Summary
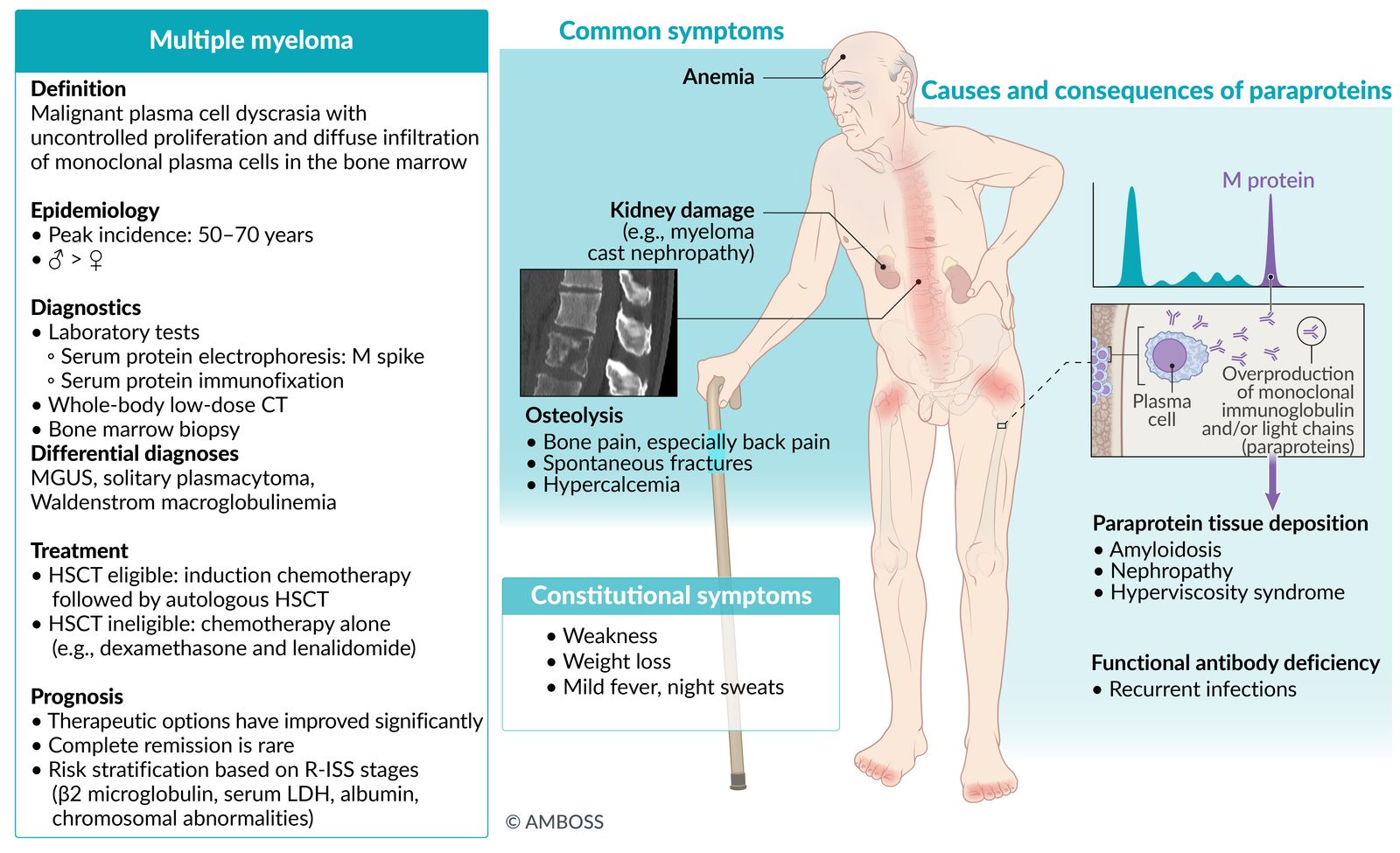
Multiple myeloma (MM) is a malignant plasma cell dyscrasia characterized by uncontrolled proliferation and diffuse infiltration of monoclonal plasma cells in the bone marrow. Malignant plasma cells produce monoclonal proteins (also known as M proteins or paraproteins) such as abnormal immunoglobulins (e.g., IgG, IgA) and free light chains (e.g., Bence Jones proteins). MM is more common in older adults and manifests with nonspecific symptoms (fever, night sweats, weight loss), symptoms of hypercalcemia, bone pain, and/or back pain. This condition is sometimes discovered incidentally in asymptomatic individuals. The proliferation of plasma cells suppresses normal bone marrow function, which may lead to anemia, bleeding, and/or infection. Plasma cell proliferation can also result in osteolysis and hypercalcemia. Renal complications are common, including myeloma cast nephropathy, light chain deposition disease, amyloid light-chain (AL) amyloidosis with renal involvement, and nephrocalcinosis. Most patients are treated with a combination of high-dose chemotherapy and autologous stem cell transplantation; patients with impaired functional status are treated with chemotherapy alone. While advancements in treatment regimens have resulted in improved patient outcomes, most patients with MM eventually relapse.

© AMBOSS
Definitions
- Plasma cell dyscrasia: a group of conditions characterized by the abnormal proliferation of the same type (=monoclonal) of a plasma cell that may also secrete a monoclonal immunoglobulin and/or immunoglobulin fragment (e.g., light chain)
- Solitary plasmacytoma: an early-stage plasma cell dyscrasia characterized by a single lesion that affects bones (solitary plasmacytoma of bone) or soft tissue (solitary extramedullary plasmacytoma), or in rare cases multiple solitary lesions in soft tissue, bone or both (multiple solitary plasmacytoma)
- Multiple myeloma: a malignant plasma cell dyscrasia characterized by uncontrolled proliferation and the diffuse infiltration of monoclonal plasma cells in the bone marrow
Epidemiology
- Sex: : ♂ > ♀ (3:2) [1]
- Peak incidence: : 50–70 years [1]
Epidemiological data refers to the US, unless otherwise specified.
Classification
-
Based on immunoglobulin type [2]
- IgG and IgA: typical multiple myeloma; majority of patients
- Bence Jones myeloma (free light chains excreted in urine): 15–20% of multiple myelomas
- IgD, IgE, and IgM: very rare subtypes of multiple myelomas
Pathophysiology
-
Neoplastic proliferation of plasma cells
- Bone marrow infiltration by malignant plasma cells → suppression of hematopoiesis → leukopenia, thrombocytopenia, anemia
- Cell proliferation → pro-osteoclastogenic factors (e.g., TNF-α, IL-1, RANK-L) → osteolytic lesions → hypercalcemia
-
Overproduction of monoclonal immunoglobulin and/or light chains → dysproteinemia (a state of pathologically increased synthesis of immunoglobulins and/or their subunits) → kidney damage (e.g., myeloma cast nephropathy) and/or paraprotein tissue deposition (may cause amyloidosis) [3][4]
- Nonfunctioning antibodies → functional antibody deficiency
- ↑ Serum viscosity → hyperviscosity syndrome
© AMBOSS
Clinical features
- Often asymptomatic
- Mild fever, night sweats, weakness, and weight loss
- Bone pain, especially back pain (most common symptom)
- Symptoms of hypercalcemia
- Spontaneous fractures
- Increased risk of infection
- Increased risk of petechial bleeding
- Foamy urine (caused by Bence Jones proteins in urine)
Enlarged lymph nodes are not a typical finding.
Diagnosis
Approach [5][6][7]
- Obtain a minimum diagnostic workup.
- Initial laboratory studies (e.g., CBC, CMP, urinalysis)
- Myeloma biomarkers (e.g., serum and urine protein electrophoresis, free light chain assay, LDH)
- Imaging to assess for bone lesions (e.g., whole-body low-dose CT scan)
- Refer to an oncologist for diagnostic confirmation via bone marrow biopsy.
- Evaluate for diagnostic criteria of multiple myeloma.
- Use the Revised International Staging System (R-ISS) to categorize the disease state.
- Consider differential diagnoses (e.g., other plasma cell dyscrasias; , other causes of hypercalcemia or bone lesions).
Evaluation of a patient with suspected multiple myeloma (e.g., a patient with CRAB criteria) should include CBC, CMP, immunoglobulin studies, LDH, β2 microglobulin, bone imaging, and a bone marrow biopsy.
Diagnostic criteria
| International Myeloma Working Group diagnostic criteria for multiple myeloma [8] | ||
|---|---|---|
| Criteria | Description | |
| Histopathology |
|
|
| Myeloma defining events | End-organ damage (CRAB criteria) |
|
| Biomarkers of malignancy |
|
|
| ||
CRAB criteria for organ damage due to a plasma cell disorder: Calcium increased, Renal insufficiency, Anemia, Bone lesions
Evaluation for biomarkers of malignancy may allow for diagnosis and treatment of multiple myeloma before end-organ damage has occurred.
Laboratory tests [7][8]
Routine studies
-
CBC (with differential and peripheral smear)
- Anemia, thrombocytopenia, and/or leukopenia
- Decreased reticulocyte count
- Rouleaux formation
-
CMP
- Increased creatinine
- Hypercalcemia
- Elevated total protein with paraprotein (gamma) gap
- Inflammatory markers: Increased ESR
- Urinalysis: : may be negative for protein

Myeloma biomarkers
-
Blood tests
-
Immunoglobulin studies (common initial tests)
- Serum protein electrophoresis (SPEP): presence of M protein (M spike)
- Serum protein immunofixation: monoclonal gammopathy
- Serum free light chain assay (SFLC): increased κ or λ light chains, increased SFLC involved:uninvolved ratio
- Quantitative immunoglobulin levels (IgA, IgG, IgM) can help determine if proteinemia on SPEP is monoclonal.
- Increased β2 microglobulin [9]
- Increased LDH
-
Immunoglobulin studies (common initial tests)
-
Urine studies
-
Urine protein electrophoresis (UPEP) with immunofixation
- Bence Jones proteins: monoclonal immunoglobulin light chains produced by neoplastic cells
- Bence Jones proteinuria is suggestive of plasma cell disorders (e.g., multiple myeloma, Waldenstrom macroglobulinemia).
- 24-hour urine protein and creatinine
-
Urine protein electrophoresis (UPEP) with immunofixation

Additional testing
Further evaluation for differential diagnoses (guided by clinical features) may include:
- Biochemical evaluation of bone disease (e.g., PTH, vitamin D levels)
- Biochemical evaluation for fatigue and unexplained weight loss (e.g., thyroid function test, diabetes mellitus screening)
- Diagnostic workup for polyneuropathy (e.g., vitamin B12 levels, nerve conduction studies)
- Thrombophilia workup (e.g., testing for hereditary thrombophilia or acquired thrombophilias)
Imaging studies [5][6][10]
Whole-body low-dose CT (WBLDCT)
-
Indications
- First-line test for baseline and follow-up bone surveillance
- More sensitive than x-rays in detecting focal lesions
- Used to guide radiotherapy, biopsies, and surgery
-
Findings
- Detection of osteolysis and osteopenia
- Identification of vertebral instability and fracture risk
- Bone marrow plasma cell infiltration in long bones
Skeletal survey
Low sensitivity; no longer considered the best initial test
-
Indications
- Obtain if other more sensitive techniques are not available.
- May be used to evaluate for skull and rib lesions, which are not well detected by WBLDCT or MRI.
-
Findings
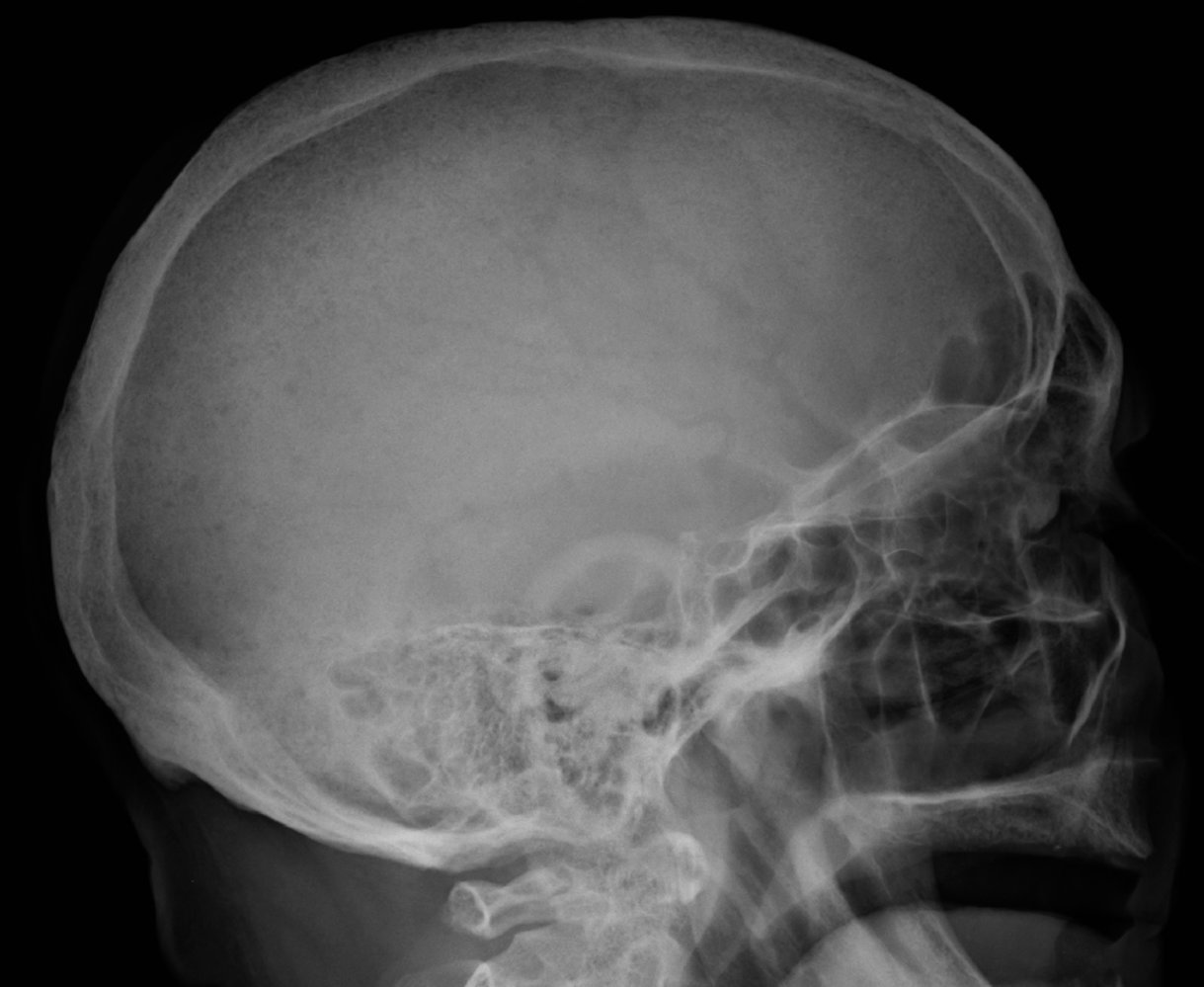
- Multiple lytic lesions ("punched-out" holes), e.g., in the skull
- Plasmacytoma





Ancillary tests
-
Indications
- Inconclusive WBLDCT
- Alternative option for baseline and follow-up bone surveillance
-
Modalities
- MRI (whole-body or spine and pelvis): highest sensitivity for diffuse bone marrow involvement
- FDG-PET/CT scan: highest sensitivity for extramedullary disease and active lytic bone lesions
Bone marrow biopsy
- Indication: : confirmatory test indicated for all patients with suspected multiple myeloma
-
Fluorescence in situ hybridization (FISH): used for staging of multiple myeloma [11]
-
High-risk chromosomal abnormalities in multiple myeloma
- Translocations: t(4;14), t(14;16), t(14;20)
- Others: deletion 17p, gain 1q, p53 mutation
- Standard risk abnormalities: t(11;14), t(6;14), trisomies
-
High-risk chromosomal abnormalities in multiple myeloma
-
Cytology: clusters of plasma cells
- Mildly organized monoclonal cells
- Perinuclear lucent zone
- Clockface nuclei: Chromatin in the periphery of the nucleus resembles a cartwheel or clock face arrangement.
- Intracytoplasmic crystalline inclusion bodies containing IgG

")


X-ray skull (left: lateral view; right: PA view) of a child with Langerhans cell histiocytosis (LCH)
Well-defined lytic lesions without sclerotic margins are seen in the frontoparietal and high-parietal regions of the calvarium (example indicated by green overlay).
Various conditions can cause lytic skull lesions. LCH lesions are typically rounded or ovoid in shape and have nonsclerotic well-defined margins. Edges may be beveled as a result of uneven destruction of the inner and outer tables. Coalescence of enlarging lesions can produce a geographic appearance.
Source: “Fig 2, In: Infiltrating the Heart and Kidney: A Rare Pediatric Case of Multisystem Langerhans Cell Histiocytosis from Pakistan” by Mahmood S, Raza M, Nusrat K, Marsia S, Abbas A, Cureus, licensed under CC BY 3.0. Modifications: Removed white arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
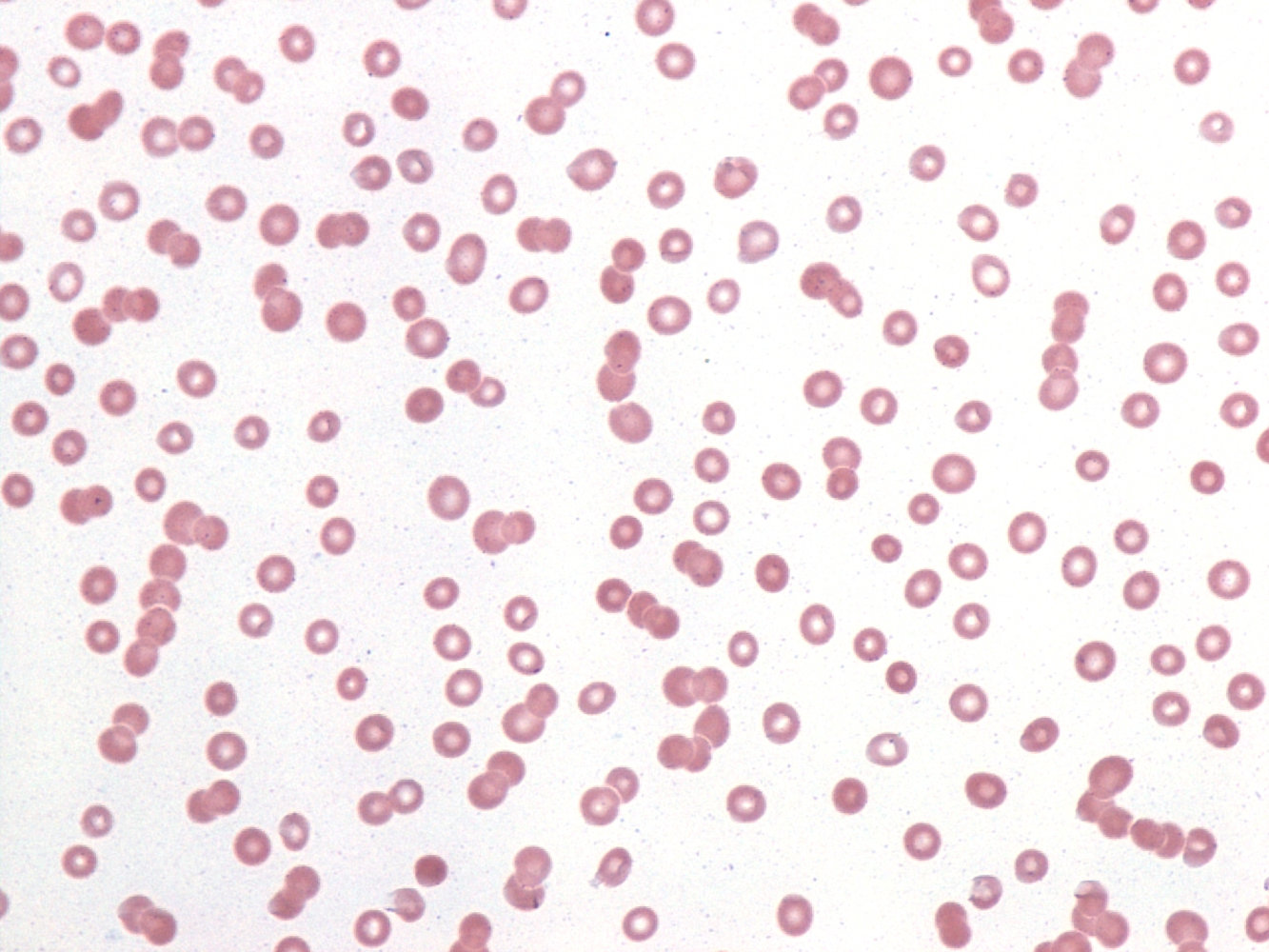
Photomicrograph of a peripheral blood smear
Red blood cells are aggregated in chains and appear like stacked coins (rouleaux formation (illustration); examples indicated by blue overlay).
This phenomenon occurs in disorders with increased serum proteins (e.g., multiple myeloma and Waldenstrom macroglobulinemia).
Source: “Rouleaux” by Gabriel Caponetti, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
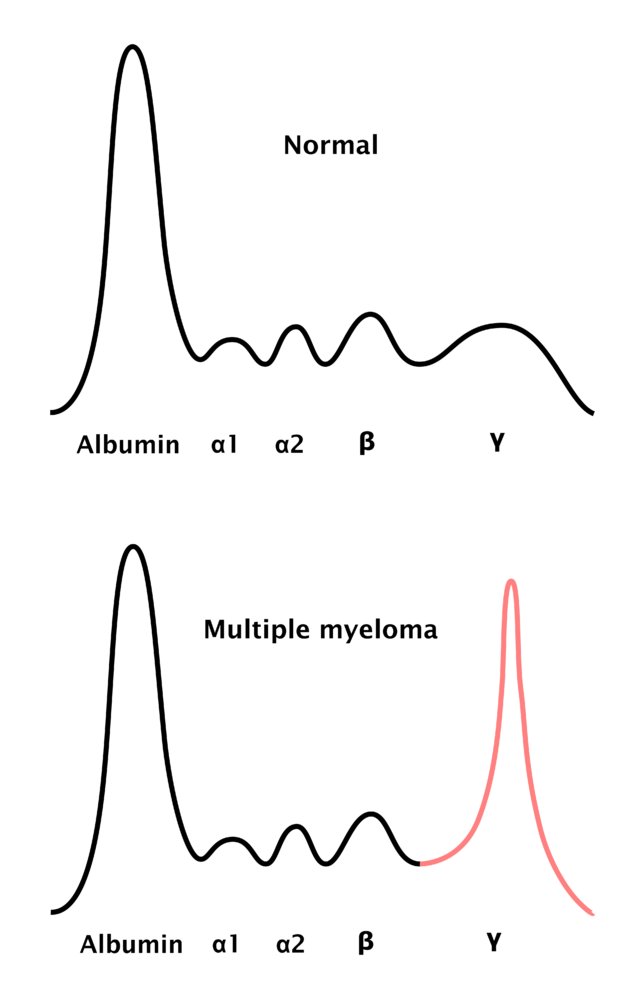
Pathological protein electrophoresis in multiple myeloma: the monoclonal antibodies cause a peak in the gamma-globulin zone of the electrophoresis, which is termed M protein (also M component, myeloma protein, spike protein, and paraprotein).
© AMBOSS

X-ray of head and neck (lateral view): multiple osteolytic regions throughout the skull bones (areas of decreased radiodensity)
These are typical findings in multiple myeloma.
Source: © IMPP

X-ray skull (lateral view) of a patient with a history of multiple myeloma
Multiple punched-out lytic lesions (examples indicated by green overlay) are visible. This appearance is termed “raindrop sign” from the resemblance of these lesions to raindrops splashing upon hitting a surface.
An expanded differential of lucent skull lesions includes osteoporosis of aging, hyperparathyroidism, metastatic disease, anemias (e.g., sickle cell and thalassemia), and the lytic phase of Paget disease.
Source: © IMPP
X-ray skull (lateral view) of a patient with a history of multiple myeloma
Numerous very small, well-circumscribed (punched-out) lytic lesions without sclerotic margins are seen (examples indicated by arrowheads).
Source: “MMPlainSkull” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}

X-ray knee (AP oblique and lateral views) of a patient with a history of POEMS syndrome
An expansile lesion (green overlay) in the metaphysis of the distal femur shows a mixed, predominantly lytic pattern. The lesion involves both trabecular and cortical bone and is accompanied by some periosteal reaction (red overlay).
Biopsy confirmed a plasmacytoma. Of note, plasmacytomas in POEMS syndrome are typically sclerotic lesions.
Source: "Plasmocytome lytique tiers inf femur", Grook Da Oger, Wikimedia Commons licensed under Public Domain
{kind=link}

X-ray forearm (oblique view) of a patient with multiple myeloma
Numerous small lytic lesions are present throughout the radius, ulna, humerus, and bones of the wrist and hand (examples indicated by green overlay) producing a moth-eaten pattern of destruction (illustration). Some lesions have well-defined margins (punched-out appearance) while others have indistinct margins. Pathologic fractures of the ulna are also seen (arrows).
Source: “Plasmozytom multiple Osteolysen Unterarm” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
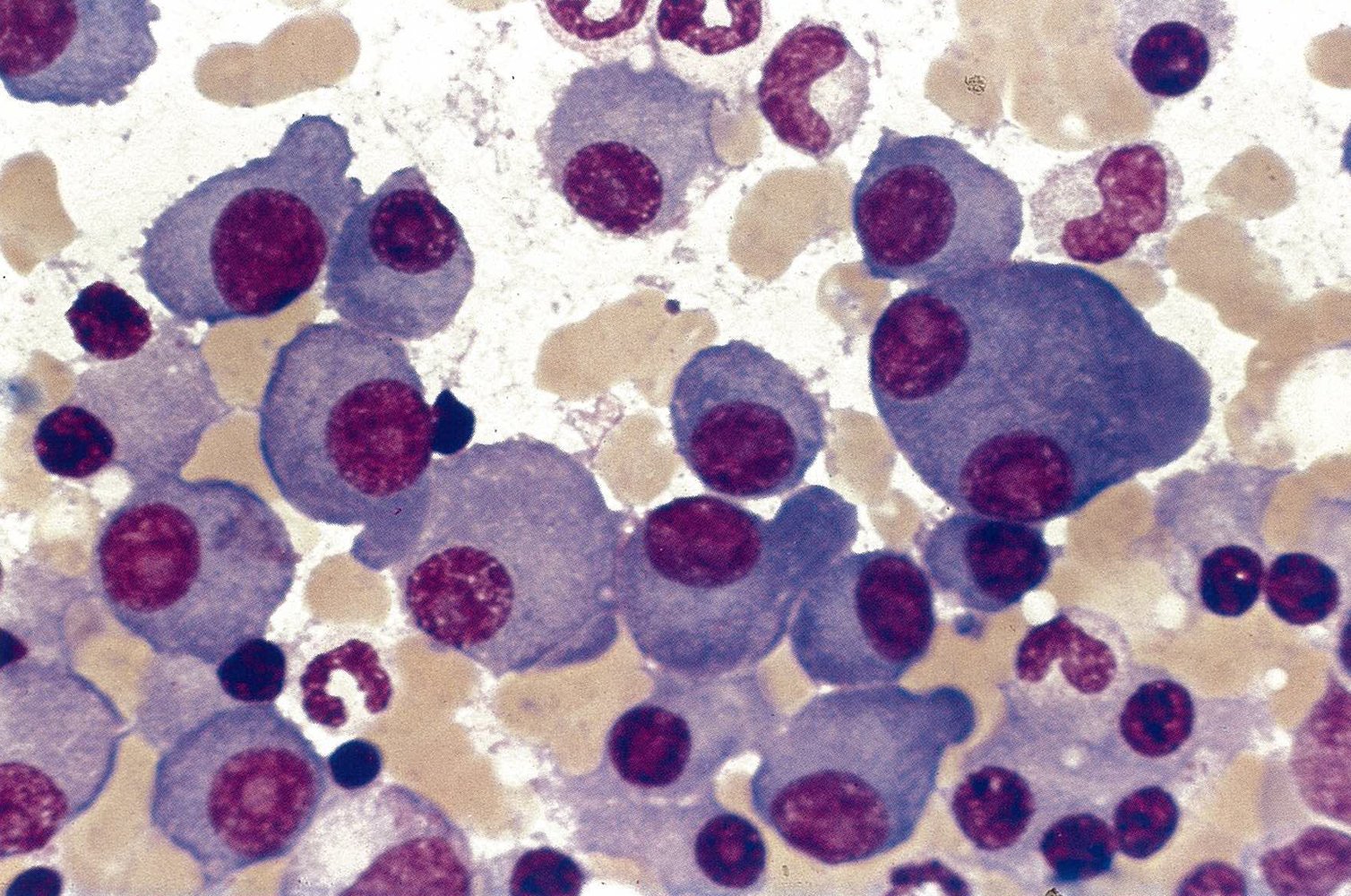
Bone marrow aspirate smear (May-Gruenwald stain; high magnification)
An increased density of plasma cells is visible. Plasma cells possess a round eccentric nucleus (example indicated by yellow hatched overlay) with clock-face chromatin (example indicated by white circle) and a perinuclear halo (perinuclear hof; example indicated by white overlay). Other cell types present include neutrophils (example indicated by blue overlay), lymphocytes (examples indicated by black arrowheads), and erythrocytes (example indicated by blue hatched overlay).
Additionally, the plasma cells in this specimen show features of atypia, e.g., multinucleated cells (example indicated by yellow outline), prominent nucleoli (example indicated by yellow arrowhead), and enlarged as well as irregularly shaped cytoplasm (example indicated by yellow overlay).
The diagnosis of multiple myeloma requires the lesion to consist of monoclonal plasma cells, which is confirmed by kappa or lambda light chain restriction.
Source: © IMPP
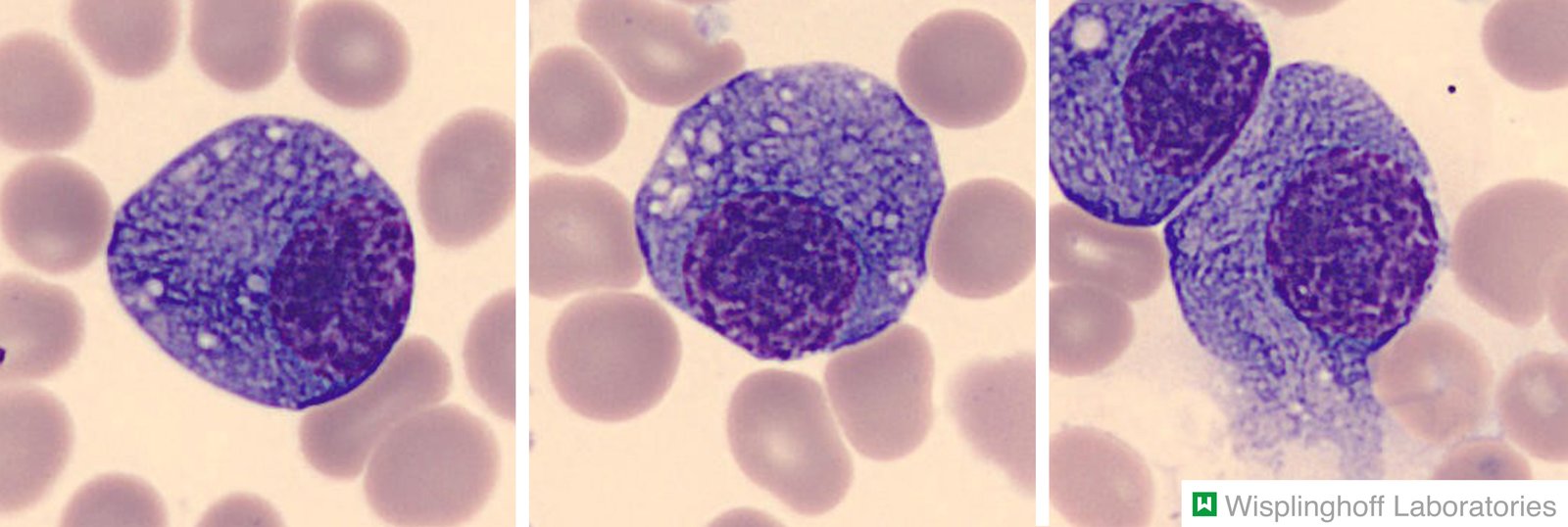
Photomicrograph of a bone marrow specimen (H&E stain)
Plasma cells are large cells that typically have an eccentric nucleus (hatched overlay) with dense, clumped chromatin. The cytoplasm is deeply basophilic due to the abundance of rough endoplasmic reticulum required for the synthesis of antibodies.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: Prof. Dr. Karl-Anton Kreuzer, Facharzt für Innere Medizin, Hämatologie und Onkologie
Staging
Revised International Staging System (R-ISS) [12]
The R-ISS is currently the most commonly used staging system.
| Revised International Staging System for multiple myeloma [12] | ||
|---|---|---|
| Stage | Laboratory features | 5-year overall survival rate |
| I |
|
|
| II |
|
|
| III |
|
|
The R-ISS for multiple myeloma incorporates LDH levels and FISH in addition to the variables used in the International Staging System (i.e., β2 microglobulin and albumin), which improves its ability to stratify risk and determine the prognosis of patients with newly diagnosed multiple myeloma. [12]
International Staging System (ISS) [13]
| International Staging System for multiple myeloma [12] | ||
|---|---|---|
| Stage | Laboratory features | Median survival from diagnosis |
| I | β2 microglobulin < 3.5 mg/L AND albumin ≥ 3.5 g/dL | > 5 years |
| II | Not stage I or stage III | 3–4 years |
| III | β2 microglobulin ≥ 5.5 mg/L | 2–3 years |
Durie-Salmon staging system
| Durie-Salmon staging system for multiple myeloma [14] | |||
|---|---|---|---|
| Stage I: All of the following must be present. | Stage II | Stage III: ≥ 1 of the following must be present. | |
| Blood: hemoglobin | > 10 g/dL | Not stage I or stage III | < 8.5 g/dL |
| Blood: serum calcium | Normal (< 2.8 mmol/L) | > 3 mmol/L | |
| Urine: monoclonal Ig | Low concentration | High concentration | |
| X-ray: bones | One (maximum) solitary osteolytic lesion | Several advanced osteolytic lesions | |
Subclassification
| |||
Management
General principles [5][6][7][15]
-
Choice of treatment based on:
- Risk stratification (e.g., R-ISS stage)
- Eligibility for autologous hematopoietic stem cell transplantation (HSCT)
- HSCT eligible: induction chemotherapy followed by autologous HSCT
- HSCT ineligible: chemotherapy alone (e.g., dexamethasone and lenalidomide)
- Goal of therapy: the highest level of remission with the best quality of life
- Prevention and management of complications (e.g., VTE, AKI, bone lesions) is an integral part of treatment.
Refer all patients to a transplant center to determine eligibility for stem cell transplantation.
Stem cell transplantation [5][6][11]
- Eligibility: based on performance status (e.g., ECOG, Karnofsky score) and comorbidities
-
Process typically includes the following:
- Preparation
- Induction chemotherapy (3–4 cycles)
- Hematopoietic stem cell collection (from peripheral blood)
- Conditioning regimen
- Autologous HSCT
- Maintenance chemotherapy or consolidation therapy (at least 2 cycles) as an alternative
- Preparation
Neither advanced age nor poor renal function are absolute contraindications for autologous stem cell transplantation.
Autologous stem cell transplantation improves median overall survival by ∼12 months but is not curative. [11]
Chemotherapy [5]
There is no expert consensus regarding the optimal chemotherapeutic regimen or number of cycles.
-
Transplant eligible patients
-
Induction therapy
- Standard risk: (e.g., R-ISS stage I or II) immunomodulator PLUS proteasome inhibitor PLUS steroid (e.g., VRd)
- High risk (e.g., R-ISS stage III): additional cancer immunotherapy (e.g., D-VRd)
- Conditioning regimen: high-dose melphalan
-
Maintenance therapy
- Standard risk: lenalidomide monotherapy; bortezomib monotherapy as an alternative
- High risk: proteasome inhibitor with or without lenalidomide
-
Induction therapy
- Transplant ineligible patients: immunomodulators and/or proteasome inhibitors PLUS a steroid (e.g., Rd, VRd)
| Overview of chemotherapeutic agents commonly used for multiple myeloma [5] | |
|---|---|
| Medication class | Common agents |
| Proteasome inhibitors |
|
| Immunomodulators |
|
| Cancer immunotherapy |
|
| Steroids |
|
| Alkylators |
|
| For the mechanism of action and common adverse effects, see “Chemotherapeutic agents.” | |
Choice of regimen depends on transplant eligibility, disease risk factors (e.g., R-ISS stage, cytogenetics), patient factors (e.g., frailty, comorbidities, functional status), and patient preferences (e.g., length and quality of life).
Monitoring [5][11][16]
-
Response to treatment
- Defined based on International Myeloma Working Group (IMWG) criteria [16]
- Categories range from stringent complete response to progressive disease
-
Clinical relapse
- Defined as recurrence or worsening of myeloma-defining events (e.g., CRAB) after clinical improvement [11]
- Management (i.e., salvage/delayed autologous HSCT and/or chemotherapy) should be individualized.
- After a relapse, therapy may be continued until the disease progresses.
Nearly all patients will relapse; the average time to first relapse is ∼ 3–4 years after initial diagnosis.
Prevention of complications [11][17]
-
Infection prophylaxis
-
Recommended immunizations [18]
- Influenza
- Recombinant zoster
- Haemophilus influenzae
- Pneumococcal vaccines
- Bacteremia and sepsis prophylaxis during the first two cycles of chemotherapy; e.g., levofloxacin (off label) [11][19]
- PCP prophylaxis for patients receiving high-dose corticosteroids; e.g., low‑dose TMP/SMX
- Herpes zoster prophylaxis for patients receiving proteasome inhibitors; e.g., valacyclovir (off label) or acyclovir (off label) [20][21]
-
Recommended immunizations [18]
- Prevention of acute kidney injury: e.g., avoid nephrotoxic medications, maintain adequate hydration status
-
VTE prophylaxis
- Indicated for all patients, especially those receiving immunomodulatory agents (e.g., lenalidomide)
- The preferred agent (e.g., aspirin, direct oral anticoagulant, LMWH, warfarin) depends on the patient's individual risk of thrombosis.
Management of complications [11]
Management should be provided under specialist guidance.
| Overview of the management of complications of multiple myeloma | ||
|---|---|---|
| Complication | Management options | |
| Bone disease [18][22] |
|
|
| Renal disease [23] |
|
|
| Peripheral neuropathy [17] |
|
|
| Hematological complications [11][17][18] | Anemia |
|
| Neutropenia |
|
|
| Thrombosis |
|
|
Treatment of pain (e.g., due to compressive myelopathy or pathological fractures) includes low-dose radiotherapy, high-dose corticosteroids, and invasive therapy (e.g., vertebroplasty, balloon kyphoplasty).
All patients with active multiple myeloma should be treated with bisphosphonates (unless contraindicated), regardless of the presence or absence of imaging findings of bone disease related to multiple myeloma.
Bisphosphonate therapy and denosumab both increase the risk of osteonecrosis of the jaw. Ensure patients undergo a comprehensive dental evaluation and any necessary dental procedures before starting therapy for bone disease. [22]
Differential diagnoses
Overview of plasma cell dyscrasias (PCDs)
Multiple myeloma should be differentiated from other plasma cell dyscrasias.
| Diagnostic criteria for plasma cell dyscrasias associated with multiple myeloma[8][18][24] | |
|---|---|
| Plasma cell dyscrasia | Diagnostic criteria |
| Smoldering multiple myeloma |
|
| Solitary plasmacytoma |
|
| Plasma cell leukemia |
|
| POEMS syndrome |
|
| Monoclonal gammopathy of undetermined significance (MGUS) |
|
| Waldenstrom macroglobulinemia [25][26] |
|
POEMS syndrome: Polyneuropathy, Organomegaly, Endocrinopathy, Monoclonal plasma cell proliferative disorders, Skin changes
Monoclonal gammopathy of undetermined significance (MGUS) [27][28]
Definition
Characterized by complete or incomplete monoclonal immunoglobulins (of any class) detectable in patient serum without accompanying clinical symptoms
Epidemiology
- Prevalence: ∼ 3% in general population ≥ 50 years of age [29]
- The most common type of plasma cell dyscrasia (PCD)
Classification
- Non-IgM MGUS (IgG, IgA, IgD MGUS): most common form of MGUS (∼ 55% of cases)
- IgM MGUS: ∼ 15% of cases
- Light-chain MGUS (LC-MGUS)
Risk stratification [30]
Patients can be stratified into the following categories according to their risk of progression to multiple myeloma or related malignancy.
-
Low-risk MGUS includes all of the following:
- IgG subtype
- M-protein concentration < 1.5 g/dL
- Normal SFLC ratio
- Moderate to high-risk MGUS: any feature not considered low-risk
Diagnostics [30][31][32]
-
General considerations
- Usually diagnosed as an incidental finding
- Universal screening is not routinely recommended.
- Diagnostic criteria may help establish a diagnosis; see “Diagnostic criteria for plasma cell dyscrasias.”
-
Initial studies
- CBC, serum creatinine, and calcium
- SPEP and UPEP with immunofixation
- Quantitative immunoglobulin assessment
- SFLC assay
-
Additional studies: usually reserved for patients with moderate to high risk of progression to malignancy or if there is evidence of transformation to another plasma cell dyscrasia (i.e., M-protein concentration ≥ 3 g/dL, findings of a severe PCD) [31]
- Bone marrow biopsy
-
Skeletal imaging
- WBLDCT (modality of choice)
- A skeletal survey is indicated if CT is not available.
- Whole-body MRI is indicated in patients with inconclusive CT results.
Management
- Management is usually expectant.
-
Long-term follow up: Monitor for progression to lymphoplasmacytic malignancy.
- Studies: CBC, serum calcium and creatinine, SPEP, and SFLC assays
- Cadence: 6 months after diagnosis and then every 1–3 years.
Monitor patients with MGUS for progression to lymphoplasmacytic malignancy.
Complications
-
Multiple myeloma
- Transformation of MGUS into multiple myeloma occurs in approx. 1% of cases per year [31]
- Typically arises from non-IgM MGUS
- Light chain amyloidosis: can occur with all forms of MGUS
- Waldenstrom macroglobulinemia: only arises from IgM MGUS
- Increased risk of thrombosis (thromboprophylaxis is usually not required) and developing osteoporosis (bone densitometry should be performed at the time of diagnosis)
- Lymphoma
Waldenstrom macroglobulinemia[26]
Definition
A type of non-Hodgkin lymphoma associated with abnormal production of monoclonal IgM antibodies
Epidemiology
Mostly occurs in older adults
Clinical features
-
Peripheral neuropathy
- Extremities are involved first with progressive, proximal, symmetrical spread
- Presents with paresthesias and weakness (sensory and motor nerve involvement)
- Impaired platelet function → hemorrhagic diathesis with petechial bleeding
- Normochromic anemia
-
Formation of cold agglutinins (IgM) with hyperviscosity syndrome
- Raynaud phenomenon
- Impaired acral blood flow
- Cerebral venous thrombosis
- Impaired vision (e.g., blurry vision)
-
Fundoscopic exam
- Retinal hemorrhages
- Dilated, engorged, and segmented retinal veins
- Impaired hearing
- Headaches
- Impaired renal and liver function
- Lymph node enlargement possible
- Constitutional symptoms (e.g., fatigue)
Diagnostics [26]
Diagnostic criteria may help establish a diagnosis; see “Diagnostic criteria for plasma cell dyscrasias.”
-
Routine studies
- CBC, CMP
- Increased ESR, uric acid, LDH, and alkaline phosphatase
- Serum β2 microglobulin level
-
Immunoglobulin studies
- SPEP and UPEP with immunofixation
- Quantitative serum immunoglobulin levels
- Bone marrow biopsy and aspirate: ≥ 10% abnormal plasma cells with Dutcher bodies (periodic acid-Schiff positive, cytoplasmic inclusions of IgM deposits that invaginate into the nucleus) [33][34]
- Imaging studies: Consider a contrast-enhanced CT scan of the chest, abdomen, and pelvis.
-
Additional studies for suspected hyperviscosity syndrome
- Serum viscosity measurement
- Ophthalmologic evaluation
Overproduction of monoclonal IgM suggests Waldenstrom macroglobulinemia rather than multiple myeloma.
Treatment
Usually reserved for symptomatic patients
- Targeted treatment: anti-CD20 antibodies (e.g., rituximab), Bruton tyrosine kinase inhibitors (e.g., ibrutinib), purine nucleoside analogs (fludarabine and cladribine), alkylating agents (e.g., cyclophosphamide)
- Hyperviscosity syndrome: plasmapheresis
Prognosis
Good, as it is a type of indolent lymphoma
POEMS syndrome
See “Diagnostic criteria for plasma cell dyscrasias” for details.
- Definition: a rare plasma cell disorder that causes chronic overproduction of proinflammatory cytokines
-
Clinical features include:
- Polyneuropathy
- Organomegaly
- Endocrinopathy
- Increased production of monoclonal plasma proteins
- Skin changes
The differential diagnoses listed here are not exhaustive.
Complications
Renal disease
-
Dysproteinemia-associated kidney disease [3][35]
-
Myeloma cast nephropathy (i.e., myeloma kidney): most common cause of renal injury and renal failure in patients with multiple myeloma
- Clinical features: oliguria, peripheral edema, dyspnea
- Pathophysiology: excessive production and filtration of light chains into the urine → precipitation of light chains in renal tubules → tubular obstruction
- Diagnosis: markedly positive urine sulfosalicylic acid test and/or urine protein electrophoresis
- May progress to end-stage renal disease (ESRD)
- Monoclonal immunoglobulin deposition disease (MIDD)
- Light chain deposition disease (LCDD)
- Heavy chain deposition disease (HCDD)
- Light and heavy chain deposition disease (LHCDD)
-
Type I cryoglobulinemia
- An immune-mediated disorder characterized by the deposition of monoclonal immunoglobulins (IgG and IgM) within blood vessels.
- Most commonly associated with protein-secreting monoclonal gammopathies, including monoclonal gammopathy of undetermined significance, Waldenstrom macroglobulinemia, and multiple myeloma.
- Type II cryoglobulinemia
- Immunotactoid glomerulopathy
- Proliferative glomerulonephritis with monoclonal immunoglobulin deposits (PGNMID)
- Monoclonal gammopathy-associated C3 glomerulopathy
- Light-chain proximal tubulopathy
- Monoclonal IgM-mediated kidney disease
- Monotypic fibrillary glomerulonephritis
-
Myeloma cast nephropathy (i.e., myeloma kidney): most common cause of renal injury and renal failure in patients with multiple myeloma
- Hypercalcemia-associated renal damage: leads to hypercalciuria and nephrocalcinosis
- Analgesic nephropathy: caused by long-term intake of NSAIDs for bone pain

Systemic manifestations
- AL amyloidosis: Light chains can accumulate as amyloids and may lead to restrictive cardiomyopathy, renal insufficiency, macroglossia, and malabsorption syndromes.
-
Infections
- Increased risk due to immunodeficiency (nonfunctional immunoglobulins) and side effects of medications
- Major cause of death in patients with multiple myeloma
-
Secondary plasma cell leukemia [36]
- Leukemic course secondary to multiple myeloma
- Diffuse spreading of abnormal cells and distribution of large amounts of plasma cells into the circulatory system
- Rare; occurs in 2–3% of cases
- Hypercalcemic crisis: Osteolysis is associated with chronically elevated calcium levels, which can result in a hypercalcemic crisis.
We list the most important complications. The selection is not exhaustive.
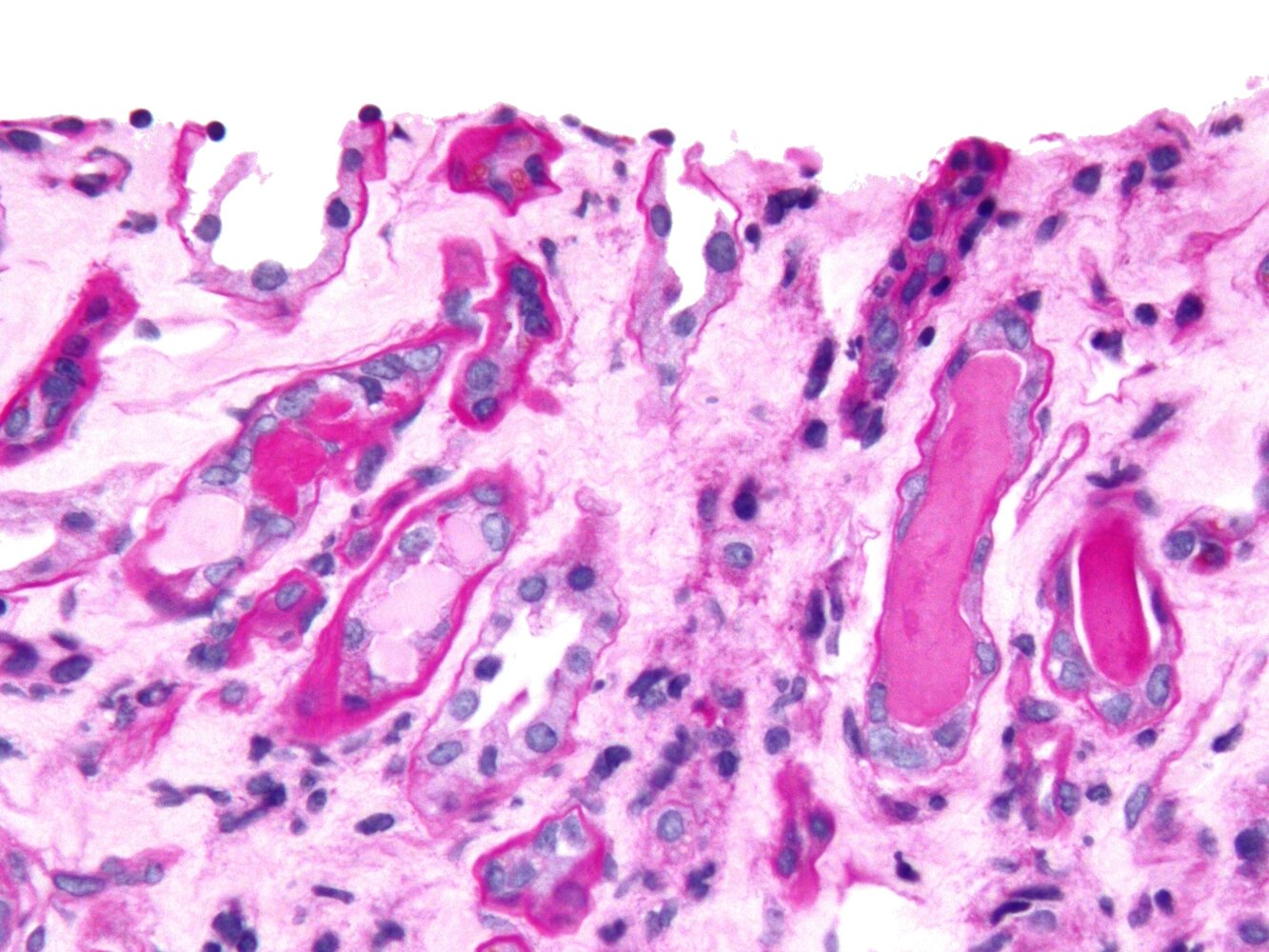
Photomicrograph of a kidney biopsy specimen (PAS stain; very high magnification)
Several dark-pink stained hyaline casts (PAS positive, examples indicated by blue overlay) and light-pink stained Myeloma casts (PAS negative, examples indicated by yellow overlay) can be seen. Myeloma casts are caused by deposition of immunoglobulin light chains, leading to renal tubule obstruction.
Source: “Cast nephropathy - 2 cropped - very high mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Prognosis
- The course of disease and prognosis are highly variable.
- Therapeutic options have improved significantly. However, complete remission is rare.
- Poor prognostic factors include
- Advanced stage according to the R-ISS staging system
- Advanced age
- ↑ β2 microglobulin
- ↓ Serum albumin
- ↑ CRP
- ↑ LDH
External Resources
References
- Kyle RA, Gertz MA, Witzig TE, et al. "Review of 1027 Patients With Newly Diagnosed Multiple Myeloma". Mayo Clinic Proceedings. 78(1). :21-33. (2003)
- Fonseca R, Bergsagel PL, Drach J, et al. "International Myeloma Working Group molecular classification of multiple myeloma: spotlight review". Leukemia. 23(12). :2210-2221. (2009)
- Mikhael J, Ismaila N, Cheung MC, et al. "Treatment of Multiple Myeloma: ASCO and CCO Joint Clinical Practice Guideline". J Clin Oncol. 37(14). :1228-1263. (2019)
- Dimopoulos MA, Moreau P, Terpos E, et al. "Multiple myeloma: EHA-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†". Ann. Oncol. 32(3). :309-322. (2021)
- Cowan AJ, Green DJ, Kwok M, et al. "Diagnosis and Management of Multiple Myeloma". JAMA. 327(5). :464. (2022)
- Rajkumar SV, Dimopoulos MA, Palumbo A, et al. "International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma". Lancet Oncol. 15(12). :e538-e548. (2014)
- Cooper EH, Plesner T. "Beta-2-microglobulin review: Its relevance in clinical oncology". Med Pediatr Oncol. 8(4). :323-334. (1980)
- Zamagni E, Tacchetti P, Cavo M. "Imaging in multiple myeloma: How? When?". Blood. 133(7). :644-651. (2019)
- Rajkumar SV, Kumar S. "Multiple myeloma current treatment algorithms". Blood Cancer Journal. 10(9). (2020)
- Mateos MV, Kumar S, Dimopoulos MA, et al. "International Myeloma Working Group risk stratification model for smoldering multiple myeloma (SMM)". Blood Cancer J. 10(10). (2020)
- Michels TC, Petersen KE. "Multiple Myeloma: Diagnosis and Treatment.". Am Fam Physician. 95(6). :373-383. (2017)
- Meletios A. Dimopoulos, Robert A. Kyle, Athanasios Anagnostopoulos, Steven P. Treon. "Diagnosis and Management of Waldenstrom's Macroglobulinemia". Journal of Clinical Oncology. 23(7). :1564-1577. (2005)
- Gertz MA. "Waldenström macroglobulinemia: 2021 update on diagnosis, risk stratification, and management". Am J Hematol. 96(2). :258-269. (2021)
- Therneau TM, Kyle RA, Melton LJ, et al. "Incidence of monoclonal gammopathy of undetermined significance and estimation of duration before first clinical recognition". Mayo Clin Proc. 87(11). :1071-1079. (2012)
- Korde N, Kristinsson SY, Landgren O. "Monoclonal gammopathy of undetermined significance (MGUS) and smoldering multiple myeloma (SMM): novel biological insights and development of early treatment strategies". Blood. 117(21). :5573-5581. (2011)
- Rajkumar SV, Kyle RA, Buadi FK. "Advances in the Diagnosis, Classification, Risk Stratification, and Management of Monoclonal Gammopathy of Undetermined Significance: Implications for Recategorizing Disease Entities in the Presence of Evolving Scientific Evidence". Mayo Clinic Proceedings. 85(10). :945-948. (2010)
- Kyle RA, Durie BGM, et al. "Monoclonal gammopathy of undetermined significance (MGUS) and smoldering (asymptomatic) multiple myeloma: IMWG consensus perspectives risk factors for progression and guidelines for monitoring and management". Leukemia. 24(6). :1121-1127. (2010)
- Go RS, Rajkumar SV. "How I manage monoclonal gammopathy of undetermined significance". Blood. 131(2). :163-173. (2018)
- Dispenzieri A, Kyle R, et al. "International Myeloma Working Group guidelines for serum-free light chain analysis in multiple myeloma and related disorders". Leukemia. 23(2). :215-224. (2008)
- Bain BJ. "Dutcher bodies". Am J Hematol. 84(9). :589-589. (2009)
- Han JH, Cho SR. "An old misconception: Dutcher bodies are intranuclear inclusions in plasma cells?". Leukemia & Lymphoma. 60(1). :265-267. (2018)
- Faiman BM, Mangan P, Spong J, Tariman JD. "Renal Complications in Multiple Myeloma and Related Disorders". Clin J Oncol Nurs. 15. :66-76. (2011)
- Hogan JJ, Alexander MP, Leung N. "Dysproteinemia and the Kidney: Core Curriculum 2019". American Journal of Kidney Diseases. 74(6). :822-836. (2019)
- Rotaru I, Găman G, Dumitrescu D, Foarfă C. "Secondary plasma cell leukemia". Rom J Morphol Embryol. 53(4). :1073-1076. (2012)
- Markowitz GS. "Dysproteinemia and the Kidney". Adv Anat Pathol. 11(1). :49-63. (2004)
- Palumbo A, Avet-Loiseau H, Oliva S, et al. "Revised International Staging System for Multiple Myeloma: A Report From International Myeloma Working Group". J Clin Oncol. 33(26). :2863-2869. (2015)
- Lu J, Lu J, Liu A, et al. "The applicability of the International Staging System in chinese patients with multiple myeloma receiving Bortezomib or Thalidomide-based regimens as induction therapy: A multicenter analysis". BioMed Res Int. 2015. :1-7. (2015)
- Durie BG, Salmon SE. "A clinical staging system for multiple myeloma. Correlation of measured myeloma cell mass with presenting clinical features, response to treatment, and survival.". Cancer. 36(3). :842-54. (1975)
- Rajkumar SV. "Multiple myeloma: 2022 update on diagnosis, risk stratification, and management". Am J Hematol. 97(8). :1086-1107. (2022)
- Durie BGM, Harousseau JL, et al. "International uniform response criteria for multiple myeloma". Leukemia. 20(9). :1467-1473. (2006)
- Palumbo A, Rajkumar SV, San Miguel JF, et al. "International Myeloma Working Group Consensus Statement for the Management, Treatment, and Supportive Care of Patients With Myeloma Not Eligible for Standard Autologous Stem-Cell Transplantation". J Clin Oncol. 32(6). :587-600. (2014)
- Drayson MT, Bowcock S, Planche T, et al. "Levofloxacin prophylaxis in patients with newly diagnosed myeloma (TEAMM): a multicentre, double-blind, placebo-controlled, randomised, phase 3 trial". Lancet Oncol. 20(12). :1760-1772. (2019)
- Fukushima T, Sato T, Nakamura T, et al. "Daily 500 mg valacyclovir is effective for prevention of Varicella zoster virus reactivation in patients with multiple myeloma treated with bortezomib.". Anticancer Res. 32(12). :5437-40. (2012)
- Minarik J, Pika T, Bacovsky J, Langova K, Scudla V. "Low-dose acyclovir prophylaxis for bortezomib-induced herpes zoster in multiple myeloma patients". Br J Haematol. 159(1). :111-113. (2012)
- Terpos E, Zamagni E, Lentzsch S, et al. "Treatment of multiple myeloma-related bone disease: recommendations from the Bone Working Group of the International Myeloma Working Group". Lancet Oncol. 22(3). :e119-e130. (2021)
- Dimopoulos MA, Sonneveld P, Leung N, et al. "International Myeloma Working Group Recommendations for the Diagnosis and Management of Myeloma-Related Renal Impairment". J Clin Oncol. 34(13). :1544-1557. (2016)