Summary
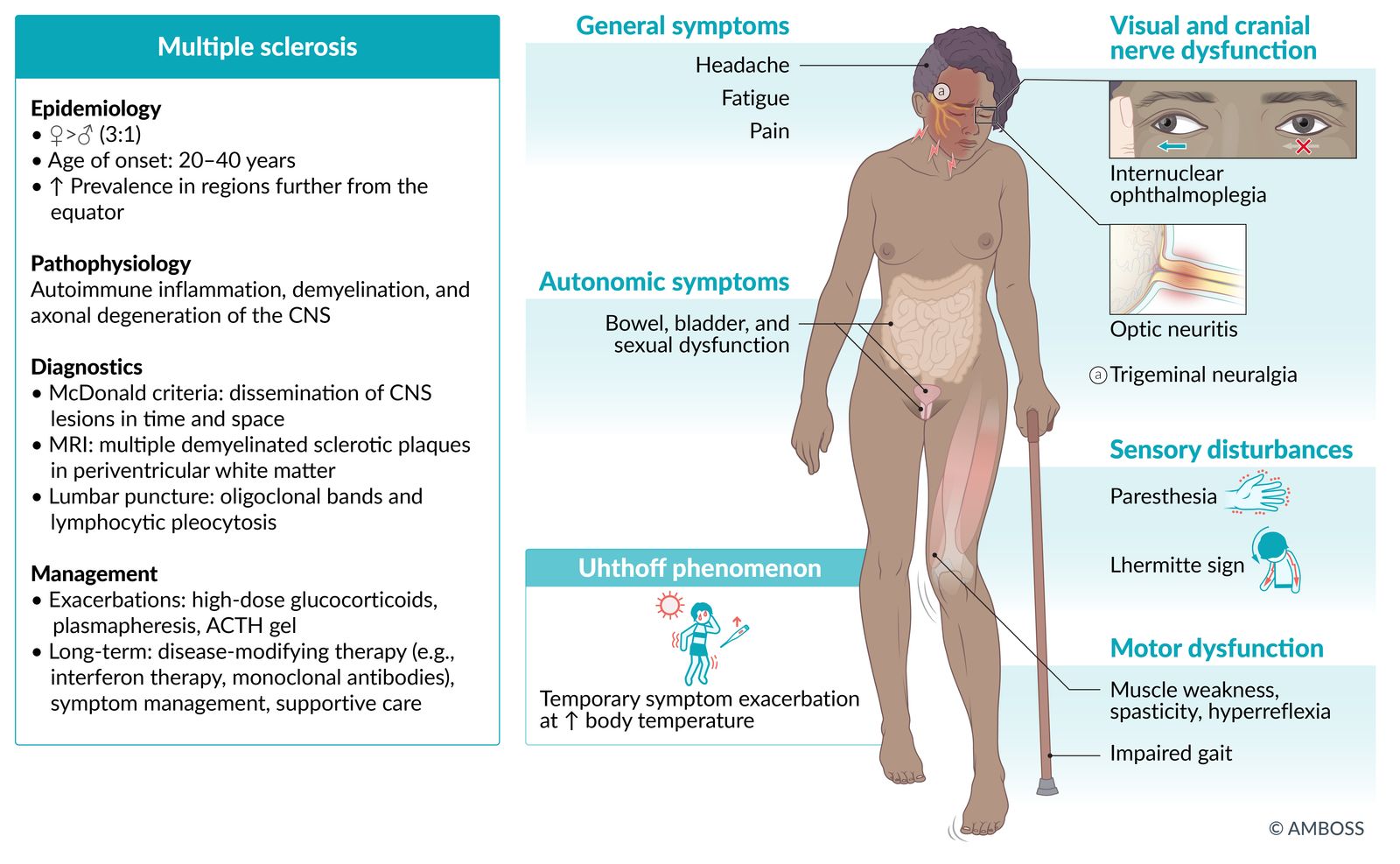
Multiple sclerosis (MS) is a chronic degenerative disease of the CNS characterized by demyelination and axonal degeneration in the brain and spinal cord, which are caused by an immune-mediated inflammatory process. The prevalence of MS is higher among women and people in temperate regions such as Europe and North America. Impaired vision (due to retrobulbar neuritis) is usually the first manifestation of MS; other neurological deficits appear as the disease progresses. The most common clinical course is characterized by exacerbations followed by periods of complete or incomplete remission. Diagnosis is made using clinical and MRI findings to identify the dissemination of CNS lesions in time and space. Characteristic MRI findings are demyelinated sclerotic plaques primarily located in white matter. Differential diagnoses of MS include other chronic demyelinating diseases and neurological infections (e.g., borreliosis, neurosyphilis). Acute exacerbations of MS are usually treated with high-dose glucocorticoids. Between exacerbations, patients may be treated with disease-modifying drugs (e.g., interferon beta, glatiramer acetate, natalizumab). There is currently no definitive treatment for MS.

© AMBOSS
Epidemiology
- Sex: : ♀ > ♂ (3:1) [1]
- Age of onset: : 20–40 years of age [2]
- Ethnicity: ↑ prevalence among the white and black population [3]
- Prevalence: 50-300 per 100 000 people (greater among people who live farther from the equator) [2]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
The etiology of multiple sclerosis is unclear; it is believed to develop in genetically predisposed people who have been exposed to certain environmental factors.
-
Genetic predisposition
- Presence of HLA-DRB1*15 allele increases the risk of MS. [4]
- Presence of HLA-A*02 allele appears to be protective against MS. [4]
- 35% disease concordance among monozygotic twins [5]
- 3–4% disease concordance among first-degree relatives [5]
-
Environmental risk factors [2][6]
- Low vitamin D levels (insufficient intake, decreased exposure to UV radiation)
- Cigarette smoking
- Pathogens: EBV, HHV 6
- Obesity early in life
Classification
Definitions [7][8]
-
MS exacerbation
- New symptoms or significant worsening of symptoms caused by CNS demyelination that last at least 24 hours and are not accompanied by fever or infection
- Also referred to as an attack, relapse, or flare
- Remission: a period of recovery after an exacerbation during which clinical symptoms resolve completely or almost completely
- Pseudorelapse: recurrence or significant worsening of existing symptoms due to stressors (e.g., infection, heat)
-
Radiologically isolated syndrome (RIS) [9]
- The presence of demyelinating lesions characteristic of MS in an asymptomatic individual
- Not considered an MS phenotype but may progress to MS
-
Clinically isolated syndrome (CIS)
- A single episode of neurological symptoms resulting from CNS demyelination
- A second episode of such symptoms increases the likelihood that the symptoms are not clinically isolated and that the patient meets the diagnostic criteria for MS.
-
Diffuse cerebral sclerosis (Schilder disease) [10][11]
- A rare inflammatory demyelinating CNS condition that affects children and young adults
- Large areas of demyelination lead to various neurological deficits and psychological changes.
Clinical course [7][12][13]
| Clinical phenotypes of multiple sclerosis [7][12][13] | ||
|---|---|---|
| Phenotype | Characteristics | Frequency |
| Relapsing-remitting MS (RR-MS) |
|
|
| Secondary progressive MS(SP-MS) |
|
|
| Primary progressive MS (PP-MS) |
|
|
")
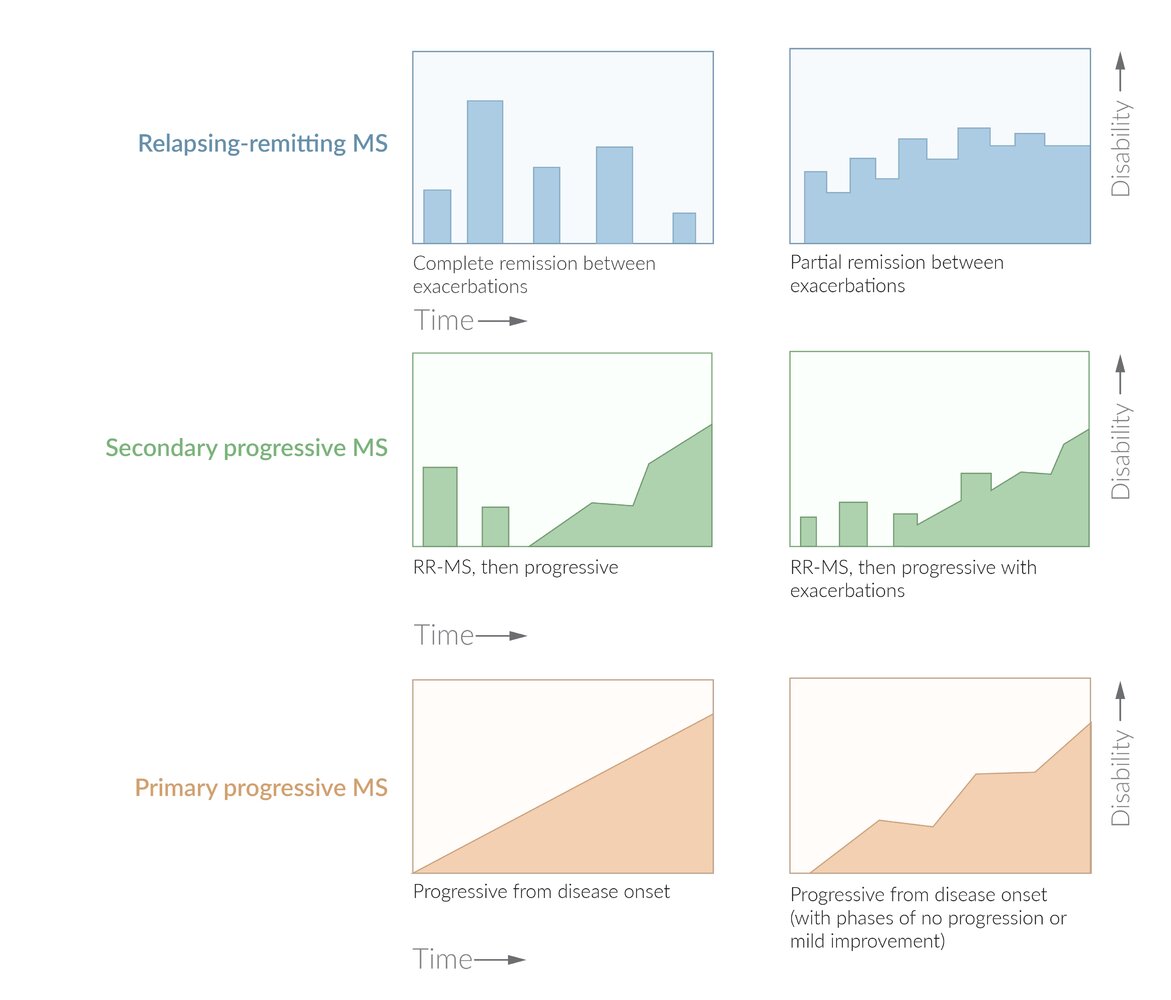
Relapsing-remitting (RR) MS (∼ 90 % of patients): either full recovery between exacerbations (left column) or increasing residual disability with each exacerbation (right column).
Secondary progressive (SP) MS: > 50 % of patients initially presenting with relapsing-remitting MS later develop a pattern of continuous progression (left column), which may also include further exacerbations (right column).
Primary progressive(PP) MS (∼ 10 % of patients): continuous worsening of symptoms from disease onset (left column), but may include phases of no progression or even mild clinical improvement (less pronounced than in relapsing-remitting MS; right column). Exacerbations may also occur (not depicted).
© AMBOSS
Pathophysiology
- Pathophysiology of MS is characterized by autoimmune inflammation, demyelination, and axonal degeneration.
- Most commonly accepted theory: Activation of autoreactive T-lymphocytes; → inflammatory processes → focal demyelination with partial preservation of axons (acute plaques) → loss of axons and atrophy of oligodendrocytes (chronic plaques) → gliosis → inadequate remyelination
-
B-lymphocyte dysfunction: The following suggests that B-lymphocytes play a role in the pathogenesis of MS, although the exact mechanism of their involvement is unclear.
- Anti-CD20 agents (ocrelizumab, ofatumumab, rituximab) are effective in preventing exacerbations.
- Presence of tertiary lymphoid organs in the meninges of individuals with secondary progressive MS [14]
- Intrathecal synthesis of IgG (oligoclonal bands; see “Diagnostics” section for more information)
- Progressive phenotypes (forms) of MS are characterized by [15]
- Chronic inflammation that occurs with an intact blood-brain barrier and is driven by immune cells compartmentalized in the leptomeninges and perivascular spaces
- Accelerated compared to relapsing-remitting phenotype brain atrophy
Clinical features
- Constitutional symptoms: fatigue, headache
-
Optic neuritis ; [16][17][18]
- Most often the earliest manifestation
- Typically unilateral
- Can be painful
- Impaired vision and color blindness
- Relative afferent pupillary defect (Marcus Gunn pupil)
-
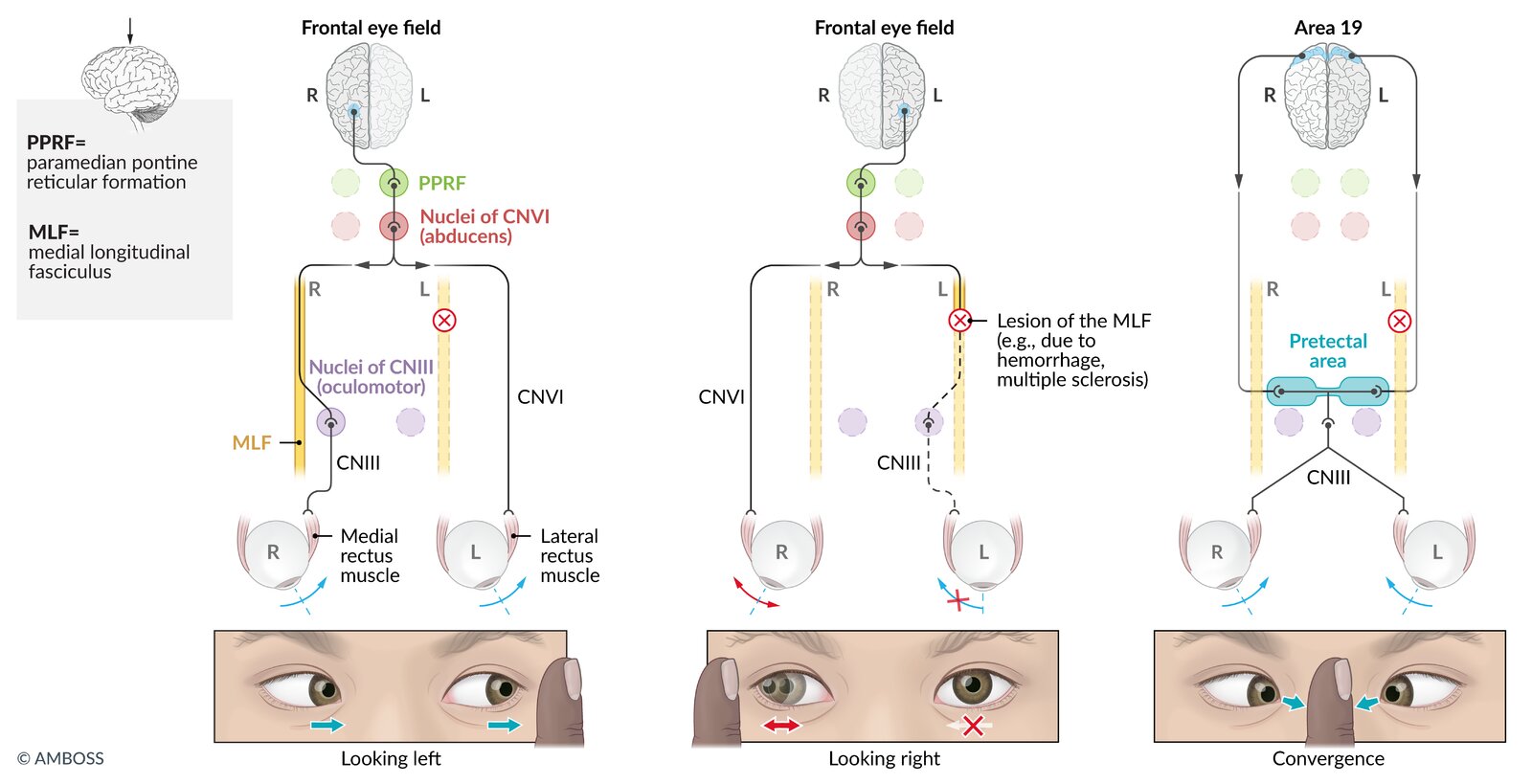
Internuclear ophthalmoplegia (INO) as a result of a lesion in the medial longitudinal fasciculus (MLF)
- Ipsilateral medial rectus weakness but an intact convergence reflex
- Disconjugate, lateral gaze nystagmus in the contralateral eye
- More frequently bilateral than unilateral
-
Demyelination of spinal cord tracts
- Lhermitte sign: a shooting electric sensation that travels down the spine upon flexion of the neck
- Pyramidal tract lesion: upper motor neuron weakness, spasticity, hyperreflexia, positive Babinski sign, impaired gait
- Dorsal spinal column lesion: loss of vibration and fine-touch sensation, numbness, paresthesias, sensory ataxia usually involving the trunk or one or more limbs
- Neuropathic pain (see “Central neuropathic pain”)
- Absent abdominal reflex [19]
- Cerebellar involvement: poor postural control, imbalance, gait dysfunction, Charcot neurological triad: of scanning speech, nystagmus, and intention tremors
-
Transverse myelitis
- Asymmetric paraplegia, unilateral sensory loss, bladder dysfunction
- Partial transverse myelitis is a common early manifestation of MS, causing asymmetric neurologic dysfunction below the lesion.
-
Cranial nerve palsies: diplopia, facial palsy, trigeminal neuralgia (can be bilateral) ; [20][21]
- Trigeminal neuralgia (TN) typically manifests unilaterally.
- Bilateral TN should raise concern for MS, especially in younger patients.
- Autonomic dysfunction: bowel and bladder neurogenic disorders (e.g., urinary incontinence), impaired sexual function
- Changes in mental state: depression, emotional changes, memory deficits, impaired concentration
- Uhthoff phenomenon: a reversible exacerbation of neurological symptoms following an increase in body temperature, e.g., physical exertion, a warm bath, or fever
Fundoscopy is normal in 60% of cases of optic neuritis. Neither the patient nor the doctor are able to see anything.
Uhthoff phenomenon triggered by a viral infection may mimic an exacerbation of MS.
MS is a chronic condition that typically manifests in a relapsing-remitting form characterized by episodic CNS dysfunction (exacerbations) with at least partial recovery between episodes.



© AMBOSS
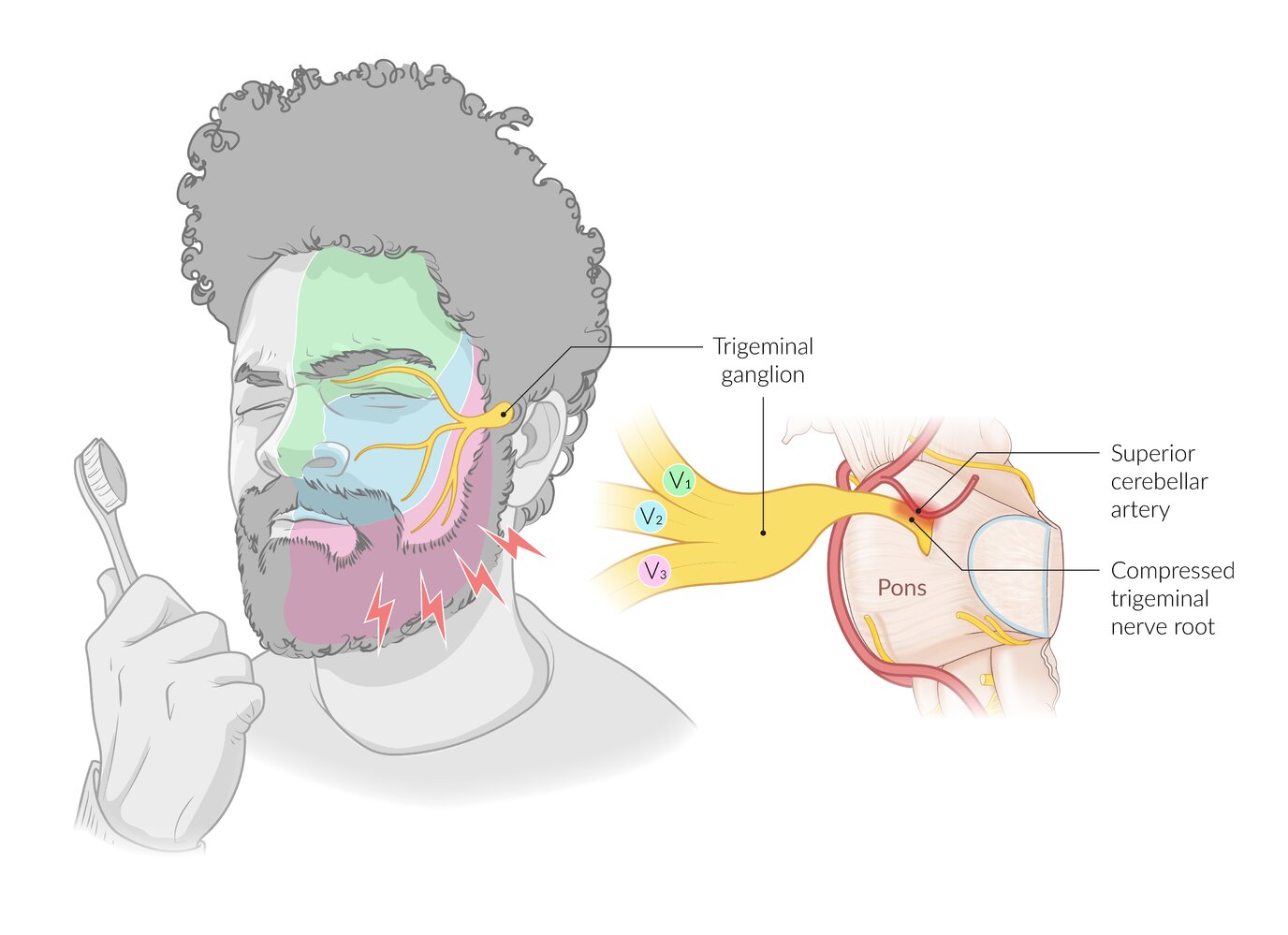
Trigeminal neuralgia is characterized by attacks of facial pain in the area of one or more branches of the trigeminal nerve. Classical trigeminal neuralgia is caused by neurovascular compression, most often by an aberrant loop of a neighboring artery (usually the superior cerebellar artery). The pain is typically very severe in intensity, has a sharp, stabbing quality, and lasts several seconds. Attacks can occur without provocation but are sometimes triggered by stimuli such as brushing teeth.
© AMBOSS
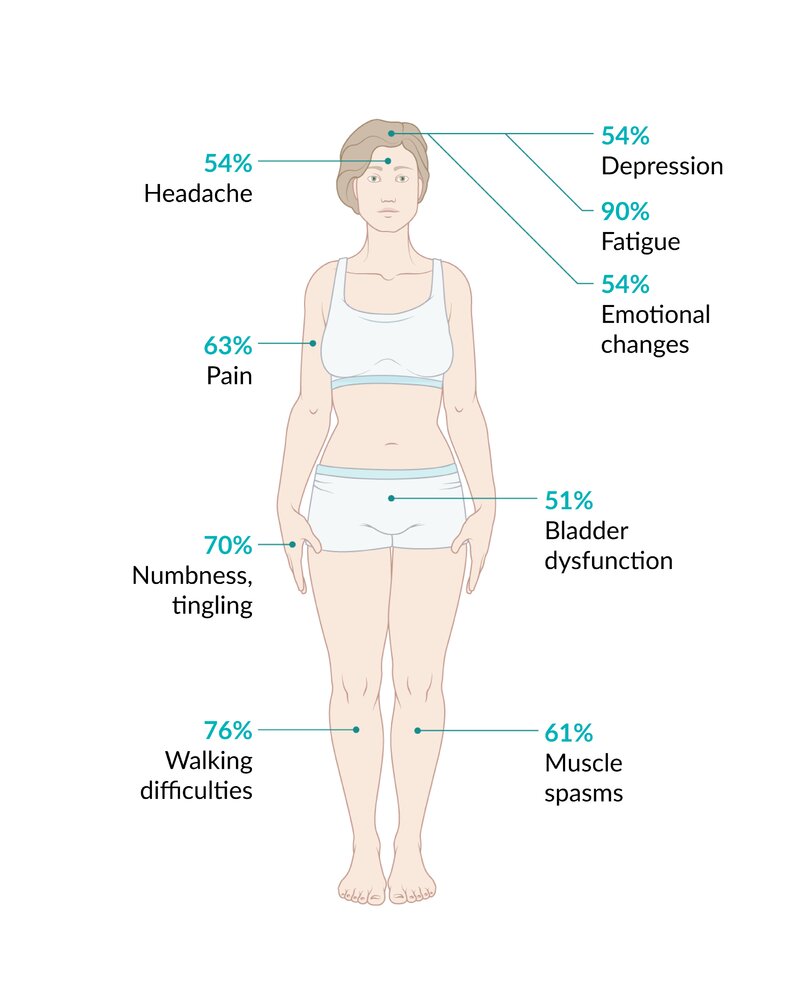
The percentage indicates how frequently a specific finding is observed or reported in patients with multiple sclerosis.
© AMBOSS
Diagnosis
General principles [7][22]
- Diagnosis of MS depends on a combination of clinical findings (e.g., optic neuritis, Lhermitte sign, sensory abnormalities, cerebellar signs), imaging, and laboratory results.
- Consider early specialist (i.e., neurology) consultation for patients with history and clinical features suggestive of MS.
-
The McDonald Criteria for both DIT and DIS must both be met to confirm a diagnosis of MS: [7]
- Dissemination in time (DIT): the appearance of new CNS lesions over time that can be confirmed clinically, with imaging, or with CSF analysis
- Dissemination in space (DIS): the presence of lesions in different regions of the CNS that can be confirmed clinically or in MRI
- In some cases, electrophysiological, CSF, and laboratory studies may be necessary to support the diagnosis and exclude differential diagnoses. [23]

Clinical evidence or MRI findings consistent with the presence of CNS lesions that are disseminated in both time and space confirm the diagnosis of MS.
Imaging for MS [7][13]
MRI is the imaging study of choice for the diagnosis and monitoring of MS.
-
Indications
- MRI brain (with and without gadolinium): all patients with suspected MS
- MRI spinal cord (with and without gadolinium): to increase diagnostic yield (e.g., in patients with nondiagnostic brain MRI or symptoms of partial myelitis ) [24]
-
Typical findings on MRI
-
Multiple sclerotic plaques (most commonly found in the periventricular white matter) ; with finger-like radial extensions (Dawson fingers) related to demyelination and reactive gliosis [13][23]
- In T1: hypointense or isointense lesions (i.e., black hole lesions) due to severe demyelination and axonal destruction [25]
- In T2 and FLAIR: hyperintense lesions, typically round or oval in shape and found in both hemispheres [26]
- Contrast-enhancement of active lesions; usually resolves after 2–8 weeks [26]
-
Multiple sclerotic plaques (most commonly found in the periventricular white matter) ; with finger-like radial extensions (Dawson fingers) related to demyelination and reactive gliosis [13][23]


")
")



Additional studies
Consider further testing for patients with nondiagnostic MRI and to rule out differential diagnoses.
-
CSF examination: commonly performed to support MS diagnosis and rule out other conditions [1][27][28]
-
Oligoclonal bands [23]
- Oligoclonal bands in the CSF but not in blood support diagnosis of MS.
- Oligoclonal bands manifest due to increased production of multiple nonspecific IgG sub-fractions in the CSF, which are caused by intrathecal inflammation.
- Detected using electrophoresis or isoelectric focusing of CSF
- Other common findings: moderate lymphocytic pleocytosis, increased myelin basic protein [28]
-
Oligoclonal bands [23]
-
Evoked potentials: Consider visual evoked potentials for patients with symptoms related to vision. [13]
- Can provide objective evidence of lesions
- May show evidence of increased latency, which occurs due to slowed optic nerve conduction.
-
Laboratory studies: to rule out other diagnoses, based on clinical suspicion [13]
- Commonly ordered: CBC, vitamin B12, TSH, ESR, ANA, RPR, serologic testing for Lyme disease
- Others: specific autoantibodies (e.g., antiphospholipid antibodies, anti-SSA, anti-SSB), HIV testing
-
Physical examination: downwards pronator drift in pronator drift test
- An examination finding of asymmetric pronation and drifting movement of the arms when the patient stands with outstretched arms and closed eyes
- Cerebellar lesions typically cause pronation and upwards drift; upper motor neuron lesions typically cause pronation and downwards drift.
The presence of multiple oligoclonal bands in CSF and their absence in the blood is highly suggestive of MS. [27][29]
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
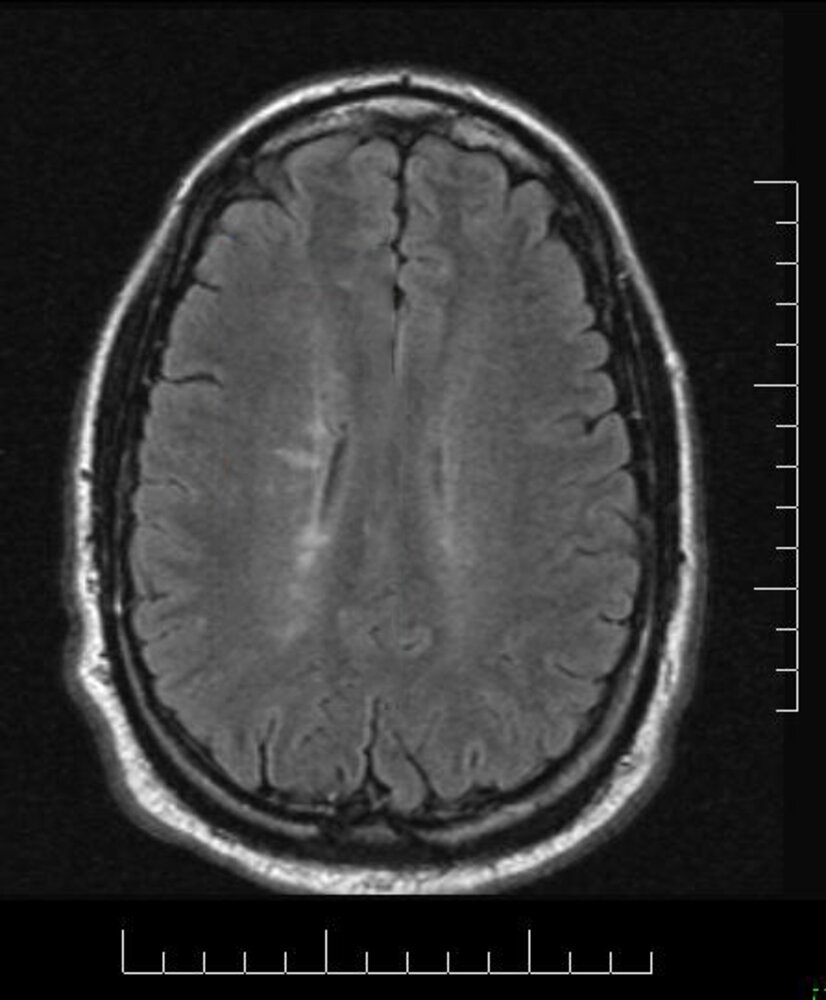
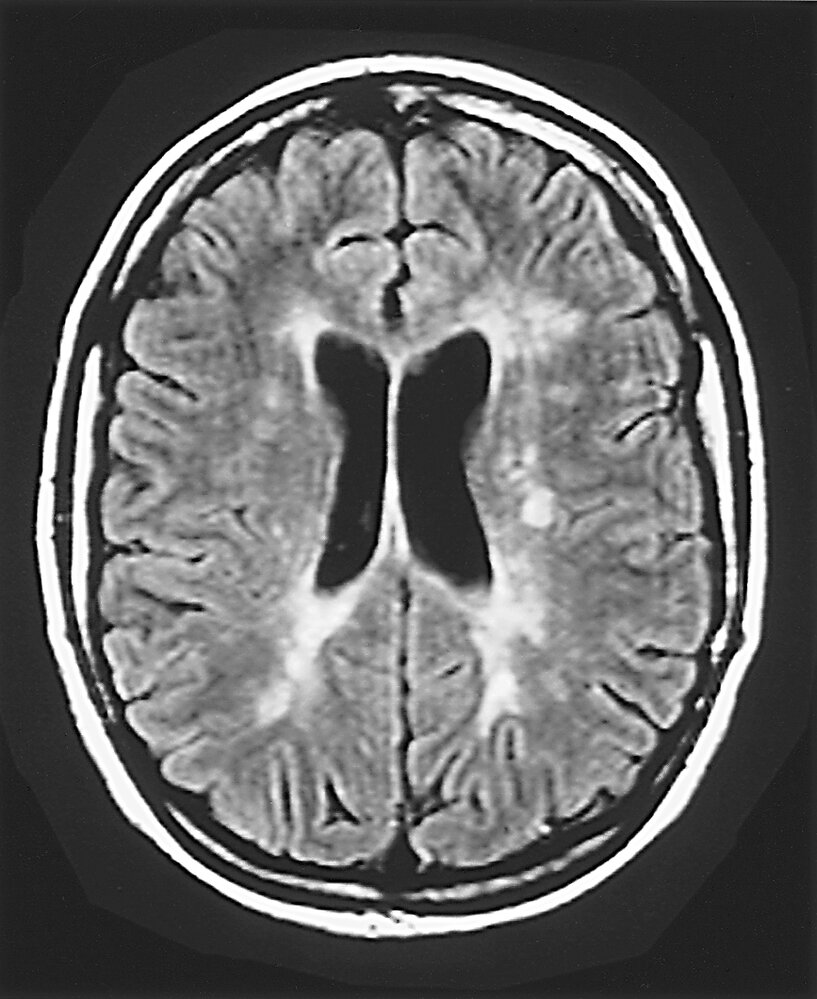
MRI Brain (FLAIR; axial view)
There are periventricular areas of linear and ovoid hyperintense signal orientated perpendicular to the body of the right lateral ventricle (green overlay).
This feature is known as Dawson fingers and is strongly associated with multiple sclerosis. It represents perivascular inflammation around the subependymal veins.
Source: “Dawsonsfingers” by VoiceOfReason, Wikimedia Foundation, licensed under CC BY-SA 3.0. Modifications: red rectangle removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
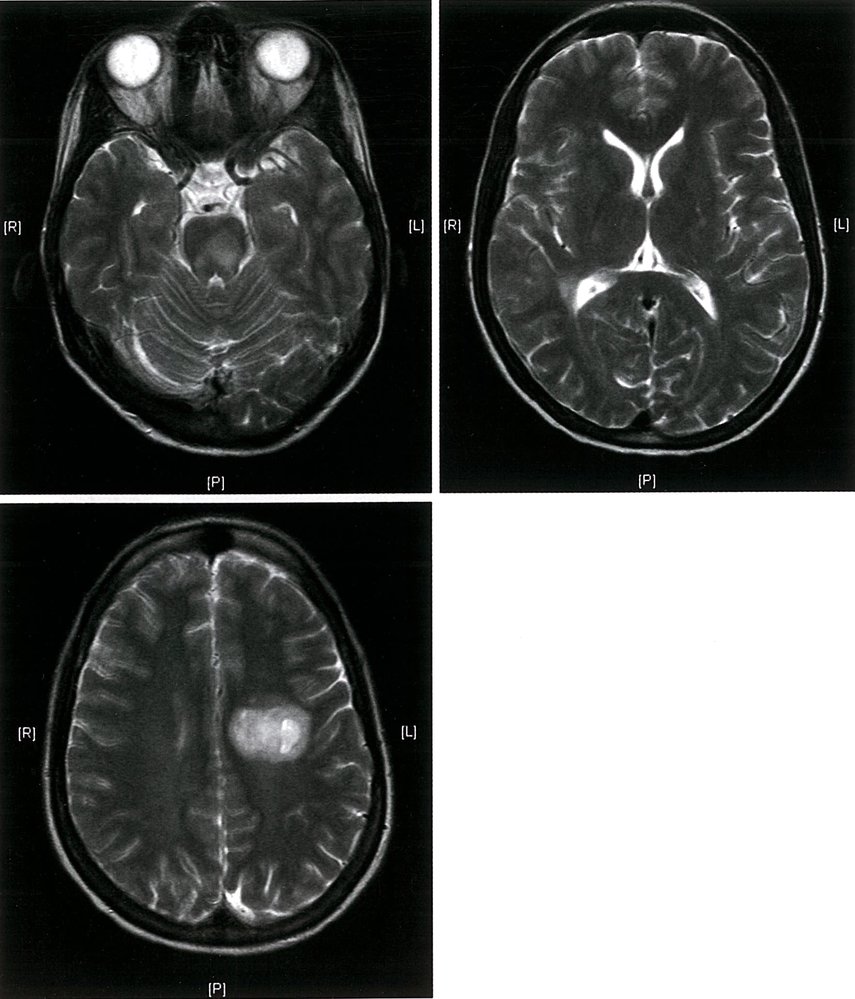
MRI (T2-weighted; axial view)
Solitary hyperintense demyelinated plaques in the telencephalon; multiple periventricular and mesencephalic hyperintensities.
Diagnosis: Multiple sclerosis
Source: © IMPP

MRI head (T2-weighted; axial plane)
Extensive bilateral demyelinating lesions (plaques) appear as hyperintensities in the periventricular white matter (green overlay). Radial extensions of these lesions (Dawson fingers) are visible. Generalized cerebral atrophy, part of the disease process for multiple sclerosis, is also visible.
Source: © IMPP
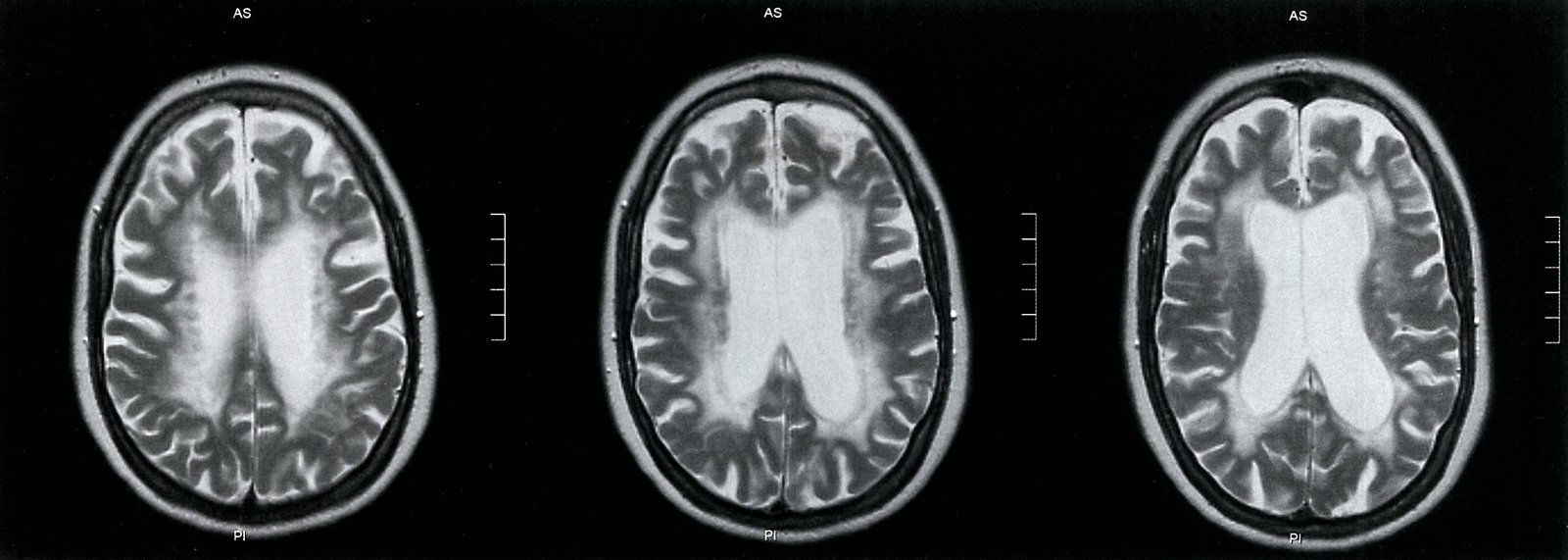
MRI head (T2-weighted; axial plane)
Extensive periventricular hyperintense signal (green overlay) is visible, representing confluent demyelinating lesions. In addition, there is generalized cerebral atrophy.
The demyelinating lesions have progressed significantly since the baseline images (see image 1/2).
Source: © IMPP
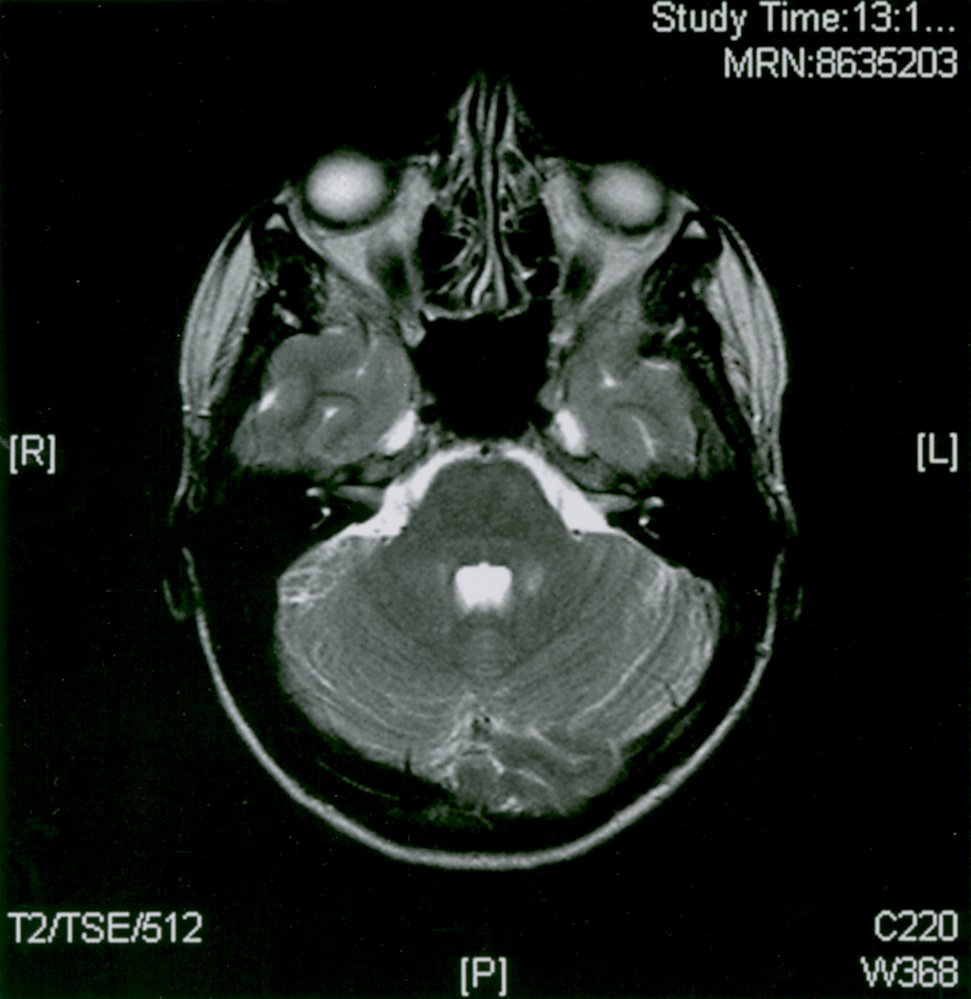
Cranial MRI (T2-weighted; axial view)
There is T2w hyperintensity without contrast in the left middle cerebellar peduncle, periventricular of the fourth ventricle. The location of the lesions is typical of an infratentorial demyelination lesions in multiple sclerosis.
Source: © IMPP

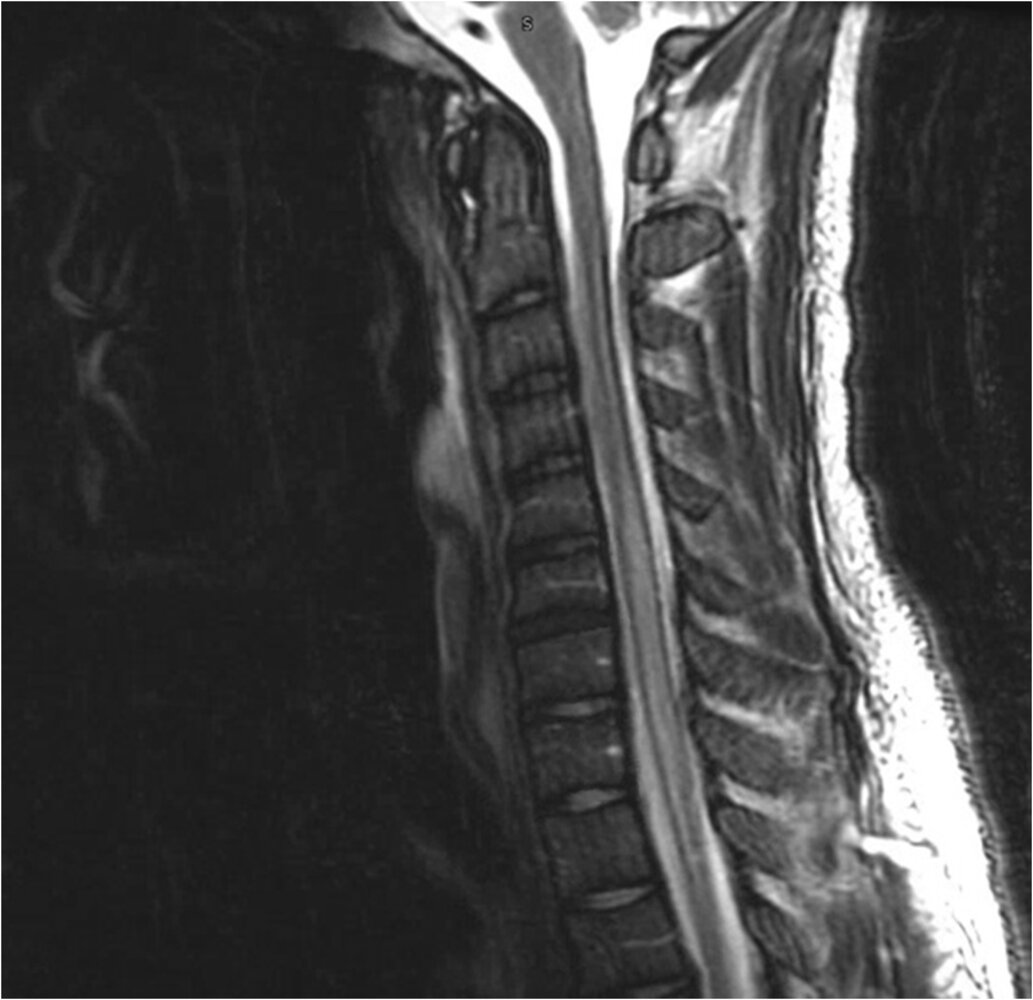
MRI cervical spine (T2-weighted; sagittal plane)
At the level of the fourth cervical vertebral body, there is an area of poorly defined hyperintensity within the spinal cord (green overlay). The first cervical vertebra is not well visualized in this image due to its shape, whereas the second cervical vertebra is well recognized due to the superior projected bony element known as the dens or odontoid process.
This is an example of a demyelinating plaque in a patient with multiple sclerosis. Spinal cord demyelinating plaques from multiple sclerosis are most often found in the cervical segment of the cord. They are usually shorter than two vertebral bodies in length.
Source: © IMPP
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
Differential diagnoses
Autoimmune diseases associated with inflammatory demyelination
Neuromyelitis optica spectrum disorders (NMOSD; previously known as Devic disease or neuromyelitis optica) [30][31]
- Definition: immune-mediated, chronic inflammatory disorders of the CNS that primarily affect the optic nerve and spinal cord
-
Epidemiology
- Incidence: 0.3-4.4 per 100,000
- More prevalent in individuals of African and Asian descent than in white populations
- Peak onset: 40-60 years
-
Pathophysiology
- Not fully understood but is thought to be an autoimmune process
- Anti-aquaporin-4 (an autoantibody that targets aquaporin-4 in the membrane of astrocytes) is involved in a humoral immune response
- Process characterized by demyelination and axonal damage of the optic nerve and spinal cord
-
Clinical features
- Closely resembles the clinical appearance of MS
-
Recurrent acute attacks with rapid stepwise deterioration, but no progression in between the attacks
- Optic neuritis (often bilateral): impaired vision, retrobulbar pain
- Transverse myelitis: symmetric paraplegia, sensory loss, bladder dysfunction
-
Diagnosis: based on
- Serological evidence of anti-aquaporin-4 (AQP4)
- The presence of clinical characteristics
- Optic neuritis
- Acute myelitis
- Area postrema syndrome (episodes of intractable nausea, vomiting, and/or hiccups)
- Acute brainstem syndrome
- Narcolepsy or acute diencephalic syndrome with typical MRI lesions
- Cerebral syndrome with typical brain lesions
- Typical MRI findings (see clinical criteria for NMOSD with negative AQP4-IgG or unknown status below)
| Diagnostic criteria of NMOSD based on AQP4-IgG status | ||
|---|---|---|
| Serological criteria | Clinical criteria | Additional criteria |
| Positive AQP4-IgG |
|
|
| Negative AQP4-IgG or unknown status |
|
|
-
Treatment
- First line: high-dose glucocorticoid therapy for 3–5 days followed by a taper for 2–8 weeks
- Plasmapheresis in severe, refractory cases
- The following biological agents are approved for use in patients with positive AQP4-IgG
- Eculizumab: antibody against C5 complement component
- Inebilizumab: antibody against CD19
- Satralizumab: antibody against IL-6 receptor
- Immune modulators used off-label (azathioprine, rituximab) may also reduce the risk of acute attacks
- Natalizumab and IFN-β (effective MS treatment options) can trigger NMOSD exacerbations
Acute disseminated encephalomyelitis (ADEM, acute demyelinating encephalomyelitis) [32]
- Definition: an immune-mediated, demyelinating CNS disease of parainfectious origin (e.g., measles) or after vaccinations (less common)
- Epidemiology: mostly affects children and young adults
-
Clinical features: rapidly progressing, usually monophasic, course with multifocal symptoms
- Evidence of motor, sensory, cranial nerve, and/or brainstem impairment
- Altered mental status (loss of consciousness is possible)
- Optic neuritis: impaired vision, retrobulbar pain
-
Diagnosis
- Lumbar puncture: lymphocytic pleocytosis and elevated protein
- Spinal and/or brain MRI (with and without contrast): typically multiple, bilateral lesions
-
Treatment
- High-dose IV corticosteroid therapy for 3–5 days
- IV immune globulin therapy or plasma exchange in patients who do not respond to corticosteroids
- Acyclovir (empiric therapy until infectious etiology is identified)
Other conditions
Transverse myelitis [33]
- Definition: an acute or subacute inflammatory myelopathy that results in motor, sensory, and autonomic symptoms below the level of the affected segment
-
Epidemiology
- Rare condition (< 5 cases per million)
- Bimodal incidence: peak in the 2nd and 4th decade of life
-
Etiology
- Most often idiopathic
- Parainfectious (e.g., enteroviruses, EBV, CMV, Listeria monocytogenes, B. burgdorferi)
- CNS demyelinating disorders (e.g., multiple sclerosis, neuromyelitis optica spectrum disorders)
- Systemic inflammatory autoimmune disorders (e.g., SLE, sarcoidosis)
- Paraneoplastic syndromes
- Drug-induced (e.g., TNF-α inhibitors, chemotherapeutic agents)
-
Clinical features
- Course of the disease
- Acute or subacute onset: symptoms may reach their peak between 4 hours and 21 days after onset
- Acute spinal shock may be present at onset
- Later, spasticity, hyperreflexia, and signs of upper motor neuron involvement (e.g., positive Babinski sign) may develop
- Neurologic dysfunction
- Motor dysfunction (e.g., paresis, paraplegia)
- Sensory dysfunction (e.g., numbness, paresthesias, circumferential dysesthesia directly above the sensory level)
- Autonomic dysfunction (e.g., bladder and/or bowel incontinence, sexual dysfunction)
- Course of the disease
| Overview of transverse myelitis types | |||
|---|---|---|---|
| Types of TM | Manifestations | MRI findings | |
| Longitudinally limited TM (LLTM) | Acute complete TM (ACTM) |
|
|
| Acute partial TM (APTM)1 |
|
|
|
| Longitudinally extensive TM (LETM) |
|
|
|
-
Diagnostics
-
MRI of the brain and spine with and without gadolinium: investigation of choice
- Finding: focal, gadolinium-enhancing lesion in the spinal cord (T2-weighted sequence)
- Brain MRI with and without gadolinium should also be performed to rule out CNS demyelinating disorders (e.g., MS)
-
Laboratory studies
- Serological testing for viral infections, syphilis, and HIV antibodies
- Inflammatory markers (ESR, CRP)
- Serum autoimmune antibody testing: antinuclear antibodies, rheumatoid factor, antiphospholipid antibodies, NMO IgG (anti-aquaporin-4)
- Serum levels of vitamin B12 and methylmalonic acid
- Thyroid function tests
-
CSF analysis [34]
- Inflammatory markers: pleocytosis and/or elevated IgG index
- Oligoclonal bands: helpful in diagnosing MS
- Cultures and viral PCR
- VDRL to rule out syphilis
- Further investigations based on clinical presentation and suspected underlying cause, e.g., paraneoplastic profile to rule out paraneoplastic syndrome, CT chest to rule out sarcoidosis, nerve conduction studies to help rule out GBS and peripheral neuropathies
-
MRI of the brain and spine with and without gadolinium: investigation of choice
-
Differential diagnoses
- Anterior spinal artery infarction
- Guillain-Barré syndrome (GBS)
- Compressive myelopathy (e.g., due to intramedullary spinal cord tumors)
- Radiation myelitis
- Metabolic myelopathy (e.g., due to vitamin B12 deficiency, copper deficiency)
-
Treatment
- Acute management
- First-line: immediate high-dose IV corticosteroids
-
Second-line
- Plasmapheresis if response to corticosteroids is insufficient
- Cyclophosphamide
- Supportive care: prevent decubitus ulcer and/or thrombosis, manage urinary retention, gastroparesis, constipation, and respiratory failure in patients with high cervical cord lesions
- Long-term management
- Neurological rehabilitation
- Ongoing treatment of underlying causes (e.g., long-term immunomodulatory therapies for systemic autoimmune conditions or demyelinating disease)
- Acute management

Other
- Vasculitis: resulting from connective tissue disorders (e.g., SLE, polyarteritis nodosa, granulomatosis with polyangiitis, Behcet disease)
-
Infections
- Neuroborreliosis: diagnosed by CSF examination (intrathecal Borrelia-specific antibodies, lymphocytosis)
- Neurosyphilis: diagnosed by a TPHA screening test
- Progressive multifocal leukoencephalopathy (PML): perform an HIV test
- HIV-encephalopathy: perform an HIV test
The differential diagnoses listed here are not exhaustive.
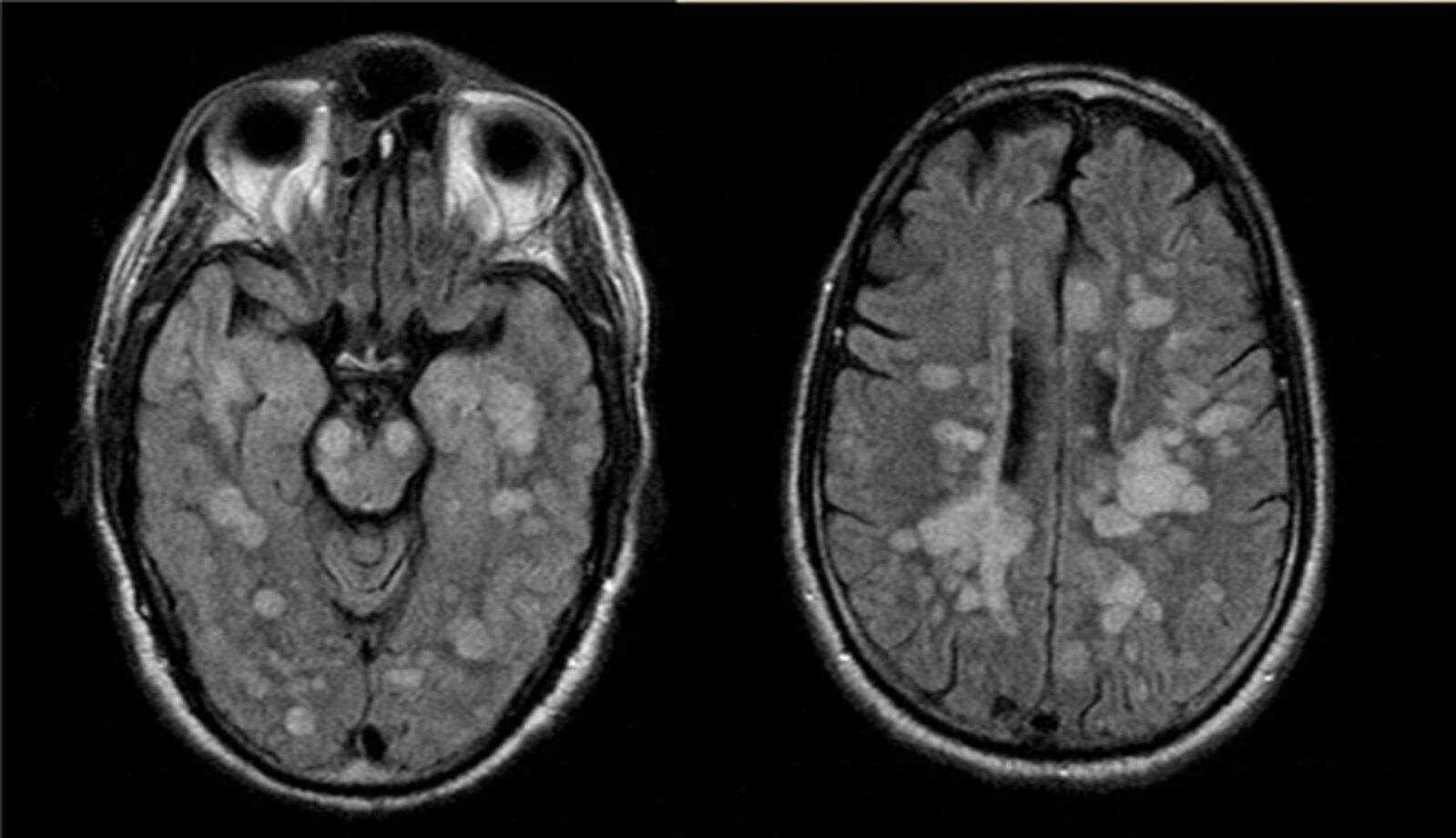
MRI head (FLAIR; axial plane) of a 60-year-old with rapid cognitive decline starting 2 weeks after an elective dental procedure.
Multiple large confluent hyperintense lesions are demonstrated in both cerebral hemispheres in an asymmetric pattern. The lesions are predominantly located within the white matter (example indicated by green overlay). In addition to these lesions in the supratentorial region, further hyperintense lesions are visible in the midbrain (example indicated by red overlay), indicating infratentorial involvement.
Acute disseminated encephalomyelitis (ADEM) is an autoimmune-mediated inflammatory demyelinating condition. It is difficult to differentiate from other inflammatory conditions, especially multiple sclerosis, and tissue diagnosis may be the only way to confirm diagnosis. An immunologic trigger may be present in the clinical history. An infection from the dental procedure in this case may have been the trigger for ADEM.
Source: “Figure 2, in: Refractory fulminant acute disseminated encephalomyelitis (ADEM) in an adult” by Federico Rodríguez-Porcel, Alejandro Hornik, Jordan Rosenblum, Ewa Borys, José Biller, Frontiers in Neurology, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
MRI cervical and thoracic spine (T2-weighted; sagittal plane) of a patient with systemic lupus erythematosus and sudden onset quadriplegia
Longitudinal hyperintensity within the spinal cord (green overlay), extending from C2 to T2, reflects edema of the spinal cord.
Source: “Fig 2, In: Longitudinally Extensive Transverse Myelitis Associated With Systemic Lupus Erythematosus: A Case Report and Literature Review” by Mehmood T, Munir I, Abduraimova M, Ramirez MA, Paghdal S, McFarlane IM, SciEP, licensed under CC BY 4.0. Modifications: - arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Treatment
General principles [35]
- All patients: Refer to a neurologist for specialized management.
-
Acute exacerbations: Treat all acute exacerbations that affect physical functioning.
- First line: high-dose IV or PO glucocorticoids (e.g., methylprednisolone)
- Alternatives: plasmapheresis or adrenocorticotropic hormone (ACTH) gel [36]
-
Long-term management: Combine pharmacological and nonpharmacological measures to prevent exacerbations and improve quality of life.
- Disease-modifying MS therapy
- Lifestyle modifications (e.g., exercise, smoking cessation) and management of comorbidities (e.g., cardiovascular disease, sleep disorders)
- Vitamin D supplementation may be beneficial. [37]
- Management of symptoms (e.g., spasticity, central neuropathic pain, bowel and bladder dysfunction)
Treatment should be initiated as early as possible; the goals of treatment are to manage the primary exacerbation, prevent further exacerbations, and slow disease progression.
Management of acute MS exacerbations [7][38]
If an acute exacerbation of MS is suspected, a specialist should be consulted immediately for management.
-
Preferred therapy:
- High-dose glucocorticoid pulse therapy (e.g., methylprednisolone ) [38][39][40]
- Start measures to prevent complications of glucocorticoid therapy (e.g., PPIs, monitoring for hyperglycemia).
- Alternatives: plasmapheresis, ACTH gel [38][41]
-
Additional considerations
- Perform a thorough neurological examination and compare with the patient's baseline.
- Evaluate for possible infectious triggers. [42]
- Consider hospital admission for patients with disabling symptoms (e.g., loss of vision, difficulty with ambulation, dysphagia). [43]
- Supportive care: physical therapy, occupational therapy, and/or speech and swallow evaluations
Mild exacerbations that do not impact physical functioning may not require medical treatment.
Disease-modifying MS therapy
- There are multiple disease-modifying drugs available to treat MS.
- The decision about agent requires careful consideration of:
- Individual patient's characteristics (e.g., clinical phenotype, comorbidities)
- Medication side effects
- Other factors (e.g., medication availability, route of administration)
- All patients receiving disease-modifying therapy for MS should use birth control.
Disease-modifying therapy for MS is generally not recommended for pregnant and breastfeeding patients. [44]
| Commonly used disease-modifying MS drugs by clinical phenotype | |
|---|---|
| Phenotype | Drugs commonly used |
| Clinically isolated syndrome [45] |
|
| Relapsing-remitting MS [7] |
|
| Secondary progressive MS [46] |
|
| Primary progressive MS [47] |
|
Monoclonal antibodies (e.g., natalizumab, ocrelizumab) have the highest efficacy for reducing exacerbations, but lower efficacy medications (e.g., interferon beta, glatiramer acetate) often have fewer side effects. [7]
| Overview of disease-modifying drugs in MS therapy(DMDs) [7][13][45] | |||
|---|---|---|---|
| Medication | Mechanism of action | Adverse effects | |
| Interferon beta |
|
|
|
| Glatiramer acetate (copolymer-1) |
|
|
|
| Dimethyl fumarate |
|
|
|
| Teriflunomide |
|
|
|
| Cladribine [1][53] |
|
|
|
| Sphingosine 1-phosphate receptor modulators [54] | Fingolimod |
|
|
| Siponimod | |||
| Ozanimod | |||
| Ponesimod | |||
| Monoclonal antibodies | Alemtuzumab |
|
|
| Natalizumab |
|
|
|
| Ocrelizumab |
|
|
|
| Ofatumumab | |||
| Mitoxantrone [23][56] |
|
|
|
Supportive care and symptom management [7][59][60]
Consider any of the following measures in a management plan tailored to the individual patient:
-
General measures
- Encourage physical activity.
- Close follow-up with neurology and primary care
- Ancillary referral as needed (e.g., physical therapists, occupational therapists, psychologists)
- Screen for major depression and start therapy with antidepressants as needed (see also “Treatment” in “Major depression disorder”).
-
Urinary and bowel dysfunction
- Urinary frequency: pelvic floor physical therapy, bladder training; Consider anticholinergics (e.g., oxybutynin) and antimuscarinics (e.g., tolterodine).
- Urinary retention: Consider intermittent catheterization and parasympathomimetic drugs (e.g., bethanechol). [61]
- Bowel dysfunction: dietary fiber and fluid intake; laxatives (e.g., senna) and stool softeners (e.g., docusate) as needed
-
Spasticity
- Stretching, avoidance of triggers (e.g., certain positions, pain, constipation)
- Medications: baclofen (centrally acting GABA agonist), tizanidine (α2-receptor agonist), gabapentin, dantrolene, botulinum toxin.
- Tremors: deep brain stimulation techniques, beta blockers (e.g., propranolol), gabapentin
- Central neuropathic pain: tricyclic antidepressants (e.g., amitriptyline): , other antidepressants (e.g., duloxetine), anticonvulsants (e.g., carbamazepine, gabapentin), transcutaneous electrical nerve stimulation (see also “Treatment” in “Trigeminal Neuralgia”)
- Walking difficulties: mobility aids (e.g., canes, walkers), consider dalfampridine [62]
-
Others
- Fatigue: Consider medications such as amantadine or modafinil.
- Sexual dysfunction: Consider medications for erectile dysfunction (e.g., sildenafil) and nonpharmacological measures (e.g., vaginal lubricants, intracavernous injection therapy) as needed.
- Psychotherapy: to reduce potential psychological issues (e.g., depression)
Physical therapy, occupational therapy, and psychotherapy are safe, nonpharmacological options that can improve multiple symptoms in patients with MS, including spasticity, fatigue, walking difficulties, and central neuropathic pain.
Prognosis
Poor prognostic factors for disease progression [63][64]
- Male sex
- Age at MS onset > 40 years
- Multiple symptoms with early motor and cerebellar involvement
- Incomplete recovery after exacerbations
- High relapse rate in the first 2 years after MS onset
Special patient groups
Multiple sclerosis in pregnancy [7][44]
Prognosis
-
Effect of pregnancy on MS
- Decreased exacerbation risk during pregnancy
- Increased risk of exacerbation in the postpartum period
- The long-term clinical course of MS remains unchanged.
-
Effect of MS on pregnancy
- Increased rate of elective cesarean sections
- Decreased birth weights [65]
Management
- Most disease-modifying therapy for MS should be discontinued ≥ 4 months prior to conception. [66]
- Avoid steroids for the treatment of exacerbations in the first trimester of pregnancy. [44]
- Breastfeeding is generally not recommended for patients receiving disease-modifying therapy for MS.
- Avoid MRI with gadolinium in pregnant patients.
Related One-Minute Telegram
- One-Minute Telegram 120-2025-3/3: D-fence against MS: vitamin D reduces MS disease activity
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- Dobson R, Giovannoni G. "Multiple sclerosis – a review". European Journal of Neurology. 26(1). :27-40. (2018)
- Thompson AJ, Baranzini SE, Geurts J, Hemmer B, Ciccarelli O. "Multiple sclerosis". The Lancet. 391(10130). :1622-1636. (2018)
- Langer-Gould AM, Gonzales EG, Smith JB, Li BH, Nelson LM. "Racial and Ethnic Disparities in Multiple Sclerosis Prevalence.". Neurology. 98(18). :e1818-e1827. (2022)
- Schmidt H, Williamson D, Ashley-Koch A. "HLA-DR15 haplotype and multiple sclerosis: A HuGE review". Am J Epidemiol. 165(10). :1097-1109. (2007)
- Hansen T, Skytthe A, Stenager E, et al. "Concordance for multiple sclerosis in Danish twins: an update of a nationwide study". Multiple Sclerosis Journal. 11(5). :504-510. (2005)
- O'Gorman C, Lucas R, Taylor B. "Environmental risk factors for multiple sclerosis: a review with a focus on molecular mechanisms". Int J Mol Sci. 13(9). :11718-52. (2012)
- Mitsdoerffer M, Peters A. "Tertiary Lymphoid Organs in Central Nervous System Autoimmunity". Frontiers in Immunology. 7. (2016)
- Correale J, Gaitán MI, Ysrraelit MC, Fiol MP. "Progressive multiple sclerosis: from pathogenic mechanisms to treatment.". Brain. 140(3). :527-546. (2017)
- Voss E, Raab P, Trebst C, Stangel M. "Clinical approach to optic neuritis: pitfalls, red flags and differential diagnosis". Ther Adv Neurol Disord. 4(2). :123-134. (2011)
- Shaygannejad V, Golabchi K, Dehghani A, et al. "Color blindness among multiple sclerosis patients in Isfahan". J Res Med Sci. 17(3). :254–257. (2012)
- Rodriguez M, Siva A, Cross SA, O'Brien PC, Kurland LT. "Optic neuritis: A population-based study in Olrnsted County, Minnesota". NEUROLOGY. 45. :244-250. (1995)
- Dick JPR. "The deep tendon and the abdominal reflexes". J Neurol Neurosurg Psychiatry. 74. :150-153. (2003)
- Di Stefano G, Maarbjerg S, Truini A. "Trigeminal neuralgia secondary to multiple sclerosis: from the clinical picture to the treatment options". The Journal of Headache and Pain. 20(1). (2019)
- Hurt RW. "The Pathophysiology of Trigeminal Neuralgia". Springer Berlin Heidelberg. :2359-2419. (2009). ISBN: 9783540699590
- McGinley MP, Goldschmidt CH, Rae-Grant AD. "Diagnosis and Treatment of Multiple Sclerosis". JAMA. 325(8). :765. (2021)
- Thompson AJ, Banwell BL, Barkhof F, et al. "Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria". The Lancet Neurology. 17(2). :162-173. (2018)
- Calabresi PA. "Diagnosis and management of multiple sclerosis.". Am Fam Physician. 70(10). :1935-44. (2004)
- Saguil A, Kane S, Farnell E. "Multiple sclerosis: a primary care perspective.". Am Fam Physician. 90(9). :644-52. (2014)
- Kearney H, Miller DH, Ciccarelli O. "Spinal cord MRI in multiple sclerosis—diagnostic, prognostic and clinical value". Nat Rev Neurol. 11(6). :327-338. (2015)
- Filippi M, Rocca MA, Ciccarelli O, et al. "MRI criteria for the diagnosis of multiple sclerosis: MAGNIMS consensus guidelines". Lancet Neurol. 15(3). :292-303. (2016)
- Filippi M, Preziosa P, Banwell BL, et al. "Assessment of lesions on magnetic resonance imaging in multiple sclerosis: practical guidelines". Brain. 142(7). :1858-1875. (2019)
- Deisenhammer F, Zetterberg H, Fitzner B, Zettl UK. "The Cerebrospinal Fluid in Multiple Sclerosis". Frontiers in Immunology. 10. (2019)
- Comabella M, Montalban X. "Body fluid biomarkers in multiple sclerosis.". Lancet Neurol. 13(1). :113-26. (2014)
- Lamers KJ, de Reus HP, Jongen PJ. "Myelin basic protein in CSF as indicator of disease activity in multiple sclerosis". Mult Scler. 4(3). :124-126. (1998)
- Barnett Y. "Conventional and Advanced Imaging in Neuromyelitis Optica". American Journal of Neuroradiology. (2014)
- Wingerchuk D. "International consensus diagnostic criteria for neuromyelitis optica spectrum disorders". American Academy of Neurology. (2015)
- Marchioni E, Tavazzi E, Minoli L et al. "Acute disseminated encephalomyelitis". Curr Infect Dis Rep. 10(4). :307-314. (2008)
- Beh SC, Greenberg BM, Frohman T, et al. "Transverse Myelitis". Neurol Clin.. (2012)
- Jacob A, Weinshenker BG. "An Approach to the Diagnosis of Acute Transverse Myelitis". Thieme Medical Publishers. (2008)
- Rae-Grant A., et al. "Practice guideline recommendations summary: Disease-modifying therapies for adults with multiple sclerosis: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology". Neurology. 92(2). :112-112. (2019)
- Montero-Melendez T. "ACTH: The forgotten therapy". Semin Immunol. 27(3). :216-226. (2015)
- Sintzel MB, Rametta M, Reder AT. "Vitamin D and Multiple Sclerosis: A Comprehensive Review". Neurol Ther. 7(1). :59-85. (2017)
- Repovic P. "Management of Multiple Sclerosis Relapses". CONTINUUM. 25(3). :655-669. (2019)
- Burton JM, O’Connor PW, Hohol M, Beyene J. "Oral versus intravenous steroids for treatment of relapses in multiple sclerosis". Cochrane Database Syst Rev. (2012)
- Olek MJ. "Multiple Sclerosis". Ann Intern Med. 174(6). :ITC81-ITC96. (2021)
- Noseworthy JH, Lucchinetti C, Rodriguez M, Weinshenker BG. "Multiple Sclerosis". N Engl J Med. 343(13). :938-952. (2000)
- Wang C, Ruiz A, Mao-Draayer Y. "Assessment and Treatment Strategies for a Multiple Sclerosis Relapse.". J Immunol Clin Res. 5(1). (2018)
- Abboud H, Mente K, Seay M, et al. "Triaging Patients with Multiple Sclerosis in the Emergency Department". Int J MS Care. 19(6). :290-296. (2017)
- Voskuhl R, Momtazee C. "Pregnancy: Effect on Multiple Sclerosis, Treatment Considerations, and Breastfeeding". Neurotherapeutics. 14(4). :974-984. (2017)
- Metz LM. "Clinically Isolated Syndrome and Early Relapsing Multiple Sclerosis". CONTINUUM. 25(3). :670-688. (2019)
- Cree BAC, Arnold DL, Chataway J, et al. "Secondary Progressive Multiple Sclerosis". Neurology. 97(8). :378-388. (2021)
- Rae-Grant A, Day GS, Marrie RA, et al. "Practice guideline recommendations summary: Disease-modifying therapies for adults with multiple sclerosis". Neurology. 90(17). :777-788. (2018)
- Dhib-Jalbut S, Marks S. "Interferon- mechanisms of action in multiple sclerosis". Neurology. 74(Issue 1, Supplement 1). :S17-S24. (2009)
- Ziemssen T. "Glatiramer acetate-specific T-helper 1- and 2-type cell lines produce BDNF: implications for multiple sclerosis therapy". Brain. 125(11). :2381-2391. (2002)
- Filippi M, Bar-Or A, Piehl F, et al. "Multiple sclerosis". Nat Rev Dis Primers. 4(1). (2018)
- Mills EA, Ogrodnik MA, Plave A, Mao-Draayer Y. "Emerging Understanding of the Mechanism of Action for Dimethyl Fumarate in the Treatment of Multiple Sclerosis". Front Neurol. 9. (2018)
- Bar-Or A, Pachner A, Menguy-Vacheron F, Kaplan J, Wiendl H. "Teriflunomide and Its Mechanism of Action in Multiple Sclerosis". Drugs. 74(6). :659-674. (2014)
- Faissner S, Gold R. "Oral Therapies for Multiple Sclerosis". Cold Spring Harb Perspect Med. 9(1). :a032011. (2018)
- Subei AM, Cohen JA. "Sphingosine 1-Phosphate Receptor Modulators in Multiple Sclerosis". CNS Drugs. 29(7). :565-575. (2015)
- Berger JR, Cree BA, Greenberg B, et al. "Progressive multifocal leukoencephalopathy after fingolimod treatment". Neurology. 90(20). :e1815-e1821. (2018)
- Dargahi N, Katsara M, Tselios T, et al. "Multiple Sclerosis: Immunopathology and Treatment Update". Brain Sci. 7(12). :78. (2017)
- Sellebjerg F, Blinkenberg M, Sorensen PS. "Anti-CD20 Monoclonal Antibodies for Relapsing and Progressive Multiple Sclerosis". CNS Drugs. 34(3). :269-280. (2020)
- Fox EJ. "Mechanism of action of mitoxantrone". Neurology. 63(Issue 12, Supplement 6). :S15-S18. (2004)
- Tobin WO. "Management of Multiple Sclerosis Symptoms and Comorbidities". CONTINUUM. 25(3). :753-772. (2019)
- Coyle PK. "Symptom Management and Lifestyle Modifications in Multiple Sclerosis". CONTINUUM. 22(3). :815-836. (2016)
- Goldman MD, Cohen JA, Fox RJ, Bethoux FA. "Multiple sclerosis: treating symptoms, and other general medical issues.". Cleve Clin J Med. 73(2). :177-186. (2006)
- Dunn J, Blight A. "Dalfampridine: a brief review of its mechanism of action and efficacy as a treatment to improve walking in patients with multiple sclerosis". Curr Med Res Opin. 27(7). :1415-1423. (2011)
- Gajofatto A, Calabrese M, Benedetti MD, Monaco S. "Clinical, MRI, and CSF Markers of Disability Progression in Multiple Sclerosis". Dis Markers. 35. :687-699. (2013)
- Iaffaldano P, Lucisano G, Patti F, et al. "Transition to secondary progression in relapsing-onset multiple sclerosis: Definitions and risk factors". Multiple Sclerosis Journal. :135245852097436. (2020)
- Andersen JB, Kopp TI, Sellebjerg F, Magyari M. "Pregnancy-Related and Perinatal Outcomes in Women With Multiple Sclerosis". Neurol Clin Pract. 11(4). :280-290. (2021)
- Krysko KM, Bove R, Dobson R, Jokubaitis V, Hellwig K. "Treatment of Women with Multiple Sclerosis Planning Pregnancy". Curr Treat Options Neurol. 23(4). (2021)
- Kantarci OH. "Phases and Phenotypes of Multiple Sclerosis". CONTINUUM. 25(3). :636-654. (2019)
- Hosseiny M, Newsome SD, Yousem DM. "Radiologically Isolated Syndrome: A Review for Neuroradiologists.". AJNR Am J Neuroradiol. 41(9). :1542-1549. (2020)
- Bacigaluppi S, Polonara G, Zavanone ML, et al. "Schilder’s disease: non-invasive diagnosis?". Neurol Sci. 30(5). :421-430. (2009)
- Jarius S, Haas J, Paul F, Wildemann B. "Myelinoclastic diffuse sclerosis (Schilder’s disease) is immunologically distinct from multiple sclerosis: results from retrospective analysis of 92 lumbar punctures". J Neuroinflammation. 16(1). (2019)
- Lublin FD, Reingold SC, Cohen JA, et al. "Defining the clinical course of multiple sclerosis: The 2013 revisions". Neurology. 83(3). :278-286. (2014)
- Spiegel HE, Nowacki G, Hsiao KJ. "Advances in Clinical Chemistry". Academic Press. (2001). ISBN: 9780080490250
- "McDonald Diagnostic Criteria for Multiple Sclerosis". https://radiopaedia.org/articles/mcdonald-diagnostic-criteria-for-multiple-sclerosis
- Feinstein A. "The Clinical Neuropsychiatry of Multiple Sclerosis". Cambridge University Press. (2007). ISBN: 9781139463904
- Ross AP, Ben-Zacharia A, Harris C, Smrtka J. "Multiple sclerosis, relapses, and the mechanism of action of adrenocorticotropic hormone". Front Neurol. 4. :21. (2013)
- Berkovich R, Agius MA. "Mechanisms of action of ACTH in the management of relapsing forms of multiple sclerosis". Ther Adv Neurol Disord. 7(2). :83-96. (2014)