Summary
Myelodysplastic syndromes (MDSs) are a group of clonal hematopoietic stem cell neoplasms characterized by impaired proliferation and differentiation of myeloid stem cells within the bone marrow. Primary (idiopathic) MDS, likely related to spontaneous mutations, is most common; secondary MDS may result from inciting events such as exposure to chemotherapy. MDS is typically seen in older adults and is evidenced by laboratory abnormalities, symptoms of cytopenia(s), and findings of extramedullary hematopoiesis. To diagnose and classify MDS, other causes of cytopenia and/or dysplasia must be excluded and bone marrow and genetic studies should be conducted. These studies typically show dysplasia and cytopenia in at least one mature myeloid cell line on CBC, bone marrow hypercellularity of myeloid precursors, and MDS-associated genetic abnormalities. All patients should receive supportive therapy as needed, including transfusions and treatment of associated iron overload. Additional treatment is guided by risk stratification in MDS. Individuals with high-risk disease are treated with hypomethylating agents and possibly intensive chemotherapy; they should also all be assessed for fitness for allogeneic hematopoietic stem cell transplantation, which is the only curative option. Treatment options for individuals with low-risk disease include expectant management, hypomethylating agents, and drugs such as lenalidomide. Close surveillance is required to determine treatment response and monitor for disease progression (e.g., to acute myelogenous leukemia or bone marrow failure).
Etiology
-
Primary MDS (90% of cases) [1]
- Most commonly manifests in older adults [1]
- Idiopathic: likely due to spontaneous mutations [1]
-
Secondary MDS (10% of cases): due to exogenous bone marrow damage [2]
- Treatment-related: following cytostatic therapy (alkylating agents, topoisomerase II inhibitors, azathioprine, etc.)
- Benzene and other organic solvents
- Radiation damage: therapeutic radiation, radioiodine therapy, ionizing radiation
- Paroxysmal nocturnal hemoglobinuria




© AMBOSS
© AMBOSS
© AMBOSS
© AMBOSS
Classification
| Classifications of MDS [3][4] | |
|---|---|
| 2022 World Health Organization (WHO) 5th edition |
|
| 2022 International Consensus Classification (ICC) |
|
MDS and AML are differentiated based on the number of myeloblasts in bone marrow or peripheral blood cells: < 20% in MDS and ≥ 20% in AML. [3][4]
In a previous WHO classification system, refractory anemia was a subtype of MDS. [5]
Clinical features
- Asymptomatic in 20% of cases
- Depending on the affected cell line: [6]
- Erythrocytopenia ; (70% of cases) → symptoms of anemia
- Leukocytopenia with increased susceptibility to bacterial infections, especially of the skin
- Thrombocytopenia ; with impaired primary hemostasis → petechial bleeding
- Hepatosplenomegaly (uncommon)
Diagnosis
Approach [7][8][9]
Workup for MDS may be prompted by symptoms related to cytopenias or by the discovery of incidental cytopenia.
- Obtain initial studies, including workup for other causes of cytopenia and dysplasia.
- If the cause is still unexplained, refer to hematology-oncology for:
- Advanced diagnostic studies (i.e., bone marrow and genetic studies)
- Confirmation of diagnosis and classification of MDS, based on the presence of ≥ 1 of the following: [3][4]
- ≥ 10% dysplastic cells in ≥ 1 myeloid cell line on bone marrow smear (see “Myeloid cell line abnormalities in MDS”)
- Increased myeloblasts [3]
- MDS-associated genetic abnormality
MDS is often identified during evaluation for unexplained cytopenia.
Initial studies [7][8][10]
- CBC with peripheral smear: will show myeloid cell line abnormalities in MDS
- Studies to exclude other causes of cytopenia and/or dysplasia
- Infectious disease studies (e.g., HIV test, viral hepatitis panel)
- Micronutrient levels (e.g., B12, folate, copper, iron) [11]
- BMP: to assess for chronic kidney disease
- Liver chemistries: to assess for chronic liver disease
- Possible additional studies: may show nonspecific abnormalities [9]
- ↑ LDH
- ↑ Uric acid
- Gamma globulins: may be decreased or elevated (both monoclonal and polyclonal gammopathies)
Advanced studies for MDS [3][7][12]
- Bone marrow studies (aspiration and/or biopsy): to evaluate for myeloid cell line abnormalities in MDS
- Genetic evaluation [4]
- Karyotype +/- FISH: to evaluate for chromosomal aberrations (e.g., 5q or 7q deletion) [13]
- Mutation analysis: to evaluate for specific mutations (e.g., SF3B1 and TP53)
Genetic evaluation is required for classification of MDS, as well as for risk-stratification of patients to estimate prognosis and guide treatment. [3][7]

Overview of hematological findings in MDS [12][14][15]
| Myeloid cell line abnormalities in MDS [12][14][15] | ||||
|---|---|---|---|---|
| Peripheral smear | Bone marrow studies | |||
| Cell count [12] |
|
|
||
| Dysplasias | Erythrocyte lineage |
|
|
|
| Leukocyte lineage |
|
|
||
| Thrombocyte lineage |
|
|
||
Anemia is the most common cytopenia in MDS, and may manifest as macrocytic anemia or normocytic anemia. [9]
The pseudo-Pelger-Huet anomaly is also seen in patients receiving certain medications (e.g., chemotherapy, transplant medications) and in other hematological disorders (e.g., myeloproliferative disorders). [16][17]




Karyogram and fluorescence in situ hybridization (FISH) of a patient with myelodysplastic syndrome and a 5q31 and 5q33 deletion.
In the karyogram (left image), the long arm of chromosome 5 is shortened (5q deletion). This deletion was further confirmed using FISH (right image). A blue probe was used to detect two copies of chromosome 5 (two blue signals). A red probe was used to display the 5q31 band and a green probe to display the 5q33 band (red and green signals correspondingly).
These findings are suggestive of isolated 5q deletion, which is classified as a specific subtype of myelodysplastic syndrome by the WHO.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.
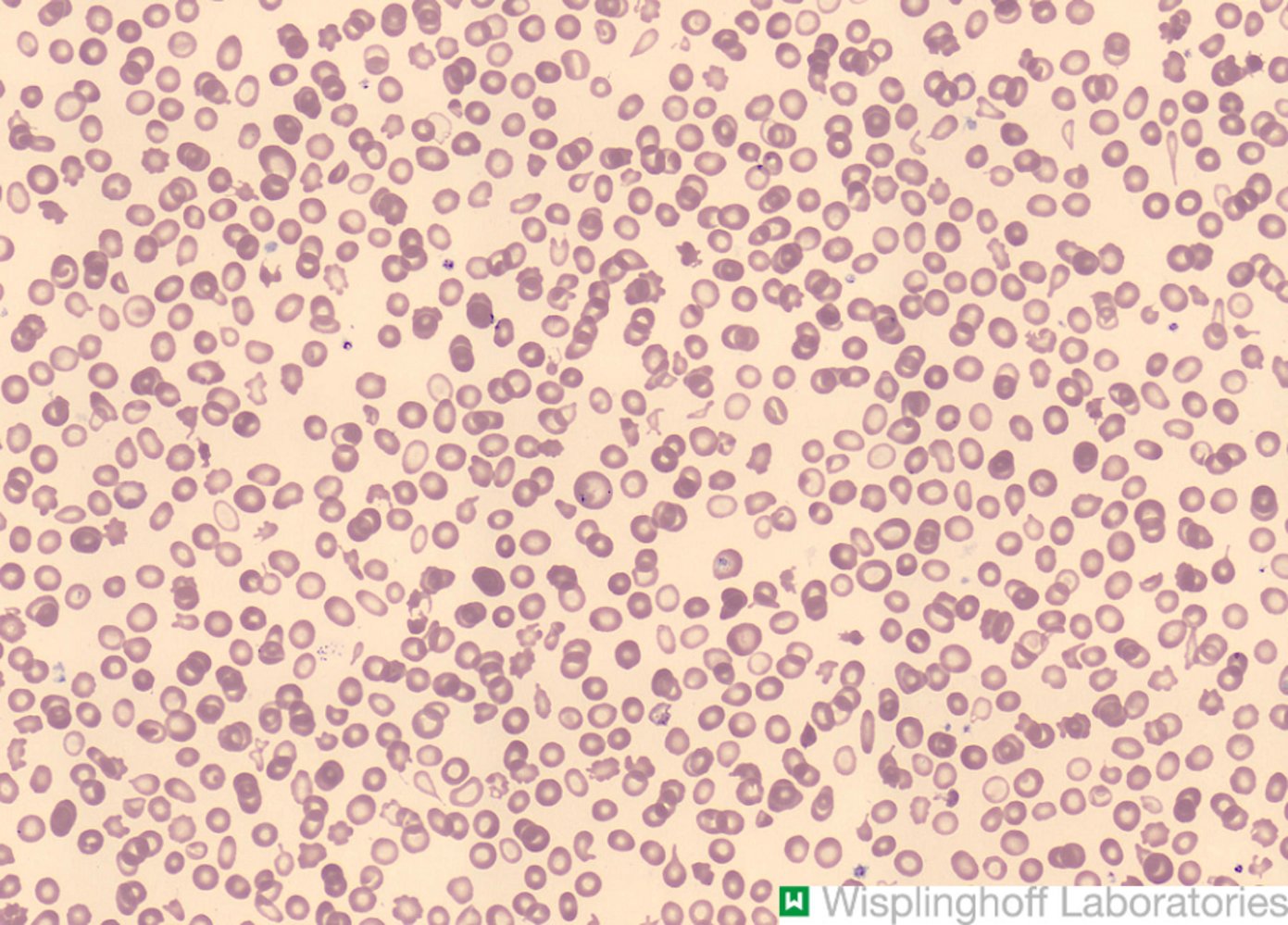
Photomicrograph of a peripheral blood smear (Pappenheim stain)
This specimen depicts anisocytosis, which are erythrocytes of different sizes (black circles), as well as poikilocytosis, which are erythrocytes of different shapes. Acanthocytes with thorny projections (light blue circles) and teardrop shaped dacrocytes (red circles) are present.
These findings suggest impaired erythropoiesis, which may be a result of impaired bone marrow hematopoiesis.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.

Peripheral blood smear (Giemsa stain)
Numerous erythrocytes (light pink disc-like structures with central pallor) can be seen throughout the image. Howell-Jolly bodies are visible as small circular basophilic inclusions in the cytoplasm of the three erythrocytes (red overlay). A neutrophil with a polysegmented basophilic nucleus (in the center) and a lymphocyte with a large central round nucleus and a rim of basophilic cytoplasm (on the right side) are also visible.
Howell-Jolly bodies are usually removed by the spleen. They are typically seen in asplenic patients but can also appear in individuals with myelodysplastic syndromes or megaloblastic anemia.
Source: “Howell-Jolly bodies: small, round inclusions seen in erythrocytes, found in various anemias and after splenectomy” by Paulo Henrique Orlandi Mourao, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
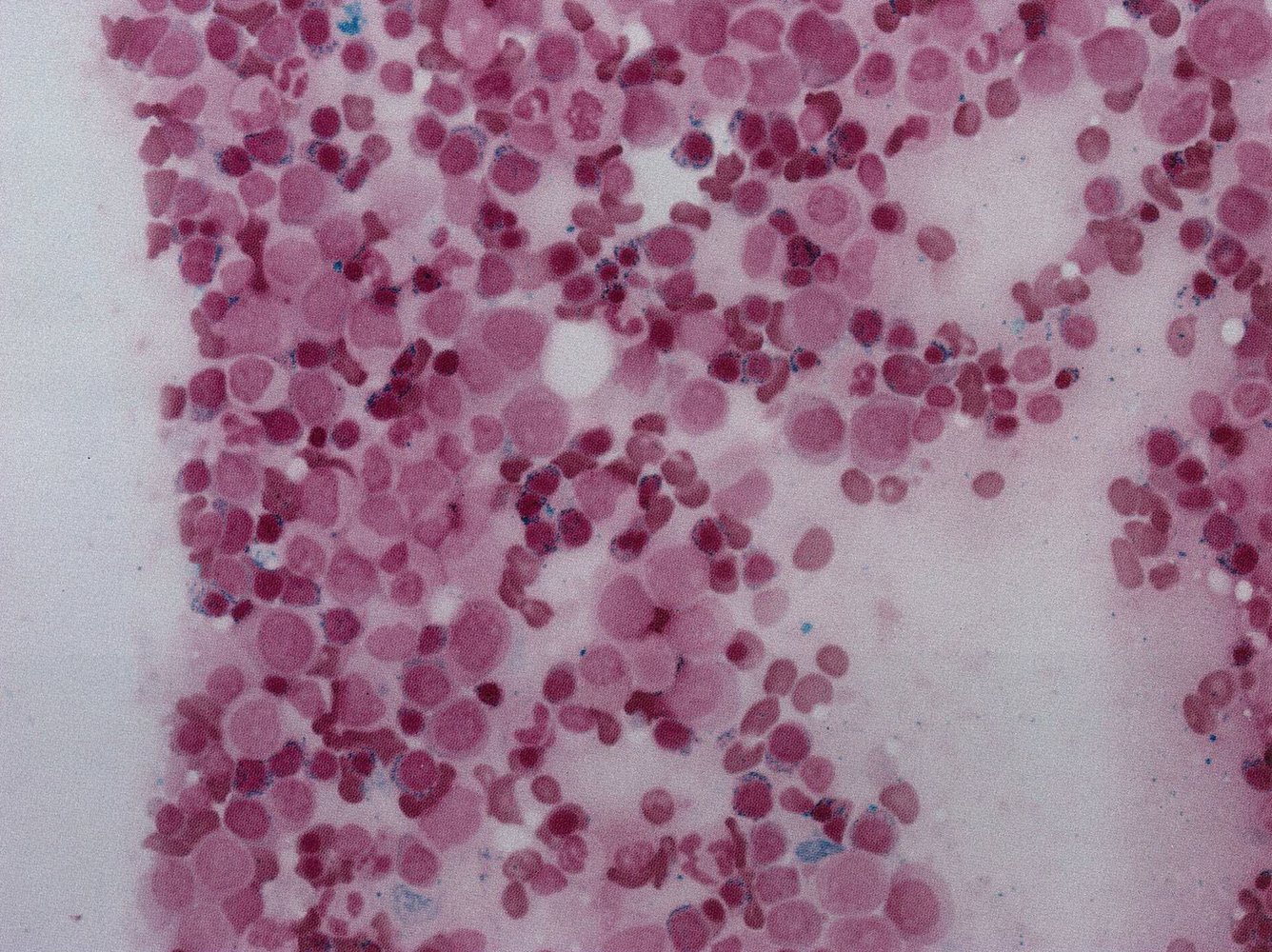
Bone marrow smear in iron stain (Prussian blue): Excess of immature blasts (B) and presence of ringed sideroblasts. Sideroblasts are erythrocytes with iron-loaded (hence blue) mitochondria (arrows). The presence of ringed sideroblasts indicates ineffective erythropoiesis.
Source: © IMPP

Photomicrograph of a blood smear (Wright-Giemsa stain; very high magnification)
A neutrophil with a bilobed nucleus (Pseudo-Pelger-Huet anomaly) can be seen.
This finding is consistent with acute and chronic myeloid disorders as well as with endogenous and drug-induced myelodysplastic disorders.
Source: “Target cells, polychromasia, and pseudo-pelger-Huet cells” by Niels Olson, Flickr, licensed under CC BY-SA 2.0.
Differential diagnoses
Other causes of cytopenia and/or dysplasia include: [7][8][10]
- Nonmalignant causes
- Deficiencies in micronutrients (e.g., B6, B12, folate, copper, iron) [10]
- Medications [18]
- Reactive changes due to acute viral illnesses
- Chronic alcohol consumption
- Infectious diseases (e.g., HIV, CMV, TB)
- Autoimmune diseases (e.g., SLE, rheumatoid arthritis)
- Chronic kidney disease
- Chronic liver disease
- Other hematological conditions [3]
- Clonal hematopoiesis
- Acute myeloid leukemia
- MDS/MPN overlap syndromes
- Aplastic anemia
- Other malignancies associated with cytopenias
Precursor clonal hematopoietic conditions can progress to MDS. MDS can itself progress to acute myeloid leukemia. [4][13]
The differential diagnoses listed here are not exhaustive.
Treatment
Approach [7][10][13]
Refer all patients to hematology-oncology for management.
- All patients
- Assess for comorbidities and discuss goals of care.
- Use scoring systems for risk stratification in MDS.
- Provide supportive therapy for symptomatic and/or significant cytopenia(s).
- Offer enrollment in clinical trials.
- Monitor regularly for treatment response and disease progression.
- Identify and treat complications (e.g., iron overload, infections, bleeding).
- High-risk MDS
- Start pharmacotherapy for MDS, which may include hypomethylating agents and chemotherapy.
- Assess suitability for allogeneic hematopoietic stem cell transplantation (HSCT). [7][13]
-
Low-risk MDS: Screen for indications for pharmacotherapy for MDS.
- If therapy is indicated:
- Treat accordingly, e.g., with hypomethylating agents, lenalidomide (for 5q deletion), or immunosuppressive agents.
- If disease is refractory to treatment, consider HSCT.
- If therapy is not indicated: Expectant management (i.e., “watch and wait”) may be appropriate. [7]
- If therapy is indicated:
Allogeneic stem cell transplantation is the only curative option for MDS.
Risk stratification in MDS [7][10][13]
- To determine treatment, patients with MDS are categorized as having either low-risk or high-risk MDS.
- Clinical scoring systems include:
- Revised International Prognostic Scoring System (IPSS-R)
- Molecular International Prognostic Scoring System (IPSS-M) [19][20]
- Common high-risk features:
- Patient > 60 years of age [10]
- Significant or multiple cytopenias
- Increased myeloblasts (≥ 5%) in the bone marrow
- Multiple and/or unfavorable genetic abnormalities
Patients with a high-risk feature may still have low-risk MDS if the total prognostic score is below the cutoff value for high-risk MDS.
")
Supportive therapy [7][10][13]
Disease-related cytopenias
-
Anemia
- pRBC transfusion
- Erythropoietin-stimulating agents (e.g., recombinant EPO) [13]
- Neutropenia: recombinant granulocyte colony-stimulating factor (G-CSF) may be used in select cases [10]
- Thrombocytopenia: platelet transfusions [10][13]
Treatment-associated complications
- Iron overload: Provide iron chelation (e.g., deferasirox) to transfusion-dependent patients with elevated ferritin levels. [13]
- Infection
- Suspected and/or confirmed infections: Treat with antibiotics (e.g., febrile neutropenia management).
- Neutropenia in patients on immunosuppressive treatment: Consider prophylactic antibiotic therapy. [13]
- See also “Anticancer treatment-related complications” in “Principles of cancer care.”
Pharmacotherapy for MDS [7][10][13]
- Pharmacotherapy is noncurative but aims to:
- Increase cell counts
- Improve symptoms and quality of life
- Reduce transfusion burden
- Delay progression to AML
| MDS treatment by risk stratification [7][13] | ||
|---|---|---|
| Indications | Treatment | |
| Higher-risk MDS |
|
|
| Lower-risk MDS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lenalidomide may cause significant neutropenia and thrombocytopenia. [7]
Inadequate response to hypomethylating agents is associated with a poor prognosis. [13]
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Complications
- Depending on the chromosomal aberrations detected in pluripotent stem cells, up to 30% of MDS cases may progress to acute myelogenous leukemia. [21]
- See “Clinical features” above.

We list the most important complications. The selection is not exhaustive.
Bone marrow smear in iron stain (Prussian blue): Excess of immature blasts (B) and presence of ringed sideroblasts. Sideroblasts are erythrocytes with iron-loaded (hence blue) mitochondria (arrows). The presence of ringed sideroblasts indicates ineffective erythropoiesis.
Source: © IMPP
External Resources
References
- Steensma DP. "Myelodysplastic Syndromes". Mayo Clinic Proceedings. 90(7). :969-983. (2015)
- Lopez Rubio M, Anna Gaya A, Morado M, et al. "Relationship between myelodysplastic syndrome and paroxysmal nocturnal hemoglobinuria: Spanish Erythropathology Group and Spanish Paroxysmal Nocturnal Hemoglobinuria Working Group Experience". Blood. 126. :4546. (2015)
- Aster JC, Stone RM, Larson A, Rosmarin AG. "Clinical Manifestations and Diagnosis of the Myelodysplastic Syndromes ". UpToDate. UpToDate. https://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-the-myelodysplastic-syndromes. [2016-11-30]
- Sekeres MA, Taylor J. "Diagnosis and Treatment of Myelodysplastic Syndromes". JAMA. 328(9). :872. (2022)
- Valent P, Orazi A, Steensma DP, et al. "Proposed minimal diagnostic criteria for myelodysplastic syndromes (MDS) and potential pre-MDS conditions". Oncotarget. 8(43). :73483-73500. (2017)
- Caligiuri M, Levi MM, Kaushansky K, et al. "Williams Hematology, 9E". McGraw-Hill Education / Medical. (2015). ISBN: 9780071833004
- Khoury JD, Solary E, Abla O, et al. "The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms". Leukemia. 36(7). :1703-1719. (2022)
- Arber DA, Orazi A, Hasserjian RP, et al. "International Consensus Classification of Myeloid Neoplasms and Acute Leukemias: integrating morphologic, clinical, and genomic data". Blood. 140(11). :1200-1228. (2022)
- Fenaux P, Haase D, Santini V, et al. "Myelodysplastic syndromes: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up". Ann Oncol. 32(2). :142-156. (2021)
- Gattermann N. "Iron overload in myelodysplastic syndromes (MDS)". Int J Hematol. 107(1). :55-63. (2018)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Garcia‐Manero G. "Myelodysplastic syndromes: 2023 update on diagnosis, risk‐stratification, and management". Am J Hematol. 98(8). :1307-1325. (2023)
- Sanz-De Pedro M, Wang W, Kanagal-Shamanna R, Khoury JD. "Myelodysplastic Syndromes: Laboratory Workup in the Context of New Concepts and Classification Criteria". Curr Hematol Malig Rep. 13(6). :467-476. (2018)
- "Myelodysplastic syndromes". https://academic.oup.com/ajcp/article/132/2/290/1761406/Myelodysplastic-Syndromes. [2015-08-01]
- Wang E, Boswell E, Siddiqi I, et al. "Pseudo–Pelger-Huët Anomaly Induced by Medications". Am J Clin Pathol. 135(2). :291-303. (2011)
- Abramson, Neil. "Pelger-Huet anomaly and pseudo (acquired) Pelger-Huet". Blood. 107(9). :3428-3428. (2006)
- Bernard E, Tuechler H, Greenberg PL, et al. "Molecular International Prognostic Scoring System for Myelodysplastic Syndromes". NEJM Evid. 1(7). (2022)
- Aguirre LE, Al Ali N, Sallman DA, et al. "Assessment and validation of the molecular international prognostic scoring system for myelodysplastic syndromes". Leukemia. 37(7). :1530-1539. (2023)
- Rollison DE, Shain KH, Lee J-H, et al. "Subsequent primary malignancies and acute myelogenous leukemia transformation among myelodysplastic syndrome patients treated with or without lenalidomide". Cancer Med. 5(7). :1694-1701. (2016)
- Vardiman JW, Thiele J, Arber DA, et al. "The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes". Blood. 114(5). :937-951. (2009)
- Mintzer DM, Billet SN, Chmielewski L. "Drug-Induced Hematologic Syndromes". Advances in Hematology. 2009. :1-11. (2009)
- "Types of Myelodysplastic Syndromes". https://www.cancer.org/cancer/myelodysplastic-syndrome/about/mds-types.html. [2015-07-02]