Quick guide
Diagnostic approach
- ABCDE survey
- Evaluation for clinical features of meningitis
- Blood cultures (two sets)
- CBC
- BMP
- CRP
- Coagulation panel
- Neuroimaging (e.g., CT head) if criteria for imaging prior to LP are present.
- LP and CSF analysis

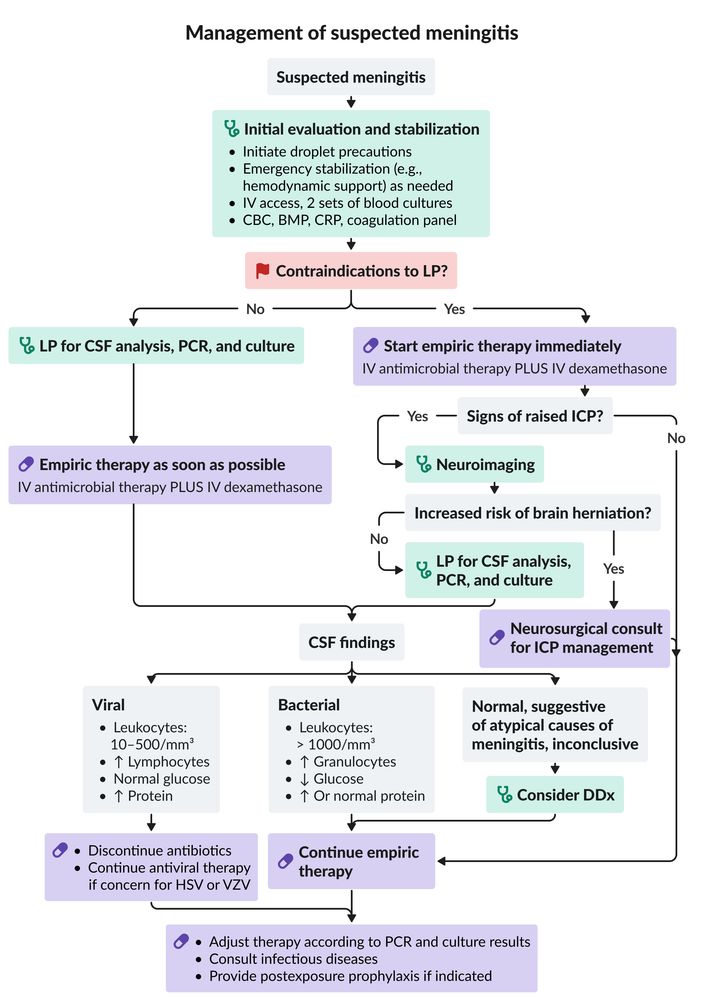
Do not delay administering antibiotics if neuroimaging is indicated prior to LP. Obtain blood cultures, start antibiotics (and steroids, if needed) immediately, then proceed with the CT and LP.
Red flag features
- Altered mental status
- Focal neurological deficits
- New-onset seizures
- Signs of increased ICP
- Petechial or purpuric rash
- Hemodynamic instability
- GCS < 8
Management checklist
- Droplet precautions
- IV access
- Continuous monitoring
- Empiric antibiotic therapy for bacterial meningitis within 1 hour
- Dexamethasone
- Acyclovir if viral encephalitis is suspected
- Hemodynamic support with fluids and/or vasopressors as indicated
- Airway management as indicated
- Consult infectious diseases.
- Consult neurology and/or neurosurgery (e.g., for elevated ICP).
BMP: basic metabolic panel
CBC: complete blood count
CRP: C-reactive protein
CSF: cerebrospinal fluid
DDx: differential diagnoses
HSV: herpes simplex virus
ICP: intracranial pressure
IV: intravenous
LP: lumbar puncture
PCR: polymerase chain reaction
VZV: varicella zoster virus
© AMBOSS
Summary
Meningitis is an infection of the meninges in the brain or spinal cord. Common causes include viruses and bacteria, although fungal, parasitic, and noninfectious causes of meningitis are possible. The most common bacterial pathogens (N. meningitidis, S. pneumoniae, H. influenzae, Group B streptococcus, and L. monocytogenes) vary depending on age and underlying medical conditions. Enteroviruses and herpes simplex virus (HSV) are the leading causes of viral meningitis. The classic triad of meningitis (fever, meningismus, altered mental state) occurs in less than half of adult patients and meningitis in children frequently presents with nonspecific symptoms. Advanced infection includes signs of increased intracranial pressure (ICP), neurological deficits, altered mental status, and seizures. Diagnosis is confirmed with CSF analysis and microbiological studies (e.g., PCR, culture). If increased ICP is suspected, a CT of the head is recommended prior to lumbar puncture (LP). Antibiotic therapy should not be delayed for diagnostic testing. Bacterial meningitis requires rapid initiation of empiric antimicrobials and sometimes glucocorticoids to prevent complications, which include neurological deficits (e.g., hearing loss) and end-organ damage (e.g., Waterhouse-Friderichsen syndrome in patients with meningococcal meningitis). While most cases of viral meningitis are self-limiting, herpesvirus infections (e.g., HSV, VZV) must be promptly recognized and treated with IV acyclovir to prevent serious complications and death. Prevention is through vaccination against common causes of meningitis, and chemoprophylaxis for exposed contacts.
Neonatal bacterial meningitis is detailed separately.
Epidemiology
- In the pediatric population, meningitis most often occurs in children < 1 year of age. [1]
- The median age for meningitis in the adult population is 43 years. [2]
- Sub-Saharan Africa has the worldwide highest incidence of meningitis caused by N. meningitidis. [3]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Common causes
- Otitis media
- Sinusitis
- CSF leak after head trauma or neurosurgery
- Maternal group B streptococcal infection during birth
- Sepsis
Risk factors
- Immunocompromise (e.g., due to AIDS, asplenia, heavy alcohol use disorder, chronic illness, cancer, sickle cell anemia, old age, pregnancy)
- Crowded occupational or living conditions (e.g., college dormitories, military barracks, retirement homes, kindergartens)
- Close contact with an infected person
Most common causative agents of bacterial meningitis by age group and underlying condition [4][5]
| Patient population | Pathogen |
|---|---|
| By age | |
| < 1 month [1][6][7] |
|
| 1 month–2 years [2][6] [9] |
|
| 2–50 years [2][12] |
|
| > 50 years [2][13] |
|
| By underlying condition | |
| Immunocompromise [14] |
|
| Basilar skull fracture [13] |
|
| Penetrating trauma [13] |
|
| Health care-associated [15] |
|
Less common bacterial pathogens
- Borrelia spp. (Lyme meningitis)
- Treponema pallidum (syphilitic meningitis)
- Mycobacterium tuberculosis (tuberculous meningitis)
- Actinomyces israelii
- Leptospira (leptospirosis)
Other etiologies
-
Viral meningitis: often associated with encephalitis (meningoencephalitis)
- Enteroviruses (especially coxsackieviruses and echoviruses): the most common cause of all types of meningitis in all patient groups [16]
- Herpesviruses: HSV (meningitis is more commonly caused by HSV2 than HSV1) , CMV, EBV, VZV
- Lymphocytic choriomeningitis virus (LCMV)
- Mumps virus
- Measles virus
- Some arboviruses (e.g., West Nile virus, TBEV in Eurasia)
- Poliovirus (nonparalytic poliomyelitis: aseptic meningitic form)
- St. Louis encephalitis virus
- California encephalitis virus
- Western equine encephalitis virus
- Influenza virus
- HIV
- JC virus [17]
-
Fungal meningitis
- Coccidioides
- Candida spp.
- Aspergillus spp.
-
Parasitic meningitis
- Helminths (e.g., Echinococcus spp., Strongyloides stercoralis, Angiostrongyliasis cantonensis, Baylisascaris procyonis)
- Protozoa (e.g., Naegleria fowleri; , Acanthamoeba)
-
Noninfectious meningitis
- Sarcoidosis
- Tumor metastases (meningeal carcinomatosis and meningeal leukemia)
- Medication (e.g., NSAIDs, sulfa drugs) [18]
Causes of meningitis in immunocompromised individuals
-
Bacterial
- Certain immune deficiencies can predispose to certain types of meningitis. [19]
- Defects in humoral immunity (including splenectomy): encapsulated bacteria (N. meningitidis, S. pneumoniae, H. influenzae, etc.)
- Defects in cell-mediated immunity (e.g., in HIV, drug-induced immunosuppression): M. tuberculosis, L. monocytogenes
- Immunocompromised individuals are at increased risk of recurrent bacterial meningitis compared to those with intact immunity. [14]
- Certain immune deficiencies can predispose to certain types of meningitis. [19]
-
Viral: Risk is higher in individuals with cell-mediated immune deficiencies (e.g., in HIV infection). [20]
- Herpesviruses: CMV, EBV, VZV, and HSV6
- HIV
- Adenovirus
- JC virus [17]
-
Fungal: Risk is higher in individuals with cell-mediated immune deficiencies (e.g., HIV infection). [21]
- Cryptococcus spp.
- Candida spp.
- Histoplasma capsulatum
- Aspergillus spp.
- Protozoal: Toxoplasma gondii (rare) [22]
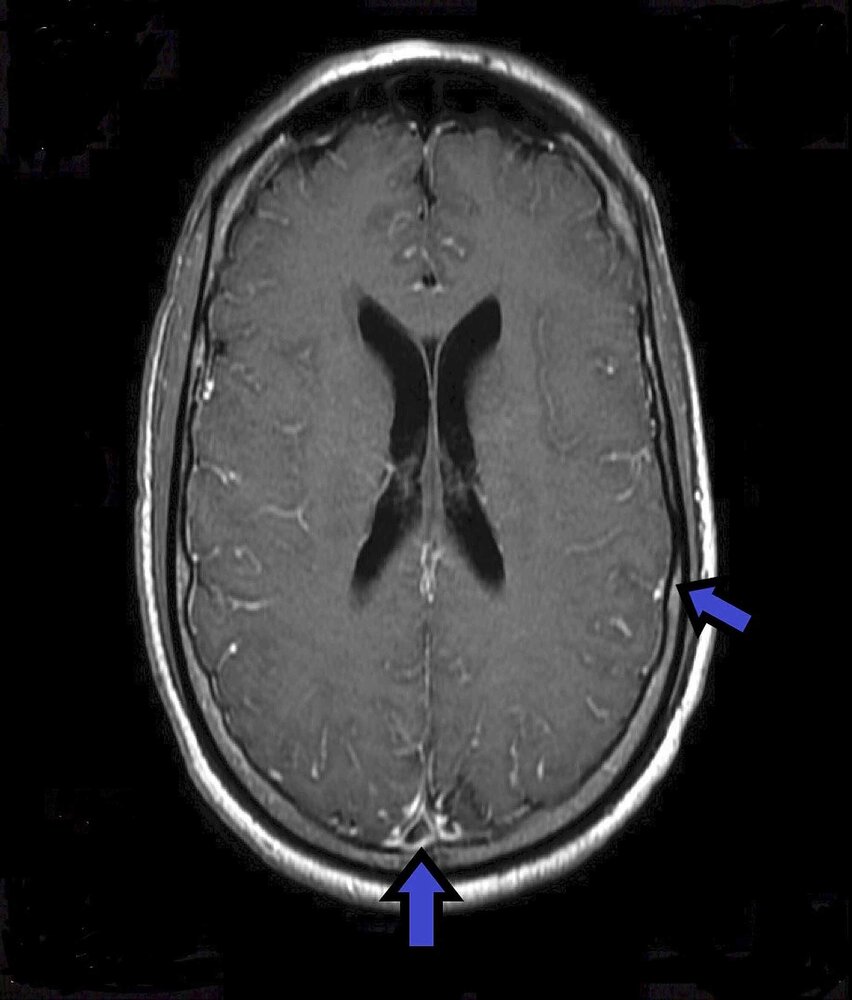
MRI head (with contrast; T1-weighted; axial plane) of a 58-year-old patient with monoclonal gammopathy and polycythemia vera who presented with confusion, fatigue, and auditory hallucinations for one week.
Mild meningeal enhancement is seen (see arrows), which is suspicious for an infectious event and caused by cryptococcosis in this case.
Source: “Figure 1, in: Disseminated Cryptococcal Disease in a Patient With Monoclonal Gammopathy of Undetermined Significance and Polycythemia Vera: A Case Report and Review of the Literature” by Guhjjar M, Ghazanfar H, Ashraf S, Gaddam S, Metela A, Cureus, licensed under CC BY 4.0.
Pathophysiology
Pathways of infection
-
Most pathogens that cause meningitis colonize the nasopharynx or the upper airways before entering the CNS via:
- Hematogenous dissemination [23]
- Contiguous spread of infections in nose, eyes, and ears
- Retrograde transport along or within peripheral or cranial nerves
- Direct infection (e.g., due to trauma or head surgery) [24]
Incubation periods
- Bacterial meningitis: usually 3–7 days [25]
- Viral meningitis: usually 2–14 days, depending on the type of virus
References:[25][26]
Clinical features
Clinical features of bacterial and viral meningitis are similar, although viral meningitis is less acute and usually self-limiting within 5–14 days. [27]
Symptoms of meningitis [4][6]
-
Classic triad of meningitis ; [6][28][29]
- Fever
-
Meningismus
- Headache
- Neck stiffness
- Photophobia
- Altered mental state
- Nausea, vomiting
- Malaise
- Seizures
- Neonates and young children often present with nonspecific symptoms (see also “Meningitis in children” and “Neonatal bacterial meningitis”)
Pathogen-specific symptoms
- Patients with N. meningitidis: signs of meningococcemia
- Myalgia: more common in children
- Possibly petechial or purpuric rash: more common in children
- Possibly Waterhouse-Friderichsen syndrome: more common in children [30]
-
Patients with viral meningitis
-
Prodrome with flu-like symptoms
- Low-grade fever
- Malaise and fatigue
- Myalgia
- Upper respiratory symptoms (e.g., sore throat)
- Pharyngitis, herpangina, and/or rash
-
Prodrome with flu-like symptoms
Less than half of adult patients have all three features of the classic triad of meningitis; the percentage is even lower in neonates and young infants, who typically present with nonspecific symptoms[4]
Subarachnoid hemorrhage manifests with the classic triad of meningitis, but it typically has a more sudden onset and affected individuals often lose consciousness.
Physical examination [31][32]
-
Signs of meningeal irritation
- Neck stiffness
- Kernig sign
- Brudzinski sign
-
Systemic signs of inflammation
- Fever
- Hypotension
- Tachycardia
- Signs of increased intracranial pressure: (< 5% of cases), e.g., cranial nerve palsies, papilledema [33]
-
Signs of underlying infections
- Bulging and redness of tympanic membrane: acute otitis media
-
Skin manifestations [34]
- Cutaneous petechiae in meningococcal meningitis: suggestive of meningococcemia
- Maculopapular rash in some viral meningitis types (e.g.,; West Nile virus, enterovirus)
- Nonblanching rash: raises suspicion for meningococcal meningitis or Rocky Mountain spotted fever (see “Subtypes and variants”)
Features suggestive of meningoencephalitis [35][36]
In addition to the features of meningitis, meningoencephalitis is characterized by signs of inflammation of the brain parenchyma (encephalitis).
- Focal neurological signs (e.g., paresis, extrapyramidal symptoms, aphasia)
- Seizures (focal-onset or generalized)
- Behavioral changes, psychosis
- Altered consciousness


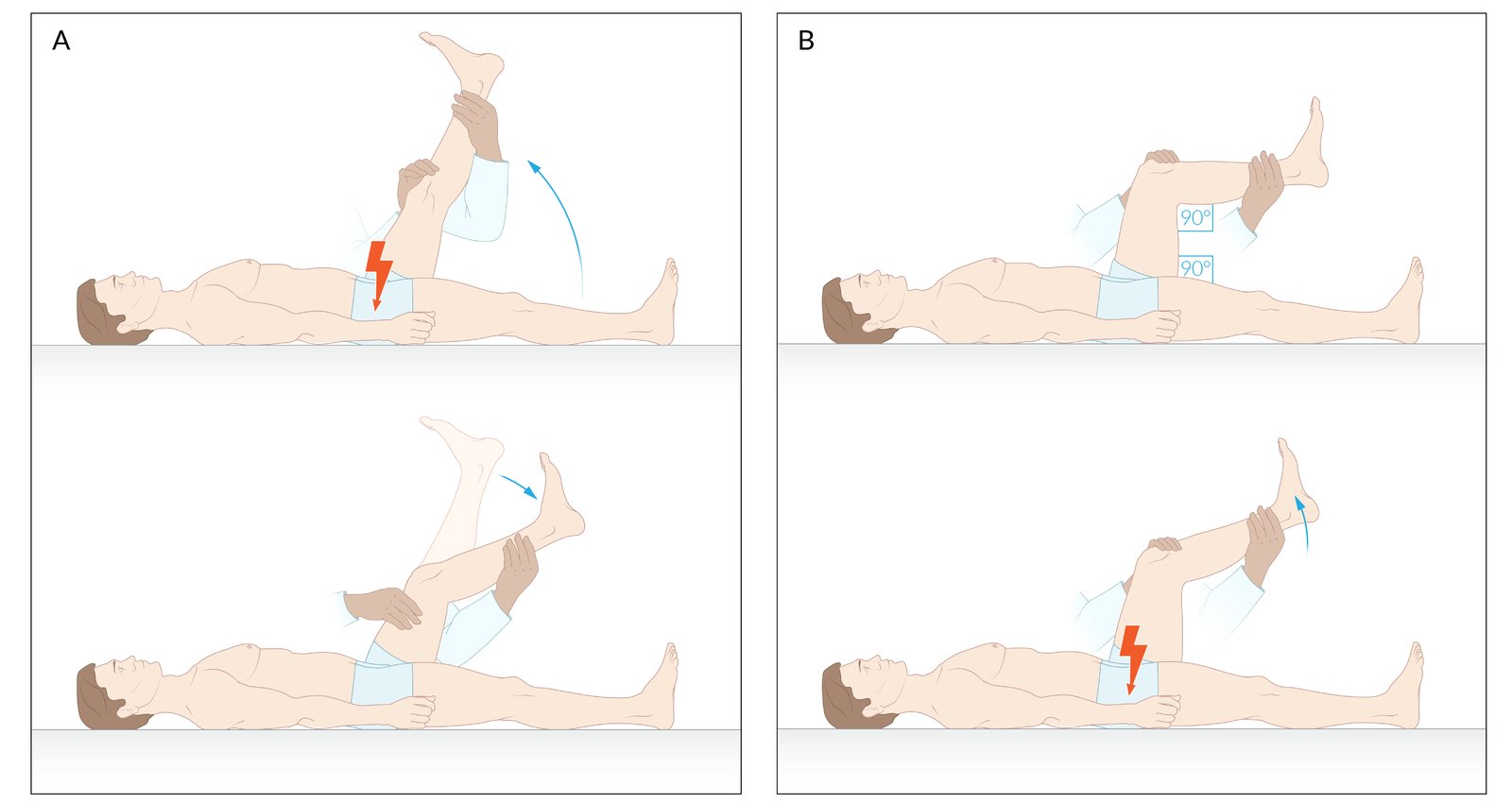
The Kernig sign can be assessed using two methods. In the first method (A), the extended leg is passively elevated at the hip joint. If there is pain, there is reflex flexion of the knee. Alternatively (B), the Kernig sign can be assessed by flexing the hip and knee at a 90° angle. Subsequent extension of the leg causes stretching of the nerve roots or meninges, which can result in pain and muscle guarding against extension.
© AMBOSS
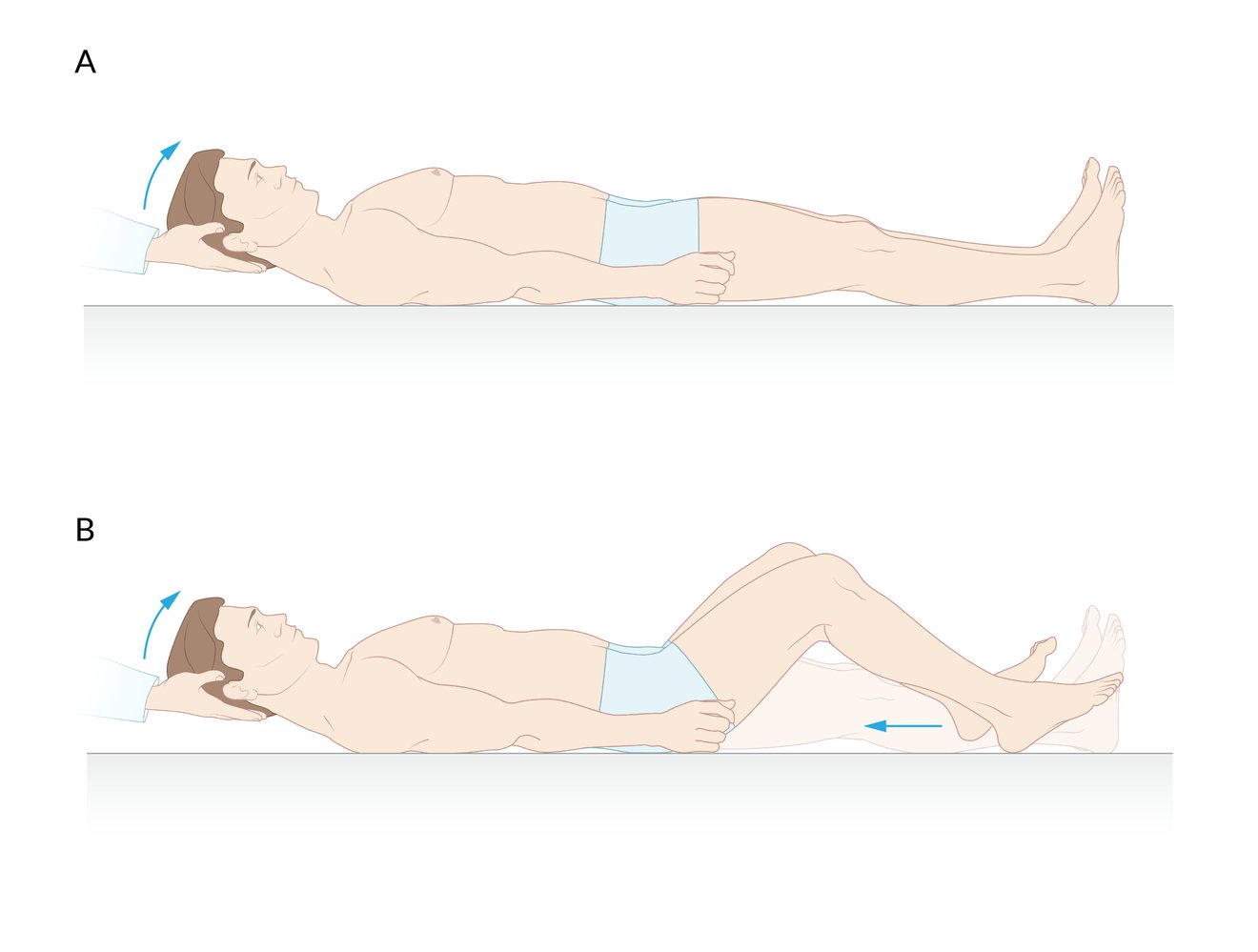
Passive flexion of the neck (A) leads to spontaneous flexion of the hips (B) as a reflex, which provides relief of painful strain on the meninges.
© AMBOSS
Initial management
General approach
- Bacterial meningitis is a medical emergency and requires immediate treatment.
- Diagnostic and treatment steps should be initiated simultaneously and empiric treatment should not be delayed for diagnostic steps.
- If the patient is stable and has no LP contraindications: Perform LP as soon as possible before starting empiric antibiotics.
- If the patient is unstable, requires neuroimaging (see criteria for imaging prior to LP in suspected meningitis), or has relative contraindications to LP (e.g., coagulopathy): Defer LP and start empiric antibiotic treatment (see empiric antibiotic therapy for bacterial meningitis). [5]
Do not delay empiric antibiotic therapy in patients suspected of having bacterial meningitis.
Challenges
-
Diagnosis
- There is a significant overlap in presentation between bacterial and other etiologies.
- LP and CSF analysis can be time-consuming and risky.
- Patients may present with relative contraindications to LP (e.g., signs of elevated ICP).
-
Treatment
- Bacterial meningitis can be rapidly progressive and life-threatening.
- Patients may present as critically ill and with complications (e.g., sepsis, multiorgan failure) requiring early aggressive supportive care.
- Empiric antibiotic treatment must be initiated as soon as possible (i.e., often prior to diagnosis).
BMP: basic metabolic panel
CBC: complete blood count
CRP: C-reactive protein
CSF: cerebrospinal fluid
DDx: differential diagnoses
HSV: herpes simplex virus
ICP: intracranial pressure
IV: intravenous
LP: lumbar puncture
PCR: polymerase chain reaction
VZV: varicella zoster virus
© AMBOSS
Diagnosis
Approach [5][28][29][37][38]
- Obtain samples immediately for blood cultures, routine laboratory tests, and screening for organ dysfunction.
- Confirm the diagnosis with LP and CSF analysis (if no LP contraindications are present).
- See also “Meningitis in children” and “Neonatal bacterial meningitis.”
Start empiric antibiotics immediately after obtaining blood cultures and CSF samples. If LP is delayed for any reason (e.g., the need for a CT or hemodynamic stabilization), obtain blood cultures and administer antibiotics until it can be performed.
Laboratory studies [5][28][29][37]
-
Routine tests
- Blood cultures (two sets): obtain before starting antibiotic therapy
-
CBC
- Normal/↑ WBC count
- In severe infections, ↓ WBC count and thrombocytopenia
-
BMP: Blood glucose is needed to analyze CSF glucose.
- Common finding: mild electrolyte disturbances (e.g., hyponatremia from SIADH)
- In critically ill patients: possible signs of acute kidney injury
- CRP: elevated [37]
-
Additional tests
- Assess for organ damage and complications.
- Coagulation panel: especially if there is suspicion for disseminated intravascular coagulation (e.g., petechiae, purpura)
- Blood gas: metabolic acidosis may be present in critically ill patients
- Consider testing for atypical infections
- Assess for organ damage and complications.
Neuroimaging in meningitis [24][37][38]
Imaging is not necessary to establish the diagnosis of meningitis in most patients and should only be considered in patients with significant risk factors for complications.
-
Indications
- To assess the risk of brain herniation precipitated by LP [37]
- Identify abscesses or other localized lesions (e.g., in postsurgical patients in whom infection is suspected) [24]
- Suspected healthcare-associated ventriculitis/meningitis [24]
- Patients with devices (e.g., CSF shunts) [24]
-
Recommended criteria for imaging prior to LP in suspected meningitis [37][38][39]
- Focal neurological deficits
- Altered mental status [38]
- Immunocompromised status (e.g., HIV, post-transplant, taking immunosuppressants)
- Papilledema
- History of CNS disease (e.g., mass, stroke, abscess)
- Seizures (new-onset) [37]
-
Modalities
- CT head (with or without IV contrast): before LP if increased ICP is suspected [40]
- MRI brain with IV contrast and diffusion: especially useful in patients with devices or after surgery [24]
-
Supportive findings
- Usually normal or showing mild meningeal enhancement
- May identify predisposing factors for the infection (e.g., fractures, mastoiditis) or complications (e.g., abscess)
- See “Subtypes and variants” for characteristic findings of specific pathogens.
To remember the indications for imaging before LP, think of LP FAILS: Focal neurological deficits, Altered mental status, Immunocompromised or ↑ ICP, Lesions (space-occupying lesions in the brain), Seizures.
Cerebrospinal fluid analysis
Lumbar puncture is indicated in all patients with suspected meningitis (see “Lumbar puncture” for details on indications, LP contraindications, procedural steps, and complications).
: materials, patient positioning, and puncture site")
: procedure")

Interpretation of CSF analysis
- Confirmatory findings: pathogen identification on CSF OR positive blood cultures in a patient with highly suggestive CSF findings
- Highly suggestive findings: pleocytosis (granulocytic or lymphocytic), low glucose, high protein
- Nonspecific findings: high opening pressure
Routine testing [37][38][39]
| Cerebrospinal fluid analysis in meningitis [37][39] | |||
|---|---|---|---|
| Normal | Bacterial meningitis | Viral meningitis | |
| Appearance |
|
|
|
| Cell count and differential |
|
|
|
| Opening pressure [41] |
|
|
|
| Lactate [38] |
|
|
|
| Protein |
|
|
|
| Glucose |
|
|
|
| Gram stain and culture [38][39] |
|
|
|
Atypical pathogen testing
Atypical pathogen testing is not necessary for all patients and should be performed as directed by clinical suspicion.
| Cerebrospinal fluid analysis in meningitis due to atypical pathogens [39] | |||
|---|---|---|---|
| Tuberculous meningitis [42] | Lyme meningitis [43] | Cryptococcal meningitis [44] | |
| Appearance |
|
|
|
| Cell count and differential |
|
|
|
| Opening pressure |
|
|
|
| Lactate [38] |
|
|
|
| Protein |
|
|
|
| Glucose |
|
|
|
Additional microbiological testing
-
Special microbiological stains
- Acid-fast staining: if there is suspicion for tuberculous meningitis
- India ink preparation: if there is suspicion for cryptococcus
- Wright or Giemsa stain: if there is suspicion for toxoplasmosis
-
Special cultures [39]
- Viral culture
- Not typically recommended
- May confirm enterovirus, herpes simplex virus infection
- M. tuberculosis cultures: Results can take up to 6 weeks. [39]
- Fungal cultures: for the identification of Candida spp., Cryptococcus spp. [39]
- For patients with CSF shunts or drains: Extend CSF cultures for at least 10 days.
- Viral culture
-
PCR for viral meningitis and specific bacterial subtypes [37][38]
- Indications
- Confirmation of viral meningitis/encephalitis (e.g., HSV)
- Detection of intracellular bacteria (e.g., TB, rickettsial infections)
- Disadvantages
- No antibiotic sensitivity data for bacterial infections
- Not readily available for unusual pathogens (especially bacteria)
- Indications
-
Latex agglutination test [37]
- Bacterial antigen detection
- Not routinely used because of variable accuracy [37]
- Consider in patients in whom there is strong suspicion for bacterial meningitis despite negative Gram stain or culture after 48 hours
- Fungal latex agglutinations: especially relevant for cryptococcal antigen testing (see cryptococcal meningitis)
- Bacterial antigen detection
BMP: basic metabolic panel
CBC: complete blood count
CRP: C-reactive protein
CSF: cerebrospinal fluid
DDx: differential diagnoses
HSV: herpes simplex virus
ICP: intracranial pressure
IV: intravenous
LP: lumbar puncture
PCR: polymerase chain reaction
VZV: varicella zoster virus
© AMBOSS
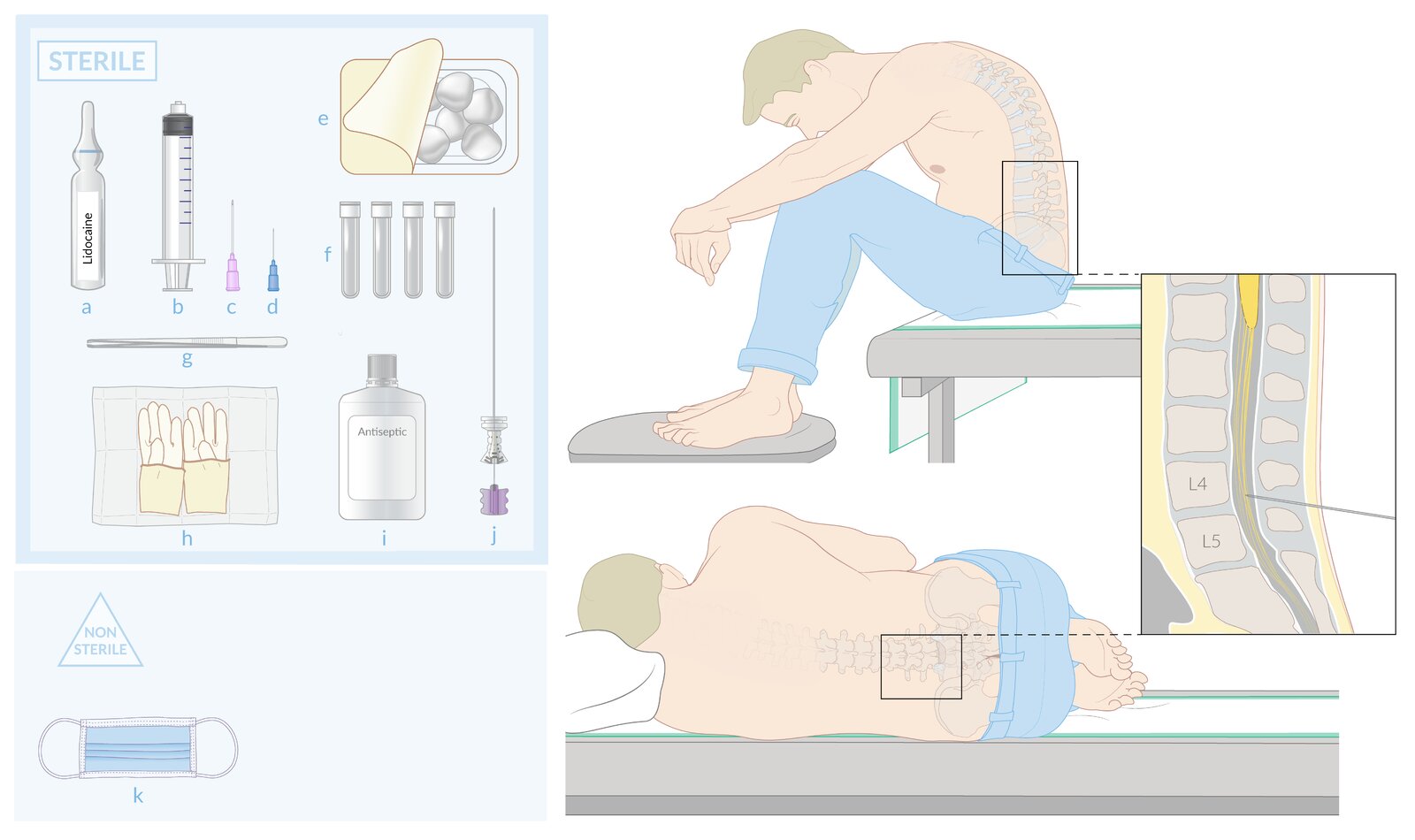
Sterile materials (upper left):
(a) Local anesthetic
(b) Syringe for application of local anesthetic
(c) and (d) Syringe and needles for superficial and deep application of local anesthetic
(e) Gauze
(f) CSF collection tubes (4)
(g) Forceps
(h) Sterile gloves
(i) Antiseptic
(j) Spinal needle
Nonsterile materials (lower left):
(k) Surgical mask
Patient positioning:
The patient is typically seated and flexed forward (upper right) or placed in a flexed lateral recumbent position with the head supported (lower right). Flexion increases the interspinous space and facilitates access to the subarachnoid space.
Puncture site (far right):
For lumbar puncture (including spinal anesthesia), the spinal needle is typically inserted in the L3–4 or L4–5 interspace and directed toward the umbilicus.
© AMBOSS

1. The skin is prepped widely with antiseptic in a spiral motion outwards from the intended needle insertion site. A sterile fenestrated drape is typically applied over the antiseptic prep (not shown).
2. Local anesthesia is injected subcutaneously with a small gauge needle, creating a skin wheal over the intended needle insertion site. Local anesthesia is then infiltrated into the deeper tissue through this skin wheal, anesthetizing the entire intended needle tract (2a).
3. The spinal needle is inserted with the tip directed towards the umbilicus and advanced until a loss of resistance is felt. Failure to direct the needle toward the umbilicus may result in the needle encountering bone before reaching the subarachnoid space (3a).
4. The stylet is withdrawn and the needle hub is observed for CSF flow. If flow is present, CSF is collected in four collection vials.
5. The stylet is replaced after the collection of CSF is complete.
6. The spinal needle and stylet are removed and a dressing is applied to the puncture site (not shown).
© AMBOSS

Original title: “How to do a lumbar puncture”. Created by: Medmastery.
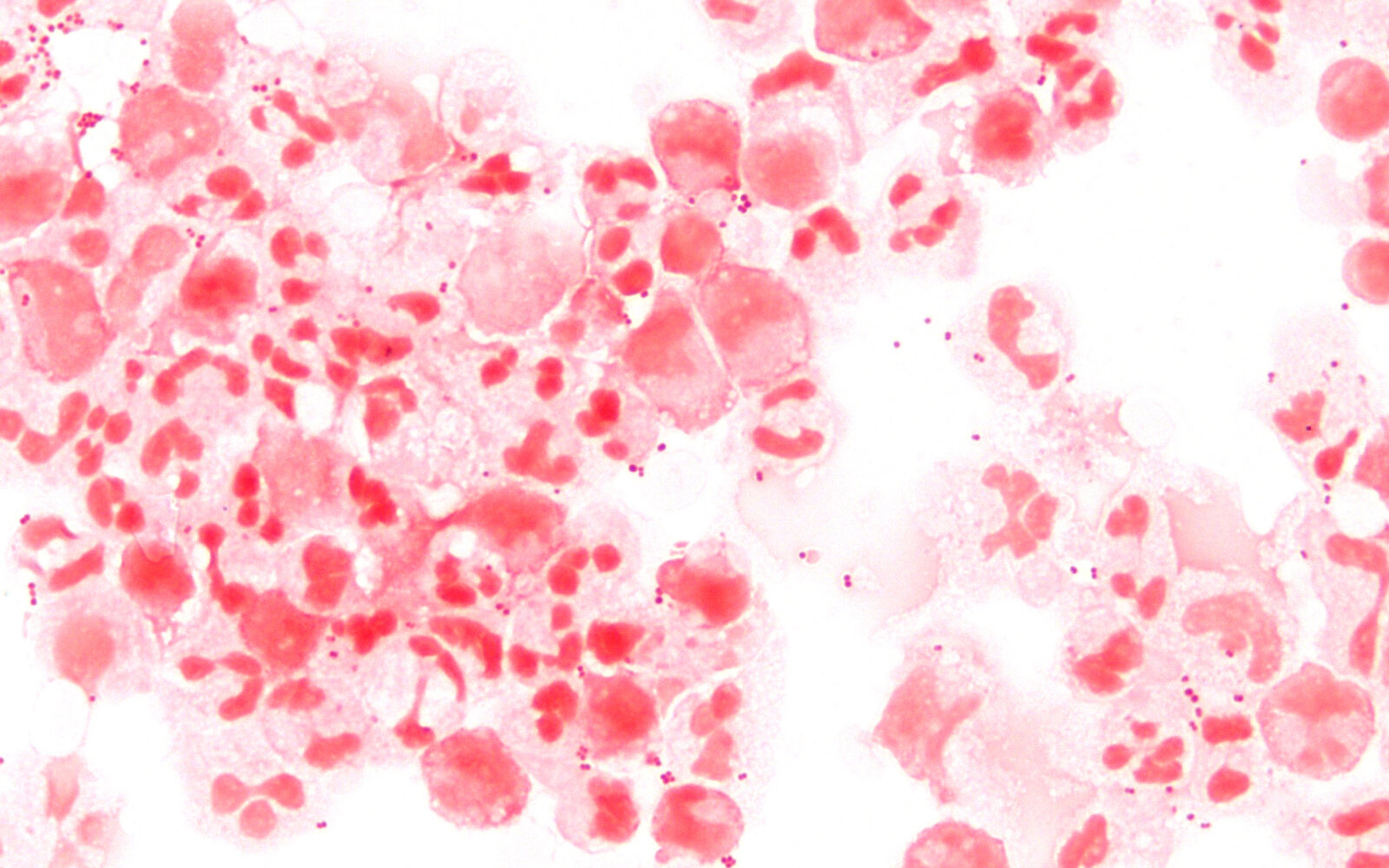
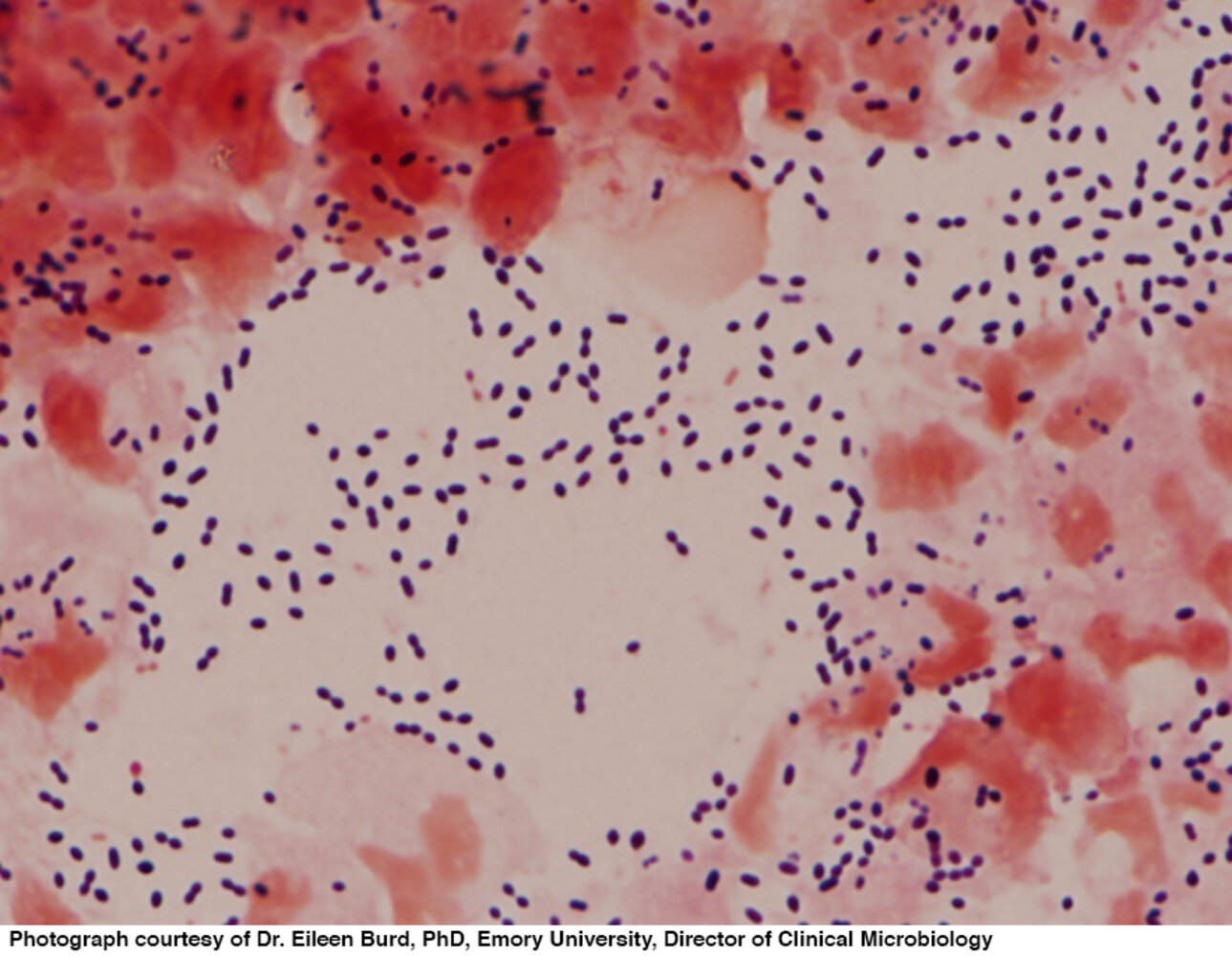
Photomicrograph of a cerebrospinal fluid (CSF) sample (Gram stain; 1000× magnification)
Gram-negative diplococci (examples indicated by arrowheads), the classic morphology of Neisseria meningitidis, are visible.
Source: “Neisseria meningitidis CSF Gram 1000” by Microman12345, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
Treatment
Approach
- Apply appropriate isolation precautions.
- Stabilize the patient as needed.
-
Administer empiric antibiotics as soon as possible, preferably within 1 hour (see empiric antibiotic therapy for bacterial meningitis).
- If LP can be performed rapidly, administer antibiotics and adjuvant therapy (e.g., dexamethasone) after obtaining CSF.
- If LP is delayed (e.g., because neuroimaging is required), administer antibiotics and adjuvant therapy (e.g., dexamethasone) immediately.
- Add other antimicrobial therapy (e.g., antivirals, antifungals) as needed (see “Subtypes and variants” for details).
- Consult the infectious disease team.
- Tailor antimicrobial therapy once the pathogen is identified.
- Provide postexposure prophylaxis for close contacts if indicated (see postexposure chemoprophylaxis for bacterial meningitis).
- See also “Meningitis in children” and “Neonatal meningitis.”
Do not delay administering antibiotics if neuroimaging is indicated prior to LP. Obtain blood cultures, start antibiotics (and steroids, if needed) immediately, then proceed with the CT and LP.
Immediate stabilization for meningitis
- Airway management: Secure the airway (e.g., intubate) if GCS < 8, the patient has intractable seizures, or there are signs of cerebral herniation (see intubation of patients with high ICP).
- Provide hemodynamic support with fluids and/or vasopressors (see “Fluid resuscitation” and “Sepsis”).
- Identify and reverse any coagulopathy (see “Anticoagulant reversal”).
- Identify and treat elevated ICP (see “ICP management”).
Antimicrobial therapy for meningitis
Empiric antibiotic therapy [37]
- The choice of initial empiric therapy depends primarily on the prevalence of organisms in certain age groups and individual patient risk factors for resistant organisms.
- Factors to consider:
- Epidemiological factors (e.g., local flora, resistance patterns)
- Bioavailability: Antimicrobial agents should cross the blood-brain barrier and higher doses may be needed.
- Individual patient risk factors and comorbidities
| Empiric antibiotic therapy for bacterial meningitis [37] | |
|---|---|
| Patient characteristics | Recommended regimen |
| Age <18 years |
|
| Age 18–50 years |
|
| Age > 50 years |
|
| Immunocompromised [45] |
|
| Healthcare-associated infections [24] |
|
| Suspected rickettsial (e.g., RMSF) or ehrlichial infection [46] |
|
| Basilar skull fracture |
|
| Penetrating head trauma |
|
Ampicillin is added if patients are at risk of Listeria spp. infection (e.g., newborns, pregnant women, adults > 50 years of age, or immunocompromised patients) because cephalosporins are ineffective against Listeria spp.
Empiric therapy for viral meningitis [46][47]
Most cases of viral meningitis (e.g., caused by enteroviruses) can be treated supportively. Specific antiviral therapy is only warranted if viral encephalitis is also suspected (see HSV encephalitis for further details).
-
Indications
-
Concern for HSV encephalitis, for example:
- Suggestive clinical features (e.g., focal neurological deficits, altered mental status, seizures, behavioral changes, coma)
- Imaging findings (e.g., temporal lobe enhancement)
- CSF: ↑ RBCs despite a nontraumatic LP (suggestive of hemorrhagic encephalitis)
- Concern for other herpesviruses, e.g., VZV, EBV
-
Concern for HSV encephalitis, for example:
-
Recommended empiric antiviral agent: acyclovir
- Continue treatment if either HSV or VZV is detected, otherwise discontinue.
Treatment with acyclovir should be started in all patients who present with typical clinical signs of viral meningoencephalitis and only discontinued after PCR and antibody tests are negative for HSV and VZV, even if CSF is initially normal.
Pathogen-specific therapy
The decision to narrow therapy should be guided by final culture and sensitivity results, as well as local resistance patterns. We list a few examples of antimicrobial agents that may be used against specific pathogens. For dosages in neonates, see “Empiric antibiotics for neonatal sepsis.”
| Pathogen-specific therapy in meningitis [9][37] | |
|---|---|
| Pathogen | Examples of antimicrobial agents |
|
S. pneumoniae(penicillin-resistant strains) |
|
| MRSA | |
| S. epidermidis | |
| H. influenzae |
|
| N. meningitidis | |
| E. coli | |
| L. monocytogenes |
|
| S. agalactiae | |
| Enterococcus spp. |
|
| P. aeruginosa |
|
| R. rickettsii |
|
| Herpes viruses |
|
| Less frequent pathogens, e.g., M. tuberculosis, C. neoformans, B. burgdorferi |
|
Corticosteroids [38][52]
- Indication: : suspected or proven meningitis due to S. pneumoniae or H. influenzae
- Mechanism: reduces the local and systemic inflammation seen in bacterial meningitis and improves outcomes
-
Recommended agent: dexamethasone for 2–4 days [38][52]
- Should be administered before or concomitant to antibiotics for optimal results [38]
- Discontinue if a pathogen other than S. pneumoniae or H. influenzae is identified.
- Disadvantages: side effects, e.g., hyperglycemia, GI bleeding [52]
- For pediatric use, see “Meningitis in children.”
Do not delay antibiotics to administer adjuvant therapy. If dexamethasone is not readily available, start antibiotics immediately.
Supportive therapy
- Electrolyte repletion
- Analgesics as needed (see pain management)
- Antipyretics as needed
- IV fluids as needed
- IV antiemetics as needed
- Ondansetron
- Metoclopramide
- Prochlorperazine
Monitoring and disposition
- Most patients with meningitis require admission; select patients may be considered for outpatient therapy with close follow-up. [37]
- Serial neuro examinations
- Consultations
- Infectious disease
- Consider also ICU , neurology, neurosurgery as needed.
BMP: basic metabolic panel
CBC: complete blood count
CRP: C-reactive protein
CSF: cerebrospinal fluid
DDx: differential diagnoses
HSV: herpes simplex virus
ICP: intracranial pressure
IV: intravenous
LP: lumbar puncture
PCR: polymerase chain reaction
VZV: varicella zoster virus
© AMBOSS
Subtypes and variants
Tuberculous meningitis
See “Tuberculous meningoencephalitis” in “Extrapulmonary tuberculosis.”
Cryptococcal meningitis
- Pathogen: Cryptococcus neoformans (a type of encapsulated yeast)
-
Risk factors
- AIDS
- Exposure to pigeon droppings
- Clinical course: : subacute onset with (low) fever, fatigue, and headaches
-
Clinical features
- See section on “Clinical features” above
- Meningeal symptoms are often absent
-
Diagnostics [53]
-
Cryptococcal antigen testing of CSF and serum
- Highly specific and sensitive [53]
- Typically performed via latex agglutination or enzyme immunoassay
-
Lumbar puncture
- High opening pressure
- CSF culture (Sabouraud agar)
- CSF gram staining: India Ink (clear halo), mucicarmine (red inner capsule)
- MRI: gelatinous pseudocysts (soap bubble appearance)
-
Cryptococcal antigen testing of CSF and serum
-
Treatment [54]
- Induction: Intravenous amphotericin B PLUS flucytosine for at least 2 weeks
- Consolidation: fluconazole for at least 8 weeks
- Maintenance: fluconazole for at least 1 year
- Manage raised ICP with therapeutic lumbar puncture.
- Important consideration: Delay initiation of cART for 4–6 weeks after starting antifungal therapy to reduce the risk of immune reconstitution syndrome.
Tick-borne diseases
-
North America
- See “Lyme meningitis.”
- See “Rocky Mountain spotted fever.”
- See “Ehrlichiosis.”
- Eurasia: See “Tick-borne meningoencephalitis.”
Primary amebic meningoencephalitis [55]
- Pathogen: Naegleria fowleri (colloquially referred to as “brain-eating amoeba”), found in warm freshwater (e.g., ponds, hot springs)
- Route of infection: via contaminated water entering the nose (e.g., while swimming) → invades the CNS directly via the olfactory nerve (perforates the cribriform plate)
- Clinical features: causes fulminant meningoencephalitis with rapid onset
-
Diagnosis
-
CSF analysis
- Findings similar to those of bacterial meningitis (e.g., neutrophilic pleocytosis, hypoglycorrhachia, increased CSF protein)
- CSF erythrocytosis (due to hemorrhagic necrosis)
- Microscopy shows trophozoites
-
CSF analysis
- Treatment: amphotericin B, miltefosine
- Prognosis: nearly always fatal [56]


References:[57][58][59][60][61][62]
Aseptic meningitis
-
Etiology [63]
- Infectious causes are most commonly viruses (e.g., enteroviruses, HSV, VZV) and less commonly bacteria, fungi, or parasites.
- Noninfectious causes include medications (e.g., NSAIDs), autoimmune diseases (e.g., sarcoidosis), and malignancies (e.g., leptomeningeal metastases). [64]
- Clinical course: less acute onset than bacterial meningitis, without altered mental status [65]
-
Diagnostics: CSF fluid analysis (if there are no contraindications for lumbar puncture)
- Nonpurulent appearance, variable cell count with elevated lymphocytes
- Negative cultures
- See “Diagnostics for meningitis.”
-
Treatment
- Most cases can be treated with supportive care.
- In drug-induced meningitis, the causative medication should be stopped.
- Herpes virus infections (e.g., HSV, VZV) require treatment with IV acyclovir.
- Prognosis: Although full recovery is common, there is a risk of long-term complications, depending on age, overall condition, immune status, and the pathogens involved. [65][66]
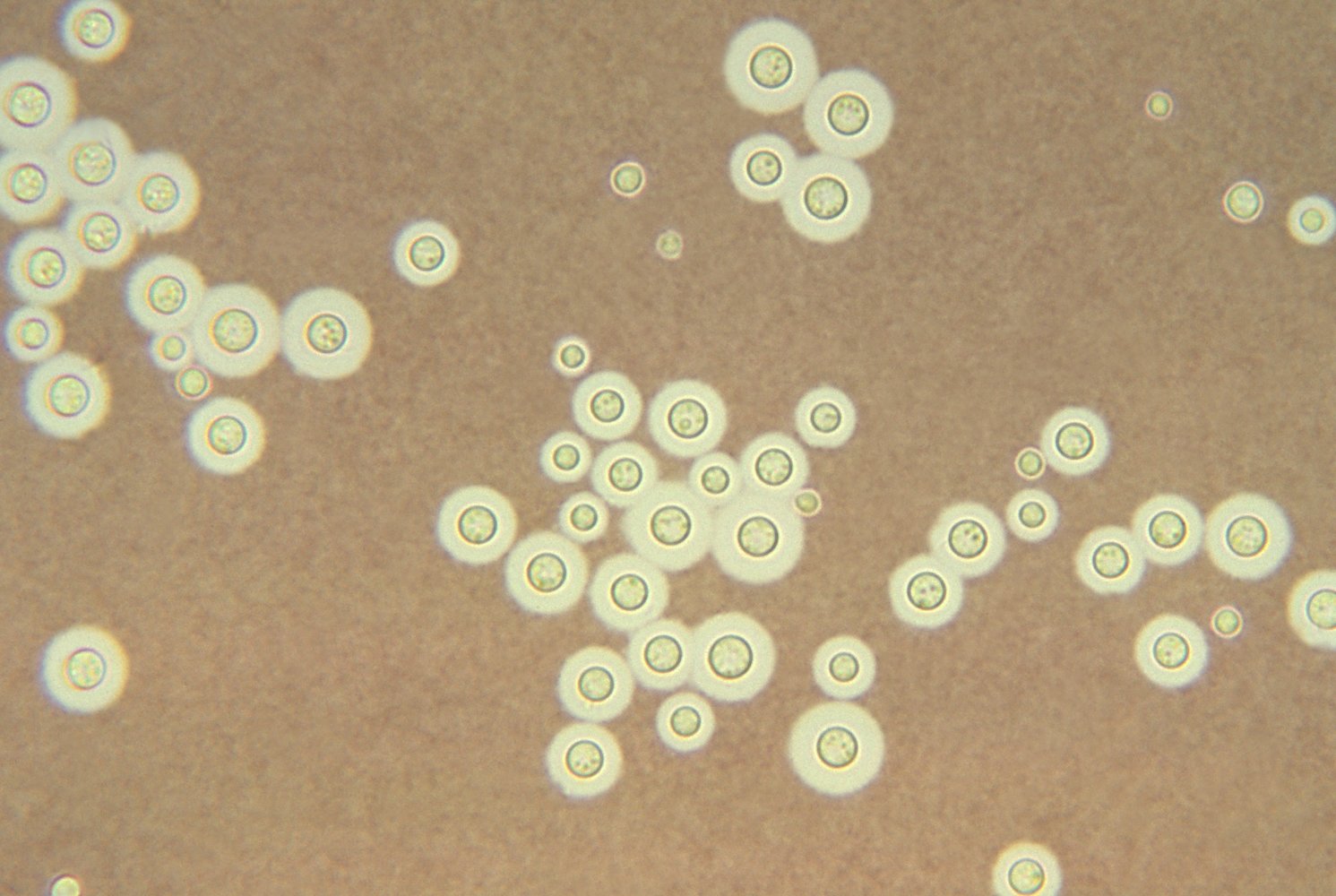
Photomicrograph of a fungal culture (India ink stain)
Numerous spherical yeast cells of different sizes can be seen. The polysaccharide capsules appear as yellowish halos around the cell walls (dark circles).
These features are characteristic of Cryptococcus neoformans under light microscopy.
Source: "ID#: 3771", CDC/ Dr. Leanor Haley, Centers for Disease Control and Prevention licensed under Public Domain Further notes: Public Health Image Library (PHIL); ID: 3771
MRI head (with contrast; T1-weighted; axial plane) of a 58-year-old patient with monoclonal gammopathy and polycythemia vera who presented with confusion, fatigue, and auditory hallucinations for one week.
Mild meningeal enhancement is seen (see arrows), which is suspicious for an infectious event and caused by cryptococcosis in this case.
Source: “Figure 1, in: Disseminated Cryptococcal Disease in a Patient With Monoclonal Gammopathy of Undetermined Significance and Polycythemia Vera: A Case Report and Review of the Literature” by Guhjjar M, Ghazanfar H, Ashraf S, Gaddam S, Metela A, Cureus, licensed under CC BY 4.0.
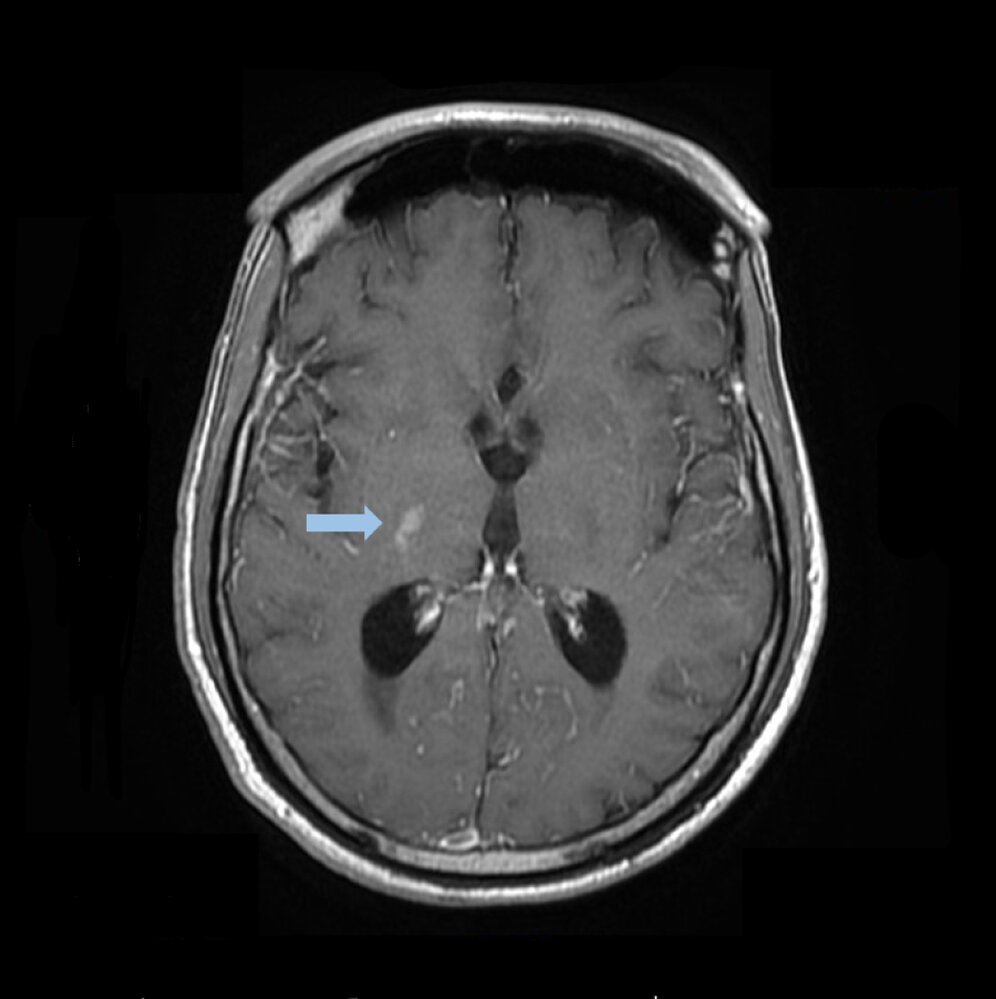
MRI head (with contrast; axial plane)
A small contrast-enhancing lesion (indicated by arrow) resulting from cryptococcosis is visible in the right basal ganglia.
In unspecific findings like this one, an inflammatory etiology should be considered as a differential on the basis of contrast enhancement and localization.
Source: “Figure 3, in: Disseminated Cryptococcal Disease in a Patient With Monoclonal Gammopathy of Undetermined Significance and Polycythemia Vera: A Case Report and Review of the Literature” by Guhjjar M, Ghazanfar H, Ashraf S, Gaddam S, Metela A, Cureus, licensed under CC BY 4.0.
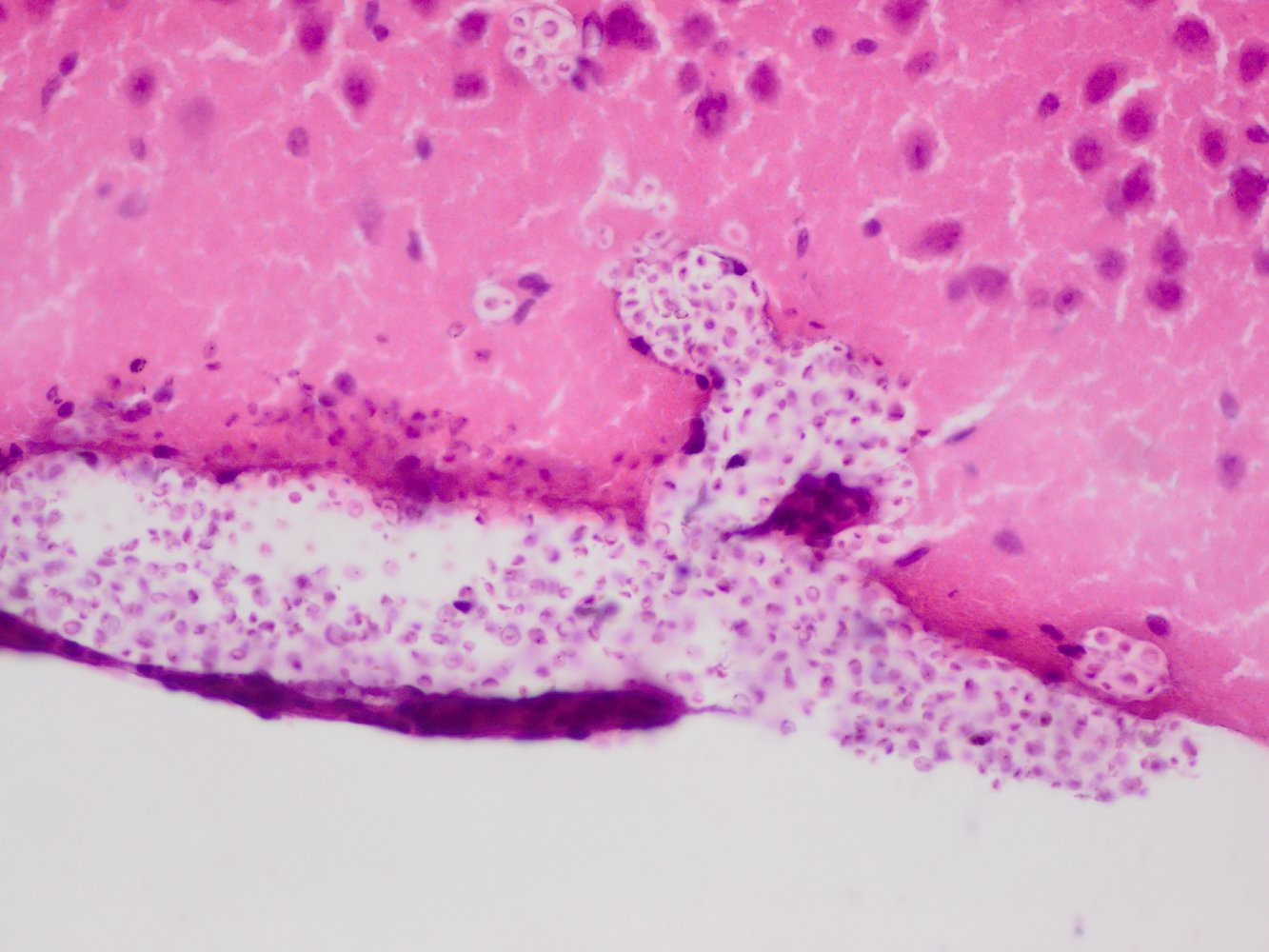
Photomicrograph of a murine brain autopsy specimen (H&E stain; high magnification)
Cryptococcus neoformans (green overlay) can be seen invading the meninges (blue overlay) and the brain parenchyma (light pink tissue). Numerous neutrophils can be seen in the meninges, indicating inflammation.
These findings are characteristic of cryptococcal meningoencephalitis.
Created by: Dr. med. Michael Meisen.
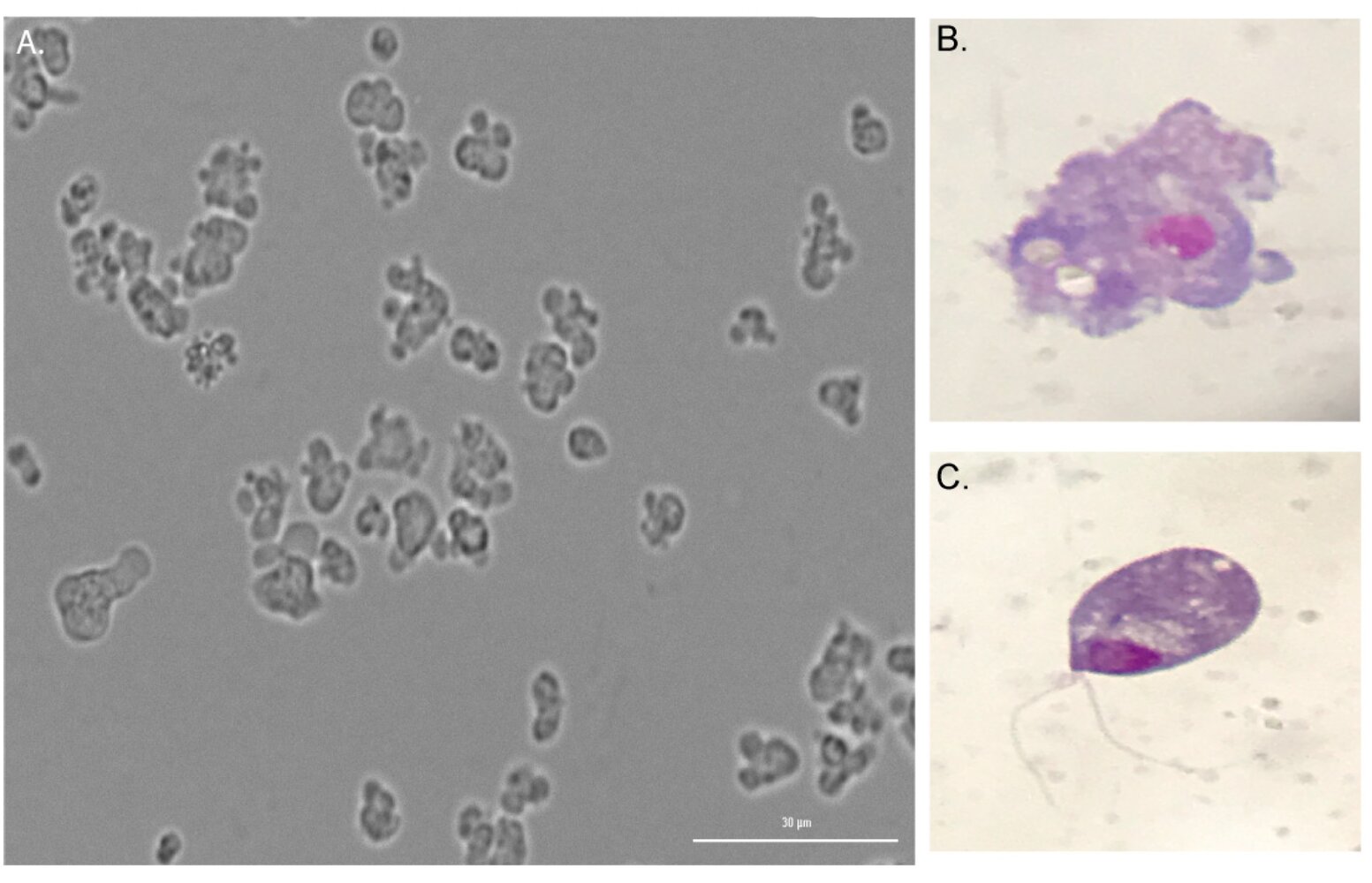
Photomicrographs of Naegleria fowleri specimens obtained from cerebrospinal fluid (CSF) samples
A: Multiple trophozoites in axenic (pure) culture
B: Trophozoite stage (Giemsa stain)
C: Flagellate stage (Giemsa stain)
© AMBOSS. This image was adapted from the image “Figure 2. in: Primary Amebic Meningoencephalitis Related to Groundwater in Costa Rica: Diagnostic Confirmation of Three Cases and Environmental Investigation” by Lissette Retana Moreira, Leidy Zamora Rojas, Muriel Grijalba Murillo, Silvia Elena Molina Castro. Elizabeth Abrahams Sandí, MDPI Open Access Journals, Pathogens, licensed under CC BY 4.0.
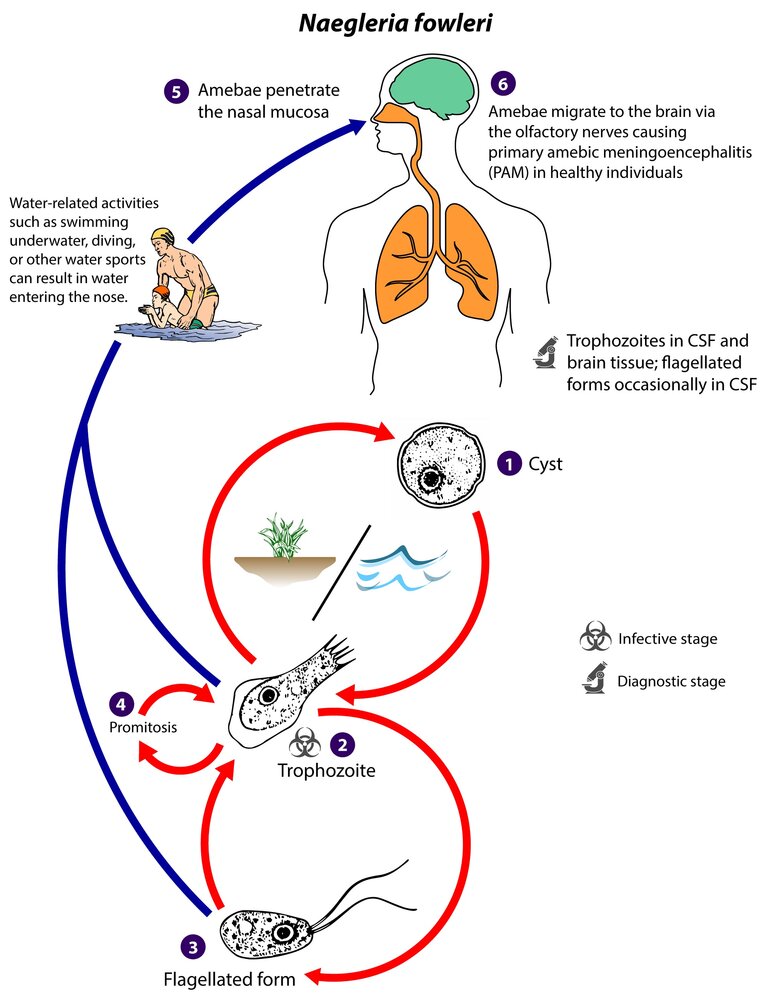
1. Amebae encyst to withstand adverse environmental conditions (e.g., desiccation, cold, diminished food supply).
2. Infective stage: Amebae excyst and develop into trophozoites once environmental conditions improve (e.g., warm or hot, poorly chlorinated fresh water). Longer exposure to adverse environmental conditions trigger encystation.
3. Trophozoites temporarily change into a flagellated form when exposed to adverse environmental conditions. When these conditions persist, the amoeba reverts to the trophozoite and encysted form.
4. The amebae multiplies through promitosis during the trophozoite stage.
5. The trophozoites or flagellates enter the nose of a human (definitive) host through contaminated water (e.g., while diving, dipping underwater in a hot tub, or during sinus irrigation) and penetrate the nasal mucosa. Flagellates revert to trophozoite form shortly after entering the nasal cavity.
6. Diagnostic stage: Amebae migrate to the brain via the olfactory nerves, causing primary amebic meningoencephalitis. Trophozoites can be found in brain tissue and CSF, whereas flagellates are occasionally found only in the CSF. Naegleria fowleri does not encyst within a definitive host.
This image is an adaptation. Source of original image: CDC/ DPDx. Original title: “Naegleria fowleri”. Created by: CDC/ DPDx. Licensed under Public Domain. Modifications to original image: CDC/DPDx logo removed by request.
Complications
Neurologic
- Most common: sensorineural hearing loss (transient or permanent)
- Focal neurological deficits [67]
- Seizures
- Cognitive impairment
- Spasticity or paresis
- Cerebral edema and elevated ICP
- Communicating hydrocephalus
- Cerebrovascular disease
- Rare: brain abscess; , subdural empyema, arteritis (risk of cerebral infarction and cerebral venous sinus thrombosis), ventriculitis, cerebritis
Waterhouse-Friderichsen syndrome
- Epidemiology: : predominantly affects small children and asplenic individuals
-
Description: acute primary insufficiency of the adrenal gland most commonly caused by adrenal hemorrhage
- Dangerous complication of a number of diseases but most commonly associated with meningococcal meningitis
- Rarer causes include DIC, endotoxic shock, and septicemia due to other pathogens (e.g., S. pneumoniae)
- Pathophysiology: coagulopathy triggered by endotoxins; , which often leads to hemorrhagic necrosis of the adrenal glands
-
Clinical features
- Fever
- Myalgia
- Nonblanching, petechial rash (mostly on trunk and legs); in severe cases, even purpura fulminans with extensive necrosis of the skin
- Severe malaise
- Hypotension or even shock
- Findings of disseminated intravascular coagulation
- Findings of acute adrenal gland failure
- Respiratory failure
-
Treatment
- Treatment of the underlying cause (see empiric antibiotic therapy for bacterial meningitis and pathogen-specific therapy in meningitis)
- Parenteral fluid therapy and management of disorders of sodium balance
- Coagulopathy treatment
- Prognosis: fatal without treatment and often fatal even with treatment, particularly if associated with meningococcal infection (> 40% mortality rate) [68]



References:[47][69]
We list the most important complications. The selection is not exhaustive.

Bluish-red, round or oval maculae (approx. 0.2 mm–1 cm in diameter) are distributed over the right lower leg. There is also an irregularly shaped macula of the same color lateral to the patella (approx. 4 × 2 cm in diameter).
This appearance is characteristic of purpura.
Source: © IMPP

Purple nonblanching macules of various sizes, consistent with purpura (larger macules) and petechiae (smaller macules), are visible.
These findings are consistent with purpura in Waterhouse-Friderichsen syndrome.
Source: © IMPP

There are multiple small, nonblanching purple macules on the upper thigh, medial aspect of the knee, and anterior lower leg.
This appearance is consistent with purpura due to Waterhouse-Friderichsen syndrome.
Source: © IMPP
Prognosis
-
Bacterial meningitis
- Fatal if left untreated
- Prognosis in treated patients depends on age, overall condition, immune status and the pathogen(s) involved.
-
Viral meningitis
- Resolves spontaneously in the majority of cases
- Residual symptoms such as sensorineural hearing loss, epilepsy, and cognitive deficits are rare.
-
Fungal meningitis
- Associated with neurological sequelae and a high mortality rate
- Treatment adherence is very important to avoid relapse.
References:[70][71]
Prevention
Primary prevention [72]
-
Follow recommended ACIP immunization schedules, particularly for:
- Meningococcal vaccine
- Pneumococcal vaccine
- Haemophilus influenzae type b vaccine
- Manage conditions that increase the risk of developing severe infections.
- Promptly treat infections that can spread to the CNS (e.g., mastoiditis, sepsis).
- Prevent vertical transmission of infections to neonates
Meningococcal vaccine [9][73]
- There are three types of meningococcal vaccine.
- Meningococcal ACWY vaccines (protein-conjugate) [73]
- Meningococcal B vaccines (protein-based) [73]
- Pentavalent meningococcal vaccine (MenABCWY) [74]
- The meningococcal vaccination schedule varies widely between countries.
- In the US vaccination is recommended for:
- Adolescents
- Individuals with risk factors for meningococcal disease
- For further information, see “ACIP immunization schedule.”
- In the US vaccination is recommended for:
Individuals for whom both the meningococcal ACWY and meningococcal B vaccine are indicated at the same visit can be offered the pentavalent meningococcal vaccine. [74]
Prevention of onward transmission
- Follow empiric droplet precautions and then adjust based on the identified pathogen. [75]
- Provide postexposure chemoprophylaxis for close contacts. [9]
- During community outbreaks of N. meningitidis: Vaccinate against the circulating serotype. [9]
Meningococcal disease is a nationally notifiable disease; other etiologies of meningitis may also be reportable depending on local state law. [76]
Postexposure chemoprophylaxis [77]
Administer chemoprophylaxis as soon as possible, preferably within 24 hours of symptom onset in the index patient. [9]
| Postexposure chemoprophylaxis for bacterial meningitis [9][77] | ||
|---|---|---|
| Pathogen | Indications | Recommended regimens [9] |
| N. meningitidis [9][78][79] |
|
|
| H. influenzae [9] [81] |
|
|
Special patient groups
Meningitis in children [6][7][9]
The following applies to children ≥ 29 days of age. For younger children, see “Neonatal bacterial meningitis.”
Etiology [6][9][82]
- Bacterial
- S. pneumonia
- N. meningitidis
- See also “Most common causative agents of bacterial meningitis by age group and underlying condition.”
- Viral
- Most common: enterovirus
- Herpes simplex virus (life-threatening; more common in neonates 1–3 weeks old) [6][9]
- Parechovirus [7]
Rates of bacterial meningitis in infants and children are declining due to a combination of vaccination against Hib and Streptococcus pneumoniae, prenatal GBS screening, and intrapartum prophylactic antibiotics for GBS. [72]
Clinical features [6][82][83]
-
Children < 2 years old often have nonspecific symptoms without meningismus.
- Poor appetite, vomiting
- Neurological signs
- Altered mental status (most common): lethargy; , irritability, seizures
- Signs of increased intracranial pressure: bulging fontanelle (in infants), cranial nerve palsies
- Hypotonia, high-pitched crying, abnormal breathing patterns [83]
- Changes in vital signs
- Temperature instability: hyperthermia, hypothermia
- Abnormal breathing patterns: tachypnea, apnea
- Heart rate changes: tachycardia, bradycardia
- For children ≥ 2 years of age, see “Clinical features of meningitis.”
Diagnostics for meningitis in children [82]
For neonates, see “Diagnostics for neonatal bacterial meningitis.”
- Diagnostics for meningitis do not differ significantly between adults and children.
- In all neonates and in children with signs of complications , consider neuroimaging. [72]
- Cranial ultrasound (neonates) [72][84]
- CT/MRI brain [72]
- A multiplex PCR meningitis panel, if available, may help guide management. [85]
- If < 60 days old (especially < 21 days old): Evaluate for red flag features for HSV in infants and, if indicated, obtain infant HSV testing. [7]
Treatment for meningitis in children [82][86]
For neonates, see “Management of neonatal bacterial meningitis.”
- Initial management of meningitis does not differ between children and adults.
- For unstable patients, initiate immediate stabilization for meningitis.
- Start empiric antimicrobial therapy as appropriate.
- Consult specialists (infectious disease, intensive care, or neurology) as needed.
Empiric antibiotic therapy
The following recommendations are for infants and children ≥ 29 days of age. For neonates, see “Empiric antibiotics for neonatal sepsis.”
- Suspected bacterial meningitis: Start empiric antibiotic therapy with vancomycin PLUS ceftriaxone. [9][37]
- Suspected viral meningitis in otherwise healthy children : Consider using a meningitis scoring system, e.g., the bacterial meningitis score. [86][87][88]
- Elevated meningitis score (indicates bacterial meningitis): Initiate empiric antibiotic therapy.
- Low meningitis score, well-appearing, and no risk factors: Consider discharge, with close follow-up. [86][88]
Avoid ceftriaxone in neonates because of the risk of kernicterus; use cefotaxime or ceftazidime when possible. [9]
Pathogen-specific management
- Initiate additional therapies if certain pathogens are suspected.
- Suspected HSV meningitis (i.e., infants with red flag features for HSV in infants) : Add acyclovir. [7][9]
-
Suspected H. influenza or S. pneumonia: Consider dexamethasone (off-label) if it can be given before or within 1 hour of initial antibiotics. [6][72]
- H. influenzae: all children ≥ 29 days of age [9]
- S. pneumonia: Consider for children ≥ 6 weeks of age. [9][49]
- Once the etiology is known, change from empiric to pathogen-specific therapy in meningitis.

Glucocorticoids are not recommended in neonates with meningitis because of a paucity of high-quality evidence to support benefits. [9][89]
Monitoring
- Repeat LP in neonates with gram-negative or HSV meningitis. [4][9][37]
- Monitor BMP to help adjust IV fluids and antimicrobial dosages, and to assess for the development of SIADH. [72]
Ongoing management [4][9][37]
- Obtain an audiology evaluation prior to discharge from the hospital. [4][72]
- In children with residual neurological defects, refer to appropriate services. [72]
- The primary medical provider should monitor closely for:
- Subsequent hearing loss
- Delays in child development and milestones [4]
Created by: QxMD.
External Resources
References
- Mount HR, Boyle SD. "Aseptic and Bacterial Meningitis: Evaluation, Treatment, and Prevention.". Am Fam Physician. 96(5). :314-322. (2017)
- Bamberger. "Diagnosis, Initial Management, and Prevention of Meningitis". American Family Physician. (2010)
- Ku LC, Boggess KA, Cohen-Wolkowiez M. "Bacterial Meningitis in Infants". Clin Perinatol. 42(1). :29-45. (2015)
- Blaney SM, Giardino AP, Orange JS, et al. "Rudolph's Pediatrics, 23rd Edition". McGraw-Hill Education / Medical. (2018). ISBN: 9781259588594
- Pantell RH, Roberts KB, Adams WG, et al. "Evaluation and Management of Well-Appearing Febrile Infants 8 to 60 Days Old". Pediatrics. 148(2). (2021)
- Ouchenir L, Renaud C, Khan S, et al. "The Epidemiology, Management, and Outcomes of Bacterial Meningitis in Infants". Pediatrics. 140(1). (2017)
- Thigpen MC, Whitney CG, Messonnier NE, et al. "Bacterial Meningitis in the United States, 1998–2007". N Engl J Med. 364(21). :2016-2025. (2011)
- AAP Committee on Infectious Diseases. "Red Book: 2021–2024 Report of the Committee on Infectious Diseases". American Academy of Pediatrics. (2021). ISBN: 9781610025218
- Tavares T, Pinho L, Bonifácio Andrade E. "Group B Streptococcal Neonatal Meningitis". Clin Microbiol Rev. 35(2). (2022)
- Wenger JD, Hightower AW, Facklam RR, Gaventa S, Broome CV. "Bacterial Meningitis in the United States, 1986: Report of a Multistate Surveillance Study". J Infect Dis. 162(6). :1316-1323. (1990)
- Castelblanco RL, Lee M, Hasbun R. "Epidemiology of bacterial meningitis in the USA from 1997 to 2010: a population-based observational study". Lancet Infect Dis. 14(9). :813-819. (2014)
- Bamberger DM. "Diagnosis, initial management, and prevention of meningitis.". Am Fam Physician. 82(12). :1491-8. (2010)
- Brouwer MC, Tunkel AR, van de Beek D. "Epidemiology, Diagnosis, and Antimicrobial Treatment of Acute Bacterial Meningitis". Clin Microbiol Rev. 23(3). :467-492. (2010)
- Srihawan C, Castelblanco RL, Salazar L, et al. "Clinical Characteristics and Predictors of Adverse Outcome in Adult and Pediatric Patients With Healthcare-Associated Ventriculitis and Meningitis". Open Forum Infectious Diseases. 3(2). :ofw077. (2016)
- Hasbun R, Rosenthal N, Balada-Llasat JM, et al. "Epidemiology of Meningitis and Encephalitis in the United States, 2011–2014". Clinical Infectious Diseases. 65(3). :359-363. (2017)
- Miskin DP, Koralnik IJ. "Novel syndromes associated with JC virus infection of neurons and meningeal cells". Curr Opin Neurol. 28(3). :288-294. (2015)
- Pires SAP, Lemos AP, Pereira EPMN, Maia PA da SV, Agro JP de S e AB do. "IBUPROFEN-INDUCED ASEPTIC MENINGITIS: A CASE REPORT". Revista Paulista de Pediatria. 37(3). :382-385. (2019)
- Overturf GD. "Indications for the Immunological Evaluation of Patients with Meningitis". Clinical Infectious Diseases. 36(2). :189-194. (2003)
- Chadwick DR. "Viral meningitis". Br Med Bull. 75-76(1). :1-14. (2005)
- Charalambous LT, Premji A, Tybout C, et al. "Prevalence, healthcare resource utilization and overall burden of fungal meningitis in the United States". J Med Microbiol. 67(2). :215-227. (2018)
- Baliu C, Sanclemente G, Cardona M, et al. "Toxoplasmic encephalitis associated with meningitis in a heart transplant recipient". Transplant Infectious Disease. 16(4). :631-633. (2014)
- Kohil A, Jemmieh S, Smatti MK, Yassine HM. "Viral meningitis: an overview". Arch Virol. 166(2). :335-345. (2021)
- Van de Beek D, de Gans J, Spanjaard L, et al. "Clinical Features and Prognostic Factors in Adults with Bacterial Meningitis". N Engl J Med. 351(18). :1849-1859. (2004)
- Weisfelt M, Van De Beek D, Spanjaard L, Reitsma JB, De Gans J. "Community-Acquired Bacterial Meningitis in Older People". J Am Geriatr Soc. 54(10). :1500-1507. (2006)
- Bissonnette B, Luginbuehl I, Engelhardt T. "Syndromes: Rapid Recognition and Perioperative Implications, 2nd edition". McGraw-Hill Education / Medical. (2019). ISBN: 9781259861789
- Agabegi SS, Agabegi ED. "Step-Up To Medicine". Wolters Kluwer Health. (2015). ISBN: 9781496306142
- Le T, Bhushan V, Chen V, King M. "First Aid for the USMLE Step 2 CK". McGraw-Hill Education. (2015). ISBN: 9780071844574
- Tunkel AR. "Clinical features and diagnosis of acute bacterial meningitis in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/clinical-features-and-diagnosis-of-acute-bacterial-meningitis-in-adults. [2016-08-17]
- Tsai J, Nagel MA, Gilden D. "Skin rash in meningitis and meningoencephalitis". Neurology. 80(19). :1808-1811. (2013)
- Daroff RB, et al. "Bradley's Neurology in Clinical Practice". Elsevier. ISBN: 9780323287838
- Silva MTT. "Viral encephalitis". Arq Neuropsiquiatr. 71(9B). :703-709. (2013)
- Tunkel AR, Hartman BJ, Kaplan SL, et al. "Practice Guidelines for the Management of Bacterial Meningitis". Clinical Infectious Diseases. 39(9). :1267-1284. (2004)
- Van de Beek D, Cabellos C, Dzupova O, et al. "ESCMID guideline: diagnosis and treatment of acute bacterial meningitis". Clinical Microbiology and Infection. 22. :S37-S62. (2016)
- Tunkel et al. "2017 Infectious Diseases Society of America’s Clinical Practice Guidelines for Healthcare-Associated Ventriculitis and Meningitis". Clin Infect Dis. 64(6). :e34-e65. (2017)
- Seehusen, et al. "Cerebrospinal Fluid Analysis". American Family Physician. (2003)
- Kastrup O, Wanke I, Maschke M. "Neuroimaging of infections". NeuroRX. 2(2). :324-332. (2005)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Thwaites G. "Neurological aspects of tropical disease: Tuberculous meningitis". Journal of Neurology, Neurosurgery & Psychiatry. 68(3). :289-299. (2000)
- Krawczuk K, Czupryna P, Pancewicz S, et al. "Comparison of Neuroborreliosis Between Children and Adults". Pediatr Infect Dis J. 39(1). :7-11. (2020)
- Bahr NC, Boulware DR. "Methods of rapid diagnosis for the etiology of meningitis in adults". Biomarkers in Medicine. 8(9). :1085-1103. (2014)
- Van de Beek D, Brouwer MC, Thwaites GE, Tunkel AR. "Advances in treatment of bacterial meningitis". Lancet. 380(9854). :1693-1702. (2012)
- Tunkel AR, Glaser CA, Bloch KC, et al. "The Management of Encephalitis: Clinical Practice Guidelines by the Infectious Diseases Society of America". Clin Infecti Dis. 47(3). :303-327. (2008)
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161
- Kim KS. "Neonatal Bacterial Meningitis". NeoReviews. 16(9). :e535-e543. (2015)
- Alamarat Z, Hasbun R. "Management of Acute Bacterial Meningitis in Children". Infect Drug Resist. Volume 13. :4077-4089. (2020)
- Tan JS, File T, Salata RA. "Expert Guide to Infectious Diseases". ACP Press. (2008). ISBN: 9781934465769
- McCollough M. "The Algorithmic Approach to the Unidentified Rash". Springer International Publishing. :215-240. (2018). ISBN: 9783319756226
- De Gans J, van de Beek D. "Dexamethasone in Adults with Bacterial Meningitis". N Engl J Med. 347(20). :1549-1556. (2002)
- Sexton DJ. "Neurologic complications of bacterial meningitis in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/neurologic-complications-of-bacterial-meningitis-in-adults. [2015-09-01]
- Braun-Falco O, Plewig G, Wolff HH, Burgdorf WHC. "Dermatology". Springer Science & Business Media. (2012). ISBN: 9783642979316
- Scheld WM, Whitley RJ, Marra CM. "Infections of the Central Nervous System". Wolters Kluwer. (2014). ISBN: 9781451173727
- Jong EC, Stevens DL. "Netter's Infectious Diseases E-Book". Elsevier Health Sciences. (2011). ISBN: 9781455712250
- Scheld WM, Whitley RJ, Marra CM. "Infections of the Central Nervous System". Lippincott Williams & Wilkins. (2004). ISBN: 9780781743273
- Swanson D. "Meningitis". Pediatr Rev. 36(12). :514-526. (2015)
- "Child and Adolescent Immunization Schedule. Recommendations for Ages 18 Years or Younger, United States, 2022". https://web.archive.org/web/20220809054312/https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html. [2022-02-17]
- "CDC committee OKs recommendations for pentavalent meningococcal, mpox vaccines". https://web.archive.org/web/20231027131159/https://publications.aap.org/aapnews/news/27054/CDC-committee-OKs-recommendations-for-pentavalent?autologincheck=redirected
- Siegel JD, Rhinehart E, Jackson M, Chiarello L. "2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Health Care Settings". Am J Infect Control. 35(10). :S65-S164. (2007)
- "CDC Clinical Info: Meningococcal Disease". https://web.archive.org/web/20231019132230/https://www.cdc.gov/meningococcal/clinical-info.html
- "Meningococcal disease". https://web.archive.org/web/20220915150242/https://www.cdc.gov/infectioncontrol/guidelines/healthcare-personnel/selected-infections/meningococcal-disease.html. [2021-11-12]
- "Manual for the Surveillance of Vaccine-Preventable Diseases: Chapter 8: Meningococcal Disease"
- Cohn AC, MacNeil JR, Clark TA, et al. "Prevention and control of meningococcal disease: recommendations of the Advisory Committee on Immunization Practices (ACIP).". MMWR: Recommendations and reports. 62(RR-2). :1-28. (2013)
- Patel K, Goldman JL. "Safety Concerns Surrounding Quinolone Use in Children.". J Clin Pharmacol. 56(9). :1060-75. (2016)
- Saag MS et al. "The Sanford Guide to Antimicrobial Therapy 2016". Antimicrobial Therapy, Inc. (2016). ISBN: 9781930808935
- American Academy of Pediatrics. "Textbook of Pediatric Care". American Academy of Pediatrics. (2016). ISBN: 9781610020473
- Ershad M, Mostafa A, Dela Cruz M, Vearrier D. "Neonatal Sepsis". Curr Emerg Hosp Med Rep. 7(3). :83-90. (2019)
- Gupta N, Grover H, Bansal I, et al. "Neonatal cranial sonography: ultrasound findings in neonatal meningitis—a pictorial review". Quant Imaging Med Surg. 7(1). :123-131. (2017)
- Nabower AM, Miller S, Biewen B, et al. "Association of the FilmArray Meningitis/Encephalitis Panel With Clinical Management". Hosp Pediatr. 9(10). :763-769. (2019)
- Young SM, Saguil A. "Bacterial Meningitis in Children.". Am Fam Physician. 105(3). :311-312. (2022)
- Nigrovic LE. "Clinical Prediction Rule for Identifying Children With Cerebrospinal Fluid Pleocytosis at Very Low Risk of Bacterial Meningitis". JAMA. 297(1). :52. (2007)
- Mintegi S, García S, Martín MJ, et al. "Clinical Prediction Rule for Distinguishing Bacterial From Aseptic Meningitis". Pediatrics. 146(3). (2020)
- Ogunlesi TA, Odigwe CC, Oladapo OT. "Adjuvant corticosteroids for reducing death in neonatal bacterial meningitis". Cochrane Database Syst Rev. 2015(11). (2015)
- Christensen H, May M, Bowen L, Hickman M, Trotter CL. "Meningococcal carriage by age: a systematic review and meta-analysis". Lancet Infect Dis. 10(12). :853-861. (2010)
- "Epidemiology and Prevention of Vaccine-Preventable Diseases"
- "Bacterial Meningitis". https://web.archive.org/web/20170502074900/https://www.cdc.gov/meningitis/bacterial.html. [2017-01-25]
- Novak RT, Ronveaux O, Bita AF, et al. "Future Directions for Meningitis Surveillance and Vaccine Evaluation in the Meningitis Belt of Sub-Saharan Africa". J Infect Dis. 220(Supplement_4). :S279-S285. (2019)
- Abassi M, Boulware DR, Rhein J. "Cryptococcal Meningitis: Diagnosis and Management Update.". Current tropical medicine reports. 2(2). :90-99. (2015)
- "Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV: Cryptococcosis". https://web.archive.org/web/20240530001102/https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-opportunistic-infections/cryptococcosis?view=full. [2024-01-10]
- Grace E et al. "Naegleria fowleri: Pathogenesis, Diagnosis, and Treatment Options". Antimicrobial Agents Chemother (Bethesda). 59(11). :6677-6681. (2015)
- "CDC — Primary Amebic Meningoencephalitis (PAM) — Treatment". https://web.archive.org/web/20210724214409/https://www.cdc.gov/parasites/naegleria/treatment.html. [2019-04-04]
- Cherian A, Thomas SV. "Central nervous system tuberculosis". Afr Health Sci. 11(1). :116-127. (2011)
- Cox GM, Perfect JR. "Epidemiology, clinical manifestations, and diagnosis of Cryptococcus neoformans meningoencephalitis in HIV-infected patients". UpToDate. UpToDate. http://www.uptodate.com/contents/epidemiology-clinical-manifestations-and-diagnosis-of-cryptococcus-neoformans-meningoencephalitis-in-hiv-infected-patients. [2016-01-04]
- Cox GM, Perfect JR. "Clinical management and monitoring during antifungal therapy of the HIV-infected patient with cryptococcal meningoencephalitis". UpToDate. UpToDate. http://www.uptodate.com/contents/clinical-management-and-monitoring-during-antifungal-therapy-of-the-hiv-infected-patient-with-cryptococcal-meningoencephalitis. [2016-02-22]
- "Tick-borne Encephalitis (TBE)". https://web.archive.org/web/20170328074157/https://www.cdc.gov/vhf/tbe/index.html. [2014-03-31]
- "Travelers' Health: Tick-borne Encephalitis". https://web.archive.org/web/20170614131906/https://wwwnc.cdc.gov/travel/diseases/tickborne-encephalitis. [2013-03-09]
- "Naegleria fowleri - Primary Amebic Meningoencephalitis (PAM)". https://web.archive.org/web/20200404122216/https://www.cdc.gov/parasites/naegleria/treatment.html. [2017-02-28]
- Wright WF, Pinto CN, Palisoc K, Baghli S. "Viral (aseptic) meningitis: A review". J Neurol Sci. 398. :176-183. (2019)
- Bihan K, Weiss N, Théophile H, Funck‐Brentano C, Lebrun‐Vignes B. "Drug‐induced aseptic meningitis: 329 cases from the French pharmacovigilance database analysis". Br J Clin Pharmacol. 85(11). :2540-2546. (2019)
- Shukla B, Aguilera EA, Salazar L, et al. "Aseptic meningitis in adults and children: Diagnostic and management challenges". Journal of Clinical Virology. 94. :110-114. (2017)
- Jakobsen A, Skov MT, Larsen L, et al. "Herpes Simplex Virus 2 Meningitis in Adults: A Prospective, Nationwide, Population-Based Cohort Study". Clin Infect Dis.. 75(5). :753-760. (2022)