Summary
Maternal complications during pregnancy include metabolic conditions, hemorrhage, infectious diseases, and dermatologic conditions. Hyperemesis gravidarum is a severe form of nausea and vomiting in pregnancy characterized by ketonuria and weight loss and typically requires inpatient admission, IV fluid hydration, and antiemetic therapy. Cervical insufficiency refers to the inability of the cervix to retain a pregnancy in the second trimester in the absence of labor, contractions, or other pathologies; cervical cerclage may be required. Pregnancy dermatoses are pruritic conditions that occur during pregnancy or in the immediate postpartum period and include gestational pemphigoid and polymorphic eruption of pregnancy. Other maternal complications of pregnancy include hypertensive pregnancy disorders, pregnancy-associated liver diseases, and gestational diabetes.
See also “Common discomforts during pregnancy.”
Overview
Metabolic complications
-
Hypertensive pregnancy disorders
- Gestational hypertension
- Preeclampsia
- Eclampsia
- Gestational diabetes
-
Pregnancy-associated liver diseases
- Hyperemesis gravidarum
- HELLP syndrome
- AFLP
- Cholestasis of pregnancy
Hemorrhagic complications
-
First trimester: See “Vaginal bleeding.”
- Spontaneous abortion
- Ectopic pregnancy
- Second and third trimester: See “Antepartum hemorrhage.”
- Placenta previa
- Abruptio placentae
- Uterine rupture
- Other: Fetomaternal hemorrhage
Infectious complications
- Chorioamnionitis
- UTI in pregnancy
- Sexually transmitted infections (e.g., pelvic inflammatory disease in pregnancy)
Other complications
- Pregnancy dermatoses
- Pregnancy luteoma
| Overview of maternal complications during pregnancy | |||||
|---|---|---|---|---|---|
| Risk factors | Clinical features | Diagnostics | Management | ||
| Uncomplicated nausea and vomiting of pregnancy |
|
|
|
|
|
| Hyperemesis gravidarum |
|
|
|
||
| Cervical insufficiency |
|
|
|
|
|
| Trauma in pregnancy | Maternal |
|
|
|
|
| Fetal |
|
|
|
||
Hyperemesis gravidarum
- Definition: severe, persistent nausea and vomiting associated with a > 5% loss of prepregnancy weight and ketonuria with no other identifiable cause [2]
-
Risk factors
- Multiple gestation
- Hydatidiform mole
- Nulliparity
- Migraine headaches
- GERD
-
Clinical features
- Nausea, vomiting
- Physical signs of dehydration
- Hypersalivation,
- Orthostatic hypotension
- Malnourishment
-
Diagnostics
- Clinical diagnosis
-
Laboratory analysis
- Electrolyte disturbances: hypokalemia and hypochloremic metabolic alkalosis or metabolic acidosis [3]
- Signs of dehydration (e.g., ↑ hematocrit)
- Ketonuria
-
Treatment
-
Antiemetic therapy: See “Antiemetic therapy for nausea and vomiting of pregnancy.” [2]
- May require glucocorticoid therapy (see stepwise approach above)
- IV fluid resuscitation/replacement (see IV fluid therapy)
- Electrolyte and thiamine repletion
- Enteral feeding or TPN is recommended in patients with persistent symptoms and weight loss despite antiemetic therapy. [2]
-
Antiemetic therapy: See “Antiemetic therapy for nausea and vomiting of pregnancy.” [2]
-
Complications [4][5]
- Maternal
- Hypokalemia
- Wernicke encephalopathy
- Fetal
- Intrauterine growth restriction
- Low birth weight
- Preterm birth
- Maternal
-
Acute management checklist for hyperemesis gravidarum [2][6][7][8]
- Rule out alternate etiologies (see differential diagnosis of nausea and vomiting).
- Identify and treat dehydration (see IV fluids).
- Thiamine repletion
- Electrolyte repletion
- IV antiemetic therapy (see antiemetic therapy for nausea and vomiting of pregnancy)
- Consider enteral tube feeding (nasogastric/nasoduodenal) or TPN.
- Closely monitor vitals and urine output.
- Monitor urine ketones, BMP, and body weight daily.
- Inpatient admission
- Consult OB/GYN.
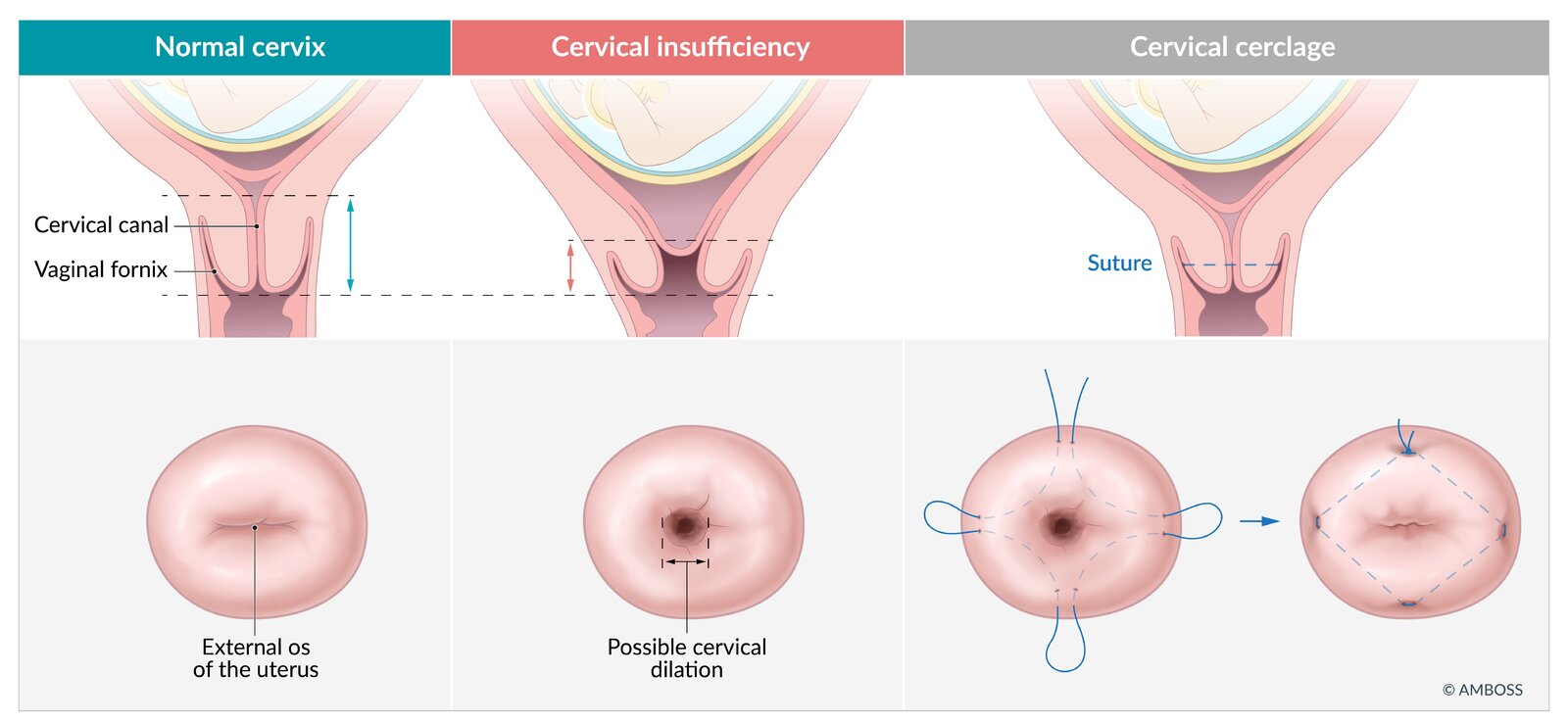
Cervical insufficiency
Definition
Cervical insufficiency is the inability of the cervix to retain a pregnancy in the second trimester in the absence of contractions, labor, or other underlying pathologies (e.g., infection, bleeding, premature rupture of membranes).
Etiology
Most cases of cervical insufficiency are idiopathic.
Risk factors [9]
- Previous midtrimester pregnancy loss or preterm birth
- Previous obstetric or gynecological trauma (e.g., termination of pregnancy, precipitous labor, multiple gestations, conization)
- Short cervical length: transvaginal cervical length < 25 mm on ultrasound before 24 weeks' gestation
- Cervical connective tissue weakness (e.g., Ehler-Danlos syndrome)
- Diethylstilbestrol exposure
Clinical features
- Painless cervical dilation with or without prolapsed membranes
- Nonspecific findings
- Pelvic cramps, back pain
- Vaginal discharge: ↑ volume, yellow or blood-stained, and/or thinner consistency
Diagnosis
- Clinical diagnosis in individuals with painless cervical dilation before 24 weeks' (may be up to 28 weeks') gestation or a history of second-trimester preterm birth or pregnancy loss related to painless cervical dilation
- A short cervical length is not diagnostic of cervical insufficiency.
- Some experts make a diagnosis of cervical insufficiency in patients with a short cervical length before 24 weeks' gestation in the current pregnancy if they have a history of ≥ 1 preterm birth or pregnancy loss related to cervical dilation between 16 and 36 weeks' gestation. [9][10]
Management of cervical insufficiency and short cervical length [11]
- In women with risk factors (e.g., previous preterm birth): serial cervical ultrasound monitoring between 16 and 24 weeks' gestation
- Intravaginal progesterone should be considered if the patient has a short cervical length.
-
Cervical cerclage ; [10][12][13]
- Definition: placement of a supportive suture in the cervicovaginal junction to prevent early pregnancy loss and preterm birth
- Methods
- McDonald cerclage: a surgical procedure performed to prevent preterm birth in women with cervical insufficiency that involves placing a suture in the cervix, typically using a transvaginal approach, to reinforce cervical closure; usually removed between 36 and 37 weeks' gestation or at the onset of preterm labor.
- Shirodkar cerclage: a surgical procedure during which a suture is placed in the cervical submucosal tissue to treat cervical insufficiency; usually removed between 36 and 37 weeks' gestation or at the onset of preterm labor (can be left in place if cesarean delivery is planned).
- Timing: < 24 weeks' gestation; most commonly performed at 13–16 weeks' gestation
-
Indications
- Cervical dilation at < 24 weeks' gestation
- Singleton pregnancy with a short cervical length before 24 weeks' gestation and a history of preterm birth or pregnancy loss
- Prior cerclage due to cervical insufficiency at < 24 weeks' gestation
- Can be considered in a singleton pregnancy without a history of preterm birth if cervical length is < 10 mm before 24 weeks' gestation
-
Contraindications
- Preterm labor
- Premature rupture of membranes
- Chorioamnionitis or vaginal infection
- ≥ 24 weeks' gestation
- Unexplained vaginal bleeding
- Strict bed rest, intramuscular progesterone injections, and cervical pessaries are not recommended.
A shortened cervical length is not sufficient to diagnose cervical insufficiency.

© AMBOSS
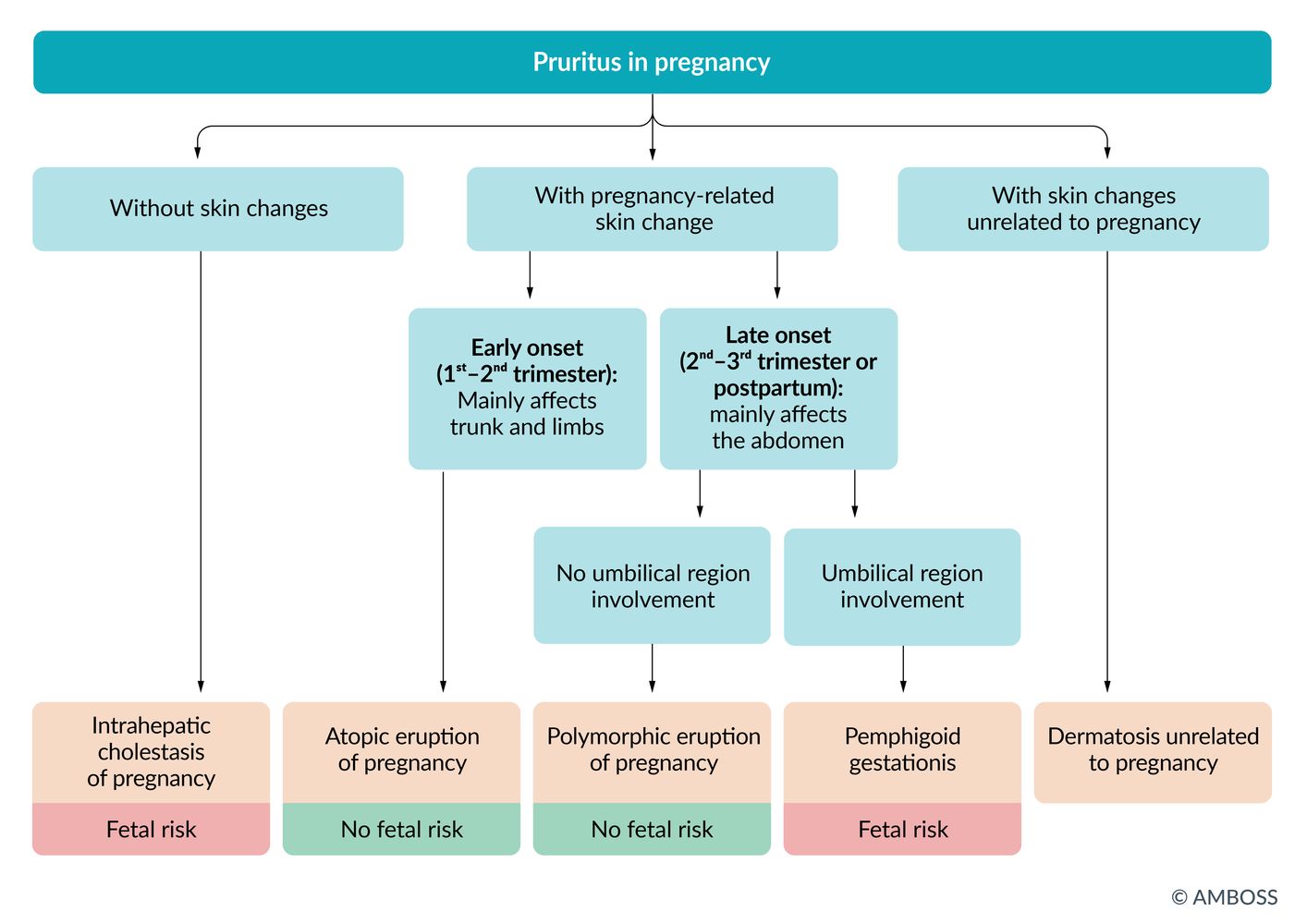
Pregnancy dermatoses
Pregnancy dermatoses include gestational pemphigoid, polymorphic eruption of pregnancy, and intrahepatic cholestasis of pregnancy.
Pemphigoid gestationis [14]
- Definition: bullous, pemphigoid-like dermatosis during pregnancy of unknown cause (most likely immunological)
- Epidemiology: 1:50,000 pregnancies (in the US)
-
Clinical features
- Commonly starts in the periumbilical region during the 2nd and 3rd trimester
- Intensely pruritic, mostly nonblistering lesions (eczema, urticarial or papular lesions) on extremities and mucous membranes
- Grouped vesicles with herpetiform appearance (“gestational herpes”) usually occur as the disease advances.
- Diagnosis: The diagnosis is confirmed via biopsy and immunofluorescence.
- Treatment: glucocorticoids (topical or systemic) at the lowest dose needed to control disease [15]
-
Prognosis
- Usually self-limited; heals spontaneously after delivery, ; but associated with complications (e.g., premature labor, ; increased lifetime risk of autoimmune disease)
- Recurrence is possible, especially appearing:
- Spontaneously in the postpartum period
- In subsequent pregnancies
- When taking contraceptives containing progestin or estrogen
- During menstruation
- Infants born to women with gestational pemphigoid can develop transient blistering that resolves spontaneously.


Polymorphic eruption of pregnancy (PEP)
- Description: A benign, inflammatory condition that most commonly affects primiparous women in the third trimester of pregnancy or immediately postpartum.
- Epidemiology: relatively common, occurring in ∼ 1:160 pregnant patients [16]
-
Clinical features
- Very pruritic, erythematous papules within abdominal striae
- Lesions can spread to the chest, back, and extremities, and coalesce into urticarial plaques, sparing the face, palms, and soles
- Lesions last 4–6 weeks and resolve spontaneously [17]
-
Differential diagnosis: gestational pemphigoid
- The early stages of PEP are similar to gestational pemphigoid.
- However, PEP typically begins in the striae (with periumbilical sparing), while the lesions in gestational pemphigoid are located periumbilical.
- Management: topical corticosteroids

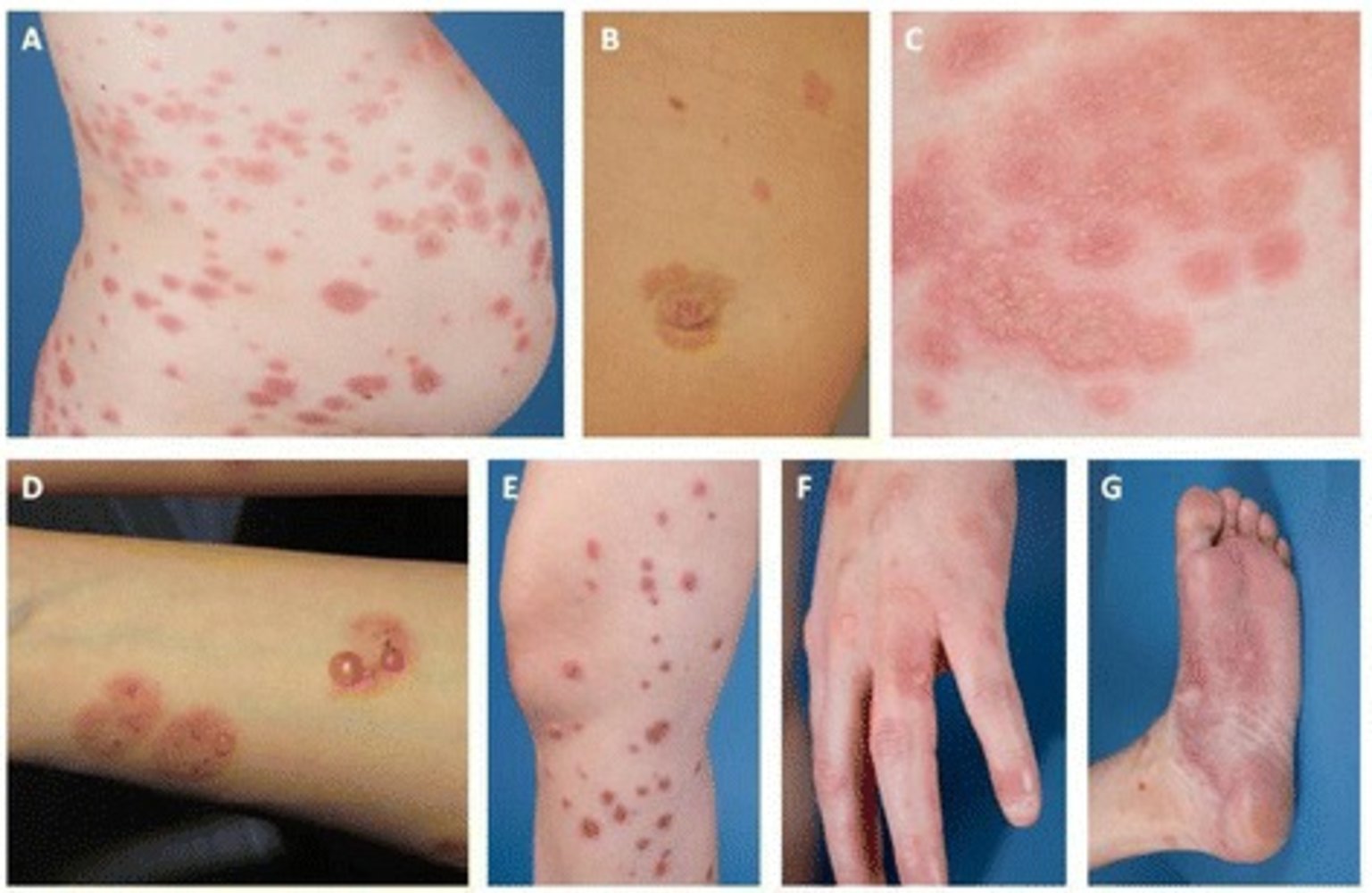
(A) Truncal urticarial papules and plaques
(B) Periumbilical plaque with two additional lesions above the navel
(C) Multiple vesicular plaques
(D) Plaques on the forearm with sporadic bullae
(E) Multiple, nonconfluent, erythematous plaques on the upper and lower leg
(F) Multiple, vesicular plaques on the left hand
(G) Large plaque of the left sole of the foot with sporadic bullae
Source: “Figure 1: Skin findings of gestational pemphigoid. in: "Gestational pemphigoid"” by Kaarin Mäkikallio, Kaisa Tasanen, Laura Huilaja, Orphanet Journal of Rare Diseases, licensed under CC BY 4.0.
© AMBOSS

Linear hyperpigmentation that runs vertically down the midline of the abdomen (linea nigra) is visible. This physiological change is commonly seen in the first trimester of pregnancy. In addition, an erythematous, urticarial rash with papules and plaques is visible in the periumbilical upper thigh region (polymorphic eruption of pregnancy).
Source: Courtesy of Dr. Gary M. White, MD
Pregnancy luteoma
- Definition: rare, benign tumors that arise in response to elevated hormone levels (e.g., β-hCG) during pregnancy
-
Clinical features
- The majority of patients are asymptomatic.
- Occasionally, they are functionally active (i.e., cause androgen hypersecretion) and manifest with symptoms of virilization of the mother or the fetus.
-
Diagnostics
-
Pelvic ultrasound
- Solid adnexal mass
- Can be unilateral or bilateral
- Significant venous or arterial flow
- 4–10 cm in diameter
- Luteomas are often diagnosed incidentally during cesarean delivery.
-
Pelvic ultrasound
-
Treatment
- Observation
- Most regress spontaneously postpartum.
External Resources
References
- Committee on Practice Bulletins-Obstetrics. "ACOG Practice Bulletin No. 189: Nausea And Vomiting Of Pregnancy". Obstet Gynecol. 131(1). :e15-e30. (2018)
- Gabra A, Habib H, Gabra M. "Hyperemesis Gravidarum, Diagnosis, and Pathogenesis". Critical Care Obstetrics and Gynecology. 05(01). (2019)
- Jennings LK, Krywko DM. "Hyperemesis Gravidarum". StatPearls. (2021)
- Petry CJ, Ong KK, Beardsall K, et al. "Vomiting in pregnancy is associated with a higher risk of low birth weight: a cohort study". BMC Pregnancy Childbirth. 18(1). (2018)
- Wegrzyniak LJ, Repke JT, Ural SH. "Treatment of hyperemesis gravidarum". Reviews in obstetrics & gynecology. 5(2). :78-84. (2012)
- Quigley EMM, Hasler WL, Parkman HP. "AGA technical review on nausea and vomiting". Gastroenterology. 120(1). :263-286. (2001)
- Quinlan JD, Hill DA. "Nausea and vomiting of pregnancy". Am Fam Physician. 68(1). :121-128. (2003)
- ROMAN A, SUHAG A, BERGHELLA V. "Overview of Cervical Insufficiency: Diagnosis, Etiologies, and Risk Factors". Clin Obstet Gynecol. 59(2). :237-240. (2016)
- American College of Obstetricians and Gynecologists. "Practice Bulletin No. 142: Cerclage for the Management of Cervical Insufficiency". Obstet Gynecol. 123(2). :372-379. (2014)
- Norwitz ER, Saade GA, Miller HS, Davidson CM. "Obstetric Clinical Algorithms". Wiley-Blackwell. (2016). ISBN: 1118849906
- Ressel GW. "ACOG Releases Bulletin on Managing Cervical Insufficiency". Am Fam Physician. 69(2). :436-439. (2004)
- ACOG. "Prediction and Prevention of Spontaneous Preterm Birth, Practice Bulletin 234". Obstet Gynecol. 138(2). :e65-e90. (2021)
- Huilaja L, Mäkikallio K, Tasanen K. "Gestational pemphigoid". Orphanet J Rare Dis. 9(1). (2014)
- Amber KT, Murrell DF, Schmidt E, Joly P, Borradori L. "Autoimmune Subepidermal Bullous Diseases of the Skin and Mucosae: Clinical Features, Diagnosis, and Management". Clin Rev Allergy Immunol. 54(1). :26-51. (2017)
- Vaughan Jones SA, Black MM. "Pregnancy dermatoses.". J Am Acad Dermatol. 40(2 Pt 1). :233-41. (1999)
- Ambros-Rudolph CM. "Dermatoses of pregnancy.". Journal der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology : JDDG. 4(9). :748-59; quiz 760-1. (2006)
- Grossman NB. "Blunt trauma in pregnancy". Am Fam Physician. 70(7). :1303-10. (2004)
- Masarie K, Katz V, Balderston K. "Pregnancy luteomas". Obstet Gynecol Surv. 65(9). :575-582. (2010)