Summary
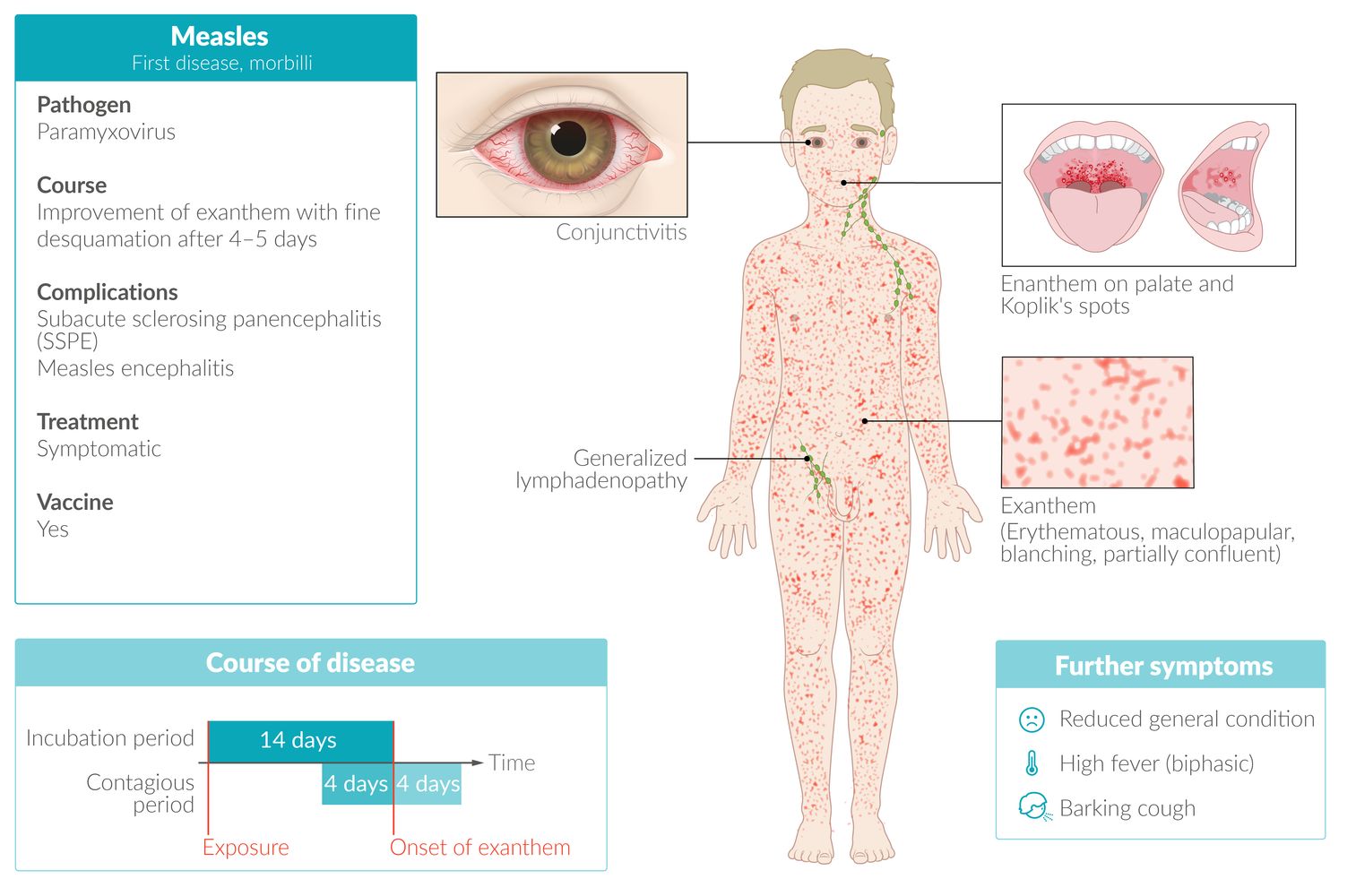
Measles (rubeola) is a highly infectious disease caused by the measles virus. There are three phases of disease: a prodromal stage, an exanthem stage, and a recovery stage. The prodromal stage is characterized by a high-grade fever with conjunctivitis, coryza, cough, and pathognomonic Koplik spots on the buccal mucosa. The exanthem stage is characterized by an erythematous maculopapular rash that originates at the hairline and spreads from the face and neck to the rest of the body. The combination of RT-PCR and serology for measles-specific IgM antibodies is preferred to confirm active disease. Treatment is supportive, including vitamin A supplementation to decrease the risk of complications. Prognosis is usually good, but measles may lead to complications such as subacute sclerosing panencephalitis, encephalitis, otitis, or pneumonia; complications are most common in young children, adults, and immunocompromised individuals. Postexposure prophylaxis is available. Routine immunization with the MMR vaccine or MMRV vaccine is recommended for all children and for adults without evidence of immunity.

© AMBOSS
Epidemiology
- Distribution: Measles typically occurs in regions with low vaccination rates and in resource-limited countries. [1]
- Peak incidence: < 12 months of age [1]
-
Risk factors for measles, mumps, and/or rubella: The following individuals are at increased risk of acquiring or transmitting measles, mumps, and/or rubella. [2][3][4]
- College students
- Health care personnel
- International travelers
- Individuals with HIV
- Household or close contacts of immunocompromised individuals
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Pathogen: measles virus (MV), an RNA virus of the Morbillivirus genus belonging to the Paramyxoviridae family
- Route of transmission: direct contact with or inhalation of virus-containing droplets [1]
-
Infectivity [1]
- ∼ 90%
- Highly contagious 4 days before and up to 4 days after the onset of exanthem. .
- Incubation period: ∼ 2 weeks after infection
Clinical features
Prodromal stage [5][6][7]
- Duration: ≤ 7 days [6]
-
Presentation
- Coryza, cough, and conjunctivitis
- Fever that gradually increases to ≤ 40.6°C (≤ 105°F) [6]
-
Koplik spots
- Pathognomonic maculopapular enanthem of the buccal mucosa
- Several tiny white or blue-white spots on an irregular erythematous background [8]
- Manifest 1–2 days before the exanthem stage [6]
The most important findings of measles are the 3 Cs and 1 K: Coryza, Cough, Conjunctivitis, and Koplik spots.


Exanthem stage [5][6][7]
- Duration: develops 3–7 days after the prodromal stage and lasts 4–7 days [5]
-
Presentation
-
Erythematous maculopapular rash that is initially blanching and can be confluent on the face and upper body ; [8]
- Begins behind the ears along the hairline
- Disseminates from the head to the rest of the body (palm and sole involvement is rare)
- Recedes in the same order as it appeared
- Desquamation may occur.
- Generalized lymphadenopathy
- Anorexia
-
Erythematous maculopapular rash that is initially blanching and can be confluent on the face and upper body ; [8]






Recovery stage
Cough may persist for up to 10 days. [8]
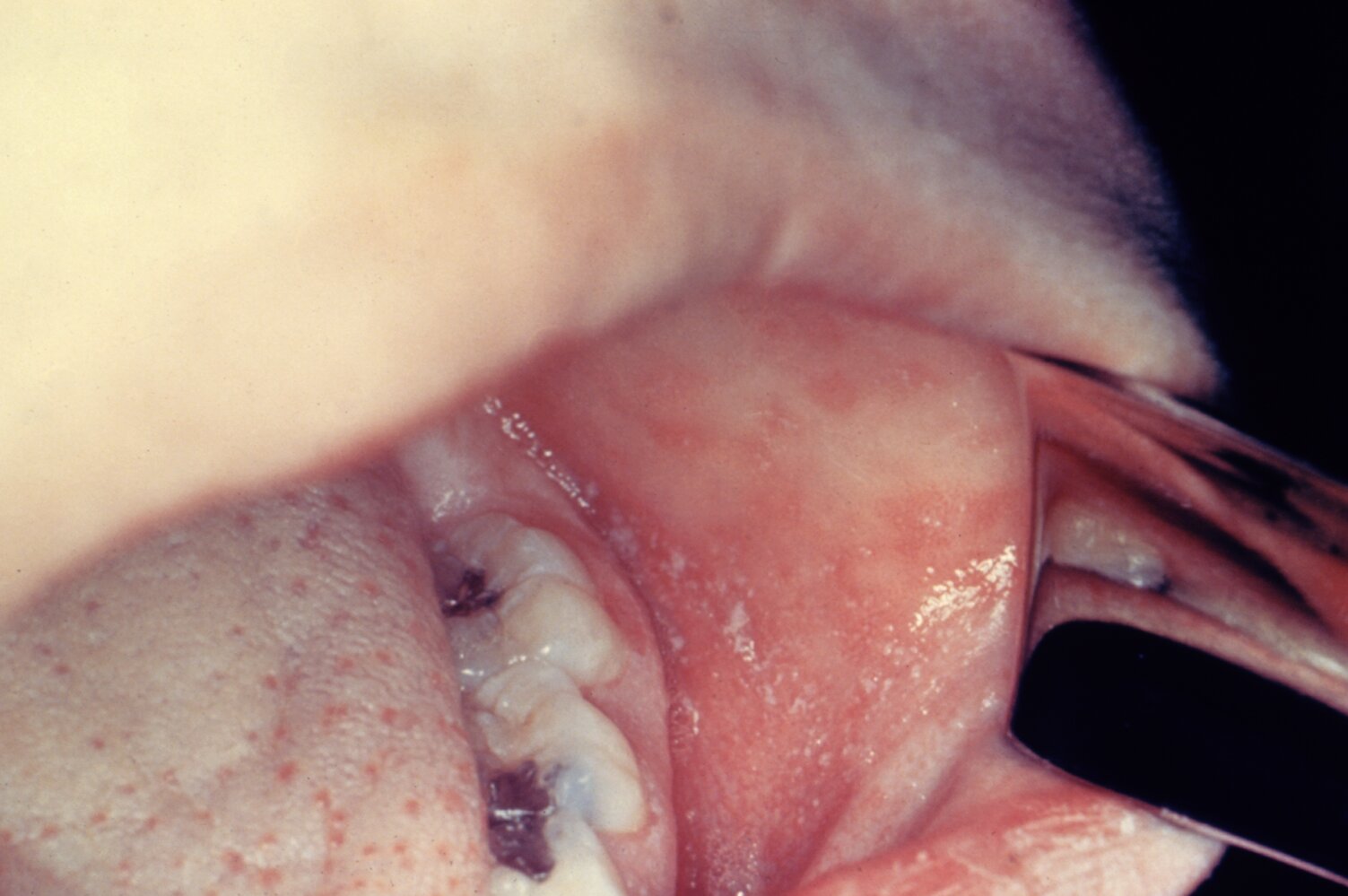
Numerous tiny white spots on an erythematous background (Koplik spots; examples indicated by arrowheads) are visible on the buccal mucosa.
Koplik spots are pathognomonic for measles infection.
This image is an adaptation. Source of original image: Centers for Disease Control and Prevention (CDC). Original title: “ID#4500”. Created by: CDC. Licensed under Public Domain. Modifications to original image: Image turned.
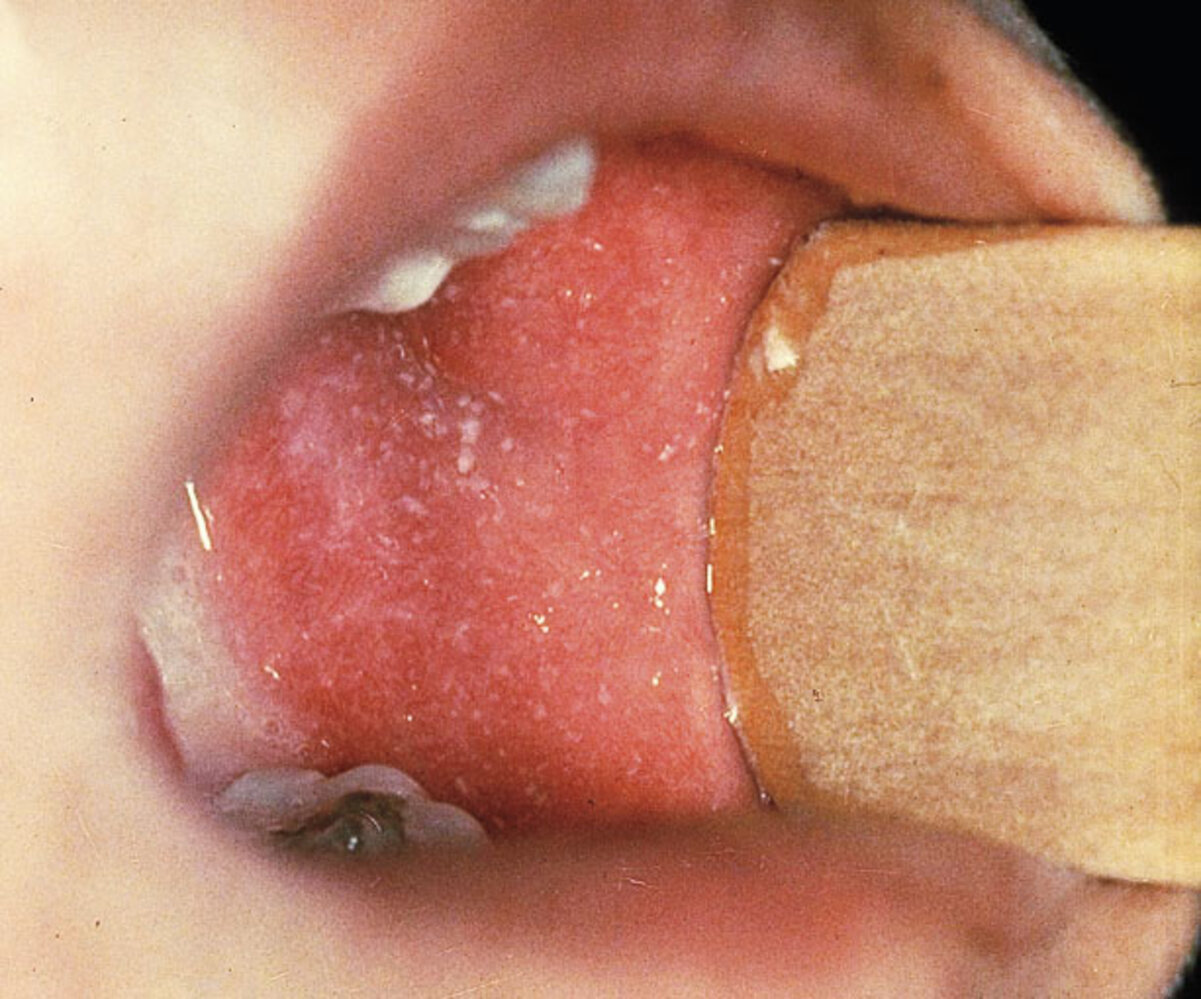
Koplik spots c/w measles
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.

Photograph of a toddler
There is a generalized erythematous maculopapular exanthem. Some confluence is visible (e.g., on the upper thighs).
Source: "Measles rash PHIL", Centers for Disease Control and Prevention, Atlanta,USA, Centers for Disease Control and Prevention licensed under Public Domain
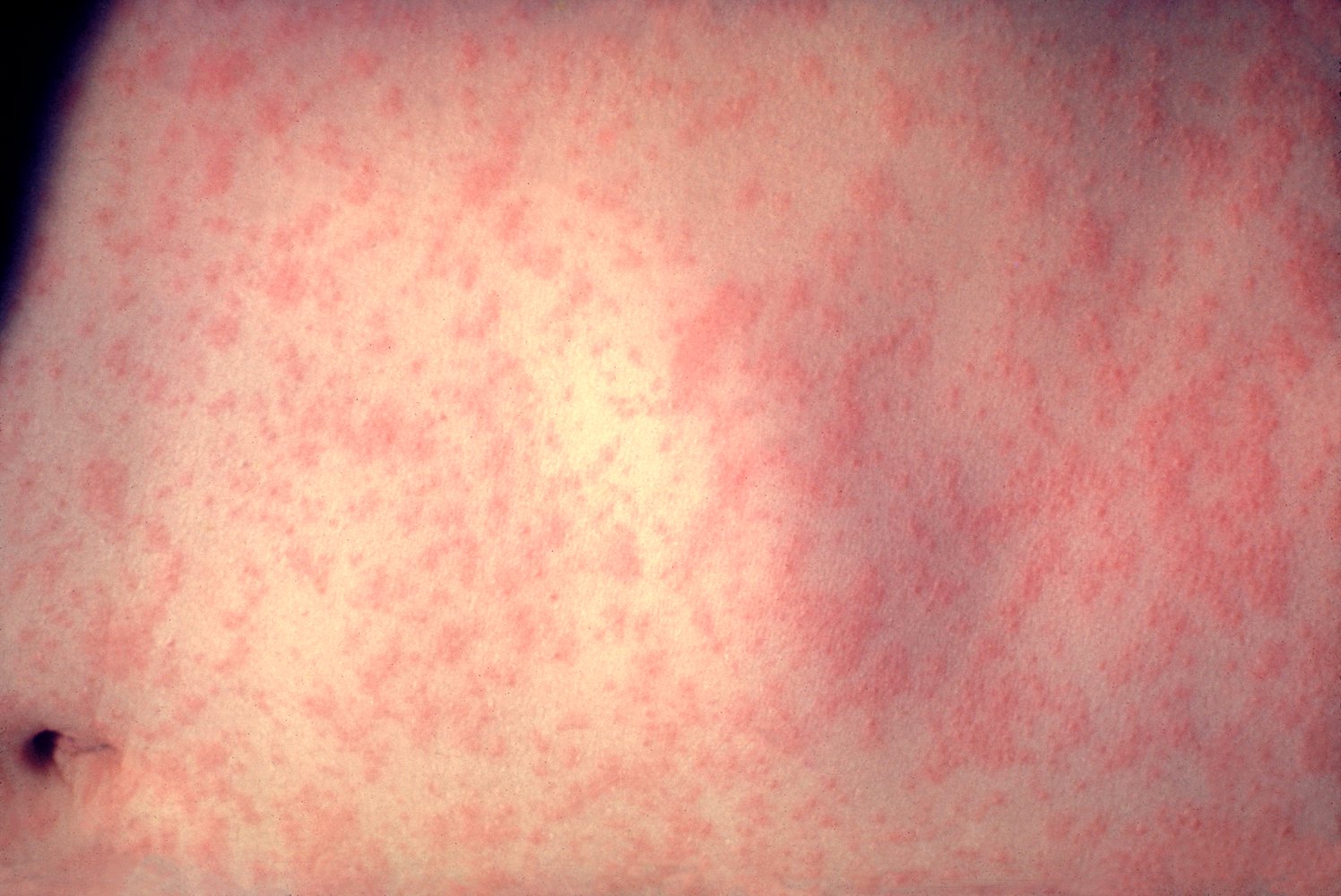
A widespread maculopapular rash is visible across the abdomen.
Source: "ID#: 3168", CDC/ Heinz F. Eichenwald, MD, Centers for Disease Control and Prevention (CDC) licensed under Public Domain

Multiple maculopapular blanching and partially confluent patches are disseminated over the head, neck, and back of this young patient.
These findings are consistent with a desquamating rash, which can occur after fading of the first erythematous exanthema, caused by an infection with the measles virus.
Source: “Figure 34, In: Atlas of Paediatric HIV Infection” by Regina E. Oladokun, Rannakoe J. Lehloenya, Carol Hlela et.al., Openbooks, licensed under CC BY-ND 4.0.

A partially confluent maculopapular exanthem is visible on the child's back.
In combination with the characteristic clinical features, these skin findings are suggestive of measles.
Source: "Measles in African Child 3", Mike Blyth, Wikimedia Commons licensed under Public Domain
{kind=link}

A maculopapular rash with an erythematous base is visible and appears partially confluent. This rash may be harder to see on darker skin.
Source: "Measles in African Child 2.JPG", Mike Blyth, Wikimedia commons licensed under Public Domain
{kind=link}

© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
Management
Initial management [6][7][9]
Suspect acute infection in a patient with typical clinical features of measles.
- Isolate patient and institute standard precautions and airborne precautions.
- Ensure that only health care professionals with evidence of measles immunity provide direct care to the patient.
- Notify the local health department immediately of suspected measles.
- Determine disposition.
- Severe disease (e.g., complications of measles): Admit to hospital. [10]
- Other patients: Manage at home while awaiting results of testing.
Measles is a nationally notifiable disease in the US; immediately report all suspected and confirmed cases to the local health department.
Diagnostics for measles [6][7][9]
Obtain and interpret diagnostic studies in all patients in coordination with the health department.
Studies
- All patients: serology for measles-specific IgM and IgG antibodies
- Patients presenting ≤ 10 days (ideally ≤ 3 days) after rash onset: [9]
- RT-PCR of a nasopharyngeal or throat swab
- If presenting close to day 10 after rash onset, also consider RT-PCR of a urine sample. [9]
Interpretation of results
The following applies to patients with clinical suspicion for measles.
-
Confirmatory results include any of the following:
- Positive RT-PCR or viral culture [9]
- Positive measles-specific IgM antibodies [9]
- A 4-fold increase in measles-specific IgG antibodies seen on two serum samples taken ∼ 2 weeks apart, starting from symptom onset [9]
-
Results that cannot rule out acute infection include:
- A single negative measles-specific IgM test collected:
- Within the first 3 days of rash onset (if generalized rash persists for > 3 days, repeat IgM test) [7]
- In a previously vaccinated patient [7]
- A single negative RT-PCR test [7]
- A single negative measles-specific IgG test
- A single negative measles-specific IgM test collected:
- If both IgM and RT-PCR are negative and patient has febrile rash: Obtain diagnostics for rubella with the same samples.
RT-PCR with measles serology (IgM) is preferred to confirm acute measles infection. RT-PCR samples should be collected as soon as possible and within 10 days of rash onset. [9]
Biopsy of an affected lymph node shows paracortical hyperplasia and Warthin-Finkeldey cells (multinucleated giant cells formed by lymphocytic fusion).
Further management [7][11]
- Provide supportive care (e.g., supportive care for pediatric fever) to all patients.
-
Vitamin A supplementation to reduce morbidity and mortality
- Administer to all children with severe measles; consider in other children. [7][11]
- Children with suspected vitamin A deficiency: Administer one additional dose 2–4 weeks after the initial regimen. [7]
- Ensure exposure control for measles.
- Administer postexposure prophylaxis for measles to affected contacts if necessary.
- Instruct on isolation precautions.
Antiviral therapy is not available for the treatment of measles. Most uncomplicated measles can be managed at home with supportive care and vitamin A. [7][10]


© AMBOSS
Differential diagnoses
See “Overview of infectious rashes in childhood.”
The differential diagnoses listed here are not exhaustive.
Complications
Subacute sclerosing panencephalitis (SSPE) [1][12]
- Definition: a lethal, generalized, demyelinating inflammation of the brain caused by persistent measles virus infection [13][14]
-
Epidemiology
- Primarily affects boys between 8 and 11 years of age
- Usually develops ≥ 7 years after measles infection
-
Clinical presentation: characterized by four clinical stages
- Stage I: dementia, personality changes
- Stage II: epilepsy, myoclonus, autonomic dysfunction
- Stage III: decerebration, spasticity, extrapyramidal symptoms
- Stage IV: vegetative state, autonomic failure
-
Diagnosis
-
Electroencephalography
- Paroxysmal delta waves (very slow, 1–3/sec)
- Periodic sharp and slow wave complexes
- Cerebrospinal fluid: ↑ anti-measles IgG
-
Electroencephalography
- Prognosis: SSPE leads to death within 1–3 years of diagnosis [15]
Other complications [1]
-
Bacterial superinfection
- Otitis media
- Pneumonia (most common cause of death)
- Laryngotracheitis
- Gastroenteritis
- Meningitis
-
Acute encephalitis
- Frequency: ∼ 1:1000 [16]
- Develops within days of infection
- Acute disseminated encephalomyelitis may develop within weeks.
- Giant cell pneumonia (viral, most commonly seen in immunosuppressed individuals)
Complications are likely to occur when the fever does not subside after a few days after onset of the exanthem.
We list the most important complications. The selection is not exhaustive.
Prognosis
- The prognosis of measles infection is good in uncomplicated cases.
- Fatal courses are more likely in newborns and immunocompromised patients.
- High fatality rate in resource-limited countries due to secondary bacterial infections.
Prevention
Vaccination [3][4]
-
Available options: live attenuated vaccines that contain multiple antigens
- Measles, mumps, rubella vaccine (MMR vaccine)
- Measles, mumps, rubella, varicella vaccine (MMRV vaccine)
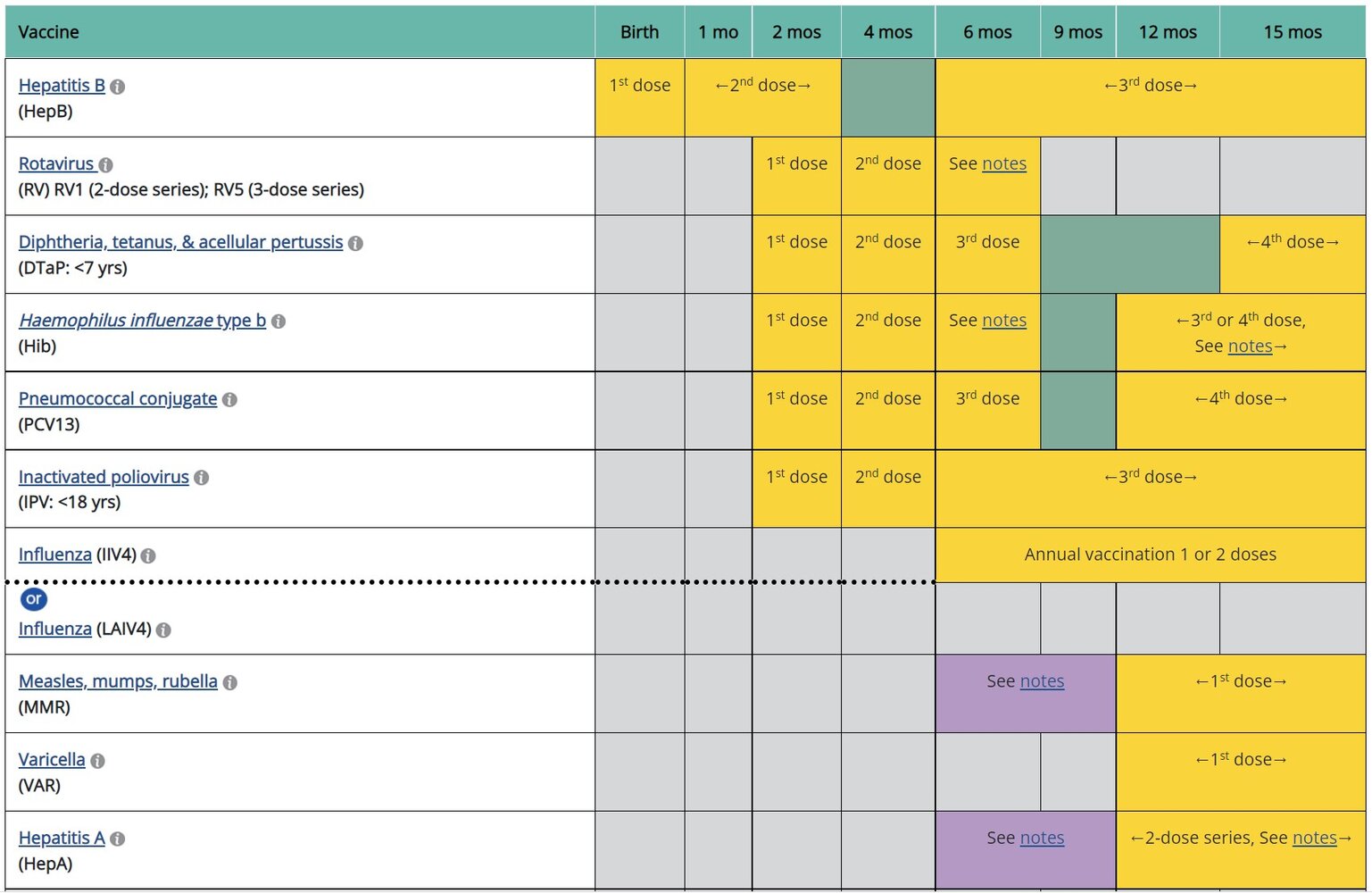
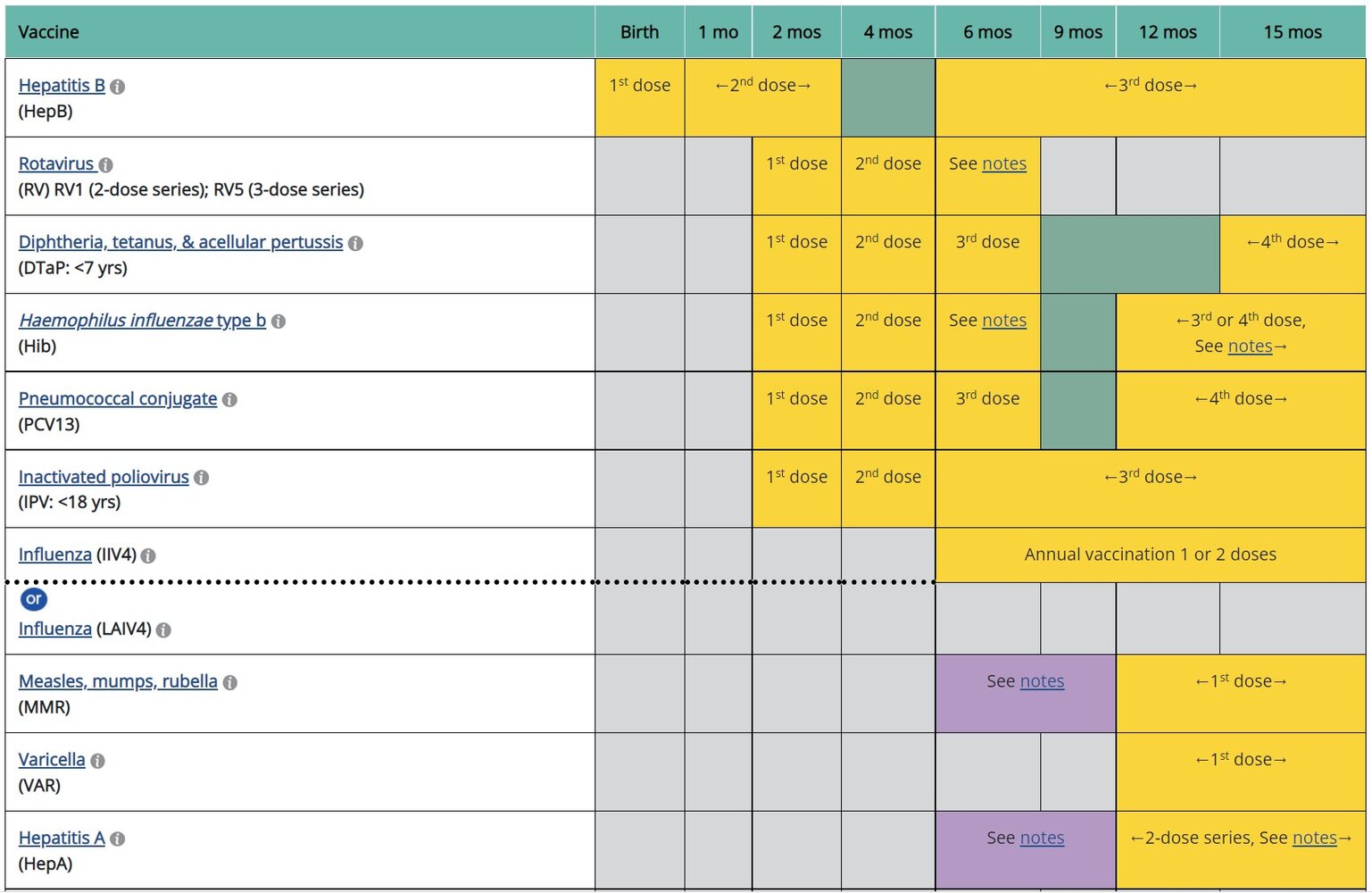
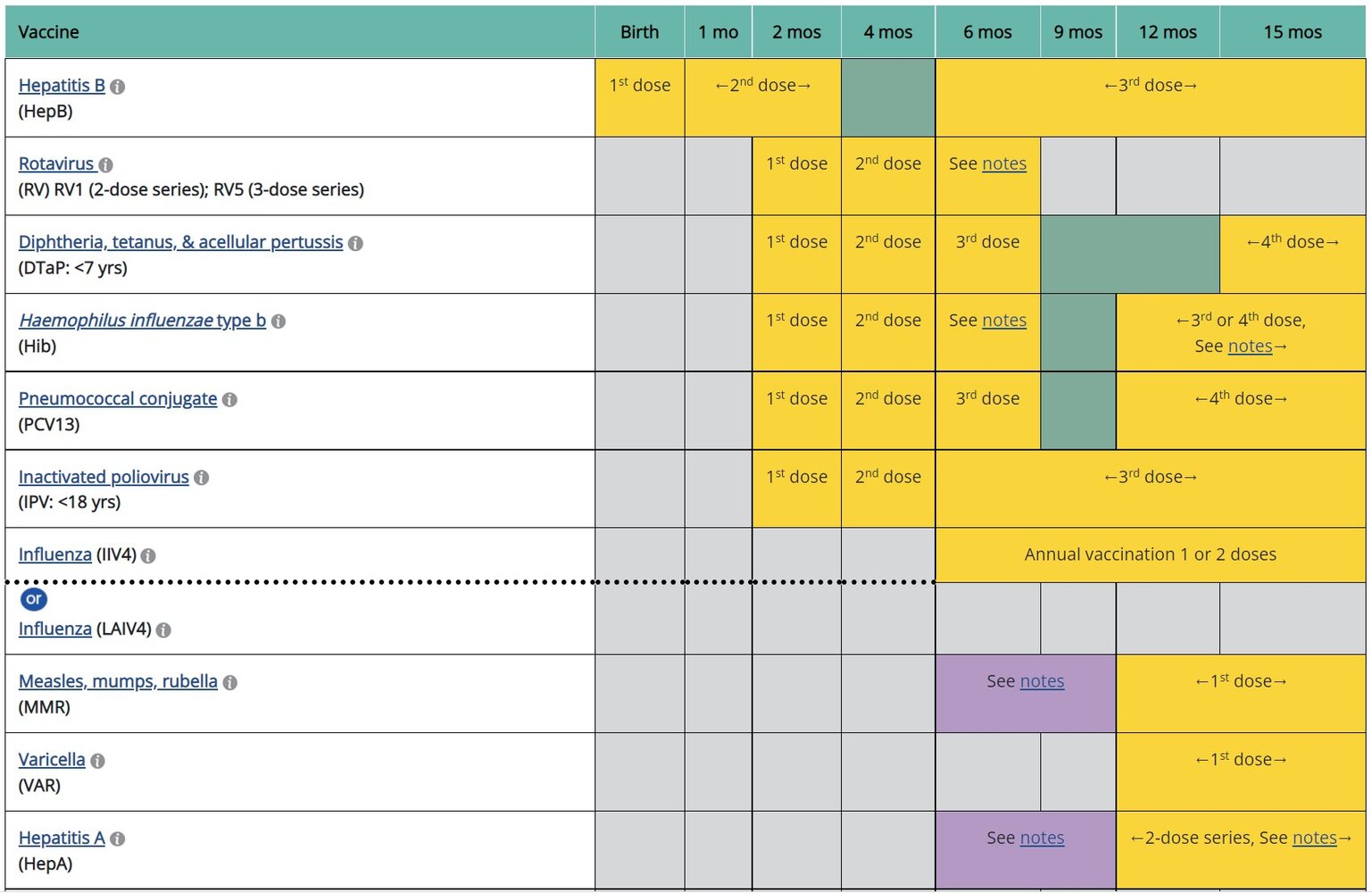
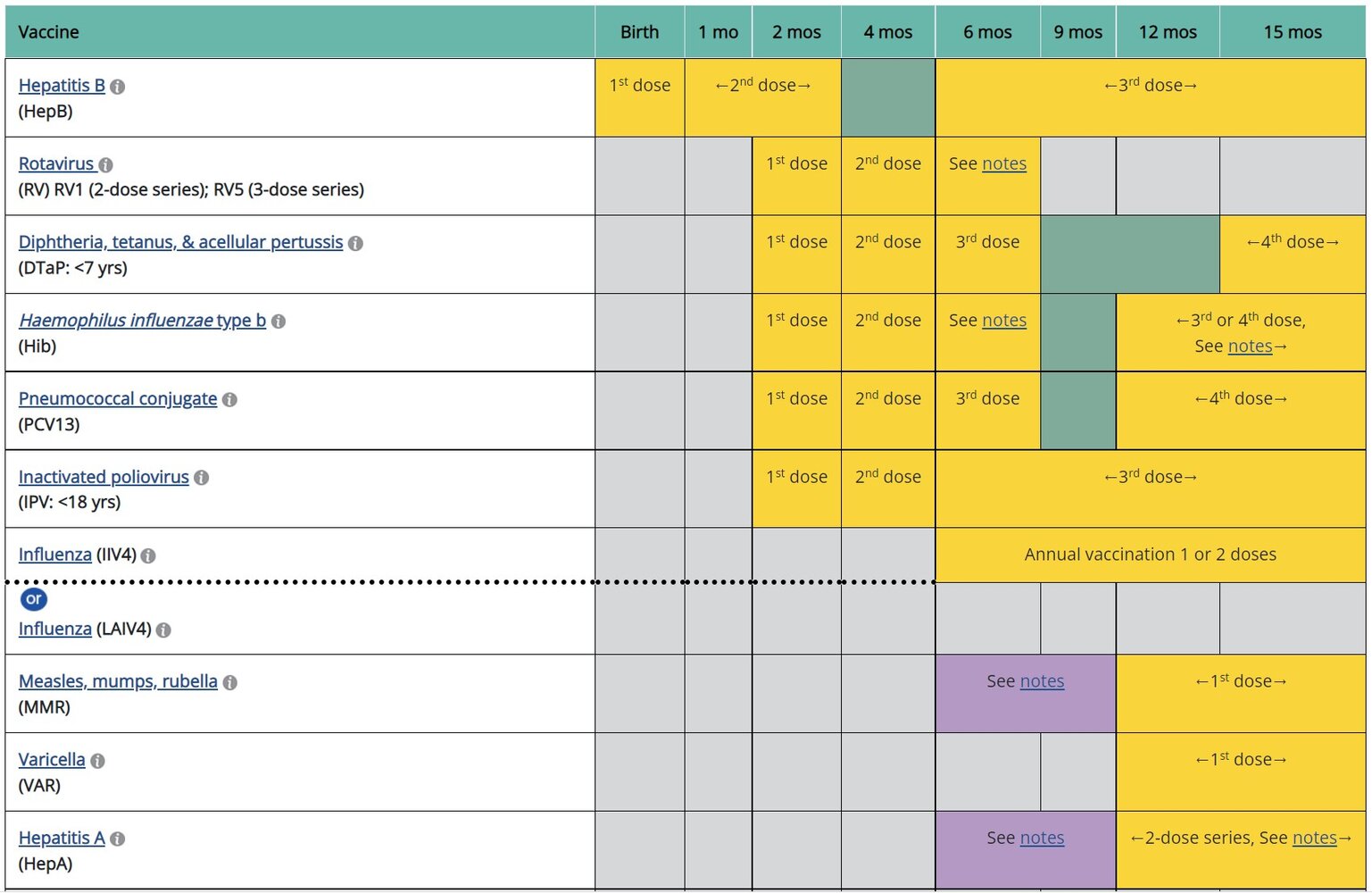
- Routine administration: See “ACIP immunization schedule” for details.
-
Individuals with risk factors for measles [2][7]
- Adults and children ≥ 12 months of age with no evidence of immunity to measles: Administer 2 doses total, ≥ 28 days apart.
- Infants 6–11 months of age with planned international travel: Administer 1 dose before departure.
-
Measles outbreak
- Consult the local health department.
- Recommendations may be similar to those for individuals with risk factors for measles; see above.
-
Contraindications [17]
- Any contraindications to live vaccines [17][18]
- History of anaphylaxis from neomycin
- HIV with severe immunosuppression [2][7]
-
Precautions [17]
- History of thrombocytopenia
- Tuberculin skin test (TST) within the preceding 4–6 weeks [17][19]
- Personal or family history of epilepsy (MMRV vaccine only) [20]
During a measles outbreak, follow local health department recommendations regarding vaccination.

Evidence of immunity [7][17]
Indications to test for immunity to measles, mumps, and rubella [7][17][21]
The following at-risk groups should be tested for immunity to determine the need for vaccination. [1][22][23]
- Pregnant individuals as part of routine prenatal care [24]
- Immunosuppressed individuals (e.g., individuals with HIV) [18][25]
-
Undervaccinated individuals with:
- Known exposure to measles, mumps, and/or rubella
- Suspected prior infection that was not confirmed with laboratory testing
- Inadequate or unknown vaccination status in individuals at increased risk of acquiring or transmitting measles, mumps, and/or rubella
Evidence of immunity to measles, mumps, and/or rubella [7][26]
Any of the following constitutes as evidence of immunity:
- Birth before 1957
- Confirmed receipt of MMR vaccine and/or MMRV vaccine [17]
- For measles and mumps immunity [7]
- Children 1–3 years of age: 1 dose
- Children 4–18 years of age: 2 doses
- Adults without risk factors for measles, mumps, and/or rubella: 1 dose
- Adults with risk factors for measles, mumps, and/or rubella: 2 doses
- For rubella immunity: 1 dose at ≥ 12 months of age
- For measles and mumps immunity [7]
- Laboratory evidence of either: [27]
- Prior infection: elevated serum IgM antibodies (for measles or rubella) or positive RT-PCR during the infection
- Immunity: elevated IgG antibody titers
The MMR vaccine is contraindicated during pregnancy. Individuals without evidence of immunity to MMR should receive one dose of MMR after delivery, preferably before discharge from the health care facility. [21]
Individuals with HIV and CD4 percentage ≥ 15% and CD4 count ≥ 200/mm3 for ≥ 6 months and no evidence of immunity to MMR should receive a 2-dose series of the MMR vaccine, administered ≥ 4 weeks apart. Live vaccines are contraindicated in individuals with severe immunocompromise (i.e., CD4 percentage < 15% and CD4 count < 200/mm3). [21]
Health care personnel with no evidence of immunity to MMR should receive a 2-dose series of MMR vaccine, administered ≥ 4 weeks apart; this should be considered even for those born before 1957. [21]
Exposure control for measles
Suspected and confirmed cases
- Hospitalized patients: Initiate standard precautions and airborne precautions.
- Isolation duration
- Immunocompetent: for 4 days from the onset of rash [28]
- Immunocompromised: for the duration of their illness [28]
Postexposure prophylaxis for measles
Postexposure prophylaxis and isolation are not required for immunocompetent individuals with evidence of immunity to measles.
-
Definition of exposure: either of the following [28]
- Being in the same airspace as an individual with measles
- Being in an airspace ≤ 2 hours after an individual with measles was in it [28]
-
Indications: confirmed exposure in the following individuals, if they present in the recommended timeframe
- Immunocompetent and pregnant individuals without evidence of immunity to measles
- Individuals in a severely immunocompromised state, regardless of immune status [17]
-
Methods
- Active immunization with a single dose of MMR vaccine
- Passive immunization with measles IgM immunoglobulin, given intramuscularly (IGIM) or intravenously (IGIV) [7]
| Postexposure prophylaxis for measles [7] | ||
|---|---|---|
| Status | Age | Recommendations |
| Immunocompetent | < 6 months |
|
| 6–11 months |
|
|
| ≥ 12 months without evidence of immunity to MMR |
|
|
| ≥ 12 months with 1 previous MMR dose |
|
|
| Severely immunocompromised |
|
|
| Pregnant without evidence of immunity to MMR | ||
-
Follow up after PEP for individuals without evidence of immunity to measles [7]
- After PEP with MMR vaccine: isolation not required, but exclude from healthcare settings for 21 days after last exposure
- After PEP with measles IgM immunoglobulin:
- Generally, isolate for 28 days after last exposure.
- Administer routine MMR vaccination at least 6–8 months later. [17]
-
Individuals who present too late for PEP
- Isolate for 21 days after last exposure.
- Then administer routine MMR vaccine if no contraindications to live vaccines.
Exposed health care workers [29]
- Administer PEP if indicated.
- No prior MMR doses: Exclude from work from day 5 after first exposure until day 21 after last exposure, regardless of whether PEP was received.
- With evidence of immunity to measles or with documented 1 dose of MMR before exposure:
- May continue to work, but monitor for symptoms from day 5 after first exposure until day 21 after last exposure.
- If only 1 dose previously, give second dose of MMR as soon as possible.
Further notes: Materials developed and hosted by the CDC and available free of charge on the CDC website. Reference to specific commercial products, manufacturers, companies, or trademarks does not constitute its endorsement or recommendation by the U.S. Government, Department of Health and Human Services, or Centers for Disease Control and Prevention.
Further notes: Materials developed and hosted by the CDC and available free of charge on the CDC website. Reference to specific commercial products, manufacturers, companies, or trademarks does not constitute its endorsement or recommendation by the U.S. Government, Department of Health and Human Services, or Centers for Disease Control and Prevention.
Further notes: Materials developed and hosted by the CDC and available free of charge on the CDC website. Reference to specific commercial products, manufacturers, companies, or trademarks does not constitute its endorsement or recommendation by the U.S. Government, Department of Health and Human Services, or Centers for Disease Control and Prevention.
Further notes: Materials developed and hosted by the CDC and available free of charge on the CDC website. Reference to specific commercial products, manufacturers, companies, or trademarks does not constitute its endorsement or recommendation by the U.S. Government, Department of Health and Human Services, or Centers for Disease Control and Prevention.
External Resources
References
- "Measles (Rubeola) - For Healthcare Professionals". https://web.archive.org/web/20241226063048/https://www.cdc.gov/measles/hcp/clinical-overview/index.html. [2016-08-10]
- "CDC/ACIP Vaccines & Immunizations: Routine Measles, Mumps, and Rubella Vaccination". https://web.archive.org/web/20250318195052/https://www.cdc.gov/vaccines/vpd/mmr/hcp/recommendations.html. [2021-01-26]
- "CDC/ACIP Vaccines & Immunizations: Immunization Schedules". https://web.archive.org/web/20250318202018/https://www.cdc.gov/vaccines/hcp/imz-schedules/index.html. [2024-11-21]
- "CDC/ACIP Vaccines & Immunizations: Catch-up Immunization Schedule for Children and Adolescents". https://web.archive.org/web/20250318202347/https://www.cdc.gov/vaccines/hcp/imz-schedules/child-adolescent-catch-up.html. [2024-11-21]
- "CDC Yellow Book: Rubeola/Measles". https://web.archive.org/web/20240418172226/https://wwwnc.cdc.gov/travel/yellowbook/2024/infections-diseases/rubeola-measles. [2023-04-04]
- "CDC Pink Book: Measles". https://web.archive.org/web/20240418171845/https://www.cdc.gov/vaccines/pubs/pinkbook/meas.html. [2021-08-01]
- Committee on Infectious Disease, American Academy of Pediatrics. "Red Book: 2024-2027 Report of the Committee on Infectious Diseases, 33rd Edition". American Academy of Pediatrics. (2024). ISBN: 9781610027373
- Orenstein WA, Perry RT, Halsey NA. "The clinical significance of Measles: a review". J Infect Dis. 189. :4-16. (2004)
- Jafri SK, Kumar R, Ibrahim S. "Subacute sclerosing panencephalitis – current perspectives". Pediatric Health, Medicine and Therapeutics. Volume 9. :67-71. (2018)
- Duyckaerts C, Litvan I. "Dementias". Elsevier. (2008). ISBN: 9780080559865
- Garg RK. "Review Subacute sclerosing panencephalitis". Postgraduate Medical Journal. 78. :63-70. (2002)
- R Garg. "Subacute sclerosing panencephalitis". Postgraduate Medical Journal. (2002)
- D.L. Fisher, S. Defres, T. Solomon. "Measles-induced encephalitis". QJM: An International Journal of Medicine. (2014)
- "Prevention of Measles, Rubella, Congenital Rubella Syndrome, and Mumps, 2013: Summary Recommendations of the Advisory Committee on Immunization Practices (ACIP)". https://web.archive.org/web/20241226075912/https://www.cdc.gov/mmwr/preview/mmwrhtml/rr6204a1.htm. [2013-06-14]
- "Birth-18 Years Immunization Schedule, By Medical Condition Recommendations for Ages 18 Years or Younger, United States, 2023". https://web.archive.org/web/20230319233710/https://www.cdc.gov/vaccines/schedules/hcp/imz/child-indications.html. [2023-02-10]
- "Tuberculin Skin Testing". https://web.archive.org/web/20230503192126/https://www.cdc.gov/tb/publications/factsheets/testing/skintesting.pdf. [2020-09-01]
- "Centers for Disease Control and Prevention (CDC) MMRV Vaccine and Febrile Seizures". https://web.archive.org/web/20220617000038/https://www.cdc.gov/vaccinesafety/vaccines/mmrv/mmrv-febrile-seizures.html. [2020-06-04]
- "Adult Immunization Schedule by Age Recommendations for Ages 19 Years or Older, United States, 2023". https://web.archive.org/web/20230324184103/https://www.cdc.gov/vaccines/schedules/hcp/imz/adult.html. [2023-02-10]
- "Child and Adolescent Immunization Schedule. Recommendations for Ages 18 Years or Younger, United States, 2023". https://web.archive.org/web/20230324163634/https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html. [2023-02-10]
- "Manual for the Surveillance of Vaccine-Preventable Diseases - Chapter 7: Measles". https://web.archive.org/web/20240419135730/https://www.cdc.gov/vaccines/pubs/surv-manual/chpt07-measles.html. [2014-04-01]
- "Serology Testing for Rubella and Congenital Rubella Syndrome (CRS)". https://web.archive.org/web/20230503193331/https://www.cdc.gov/rubella/lab/serology.html. [2023-04-12]
- "Altered Immunocompetence: General Best Practice Guidelines for Immunization". https://web.archive.org/web/20230317144823/https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/immunocompetence.html. [2023-02-10]
- "Vaccines and Preventable Diseases: Routine Measles, Mumps, and Rubella Vaccination". https://web.archive.org/web/20240625090847/https://www.cdc.gov/vaccines/vpd/mmr/hcp/recommendations.html#hcp. [2021-01-26]
- AAP Committee on Infectious Diseases. "Red Book: 2021–2024 Report of the Committee on Infectious Diseases". American Academy of Pediatrics. (2021). ISBN: 9781610025218
- "Interim Infection Prevention and Control: Recommendations for Measles in Healthcare Settings". https://web.archive.org/web/20240625224359/https://www.cdc.gov/infection-control/hcp/measles/index.html. [2024-04-12]
- "Infection Control in Healthcare Personnel: Epidemiology and Control of Selected Infections Transmitted Among Healthcare Personnel and Patients (2024) guideline". https://web.archive.org/web/20240625155523/https://www.cdc.gov/infection-control/hcp/healthcare-personnel-epidemiology-control/index.html. [2024-04-08]
- "Recommendations for Measles, Mumps, Rubella, and Varicella Testing for Clinicians". https://web.archive.org/web/20240419195612/https://www.cdc.gov/chickenpox/downloads/MMRV-Testing-for-Clinicians.pdf. [2020-12-31]
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- "Clinical Overview of Measles". https://web.archive.org/web/20240524073739/https://www.cdc.gov/measles/hcp/clinical-overview. [2024-05-09]