Summary
Multifetal gestation is a pregnancy with two or more fetuses. Previous multifetal gestation and use of assisted reproductive technology increase the risk of multifetal gestation, which may be fraternal (multizygotic) or identical (monozygotic). The diagnosis is suspected in individuals who present with exaggerated features of pregnancy (e.g., hyperemesis gravidarum, excessive weight gain) and fundal height unusually large for the gestational age. Ultrasound is used to confirm the diagnosis and determine chorionicity. Increased prenatal care, including more frequent ultrasound surveillance, is recommended for multifetal gestations. Multifetal reduction may be recommended to improve outcomes in triplet or higher-order pregnancies; selective termination may be recommended for severe health problems in one fetus. Antepartum fetal surveillance is recommended in the third trimester, with delivery usually scheduled between 32 and 38 weeks' gestation for twin pregnancies. Pregnancies with more than one fetus are considered high-risk pregnancies and carry an increased risk of almost all complications of pregnancy, including hypertensive pregnancy disorders, pregnancy loss, and preterm labor. Monochorionic multifetal pregnancies are associated with a higher risk of complications and fetal anomalies than multichorionic pregnancies and should be monitored closely.
Definitions
-
Zygosity
- The genetic classification of embryos in a multifetal gestation
- Monozygotic multiples are genetically identical.
- Multizygotic multiples are genetically distinct.
-
Chorionicity
- The type of placentation in multifetal gestations
- In monochorionic placentation, all fetuses share one placenta.
- In multichorionic placentation, each fetus has a separate placenta.
- Does not reflect zygosity (e.g., monozygotic twins may be monochorionic or dichorionic)
-
Amnionicity
- The number of amniotic sacs in multifetal gestations
- In monoamniotic pregnancies, all fetuses share one amniotic sac.
- In multiamniotic pregnancies, each fetus has a separate amniotic sac (e.g., diamniotic twin pregnancies; triamniotic triplet pregnancies).
Epidemiology
- The frequency of multiple births is calculated in accordance with Hellin's law. [1]
- Twins: ∼ 1:89
- Triplets: ∼ 1:892 (1:7,921)
- Quadruplets: ∼ 1:893 (1:704,969)
- The incidence of multifetal gestations (particularly dizygotic) has increased since the 1980s as assisted reproductive technology has become readily available.
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Predisposing factors include: [2]
- Advanced maternal age (≥ 35 years)
- Previous multifetal gestation
- Use of assisted reproductive technology
- Maternal family history of dizygotic twins
Subtypes and variants
Twin gestations
Monozygotic vs. dizygotic twins [2]
| Comparison of monozygotic vs. dizygotic twins | ||
|---|---|---|
| Identical twins (monozygotic twins) | Fraternal twins (dizygotic twins) | |
| Frequency |
|
|
| Origin |
|
|
| Genetics of the individual |
|
|
| Chorionic cavity and amniotic sac |
|
|
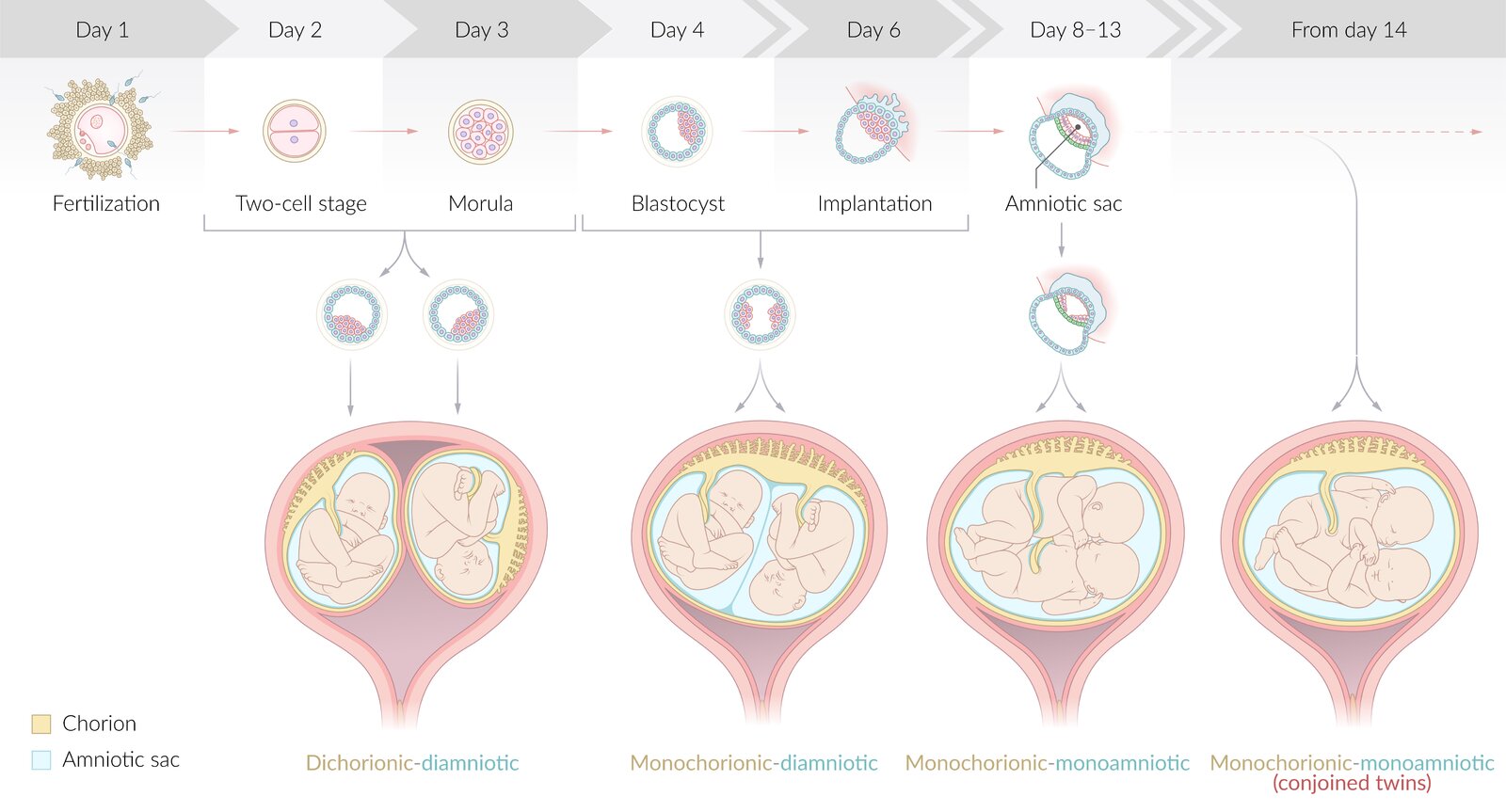
Chorionicity in twin gestations [2]
- Dizygotic pregnancy results in a dichorionic-diamniotic pregnancy.
- In monozygotic pregnancies, there are various pathways in which the amniotic sac and placenta are shared.
| Chorionicity of monozygotic twin pregnancy | |||
|---|---|---|---|
| Description | Time of division of the zygote [3] | Frequency in monozygotic twins | |
| Dichorionic-diamniotic (DCDA) |
|
|
|
| Monochorionic-diamniotic (MCDA) |
|
|
|
| Monochorionic-monoamniotic (MCMA) |
|
|
|
| Monochorionic-monoamniotic (conjoined twins) |
|
|
|

A four-wheeler has SPACe for twins. 1st four days (0–3): Separate placenta and amniotic sac; 2nd four days (4–7): shared Placenta; 3rd four days (8–11): shared Amniotic sac; day 12 and beyond: Conjoined twins.
Most twin pregnancies are dichorionic-diamniotic because most twins are dizygotic twins. Among monozygotic twins, however, the most common configuration is monochorionic-diamniotic. [2]
Higher-order multifetal gestations
- Higher-order multifetal gestations (e.g., triplets, quadruplets) may be fraternal (multizygotic) or identical (monozygotic). [4]
- Multizygotic multiples are genetically distinct; monozygotic multiples are genetically identical.
- In higher-order multifetal gestations, a combination of monozygotic and multizygotic multiples is common.
- Type of placentation: either monochorionic or multichorionic; and either monoamniotic or multiamniotic
Pregnancies with more than two fetuses may assume a variety of forms (e.g., triplets with two monochorionic fetuses and one fetus with its own placenta).
© AMBOSS
Clinical features
- Exaggerated symptoms of pregnancy (e.g., hyperemesis gravidarum, excessive weight gain) [5]
- Features of complications of pregnancy (e.g., preeclampsia, gestational diabetes, iron deficiency anemia) [5]
-
Physical examination findings [6]
- Fundal height and abdominal girth unusually large for the gestational age
- More than one fetus felt on palpation
- Two or more fetal heart rates heard on auscultation
Diagnosis
- The diagnostic approach is similar for singleton and multifetal gestation.
- Ultrasound is confirmatory.
- Laboratory studies may provide supportive evidence.
- See also “Diagnosis of pregnancy” and “Prenatal ultrasound.”
Laboratory studies
The following parameters are elevated for gestational age in multifetal pregnancies compared to singleton pregnancies.
- HCG [7]
- Additional studies [5][8]
- Maternal serum alpha-fetoprotein
- Human placental lactogen
Ultrasound (transvaginal or transabdominal) [3][9][10]
-
First-trimester ultrasound is used:
- To confirm multifetal gestation
- To determine chorionicity and amnionicity
- As part of prenatal genetic testing
- Second-trimester ultrasound is used to monitor for complications and fetal anomalies (see “Management” section for details).
Diagnostic confirmation
Any of the following confirms multifetal gestation.
- Multiple gestational sacs and yolk sacs (in dichorionic pregnancies)
- Multiple embryos (fetal poles) and/or fetal cardiac activity

Determination of chorionicity and amnionicity
The findings are similar in twin and higher-order pregnancies.
-
Chorionicity and amnionicity is best determined between 11 and 14 weeks' gestation. [3][10][11][12]
-
DCDA fetuses
- The chorionic cavities are separated from one another.
- Lambda sign: separation of the chorionic and amniotic sacs resembles the Greek symbol λ (lambda)
-
MCDA fetuses
- One chorionic cavity is present, and each twin has an individual amniotic sac.
- T-sign: Separation of the amniotic sacs resembles the letter T on ultrasound.
- MCMA fetuses: single chorionic cavity gestational sac
-
DCDA fetuses
- Findings on a second-trimester scan [11]
-
Monochorionic pregnancies
- A single placenta is present.
- Fetuses are of the same sex.
-
Multichorionic pregnancies
- Each fetus has its own distinct placenta.
- Sex of the fetuses may differ.
-
Monochorionic pregnancies
 in twin pregnancy")



Monochorionic multifetal pregnancies are associated with a higher risk of complications and fetal anomalies than multichorionic pregnancies. Identification of chorionicity and amnionicity in the first trimester or early second trimester is recommended to facilitate close monitoring of this group of patients. [10][11][12]
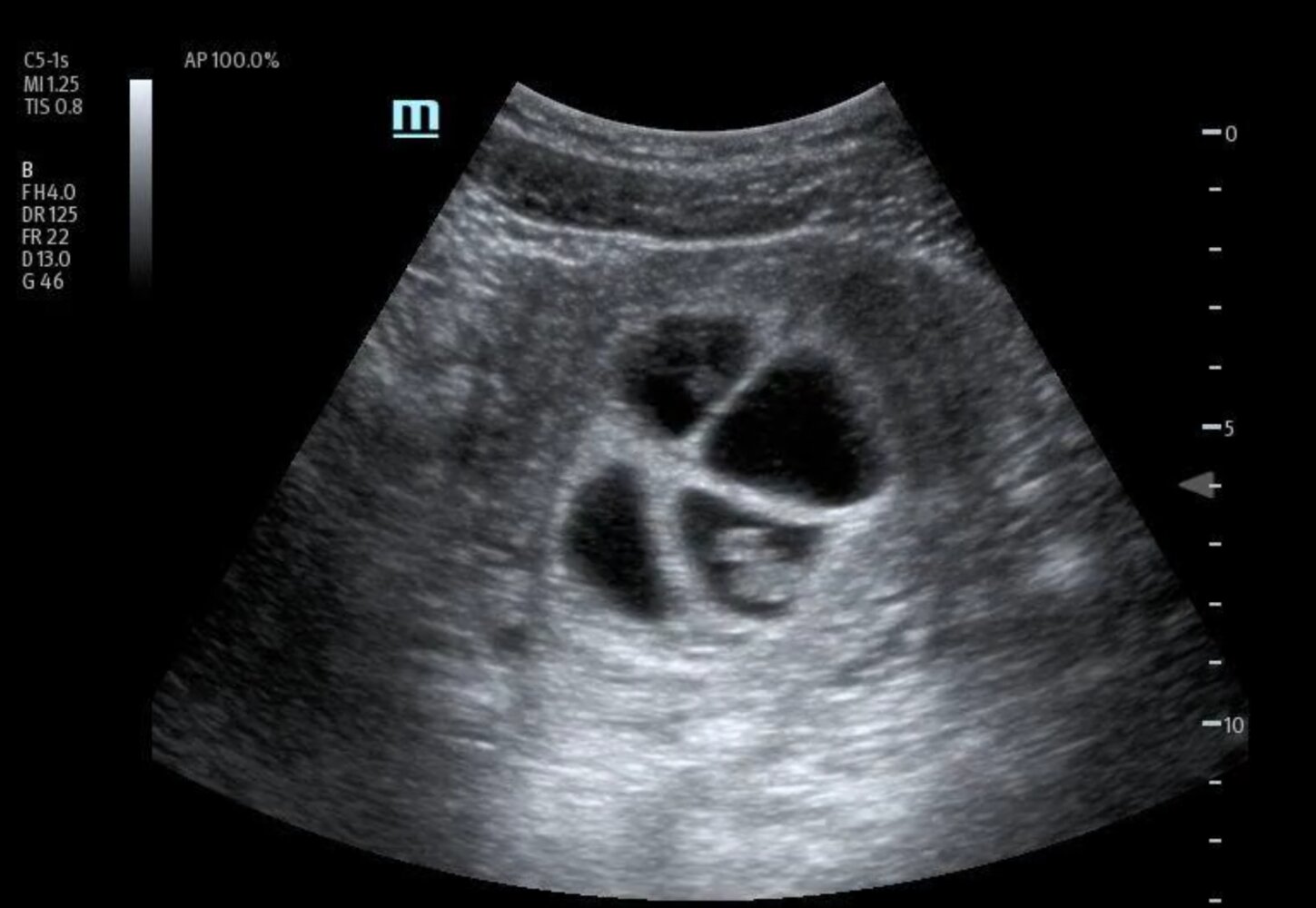
Ultrasound pelvis (transabdominal) of patient 1 month after in vitro fertilization (IVF)
Four intrauterine gestational sacs (yellow overlay) are seen within the gravid uterus. An embryo was identified within each sac during real time ultrasound evaluation, even though only one embryo (E) is fully visualized on this ultrasound image.
IVF increases the likelihood of a multiple gestation pregnancy.
Blue overlay: uterine wall
Source: “Fig 2, In: Optimizing Care for High-Risk Multiple Pregnancy with POCUS – A Case of Quadruplet Pregnancy Early Diagnosis” by Pimentel BV, Tsoutsoulas C, Lythgoe K, Myslik F, POCUS Journal, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

Transabdominal ultrasound of a pregnant patient
A dichorionic diamniotic twin pregnancy in the first trimester is seen. The triangular appearance of the chorion insinuating between layers of the intertwin membrane resembles the Greek letter lambda (λ; blue overlay). The lambda sign (also known as the “twin peak sign”) strongly suggests a dichorionic twin pregnancy.
Green overlay: placenta; red overlay: uterus; yellow overlay: fetus
© AMBOSS

Ultrasound pelvis (gravid uterus)
A thick inter-twin membrane containing both amnion and chorion separates adjacent twin embryos, with a triangular projection of chorion visible at the base of the membrane. The appearance produced by this projection of tissue has been termed the lambda sign (also the twin peak sign) because of its resemblance to the Greek symbol λ (blue overlay).
Although its absence is not sufficient to exclude dichorionicity, the lambda sign is a strong indicator of a dichorionic diamniotic pregnancy. In a monochorionic diamniotic pregancy, the inter-twin membrane may either terminate in a T configuration (T sign) or create a black triangular space with the uterine wall, sometimes termed the black lambda sign.
E: embryo; yellow overlay: uterine wall
Source: © IMPP

Ultrasound pelvis (gravid uterus)
Adjacent twins are separated by a thin membrane, which terminates at the placenta in a T configuration (T sign). This T sign is an indicator of a monochorionic diamniotic twin pregnancy.
A monochorionic diamniotic gestation may alternatively create a black triangular space (known as black lambda sign) at the uterine wall. This should not be confused with the triangular projection of chorion, which creates the lambda sign of a dichorionic pregnancy.
© AMBOSS

Ultrasound pelvis (15 weeks' gestation)
Twin pregnancy shows a single placenta. There is no intertwin membrane. The left twin is imaged in the coronal plane. The right twin is imaged in the sagittal plane.
A: amniotic fluid; H: head; P: placenta
Source: “Monoamniotic twins at 15 weeks” by Häggström, Mikael, WikiJournal of Medicine, licensed under CC0 1.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
Management
General principles [10][11][12]
- Multifetal gestations are high-risk pregnancies and require appropriate prenatal care and delivery planning.
- Prenatal care may require referral to various specialists (e.g., obstetrician specialized in multifetal gestations, maternal-fetal medicine, neonatology). [9][13]
- Management of preterm labor is often required.
Spontaneous labor before 37 weeks' gestation occurs in 60% of twin pregnancies. [10]
Prophylactic measures to prevent preterm delivery (e.g., bed rest, hospitalization, cervical cerclage, tocolytics) are not routinely recommended in the management of uncomplicated multifetal gestations. [11]
Prenatal care [11][12]
Modifications to routine prenatal care for multifetal pregnancies include the following:
- Counseling regarding the complications of multifetal gestation, including spontaneous loss of a fetus [11][12]
- Discussion of the challenges of prenatal genetic screening, e.g.:
- Typically less reliable in multifetal gestations
- Risk of sampling the wrong fetus with amniocentesis or chorionic villus sampling
-
Nondirective counseling on elective fetal termination ; [10][12][13]
- Multifetal reduction to improve outcomes for the remaining fetus or fetuses and birthing parent; typically performed in the first trimester
- Selective fetal termination if fetal anomalies are detected; typically performed in the second trimester
- Initiation of aspirin for preeclampsia prophylaxis
- Additional ultrasound monitoring includes regular assessment of: [9][10]
- Fetal biometry
- Umbilical artery Doppler velocimetry to assess for twin-to-twin transfusion syndrome in monochorionic pregnancies [10][14]
- Third-trimester antepartum fetal surveillance [15]
- Consideration of increased nutritional requirements for multifetal gestations (e.g., additional iron and folate supplementation) [12]
Monitor uncomplicated dichorionic gestations with ultrasound every 4 weeks after the second-trimester scan and uncomplicated monochorionic gestations every 2 weeks after 16 weeks' gestation. Increase frequency of scans for patients with complicated multifetal gestation. [9][10][11]
Delivery planning [10][11][12]
Early delivery of multifetal gestations is recommended, as perinatal mortality increases after 38 weeks' gestation. There is a paucity of data on the optimal timing and route of delivery of triplet and higher-order gestations.
- Consider antenatal corticosteroid therapy for fetal maturation and schedule delivery: [11]
- DCDA twins: 38 weeks' gestation
- MCDA twins: 34–38 weeks' gestation
- MCMA twins: 32–34 weeks' gestation
- Higher-order gestations: Optimal timing is unknown. [12]
-
Indications for cesarean delivery include: [11][12]
- Presenting fetus in breech position
- MCMA pregnancies
- Lack of obstetrician experience in delivering multifetal gestations
- See also “Management of high-risk pregnancies” and “Preterm labor and birth.”
Complications
Multifetal gestations are associated with increased risk of maternal and fetal and/or neonatal morbidity and mortality. Nearly all complications associated with normal pregnancies are more likely in multifetal gestations.
Maternal complications [11][12]
- Antenatal complications
- Hyperemesis gravidarum
- Gestational diabetes
- Hypertensive disorders of pregnancy
- Cervical incompetence
-
Intrapartum complications
- Preterm labor and birth (most common complication)
- Premature rupture of membranes [16]
- Prolonged first stage of labor , premature placental abruption after birth of the first fetus, prolapsed cord [17]
- Uterine atony
- Placenta previa [12][18]
Fetal complications [11][12]
- Intrauterine demise (spontaneous abortion)
- Vanishing twin syndrome: spontaneous fetal reduction; mostly occurs in the first trimester
- Twin-to-twin transfusion syndrome (in monochorionic pregnancies)
- Placental insufficiency, hypotrophy, and intrauterine malnutrition of at least one fetus
- Umbilical cord entanglement: can occur only in monoamniotic twin pregnancies
- Intrauterine growth restriction
- Congenital abnormalities
Neonatal or long-term complications [12]
- Complications of prematurity (e.g., neonatal respiratory distress syndrome, intraventricular hemorrhage)
- Cerebral palsy
- Blindness
- Deafness
We list the most important complications. The selection is not exhaustive.
Twin-to-twin transfusion syndrome
- Affects 10–15% of monochorionic twin pregnancies (twins that share the placenta)
- Predominantly affects MCDA pregnancies but may also affect MCMA pregnancies [14]
- Blood is continuously shunted from one twin to the other through vascular anastomoses on the shared placenta, posing a risk to both fetuses.
-
Recipient twin
- Polycythemia
- Hypervolemia
- Polyhydramnios in diamniotic pregnancies
-
Donor twin
- Anemia
- Fetal growth restriction
- Hypovolemia, dehydration (stuck twin or cocooned appearance)
- Oligohydramnios in diamniotic pregnancies
- Management options include: [14]
- Suspected twin-to-twin transfusion syndrome : fetal surveillance (at least weekly)
- Confirmed twin-to-twin transfusion syndrome
- Termination of significantly affected fetus or complete pregnancy
- Fetoscopic laser surgery of intertwin placental anastomoses at 16–26 weeks' gestation
Twin-to-twin transfusion syndrome may occur in monochorionic twins. [3]
References
- Sel G. "Multiple Pregnancies". Springer International Publishing. :81-85. (2019). ISBN: 9783030296681
- Yeaton‐Massey A, Sparks TN, Norton ME, Jelliffe‐Pawlowski L, Currier RJ. "Twin chorionicity and zygosity both vary with maternal age". Prenat Diagn. 41(9). :1074-1079. (2021)
- Jha P, Feldstein VA, Poder L, et al. "ACR Appropriateness Criteria® Multiple Gestations: 2024 Update". J Am Coll Radiol. 21(11). :S413-S432. (2024)
- Rathod S, Samal SK, Singh S, Swain S. "Quadruplet pregnancy following spontaneous conception: a rare case report". Journal of clinical and diagnostic research : JCDR. 9(4). :QD01-2. (2015)
- Gabbe SG, Niebyl JR, Galan HL, et al. "Obstetrics: Normal and Problem Pregnancies E-Book". Elsevier Health Sciences. (2016). ISBN: 9781455733958
- Ball JW, Dains JE, Flynn JA, Solomon BS, Stewart RW. "Seidel's Guide to Physical Examination - E-Book". Elsevier Health Sciences. (2021). ISBN: 9780323761857
- Póvoa A, Xavier P, Matias A, Blickstein I. "First trimester β-hCG and estradiol levels in singleton and twin pregnancies after assisted reproduction". J Perinat Med. 46(8). :853-856. (2017)
- Blickstein I, Keith LG. "Multiple Pregnancy". CRC Press. (2005). ISBN: 9781439804513
- Khalil A, Rodgers M, Baschat A, et al. "ISUOG Practice Guidelines: role of ultrasound in twin pregnancy". Ultrasound Obstet Gynecol. 47(2). :247-263. (2016)
- FIGO Working Group on Good Clinical Practice in Maternal-Fetal Medicine. "Good clinical practice advice: Management of twin pregnancy". Int J Gynaecol Obstet. 144(3). :330-337. (2019)
- ACOG. "ACOG: Multifetal Gestations: Twin, Triplet, and Higher-Order Multifetal Pregnancies". Obstet Gynecol. 137(6). :e145-e162. (2021)
- STONE J, KOHARI KS. "Higher-order Multiples". Clin Obstet Gynecol. 58(3). :668-675. (2015)
- ACOG. "Prediction and Prevention of Spontaneous Preterm Birth, Practice Bulletin 234". Obstet Gynecol. 138(2). :e65-e90. (2021)
- Leftwich HK, Zaki MN, Wilkins I, Hibbard JU. "Labor patterns in twin gestations". Am J Obstet Gynecol. 209(3). :254.e1-254.e5. (2013)
- Weis MA, Harper LM, Roehl KA, Odibo AO, Cahill AG. "Natural History of Placenta Previa in Twins". Obstet Gynecol. 120(4). :753-758. (2012)
- ACOG. "Committee Opinion No. 719 Summary: Multifetal Pregnancy Reduction (reaffirmed 2020)". Obstet Gynecol. 130(3). :670-671. (2017)
- Miller RS, Miller JL, Monson MA, et al. "Society for Maternal-Fetal Medicine Consult Series #72: Twin-twin transfusion syndrome and twin anemia-polycythemia sequence". Am J Obstet Gynecol. 231(4). :B16-B37. (2024)
- ACOG. "Indications for Outpatient Antenatal Fetal Surveillance (reaffirmed 2024)". Obstetrics & Gynecology. 137(6). :e177-e197. (2021)
- Bamberg C, Hecher K. "Update on twin-to-twin transfusion syndrome". Best Practice & Research Clinical Obstetrics & Gynaecology. 58. :55-65. (2019)