Summary
Mechanical ventilation is used to assist or replace spontaneous breathing to reduce the work of breathing and/or reverse life-threatening respiratory derangement in critically ill patients or to maintain respiratory function in those undergoing general anesthesia. It involves the application of positive pressure, which can be invasive (i.e., in intubated patients) or noninvasive (e.g., CPAP or BiPAP). Indications include hypoxemic and hypercapnic respiratory failure, hemodynamic compromise, and the need for close ventilatory control (e.g., therapeutic hyperventilation). Settings such as ventilation modes (e.g., assist-control, pressure-support) and parameters (e.g., tidal volume, respiratory rate, FiO2, PEEP) should be adjusted to patient needs in order to minimize complications and restore homeostasis. A variety of ventilation strategies have been described for treating different types of respiratory failure. These should be implemented in a critical care setting with close monitoring in collaboration with specialists, nurses, and respiratory therapists. Complications of mechanical ventilation include ventilator-induced lung injury and ventilator-associated pneumonia, as well as extrapulmonary complications such as GI ulcers and venous thromboembolism. A systematic approach to common problems in mechanical ventilation (e.g., sudden deterioration, problems with oxygenation and ventilation, hemodynamic compromise, patient-ventilator dyssynchrony, dynamic hyperinflation) is recommended to prevent morbidity and mortality. Once patients show sufficient spontaneous breathing, they are weaned off ventilation support. See also airway management.
Definitions
- Mechanical ventilation: use of a ventilator to assist or completely replace spontaneous breathing
Positive-pressure ventilation
Positive-pressure ventilation (PPV) is the underlying mechanism of modern mechanical ventilators [1]
-
Definition: Oxygenated air is pushed into the lungs by a mechanical ventilation device that generates a positive pressure gradient.
- Exhalation occurs through passive elastic recoil.
- May be administered invasively (e.g., via endotracheal or tracheostomy tube) or noninvasively (e.g., via a secured mask, as in BiPAP or CPAP)
-
Effects of positive-pressure ventilation
- Increased airway pressures
- Promotes gas exchange and recruitment/stenting of alveoli
- ↑ Risk of ventilator-induced lung injury (e.g., barotrauma)
- ↑ Pulmonary artery pressure
- ↑ Pulmonary vascular resistance
-
Increased intrathoracic pressure → ↑ pulmonary vascular resistance and ↓ venous return → ↓ venous drainage of extrathoracic organs and ↓ cardiac output [2]
- Right heart: ↓ right atrium filling, ↓ right ventricle (RV) preload, ↓ RV stroke volume, ↑ RV work, ↑ RV afterload
- Left heart: ↓ left ventricle (LV) preload, ↓ LV stroke volume, ↓ LV afterload, ↓ LV work
- Abdominal: ↑ gastric distension, ↑ risk of vomiting/aspiration, ↑ abdominal compartment pressure, ↓ organ perfusion
- Increased airway pressures

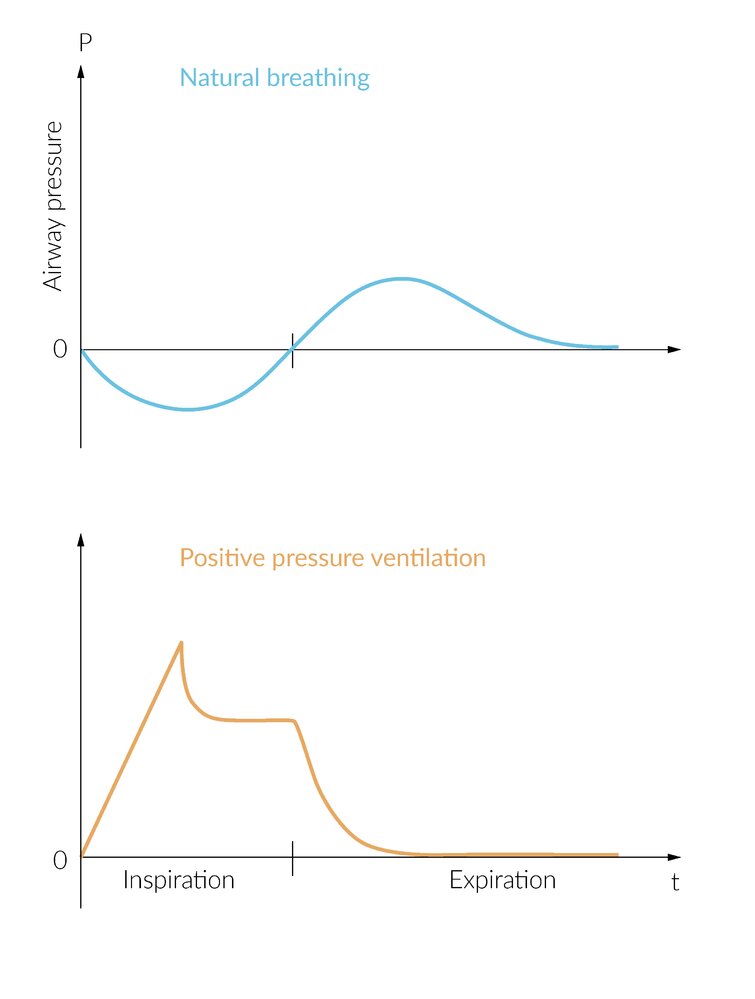
In spontaneous breathing, the thoracic volume increases during inspiration due to respiratory muscles. The resulting negative intrathoracic pressure "sucks" air into the lungs. During expiration, the passive elastic recoil of the lungs (for the most part) creates a positive airway pressure to expel the air. The airway pressure may increase further during expiration with additional active expiration (not shown here).
In mechanical ventilation, the ventilator pushes air into the lungs against the airway resistance creating a positive pressure gradient. The pressure increase may level off as it progresses, depending on the compliance of the lungs. The highest pressure is reached at the end of the so-called flow phase when the entire tidal volume has been administered by the ventilator. Subsequently, no further gas flows in and the airway pressure remains unchanged (so-called no-flow phase or inspiratory pause). With the start of expiration, the ventilator releases the built-up pressure and the airway pressure drops to the initial value.
© AMBOSS
Noninvasive positive-pressure ventilation
Types of noninvasive positive-pressure ventilation (NIPPV) [3]

Continuous positive airway pressure (CPAP)
- The ventilator delivers one constant airway pressure throughout the respiratory cycle (e.g., 5 cm H2O).
- Equivalent to providing PEEP without any other support
- Used in hypoxemic respiratory failure; (e.g., cardiogenic pulmonary edema, OSA)
")
Bilevel positive airway pressure (BIPAP)
-
The ventilator delivers two pressure levels and cycles between them.
-
Expiratory positive airway pressure (EPAP): baseline pressure provided
- Safe range: < 10–15 cm H2O
-
Inspiratory positive airway pressure (IPAP): EPAP plus added inspiratory pressure support (PS)
- Safe range: < 20–25 cm H2O
- If there is no added inspiratory pressure support (i.e., when IPAP = EPAP), then the EPAP setting is equivalent to CPAP.
- If there is added inspiratory pressure support (i.e., IPAP > EPAP), then EPAP is equivalent to PEEP (see invasive mechanical ventilation).
-
Expiratory positive airway pressure (EPAP): baseline pressure provided
- Used in hypercapnic respiratory failure and hypoxemic respiratory failure
CPAP only delivers one airway pressure, equivalent to PEEP. BIPAP cycles between two airway pressures and offers inspiratory pressure support.
")
Indications for NIPPV [4][5]
- Treatment of respiratory distress in patients with:
- Acute COPD exacerbation with respiratory acidosis (e.g., pH ≤ 7.35, PaCO2> 45 mm Hg, RR > 20–24)
- Cardiogenic pulmonary edema (without shock or ACS)
- Asthma exacerbations: This is a controversial indication.
- Treatment of acute respiratory failure in patients with:
- Immunocompromise (e.g., solid organ and bone marrow transplant)
- Chest trauma
- Postoperative deterioration
- Bridging to intubation in patients with challenging preoxygenation (e.g., ARDS) [6]
- Bridging back to unassisted breathing
- Weaning from invasive mechanical ventilation in patients with acute hypercapnic respiratory failure
- Prophylactic use after planned extubation in patients at high risk for recurrent respiratory failure
- Patients with a level of care precluding invasive mechanical ventilation
- Patient with a do-not-intubate order [3]
- Trial of therapy while the underlying disease is treated
- Temporizing measure to provide life support until the arrival of family/friends
- Palliative therapy for terminal cancer patients with dyspnea
- Patient with a do-not-intubate order [3]
Contraindications for NIPPV [7][8]
- Impaired/absent spontaneous breathing and/or patient not cooperative with NIPPV
- Cardiac or respiratory arrest
- Severe encephalopathy (GCS < 10)
- Uncontrolled agitation
- Impaired airway protection
- Upper airway obstruction
- Inability to clear respiratory secretions
- Severe upper GI bleeding
- High risk of aspiration [9]
- Impaired mask seal
- Facial trauma
- Surgery
- Deformity
- High risk of adverse effects from positive pressure
- Recent upper airway or upper gastrointestinal surgery
- Hemodynamic instability or cardiac arrhythmia
Uncontrolled agitation is a contraindication for NIPPV.
Procedure [3][5][8]
The following steps are pertinent to adults newly requiring NIPPV. Stable patients continuing home therapy (e.g., CPAP for longstanding OSA) should be started on their preferred interface and baseline settings.
-
Preparation
- Obtain baseline ABG if feasible.
- Make sure the patient is comfortable, alert, and in sitting position.
- Monitor pulse oximetry, blood pressure, ECG, ABG, exhaled tidal volume, and respiratory mechanics.
- Explain the procedure to the patient.
- Prepare for intubation in case respiratory and clinical status deteriorates.
-
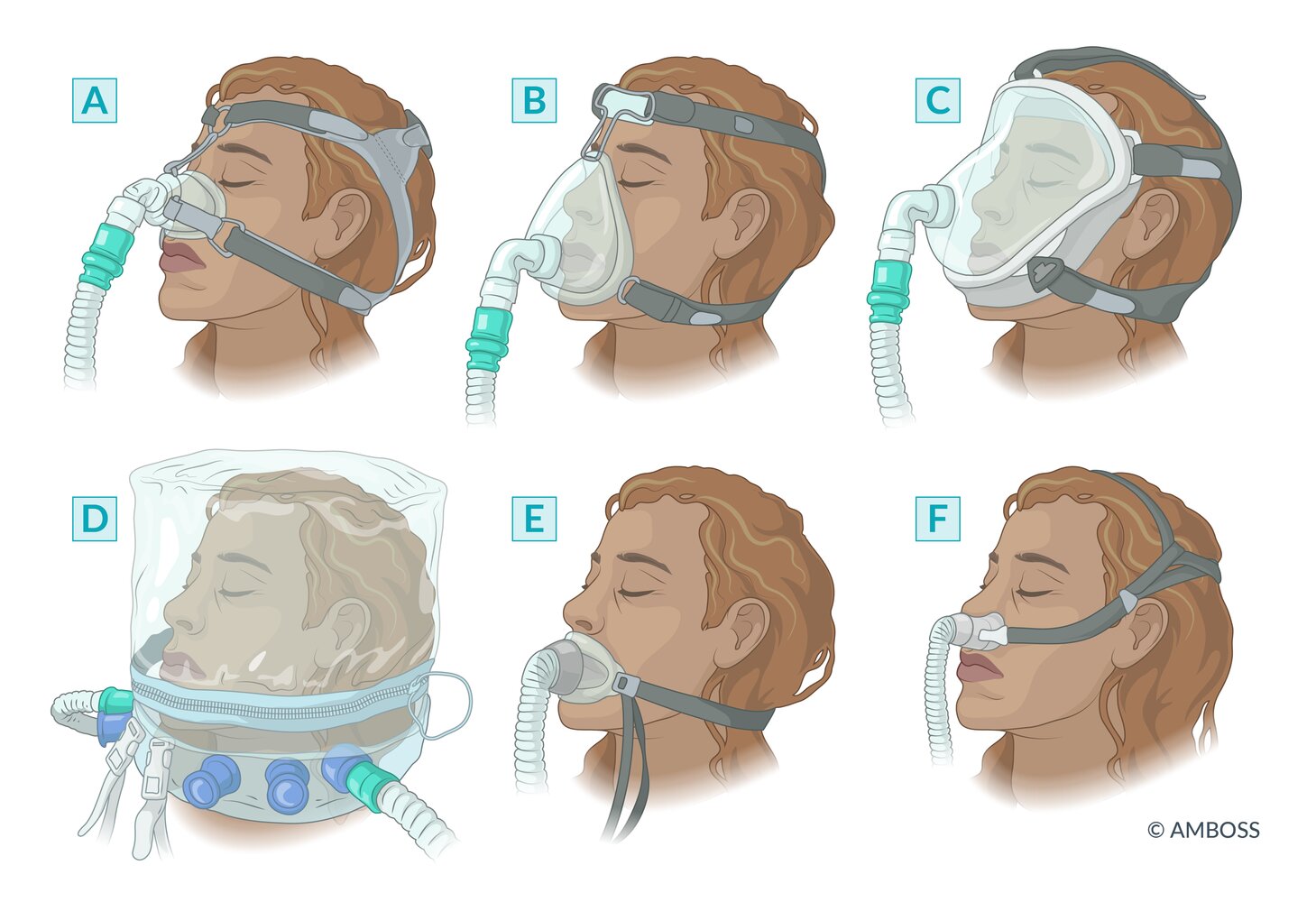
Choice of interface [8]
- Oronasal mask
- Total-face masks
- Nasal mask or nasal pillows
- Helmet
-
NIPPV settings [5]
- BIPAP mode [3]
- Low-high approach: Start with low pressures and adjust upward as needed and tolerated.
- Start EPAP at 3–5 cm H2O.
- Start IPAP at 10 cm H2O.
- High-low approach: Start with high pressures and adjust downward as needed and tolerated.
- Start EPAP at 5–8 cm H2O.
- Start IPAP at 20–25 cm H2O.
- Low-high approach: Start with low pressures and adjust upward as needed and tolerated.
- CPAP mode: Set PEEP to 5–12 cm H2O.
- Titrate FiO2 (between 30% and 50%) to the desired oxygenation target (e.g., SpO2 88–92% for COPD).
- BIPAP mode [3]
-
Monitoring and adjustments
- Initially administer NIPPV for 30–60 minutes.
- Titrate initial pressures (PEEP/EPAP and IPAP) to:
- ↓ Work of breathing and dyspnea
- ↓ Respiratory rate
- ↑ Tidal volume
- ↓ Patient-ventilator dyssynchrony
- ↓ Work of breathing and dyspnea
- Check ABG after 20–30 minutes.
- If SpO2 is low, increase FiO2 and PEEP/EPAP.
- If PaCO2 is high, increase IPAP.
- If patient's condition worsens , prepare to switch to invasive mechanical ventilation (see endotracheal intubation).
Do not delay invasive mechanical ventilation (e.g., intubation) if a patient's condition is worsening with NIPPV.

Complications [8]
- Air leaks
- Aspiration and potential aspiration pneumonia
- Ventilator-associated lung injury: barotrauma or pneumothorax
- Severe gastric distention that necessitates NG tube insertion
- Skin irritation, abrasions, and nasal bridge ulceration
- Mucus plugging
- Mucosal dryness
Original title: “Improving ventilation”. Created by: Medmastery.
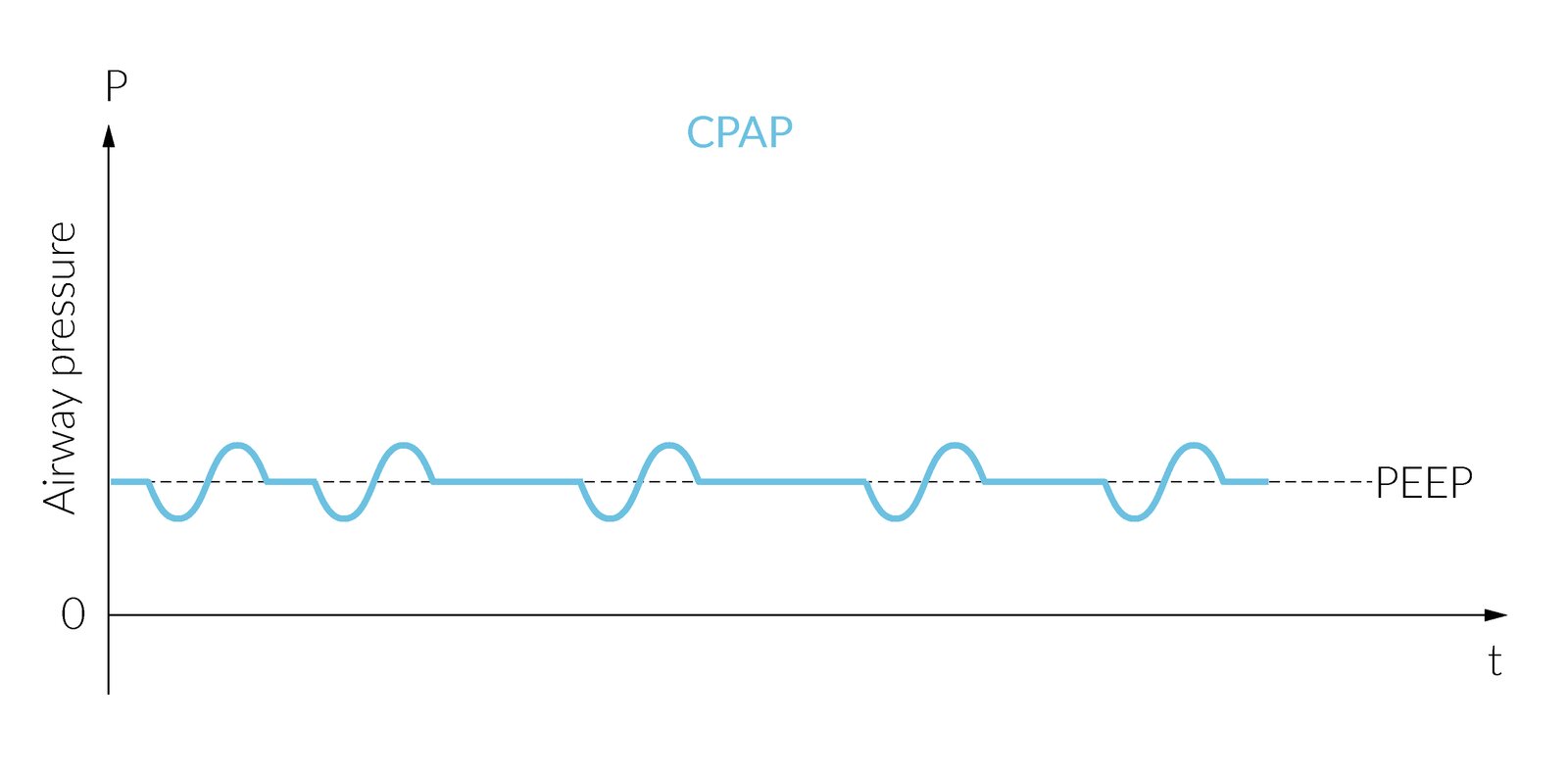
Airway pressure in the course of assisted ventilation with CPAP
A continuous positive airway pressure (equivalent to providing PEEP) is maintained by the ventilator. At this pressure level, the treated person can breathe spontaneously and determine the tidal volume, respiratory rate, and inspiratory flow.
During inspiration, spontaneous breathing efforts create suction, and airway pressure decreases. During expiration, pressure rises above the respiratory rest value, as in physiological breathing.
© AMBOSS
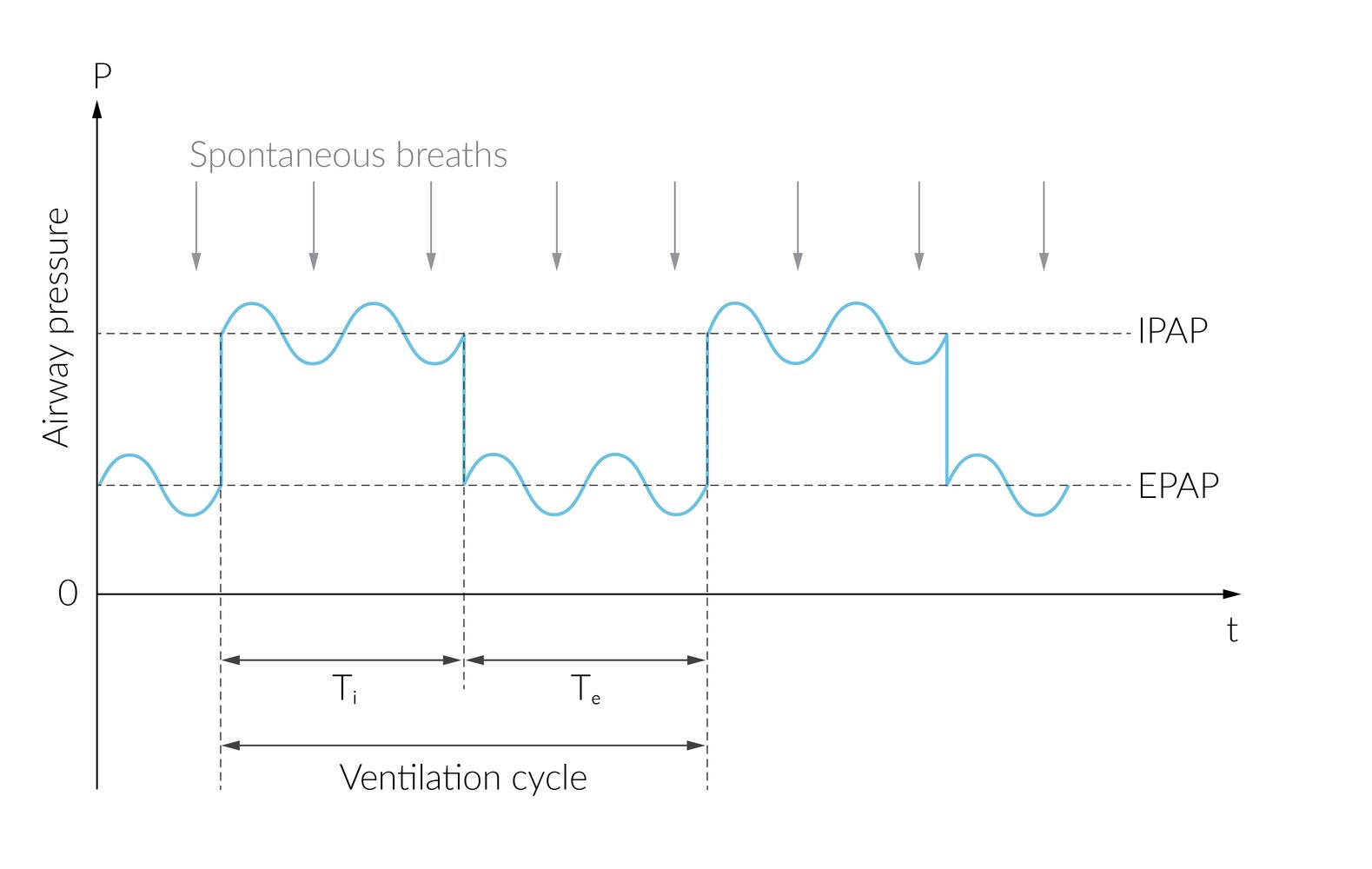
Airway pressure in the course of assisted ventilation with BIPAP
BIPAP is characterized by the biphasic alternation between two positive airway pressures (dashed lines). The lower pressure level (EPAP) corresponds to PEEP, while the upper pressure level (IPAP) corresponds to EPAP plus inspiratory pressure support. The alternation frequency is determined by the respiratory rate.
The ventilated patient can breathe spontaneously at both pressure levels (indicated by blue line) and thus (co)determine the respiratory rate and tidal volume. A decrease in airway pressure corresponds to the suction generated by the ventilated person during inspiration, while the following increase represents expiration.
© AMBOSS
Invasive mechanical ventilation
General principles [3][10]
- Description: positive pressure ventilation administered through an invasive airway device, e.g., endotracheal (ET) or tracheostomy tube (see “Airway management” for details)
-
Goals
- Reduce work of breathing (WOB). [11]
- Prevent respiratory arrest.
- Alleviate myocardial oxygen demand.
- Prevent multiorgan dysfunction.
- Treat life-threatening hypoxemia and hypercarbia.
- Ensure aggressive bronchopulmonary hygiene.
- Support breathing in patients requiring intubation for airway protection.
- Reduce work of breathing (WOB). [11]
- Risks: The ET tube and ventilator tubing/circuit increase instrumental dead space, which leads to higher airway resistance and pressure, thereby raising the risk of ventilator-induced lung injury.
Indications for invasive mechanical ventilation [12][13]
- Hypercapnic respiratory failure
- Hypoxemic respiratory failure
- Hemodynamic compromise
- Early mechanical ventilation offloads the heart by reducing the MVO2 required to maintain the work of breathing. [12]
- Useful in conditions with ↑ systemic oxygen demand and/or ↓ cardiac output (e.g., polytrauma, burns, septic shock, severe MI, cardiogenic shock)
- The benefits must be weighed against the hemodynamic risks of positive-pressure ventilation (see PPV).
- Hyperventilation therapy: short-term measure to treat patients with increased ICP [14]
- GCS ≤ 8 [15]
Contraindications
- No absolute contraindications
- Relatively contraindicated in patients with advanced directives against mechanical ventilation
Initiating mechanical ventilation in patients with severe obstructive lung disease, acidosis, and shock is associated with significant morbidity and mortality. These conditions require special care and preparation (see high-risk indications for mechanical ventilation).
Adjunctive care of ventilated patients
Sedation, analgesia, and muscle relaxants [16][17][18]
-
Goals
- Decrease patient discomfort.
- Suppress respiratory drive.
- Decrease muscular resistance to mechanical ventilation.
- Decrease patient-ventilator dyssynchrony.
-
Sedation
- Start immediately after intubation for patient comfort: Do not mistake paralysis for sedation, especially if a long-acting muscle relaxant (e.g., rocuronium) was used during the induction.
- Titrate to patient comfort (e.g., RASS range 0 to -5).
- Consider lighter sedation in patients requiring serial neurological examination.
- Agents
- Propofol
- Midazolam
- Dexmedetomidine
- Ketamine [19]
-
Analgesia
- Spontaneously breathing patients should be monitored for respiratory depression.
- Agents
- Fentanyl (off-label)
- Morphine (off-label)
-
Muscle relaxants [20][21]
- Allow a higher level of ventilatory control when desired (e.g., in refractory ARDS)
- Should only be used in sedated patients.
- Agents
- Rocuronium
- Pancuronium
- Cisatracurium -
Sedation should be started immediately after intubation and should not be mistaken or confused for the paralysis caused by some induction agents. Paralysis without sedation should be avoided at all costs!
Bronchopulmonary hygiene [22]
- Oral and airway hygiene
- Tracheal suctioning
- Mucolytics
- Bronchoscopy
- Chest physiotherapy and kinetic therapy
Supportive care
- Orogastric or nasogastric tube insertion
- Pressure ulcer prophylaxis
- VTE prophylaxis
- Consider stress ulcer prophylaxis (routine use is controversial)
Ventilator settings
Basic ventilation parameters [1][3][10][23][24][25]
-
Tidal volume (Vt): the volume of air delivered to or taken by the patient per breath
- Set by the clinician in volume-controlled modes (e.g., 8–12 mL/kg ideal body weight)
- Measured by the ventilator in pressure-controlled or pressure-supported modes (e.g., PRVC and PSV)
-
Respiratory rate (RR): breaths taken or delivered per minute
- Set by the clinician in the absence of patient-initiated breaths (e.g., ∼ 10–15/min)
- Set by the patient in spontaneous breathing modes
- Commonly a combination of patient-triggered assisted breaths and a clinician-set backup RR
-
Fraction of inspired oxygen (FiO2): the fraction of oxygen (by volume) in the inspired air
- FiO2 of room air = 21%
- FiO2 up to 100% can be delivered in perfectly sealed ventilator circuits.
-
Positive end-expiratory pressure (PEEP):
- Definition
- Positive pressure in the lung maintained over the entire inhalation and expiration phases
- Measured in centimeters of water (cm H2O)
- Also known as extrinsic PEEP (as it is applied to the patient by the device)
- Mechanism of action: keeps airway pressure above the atmospheric level at the end of exhalation → increases alveolar pressure and volume → reopens collapsed or unstable alveoli → improves ventilation/perfusion relation
-
Indications: PEEP is typically justified when a PaO2 of 60 mm Hg cannot be achieved with an FiO2 of 60%.
- Almost all patients need a minimum amount of PEEP (3–5 cm H2O).
- Higher PEEP is indicated in conditions involving a right-to-left pulmonary shunt pathology.
- Advantages
- Prevent atelectasis
- ↑ Oxygenation without increasing the risk of oxygen toxicity
- ↑ Gas exchange area
- ↑ Functional residual capacity
- ↑ Pulmonary compliance
- Adverse effects
- Ventilator-induced lung injury
- Patient-ventilator dyssynchrony
- See “adverse effects” of positive pressure ventilation.
- See hemodynamic compromise in mechanically ventilated patients.
- Definition
Ventilator modes [1][3][10][23][24][25]
Mandatory ventilation modes
Mandatory modes are useful when respiratory musculature is weak/paralyzed and respiratory drive is impaired.
-
Examples
- Assist-control (AC) ventilation: can consist of volume-control ventilation (VCV) or pressure-control ventilation (PCV)
- Pressure-regulated volume control (PRVC)
-
Description
- Breath frequency and waveforms are mostly controlled by the clinician.
- A minimum number of breaths per minute are delivered by the ventilator.
- Patients can trigger additional breaths above the minimum set rate.
- The breath volume and/or pressure are fixed and are independent of patient effort.


Spontaneous ventilation modes
Spontaneous modes are useful for when respiratory musculature is intact/weak and respiratory drive is intact.
- Example: pressure-support ventilation (PSV)
-
Description:
- Breath frequency and waveforms are mostly controlled by the patient.
- The ventilator only provides inspiratory pressure to support breathing.
- Almost all breaths are patient-triggered.
- Breath volume and duration depend on patient effort and the degree of inspiratory pressure provided.
Comparison of commonly used ventilator modes
| Comparison of ventilator modes [3][23][24][25] | |||
|---|---|---|---|
| Mode | Programming | Advantages | Disadvantages |
| Volume-control ventilation (VCV) |
|
|
|
| Pressure-control ventilation (PCV) |
|
|
|
| Pressure-regulated volume-control (PRVC) |
|
|
|
| Pressure-support ventilation (PSV) |
|
|
|
Advanced settings
-
Pressure support (PS): positive pressure added on top of PEEP during inspiration in pressure-supported ventilation modes (e.g., PSV)
- Ranges from 5 cm H2O (minimal support) to 30 cm H2O (maximal support)
- Work of breathing is mostly accomplished by the ventilator if PS > 20 cm H2O.
- PS is typically increased to compensate for respiratory muscle fatigue, then gradually decreased during weaning from mechanical ventilation to allow patients to strengthen their respiratory musculature, with the goal of them breathing unassisted.
-
Peak inspiratory pressure (PIP) limit/target: preset parameter in pressure-controlled and pressure-regulated ventilation modes
- In other ventilator modes, PIP is a variable (see “monitoring” below).
- Typically set at ∼ 20–25 cm H2O to prevent barotrauma
-
Inspiratory flow rate (VI): the rate of airflow sent into lungs during the inspiratory phase
- Adjustable; flow rate typically set at at 60 L/min
-
Inspiratory:expiratory ratio (I:E ratio): the ratio of inspiratory time to expiratory time in a given breathing cycle
- Usually expressed in whole numbers (e.g., 1:2, 1:3)
- Can be adjusted directly or indirectly depending on the device
- Target I:E ratios are desirable in certain conditions (e.g., 1:4–1:5 for obstructive lung disease).
- Lower I:E ratios improve CO2 clearance, minimize air trapping (auto-PEEP), and minimize the effect of positive-pressure on hemodynamics.
- Higher I:E ratios increase mean airway pressure and may enhance oxygenation and recruitment.
- Depends on other parameters
- ↑ RR→ ↓ time available for passive expiration → ↑ I:E ratio
- ↑ Vt → ↑ time required for inspiration → ↑ I:E ratio
- ↑ VI → ↓ time required for inspiration → ↓ I:E ratio
- Inspiratory time = Vt/VI
- Expiratory time = [breath cycle time (1/RR) - inspiratory time]
- I:E ratio = inspiratory time/expiratory time
-
Trigger sensitivity (mechanical ventilation): the threshold of inspiratory pressure or flow-gradient at which the ventilator identifies the patient's attempt to initiate a breath
- Typically standard to the device (1–3 cm H2O)
- Not commonly adjusted by clinicians
- Low sensitivity helps to decrease work of breathing
- High sensitivity helps to decrease oversensing of breaths

Original title: “The what and why of mechanical ventilation”. Created by: Medmastery.
Original title: “Assist control (AC) and synchronized intermittent mandatory ventilation (SIMV) modes”. Created by: Medmastery.

Original title: “Volume versus pressure control”. Created by: Medmastery.
Monitoring
General principles
All mechanically ventilated patients require close clinical, biomechanical, and laboratory monitoring in a critical care unit. This should include:
- One-to-one nursing care
- Continuous cardiac and hemodynamic monitoring
- Respiratory monitoring: Sensors can be externally applied or built into modern ventilators.
- Temperature monitoring
- Blood gas analysis monitoring
External monitoring [27]
-
Pulse oximetry
- Advantages
- Widely available and portable
- Easy to interpret in real-time
- High accuracy if SpO2 > 70%
- Disadvantages: not as accurate as PaO2
- ↓ Accuracy in the case of: hypovolemia, hypothermia, vasopressor use, dyshemoglobinemia (e.g., carboxyhemoglobin, methemoglobin)
- Poor sensitivity for hyperoxia
- Advantages
-
Capnometry (portable): numerical measurement of end-tidal CO2 (EtCO2) [28]
- Description
- Externally-applied devices are being used with increasing frequency.
- Expired air is sampled through a tube.
- A transducer detects CO2 and the amount is displayed on the monitor.
- Primary uses
- Determining the adequacy of ventilation
- Confirming ET tube placement
- RR monitoring
- Secondary uses
- Short term guidance of hyperventilation therapy (e.g., treating ↑ ICP)
- Diagnosing pulmonary embolism
- Preventing hypercapnia, e.g., in brain-injured and post-cardiac arrest patients
- Assessing CPR quality
- Disadvantages: underestimates PaCO2 compared to ABG
- Description
-
Advanced monitoring to consider: especially for conditions exacerbated by positive pressure ventilation.
- Hemodynamically unstable patients: CVP monitoring; IVC diameter and collapsibility
- Patients at risk of abdominal compartment syndrome: abdominal compartment pressures

Ventilator-based monitoring [3][10][27]
The following are standard measurements built into most newer generation ventilators.
Capnography
-
Description
- Waveform version of capnometry displaying CO2 measurements in exhaled air over time
- The EtCO2 is measured at the end of the expiratory phase of the breathing cycle.
- Sensors are typically integrated into the ventilator but can be portable in rare cases.
-
Interpretation
- Normal waveform: rapid increase of the CO2 concentration → plateau → rapid decrease in the CO2 concentration during inspiration.
- Loss of waveform
- Cardiac arrest
- Accidental extubation
- Complete tube obstruction
- Significant decrease in waveform amplitude
- Partial tube obstruction
- Airway leak
- Hypotension
Pressure monitoring [13][29]
-
Peak inspiratory pressure (PIP):
- Definition: the maximum pressure measured at any point throughout the inspiratory phase
- Description: primarily reflects airway resistance; lung compliance reflected to a lesser degree
-
VCV
- Measured PIP is greatly influenced by airway resistance.
- Less reflective of alveolar pressure and risk of VILI
-
PCV/PRVC
- PIP = inspiratory pressure target + PEEP
- Accurately reflects alveolar pressure and correlates well with VILI risk
-
VCV
- Interpretation: PIP > 35–40 cm H2O is generally considered elevated.
-
Plateau pressure (PPlat)
- Definition: the maximum air pressure measured during a pause at the end of inspiration
- Description: reflects lung compliance
- VCV: more accurately reflects alveolar pressure and risk of VILI than PIP
- Interpretation: Pplat > 30 cm H2O is considered elevated.
-
Auto-PEEP (intrinsic PEEP) [30]
- Definition: PEEP remaining in the circuit at the end of expiration that is not delivered by the ventilator, i.e., generated by the patient
- Description
- Tends to occur in conditions in which the expiratory outflow is impaired (e.g., asthma)
- Expiration is incomplete at the end of a breath cycle → air trapping → dynamic hyperinflation
- Estimated using expiratory hold maneuver
- The circuit is paused for 3–5 seconds at the end of expiration.
- The change in pressure waveform back to baseline is measured as it reaches equilibrium in the circuit, which is the total PEEP.
- Auto-PEEP = total PEEP - extrinsic PEEP
- Interpretation:
- Ideally, no auto-PEEP should be present.
- The presence and degree of auto-PEEP correlates with a higher risk of complications (e.g., dynamic hyperinflation, adverse effects of positive pressure ventilation).

Laboratory monitoring [31]
Arterial blood gas monitoring
-
General considerations
- More accurate than pulse oximetry for assessing oxygenation
- Essential for calculation of P/F ratio
- Consider an arterial line for patients requiring frequent arterial sampling.
- Normal physiological/compensated ranges are typically desirable (exceptions include permissive hypercapnia).
-
Sampling frequency
- Within 30 minutes of intubation
- Within 1 hour of changes in ventilator settings or patient status
- Every 8–24 hours otherwise
-
Interpretation: See also arterial blood gas analysis.
- Ventilation: pH, PaCO2, HCO3
- Respiratory acidosis pattern: insufficient minute ventilation
- Respiratory alkalosis patterns: iatrogenic hyperventilation
- Metabolic acidosis/alkalosis patterns: Consider adjusting minute ventilation for compensation.
- See improving ventilation in mechanically ventilated patients.
- Oxygenation: PaO2
- For interventions, see improving oxygenation in mechanically ventilated patients.
- Ventilation: pH, PaCO2, HCO3
| Interpretation of oxygenation using ABG in mechanically ventilated patients | ||
|---|---|---|
| Condition | PaO2 (mm Hg) | |
| Hypoxemia | < 70 | |
| Normoxemia | 70–120 | |
| Hyperoxia [32][33] | Mild | 121–200 |
| Moderate | 201–300 | |
| Severe | > 300 | |
Venous blood gas [10]
- Generally correlates well with ABG for pH
- Venous PCO2 is not as reliable as capnography.
- Venous PO2 is not as reliable as pulse oximetry.


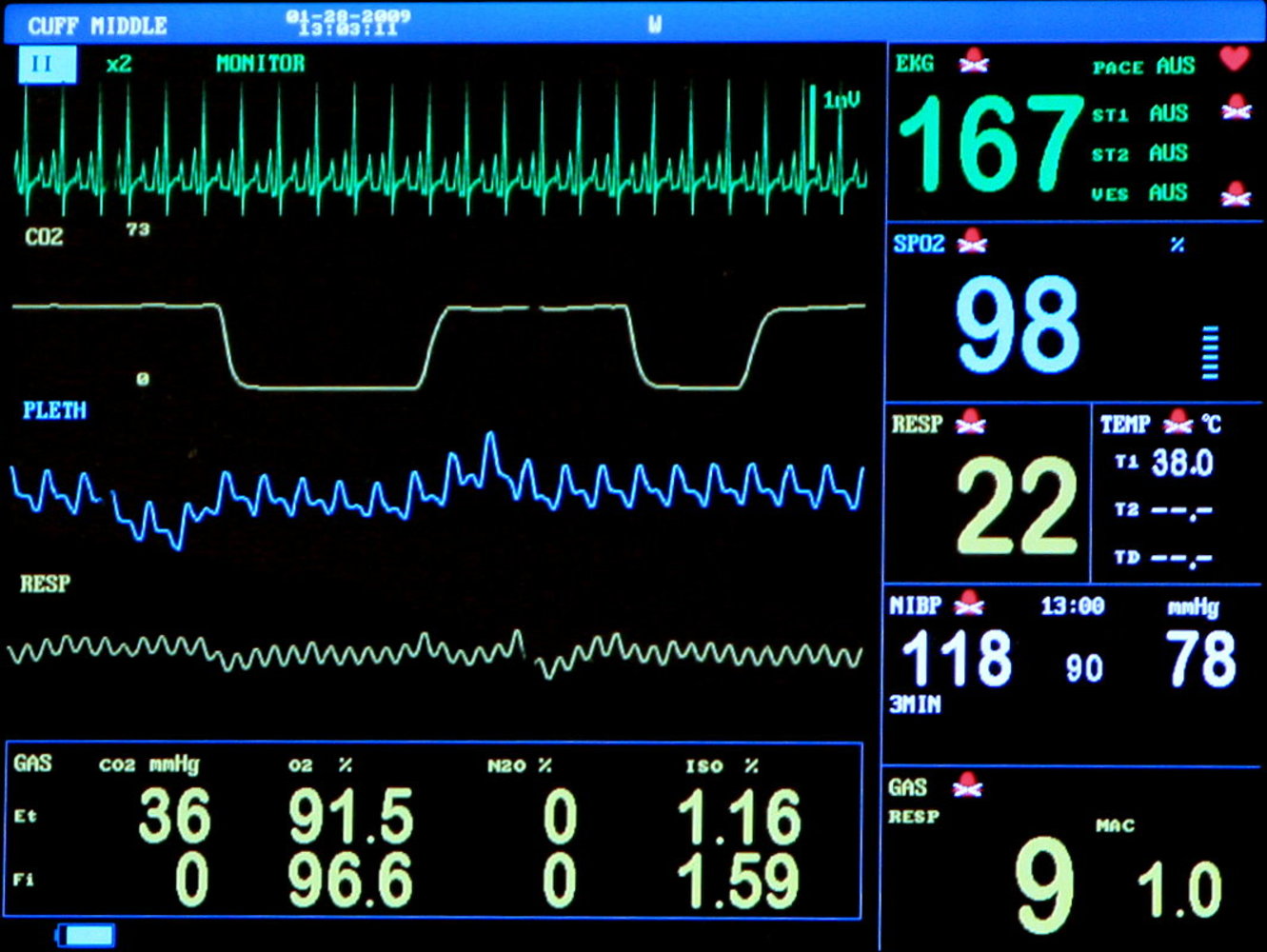
Photograph of a typical monitor used for mechanically-ventilated patients (in this case, during general anesthesia)
On the left side of the monitor from top to bottom shows the single lead EKG (green) trace, capnography (yellow), plethysmography (blue), and respiratory waveform (yellow). The bottom of the screen represents expiratory (Et) and inspiratory (Fi) pressures and percentages of different gasses: carbon dioxide (CO2), oxygen (O2), nitric oxide (N2O), and anesthetic gas (isoflurane).
The right side of the monitor from top to bottom shows heart rate (green), pulse oximetry (blue), respiratory rate (yellow) and temperature (light blue), systolic and diastolic blood pressure (white), and mean alveolar concentration (yellow).
Source: “Ansicht eines Narkosemonitors mit verschiedenen Parametern” by Kalumet, Wikimedia Commons, licensed under CC BY-SA 3.0.
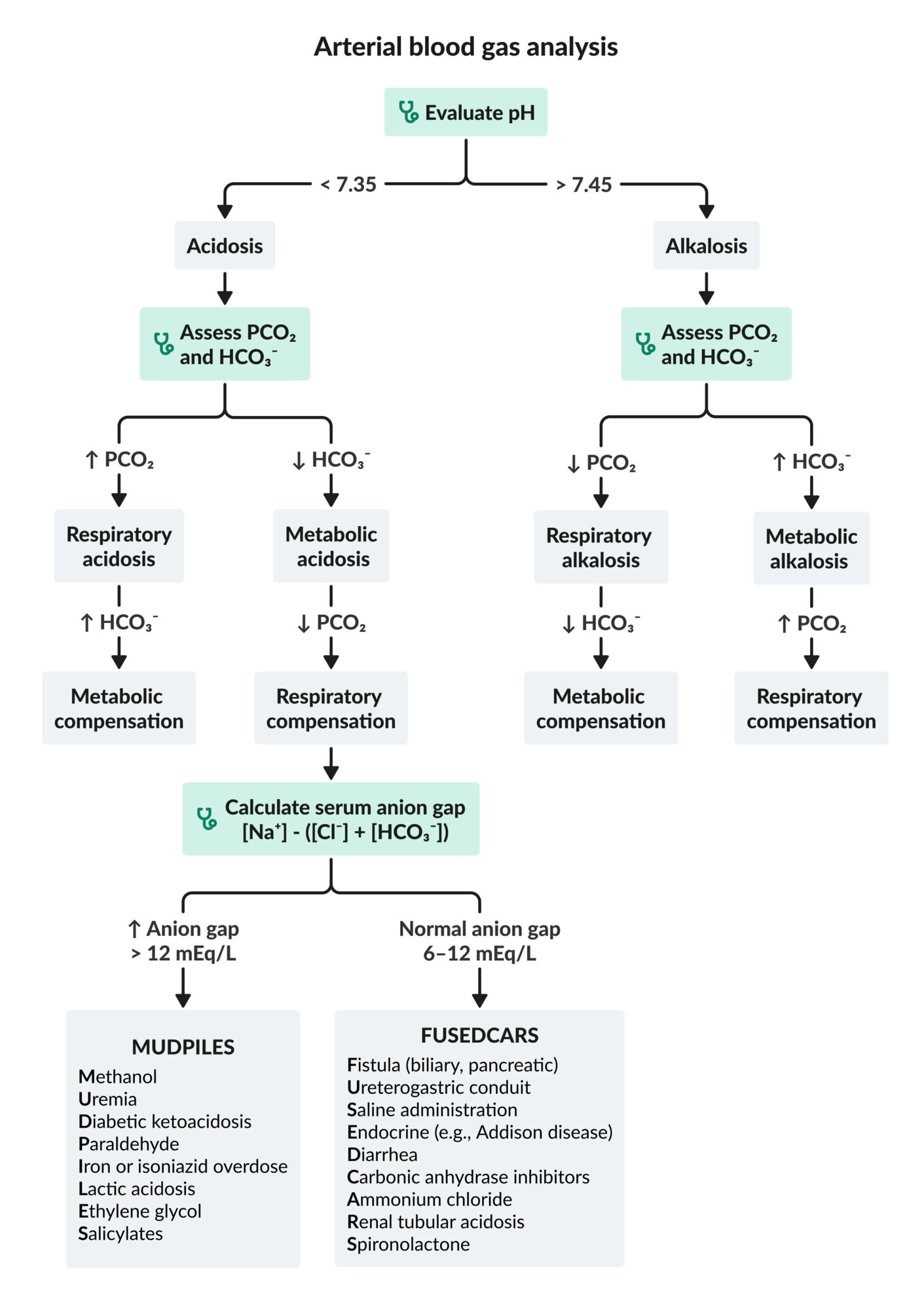
This algorithm does not account for mixed acid-base disorders.
Cl-: chloride
HCO3-: bicarbonate
Na+: sodium
PCO2: partial pressure of carbon dioxide
© AMBOSS
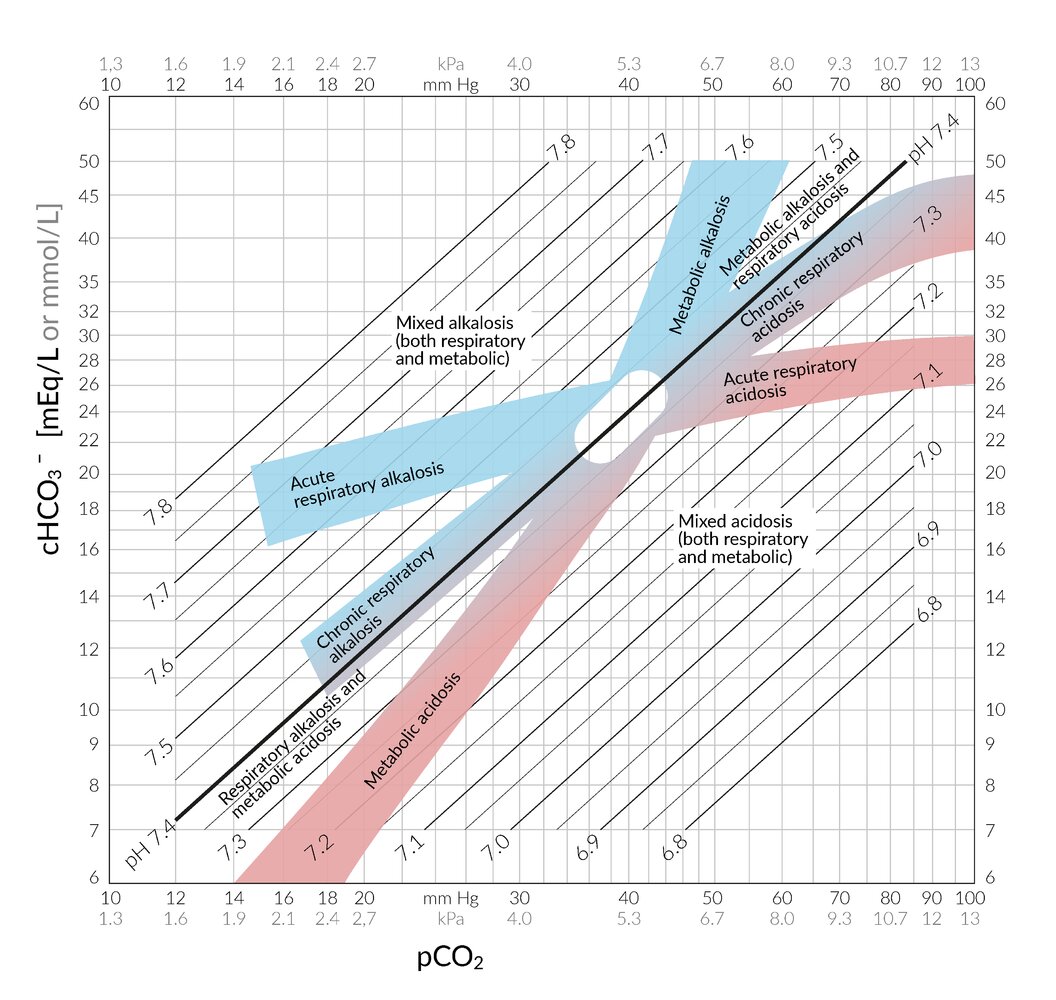
This nomogram can be used for the interpretation of an arterial blood gas analysis in the context of acid-base disorders.
PCO2 is on the x-axis and the concentration of HCO3- (cHCO3-) is on the y-axis; both are displayed logarithmically, allowing the pH to be displayed on parallel straight lines. The important areas for acid-base disorders are highlighted and labeled. The oval area in the middle around PCO2 = 40 mm Hg and cHCO3- = 24 mEq/L represents the reference range.
© AMBOSS
Complications
Ventilator-induced lung injury (VILI) [3][27]
VILI refers to both pulmonary and extrapulmonary injuries resulting from any combination of the following.
-
Pulmonary barotrauma [34]
- Mechanism: excess pressure in circuit → ↑ extra-alveolar air dissecting into other fascial planes and compartments
-
Aggravating factors
- ↑ PEEP
- ↓ Lung compliance
- ↑ Airway resistance
- ↑ Inspiratory flow rate
- Consequences
- Pneumothorax and/or tension pneumothorax
- Pneumomediastinum
- Pneumoperitoneum
- Subcutaneous emphysema
-
Volutrauma
- Mechanism: excess volume delivered → alveolar overdistention → disruption of alveolar-capillary membrane → release of inflammatory mediators
- Aggravating factors: ↑ Vt and ↓ lung compliance
-
Atelectrauma
- Mechanism: repeated opening and closing of alveoli (i.e., atelectasis) → shear stress → release of inflammatory mediators
- Aggravating factors: ↓ PEEP , ↓ Vt, ↓ pulmonary surfactant
-
Biotrauma
- Mechanism: release of inflammatory mediators from lung → systemic organ dysfunction
- Aggravating factors: volutrauma, atelectrauma
-
Oxygen toxicity [32][33]
- Mechanism: excess oxygen concentration → free radical formation, causing direct tissue injury (e.g., diffuse alveolar damage, tracheobronchitis) [13]
- Aggravating factor: ↑ FiO2
- Consequences: Hyperoxia is associated with higher mortality in critically ill patients than normoxemia.
Other complications
Intrapulmonary
- VAP: See “Prevention of ventilator-associated infections” and “Empiric antibiotic therapy for ventilator-associated pneumonia.”
- Inspiratory muscle weakness and deconditioning [35]
- Ventilator-associated pulmonary fibrosis: occurs in the subacute phase of ARDS [36][37]
Extrapulmonary [27]
- Gastric mucosal injury (e.g., PUD, GI bleed)
- Venous thromboembolism [27]
- Systemic deconditioning
- Pressure ulcers
- Contractures
We list the most important complications. The selection is not exhaustive.
Ventilation strategies

See "Mechanical ventilation in children" for pediatric ventilation strategies.
| Overview of high-risk indications for mechanical ventilation [38][39] | ||
|---|---|---|
| Condition | Cause of periintubation mortality | Preventative measures |
| Obstructive lung disease (e.g., asthma) |
|
|
|
|
|
| Severe acidosis HAGMA conditions (e.g., salicylate toxicity) CO2 narcosis (e.g., due to AECOPD) |
|
|
| Shock (e.g., sepsis) |
|
|
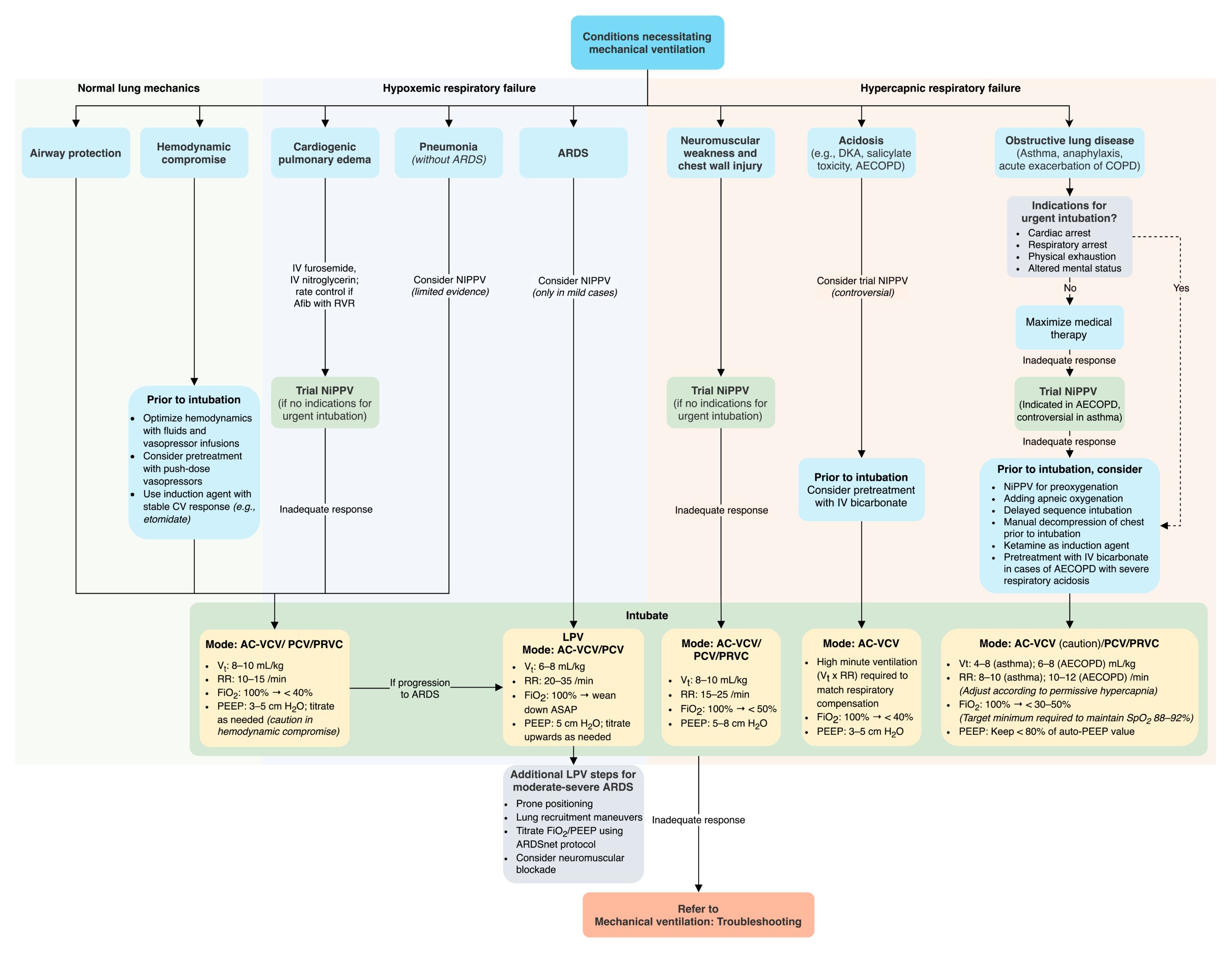
Normal lung mechanics [10][13][42]
-
Common uses
- Healthy patient undergoing elective surgery
- Intubation for airway protection (e.g., TBI, poisoning)
-
Typical settings
- Mode: initially any mandatory or mixed mode (AC/VCV, PCV, PRVC), then switch to PSV or SIMV
- Vt: 8–10 mL/kg ideal body weight
- RR: 10–15 breaths/min
- FiO2: Start at 100%, then rapidly titrate to < 40%
- PEEP: Start at 3–5 cm H2O.
-
Additional parameters
- I:E ratio: 1:2
- If switching to pressure support: See ventilator weaning.
- Positioning: supine
Permissive hypercapnia [43][44][45][46][47]
- Definition: the acceptance of hypercapnia (PaCO2> 45 mm Hg) as a byproduct of a given ventilation strategy
-
Rationale
- In some conditions (e.g., ARDS, asthma, AECOPD), targeting normocapnia increases the risk of VILI.
- Generally considered safe [48][49][50]
- Relative contraindication: acute intracranial disorders [49][51]
-
Procedure
- Ventilatory parameters are adjusted according to patient needs: See lung-protective ventilation strategy and obstructive lung disease ventilation strategy.
-
Arterial blood gas targets
- PaCO2: no clear upper limit; Experts suggest maintaining < 50 mm Hg as much as possible. [49]
- pH ≥ 7.25 generally acceptable [52]
-
Complications
- Acute cor pulmonale
- Organ dysfunction: cardiovascular and renal
Ventilation strategy for obstructive lung disease [10][13][42]
These are conditions with a high-risk of periintubation mortality.
-
Challenges
- Oxygenation
- Rapid desaturation, impaired lung dynamics, high oxygen demand and consumption
- Poor patient cooperation during preoxygenation due to hypoxia and distress
- Ventilation
- Severe bronchospasm/airway inflammation leads to increased resistance in the circuit and increased risk of barotrauma.
- Breath stacking leads to dynamic hyperinflation (DHI) and auto-PEEP.
- Oxygenation
-
Prevention
- Maximize noninvasive therapy prior to mechanical ventilation if time allows.
- Optimize periintubation medical treatment
- See high-risk indications for mechanical ventilation for the prevention of hypoxia, respiratory acidosis, and DHI.
Patients with obstructive lung disease are at high risk of periintubation mortality.
Asthma and anaphylaxis [53][54]
See “Intubation and mechanical ventilation in asthma” and “Airway management and ventilation in anaphylaxis” for details on indications and initial management.
-
Typical settings
- Mode
- Use caution with continuing AC/VCV.
- Consider switching to PCV or PRVC.
- Vt: 4–8 mL/kg, then adjust according to ABG
- RR: Adjust according to permissive hypercapnia.
- Increase if pH < 7.25.
- Acceptable ranges: 8–10 breaths/min
-
FiO2
- Initially 100%; rapid titration to < 30–50%
- Target minimum required to maintain SpO2 88–92%
- PEEP: Keep < 80% of auto-PEEP value (0–5 cm H₂O).
- Mode
-
Additional parameters
- Maximize expiratory time (e.g., consider I:E ratio 1:4 rather than 1:2).
- VI: 60–80 L/min
- Auto-PEEP: Keep to a minimum.
AECOPD [13][42]
- Indication: See indications for intubation in patients with AECOPD.
-
Typical settings
- Mode:
- Use caution with continuing AC/VCV.
- Consider switching to PCV or PRVC.
- Vt: 6–8 mL/kg
- RR: Adjust according to permissive hypercapnia.
- Increase if pH < 7.25.
- Acceptable ranges; 10–12 breaths/min
-
FiO2
- Initially 100%; rapid titration to < 30–50%
- Target minimum required to maintain SpO2 88–92%.
- PEEP: Keep < 80% of auto-PEEP value.
- Mode:
-
Additional parameters
- Maximize expiratory time (e.g., consider I:E ratio 1:4 rather than 1:2).
- VI: 60–80 L/min
- Auto-PEEP: Keep to a minimum.
Use the I:E ratio to maximize expiratory time and prevent auto-PEEP in obstructive lung disease.
Ventilation strategy for severe acidosis [10][13]
These are conditions with a high-risk of peri-intubation mortality.
-
Challenges
- The maximal respiratory compensation achievable by a ventilator is inferior to the patient's endogenous capacity.
- Apneic periods during intubation can dangerously lower pH due to CO2 buildup.
- Preparation: See high-risk indications for mechanical ventilation.
- Common uses: respiratory muscle fatigue in cases of salicylate toxicity, DKA, toxic alcohol poisoning, renal failure, COPD
-
Typical settings
- Mode: AC/VCV
- Vt/RR: needs to be optimized to match respiratory compensation [55]
- Use the Winter formula to identify desired PaCO2.
- In adults, can estimate initial target minute ventilation (Vt × RR) based on desired PaCO2
- 40 mm Hg: 6–8 L
- 30 mm Hg: 12–14 L
- 20 mm Hg: 18–20 L
- Adjust subsequent targets using the following formula:
- Target minute ventilation = (measured PaCO2 × current minute ventilation) ÷ desired PaCO2 [56]
- FiO2: Start at 100%, then rapidly titrate to < 40%.
- PEEP: Start at 3–5 cm H2O.
Optimizing the tidal volume and respiratory rate to match the patient's respiratory compensation is critical in patients with severe acidosis to avoid cardiac arrest.
Lung-protective ventilation strategy [10][13][20][31][42][57][58][59][60]
This is used in very high-risk and challenging clinical situations. Expert consultation is crucial during initiation and adjustment.
-
Rationale: LPV improves gas exchange while reducing the risk of VILI.
- Permissive hypercapnia is applied.
- Low tidal volumes to prevent volutrauma
- Low pressures (PPlat ≤ 30 cm H₂O) to prevent barotrauma
- Collapsed alveoli are recruited through various methods, e.g., PEEP titration and treatment of the underlying disease
- Deep sedation to reduce patient-ventilator dyssynchrony and oxygen demand (see adjunctive care of ventilated patients).
-
Common uses
- ARDS
- Acute lung injury (e.g., inhalational injury, TRALI)
- Severe VILI
-
Typical settings
- Mode: AC/VCV or AC/PCV [61]
- Vt: 6–8 mL/kg; Decrease to 4–6 mL/kg if PPlat > 30 cm H2O.
- RR
- Increase if pH < 7.25.
- Acceptable ranges: 20–35 breaths/min
-
FiO2 and PEEP: should be adjusted in tandem to the lowest PEEP/FiO2 combination defined in the ARDSnet protocol (see ARDS)
- FiO2: Start at 100% and wean down as soon as possible.
- PEEP: Start at 5 cm H₂O and adjust upwards as needed.
- Further titration of these parameters should follow the ARDSnet protocol increments.
Ventilation strategy for elevated ICP [14][62]
Elevated ICP is a high-risk condition primarily due to the adverse effects of induction medications and laryngoscopy. See intubation of patients with high ICP for airway management.
-
Common use
- High ICP refractory to other lowering measures
- Should only be used as a temporizing measure
- Avoid in the first 24 hours after head injury. [10][63]
-
Typical settings
- Mode: AC/VCV
- FiO2: 100%
- PEEP: ≤ 5 cm H₂O
- Vt/RR
- First 30 minutes
- Set initial Vt ≥ 8 mL/kg.
- Adjust RR to target PaCO2 30–35 mm Hg.
- Subsequently can reduce Vt to 6–8 mL/kg and adjust RR to target normocapnia (i.e., 35–40 mm Hg).
- First 30 minutes
- Additional parameters: Raise the head of the bed.
Ventilation strategy for neuromuscular weakness and chest wall injury [10][13]
-
Common uses
- Myelopathy
- Guillain-Barré syndrome
- Myasthenia gravis
- Flail chest
-
Typical settings
- Mode: AC/VCV, PCV, PRVC
- Vt: 8–10 mL/kg ideal body weight
- RR: 15–25 breaths/min
- FiO2: Start at 100%, then rapidly titrate to < 50%.
- PEEP: Start at 5–8 cm H₂O.
-
Additional parameters
- VI: 60–80 L/min
Ventilator weaning
- Definition: the process of easing a patient off mechanical ventilatory support
-
Typical settings
- Mode: PSV
- Vt/RR: set by patient
- FiO2: Begin at level from prior ventilatory mode (e.g., AC/VCV) and reduce to < 40%.
- PEEP: Begin at level from prior ventilatory mode (e.g., AC/VCV) and reduce to 3–5 cm H₂O.
-
Pressure support (PS)
- Range: 5–20 cm H₂O
- Initially choose the amount required to match the Vt delivered on the previous ventilation mode.
- Progressively reduce, as tolerated by the patient's clinical status and ventilatory parameters.
-
Spontaneous breathing trial [64]
- A test that is used to determine whether a mechanically ventilated patient is ready to breathe without a ventilator
- Criteria for extubation
- Patient is able to spontaneously initiate an inspiratory effort (i.e., good neuromuscular function).
- Underlying lung disease is stable/resolving.
- Adequate PaO2 and SpO2 on minimal support (e.g., PS ≤ 5 cm H₂O)
- pH ≥ 7.25
- Hemodynamically stable with little or no vasopressor therapy
Extubation with inadequate weaning (i.e., without proper muscle restrengthening) can lead to respiratory failure and require reintubation.
© AMBOSS
Pitfalls and troubleshooting

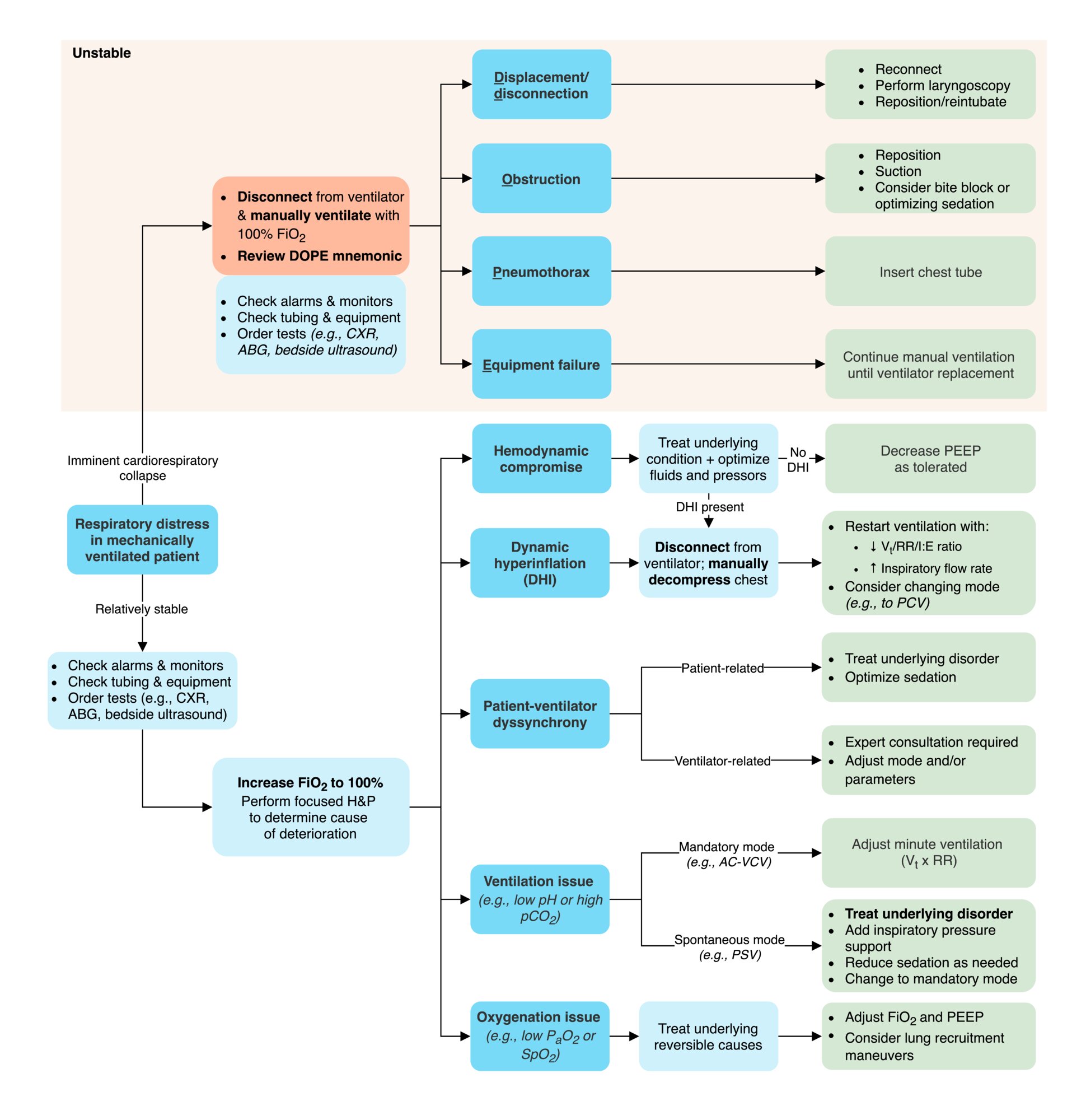
Approach to mechanically-ventilated patient in respiratory distress [3][10][13][27][38]
- If hemodynamically unstable: Disconnect the patient from the ventilator and switch to manual ventilation with 100% FiO2.
- If hemodynamically stable: Increase FiO2 to 100% until further assessment is complete.
- Perform focused clinical evaluation.
- Historical clues
- Changes in ventilator settings
- Changes in patient symptoms
- Recent instrumentation
- Attempts at repositioning
-
Physical examination
- Airway: position, patency, and presence of leaks
- Breathing: chest rise, lung auscultation, skin crepitus
- Circulation: signs of perfusion and hemodynamic status
- Historical clues
- Check monitors and alarms: Review PIP and PPlat.
- Inspect ventilator equipment and tubing.
- Perform bedside ultrasound or order portable CXR, as guided by clinical suspicion (e.g., to rule out pneumothorax).
In patients who are hemodynamically unstable, disconnect them from the ventilator and start manual ventilation with 100% FiO2.
Causes of sudden deterioration post-intubation [65][66]
-
Displacement/disconnection
- See airway management for ET tube troubleshooting.
- Check for disconnection in the circuit.
-
Obstruction: See airway management for causes.
- Deep suctioning with saline flushes
- Undo kinks in tubing.
- Evaluate patients biting ET tubes for causes of pain/discomfort.
- Adjust sedation and analgesia accordingly
- Apply a bite block.
-
Pneumothorax
- See “diagnostics” in pneumothorax for bedside ultrasound assessment.
- All mechanically ventilated patients with pneumothorax require urgent tube thoracostomy.
- If a tension pneumothorax is suspected, perform an urgent needle decompression.
-
Equipment failure
- If suspected, disconnect the patient from the ventilator and manually ventilate with 100% FiO2 until it can be replaced.
- Troubleshoot with a respiratory therapist.
Causes of sudden deterioration after intubation can be recalled using the DOPE mnemonic: Displacement/Disconnection, Obstruction, Pneumothorax, Equipment failure.
Improving oxygenation in mechanically ventilated patients
- Especially challenging in patients with hypoxemic respiratory failure
- Adjust FiO2 and PEEP.
- Increase FiO2 to rapidly deliver a higher oxygen concentration.
- Avoid prolonged exposure to high FiO2 levels (> 60%) to prevent hyperoxia/oxygen toxicity. [32][33]
- Avoid SpO2 ≥ 95% for prolonged periods, unless specifically indicated.
- If SpO2 is persistently 100%, check PaO2 on ABG (see “monitoring” above).
- Avoid prolonged exposure to high FiO2 levels (> 60%) to prevent hyperoxia/oxygen toxicity. [32][33]
- Increase PEEP if FiO2 > 60% is required. [67][68][69][70]
- Titrate up as needed to allow FiO2 to be reduced to less risky levels.
- Avoid prolonged exposure to high PEEP to minimize VILI.
- Aim for the lowest PEEP tolerated to maintain oxygenation target.
- Increase FiO2 to rapidly deliver a higher oxygen concentration.
- Treat reversible underlying causes of hypoxemia.
- Consider lung recruitment maneuvers for refractory hypoxemia.
Improving ventilation in mechanically ventilated patients
- Especially challenging in patients with hypercapnic respiratory failure
- Adjust minute ventilation (RR + Vt)
- If ABG is consistent with alkalosis (hypocapnia): Decrease minute ventilation.
- Decrease Vt.
- Decrease RR.
- If ABG is consistent with acidosis (hypercapnia): Increase minute ventilation.
- Increase Vt: limited by risk of VILI
- Increase RR: limited by expiration time (risk of DHI)
- If in PSV mode, acidosis and/or hypercapnia may indicate low volumes inspired.
- If due to oversedation: Reduce sedative dose.
- If due to respiratory muscle fatigue or decrease in lung compliance:
- Add inspiratory pressure.
- Switch to mode with greater assistance (e.g., AC, PRVC).
- Address reversible underlying disorders (e.g., asthma exacerbation, AECOPD, acute heart failure, pneumothorax).
- If ABG is consistent with alkalosis (hypocapnia): Decrease minute ventilation.
- If patient-ventilator dyssynchrony present: Increase sedation and consider paralysis.
Hemodynamic compromise in mechanically ventilated patients [3][11][71]
- Mechanism: PPV can cause or exacerbate shock (see “Effects” in “Positive pressure ventilation”).
-
Aggravating factors
- Induction agents with vasodilatory side effects (e.g., propofol)
- RV dysfunction
- Hypovolemia, peripheral vasodilation
- ↑ PEEP and auto-PEEP
-
Consequences
- Obstructive shock
- Circulatory collapse
- Cardiac arrest
-
Management
- Treat DHI if present.
- Decrease PEEP if tolerated.
- Optimize fluid resuscitation.
- Consider vasopressor infusions and push-dose pressors.
Patient-ventilator dyssynchrony [72]
-
Description
- A mismatch between patient and equipment
- Airflow: The flow delivered by the ventilator is inconsistent with the patient's demand.
- Phase: The timing and cycle of ventilator-delivered breaths are misaligned with the patient's respiratory drive.
- A mismatch between patient and equipment
-
Recognition
- Often identified by nursing staff or respiratory therapists
- Possible clues [72]
- Biological: unstable vital signs, pressure/flow waveform patterns, changes in ABG parameters, EtCO2
- Behavioral: coughing, signs of increased respiratory effort , agitation
-
Aggravating factors
- Patient-related
- ↑ Respiratory drive: hypoxemia, hypercapnia, metabolic acidosis, hypermetabolic states, anxiety, fever, pain, medications
- ↓ Respiratory drive: metabolic alkalosis, medications (e.g., sedatives, opioids), hypometabolic states
- Lung mechanics: weak respiratory musculature, prolonged expiration time (e.g., obstructive lung disease), impaired neuromuscular control
- Underlying disease: delirium, obstructive lung disease, ARDS, pulmonary edema, pulmonary embolism, pneumothorax
- Other conditions: poor positioning, chest wall splinting, abdominal distention
- Ventilator-related
- Airway: mucus plugs, poor sizing
- Leaks and disconnections in system
- Increased instrumental dead space
- FiO2 too low
- Inappropriate PEEP setting
- Inappropriate triggers sensitivity
- Patient-related
-
Consequences
- Discomfort
- Hypoxia, barotrauma
- Prolonged mechanical ventilation
- Patient biting on ET tube, causing obstruction
-
Management
- Check ventilator circuitry for reversible malfunction.
- Check ventilation monitors, waveforms, and alarms.
- Examine the patient and order appropriate diagnostic tests (see “aggravating factors” above).
- Collaborate with nursing staff and respiratory therapists for guidance.
- Identify and treat the underlying cause.
- Change ventilation parameters or mode to match patient needs.
- Ensure adequate patient sedation in line with patient needs and goals of care.
Dynamic hyperinflation (DHI) [30][66]
- Description: progressively increased airway and intrathoracic pressures with each ventilation cycle
- Mechanism: Initiation of new breath before full expiration → breath stacking → progressively increased intrathoracic pressure
-
Recognition
- Respiratory distress
- High pressure or low volume alarms
- Hemodynamic instability
-
Aggravating factors
- Patients at high risk of developing auto-PEEP (e.g., patients with obstructive lung disease)
- Poorly set ventilatory parameters (e.g., Vt/RR that are too high)
-
Consequences
- Increased work of breathing
- Ineffective ventilation
- Ventilator dyssynchrony
- Barotrauma and volutrauma (see VILI)
- Shock and circulatory collapse (see “hemodynamic comprise” above)
- Unreliable monitoring
-
Management
- Disconnect the patient from the ventilator.
- Externally compress the chest to deflate the lung.
- Adjust ventilator settings before reconnecting (see “prevention” below).
- Identify and treat any underlying reversible conditions.
- Treat expiratory airflow obstruction: e.g., bronchodilators, suctioning.
- Treat central drivers of hyperventilation: e.g., analgesia, sedation.
- Treat refractory patient-ventilator dyssynchrony; e.g., muscle relaxants.
-
Prevention
- Goal: Allow more expiratory time to minimize auto-PEEP.
- Choose mode with ↓ risk of DHI: e.g., PCV
- Parameter adjustments
- Decrease Vt.
- Decrease RR.
- Decrease I:E ratio.
- Increase VI.
© AMBOSS
Ventilator alarms
There are currently no accepted consensus guidelines on appropriate alarm settings or responses. Ranges vary by patient, ventilator model, type of critical care unit, and institution. Refer to local alarm thresholds and ranges, or consult an experienced critical care specialist and/or respiratory therapist. [27][54][73][74]
Treat ventilator alarms as a critical issue. Beware of alarm fatigue.
| Interpretation of ventilator alarms | ||
|---|---|---|
| Alarm | Possible causes | |
| High PIP | PPlat elevated |
|
| PPlat low or normal |
|
|
| Low pressure |
|
|
| High RR |
|
|
This algorithm does not account for mixed acid-base disorders.
Cl-: chloride
HCO3-: bicarbonate
Na+: sodium
PCO2: partial pressure of carbon dioxide
© AMBOSS
Related One-Minute Telegram
- One-Minute Telegram 145-2026-3/3: Less restraint for ventilated ICU patients does not improve outcomes
- One-Minute Telegram 145-2026-1/3: High-flow vs. standard O2 in the ICU: less intubation, similar mortality
- One-Minute Telegram 108-2024-1/3: Can high-intensity NIPPV prevent intubation in AECOPD?
- One-Minute Telegram 20-2021-1/3: Better outcomes after implementation of critical care management protocols?
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- Sign up for the One-Minute Telegram
- 2017 Official ATS/ESICM/SCCM Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with ARDS
- 2017 Official ERS/ATS Clinical Practice Guidelines: Noninvasive Ventilation for Acute Respiratory Failure
- 2016 BTS/ICS Guideline for the Ventilatory Management of Acute Hypercapnic Respiratory Failure in Adults
- 2016 SCCM Clinical Practice Guidelines for Sustained Neuromuscular Blockade in the Adult Critically Ill Patient
References
- Roberts JR. "Roberts and Hedges' Clinical Procedures in Emergency Medicine and Acute Care". Elsevier. (2018). ISBN: 9780323354783
- Rochwerg B, Brochard L, Elliott MW, et al. "Official ERS/ATS clinical practice guidelines: noninvasive ventilation for acute respiratory failure". Eur Respir J.. 50(2). :1602426. (2017)
- Davidson AC, Banham S, Elliott M, et al. "BTS/ICS guideline for the ventilatory management of acute hypercapnic respiratory failure in adults". Thorax. 71(Suppl 2). :ii1-ii35. (2016)
- Weingart SD, Levitan RM. "Preoxygenation and Prevention of Desaturation During Emergency Airway Management". Ann Emerg Med. 59(3). :165-175.e1. (2012)
- American Thoracic Society. "International Consensus Conferences in Intensive Care Medicine: Noninvasive Positive Pressure Ventilation in Acute Respiratory Failure". Am J Respir Crit Care Med. 163(1). :283-291. (2001)
- Kelly CR, Higgins AR, Chandra S. "Noninvasive Positive-Pressure Ventilation". N Engl J Med. 372(23). :e30. (2015)
- "Aspiration Risk". https://www.ncbi.nlm.nih.gov/pubmed/29262188. [2019-01-01]
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Delbove A, Darreau C, Hamel JF, Asfar P, Lerolle N. "Impact of endotracheal intubation on septic shock outcome: A post hoc analysis of the SEPSISPAM trial". J Crit Care. 30(6). :1174-1178. (2015)
- Mosier JM, Hypes C, Joshi R, et al. "Ventilator Strategies and Rescue Therapies for Management of Acute Respiratory Failure in the Emergency Department". Ann Emerg Med. 66(5). :529-541. (2015)
- Archambault PM, St-Onge M. "Invasive and Noninvasive Ventilation in the Emergency Department". Emerg Med Clin North Am. 30(2). :421-449. (2012)
- Godoy DA, Seifi A, Garza D, Lubillo-Montenegro S, Murillo-Cabezas F. "Hyperventilation Therapy for Control of Posttraumatic Intracranial Hypertension". Frontiers in Neurology. 8. :250. (2017)
- Robba C, Poole D, McNett M, et al. "Mechanical ventilation in patients with acute brain injury: recommendations of the European Society of Intensive Care Medicine consensus". Intensive Care Med. 46(12). :2397-2410. (2020)
- Devlin JW, Skrobik Y, Gélinas C, et al. "Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU". Crit Care Med. 46(9). :e825-e873. (2018)
- Patel SB, Kress JP. "Sedation and Analgesia in the Mechanically Ventilated Patient". Am J Respir Crit Care Med. 185(5). :486-497. (2012)
- Pandharipande P, Hughes, McGrane. "Sedation in the intensive care setting". Clinical Pharmacology: Advances and Applications. 4. :53-63. (2012)
- Manasco AT, Stephens RJ, Yaeger LH, Roberts BW, Fuller BM. "Ketamine sedation in mechanically ventilated patients: A systematic review and meta-analysis". J Crit Care. 56. :80-88. (2020)
- The National Heart, Lung, and Blood Institute PETAL Clinical Trials Network. "Early Neuromuscular Blockade in the Acute Respiratory Distress Syndrome". N Engl J Med. 380(21). :1997-2008. (2019)
- Murray MJ, DeBlock H, Erstad B, et al. "Clinical Practice Guidelines for Sustained Neuromuscular Blockade in the Adult Critically Ill Patient". Crit Care Med. 44(11). :2079-2103. (2016)
- Jelic S, Cunningham JA, Factor P. "Clinical review: Airway hygiene in the intensive care unit". Critical Care. 12(2). :209. (2008)
- Kacmarek RM. "The Mechanical Ventilator: Past, Present, and Future". Respir Care. 56(8). :1170-1180. (2011)
- Silva PL, Rocco PRM. "The basics of respiratory mechanics: ventilator-derived parameters". Annals of Translational Medicine. 6(19). :376-376. (2018)
- Miller N. "Set the stage for ventilator settings". Nursing Made Incredibly Easy!. 11(3). :44-52. (2013)
- Pham T, Brochard LJ, Slutsky AS. "Mechanical Ventilation: State of the Art". Mayo Clinic Proceedings. 92(9). :1382-1400. (2017)
- Singh G, Chien C, Patel S. "Pressure Regulated Volume Control (PRVC): Set it and forget it?". Respiratory Medicine Case Reports. :100822. (2019)
- Goligher EC, Ferguson ND, Brochard LJ. "Clinical challenges in mechanical ventilation". The Lancet. 387(10030). :1856-1866. (2016)
- Mosier J, Joshi R, Hypes C, et al. "The Physiologically Difficult Airway". Western Journal of Emergency Medicine. 16(7). :1109-1117. (2015)
- Stolbach AI, Hoffman RS, Nelson LS. "Mechanical Ventilation Was Associated with Acidemia in a Case Series of Salicylate-poisoned Patients". Academic Emergency Medicine. 15(9). :866-869. (2008)
- Kuzak N, Brubacher JR, Kennedy JR. "Reversal of salicylate-induced euglycemic delirium with dextrose". Clin Toxicol. 45(5). :526-529. (2007)
- Weingart SD. "Managing Initial Mechanical Ventilation in the Emergency Department". Ann Emerg Med. 68(5). :614-617. (2016)
- Acute Respiratory Distress Syndrome Network, Brower RG, Matthay MA, et al. "Ventilation with Lower Tidal Volumes as Compared with Traditional Tidal Volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome". N Engl J Med. 342(18). :1301-1308. (2000)
- Bigatello LM, Patroniti N, Sangalli F. "Permissive hypercapnia.". Curr Opin Crit Care. 7(1). :34-40. (2001)
- Bidani A, Tzouanakis AE, Cardenas VJ Jr, Zwischenberger JB. "Permissive hypercapnia in acute respiratory failure.". JAMA. 272(12). :957-62. (1994)
- Feihl F, Perret C. "Permissive hypercapnia. How permissive should we be?". Am J Respir Crit Care Med. 150(6). :1722-1737. (1994)
- Barnes T, Zochios V, Parhar K. "Re-examining Permissive Hypercapnia in ARDS". Chest. 154(1). :185-195. (2018)
- Rogovik A, Goldman R. "Permissive Hypercapnia". Emerg Med Clin North Am. 26(4). :941-952. (2008)
- Garg SK. "Permissive hypercapnia: Is there any upper limit?". Indian Journal of Critical Care Medicine. 18(9). :612-614. (2014)
- O'Croinin D, Ni Chonghaile M, Higgins B, Laffey JG. "Bench-to-bedside review: Permissive hypercapnia.". Crit Care. 9(1). :51-9. (2005)
- Roberts BW, Karagiannis P, Coletta M, et al. "Effects of PaCO2 derangements on clinical outcomes after cerebral injury: A systematic review.". Resuscitation. 91. :32-41. (2015)
- Lipes J, Bojmehrani A, Lellouche F. "Low Tidal Volume Ventilation in Patients without Acute Respiratory Distress Syndrome: A Paradigm Shift in Mechanical Ventilation". Critical Care Research and Practice. 2012. :1-12. (2012)
- Leatherman J. "Mechanical Ventilation for Severe Asthma". Chest. 147(6). :1671-1680. (2015)
- Laher AE, Buchanan SK. "Mechanically Ventilating the Severe Asthmatic". J Intensive Care Med. 33(9). :491-501. (2017)
- "Simplifying Mechanical Ventilation – Part 3: Severe Metabolic Acidosis". https://rebelem.com/simplifying-mechanical-ventilation-part-3-severe-metabolic-acidosis/. [2018-06-18]
- Wexler HR, Lok P. "A simple formula for adjusting arterial carbon dioxide tension". Can Anaesth Soc J. 28(4). :370-372. (1981)
- Fan E, Del Sorbo L, Goligher EC, et al. "An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome". Am J Respir Crit Care Med. 195(9). :1253-1263. (2017)
- Curley GF, Laffey JG, Zhang H, Slutsky AS. "Biotrauma and Ventilator-Induced Lung Injury". Chest. 150(5). :1109-1117. (2016)
- Weiss CH, McSparron JI, Chatterjee RS, et al. "Summary for Clinicians: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome Clinical Practice Guideline". Annals of the American Thoracic Society. 14(8). :1235-1238. (2017)
- Wright BJ. "Lung-protective Ventilation Strategies and Adjunctive Treatments for the Emergency Medicine Patient with Acute Respiratory Failure". Emerg Med Clin North Am. 32(4). :871-887. (2014)
- Papazian L, et al. "Formal guidelines: management of acute respiratory distress syndrome". Annals of Intensive Care. 9(1). (2019)
- Bein T, Grasso S, Moerer O, et al. "The standard of care of patients with ARDS: ventilatory settings and rescue therapies for refractory hypoxemia". Intensive Care Med. 42(5). :699-711. (2016)
- Asehnoune K, Roquilly A, Cinotti R. "Respiratory Management in Patients with Severe Brain Injury". Critical Care. 22(1). :76. (2018)
- American College of Surgeons and the Committee on Trauma. "ATLS Advanced Trauma Life Support". American College of Surgeons. (2018). ISBN: 9780996826235
- MacIntyre NR. "Evidence-Based Guidelines for Weaning and Discontinuing Ventilatory Support". Chest. 120(6). :375S-395S. (2001)
- Wood S, Winters ME. "Care of the Intubated Emergency Department Patient". J Emerg Med. 40(4). :419-427. (2011)
- Kleinman ME, Chameides L, Schexnayder SM, et al. "Part 14: Pediatric Advanced Life Support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care". Circulation. 122(18_suppl_3). :S876-S908. (2010)
- Kapil S, Wilson JG. "Mechanical Ventilation in Hypoxemic Respiratory Failure". Emerg Med Clin North Am. 37(3). :431-444. (2019)
- Page D, Ablordeppey E, Wessman BT, et al. "Emergency department hyperoxia is associated with increased mortality in mechanically ventilated patients: a cohort study". Critical Care. 22(1). :9. (2018)
- Durlinger EMJ, Spoelstra-de Man AME, Smit B, et al. "Hyperoxia: At what level of SpO 2 is a patient safe? A study in mechanically ventilated ICU patients". J Crit Care. 39. :199-204. (2017)
- Kallet RH, Branson RD. "Respiratory controversies in the critical care setting. Do the NIH ARDS Clinical Trials Network PEEP/FIO2 tables provide the best evidence-based guide to balancing PEEP and FIO2 settings in adults?". Respir Care. 52(4). :461-75; discussion 475-7. (2007)
- Cavalcanti AB, Amato MBP, Serpa-Neto A. "The Elusive Search for “Best PEEP” and Whether Esophageal Pressure Monitoring Helps". JAMA. 321(9). :839. (2019)
- Sahetya SK. "Searching for the optimal positive end-expiratory pressure for lung protective ventilation". Curr Opin Crit Care. 26(1). :53-58. (2020)
- Hubmayr RD, Malhotra A. "Still Looking for Best PEEP". Anesthesiology. 121(3). :445-446. (2014)
- Weingart S. "Push-dose pressors for immediate blood pressure control". Clinical and Experimental Emergency Medicine. 2(2). :131-132. (2015)
- Mellott KG, Grap MJ, Munro CL, Sessler CN, Wetzel PA. "Patient-Ventilator Dyssynchrony: Clinical Significance and Implications for Practice". Crit Care Nurse. 29(6). :41-55. (2009)
- Marini JJ. "Dynamic Hyperinflation and Auto–Positive End-Expiratory Pressure". Am J Respir Crit Care Med. 184(7). :756-762. (2011)
- Ioannidis G, Lazaridis G, Baka S, et al. "Barotrauma and pneumothorax.". Journal of thoracic disease. 7(Suppl 1). :S38-43. (2015)
- Moodie LH, Reeve JC, Vermeulen N, Elkins MR. "Inspiratory muscle training to facilitate weaning from mechanical ventilation: protocol for a systematic review". BMC Research Notes. 4(1). :283. (2011)
- Zhang R, Pan Y, Fanelli V, et al. "Mechanical Stress and the Induction of Lung Fibrosis via the Midkine Signaling Pathway". Am J Respir Crit Care Med. 192(3). :315-323. (2015)
- Cabrera-Benitez NE, Laffey JG, Parotto M, et al. "Mechanical Ventilation–associated Lung Fibrosis in Acute Respiratory Distress Syndrome". Anesthesiology. 121(1). :189-198. (2014)
- Richardson M, Moulton K, Rabb D, et al. "Capnography for Monitoring End-Tidal CO2 in Hospital and Pre-hospital Settings: A Health Technology Assessment". CADTH Health Technology Assessment. (2016)
- Cvach MM, Stokes JE, Manzoor SH, et al. "Ventilator Alarms in Intensive Care Units". Anesthesia & Analgesia. 130(1). :e9-e13. (2020)
- Scott JB, De Vaux L, Dills C, Strickland SL. "Mechanical Ventilation Alarms and Alarm Fatigue". Respir Care. 64(10). :1308-1313. (2019)
- Hess DR. "Respiratory Mechanics in Mechanically Ventilated Patients". Respir Care. 59(11). :1773-1794. (2014)
- Corp A, Thomas C, Adlam M. "The cardiovascular effects of positive pressure ventilation". BJA Education. 21(6). :202-209. (2021)
- "Management of bronchospasm during general anaesthesia"
- Thompson BT, et al. "Acute Respiratory Distress Syndrome". N Engl J Med. 377(6). :562-572. (2017)
- Rawal G, et al. "Acute respiratory distress syndrome: An update and review". Journal of Translational Internal Medicine. 6(2). :74-77. (2018)
- Papazian L, et al. "Neuromuscular Blockers in Early Acute Respiratory Distress Syndrome". N Engl J Med. 363(12). :1107-1116. (2010)
- Griffiths MJD, et al. "Guidelines on the management of acute respiratory distress syndrome". BMJ Open Respiratory Research. 6(1). :e000420. (2019)
- Guérin C, et al. "Prone Positioning in Severe Acute Respiratory Distress Syndrome". N Engl J Med. 368(23). :2159-2168. (2013)
- Messerole E, et al. "The Pragmatics of Prone Positioning". Am J Respir Crit Care Med. 165(10). :1359-1363. (2002)
- Walkey AJ, Del Sorbo L, Hodgson CL, et al. "Higher PEEP versus Lower PEEP Strategies for Patients with Acute Respiratory Distress Syndrome. A Systematic Review and Meta-Analysis". Annals of the American Thoracic Society. 14(Supplement_4). :S297-S303. (2017)
- Hess DR. "Recruitment Maneuvers and PEEP Titration". Respir Care. 60(11). :1688-1704. (2015)