Summary
Neonatal respiratory distress syndrome (NRDS), or surfactant deficiency disorder, is a lung disorder in infants that is caused by a deficiency of pulmonary surfactant. It is most common in preterm infants, with the incidence and severity decreasing with gestational age. Surfactant deficiency causes the alveoli to collapse, resulting in impaired blood gas exchange. Symptoms manifest shortly after birth and include tachypnea, tachycardia, increased breathing effort, and/or cyanosis. Suspected diagnosis is based on clinical features and confirmed by evaluating the extent of atelectasis via an x-ray of the chest. Blood gases show respiratory and metabolic acidosis in addition to hypoxia. Treatment primarily involves emergency resuscitative measures, including nasal continuous positive airway pressure (CPAP) and the stabilization of blood sugar levels and electrolytes. Intratracheal surfactant should be administered if infants require an increased FiO2 to maintain a sufficient oxygen saturation despite receiving noninvasive positive pressure ventilation. Intratracheal surfactant should be administered if ventilation alone is unsuccessful. Most cases resolve within 3–5 days of treatment. However, complications such as hypoxemia, tension pneumothorax, bronchopulmonary dysplasia, or sepsis may still occur. In rare cases, NRDS may lead to neonatal death. NRDS can be prevented by administering antenatal glucocorticoids to the mother if premature delivery is expected.
Etiology
Neonatal respiratory distress syndrome is caused by impaired synthesis and secretion of surfactant. Risk factors include:
- Premature birth
- Maternal diabetes mellitus: leads to ↑ fetal insulin, which inhibits surfactant synthesis
- Hereditary [1]
- Cesarean delivery: results in lower levels of fetal glucocorticoids than vaginal delivery, in which higher levels are released as a response to stress from uterine contractions
- Hydrops fetalis
- Multifetal pregnancies
- Male sex
Epidemiology
-
Incidence [2]
- 1% of all newborns
- 10% of all preterm babies
- The risk of developing NRDS depends on gestational age. [2]
- < 28 weeks of gestation: > 50%
- > 37 weeks of gestation: < 5%
Epidemiological data refers to the US, unless otherwise specified.
Pathophysiology
Surfactant [3]
- Pulmonary surfactant is a mixture of phospholipids and proteins produced by lamellar bodies of type II alveolar cells. These phospholipids reduce alveolar surface tension, preventing the alveoli from collapsing.
-
Surfactant deficiency is most likely to occur in preterm infants, because:
- Surfactant production begins at approximately 20 weeks gestation.
- Distribution throughout the lungs begins at 28-32 weeks' gestation and does not reach sufficient concentration until 35 weeks gestation.
Surfactant deficiency
- Little or no reduction of alveolar surface tension → increased alveolar collapse → atelectasis → decreased lung compliance and functional residual capacity → hypoxemia and hypercapnia
- Hypoxemia and hypercapnia → vasoconstriction of the pulmonary vessels (hypoxic vasoconstriction) and respiratory acidosis → intrapulmonary right-to-left shunt → increased permeability due to alveolar epithelial damage → fibrinous exudation within the alveoli → development of hyaline membranes in the lungs (hyaline membrane disease)


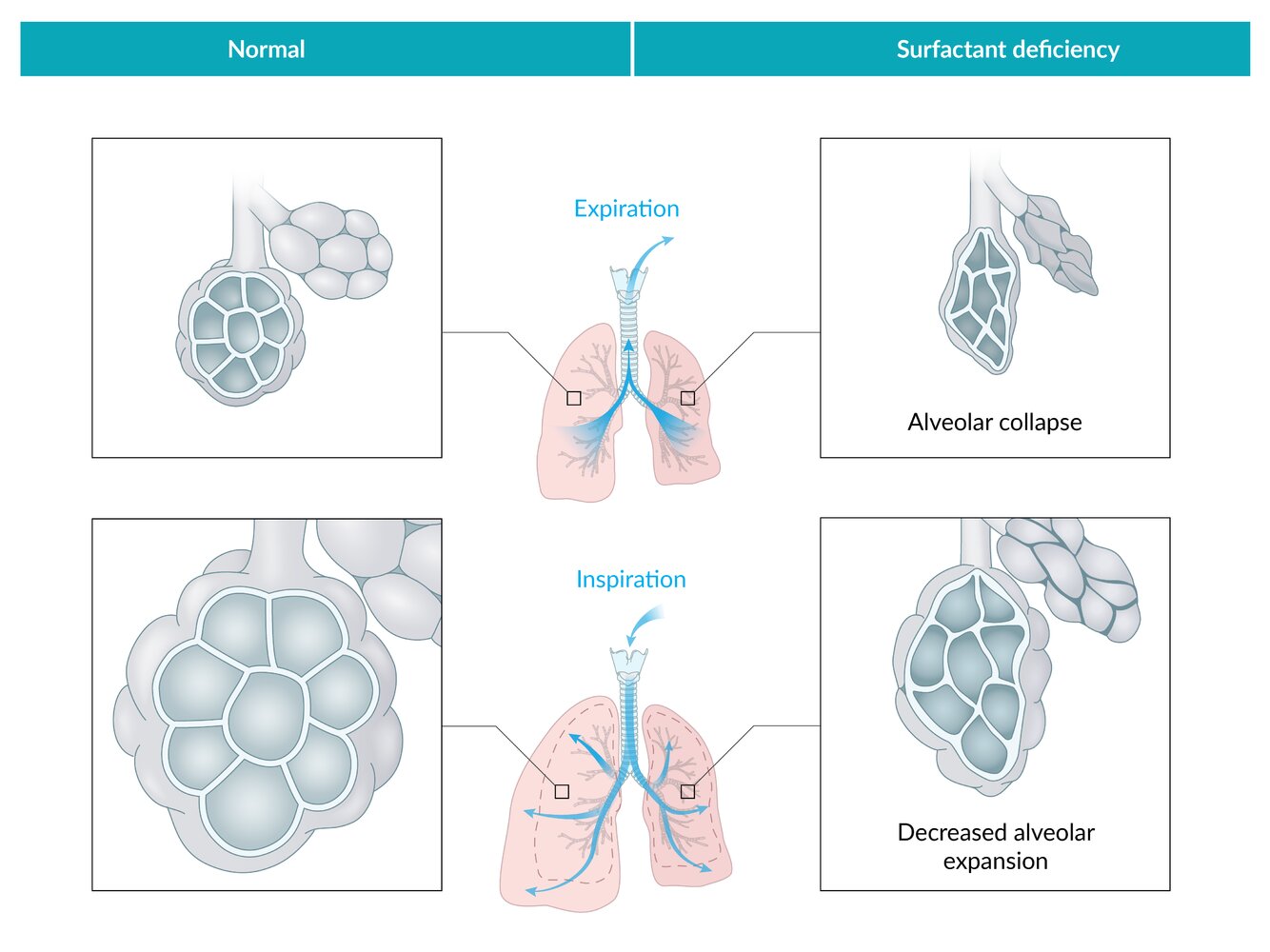
Surfactant reduces alveolar surface tension. In surfactant deficiency, increased surface tension results in increased alveolar collapse during expiration and decreased alveolar expansion during inspiration.
© AMBOSS
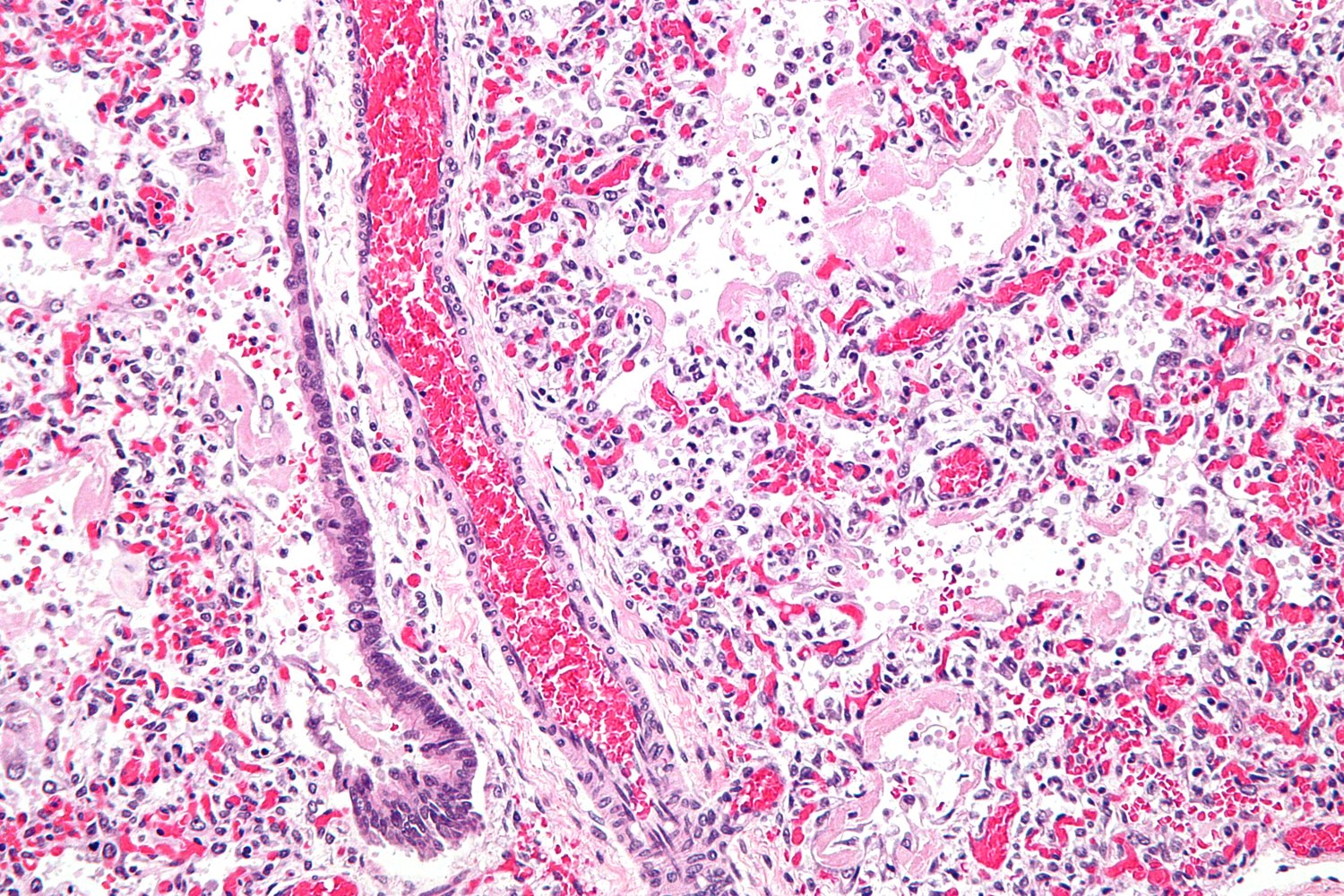
Photomicrograph of lung tissue (H&E stain; 400x magnification)
The alveolar walls are lined by eosinophilic hyaline membranes (example indicated by green overlay). The normal basophilic alveolar epithelial lining is absent. Within the interstitium, there is an extensive inflammatory infiltrate, which is visible as numerous basophilic nuclei (large basophilic nuclei: macrophages; multilobed nuclei: neutrophils). There are numerous microthrombi, visible as extracapillary aggregates of RBCs. The capillaries appear congested.
Loss of alveolar epithelium, presence of alveolar hyaline membranes, and interstitial inflammation, edema, and congestion are the typical features of the acute exudative phase of ARDS.
Source: “Hyaline membranes - intermed mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Clinical features
- Maternal history of premature birth
- Onset of symptoms: usually immediately after birth but can occur up to 72 hours postpartum
-
Signs of increased respiratory effort
- Tachypnea
- Nasal flaring and moderate to severe subcostal/intercostal and jugular retractions
- Characteristic expiratory grunting
- Decreased breath sounds on auscultation
- Cyanosis due to pulmonary hypoxic vasoconstriction
Reference:[4]
Diagnosis
- Physical examination: see “Clinical features” above
- Maternal history: previous preterm birth
-
X-ray chest
- Interstitial pulmonary edema with perihilar streaking
- Diffuse, fine, reticulogranular (ground-glass) densities with low lung volumes and air bronchograms
- Atelectasis
-
Blood gas analysis
- Hypoxia with respiratory acidosis; may lead to increased lactate levels
- Evaluate for partial respiratory failure or global respiratory failure
-
Amniocentesis for prenatal testing of NRDS: screening for markers of fetal lung immaturity
-
Lecithin-sphingomyelin ratio < 1.5 (≥ 2 is considered mature)
- The amount of sphingomyelin in the amniotic fluid remains relatively consistent during pregnancy.
- The amount of lecithin, which is the major component of surfactant, starts increasing after week 26 of gestation.
- The lower the lecithin-sphingomyelin ratio, the more likely it is that the lungs are immature.
-
Foam stability index < 0.48
- A semi-quantitative test used to assess fetal lung maturity
- Amniotic fluid is mixed with ethanol until foam formation ceases to occur
- The index refers to the highest quantity of ethanol that can be added to amniotic fluid still permitting the formation of foam.
- Low surfactant-albumin ratio
-
Lecithin-sphingomyelin ratio < 1.5 (≥ 2 is considered mature)
-
Histological findings [5]
-
Hyaline membranes lining the alveoli
- Composed of fibrin, cellular debris, and red blood cells
- Eosinophilic appearance, amorphous material lining the alveolar surface
- Engorged and congested capillary vessels in the interstitium
-
Hyaline membranes lining the alveoli
")
")
")


References:[2][6][7]
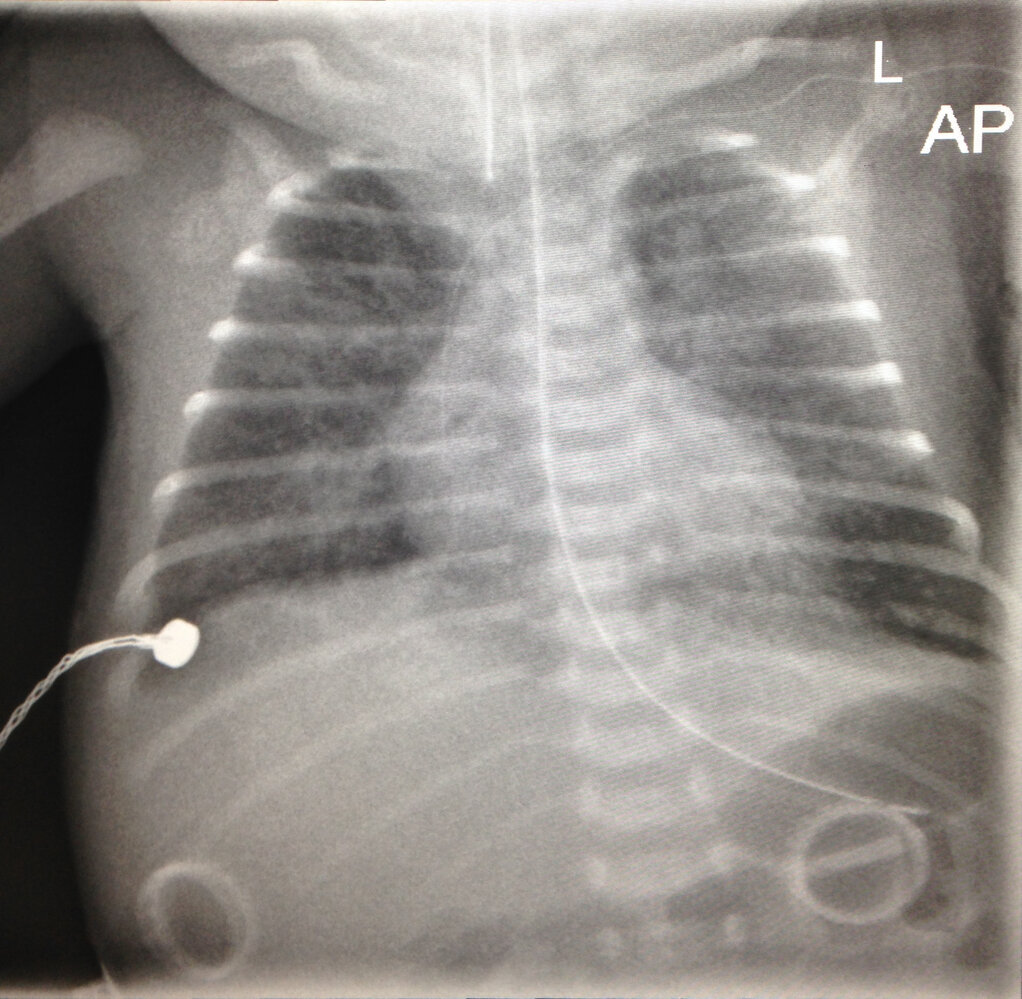
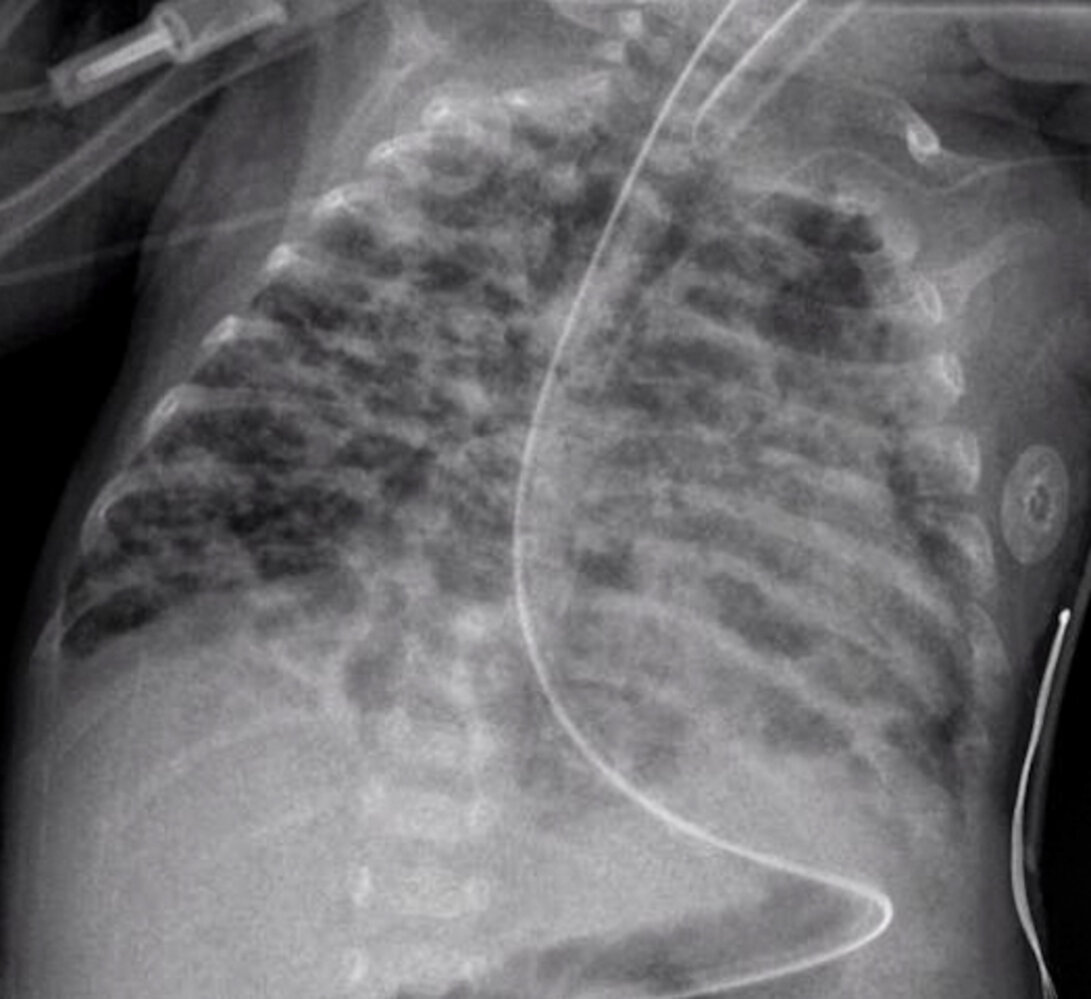
X-ray chest (AP view)
The lungs show a diffuse granular pattern with low volumes. Also, an air bronchogram (example indicated by green overlay) can be seen. Endotracheal (red) and nasogastric (yellow) tubes are present. There is also a left central line (blue).
© AMBOSS
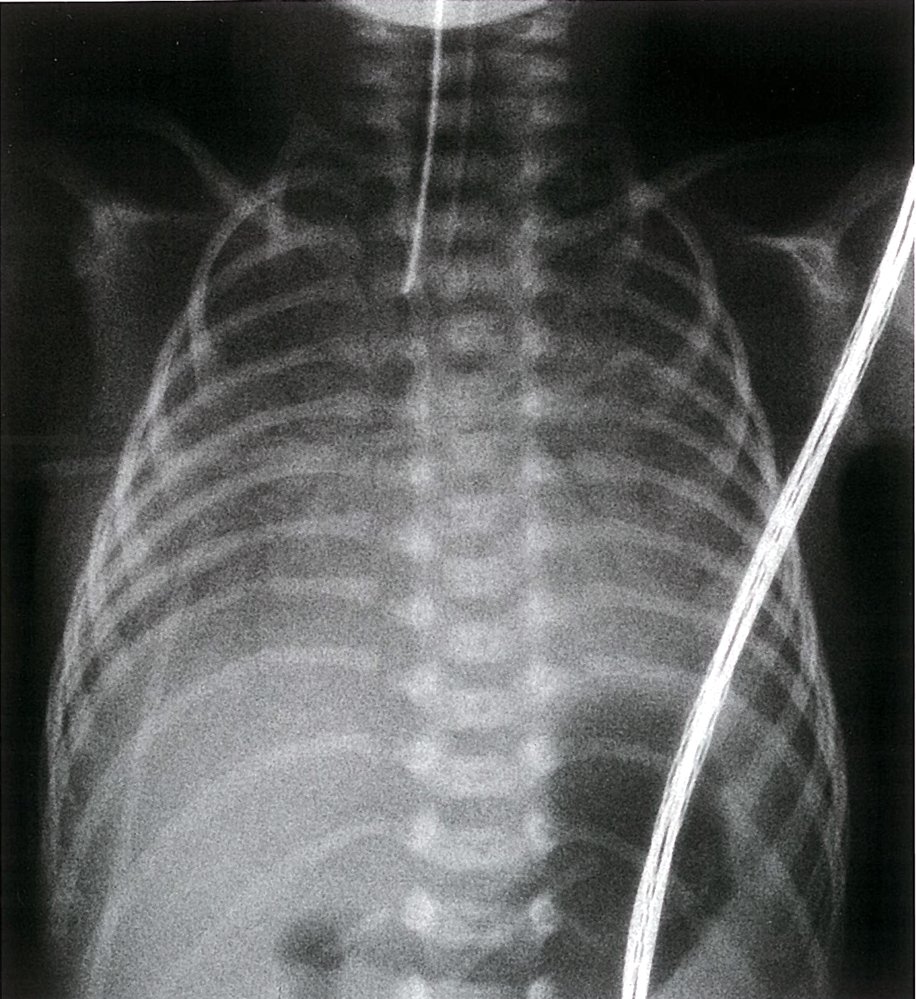
X-ray chest (frontal view) of a premature infant
The lungs are opacified and have a granular appearance. Air bronchograms (green overlay) extend to the lung periphery. An endotracheal tube (red outlines) is well-positioned above the carina.
In neonatal respiratory distress syndrome (RDS), surfactant deficiency results in alveolar collapse and noncompliant lungs. Air bronchograms are visible when aerated bronchi and bronchioles are surrounded by acinar atelectasis.
Source: © IMPP
Photomicrograph of lung tissue (H&E stain; 400x magnification)
The alveolar walls are lined by eosinophilic hyaline membranes (example indicated by green overlay). The normal basophilic alveolar epithelial lining is absent. Within the interstitium, there is an extensive inflammatory infiltrate, which is visible as numerous basophilic nuclei (large basophilic nuclei: macrophages; multilobed nuclei: neutrophils). There are numerous microthrombi, visible as extracapillary aggregates of RBCs. The capillaries appear congested.
Loss of alveolar epithelium, presence of alveolar hyaline membranes, and interstitial inflammation, edema, and congestion are the typical features of the acute exudative phase of ARDS.
Source: “Hyaline membranes - intermed mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
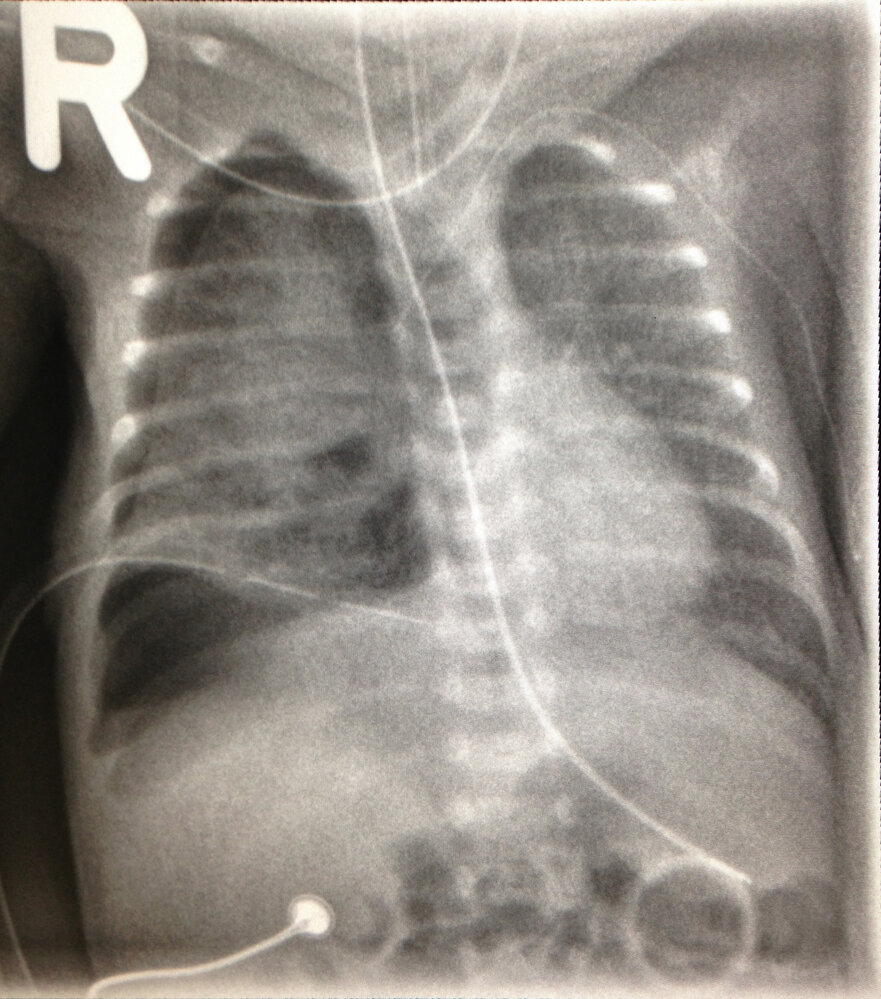
X-ray chest (AP view)
A right tension pneumothorax has developed. It is accompanied by depression of part of the right hemidiaphragm (indicated by red line and arrow) and leftward shift of the mediastinum (indicated by blue line and arrow). The right lung (green overlay) is partially collapsed. A chest tube has been placed in the lower hemithorax, and endotracheal and nasogastric tubes are present. There is a left central line.
© AMBOSS
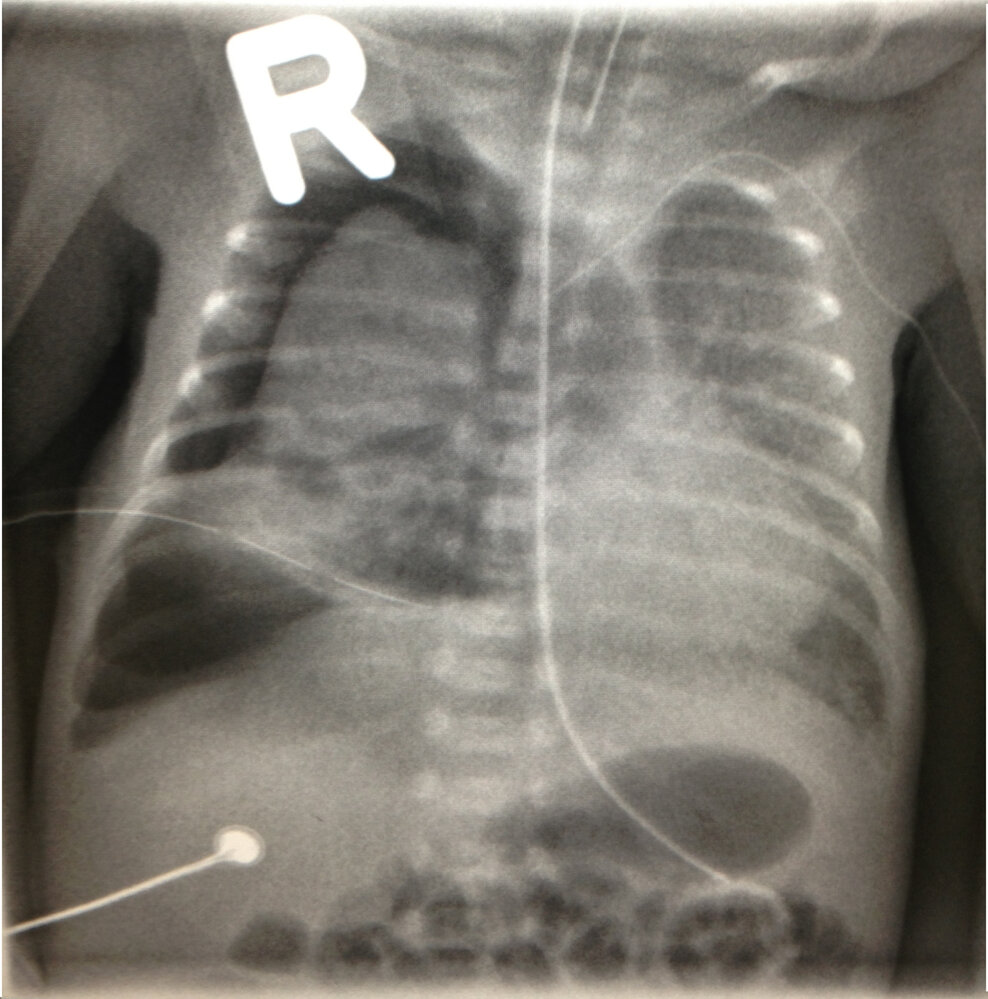
X-ray chest (AP view)
The right tension pneumothorax surrounding the lung has increased in size despite chest tube placement, and lung collapse (green overlay) has worsened. There is increased leftward shift of the mediastinum (indicated by blue line and arrow) and depression of part of the right hemidiaphragm (indicated by red line and arrow). An endotracheal tube, nasogastric tube, and right central line are shown.
© AMBOSS

X-ray chest of a premature infant
Source: “Figure 1, in:Two Mutations in Surfactant Protein C Gene Associated with Neonatal Respiratory Distress” by Tarocco A, Ballardini E, Contiero M R, et al., Hindawi - Case Reports in Pediatrics, licensed under CC BY 3.0. Modifications: Image cropped.
Differential diagnoses
-
Pulmonary hypoplasia
- Underdevelopment of the lungs characterized by a decreased number of alveoli and small airways and reduced lung volumes in one or both lobes
- Results in impaired gas exchange and severe respiratory distress that may require intubation
- Associated with congenital diaphragmatic hernia (usually left-sided), oligohydramnios, and Potter sequence
- Congenital diaphragmatic hernia
- Pneumothorax
- Neonatal pneumonia
| Overview of NRDS and its differential diagnoses | |||||
|---|---|---|---|---|---|
| Characteristics | Neonatal respiratory distress syndrome | Apnea of prematurity (AOP) | Transient tachypnea of the newborn (wet lung disease) [8] | Persistent pulmonary hypertension of the newborn (PPHN) [9][10] | Meconium aspiration syndrome [11][12][13] |
| Term |
|
|
|
|
|
| Etiology |
|
|
|
|
|
| Risk factors |
|
|
|
|
|
| Onset of symptoms |
|
|
|
|
|
| Clinical features |
|
|
|
|
|
| Imaging |
|
|
|
|
|
| Treatment |
|
|
|
|
|
| Complications |
|
|
|
|
|
The differential diagnoses listed here are not exhaustive.
Treatment
- Ventilation [8]
- Nasal CPAP with a PEEP of 3–8 cm H2O
- If respiratory insufficiency persists, start intubation with mechanical ventilation and O2 inhalation.
- Endotracheal administration of artificial surfactant within 2 hours postpartum
- Supportive measures: IV fluid replacement; stabilization of blood sugar levels and electrolytes
Physiologic O2 saturation in neonates is around 90%. A saturation of 100% is considered toxic for neonates!
Complications
Bronchopulmonary dysplasia (BPD) [16]
- Definition: chronic lung condition secondary to prolonged mechanical ventilation and oxygen therapy for NRDS
- Etiology: Pulmonary barotrauma and oxygen toxicity with subsequent inflammation of lung tissue due to ventilation of the immature lung (ventilation for more than 28 days)
-
Clinical features
- Seen in infants < 32 weeks
- Persistence of symptoms similar to NRDS (e.g., tachypnea, grunting, nasal flaring)
- Episodes of desaturation
-
Diagnostics
- X-ray chest: diffuse, fine, granular densities, areas of atelectasis interspersed with areas of hyperinflation
- Blood gas analysis: respiratory and metabolic acidosis
- Histology: atelectasis, fibrosis, emphysematous alveolar changes (decreased number and septation of alveoli)
- Treatment: controlled oxygenation, diuretics, rarely glucocorticoids

Further complications
- Pneumothorax
- Patent ductus arteriosus (the persistently low partial pressure of oxygen in the blood contributes to PDA)
- Hypoxia
- Cardiovascular arrest
- Neonatal sepsis
- Complications of O2 inhalation: retinopathy of prematurity, bronchopulmonary dysplasia, intraventricular hemorrhage
Baby oxen have RIBs: Babys receiving too much oxygen get Retinopathy of prematurity, Intraventricular hemorrhage, and Bronchopulmonary dysplasia.
We list the most important complications. The selection is not exhaustive.
X-ray chest (AP view) of an intubated newborn with bronchopulmonary dysplasia
Ill-defined reticular markings (examples indicated by red arrowheads) and small rounded lucent areas (examples indicated by green arrowheads) are diffusely present throughout both lungs.
An endotracheal tube (green overlay), nasogastric tube (red overlay), and central venous catheter (yellow overlay) are properly positioned. Rotation of the patient to the left has resulted in an appearance of elongation of the left ribs compared to the right ribs and leftward positioning of the cardiomediastinal silhouette.
Source: “CXR - Bronchopulmonary dysplasia” by Pulmonological, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Prognosis
- Mortality rate: < 10% [17]
- Most cases resolve within 3–5 days if treated promptly
Prevention
- Prevent premature birth if possible. See tocolysis.
-
Antenatal corticosteroid therapy administered to the mother (stimulates infant lung maturation) [18]
- Given 48 hours before delivery
- 2 doses of IM betamethasone 24 hours apart or 4 doses of IM dexamethasone 12 hours apart
References
- Besnard AE, Wirjosoekarto SAM, Broeze KA, Opmeer BC, Mol BWJ. "Lecithin/sphingomyelin ratio and lamellar body count for fetal lung maturity: a meta-analysis". Eur J Obstet Gynecol Reprod Biol. 169(2). :177-183. (2013)
- Jo HS. "Genetic risk factors associated with respiratory distress syndrome". Korean J Pediatr .. 57(4). :157. (2014)
- Andreeva AV, Kutuzov MA, Voyno-Yasenetskaya TA. "Regulation of surfactant secretion in alveolar type II cells". Am J Physiol Lung Cell Mol Physiol. 293(2). :L259-L271. (2007)
- Hermansen CL, Mahajan A. "Newborn Respiratory Distress.". Am Fam Physician. 92(11). :994-1002. (2015)
- Dishop MK. "Developmental and Pediatric Lung Disease". Elsevier. :99-124.e5. (2018). ISBN: 9780323442848
- Wilmott RW, Kendig EL, Boat TF, Bush A, Chernick V. "Kendig and Chernick's Disorders of the Respiratory Tract in Children". Elsevier Health Sciences. (2012). ISBN: 9781437719840
- Sher G, Statland BE, Freer DE. "Clinical evaluation of the quantitative foam stability index test". Obstet Gynecol. 55(5). :617-20. (1980)
- Reuter S, Moser C, Baack M. "Respiratory distress in the newborn". Pediatr Rev. 35(10). :417-429. (2014)
- Abman et al. "Guidelines From the American Heart Association and American Thoracic Society: Pediatric Pulmonary Hypertension". Circulation. 132(21). :2037-2099. (2015)
- Lesneski A, Hardie M, Ferrier W, Lakshminrusimha S, Vali P. "Bidirectional Ductal Shunting and Preductal to Postductal Oxygenation Gradient in Persistent Pulmonary Hypertension of the Newborn". Children. 7(9). :137. (2020)
- Usta et al. "Risk factors for meconium aspiration syndrome.". Obstet Gynecol. 86(2). :230-4. (1995)
- Dargaville PA. "The Epidemiology of Meconium Aspiration Syndrome: Incidence, Risk Factors, Therapies, and Outcome". Pediatrics. 117(5). :1712-1721. (2006)
- Committee on Obstetric Practice. "Committee Opinion No 689: Delivery of a Newborn With Meconium-Stained Amniotic Fluid". Obstet Gynecol.. 129(3). :e33-e34. (2017)
- Townsel CD, Emmer SF, Campbell WA, Hussain N. "Gender Differences in Respiratory Morbidity and Mortality of Preterm Neonates". Front Pediatr. 5. (2017)
- Lakshminrusimha S, Keszler M. "Persistent Pulmonary Hypertension of the Newborn". NeoReviews. 16(12). :e680-e692. (2015)
- Kinsella JP, Greenough A, Abman SH. "Bronchopulmonary dysplasia". The Lancet. 367(9520). :1421-1431. (2006)
- Dyer J. "Neonatal Respiratory Distress Syndrome: Tackling A Worldwide Problem.". J Clin Pharm Ther. 44(1). :12-14. (2019)
- Romejko-Wolniewicz E, Teliga-Czajkowska J, Czajkowski K. "Antenatal steroids: can we optimize the dose?". Curr Opin Obstet Gynecol. 26(2). :77-82. (2014)
- "Respiratory Distress Syndrome in Neonates (Hyaline Membrane Disease)". http://www.msdmanuals.com/professional/pediatrics/perinatal-problems/respiratory-distress-syndrome-in-neonates#v1089988. [2015-01-01]
- Kaplan. "USMLE Step 2 CK Lecture Notes 2017: Pediatrics". Kaplan. (2016). ISBN: 9781506208244