-
Agent selection based on: [16]
- Infecting Plasmodium species
- Prior use of chemoprophylaxis
- Likelihood of chloroquine-resistance
- See “Overview of treatment of uncomplicated malaria.”
-
Additional considerations in P. vivax and P. ovale [16]
- Check G6PD activity levels.
- Give primaquine or tafenoquine to eradicate hypnozoites dormant in hepatocytes.
-
Disposition: Consider admission for observation and serial monitoring of parasite concentration. [16][19]
- P. falciparum or P. knowlesi infections: Patients are typically hospitalized.
- P. vivax, P.ovale, P. malariae infections: Patients who tolerate PO medicine may receive outpatient treatment. [22]
| Overview of treatment of uncomplicated malaria in adults [30] | ||
|---|---|---|
| Plasmodium species | Acquired area | Treatment |
| P. vivax, P. ovale (tertian malaria) | No chloroquine resistance |
|
| With chloroquine resistance |
|
|
| Uncomplicated falciparum malaria | No chloroquine resistance |
|
| With chloroquine resistance |
|
|
| P. malariae, P. knowlesi (quartan malaria) [16] |
|
|
Do not use medications that the patient has already used for chemoprophylaxis. [16]
Plasmodium falciparum and, more recently, Plasmodium vivax are becoming increasingly resistant to chloroquine.
Antimalarial medications
Overview of antimalarial drugs
| Indications and pharmacology of antimalarial medication | ||||
|---|---|---|---|---|
| Agents | Indications | Mechanism of action | Most common adverse effects [31][32][33][34] | |
| Chloroquine |
|
|
|
|
| Hydroxychloroquine |
|
|||
| Doxycycline/ tetracycline |
|
|
|
|
| Mefloquine |
|
|
||
| Quinine |
|
|
|
|
| Artemether-lumefantrine |
|
|||
| Atovaquone-proguanil |
|
|
|
|
| Quinidine |
|
|
|
|
| Artesunate |
|
|
||
| Primaquine |
|
|
|
|
Mefloquine should not be prescribed for malaria prophylaxis in patients with a history of seizures, active or recent depression, generalized anxiety disorder, psychosis, schizophrenia, or other major psychiatric disorders, due to the risk of severe neuropsychiatric side effects.



The skin on the dorsum of the hands shows a blistering rash with areas of secondary scarring. The scarred lesions mostly appear white-grayish, a few erythematous erosions can also be seen.
These findings are characteristic of porphyria cutanea tarda and usually occur on sun-exposed skin.
Source: “Figure 7, in: Photosensitive disorders in HIV” by Karen Koch, AOSIS, licensed under CC BY 4.0.
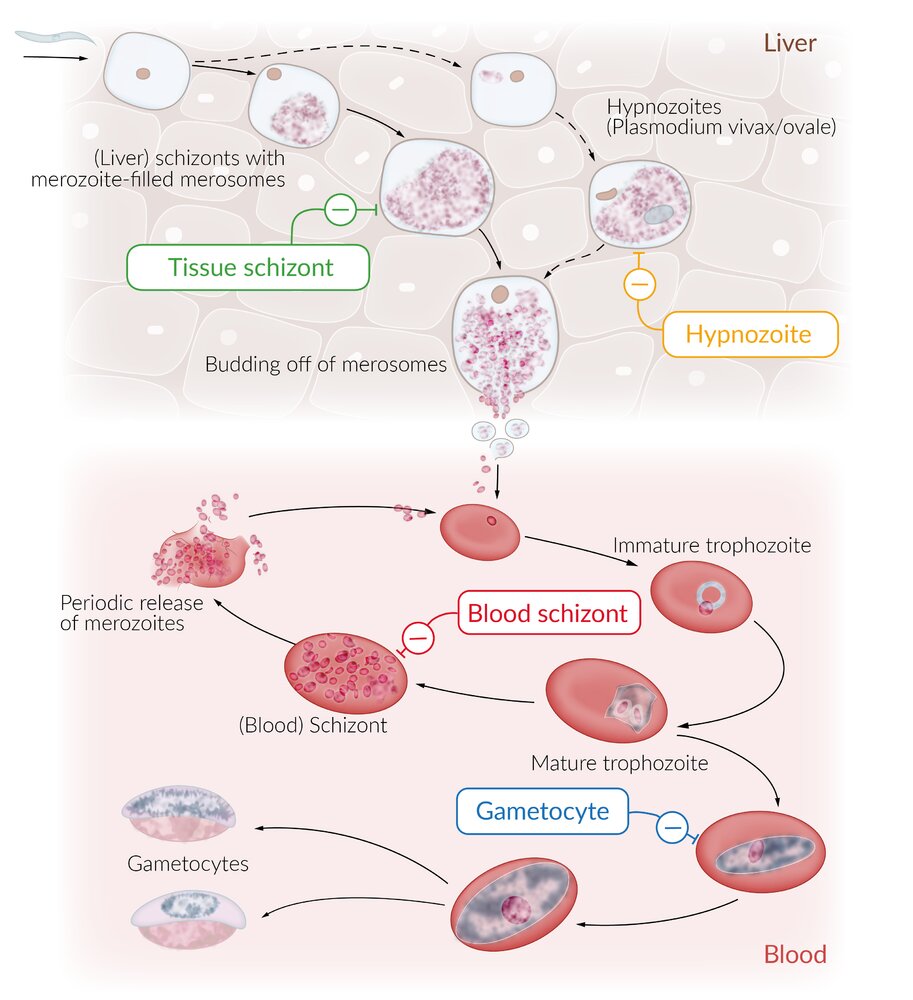
Illustration depicting the stages of a malaria parasite within a human host
- Right: legend of antimalarial drugs and their targets
- Bottom left: erythrocytic cycle (within blood)
- Top left: exoerythrocytic cycle (within the liver)
The four main targets of antimalarial drugs are the tissue schizont, hypnozoite, blood schizont, and gametocyte, which are the asexual developmental stages of malaria parasites that occur within the liver and blood of an infected human host. Most antimalarial drugs act on the erythrocytic stages of the malaria parasite, especially the blood schizonts. Primaquine is the only antimalarial that attacks the hypnozoites, which are the dormant stages of P. vivax and P. ovale, responsible for relapses of malaria.
© AMBOSS
Prevention
Mosquito bite prevention [42]
-
Avoid exposure
- Exercise particular caution during peak biting periods [43]
- Mosquito nets
- Protective clothing (covering most of the skin, light colors)
- Mosquito repellent, such as DEET (N,N-diethyl-meta-toluamide)
-
Mosquito control
- Reduce breeding sites (e.g., eliminate pools of water, optimize plant watering)
- Insecticide spraying
Malaria prophylaxis [44]
- Should be initiated before traveling to regions with a high risk of malaria (e.g., tropical Africa, Asia, and Central and South America)
-
Drug of choice is based on the region of travel and Plasmodium species.
-
All malaria-endemic regions (including those with chloroquine-resistant P. falciparum )
- Atovaquone-proguanil [44]
- Doxycycline [44]
- Mefloquine [44]
- Tafenoquine
-
Additional options for regions without chloroquine resistance
- Chloroquine [44]
- Hydroxychloroquine [44]
- Primaquine (off-label) : if traveling to P. vivax-dominant regions (> 90% P. vivax) for < 6 months [44]
-
All malaria-endemic regions (including those with chloroquine-resistant P. falciparum )
- Agents that are safe during pregnancy: chloroquine, mefloquine (see also “Malaria in pregnancy”)
- Take throughout travel and for 1–4 weeks afterward. [44]
- See “Tips & Links” for information from the CDC Yellow Book about malaria travel advisories and prophylaxis agents.
Prophylactic medication cannot prevent infection but instead suppresses the course of the disease and its symptoms by killing the parasite within the host before it can cause severe disease. There is no prophylactic medication that provides protection against all species of the Plasmodium genus.
Malaria vaccines are available, but they are currently only recommended for children living in endemic areas, not for travelers. [29]
Standby emergency treatment [45]
-
Indication
- Traveling to endemic regions with a medium to high risk of malaria
- Depending on the risk, either prophylactic or standby emergency treatment may be recommended (when in doubt: prophylactic medication).
-
Drugs
- Atovaquone-proguanil
- Artemether-lumefantrine
- Chloroquine with limitations: there are now many chloroquine-resistant Plasmodium strains with membrane pumps that lower intracellular chloroquine concentrations
Public health surveillance
- Malaria is a reportable disease in the US and is subject to active surveillance globally.
- Transmission and treatment resistance data informs travel advisories and chemoprophylaxis recommendations.
Special patient groups
The approach to malaria requires additional considerations in children and pregnant individuals.
Malaria in pregnancy
- Malaria during pregnancy can lead to serious complications, including: [29][46][47]
- Maternal anemia, preeclampsia, and/or death
- Pregnancy loss
- Preterm birth and low birth weight
- Congenital malaria and neonatal death
- Clinical features, diagnosis, and treatment of malaria are similar to those in nonpregnant individuals, with the following additional considerations:
- Severe malaria is three times more common than in nonpregnant individuals. [29][46]
- Malaria parasite density measurements may be unreliable in pregnant individuals with P. falciparum infection. [48]
- Pharmacological options for treatment and prophylaxis are more limited.
Travel to areas with malaria is not recommended during pregnancy. For essential travel, emphasize the importance of malaria prevention, including mosquito bite prevention. [44][49]
Pharmacotherapy for malaria in pregnancy
Malaria treatment
- Severe malaria: IV artesunate [29][46]
-
Uncomplicated malaria [29][46]
- Preferred
- Artemether-lumefantrine
- OR chloroquine
- OR hydroxychloroquine
- OR quinine sulfate PLUS clindamycin [29]
- Alternative: mefloquine [50]
- Preferred
-
Relapse prevention (P. vivax or P. ovale only)
- Give chloroquine chemoprophylaxis until delivery. [44][46]
- Relapse prevention after delivery is based on breastfeeding status. [46]
- Not breastfeeding: primaquine or tafenoquine
- Breastfeeding an infant with normal G6PD activity: primaquine
- Breastfeeding an infant with abnormal G6PD activity: Continue chloroquine chemoprophylaxis for one year after onset of acute malaria.
Malaria prophylaxis [44]
- Areas with no chloroquine resistance: chloroquine or hydroxychloroquine
- Areas with chloroquine resistance: mefloquine
Malaria in children
Epidemiology
- Worldwide, most malaria deaths occur in children < 5 years of age. [49][51]
- Approximately 15% of malaria infections in the US occur in children. [44][52]
Clinical features [49]
Clinical features of malaria are similar to those in adults with the following considerations in children.
- Young children often present with nonspecific viral symptoms. [49]
- Findings more common in children include:
- Severe malaria, particularly in those < 5 years of age [53][54][55]
- Malaria-associated nephrotic syndrome [49][56]
- Congenital malaria following perinatal infection is rare, but symptoms can mimic neonatal sepsis, e.g.: [49]
- Fever
- Poor feeding
- Irritability
- Decreased responsiveness
Hepatosplenomegaly is common in children living in areas endemic for malaria. [49]
Diagnosis [49][54]
- Same as diagnosis of malaria in adults, with similar laboratory abnormalities (e.g., anemia, thrombocytopenia)
-
Severe malaria
- Acute kidney injury is common in children. [49][57]
- Severe anemia (≤ 5 g/dL in children aged < 12 years, < 7 g/dL in children aged ≥ 12 years) is more common than in adults. [49][57]
Management
Consult infectious disease and consider hospital admission for all children. [53]
-
Severe malaria
- Admit to the ICU. [49][53]
- Start artesunate under specialist supervision. [29][49][50]
- Uncomplicated malaria: Start pharmacotherapy based on the infecting species, local resistance, and prior chemoprophylaxis use. [49][50]
| Pharmacotherapy for uncomplicated malaria in children | ||
|---|---|---|
| Plasmodium species | Chloroquine sensitivity | Treatment |
| P. vivax, P. ovale | Chloroquine-sensitive |
|
| Chloroquine-resistant |
|
|
| P. falciparum or not known | Chloroquine-sensitive |
|
| Chloroquine-resistant |
|
|
| P. malariae, P. knowlesi | Chloroquine-sensitive |
|
Check G6PD activity levels before prescribing primaquine. [29][49][50]
Prevention [44][49]
- Recommend mosquito bite prevention.
- Agents for malaria prophylaxis in children include:
- All regions: atovaquone-proguanil (children ≥ 5 kg (≥ 10 lb)) OR doxycycline (children ≥ 8 years of age) [44][49]
- Regions without chloroquine resistance [44]
- Chloroquine
- Hydroxychloroquine [44][49]
- Primaquine: if traveling to P. vivax-dominant regions (> 90% P. vivax) for < 6 months
- Mefloquine (if no known mefloquine resistance) [44][49]
- Childhood vaccination is recommended in endemic areas to prevent P. falciparum malaria. [29][49]
Atovaquone-proguanil is available in pediatric tablets that can be crushed and mixed with a sweet food or drink. [44]
Acute management checklist
All patients
- Order thick and thin blood smear on all patients to confirm the diagnosis and determine malaria parasitemia.
- Consider rapid diagnostic tests initially if blood smear microscopy is delayed or unavailable.
- Order additional tests: CBC, CMP, coagulation panel, type and screen, urinalysis, and blood culture
- Identify criteria of severe malaria.
- Consult infectious disease service.
Severe malaria
- Admit to ICU.
- Begin IV artesunate.
- Check glucose every 4 hours.
- Check CBC every 6–12 hours.
- Check renal function every 24 hours.
- Treat fever with acetaminophen, tepid sponging, cooling blanket.
- Rule out bacterial coinfection.
- Avoid excessive fluid administration.
- Repeat malaria parasitemia every 12–24 hours.
Uncomplicated malaria
- Determine species of Plasmodium.
- Review patient travel history.
- Inquire about patient malaria chemoprophylaxis use.
- Begin appropriate antimalarial medication under specialist guidance.
- Admit the patient to hospital for observation.
- Obtain serial measurements of malaria parasitemia.
Related One-Minute Telegram
- One-Minute Telegram 129-2025-2/3: Ivermectin: a new bite at malaria control?
- One-Minute Telegram 93-2024-2/3: Promising malaria vaccine results
- One-Minute Telegram 64-2022-2/3: New weapon in the fight against malaria
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- "Malaria". http://www.who.int/mediacentre/factsheets/fs094/en/. [2016-12-01]
- "Malaria". https://web.archive.org/web/20221004073720/https://www.who.int/news-room/fact-sheets/detail/malaria. [2022-07-26]
- WHO. "World malaria report 2021". World Health Organization. (2021). ISBN: 9789240040496
- Mueller I, Zimmerman PA, Reeder JC. "Plasmodium malariae and Plasmodium ovale – the ‘bashful’ malaria parasites". Trends Parasitol. 23(6). :278-283. (2007)
- "DPDx - Malaria". https://web.archive.org/web/20220901035714/http://www.cdc.gov/dpdx/malaria/index.html. [2020-10-06]
- Lee WC, Cheong FW, Amir A, et al. "Plasmodium knowlesi: the game changer for malaria eradication". Malar J. 21(1). (2022)
- Williams TN, Mwangi TW, Wambua S et al. "Sickle cell trait and the risk of Plasmodium falciparum malaria and other childhood diseases". J Infect Dis. 192(1). :178-186. (2005)
- Gledson Barbosa de Carvalho and Glauber Barbosa de Carvalho. "Duffy Blood Group System and the malaria adaptation process in humans". Revista Brasileira de Hematologia e Hemoterapia. (2011)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Finnel L. "Tintinalli's Emergency Medicine Manual, Eighth Edition". McGraw Hill Professional. (2017). ISBN: 9780071837040
- Mvumbi DM, Bobanga TL, Melin P et al. "High Prevalence of Plasmodium falciparum Infection in Asymptomatic Individuals from the Democratic Republic of the Congo". Malar Res Treat. 2016(2016). :5405802. (2016)
- Antinori S, Galimberti L, Milazzo L, Corbellino M. "Biology of human malaria plasmodia including Plasmodium Knowlesi". Mediterr J Hematol Infect Dis. 4(1). :2012013. (2012)
- "Malaria - Biology". https://web.archive.org/web/20171215213651/https://www.cdc.gov/malaria/about/biology/. [2017-03-01]
- "Malaria - Disease". https://web.archive.org/web/20181207081118/https://www.cdc.gov/malaria/about/disease.html. [2015-10-07]
- Cheaveau J, Mogollon DC, Mohon MAN, et al. "Asymptomatic malaria in the clinical and public health context". Expert Rev Anti Infect Ther. 17(12). :997-1010. (2019)
- "Treatment of Malaria: Guidelines for Clinicians (United States) 2020". https://web.archive.org/web/20240507153213/https://www.cdc.gov/malaria/diagnosis_treatment/clinicians1.html. [2020-05-20]
- World Health Organization. "Severe Malaria". Trop Med Int Health. 19. :7-131. (2014)
- "Treatment of Malaria: Guidelines For Clinicians (United States)". https://web.archive.org/web/20220302144422/https://www.cdc.gov/malaria/resources/pdf/Malaria_Treatment_Guidelines.pdf. [2020-05-11]
- Ashley EA, Pyae Phyo A, Woodrow CJ. "Malaria". Lancet. 391(10130). :1608-1621. (2018)
- Mace KE, Lucchi NW, Tan KR. "Malaria Surveillance — United States, 2017". MMWR. 70(2). :1-35. (2021)
- "WHO Guidelines for malaria". https://www.who.int/publications/i/item/guidelines-for-malaria. [2022-03-31]
- Daily JP, Minuti A, Khan N. "Diagnosis, Treatment, and Prevention of Malaria in the US". JAMA. 328(5). :460. (2022)
- Kotepui M, Piwkham D, PhunPhuech B, et al. "Effects of Malaria Parasite Density on Blood Cell Parameters". PLoS ONE. 10(3). :e0121057. (2015)
- Njim T, Dondorp A, Mukaka M, Ohuma EO. "Identifying risk factors for the development of sepsis during adult severe malaria". Malar J. 17(1). (2018)
- Mathison BA, Pritt BS. "Update on Malaria Diagnostics and Test Utilization". J Clin Microbiol. 55(7). :2009-2017. (2017)
- Berzosa P, de Lucio A, Romay-Barja M, et al. "Comparison of three diagnostic methods (microscopy, RDT, and PCR) for the detection of malaria parasites in representative samples from Equatorial Guinea". Malar J. 17(1). (2018)
- Stauffer WM, Cartwright CP, Olson DA, et al. "Diagnostic Performance of Rapid Diagnostic Tests versus Blood Smears for Malaria in US Clinical Practice". Clin Infect Dis. 49(6). :908-913. (2009)
- Grigg MJ, Lubis IN, Tetteh KKA, et al. "Plasmodium knowlesi detection methods for human infections-Diagnosis and surveillance.". Adv Parasitol. 113. :77-130. (2021)
- "CDC Malaria Treatment Table". https://web.archive.org/web/20220417033509/https://www.cdc.gov/malaria/resources/pdf/Malaria_Treatment_Table.pdf
- "Protection against Mosquitoes, Ticks, & Other Arthropods". https://web.archive.org/web/20161125231342/https://wwwnc.cdc.gov/travel/yellowbook/2016/the-pre-travel-consultation/protection-against-mosquitoes-ticks-other-arthropods. [2015-07-10]
- "Anopheles Mosquitoes". https://web.archive.org/web/20170713141826/https://www.cdc.gov/malaria/about/biology/mosquitoes/. [2015-10-21]
- "CDC Yellow Book: Health Information for International Travel - Malaria". https://web.archive.org/web/20250826134348/https://www.cdc.gov/yellow-book/hcp/travel-associated-infections-diseases/malaria.html. [2025-04-23]
- World Health Organization. "WHO guidelines for malaria, 13 August 2025". (2025)
- "Infectious Diseases Related to Travel - Malaria". https://web.archive.org/web/20170321083948/https://wwwnc.cdc.gov/travel/yellowbook/2016/infectious-diseases-related-to-travel/malaria#4660. [2015-07-10]
- "Artemether / Lumefantrine Side Effects". https://www.drugs.com/sfx/artemether-lumefantrine-side-effects.html. [2018-02-02]
- "Quinine Side Effects". https://www.drugs.com/sfx/quinine-side-effects.html. [2018-02-02]
- "Quinidine Side Effects". https://www.drugs.com/sfx/quinidine-side-effects.html. [2018-02-02]
- Luzzi GA, Peto TEA. "Adverse Effects of Antimalarials". Drug Saf. 8(4). :295-311. (1993)
- Aghahowa S, Obianwu H, Isah A, Arhewoh I. "Chloroquine-induced Pruritus". Indian J Pharm Sci. 72(3). :283. (2010)
- "Mefloquine". https://go.drugbank.com/drugs/DB00358
- "Quinine". https://go.drugbank.com/drugs/DB00468
- "Artemether". https://go.drugbank.com/drugs/DB06697
- "Atovaquone". https://go.drugbank.com/drugs/DB01117
- "Artesunate". https://go.drugbank.com/drugs/DB09274
- "Primaquine". https://go.drugbank.com/drugs/DB01087
- "CDC Clinical Guidance for Malaria Diagnosis & Treatment in the U.S.: Alternatives for Pregnant Women". https://web.archive.org/web/20250902154739/https://www.cdc.gov/malaria/hcp/clinical-guidance/pregnant-women.html
- Rasmussen SA, Arguin PM, Jamieson DJ. "Malaria and Pregnancy". Obstet Gynecol. 142(6). :1303-1309. (2023)
- Di Santi SMF. "The silent threat of submicroscopic Plasmodium infections during pregnancy". Lancet Glob Health. 11(7). :e991-e992. (2023)
- Committee on Infectious Disease, American Academy of Pediatrics. "Red Book: 2024-2027 Report of the Committee on Infectious Diseases, 33rd Edition". American Academy of Pediatrics. (2024). ISBN: 9781610027373
- "Malaria in the United States: Treatment Tables". https://web.archive.org/web/20250826155447/https://www.cdc.gov/malaria/hcp/clinical-guidance/malaria-treatment-tables.html. [2024-08-14]
- World Health Organization. "World malaria report 2024: addressing inequity in the global malaria response". World Health Organization. (2024). ISBN: 9789240104440
- "Malaria Surveillance, United States, 2022". https://web.archive.org/web/20250829085128/https://www.cdc.gov/malaria/php/surveillance-report/2022.html. [2025-05-28]
- Cohee LM, Laufer MK. "Malaria in Children". Pediatr Clin North Am. 64(4). :851-866. (2017)
- Kafai NM, Odom John AR. "Malaria in Children". Infect Dis Clin North Am. 32(1). :189-200. (2018)
- Shahbodaghi SD, Rathjen NA. "Malaria: Prevention, Diagnosis, and Treatment". Am Fam Physician. 106(3). :270-278. (2022)
- Rovin BH, Adler SG, Barratt J, et al. "KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases". Kidney Int. 100(4). :S1-S276. (2021)
- Daily JP, Parikh S. "Malaria". N Engl J Med. 392(13). :1320-1333. (2025)