Quick guide
Diagnostic approach
- Primary survey
- eFAST
- Portable CXR and/or pelvic x-ray
- Secondary survey
- CBC
- CMP
- Coagulation studies
- Type and screen
- Pregnancy test
- POC glucose
- Urinalysis
- ABG
- Lactate
- 12-lead ECG
- CT imaging in trauma

Follow a systematic approach to the secondary survey to avoid missing occult injuries (e.g., to the axilla, groin, back).
Red flag features
- Airway obstruction
- Tension pneumothorax
- Massive hemothorax
- Open pneumothorax
- Flail chest
- Cardiac tamponade
- Hemorrhagic shock
- Traumatic brain injury
Management checklist
- Secure airway.
- C-spine immobilization
- Continuous cardiac monitoring and pulse oximetry
- Supplemental O2
- Suspected tension pneumothorax: emergency chest decompression
- Massive hemothorax: chest tube placement
- Open pneumothorax: 3-sided occlusive dressing
- Two large-bore IVs (≥ 18-gauge)
- 1 L warmed isotonic crystalloid bolus
- Cardiac tamponade: urgent thoracotomy
- External hemorrhage: pressure or tourniquet
- Suspected bleeding pelvic fracture: pelvic binder
- Consult trauma surgery.
1. Right upper quadrant
Place the transducer over the right anterior axillary line along the subcostal margin or over the inferior intercostal spaces. Angle the transducer superiorly to assess the right costodiaphragmatic recess and right subphrenic space, and inferiorly to assess the hepatorenal space and inferior pole of the right kidney.
2: Left upper quadrant
Place the transducer over the left midaxillary line in one of the inferior intercostal spaces. Angle the transducer superiorly to assess the left costodiaphragmatic recess and left subphrenic space, and inferiorly to assess the splenorenal space and inferior pole of the left kidney.
3. Subxiphoid
Place the transducer in the subxiphoid space and tilt it up and toward the left shoulder to assess the pericardial space.
4. Pelvic
Place the transducer just above the pubic bone to assess the rectovesical space (♂) or rectouterine space (♀). Obtain transverse and longitudinal views.
5. Anterior thoracic
Place the transducer vertically over the 2nd or 3rd intercostal space along the midclavicular line on both sides. Sliding inferiorly may be necessary to appraise a sufficient number of intercostal spaces.
© AMBOSS
Summary
Trauma is one of the leading causes of death worldwide and, in the United States, the leading cause of death in young adults. Traumatic injuries range from isolated wounds to life-threatening multi-organ injuries. Advanced trauma life support (ATLS) is a framework for the systematic evaluation of trauma patients to improve outcomes and reduce missed injuries. Prehospital trauma care involves life-saving interventions and basic life support in the field by emergency medical services while providing rapid transportation to the nearest appropriate hospital. In the hospital, the assessment of trauma patients begins with a primary survey in which life-threatening conditions are identified and treated using the sequential ABCDE approach. After the patient is stabilized, the secondary survey is performed, which involves a thorough history and physical examination as well as diagnostic testing to identify other injuries. The tertiary survey is performed within 24 hours of presentation to identify missed injuries. If at any point during the evaluation the patient's needs exceed the hospital's capabilities, the process to transfer the patient to a trauma center should be initiated. Trauma management of pregnant, geriatric, and pediatric patients requires additional considerations given their unique physiology.
See also “Blunt trauma” and “Penetrating trauma.”
Definitions
-
Trauma center [1]
- A health facility that provides specialized care to patients with serious traumatic injuries.
- Different levels (e.g., I–V) of trauma center can be designated
-
Trauma team [1]
- A multidisciplinary team that provides care to patients at trauma centers
- Consists of specialists from trauma surgery, emergency medicine, intensive care, and nursing
- Members typically include a team leader, airway manager, assessment physician, proceduralist, trauma nurse, trauma technician, respiratory therapist, radiographer, and scribe.
- See also “Criteria for trauma team activation.”
-
Advanced trauma life support (ATLS) [1]
- A framework for managing patients with serious injuries in prehospital and hospital settings.
- Describes management sequences (e.g., ABCDE algorithm) that prioritize the most immediately life-threatening injuries first.
- Aims to standardize trauma care across centers with varying resources and experience with trauma management
- Polytrauma: severe injuries occurring in more than one anatomic region that cause systemic physiological disturbances [2]
Overview
Trauma care varies based on patient injuries, receiving center resources (e.g., equipment, consultants), and institutional and regional guidelines. Recommendations in this article are consistent with the 2018 Advanced Trauma Life Support guidelines. [1]
Overview of ATLS [1]
Sequence of trauma care
- Prehospital trauma care and transportation to hospital
- Primary survey
- Transfer to trauma center (if needed)
- Secondary survey
- Tertiary survey
Key components of ATLS
| Overview of ATLS | |
|---|---|
| Key components | |
| Primary survey |
|
| Secondary survey |
|
| Tertiary survey |
|
| Special patient groups |
|
Overview of injury mechanisms
| Overview of injury mechanisms [1] | ||
|---|---|---|
| Mechanisms of injury | Potential injuries | |
| Blunt trauma |
|
|
| Penetrating trauma |
|
|
| Thermal injury |
|
|
| Blast injuries |
|
|
| Other environmental injuries |
|
|
Overview of immediately life-threatening injuries
| Recognition and initial management of common critical injuries | ||
|---|---|---|
| Suggestive findings | Initial management | |
| Airway compromise |
|
|
| Tension pneumothorax |
|
|
| Massive hemothorax |
|
|
| Open pneumothorax |
|
|
| Cardiac tamponade |
|
|
| External hemorrhage |
|
|
| Internal hemorrhage |
|
|
Prehospital trauma care
Prehospital trauma care is situation-dependent and centered on field stabilization of the patient and prompt transport to the closest trauma center.
Bystanders [1][3]
- Shout for help and/or call 911.
- Assess scene safety prior to providing assistance.
- Remove the patient from dangerous situations.
- Initiate basic life support (BLS).
- Perform life-saving interventions.
- Airway opening maneuvers
- Hemorrhage control
- Spinal immobilization
Emergency medical services (EMS) [1][4]
Prehospital trauma care provided by physicians varies regionally. [5]
- EMS typically perform an abbreviated version of the primary survey.
-
Provide life-saving interventions.
- Airway management for respiratory distress or altered mental status
- Hemorrhage control (e.g., use of tourniquets or pressure bandages)
- Immediate hemodynamic support (e.g., IV fluids)
- Prevent additional injury.
- Spinal immobilization (e.g., cervical collar placement, backboard)
- Fracture stabilization
- Provide parenteral analgesia, as needed.
- Rapidly transport the patient to the closest appropriate hospital. [6][7]
- Notify the receiving hospital.
- Signout of patient to trauma team lead upon arrival
Primary survey
The ABCDE algorithm in ATLS provides a sequence to help prioritize treating the most rapidly life-threatening injuries first. In clinical practice, trauma team members evaluate and treat these simultaneously, continually reassessing each injury's severity throughout the resuscitation. [1]
Airway (and C-spine immobilization) [1]
Identify and treat airway obstruction (e.g., due to blood, direct injury, edema) and/or loss of airway protective reflexes, (e.g., due to AMS or coma), while preventing further C-spine injury.
-
Assess the airway.
- Ask the patient to state their name; the ability to answer typically correlates with a patent airway.
- Evaluate for signs of airway compromise and signs of respiratory distress.
- Examine the airway for foreign bodies or injury (e.g., facial fractures, soot, burns).
-
Perform initial interventions.
- Suction oropharyngeal secretions and/or blood.
- Perform airway opening maneuvers.
- Insert basic airway adjuncts.
-
Intubate patients with: [8]
- Airway obstruction and/or respiratory failure
- Depressed mental status (e.g., GCS ≤ 8) [8][9]
- Severe shock and/or cardiac arrest
- At-risk inhalation injury
-
Stabilize the C-spine.
- Assume C-spine injury in patients with blunt trauma and indications for spinal immobilization.
- Perform airway management with necessary spinal motion restrictions.
- See “Initial management of C-spine injury” for details.
Perform cricothyrotomy in case of intubation failure.
Consider early intubation for impending airway obstruction in patients with signs of inhalation injury, moderate to severe facial and oropharyngeal burns, and extensive body burns. [8]
Breathing [1]
Identify and treat chest injuries, e.g., tension pneumothorax, open pneumothorax, massive hemothorax, flail chest, and tracheobronchial injuries.
- Assess oxygenation: Evaluate SpO2 and start continuous pulse oximetry.
-
Assess ventilation
- Vital signs: Monitor rate and quality of respirations; consider EtCO2 monitoring.
- Neck: Inspect for jugular venous distension and tracheal deviation
- Chest: Auscultate and inspect for chest wall injuries: e.g., penetrating wounds, subcutaneous emphysema, absent breath sounds, paradoxical chest movement
- Consider eFAST to help identify pneumothorax at the bedside.
-
Perform initial interventions.
- Supplemental O2
- Emergency chest decompression for suspected tension pneumothorax.
- 3-sided dressing for sucking chest wound
- BMV or mechanical ventilation for respiratory failure
If traumatic pneumothorax is suspected in a patient requiring positive pressure ventilation, perform tube thoracostomy immediately to prevent progression to tension pneumothorax. [1]
Circulation [1]
Provide immediate hemodynamic support and hemostatic measures while identifying sources of bleeding, e.g., external hemorrhage, thoracic cavity, abdominal cavity, thighs, retroperitoneal space.
-
Assess hemodynamic status.
- Assess central pulses, level of consciousness, and capillary refill time.
- Monitor vitals and continuous cardiac telemetry.
-
Perform initial interventions.
- Place two large-bore IVs (at least 18-gauge).
- Consider intraosseous access if peripheral IV cannot be obtained.
- Administer 1 L warmed isotonic crystalloid bolus.
- If unresponsive to IV fluid, proceed to blood transfusion.
-
Localize hemorrhage.
- Perform FAST to rapidly identify hemopericardium, and intrathoracic, intraabdominal, and/or intrapelvic bleeding in unstable patients.
- Identify obvious pelvic or long bone (e.g., femur) deformity.
- Identify major bleeding vessels (e.g., in the neck, groin, chest, or proximal extremities).
- Identify indications for immediate surgery (e.g., exploratory laparotomy, urgent thoracotomy) and/or angioembolization.
-
Treat hemorrhagic shock.
- Administer emergency transfusion with universal donor blood products (e.g., type O blood) if required.
- Provide crossmatched blood products as soon as they are available.
- Follow local massive transfusion protocol if indicated, e.g., plasma, platelets, and pRBCs at a 1:1:1 ratio.
- Consider tranexamic acid (TXA). [10][11]
- Consider reversal of anticoagulation.
- Allow for permissive hypotension.
-
Perform bedside hemorrhage control.
- Apply pressure or tourniquet to control active external hemorrhage.
- Apply pelvic binder for suspected bleeding pelvic fractures
- Insert chest tube for suspected massive traumatic hemothorax
- Treat obstructive shock: e.g., chest tube insertion for tension pneumothorax, pericardial window for cardiac tamponade
If there is a loss of vital signs, treat traumatic cardiac arrest with emergency chest decompression and emergency thoracotomy.
Suspect cardiac tamponade in patients with penetrating chest injury with Beck triad and a positive FAST scan, and expedite urgent pericardial fluid drainage via thoracotomy.
Penetrating abdominal injury with signs of shock is usually an indication for exploratory laparotomy.
Disability [1]
Identify life-threatening traumatic brain injury (TBI), begin measures to limit secondary brain injury, and expedite definitive surgery if indicated.
-
Perform rapid neurological evaluation.
- Calculate GCS.
- Assess pupillary light response.
- Assess motor and sensation functions.
-
Initiate TBI management.
- Consult neurosurgery.
- Start neuroprotective measures.
- Start ICP management if a cerebral herniation syndrome is present.
Remain vigilant for signs of traumatic brain injury in intoxicated patients. [1]
")
Exposure (and environmental control) [1]
- Undress the patient completely.
- Examine the entire patient for signs of occult injury, including the axilla, groin, and back.
- Prevent and/or manage hypothermia with rewarming techniques.
Diagnostic adjuncts [1]
Consider the following studies during the primary survey if they are likely to impact immediate management:
- Portable CXR
- Portable pelvic x-ray
- FAST or eFAST
- Diagnostic peritoneal lavage (if POCUS is unavailable)
- See “Diagnostics in trauma” for details.
Use bedside studies for rapid diagnostics in patients that are too unstable for transport to imaging suites.
Traumatic circulatory arrest [1]
- Common causes include tension pneumothorax, cardiac tamponade, and hemorrhagic shock.
-
Management
- First line: bilateral chest decompression with finger thoracostomy
- Consider emergency thoracotomy
- Expedite definitive surgery and operative stabilization of survivors.
Traumatic cardiac arrest requires bedside surgical interventions by trained personnel and subsequent operative treatment and stabilization. Do not follow standard ACLS algorithms as these are unlikely to be effective.

Resuscitative thoracotomy [12]
The following is consistent with the 2015 Eastern Association for the Surgery of Trauma (EAST) recommendations on emergency department thoracotomy. Follow local policies as indications vary regionally. [12]
- Definition: a bedside procedure performed in the emergency department or trauma bay to obtain emergency access to the thoracic cavity to provide temporizing lifesaving measures in pulseless patients
-
Purpose
- Relieve cardiac tamponade via pericardiotomy and/or repair of myocardial injury
- Control intrathoracic hemorrhage
- Perform open cardiac massage
- Cross-clamp the descending aorta
-
Indications
- Pulseless patients after penetrating thoracic injury
- Pulseless patients after penetrating extrathoracic injury, excluding isolated cranial injuries
- Pulseless patients with recently documented signs of life in the field or at the hospital after blunt injury
- Contraindication: pulseless patients without any documented signs of life in the field or at the hospital after blunt injury
Do not perform resuscitative thoracotomy unless a qualified surgeon is present. [1]
Interim management
Consider the following once the primary survey is complete:
- Reassess the effectiveness of life-saving bedside interventions.
- Prepare for urgent time-sensitive imaging (e.g., CT head) once the patient is stable enough.
- Determine if the patient needs immediate surgery, urgent interfacility transfer, or immediate specialty consult (see “Disposition”).
- Next steps: See “Secondary survey.”
If there is clinical deterioration at any time, repeat the primary survey to identify a critical cause.
Urgent interfacility transfer [1]
The following applies to patients initially evaluated at facilities that are not trauma centers:
- The decision to transfer a patient to a trauma center for definitive care is multifactorial.
- See “Criteria for trauma team activation” for conditions that typically require management by a trained trauma team.
- If tests are required prior to transfer, keep them limited to tests that will ensure a safe transfer.
- Communicate with the receiving physician and transportation team about clinical and diagnostic findings.
Do not delay an urgent transfer in order to complete an in-depth diagnostic evaluation.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
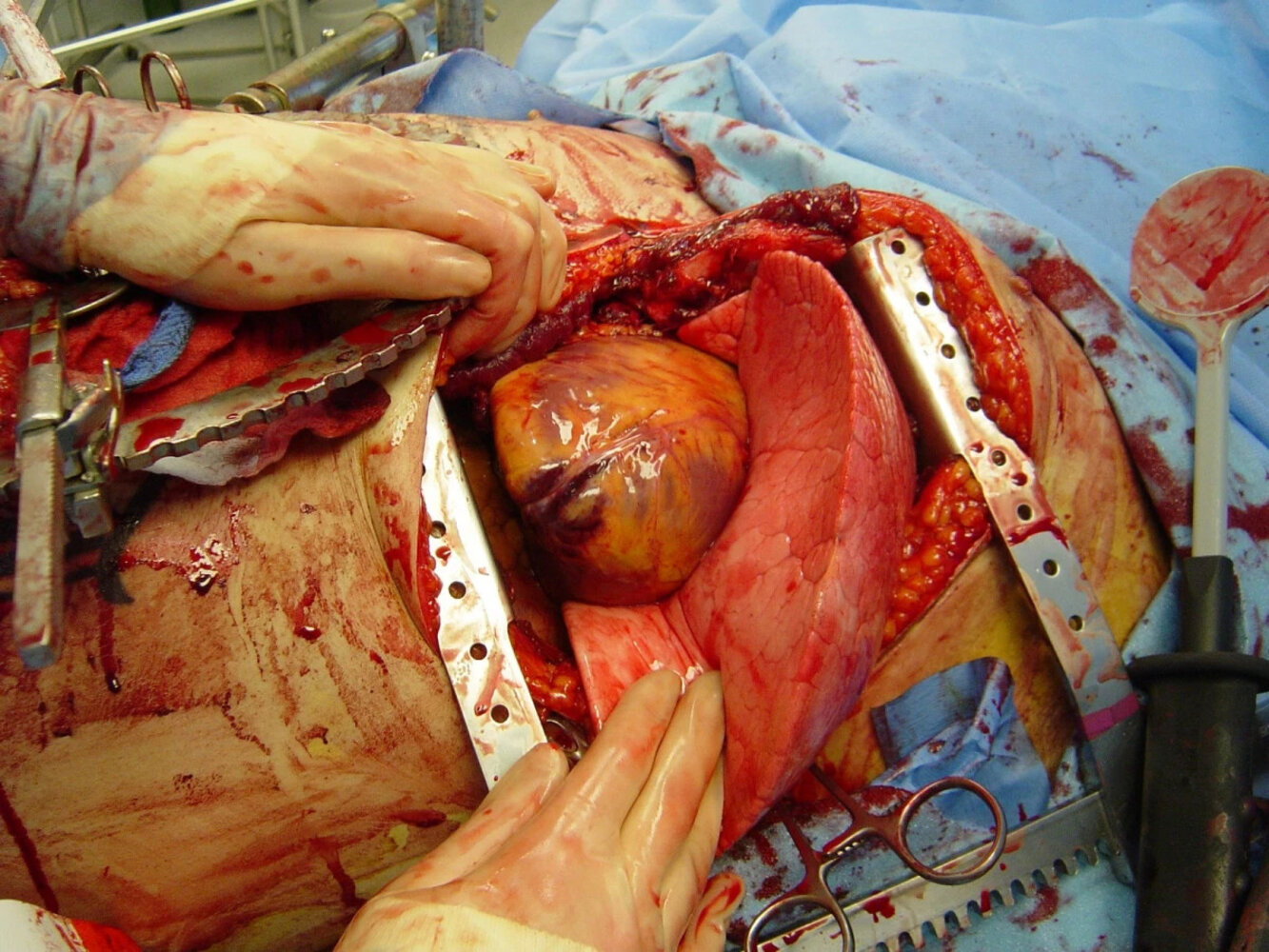
A resuscitative thoracotomy incision is performed through the fourth or fifth intercostal space. The incision should begin at the right of the sternum, and should then curve into the axilla at the level of the left nipple. If a transverse sternal split is required, the Finochiettos' rib retractor is placed with the handle directed inferiorly toward the bed.
That procedure can be performed as an emergency measure in the management of traumatic cardiac arrest.
Source: “Fig 2, In: Emergency department thoracotomy for the critically injured patient: Objectives, indications, and outcomes” by Cothren CC, Moore EE, BMC, licensed under CC BY 2.0.
Secondary survey
The secondary survey is performed after the patient is stabilized and it involves a thorough history and physical examination as well as diagnostic testing to identify other injuries.
History [1]
Obtain the following to anticipate likely injuries and estimate patient's physiological reserve.
-
AMPLE history: a focused history approach recommended in the rapid evaluation of patients with trauma
- Allergies
- Medications
- Past medical history and pregnancy status
- Last meal
- Events and environment related to the injury
-
Mechanism of injury
- Injury patterns can provide clues to the mechanism of injury (e.g., direction, amount of energy).
- Commonly divided into blunt trauma and penetrating trauma
- See “Blunt trauma injury mechanisms.”
- See “Gunshot injuries” and “Penetrating trauma.”
Obtain collateral information from EMS, family, and/or witnesses, especially if the patient is unable to provide a reliable history.
Physical examination [1]
A systematic head-to-toe physical examination must be completed to identify additional injuries.
- Assess each body part for open wounds, lacerations, abrasions, foreign bodies, and/or bruising.
- Identify any bony deformities, areas with focal tenderness, or edema.
- Document all findings.
| Secondary survey in trauma patients [1] | ||
|---|---|---|
| Examination | Injuries | |
| Head |
|
|
| Maxillofacial |
|
|
| Cervical spine and neck |
|
|
| Chest |
|
|
| Abdomen and pelvis |
|
|
| Genitourinary |
|
|
| Back and flank |
|
|
| Musculoskeletal |
|
|
| Neurological |
|
|
Do not forget to log roll patients who are under C-spine precautions to examine the back and spine.
Diagnostic adjuncts [1]
Consider the following diagnostic studies and procedures during the secondary survey once the patient is stable:
- Whole-body CT (WBCT)
- CT head without IV contrast
- CT cervical spine without IV contrast
- CT thoracic and/or lumbar spine without IV contrast
- CT chest with IV contrast or CTA chest
- CT abdomen and pelvis with IV contrast
- X-rays of the extremities
- Laboratory studies
- Ancillary testing (e.g., bronchoscopy, esophagoscopy)
- See “Diagnostics in trauma” for details.
Further management
- Ensure imaging is ordered for all identifiable injuries.
- Consider using decision rule to clinically rule out C-spine injury and allow early removal of C-spine precautions.
- Order routine trauma laboratory studies, including any emergency preop diagnostics and tests required to evaluate medical comorbidies.
- Order appropriate monitoring, e.g., continuous cardiac monitoring, neurovitals.
- Provide adequate analgesia and other supportive care (e.g., antiemetics, maintenance fluids).
- Provide tetanus prophylaxis for open wounds.
- If intraperitoneal injury is suspected, administer empiric antibiotics for intraabdominal infections.
- Evaluate the need for admission, interfacility transfer, and further consults to address newly identified injuries (See “Disposition”).
- Next steps: See “Tertiary survey.”
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Tertiary survey
Goal [1][13]
- Identify injuries undetected during primary and secondary surveys.
- Ensure patient safety.
- Complete the tertiary survey within 24 hours of presentation.
A standardized tertiary survey with high-quality imaging may limit the incidence of missed injuries. [14]
Approach [1][13]
- Obtain collateral information if trauma history remains unclear.
- Identify and rectify gaps in the patient's medical history (e.g., chronic conditions, medications, allergies).
- Repeat examination of the patient focusing on musculoskeletal injuries and detailed neurovascular examination.
- Review previously obtained diagnostic studies.
- Order additional studies based on tertiary survey findings.
- Screen for suicidality and nonsuicidal self-injury if self-harm is suspected.
- Screen for sexual violence, intimate partner violence, older adult abuse, and child abuse in at-risk individuals.
Hand and foot injuries are the most common missed injuries. [15][16]
Missed injuries [15][16][17]
Missed injuries are an important area of focus for quality and safety in trauma care, however, high-quality evidence is limited. [14]
Risk factors [1][13][18][19]
-
Patient risk factors include:
- Altered mental status
- Concomitant TBI
- Polytrauma with distracting injuries
- Higher overall injury severity
- Need for urgent surgery
- Age > 30
- Dangerous injury mechanism: e.g., assault, fall from height, MVC, pedestrian struck, GSW, stab wounds
-
System-associated risk factors include:
- Limited initial clinical evaluation
- Radiological imaging lacking or delayed
- Cognitive biases
- See “Health care personnel-associated risk factors” in “Quality and safety” for details.
Beware of anchoring bias and premature closure bias during the tertiary survey.
Injuries at risk of missed or delayed diagnosis [14][15][16]
The following have a higher potential to remain undetected after initial evaluation.
Surface wounds
- Scalp, nose, and mouth
- Axillae
- Groin and perineum
Extremity
- MSK injuries involving the hand and foot
- Neurovascular injury
- Compartment syndrome
- Occult extremity fractures
Head, neck, and spine
- Small or delayed intracranial hemorrhages
- Occult facial fractures and C-spine fracture
- Carotid and vertebral artery injuries
Thorax
- Blunt cardiac injury
- Penetrating and blunt thoracic aortic injury
- Diaphragmatic injury
- Esophageal perforation
Abdominopelvic
- Hollow viscus injury
- Retroperitoneal injury (e.g., pancreatic and duodenal bulb injuries)
- Subtle liver or splenic laceration
- Genitourinary trauma (e.g., ureter injury)
- Penetrating rectal injury
Diagnostics
Approach
- Consider clinical judgment, mechanism of injury, and patient factors (e.g., age, hemodynamic status) when choosing diagnostic studies.
- Weigh the need and timing of diagnostic studies against the need for urgent interfacility transfer or surgical intervention for each patient.
- Follow local policies on diagnostic imaging strategy (e.g., liberal vs. selective) as these vary by institution and region (see “CT imaging in trauma” for details).
ECG [1]
- Indications: mechanisms that may result in cardiac injury (e.g., in blunt chest trauma)
- Findings
- Blunt cardiac injury (e.g., dysrhythmia, ST segment changes)
- Pericardial effusion and cardiac tamponade (e.g., electrical alternans, low voltage QRS)
Laboratory studies [1]
- Routine studies: CBC, BMP, LFTs
- Preoperative studies: coagulation studies, type and screen
- Pregnancy test (e.g., serum or urine β-hCG)
- POC glucose
- Urinalysis (See “Approach to genitourinary trauma” for details.)
- Lactate
- ABG: to evaluate PaO2, PaCO2, pH and base deficit
Normotensive patients with trauma may have subclinical hypoperfusion. Evaluate for other clinical features of shock and check hemodynamic parameters (e.g., serum lactate, base deficit).
FAST and eFAST [1][20]
See “Point-of-care ultrasound” (POCUS) for procedural details (e.g., image generation and troubleshooting).
- Focused assessment with sonography for trauma (FAST): thoracoabdominal POCUS used in trauma patients to detect free fluid within the peritoneal, pericardial, and pleural cavities
- Extended FAST (eFAST): an extension of the FAST scan that includes evaluation of the chest for lung sliding
-
Clinical applications in trauma
- Can identify internal hemorrhage (e.g., hemoperitoneum, hemopericardium, hemothorax) requiring operative intervention in unstable patients
- eFAST can additionally help identify pneumothorax
- Used primarily as a diagnostic adjunct during the primary survey
- Can be used as an adjunct for serial reassessments
-
Limitations
- Limited sensitivity in stable patients
- Needs to be interpreted alongside other diagnostic and clinical findings
- Technique: Sonography of the subxiphoid, RUQ, LUQ, pelvic, and anterior thoracic regions is typically performed (see “FAST and eFAST” in “POCUS” for details).
-
Findings: See “FAST and eFAST” in “POCUS” for details.
- Free fluid can be seen in the following spaces:
- Pericardial
- Pleural
- Hepatorenal
- Splenorenal and/or subphrenic
- Pelvic
- Lung sliding may be absent in pneumothorax
- Free fluid can be seen in the following spaces:
Interpret FAST and eFAST alongside other diagnostic parameters and clinical judgment. POCUS does not replace definitive diagnostic studies. [20]
A positive FAST exam in a hemodynamically unstable patient with trauma is usually an indication for urgent operative intervention (e.g., exploratory laparotomy, urgent thoracotomy, pericardiotomy).













Radiography [1]
Bedside chest and pelvic x-rays are commonly performed during the primary survey, while extremity and spine X-rays are typically reserved for the secondary survey.
CXR
- Indications: blunt or penetrating trauma to the chest or abdomen
-
Findings
- Pneumothorax
- Hemothorax
- Pneumoperitoneum
- Pneumomediastinum
- Widened mediastinum
Pelvic X-ray
-
Indications
- Blunt or penetrating trauma to the abdomen
- Unstable pelvis
- Findings: pelvic fracture
Extremity X-rays
- Indications: pain, redness, swelling, or deformity at the injury site
- Findings: fracture and/or dislocation
Spinal X-rays
Spinal x-rays have been replaced by CT imaging in most trauma centers.
-
Indications
- Spinal tenderness to palpation
- Disruption of the vertebral process alignment (i.e., step-off deformity)
- Extremity numbness, tingling, or weakness
- Neurogenic shock
-
Findings
- Vertebral compression fracture
- Burst fracture
- Chance fracture
- Transverse process fracture
- Spinous process fracture
- Spondylolisthesis
CT imaging in trauma [1]
Approach
- Perform CT scans preferentially during the secondary survey in hemodynamically stable patients with no obvious indications for emergent laparotomy.
- Make decisions about the timing, necessity, and sequence of CT scans together with all relevant specialists on the trauma team, especially for patients with polytrauma.
- If a crucial CT scan cannot be delayed as it impacts operative management, ensure trauma teams are at the bedside with stabilizing treatments throughout the procedure.
- Follow local protocols for CT imaging (e.g., WBCT vs. selective CT imaging) under specialist guidance. [21][22][23][24][25]
Avoid transporting unstable patients out of resuscitation areas to obtain CT scans whenever possible.
Whole-body CT (pan scan) [21]
- May be performed to evaluate patients with multiple injuries after significant trauma
- Commonly includes:
- CT head without IV contrast
- CT cervical spine without IV contrast
- CT thoracic and lumbar spine with IV contrast
- CT chest with IV contrast
- CTA chest
- CT abdomen and pelvis with IV contrast
CT head and spine
- CT head without IV contrast: See “Diagnostic imaging in traumatic brain injury.”
-
CT cervical spine without IV contrast
- Indications
- Clinical suspicion of C-spine injury based on mechanism and examination
- Inability to clear C-spine clinically using a validated tool (e.g., NEXUS C-spine criteria , Canadian C-spine rule (CCR) )
- Findings
- Bony deformity and/or fracture of the vertebral body or processes
- Loss of alignment of the vertebral bodies
- Increased distance between vertebrae
- Narrowing of vertebral canal
- Increased prevertebral soft tissue swelling
- Indications
-
CT thoracic and lumbar spine without IV contrast
- Indications: clinical suspicion of T-spine and/or or L-spine injury based on mechanism and examination
- Findings: similar to CT cervical spine
Consider imaging for spinal fractures in patients with evidence of high-energy trauma to the lower extremities (e.g., calcaneus fracture) after falling from a height.
Obtain CT cervical spine if C-spine injury cannot be ruled out using validated clinical decision tools. [26]
CT chest with IV contrast [27][28]
-
Indications
- Inability to rule out blunt chest trauma with validated clinical decision tools
- Penetrating chest trauma
-
Findings
- Cardiac injury (e.g., blunt cardiac injury)
- Lung injury (e.g., pneumothorax, hemothorax, pulmonary contusion)
- Tracheal injury
- Diaphragm injury
- Esophageal injury
- Chest wall injury (e.g., rib fracture)
CTA chest
-
Indications
- Inability to rule out blunt chest trauma with validated clinical decision tools
- Penetrating chest trauma with concern for great vessel injury.
-
Findings
- Cardiac injury (e.g., blunt cardiac injury)
- Blunt thoracic aortic injury
- Vascular injury (e.g., penetrating chest trauma) [29]
Consider CTA chest to evaluate for blunt thoracic aortic injury in patients with high-energy trauma and a wide mediastinum on CXR.
CT abdomen and pelvis with IV contrast
-
Indications
- Blunt and/or penetrating abdominal trauma
- Penetrating back and/or flank trauma with no other indications for immediate laparotomy
-
Findings
- Stomach injury
- Splenic injury (e.g., splenic rupture)
- Liver injury (e.g., liver hematoma)
- Small and large bowel injuries (e.g., gastrointestinal perforation)
- Kidney injury (e.g., renal laceration, renal hematoma)
- Bladder injury (e.g., rupture of the bladder)
- Pelvic fracture
Diagnostic peritoneal lavage (DPL)
- Definition: an invasive diagnostic test used to assess for hemoperitoneum or viscus perforation in abdominal trauma
- Indications: : may be performed after the primary survey for suspected hemoperitoneum with equivocal or unavailable FAST [1]
- Procedure: A catheter is placed into the abdomen and contents are aspirated to assess for the presence of blood or fecal matter. If neither is observed, a liter of warm saline is instilled and then collected for cytological analysis.
- Findings: The presence of bile, fecal matter, or ≥ 10 cc of blood is considered a positive test and is an indication for emergent laparotomy.
Ancillary testing
Additional testing may be performed depending on the mechanism of injury and clinical evaluation, and may include:
- Bronchoscopy for tracheobronchial injury
- Esophagoscopy for esophageal perforation
- Assessment for features of GU trauma (e.g., using CT urography, retrograde urethrogram): for renal, ureteral and urethral injuries
- Echocardiography for blunt cardiac injury
Assess patients for features of GU trauma (e.g., with retrograde urethrogram) if there is hematuria, blood at the meatus, inability to void, need for pelvic binder, scrotal hematoma, or perineal ecchymosis.
Suspect tracheobronchial injury in patients with extensive subcutaneous emphysema.

Echocardiography (transthoracic; parasternal long axis)
The image was taken in ventricular diastole with the mitral valve (M) open. Anechoic pericardial effusion (green overlay) surrounds the heart.
LV: left ventricle; RV: right ventricle
Source: © IMPP
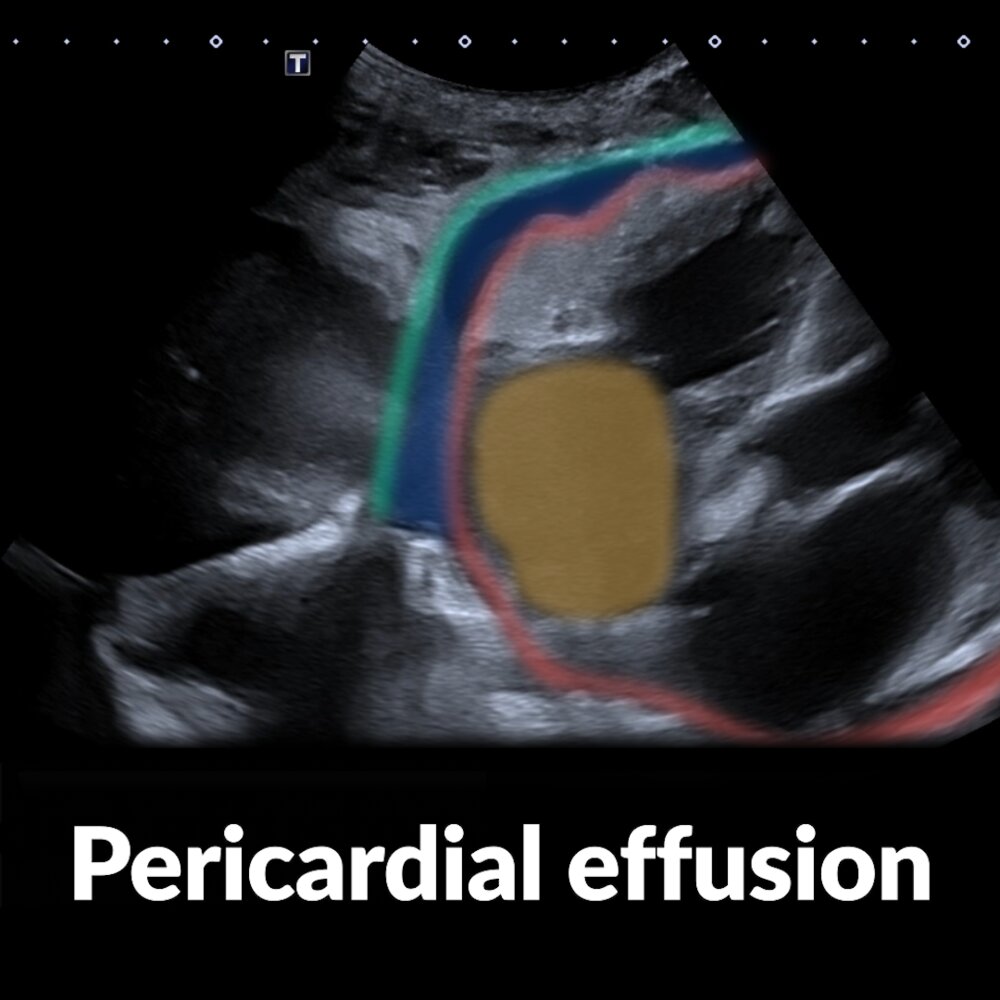
Short video of a subxiphoid ultrasound examination of the heart (a marker indicates the probe position) showing a pericardial effusion
The right atrium (yellow overlay) is seen in the center of the image. The visceral pericardium (epicardium; red line) is clearly separated from the parietal and fibrous pericardium (green line) by a hypoechoic area (blue overlay), which corresponds to a pericardial effusion.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Ultrasound chest (posterior right hemithorax)
Anechoic fluid (green overlay; F) is visible in the costodiaphragmatic recess between the right hemidiaphragm (D) and atelectatic lung (Lu).
Li: liver
© AMBOSS
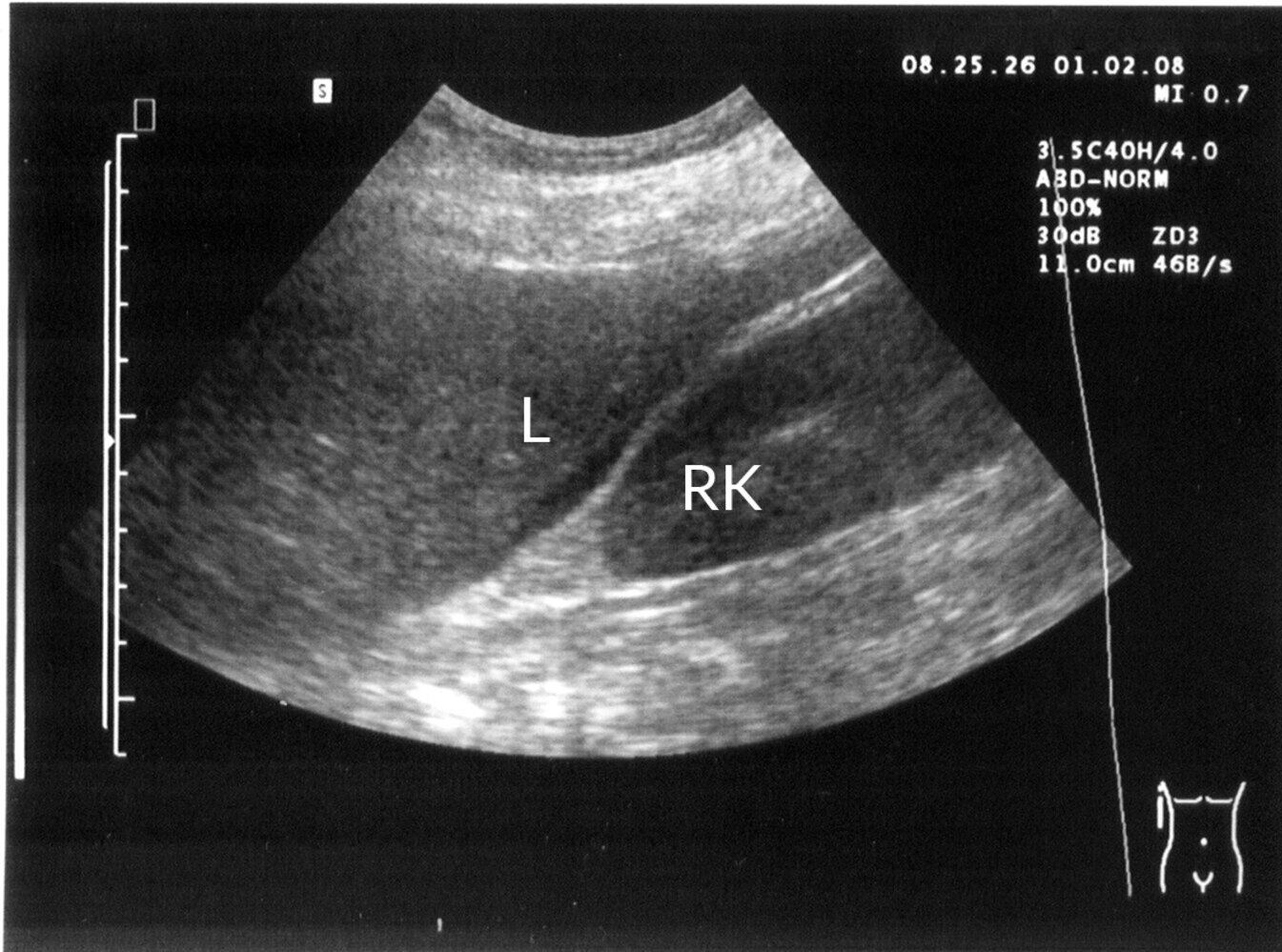
Ultrasound right upper quadrant (coronal plane)
The hepatorenal recess (green overlay), also termed the posterior right subhepatic recess or Morison pouch, is a potential space between the liver (L) and right kidney (RK). It is one of the dependent locations where intraperitoneal free fluid (red overlay) may accumulate in the supine position.
Source: “Morison004” by Drahreg01, Wikimedia Foundation, licensed under CC BY-SA 3.0. Modifications: removed in-image text, translated in-image text. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
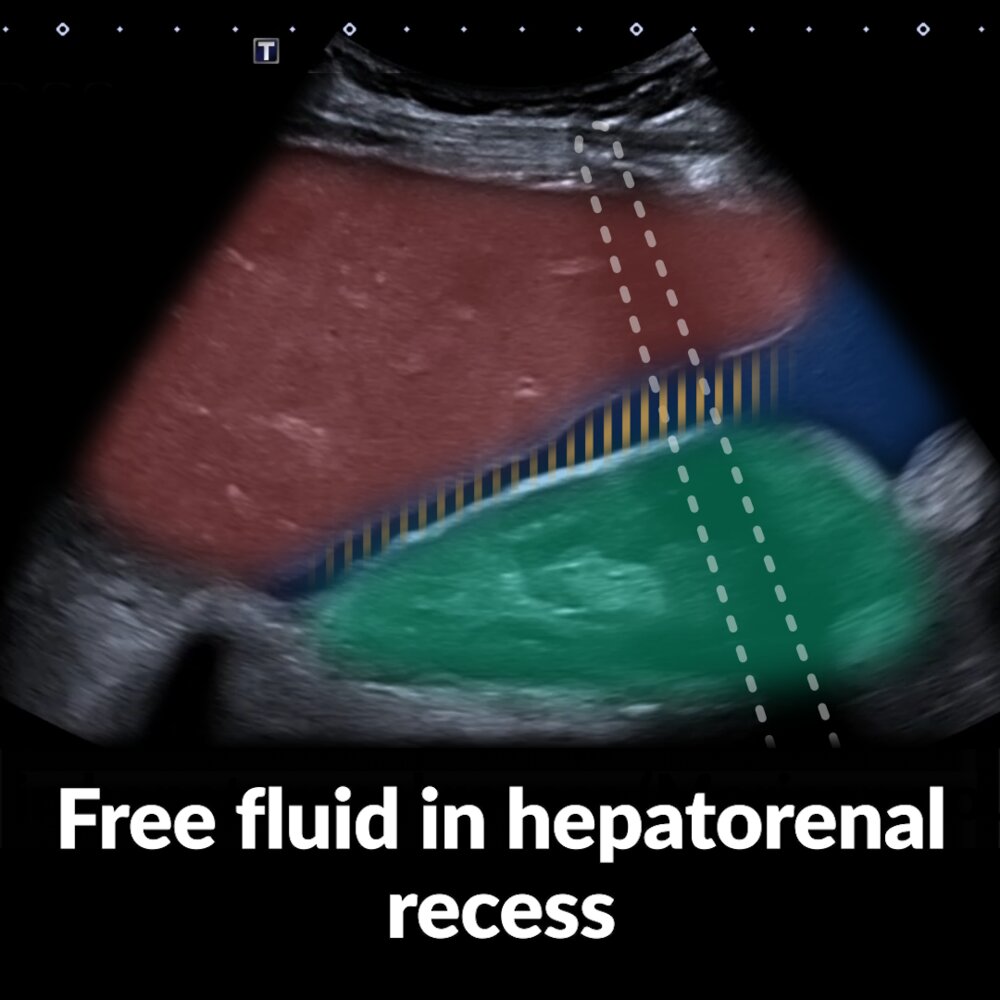
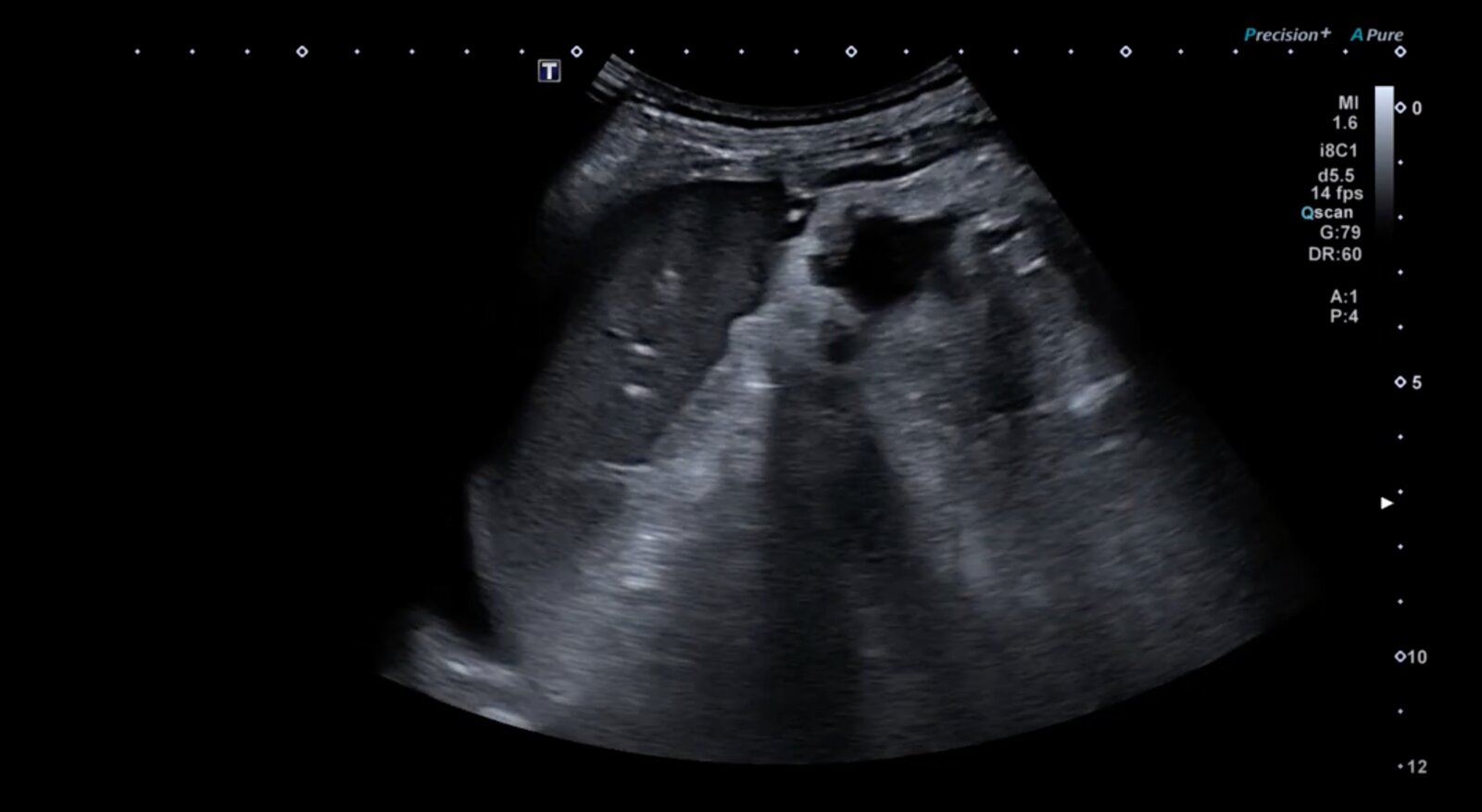
Short video of three right upper quadrant (RUQ; markers indicate the probe positions) ultrasound examinations showing free fluid in the hepatorenal recess (Morison pouch)
Case 1: The liver (red overlay) is visible near the top left of the image, the right kidney (green overlay) with its hyperechoic capsule is visible in the center and bottom right. A hypoechoic area (blue overlay) consistent with free fluid is visible within the hepatorenal recess (yellow hatching) and extending beyond the liver to the right of the image.
Case 2: The liver (red overlay) is visible near the top left of the image, the right kidney (green overlay) is visible near the bottom left. A hypoechoic area (blue overlay) consistent with free fluid is visible within the hepatorenal recess (yellow hatching) and extending beyond the liver to the right of the image.
Case 3: The liver (red overlay) is visible near the top left of the image, the right kidney (green overlay) with its hyperechoic capsule is visible near the bottom center. A hypoechoic area (blue overlay) consistent with free fluid is visible within the hepatorenal recess (yellow hatching) and extending beyond the liver to the right of the image.
Ultrasound can detect even small amounts of fluid in the hepatorenal recess.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.

Point of care ultrasound left upper abdominal quadrant (curvilinear transducer; B-mode)
Anechoic fluid collections (arrows) are visible in the splenorenal recess.
In the setting of trauma, anechoic fluid collection in potential space is assumed to be hemorrhage until proven otherwise.
Green overlay: kidney; S: spleen
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.

Short video of three left upper quadrant (LUQ; markers indicate the probe positions) ultrasound examinations showing free fluid in the splenorenal recess
Case 1: The spleen (red overlay) is visible as a relatively homogeneous structure at the top left of the image, the left kidney (green overlay) with its hyperechoic capsule and more heterogeneous appearance is visible in the center and bottom right. At the beginning of the video, there is no evidence of free fluid in the splenorenal recess (yellow shading). Fanning the ultrasound beam ventrally (by tilting the transducer dorsally) reveals a homogeneous, hypoechoic area consistent with free fluid (blue overlay) medial to the spleen. At the end of case 1, we again see the classic view of the splenorenal recess, which does not show the pathology.
Case 2: The spleen (red overlay) is visible at the top left, the left kidney (green overlay) at bottom right. In the initial view there is again no evidence of free fluid in the splenorenal recess (yellow hatching). As in case 1, fanning the ultrasound beam ventrally reveals a homogeneous, hypoechoic area consistent with free fluid (blue overlay).
Case 3: The spleen (red overlay) is visible at the top of the image, the left kidney (green overlay) at the bottom. A hypoechoic area (blue overlay) consistent with free fluid extends from the splenorenal recess (yellow hatching) towards the top right of the image (anatomically inferior to the spleen).
Ultrasound can detect even small amounts of fluid in the splenorenal recess.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
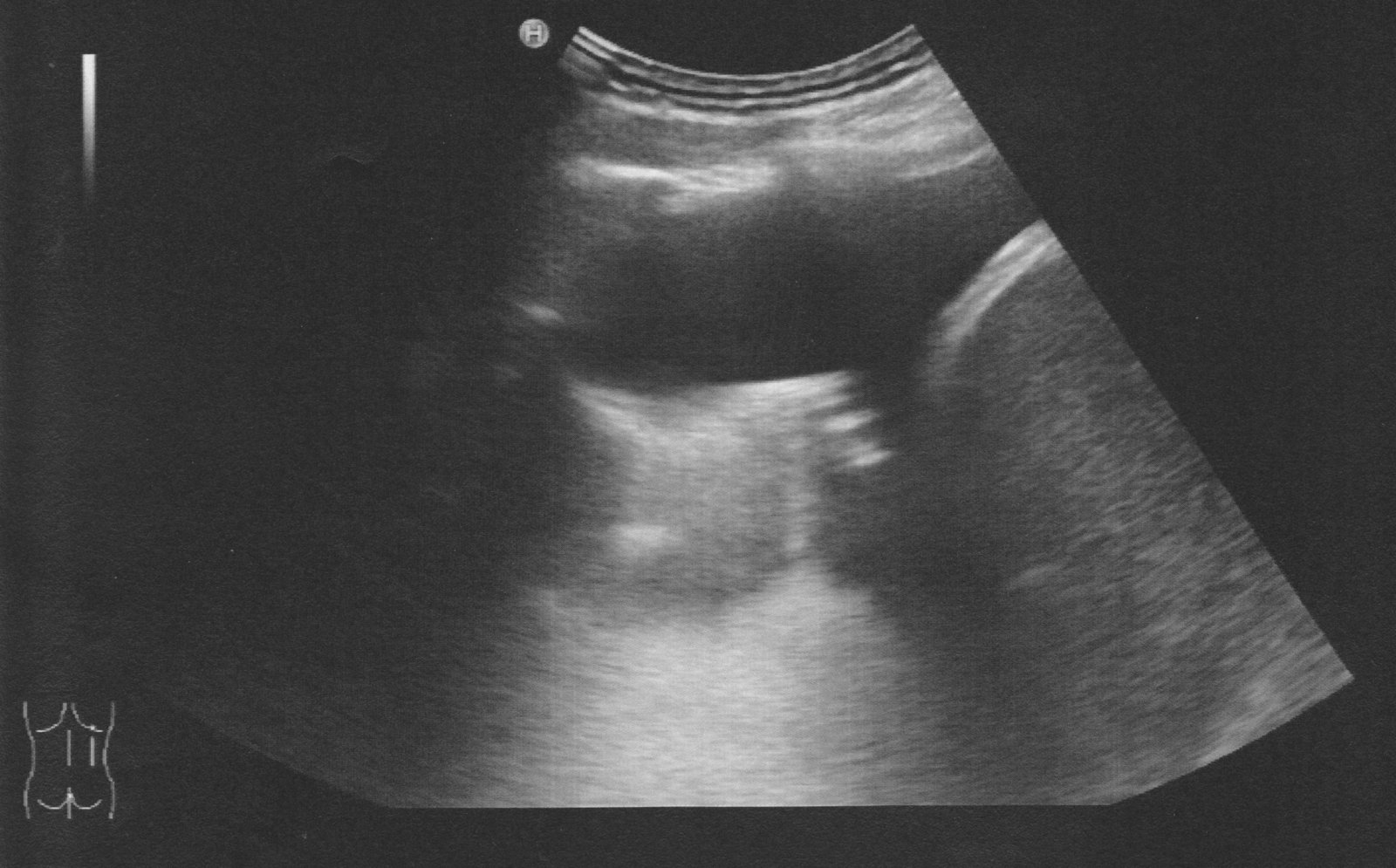
Point of care ultrasonography of the left upper quadrant of the abdomen (curvilinear transducer; B-mode)
There is an anechoic collection between the spleen and the diaphragm.
In the setting of trauma, anechoic collections within potential spaces should be assumed to be hemorrhage until proven otherwise.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
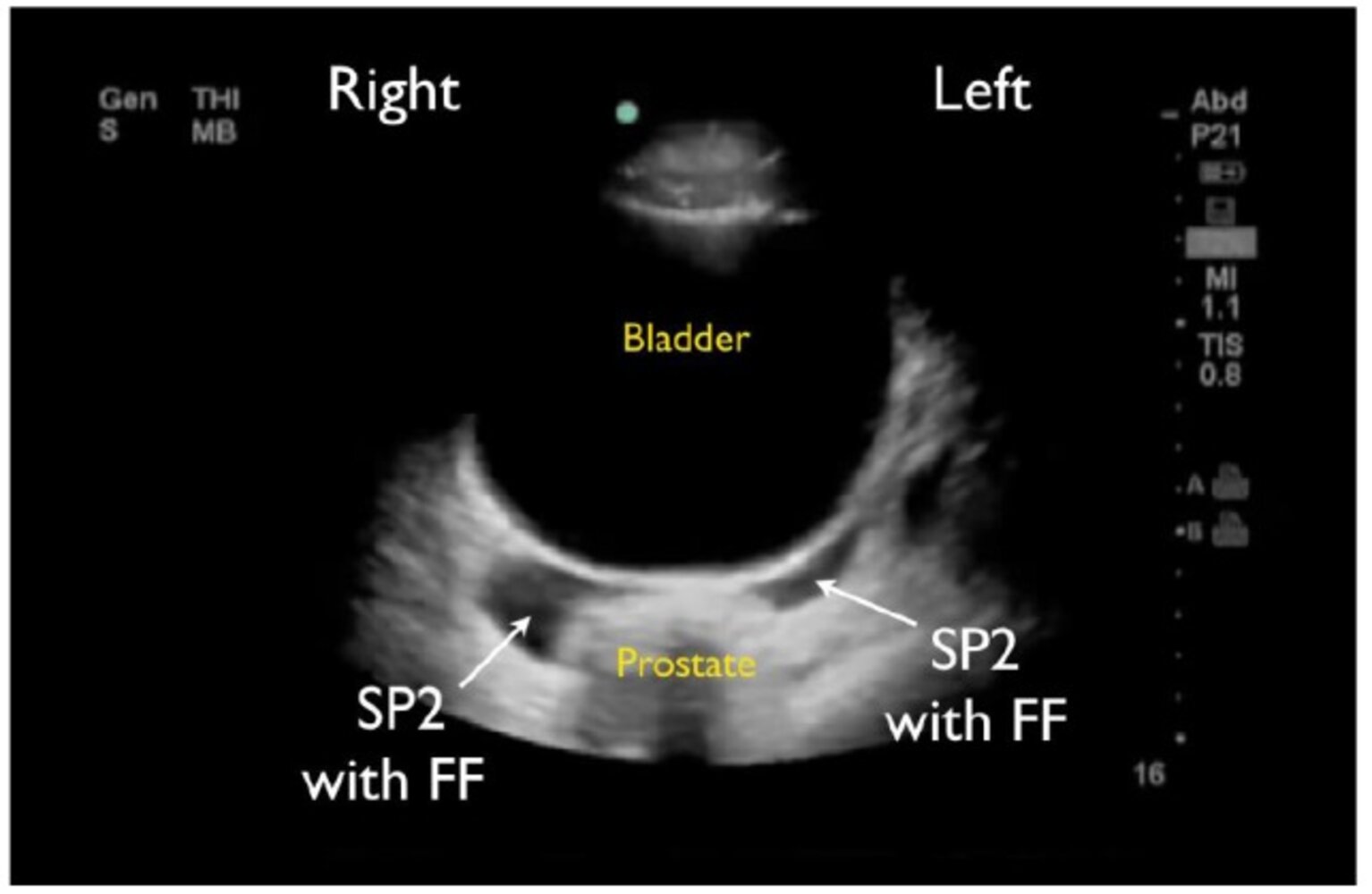
Ultrasound pelvis (suprapubic view; transverse plane)
Normal image shows free fluid (FF) in the space between the bladder and prostate gland (SP2).
Source: “Figure 8 in Caudal Edge of the Liver in the Right Upper Quadrant (RUQ) View Is the Most Sensitive Area for Free Fluid on the FAST Exam” by Lobo V, Hunter-Behrend M, Cullnan E et al., Western Journal of Emergency Medicine: Integrating Emergency Care with Population Health, licensed under CC BY 4.0.
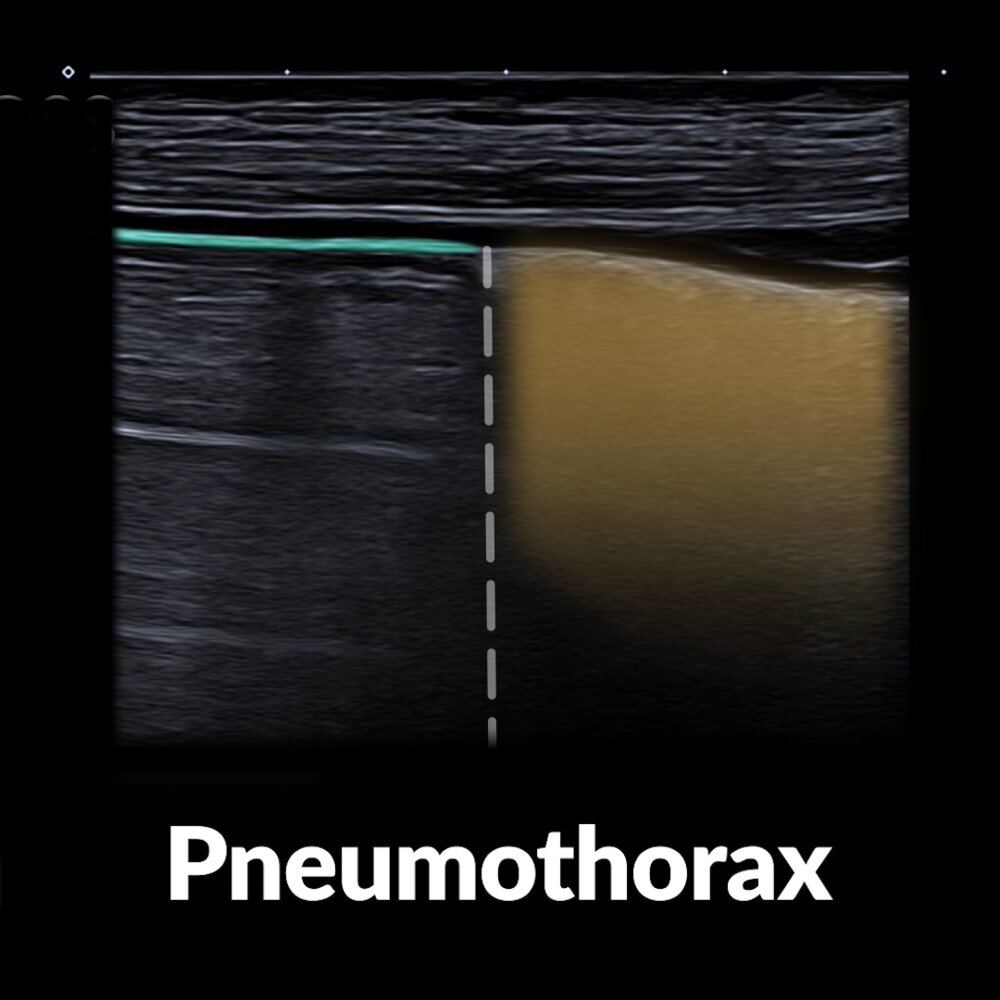
Short video of an ultrasound examination of the lungs in anterior thoracic (parasternal) transducer position (a marker indicates the probe position) showing a pneumothorax
At the location of a pneumothorax, normal lung sliding is abolished. The interface between the pneumothorax and adjacent sliding lung is known as the “lung point sign.” Pneumothorax on the left side in the video is identified by the presence of repetitive uniformly spaced horizontal lines (A-lines; reverberation artifact) deep to the pleural line (green overlay) and the absence of the normal B-lines that are visible in lung on the right. Although A-lines can be seen both in pneumothorax and normal lung tissue, B-lines are not seen in pneumothorax since they are generated from visceral pleura.
In M-mode, normal sliding lung appears as the seashore sign, in which the pleura and overlying chest wall are seen as horizontal echogenic waves and the lung has a grainy, sand-like appearance. In pneumothorax, lung sliding is abolished and the grainy appearance is replaced by parallel lines, which are termed the “barcode” or “stratosphere sign.”
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
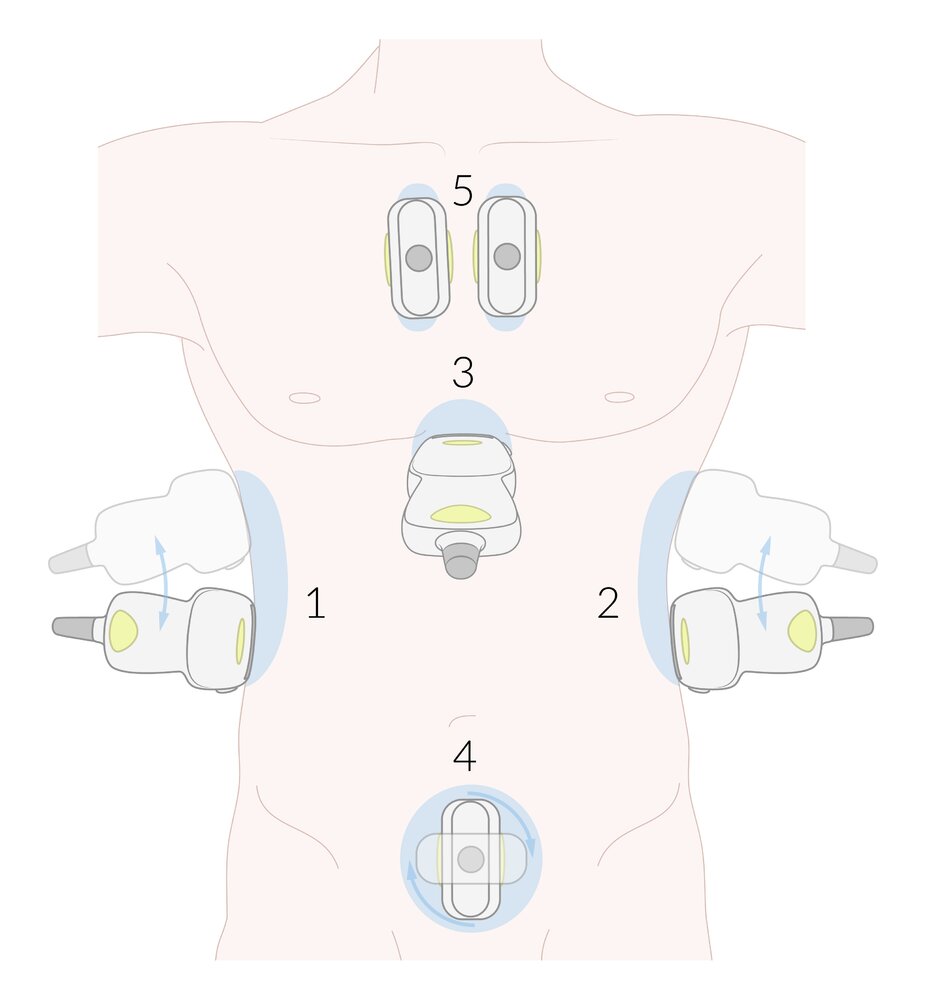
1. Right upper quadrant
Place the transducer over the right anterior axillary line along the subcostal margin or over the inferior intercostal spaces. Angle the transducer superiorly to assess the right costodiaphragmatic recess and right subphrenic space, and inferiorly to assess the hepatorenal space and inferior pole of the right kidney.
2: Left upper quadrant
Place the transducer over the left midaxillary line in one of the inferior intercostal spaces. Angle the transducer superiorly to assess the left costodiaphragmatic recess and left subphrenic space, and inferiorly to assess the splenorenal space and inferior pole of the left kidney.
3. Subxiphoid
Place the transducer in the subxiphoid space and tilt it up and toward the left shoulder to assess the pericardial space.
4. Pelvic
Place the transducer just above the pubic bone to assess the rectovesical space (♂) or rectouterine space (♀). Obtain transverse and longitudinal views.
5. Anterior thoracic
Place the transducer vertically over the 2nd or 3rd intercostal space along the midclavicular line on both sides. Sliding inferiorly may be necessary to appraise a sufficient number of intercostal spaces.
© AMBOSS
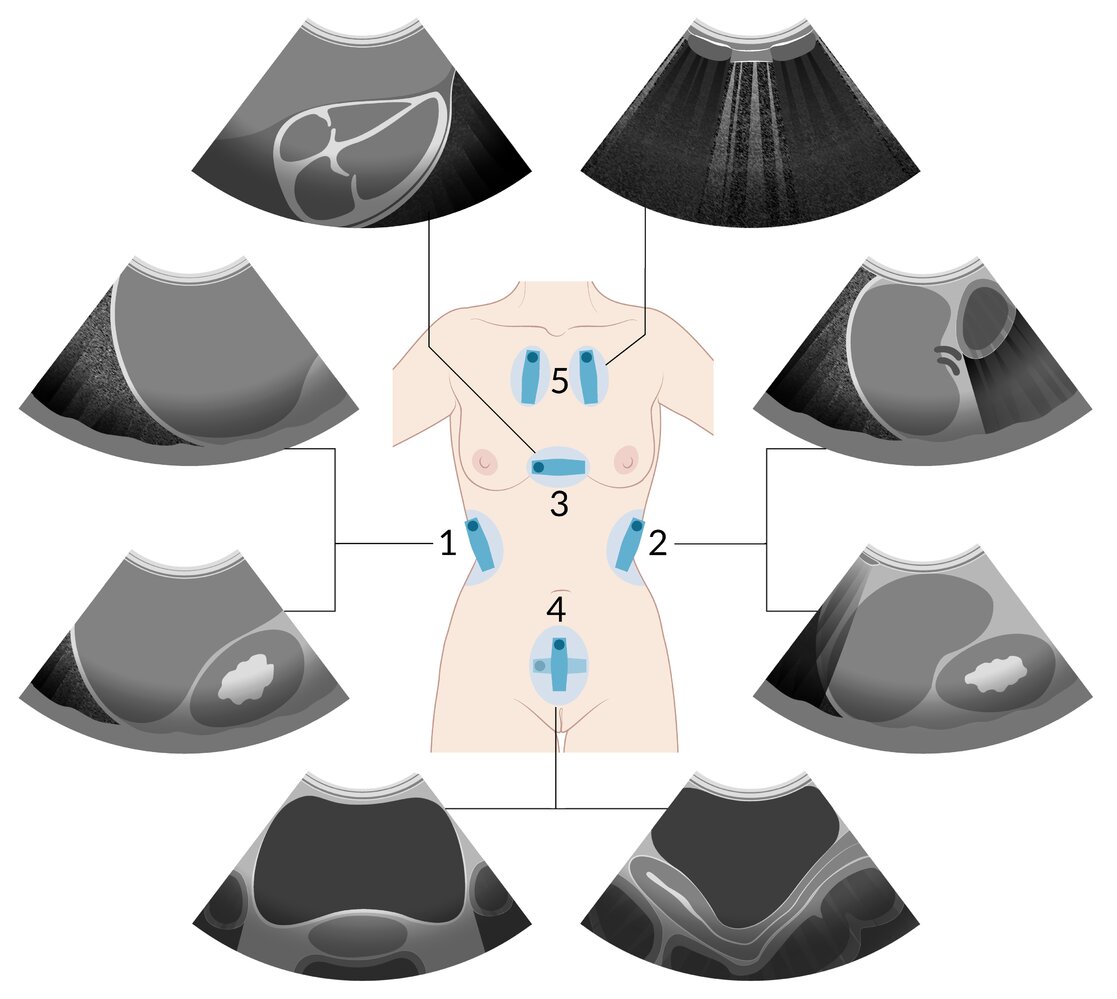
1: Right upper quadrant
– Right costodiaphragmatic recess
– Hepatorenal space
2: Left upper quadrant
– Left costodiaphragmatic recess
– Splenorenal space
3: Subxiphoid
– Pericardial space
4: Pelvic
– ♀: Rectouterine space
– ♂: Rectovesical space (not shown here)
5: Anterior thoracic
– Lung sliding
© AMBOSS
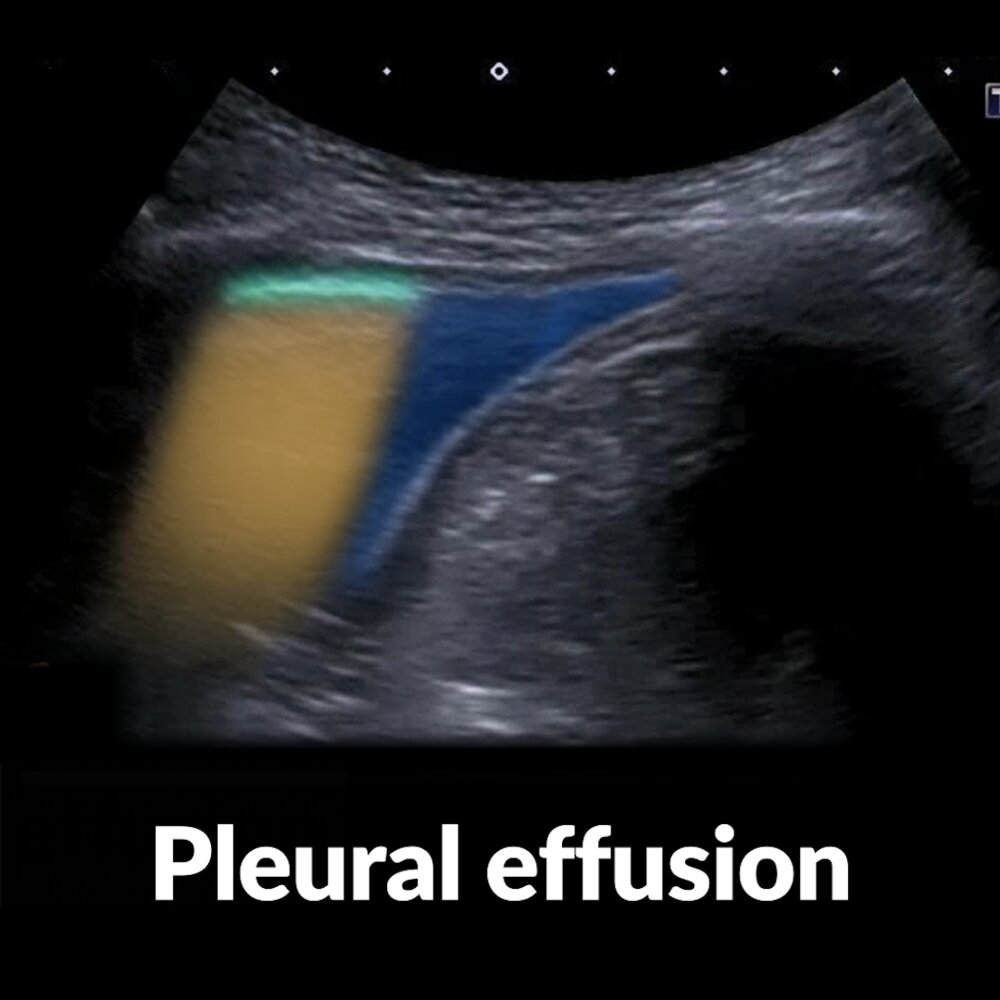
Short video of an ultrasound examination of the lower left hemithorax (a marker indicates the probe position) showing pleural effusion
An anechoic pleural effusion (blue overlay) is visible in the costodiaphragmatic recess (costophrenic sulcus) near the middle of the video. On the left side of the video, aerated lung is visible. Since ultrasound waves are not transmitted through normal aerated lung, the lung is recognized by to and fro movement of the hyperechoic pleural line (green overlay) during respiration and the presence of horizontal lines (A-lines; reverberation artifact; yellow overlay) deep to the pleural line.
A pleural effusion (collection of fluid in the pleural space between the lungs and the chest wall) is a pathological finding.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
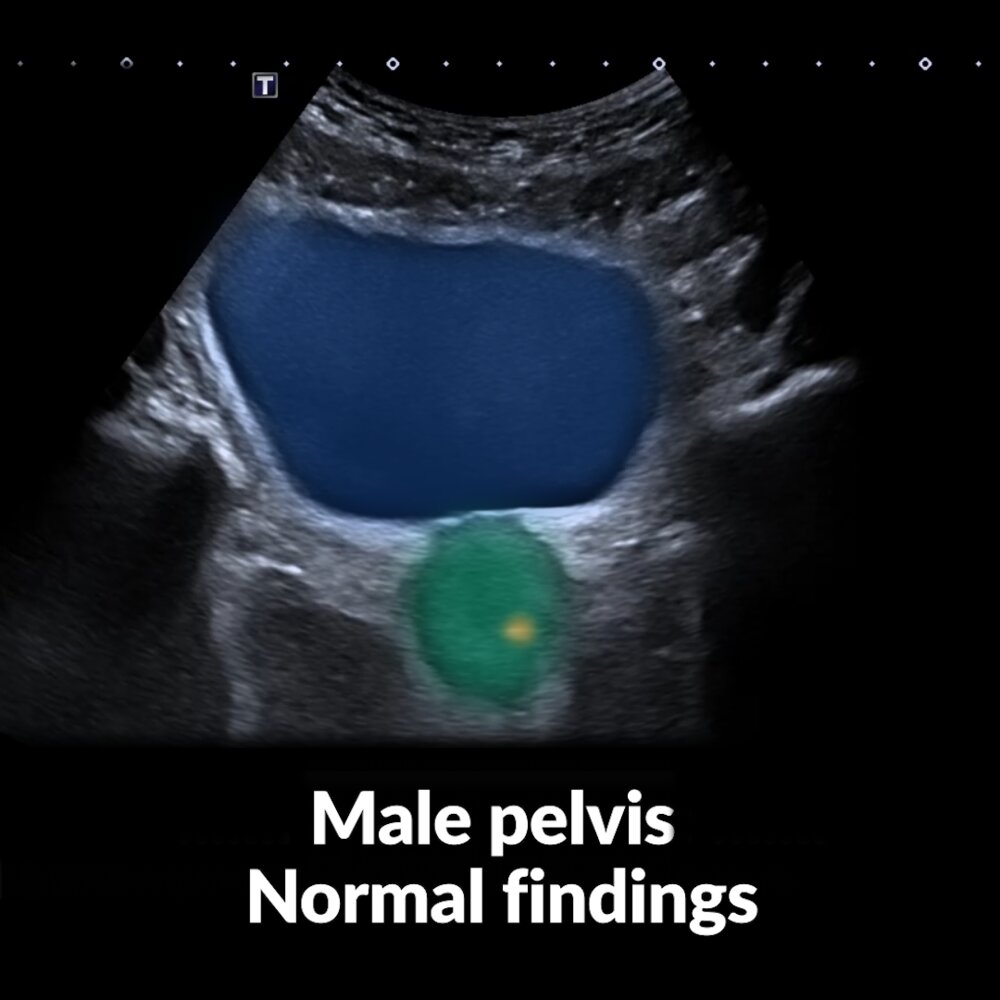
Short video of a lower abdomen ultrasound examination of the male pelvis in transverse and sagittal plane view (markers indicate the probe positions)
The first part of the video (transverse plane view) shows the bladder (blue overlay) and the inferior prostate (green overlay) with small calcifications (yellow overlay). Fanning the ultrasound beam cranially from this position (by tilting the transducer caudally) visualizes the paired seminal glands (red overlay).
In the second part of the video, the bladder (blue overlay) is still central in the sagittal plane view. Posterior to the bladder, the rectum (yellow overlay) and the prostate with the seminal glands (red overlay) can be seen, with the rectovesical pouch lying in-between (dashed green overlay)
The female analogue to the rectovesical pouch is the rectouterine pouch (of Douglas), which is located between the rectum and uterus. Examination of either pouch is performed to detect free fluid in the abdomen.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Disposition
Criteria for trauma team activation [1]
-
Mechanism of injury
- Falls from > 5 meters
- Impact from high-speed MVC
- Ejection from vehicle
- Any MVC > 18 mph (29 km/h) involving impact with a pedestrian, cyclist, or motorcyclist
- Death of a vehicle co-passenger
-
Specific injuries
- Injury to > 2 body regions
- Penetrating injury to the head, neck, torso, or proximal limb
- Traumatic amputation
- > 15% estimated BSA burns in adults or > 10% in children; or signs of airway involvement
- Airway obstruction
-
Physiological derangements
- Hypotension
- Tachycardia
- Bradypnea or tachypnea
- GCS < 14
-
Special patient groups
- Pregnant patients > 24 weeks' gestation with chest and/or abdominal injury
- Individuals > 70 years of age with chest injury
Specialty consults
Indications for urgent trauma surgeon consult [4]
At level 1 trauma centers, a trauma surgeon's presence at the bedside within 15 minutes of patient arrival is indicated for any of the following:
- Systolic BP < 90 mmHg
- GSW to neck, thorax, abdomen, pelvis, or proximal extremities
- Prehospital endotracheal intubation
- Intubation for respiratory failure
- GCS < 8 due to trauma
- Emergency physician discretion
Other specialists
Consult all specialists outside the trauma team responsible for managing identified injuries:
- Thoracic surgery: e.g., for operative cardiopulmonary injuries
- Neurosurgery: e.g., for TBI
- Orthopedics: e.g., for operative fractures
- OB-GYN and/or urology: e.g., for genitourinary trauma
- Plastic surgery: e.g., for extensive soft tissue injuries such as degloving, burns
- Vascular surgery: e.g., for major vessel injuries
- Interventional radiology: e.g., for angioembolization
- Others: hand surgery, oromaxillofacial surgery, spine surgery
Interfacility transfers
- Initiate the transfer process to a higher level trauma center as soon as the patient's needs exceed the capability of the current hospital.
- Transfer decision depends on multiple factors, e.g.:
- The patient's injuries
- Resources and equipment available at the current hospital
- Availability of consultant physicians
- Institutional and regional guidelines
- Transfer to a burn unit may also be indicated (see “Treatment of burns” for details).
An indication for trauma team activation is generally an indication that the patient requires transfer to a trauma center. [1]
Surgical admission
-
Operating room: transfer patients to the OR for operative management of critical findings.
- Traumatic brain injury: See “Management of moderate and severe TBI.”
- Thoracotomy: See “Resuscitative thoracotomy” and “Urgent thoracotomy.”
- Laparotomy: See “Emergency exploratory laparotomy.”
-
Trauma ICU
- Admit all hemodynamically unstable or intubated patients to critical care settings.
- Patients may require postoperative admission to ICU.
Discharge from emergency settings
- Most patients with major trauma require admission for treatment and observation.
- Consider discharge with outpatient follow-up for patients with all of the following after complete workup and observation:
- Only minor injuries (e.g., isolated fracture)
- Adequate analgesia
- Normal mental status
- Ability to function with ADLs and IADLs
- Good social supports
- No other indications for admission
Special patient groups
Trauma in pregnant individuals
Overview
| Overview of trauma in pregnancy | ||
|---|---|---|
| Maternal | Fetal | |
| Clinical features |
|
|
| Diagnostics |
|
|
| Management |
|
|
Avoid examining the mother in the supine position in order to avoid possible supine hypotensive syndrome.
The mother should be evaluated and treated before the fetus. Early and optimal diagnostics and trauma management of the mother is the best treatment for the fetus.
Epidemiology [30]
- Incidence: every 12th pregnant woman experiences trauma
- Trauma in pregnancy is the leading cause of nonobstetrical maternal death in the US.
Etiology [31][32]
- Unintentional trauma (e.g., due to falls, MVCs)
-
Intentional trauma:
- Intimate partner violence
- Assault
- Suicide attempt
Classification [33]
- Minor trauma (90%): trauma for which obstetrical surveillance suffices
- No abdominal involvement
- No rapid compression or deceleration
- No pain or vaginal bleeding
- No loss of fluid
- Normal fetal movement
- Major trauma (10%): trauma that requires further assessment in a trauma center
- Abdominal involvement with abdominal pain
- Signs and symptoms of internal bleeding
- Hematuria
- Vaginal bleeding and/or loss of fluid
- Loss of consciousness
- Rapid compression and/or deceleration
- Decreased fetal movement
Management of pregnant patients with trauma [1][34][35]
-
All pregnant trauma patients
- Begin initial resuscitation using the ABCDE approach.
- Assess for signs of abruption and uterine rupture.
- Perform a fetal status assessment.
- Consider imaging: ultrasound and/or CT (should not be deferred because of fetal radiation concerns)
- Obtain coagulation studies, including fibrinogen. [33]
- Order a Kleihauer-Betke test.
- Administer anti-D immunoglobulin for Rh-negative mothers.
- Consult OB/GYN if there is any concern for obstetric injuries.
-
Trauma patients > 20 weeks' gestation
- Initiate tocodynamometry for at least 4–6 hours.
- Continue monitoring for 24 hours if any of the following are present : [1][33]
- High-impact mechanism of injury
- ≥ 6 uterine contractions per hour
- Vaginal bleeding, significant abdominal pain, or uterine tenderness
- Rupture of the membranes
- Abnormal fetal heart rate pattern
- Maternal tachycardia (HR > 110/minute)
-
Further management
- Management of nonobstetric injuries as for nonpregnant patients
- Emergency delivery in consultation with OB/GYN if there is nonreassuring fetal status or maternal hemodynamic instability
- See also:
- “Management of placental abruption”
- “Management of uterine rupture”
- “Management of preterm labor”
Even minor trauma poses a risk for placental abruption. [34][36]
Complications
- Due to physiological changes during pregnancy
- Superior displacement of abdominal organs
- Increased risk of gastrointestinal injury from chest or upper abdominal trauma
- Increased risk of aspiration during intubation
- Decrease of blood pressure (by 15–20 mmHg only during 2nd trimester): increased risk of hypotensive complications (e.g., falls due to syncope) and missing pathological causes underlying hypotension
- Increase of the heart rate (by 15–20 bpm only during 3rd trimester): increased risk of complications from tachycardia (e.g., arrhythmias) and missing pathological causes underlying tachycardia
- Increase of blood volume: increased risk of overlooked blood loss
- Superior displacement of abdominal organs
- Placental abruption and preterm labor
- Fetal loss (60–70% caused by minor trauma, with placental abruption being the most common complication)
- Supine hypotensive syndrome following trauma (see “Supine hypotensive syndrome” in “Other complications” below)
- Uterine rupture and exsanguination
- Maternal death
Prevention
Screen all pregnant women for intimate partner violence; for more information see “Intimate partner violence.”
Trauma in older adults [1][37]
Common mechanisms of injury
- Falls [1]
- Impact from MVCs
- Burns
- Penetrating injuries
General principles
- Consider any physiological events that may have led to the trauma (e.g., cardiac arrhythmia leading to syncope and resulting in a fall).
- Determine medication effects.
- Assess for older adult abuse.
- Determine goals of care.
Geriatric modifications to the primary survey
-
Airway
- Loss of protective airway reflexes
- Dentures and arthritic changes may impede airway management.
-
Breathing
- Limited respiratory reserve with potential for rapid deterioration to respiratory failure
- At risk for respiratory failure following rib fractures; provide adequate analgesia and pulmonary toilet.
-
Circulation
- Patients with preexisting hypertension may appear normotensive, but this may represent a relatively hypotensive state (e.g., hemorrhagic shock).
- Use of cardiac medicine may blunt tachycardia.
- Consider advanced monitoring (e.g., central venous pressure, ECHO) during resuscitative efforts.
-
Disability
- Increased risk for TBI
- Cortical atrophy may delay signs of intracranial bleeding.
- More likely in patients taking anticoagulant and antiplatelet medications
- Preexisting neurological or psychiatric disease may impede evaluation.
- Increased risk for TBI
- Exposure: Loss of subcutaneous fat puts patients at risk for hypothermia, as well as pressure injury from immobilization.
Trauma in children [1]
Common mechanisms of injury
- MVCs [1]
- Drowning
- House fires
- Nonaccidental injury
- Falls
General principles
- Normal pediatric vital signs vary by age.
- Smaller body mass results in greater force applied per unit of body area, leading to a greater risk for multiple injuries than adults.
- Developmental age may hinder history and examination.
- Use Broselow tape to recommend common drug dosing and equipment sizes.
- Assess for red flags for child maltreatment.
- Practice judicious use of CT scans. [38]
Pediatric modifications to the primary survey [1]
-
Airway
- Proportionally larger head results in passive cervical spine flexion, which may obstruct the airway.
- Visualization during intubation is difficult.
- Shorter airway is located higher in the neck.
- Anterior attachment of vocal cords is located more inferiorly than the posterior attachment.
-
Breathing
- Higher normal respiratory rate than adults
- Use a pediatric bag-valve-mask for children < 30 kg.
-
Circulation
- Higher normal heart rate and lower normal blood pressure than adults
- Increased physiological reserve allows children to maintain normal systolic blood pressure during hemorrhagic shock.
- See also “Basic life support in infants and children.”
-
Disability
- Proportionally larger head leading to an increased risk of TBI
- Modified GCS may be used in children < 4 years of age.
- See also “PECARN blunt head-trauma prediction rule.”
- Exposure: at increased risk for accidental hypothermia because of greater body surface area to mass ratio than adults [39]
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
External Resources
- 2015 EAST guidelines: Patient selection for emergency department thoracotomy
- 2017 EAST guidelines: Damage control resuscitation in patients with severe traumatic hemorrhage
- 2014 ACS TQIP massive transfusion in trauma guidelines
- 2021 TCCC guidelines for medical personnel
- ACS TQP Best Practice Guidelines
- EAST- Landmark Papers in Trauma and Acute Care Surgery
- EAST Practice Management Guidelines
- Western Trauma Association Algorithms
- Western Trauma Association Algorithm publications
References
- American College of Surgeons and the Committee on Trauma. "ATLS Advanced Trauma Life Support". American College of Surgeons. (2018). ISBN: 9780996826235
- Pape HC, Lefering R, Butcher N, et al. "The definition of polytrauma revisited". J Trauma Acute Care Surg. 77(5). :780-786. (2014)
- Panchal AR, Bartos JA, Cabañas JG, et al. "Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care". Circulation. 142(16_suppl_2). (2020)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Spoelder EJ, Slagt C, Scheffer GJ, van Geffen GJ. "Transport of the patient with trauma: a narrative review". Anaesthesia. 77(11). :1281-1287. (2022)
- Newgard CD, Schmicker RH, Hedges JR, et al. "Emergency Medical Services Intervals and Survival in Trauma: Assessment of the “Golden Hour” in a North American Prospective Cohort". Ann Emerg Med. 55(3). :235-246.e4. (2010)
- Newgard CD, Meier EN, Bulger EM, et al. "Revisiting the “Golden Hour”: An Evaluation of Out-of-Hospital Time in Shock and Traumatic Brain Injury". Ann Emerg Med. 66(1). :30-41.e3. (2015)
- Mayglothling J, Duane TM, Gibbs M, et al. "Emergency tracheal intubation immediately following traumatic injury". J Trauma Acute Care Surg. 73(5). :S333-S340. (2012)
- Hatchimonji JS, Dumas RP, Kaufman EJ, et al. "Questioning dogma: does a GCS of 8 require intubation?". Eur J Trauma Emerg Surg. (2020)
- CRASH-2 trial collaborators., Shakur H, Roberts I, et al. "Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial". Lancet. 376(9734). :23-32. (2010)
- CRASH-2 collaborators., Roberts I, Shakur H, et al. "The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the CRASH-2 randomised controlled trial". Lancet. 377(9771). :1096-101, 1101.e1-2. (2011)
- Seamon MJ, Haut ER, Van Arendonk K, et al. "An evidence-based approach to patient selection for emergency department thoracotomy: A practice management guideline from the Eastern Association for the Surgery of Trauma.". The journal of trauma and acute care surgery. 79(1). :159-73. (2015)
- American College of Emergency Physicians. "Emergency ultrasound imaging criteria compendium". Ann Emerg Med. 48(4). :487-510. (2006)
- Caputo ND, Stahmer C, Lim G, Shah K. "Whole-body computed tomographic scanning leads to better survival as opposed to selective scanning in trauma patients". J Trauma Acute Care Surg. 77(4). :534-539. (2014)
- Henry R, Ghafil C, Pott E, et al. "Selective Computed Tomography (CT) Imaging is Superior to Liberal CT Imaging in the Hemodynamically Normal Pediatric Blunt Trauma Patient". J Surg Res. 266. :284-291. (2021)
- Gupta M, Schriger DL, Hiatt JR, et al. "Selective Use of Computed Tomography Compared With Routine Whole Body Imaging in Patients With Blunt Trauma". Ann Emerg Med. 58(5). :407-416.e15. (2011)
- Sierink JC, Treskes K, Edwards MJR, et al. "Immediate total-body CT scanning versus conventional imaging and selective CT scanning in patients with severe trauma (REACT-2): a randomised controlled trial". The Lancet. 388(10045). :673-683. (2016)
- Long B, April MD, Summers S, Koyfman A. "Whole body CT versus selective radiological imaging strategy in trauma: an evidence-based clinical review". Am J Emerg Med. 35(9). :1356-1362. (2017)
- "American College of Radiology ACR Appropriateness Criteria, Suspected Spine Trauma"
- Stojanovska J, Hurwitz Koweek LM, Chung JH, et al. "ACR Appropriateness Criteria® Blunt Chest Trauma-Suspected Cardiac Injury". J Am Coll Radiol. 17(11). :S380-S390. (2020)
- Henry TS, Donnelly EF, Boiselle PM, et al. "ACR Appropriateness Criteria® Rib Fractures". J Am Coll Radiol. 16(5). :S227-S234. (2019)
- Karmy-Jones R, Namias N, Coimbra R, et al. "Western Trauma Association Critical Decisions in Trauma". J Trauma Acute Care Surg. 77(6). :994-1002. (2014)
- Biffl WL, Harrington DT, Cioffi WG. "Implementation of a Tertiary Trauma Survey Decreases Missed Injuries". J Trauma. 54(1). :38-44. (2003)
- Pfeifer R, Pape HC. "Missed injuries in trauma patients: A literature review". J Patient Saf. 2(1). (2008)
- Stevens NM, Tejwani N. "Commonly Missed Injuries in the Patient with Polytrauma and the Orthopaedist’s Role in the Tertiary Survey". JBJS Reviews. 6(12). :e2-e2. (2018)
- Ferree S, Houwert RM, van Laarhoven JJEM, et al. "Tertiary survey in polytrauma patients should be an ongoing process". Injury. 47(4). :792-796. (2016)
- Stawicki S, Lindsey D. "Missed traumatic injuries: A synopsis". Int J Acad Med. 3(3). :13. (2017)
- Giannakopoulos GF, Saltzherr TP, Beenen LFM, et al. "Missed injuries during the initial assessment in a cohort of 1124 level-1 trauma patients". Injury. 43(9). :1517-1521. (2012)
- Banaste N, Caurier B, Bratan F, et al. "Whole-Body CT in Patients with Multiple Traumas: Factors Leading to Missed Injury". Radiology. 289(2). :374-383. (2018)
- Grossman NB. "Blunt trauma in pregnancy". Am Fam Physician. 70(7). :1303-10. (2004)
- Linda E. Saltzman, Christopher H. Johnson, Brenda Colley Gilbert, Mary M. Goodwin. "Physical Abuse Around the Time of Pregnancy: An Examination of Prevalence and Risk Factors in 16 States". Matern Child Health J. 7(1). :31-43. (2003)
- Krulewitch CJ, Pierre-Louis ML, de Leon-Gomez R, Guy R, Green R. "Hidden from view: violent deaths among pregnant women in the District of Columbia, 1988-1996". J Midwifery Womens Health. 46(1). :4-10. (2001)
- Jain V, Chari R, Maslovitz S, et al. "Guidelines for the Management of a Pregnant Trauma Patient". Journal of Obstetrics and Gynaecology Canada. 37(6). :553-571. (2015)
- Murphy NJ, Quinlan JD. "Trauma in pregnancy: assessment, management, and prevention". Am Fam Physician. 90(10). :717-22. (2014)
- Greco PS, Day LJ, Pearlman MD. "Guidance for Evaluation and Management of Blunt Abdominal Trauma in Pregnancy". Obstet Gynecol. 134(6). :1343-1357. (2019)
- Jafari Kafiabadi M, Sabaghzadeh A, Khabiri SS, et al. "Orthopedic Trauma During Pregnancy; a Narrative Review". Arch Acad Emerg Med. 10(1). :e39. (2022)
- Tintinalli JE, Stapczynski JS, Ma OJ, et al. "Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9th edition". McGraw Hill Professional. (2019). ISBN: 9781260019940
- "Avoid the routine use of whole-body CT scanning (pan-scanning) in pediatric trauma patients". https://www.choosingwisely.org/clinician-lists/aap-sosu-avoid-routine-use-of-whole-body-ct-scanning-in-trauma-patients/. [2019-11-04]
- McDaniel L. "Hypothermia and Cold Injury in Children". Pediatr Rev. 43(1). :58-60. (2022)