Summary
Metabolic dysfunction-associated steatotic liver disease (MASLD) is the accumulation of excess fat in hepatocytes in individuals with at least one cardiometabolic risk factor (e.g., hypertension, impaired glucose tolerance) in the absence of an alternative cause (e.g., heavy alcohol use, drug-induced liver injury). MASLD was previously known as nonalcoholic fatty liver disease. It is highly prevalent in patients with type 2 diabetes mellitus (T2DM), obesity, and/or metabolic syndrome. MASLD is usually asymptomatic and is a diagnosis of exclusion. Diagnostic findings may include hepatic steatosis on imaging and elevated transaminases. Patients with MASLD should be assessed for advanced liver fibrosis using a combination of laboratory-based noninvasive testing, such as the FIB-4, and vibration-controlled transient elastography. Metabolic dysfunction-associated steatohepatitis (MASH) is a subtype of MASLD characterized by chronic hepatocyte inflammation and damage due to lipid accumulation and is associated with a higher risk of progression to liver fibrosis and cirrhosis. MASH was previously known as nonalcoholic steatohepatitis (NASH). Biopsy may be indicated if there is diagnostic uncertainty. Management focuses on the prevention and treatment of associated metabolic conditions.
Definitions
The nomenclature for steatotic liver disease was updated by international liver disease societies in June 2023. [1]
-
Metabolic dysfunction-associated steatotic liver disease (MASLD) [1]
- A type of steatotic liver disease that occurs in individuals with ≥ 1 criterion for metabolic syndrome in the absence of an alternative cause (e.g., heavy alcohol use)
- Previously referred to as nonalcoholic fatty liver disease (NAFLD)
-
Metabolic dysfunction-associated steatohepatitis (MASH) [1]
- A subtype of MASLD characterized by chronic hepatocellular inflammation and damage
- Previously referred to as nonalcoholic steatohepatitis (NASH)
Epidemiology
-
Global prevalence in the general adult population
- MASLD: 25–30% [2][3]
- MASH: 12–14% [2]
-
Prevalence in US patients with T2DM
- MASLD: ∼ 70% [2]
- MASH: 30–40% [2]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
MASLD is a multifactorial disease with metabolic and genetic components. [2]
-
Cardiometabolic risk factors: any criterion for metabolic syndrome [4]
- Central obesity
- Prediabetes or T2DM
- Hypertension ≥ 130/85 mm Hg or taking antihypertensives
- Hypertriglyceridemia, low HDL cholesterol , or taking lipid-lowering drugs
- Genetic factors: Individuals with a first-degree relative with MASH-related cirrhosis are at increased risk. [2]
Pathophysiology
- MASLD; : excess energy supply → insulin resistance →; ↑ circulating dietary sugars and free fatty acids → ↑ hepatic free fatty acids → ↑ triglyceride synthesis → hepatic steatosis [2]
- MASH cirrhosis; : oxidative stress, endoplasmic reticulum stress, and inflammasome activation → inflammation and hepatocyte stress and/or death → fibrogenesis → cirrhosis [2]
Clinical features
- Often asymptomatic
-
MASH can manifest with signs of advanced liver disease, e.g.:
- Hepatomegaly, splenomegaly
- Clinical features of cirrhosis
Screening
Screening for MASLD-related liver fibrosis is indicated in some high-risk populations, even in the absence of a prior diagnosis of MASLD; see "Noninvasive evaluation for liver fibrosis" for details.
Diagnosis
Approach [2][3][4][5]
Suspect MASLD in patients with risk factors for MASLD, incidental hepatic steatosis on imaging, and/or idiopathic elevation of transaminases for ≥ 6 months.
- MASLD is diagnosed in patients who meet all of the following criteria: [1]
- ≥ 1 criterion for metabolic syndrome
- Hepatic steatosis on imaging or biopsy
- Exclusion of alternative causes of hepatic steatosis based on patient history (e.g., current or prior heavy alcohol use) and laboratory studies ± imaging
- Perform noninvasive evaluation for liver fibrosis (i.e., with FIB-4 score ± imaging) in patients with known or suspected MASLD.
- Consider referral for liver biopsy if the diagnosis remains uncertain or MASH is suspected.
It is only possible to distinguish MASLD from alcohol-associated fatty liver disease using patient history.
Initial studies
Laboratory studies [4]
-
Liver chemistries
-
Transaminases
- Normal or ↑ AST and/or ALT
- AST/ALT ratio usually < 1
- AST/ALT ratio of > 1 may indicate progression to cirrhosis.
- Normal or ↓ serum albumin
-
Transaminases
- CBC: normal or ↓ platelet count
-
Tests to rule out alternative diagnoses
- All patients: serology for hepatitis B and hepatitis C
- Additional studies based on clinical suspicion, e.g.: [2]
- Serology for type 1 autoimmune hepatitis
- Tissue transglutaminase IgA for celiac disease
- Serum ferritin and transferrin saturation for iron overload disorders
- Testing for alpha-1 antitrypsin deficiency
- Serum ceruloplasmin to screen for Wilson disease
There is often more ALT than AST (AST/ALT ratio < 1) when Lipids infiltrate the Liver.
Abdominal ultrasound [6]
- May be used to confirm hepatic steatosis and/or exclude alternative diagnoses [2]
- Often nondiagnostic in patients with mild steatosis
- Supportive finding: ↑ liver echogenicity
Transaminase levels and abdominal ultrasound findings can be normal even in patients with advanced MASH and/or liver fibrosis and therefore should not be used to exclude advanced liver disease. [2]
Noninvasive evaluation for liver fibrosis [2][3][4][5]
Indications for noninvasive evaluation for liver fibrosis
- Known MASLD
- Prediabetes or T2DM [7]
- ≥ 2 criteria for metabolic syndrome [3]
- First-degree relative with MASH-related cirrhosis
- Incidental finding of hepatic steatosis on imaging
- Idiopathic elevated transaminases for ≥ 6 months
Serology
-
FIB-4: preferred [2]
- Low-risk score (i.e., < 1.3 in adults 35–65 years or < 2.0 in adults ≥ 65 years) [2][8]
- Prediabetes, T2DM, and/or ≥ 2 criteria for metabolic syndrome: Repeat FIB-4 score every 1–2 years. [7]
- All others: Repeat FIB-4 score every 2–3 years.
- Indeterminate score: Obtain imaging for liver stiffness measurement, if available; consider referral to hepatology. [2][3]
- High-risk score (i.e., > 2.67): Refer to hepatology for advanced diagnostics. [2][8]
- Low-risk score (i.e., < 1.3 in adults 35–65 years or < 2.0 in adults ≥ 65 years) [2][8]
- NAFLD score
- APRI score
Imaging tests
Imaging tests are used for liver stiffness measurement.
-
Vibration-controlled transient elastography (VCTE): best initial test for patients with an indeterminate or high risk on noninvasive testing [2][4]
- Low risk (< 8.0 kPA): Continue with FIB-4 screening every 1–3 years.
- Indeterminate risk (8.0–12 kPA) or high risk (> 12.0 kPA): Refer to hepatology.
- MR elastography: Consider if there is diagnostic uncertainty after VCTE. [3]

Liver biopsy [3][4]
-
Indications
- Diagnostic uncertainty after noninvasive testing and imaging
- Suspicion of MASH (gold standard)
- Supportive findings for MASLD: hepatocellular lipid accumulation, mostly macrovesicular
-
Additional findings in MASH
- Necrosis and ballooning degeneration
- Inflammatory infiltrates with scattered lymphocytes, neutrophils, and Kupffer cells
- Steatosis
The diagnosis of MASH requires histological evidence of steatohepatitis. Noninvasive testing can estimate fibrosis stage but cannot confirm MASH. [2]
")
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
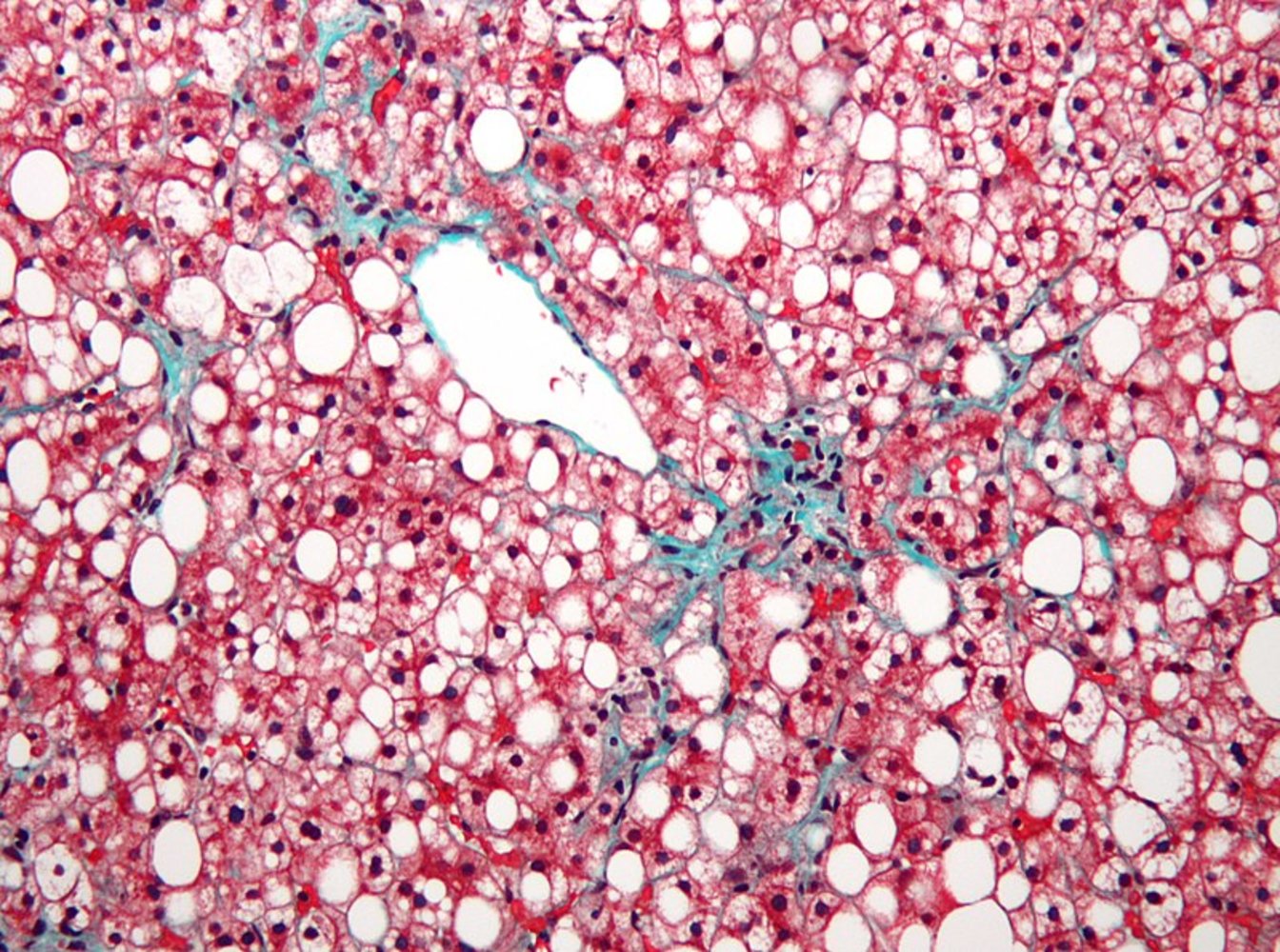
Photomicrograph of hepatic tissue (Masson trichrome stain; high magnification)
There is prominent macrovesicular steatosis of the centrilobular hepatocytes. A typical steatotic hepatocyte is enlarged in the overlay zoombox: The large lipid vacuole (blue overlay) has pushed the nucleus (black dashed line) against the cell membrane (white dashed line), creating a signet ring appearance (not to be confused with signet ring cells in gastric carcinoma). There is also mild fibrosis (example indicated by arrowhead; collagen fibers are stained blue-green with trichrome stain).
This appearance is characteristic of MASLD (previously known as nonalcoholic fatty liver disease).
Source: “Non-alcoholic fatty liver disease1” by Nephron, Wikimedia Commons, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
Management
General principles
- Management is focused on the prevention and treatment of associated metabolic conditions.
- Provide multidisciplinary care (e.g., involve the primary care physician, endocrinologist, hepatologist, and dietitian).
- Patients previously classified as low risk for liver fibrosis: Continue ongoing periodic noninvasive evaluation for liver fibrosis based on risk factors.
- Refer to hepatology for:
- Further assessment in patients with indeterminate or high-risk noninvasive test results
- Pharmacological management to reduce hepatic steatosis
- Management of advanced liver fibrosis or cirrhosis
Nonpharmacological management [2][3][4][9]
-
Lifestyle changes
- Healthy diet (e.g., Mediterranean diet)
- Regular exercise
- Avoidance of alcohol
- Weight loss for patients with overweight
-
Management of associated metabolic conditions
- Management of diabetes mellitus
- Management of obesity
- Management of hypertension
- Management of ASCVD
- Management of malnutrition in adults
Pharmacological management [2][3]
Consider the following medications in consultation with a specialist (e.g., hepatologist) to achieve weight loss goals and/or reduce hepatic steatosis and/or steatohepatitis:
-
MASLD
- SGLT-2 inhibitor (e.g., dapagliflozin or empagliflozin) for patients with T2DM [10][11]
- Tirzepatide for patients with T2DM or obesity [12]
-
MASH
- All patients without cirrhosis: vitamin E (off-label) [9]
- Patients with moderate to advanced fibrosis (stages F2-F3)
- GLP-1 receptor agonist (e.g., semaglutide ) [13]
- OR resmetirom [14]
- Patients with concomitant TD2M: pioglitazone [2]
There are currently no FDA-approved medications for the treatment of MASLD without fibrosis. Semaglutide or resmetirom are approved for MASH with moderate to advanced fibrosis. [13][14]
Differential diagnoses
- Alcohol-associated liver disease
-
Drug-induced liver injury due to:
- Amiodarone
- Methotrexate
- Tamoxifen
- Valproate
- Antiretroviral drugs
- Corticosteroids
-
Viral hepatitis
- Hepatitis C
- Hepatitis B
- Inherited or autoimmune disorders
- Hemochromatosis
- Alpha-1 antitrypsin deficiency
- Wilson disease
- Autoimmune hepatitis
- Reye syndrome
-
Pregnancy-related conditions
- HELLP syndrome
- Acute fatty liver of pregnancy
- Nutrition-related conditions
- Malnutrition
- Acute weight loss (e.g., from metabolic surgery or starvation)
- Celiac disease
- Parenteral nutrition
- See also “Causes of elevated transaminases.”
The differential diagnoses listed here are not exhaustive.
Complications
- Advanced liver fibrosis, cirrhosis
- Hepatocellular carcinoma
We list the most important complications. The selection is not exhaustive.
Prognosis
-
MASLD [4]
- Low risk of progression to cirrhosis or hepatocellular carcinoma in patients with only one cardiometabolic risk factor
- The risk of progression increases with each additional risk factor.
- Approximately 20% of patients with MASH develop liver fibrosis. [3]
Related One-Minute Telegram
- One-Minute Telegram 126-2025-3/3: A DAPA-tive response to MASH?
- One-Minute Telegram 96-2024-1/3: An aspirin a day keeps the hepatologist away
- One-Minute Telegram 93-2024-1/3: Type 2 diabetes and MASLD: a sweet victory for SGLT2 inhibitors?
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- Subscribe to the One-Minute Telegram
- 2025 ACG Clinical Guideline: Malnutrition and Nutritional Recommendations in Liver Disease
- 2023 AASLD Practice Guidance on the Clinical Assessment and Management of NAFLD
- 2023 Multi-society Delphi Consensus Statement on New Fatty Liver Disease Nomenclature
- 2022 AACE Clinical Practice Guideline for the Diagnosis and Management of NAFLD
- 2021 AGA Clinical Care Pathway for the Risk Stratification and Management of Patients With NAFLD
References
- Rinella ME, Lazarus JV, Ratziu V, et al. "A multi-society Delphi consensus statement on new fatty liver disease nomenclature". Hepatology. Publish Ahead of Print. (2023)
- Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, et al. "AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease". Hepatology. 77(5). :1797-1835. (2023)
- Cusi K, Isaacs S, Barb D, et al. "American Association of Clinical Endocrinology Clinical Practice Guideline for the Diagnosis and Management of Nonalcoholic Fatty Liver Disease in Primary Care and Endocrinology Clinical Settings". Endocr Pract. 28(5). :528-562. (2022)
- Kanwal F, Shubrook JH, Adams LA, et al. "Clinical Care Pathway for the Risk Stratification and Management of Patients With Nonalcoholic Fatty Liver Disease (Retired 2026)". Gastroenterology. 161(5). :1657-1669. (2021)
- Tilg H, Petta S, Stefan N, Targher G. "Metabolic Dysfunction–Associated Steatotic Liver Disease in Adults". JAMA. (2025)
- Hamer OW, Aguirre DA, Casola G, et al. "Fatty Liver: Imaging Patterns and Pitfalls". RadioGraphics. 26(6). :1637-1653. (2006)
- American Diabetes Association Professional Practice Committee for Diabetes*, Bajaj M, McCoy R, et al. "4. Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Care in Diabetes—2026". Diabetes Care. 49(Supplement_1). :S61-S88. (2025)
- Vallet-Pichard A, Mallet V, Nalpas B, et al. "FIB-4". Hepatology. 46(1). :32-36. (2007)
- Singal AK, Wong RJ, Dasarathy S, et al. "ACG Clinical Guideline: Malnutrition and Nutritional Recommendations in Liver Disease". Am J Gastroenterol. 120(5). :950-972. (2025)
- Latva-Rasku A, Honka MJ, Kullberg J, et al. "The SGLT2 Inhibitor Dapagliflozin Reduces Liver Fat but Does Not Affect Tissue Insulin Sensitivity: A Randomized, Double-Blind, Placebo-Controlled Study With 8-Week Treatment in Type 2 Diabetes Patients". Diabetes Care. 42(5). :931-937. (2019)
- Kuchay MS, Krishan S, Mishra SK, et al. "Effect of Empagliflozin on Liver Fat in Patients With Type 2 Diabetes and Nonalcoholic Fatty Liver Disease: A Randomized Controlled Trial (E-LIFT Trial)". Diabetes Care. 41(8). :1801-1808. (2018)
- Gastaldelli A, Cusi K, Fernández Landó L, et al. "Effect of tirzepatide versus insulin degludec on liver fat content and abdominal adipose tissue in people with type 2 diabetes (SURPASS-3 MRI): a substudy of the randomised, open-label, parallel-group, phase 3 SURPASS-3 trial". The Lancet Diabetes Endocrinol. 10(6). :393-406. (2022)
- Bansal M, Patton H, Morgan T, et al. "Semaglutide therapy for metabolic dysfunction-associated steatohepatitis: November 2025 updates to AASLD Practice Guidance". Hepatology. (2025)
- Chen V, Morgan T, Rotman Y, et al. "Resmetirom therapy for metabolic dysfunction-associated steatotic liver disease: October 2024 updates to AASLD Practice Guidance". Hepatology. 81(1). :312-320. (2024)