CME information and disclosures
To see contributor disclosures related to this article, click on this reference: [1]
Physicians can earn CME/MOC credit by using this article to address a clinical question and completing a brief evaluation about how they applied the information in their practice.
AMBOSS designates this internet point-of-care activity for a maximum of 0.5 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
For answers to questions about AMBOSS CME, including how to redeem CME/MOC credit, see “Tips and links” at the bottom of this article.
Summary
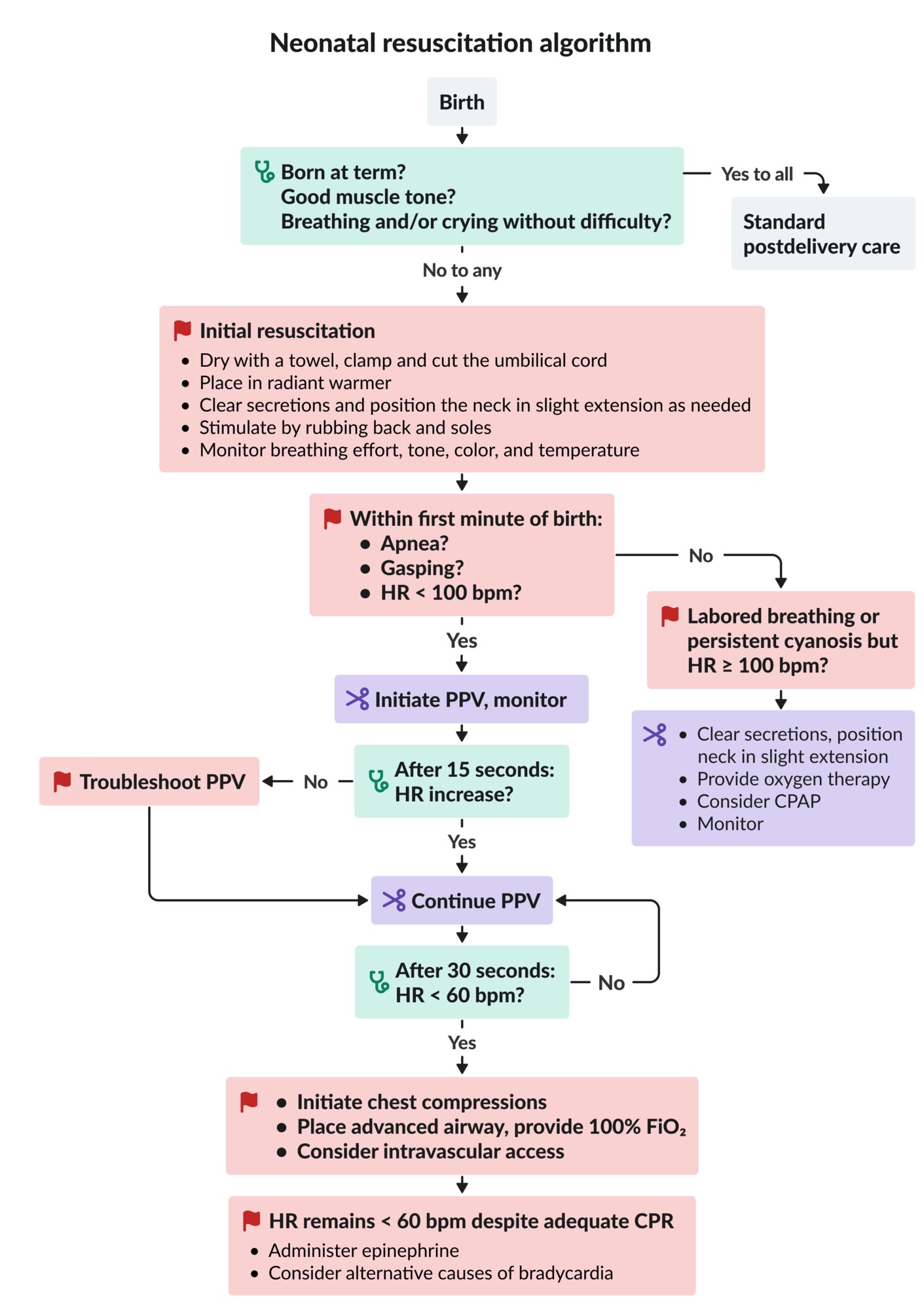
The neonatal resuscitation algorithm provides a structured approach to care of neonates immediately after birth. Initial interventions include drying, warming, and stimulating the neonate while assessing the heart rate and respiratory effort. Additional respiratory support may include oxygen therapy, continuous positive airway pressure (CPAP), positive-pressure ventilation (PPV), and/or endotracheal intubation. Additional cardiac support may include chest compressions, fluid resuscitation, and/or epinephrine administration. Postresuscitation care includes monitoring for hypoxic-ischemic encephalopathy, hypothermia, and hypoglycemia.
Risk factors for neonatal distress
-
Maternal factors [2]
- < 19 years or ≥ 40 years of age
- Diabetes
- Hypertension
- Substance use
- Previous miscarriage or stillbirth [3]
-
Fetal factors [2]
- Prematurity or postmaturity
- Congenital abnormalities
- Multiple gestation
-
Complications of pregnancy [2]
- Placental anomalies
- Oligohydramnios or polyhydramnios
- Chorioamnionitis
- Meconium-stained amniotic fluid
- Abnormal fetal heart rate
-
Complicated delivery [2]
- Transverse or breech position
- Suction-assisted or forceps delivery
- Cesarean birth
Neonatal resuscitation algorithm
The neonatal resuscitation algorithm provides guidance on how to resuscitate and stabilize neonates immediately after birth. Follow the pediatric advanced life support algorithm for all other pediatric patients.

Initial neonatal assessment [4]
- Assess the following:
- Is the newborn at term gestation (by history and appearance)?
- Is muscle tone good?
- Is the newborn crying and/or breathing without difficulty?
- All items yes: Continue postdelivery care of the newborn.
- Any item no: Begin initial neonatal resuscitation.
Initial neonatal resuscitation
- Dry the skin with a towel.
- Clamp and cut the umbilical cord.
- Consider delaying umbilical cord clamping for ≥ 30 seconds (even if the newborn is nonvigorous) if the newborn does not require immediate resuscitation. [5]
- Consider milking the umbilical cord if gestation is > 28 weeks and the newborn does not require immediate resuscitation. [5][6][7]
- Place the newborn in a radiant warmer.
- Perform initial neonatal airway interventions as needed.
- Stimulate the newborn by rubbing the newborn's back and soles if the respiratory effort remains suboptimal. [4]
- Assess the effectiveness of initial resuscitation.
- Monitor the newborn's breathing effort, tone, color, and temperature continuously.
- Check heart rate (auscultation over precordium recommended) within the first minute of birth. [8][9]
- Begin advanced neonatal resuscitation if the HR is < 100 bpm or respiratory effort is abnormal.

Advanced neonatal resuscitation [4][5][10]
Monitoring
- Place a pulse oximeter on the right hand or wrist to measure preductal oxygen saturation.
- Establish continuous ECG monitoring.
- Monitor the newborn's respiratory effort, tone, color, and heart rate throughout the resuscitation.
- Reassess within 30–60 seconds of any therapeutic intervention. [4]
Labored breathing or persistent cyanosis but HR ≥ 100 bpm
- Perform initial neonatal airway interventions.
- Start neonatal oxygen therapy and titrate to normal preductal oxygen saturation in newborns.
- Consider neonatal CPAP. [4]
- Initiate if breathing is labored or need for oxygen persists beyond the first few minutes. [4]
- Use only in newborns with spontaneous breathing and HR ≥ 100 bpm.
Apnea, gasping, or HR < 100 bpm
- Initiate neonatal PPV.
- Reassess HR 15 seconds after beginning neonatal PPV.
- If HR does not increase: Troubleshoot inadequate neonatal PPV.
- If HR increases: Continue current neonatal PPV.
- Reassess HR 30 seconds after verifying adequate chest expansion.
- If HR < 60 bpm: Initiate neonatal chest compressions.
- If HR 60–100 bpm: Continue current neonatal PPV.
HR < 60 bpm after 30 seconds of adequate PPV
- Begin neonatal chest compressions.
- Place an advanced airway (e.g., ETT, LMA) and provide 100% FiO2.
- Consider establishing intravascular access (e.g., with an umbilical vein catheter or intraosseous needle).
HR < 60/minute despite adequate CPR
- Administer neonatal epinephrine.
- Consider alternative causes of bradycardia, e.g.:
- Hypovolemia: Provide neonatal fluid resuscitation.
- Pneumothorax: Perform thoracentesis.
CPAP: continuous positive airway pressure
CPR: cardiopulmonary resuscitation
ECG: electrocardiogram
FiO2: fraction of inspired oxygen
HR: heart rate
PPV: positive pressure ventilation
SpO2: oxygen saturation on pulse oximetry

Source: “Untitled - panoramio - Pedro Martha (19)” by Pedro Martha, Wikimedia Commons, licensed under CC BY 3.0. Modifications: image cropped.
.jpg){kind=link}
Neonatal respiratory support
Adequate ventilation is the most important feature of neonatal resuscitation. [10] See “Airway management” for a general overview of respiratory support.
Initial neonatal airway interventions
- Clear airway secretions by wiping the newborn's mouth and nose.
- Position the newborn supine with the neck slightly extended.
Suction the airway only when there is obvious obstruction, as suctioning may cause bradycardia. [10]
If airway suctioning is required, always use a pressure < 100 mm Hg to reduce the risk of vagal stimulation and apnea. [9]
Neonatal oxygen therapy [4][10]
- Indications: neonates with labored breathing or persistent cyanosis but HR ≥ 100 bpm
-
Technique
- Choose the initial oxygen concentration based on gestational age.
- Gestational age ≥ 35 weeks: FiO2 21%
- Gestational age < 35 weeks: FiO2 21–30%
- Titrate the oxygen concentration to attain the normal preductal oxygen saturation in newborns.
- Choose the initial oxygen concentration based on gestational age.
Exposure to high oxygen levels can cause short- and long-term harm. Use the lowest oxygen concentration needed to maintain normal preductal oxygen saturation. [2][10]
Normal preductal oxygen saturation in newborns [11]
| Normal preductal oxygen saturation in newborns [11] | |
|---|---|
| Time since birth (minutes) | Oxygen saturation |
| 1 | 60–65% |
| 2 | 65–70% |
| 3 | 70–75% |
| 4 | 75–80% |
| 5 | 80–85% |
| 10 | 85–95% |
Oxygen saturation measured distal to the ductus arteriosus is 10–15% lower than saturation measured proximal to the ductus for up to 15 minutes after birth. Always use the oxygen saturation in the right hand or wrist to guide resuscitation. [2][12]
Neonatal CPAP [4][10]
- Indications: labored breathing or persistent cyanosis in spontaneously breathing newborns with HR ≥ 100 bpm
-
Technique
- Set initial CPAP to 5 cm H2O.
- T-piece resuscitator: Set the desired CPAP on the PEEP valve.
- Flow-inflating bag: Adjust flow control valve until the desired CPAP is attained.
- Increase CPAP and/or oxygen concentration to maintain normal preductal oxygen saturation in newborns.
- Set initial CPAP to 5 cm H2O.
CPAP > 7 cm H2O may be needed but may also reduce cardiac output and/or result in pneumothorax. [13]
Neonatal CPAP improves functional residual capacity, reduces work of breathing, and may prevent need for intubation. [14]
Neonatal positive-pressure ventilation [4][10]
See also “Noninvasive positive-pressure ventilation.”
Indications
- Inadequate respiratory effort (e.g., gasping, apnea)
- Heart rate ≤ 100 bpm
- Neonatal oxygen therapy and/or neonatal CPAP is insufficient to maintain normal preductal oxygen saturation in newborns.
Technique [4]
- Suction secretions from the airway.
- Position head and neck (neutral or slight extension).
- Choose a mask that covers the mouth and nose but not the eyes.
- Connect T-piece resuscitator, self-inflating bag, or flow-inflating bag. [5][15]
- Start ventilating with peak inspiratory pressure 20–25 cm H2O. [4]
- Provide 40–60 breaths per minute.
- Verify adequate chest rise, monitor HR, and troubleshoot inadequate neonatal PPV as needed.
Troubleshooting inadequate neonatal PPV
- Readjust mask and/or head position.
- Suction secretions.
- Increase PIP by 5–10 cm H2O.
- Consider placing an advanced airway, e.g., LMA, ETT.
Complications
- Pneumothorax
- Gastric distention
Insert an orogastric tube to decompress the stomach after 2 minutes of bag-mask ventilation. [9]
Neonatal airway adjuncts [16]
See also “Basic airway adjuncts.”
- Indications: respiratory distress caused by nasal obstruction, e.g., choanal atresia, mucus plugging
-
Options
- Oropharyngeal airways (30–40 mm)
- Nasopharyngeal airways (size 3) [16]
Neonatal supraglottic airway devices [17][18]
See also “Supraglottic airway devices.”
-
Indications
- Difficult mask ventilation
- Prolonged PPV is required.
- Rescue device in cannot intubate, cannot ventilate scenarios
-
Contraindications
- < 34 weeks' gestation
- < 1,500 g birth weight
-
Options
- Size 1 LMA
- Size 1 I-Gel®
The use of supraglottic airways during chest compression is not well studied. Endotracheal intubation is preferred. [10]
Neonatal endotracheal intubation [10]
See also “Endotracheal intubation.”
-
Indications
- Prolonged PPV
- Inadequate PPV with a mask or LMA
- Chest compressions
- Equipment: See “Weight-based neonatal ETT equipment and placement guidance.”
End-tidal CO2 detection and an increasing heart rate are the primary methods to confirm ETT placement. Always obtain a chest x-ray for final confirmation. [4]
Weight-based neonatal ETT equipment and placement guidance
| Weight-based neonatal ETT equipment and placement guidance [4][9][19] | ||||
|---|---|---|---|---|
| Weight | Laryngoscope blade size | Uncuffed ETT size (mm in diameter) | ETT depth (cm) | Suction catheter |
| < 1 kg |
|
|
|
|
| 1 kg–2 kg |
|
|
|
|
| 2 kg–3 kg |
|
|
|
|
| > 3 kg |
|
|
|
|
Neonatal hemodynamic support
Neonatal chest compressions [10][20]
- Indication: heart rate < 60 bpm despite adequate ventilation for 30 seconds
-
Key targets
- Rate: 90 compressions and 30 ventilations per minute
- Ratio: 3:1 compressions to ventilations
- Depth: one-third of the depth of the chest
-
Techniques
- Two thumb-encircling hands technique (preferred) [10]
- Two-finger technique
-
Reassess
- Check heart rate every 30 seconds.
- Continue chest compressions until heart rate reaches > 60 bpm.
Always increase FiO2 to 100% when chest compressions are started. [4]
Neonatal chest compression techniques
-
Two thumb-encircling hands technique
- Encircle the chest with both hands and place both thumbs over the lower third of the sternum.
- Compress the lower sternum with both thumbs.
-
Two-finger technique
- Place the index and middle fingers on the lower half of sternum (just below the intermammary line).
- Compress the lower sternum with both fingers.
The two thumb-encircling hands technique is associated with better blood pressure and decreased provider fatigue compared to the two-finger technique. [10]


Intravascular access
Umbilical vein catheterization is the preferred method for obtaining intravascular access; alternative methods include peripheral venous access or intraosseous access.
Umbilical vein catheter [9][21]
Preparation
- Place the neonate in a radiant warmer.
- Apply antiseptic to the umbilical stump.
- Drape the umbilical area, leaving the head exposed for observation.
- Pre-flush an umbilical vein catheter with sterile heparinized saline.
- Preterm infants: 3.5 Fr catheter
- Fullterm infants: 5.0 Fr catheter
Procedure
- Place a loosely tied loop of suture or umbilical tape at the junction of the abdomen and umbilical cord.
- Cut the cord 1 cm above the junction of the cord and abdomen.
- Identify the thin-walled umbilical vein and dilate it with forceps.
- Advance the pre-flushed catheter into the umbilical vein until blood returns freely.
- Advance the catheter an additional 1–2 cm.
- Secure the catheter with the suture or umbilical tape.
- Aspirate and flush the catheter.
- A catheter may be used immediately for resuscitation, but verify placement with an x-ray as soon as feasible.
Alternatives [9]
- Peripheral venous access
-
Intraosseous access, e.g.:
- Distal femur
- Proximal tibia



Neonatal epinephrine [10]
- Indication: heart rate < 60 bpm despite adequate ventilation and chest compressions for at least 30–60 seconds
-
Dosage
- IV or IO epinephrine [10]
- Endotracheal epinephrine [10]
Neonatal fluid resuscitation [10]
-
Indication
- Suspected hypovolemia (e.g., pale appearance, weak pulses)
- Persistent bradycardia despite quality ventilation, chest compression, and epinephrine administration
- Dosage: 10 mL/kg fluid or blood bolus over 5–10 minutes; repeat as needed
-
Options
- Normal saline
- Lactated Ringer's solution
- Uncrossmatched Rh-negative type O blood (preferred for substantial blood loss)
Hypovolemia is uncommon and typically caused by maternal or fetal hemorrhage. [10]
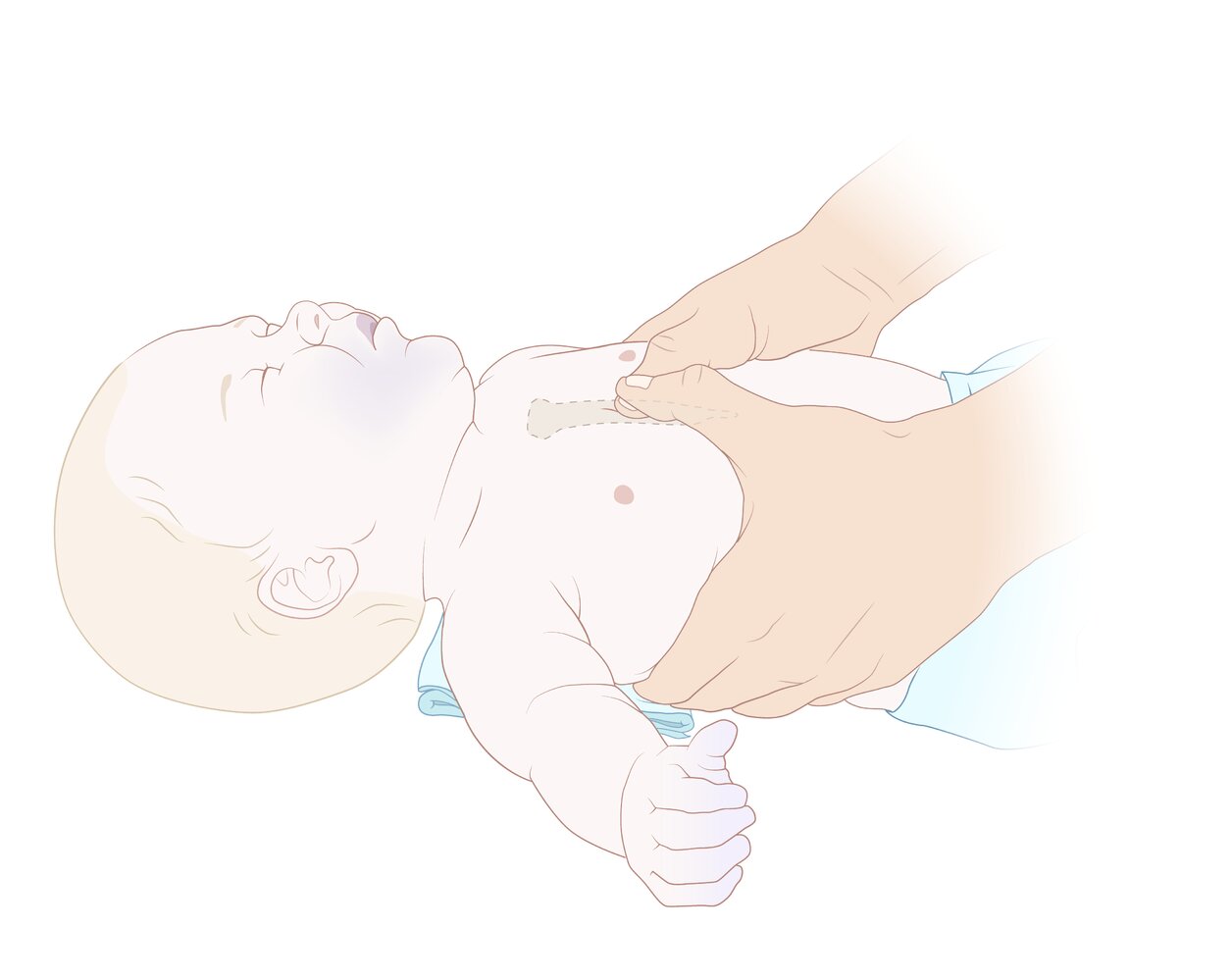
Recommended technique if two healthcare providers are present: Both hands are used to encircle the chest, and chest compressions are performed with both thumbs placed on top of each other over the lower third of the sternum.
This technique produces higher coronary artery perfusion pressure than the two-finger technique and more consistently results in effective compressions.
© AMBOSS
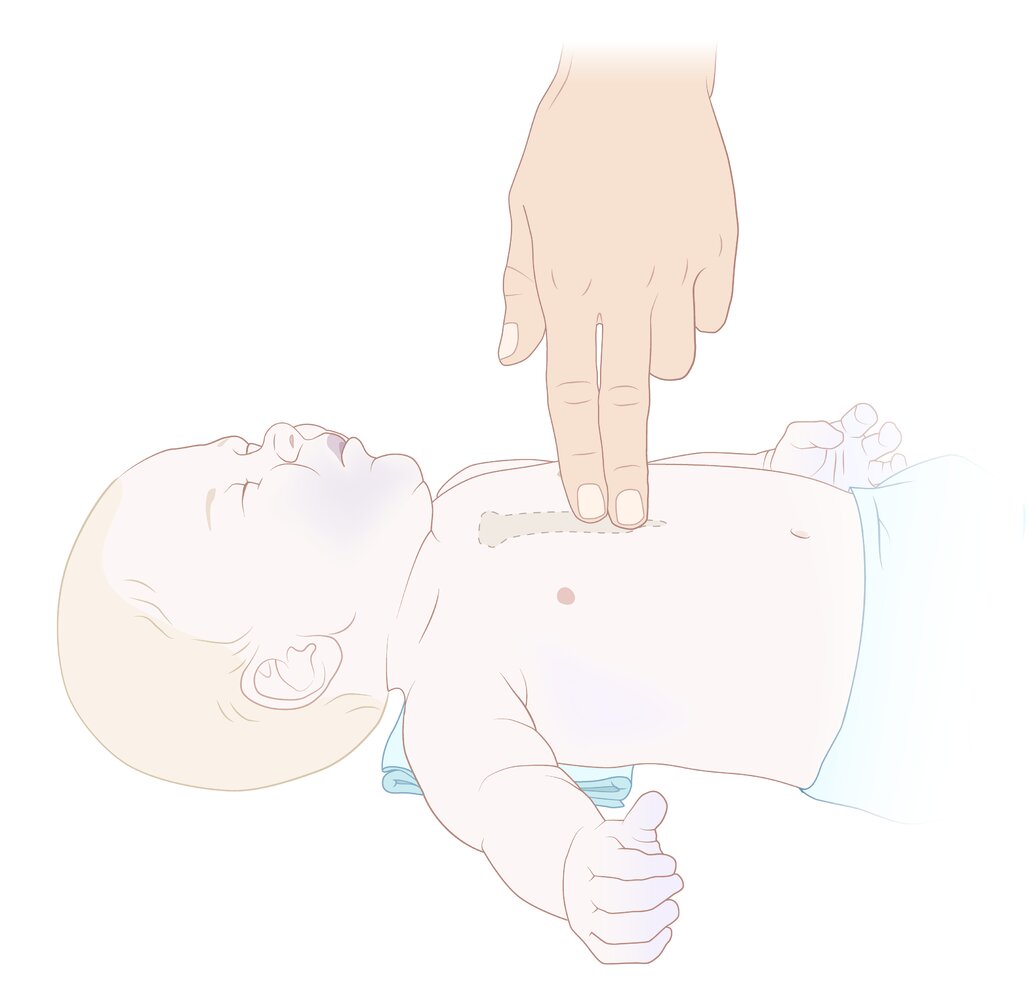
Recommended technique if only one healthcare provider is present: The chest is compressed using two fingers, which are placed on the lower half of the sternum (just below intermammary cleft).
In comparison to the two-thumb-encircling hands technique, this allows for faster changes between compressions and delivering breaths when there is only one rescuer.
© AMBOSS
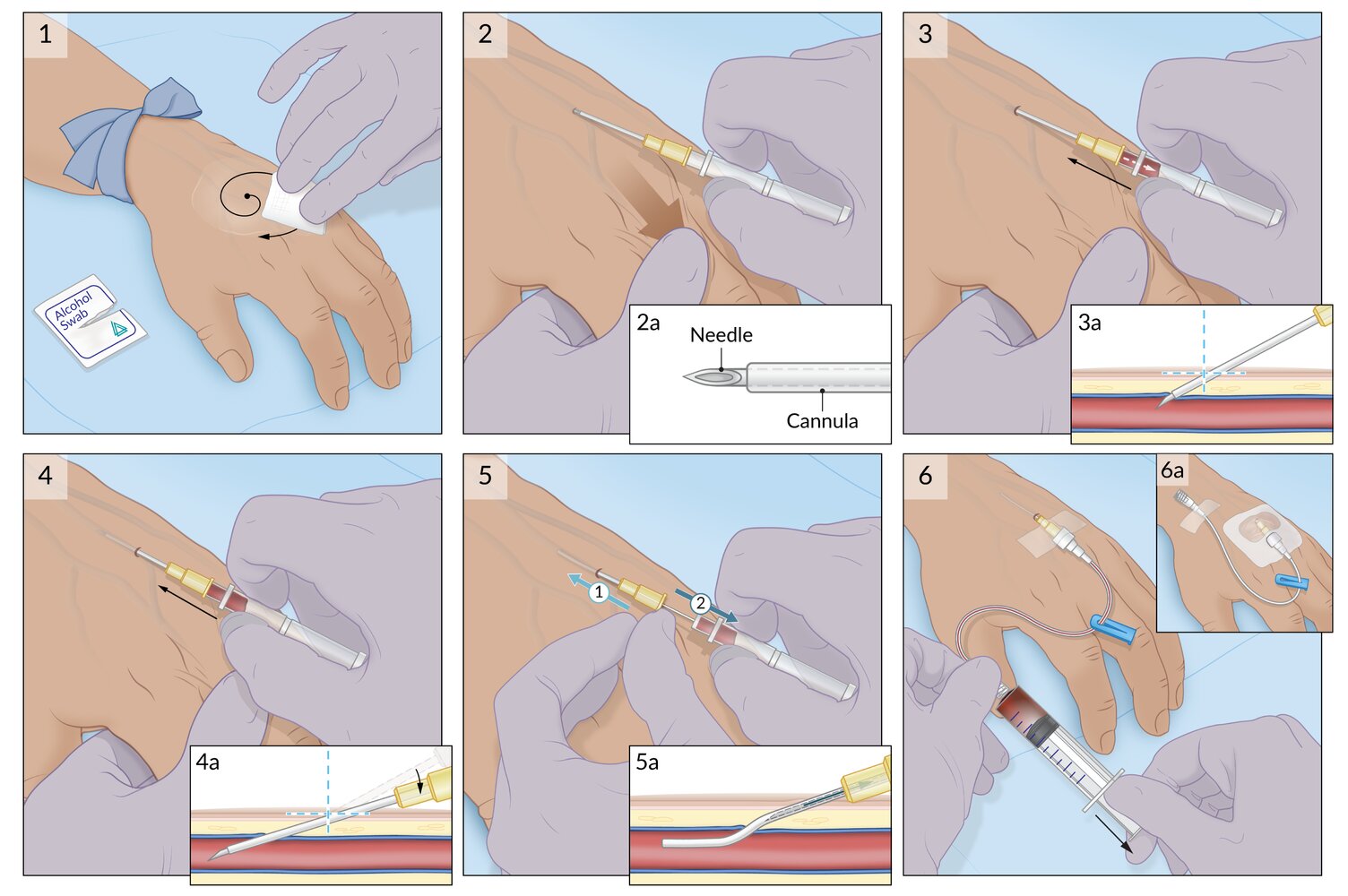
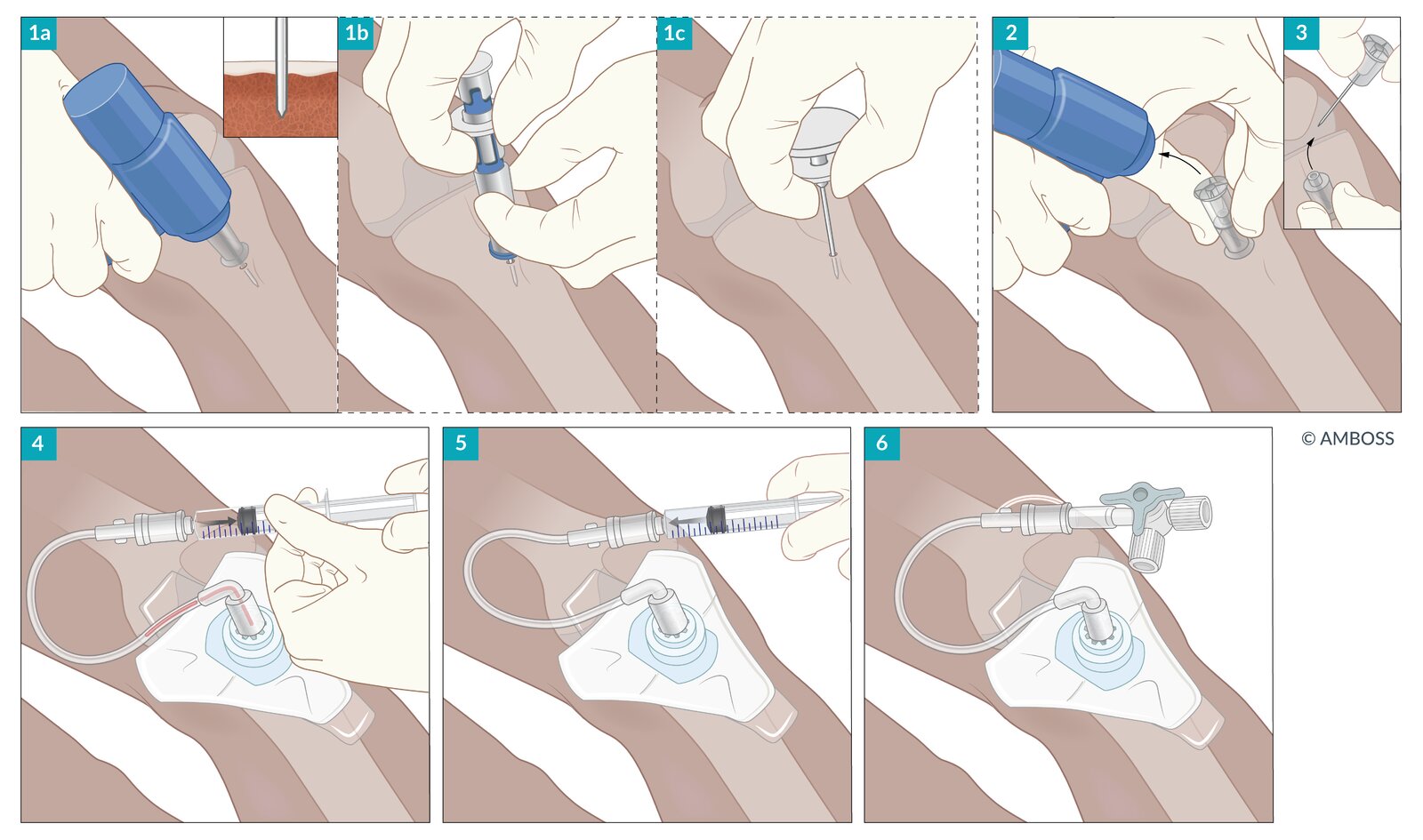
1. A tourniquet is placed 5–10 cm above the insertion site and the skin is sterilized with an antiseptic solution.
2. Traction is applied to the skin with the nondominant hand and the needle is placed over the vein with the bevel facing upward. The distance from the bevel opening to the catheter tip is noted (2a).
3. The needle is advanced into the vein at a 10–30° angle (3a) until blood flashback is seen.
4. The angle of the needle is depressed (4a) and the needle is advanced 1–2 mm to ensure the distal end of the catheter is within the lumen of the vein.
5. The catheter is advanced while the needle remains in the vein, then the needle is withdrawn (5a).
6. The catheter is aspirated or flushed to verify intravenous placement and a sterile dressing is applied (6a).
© AMBOSS
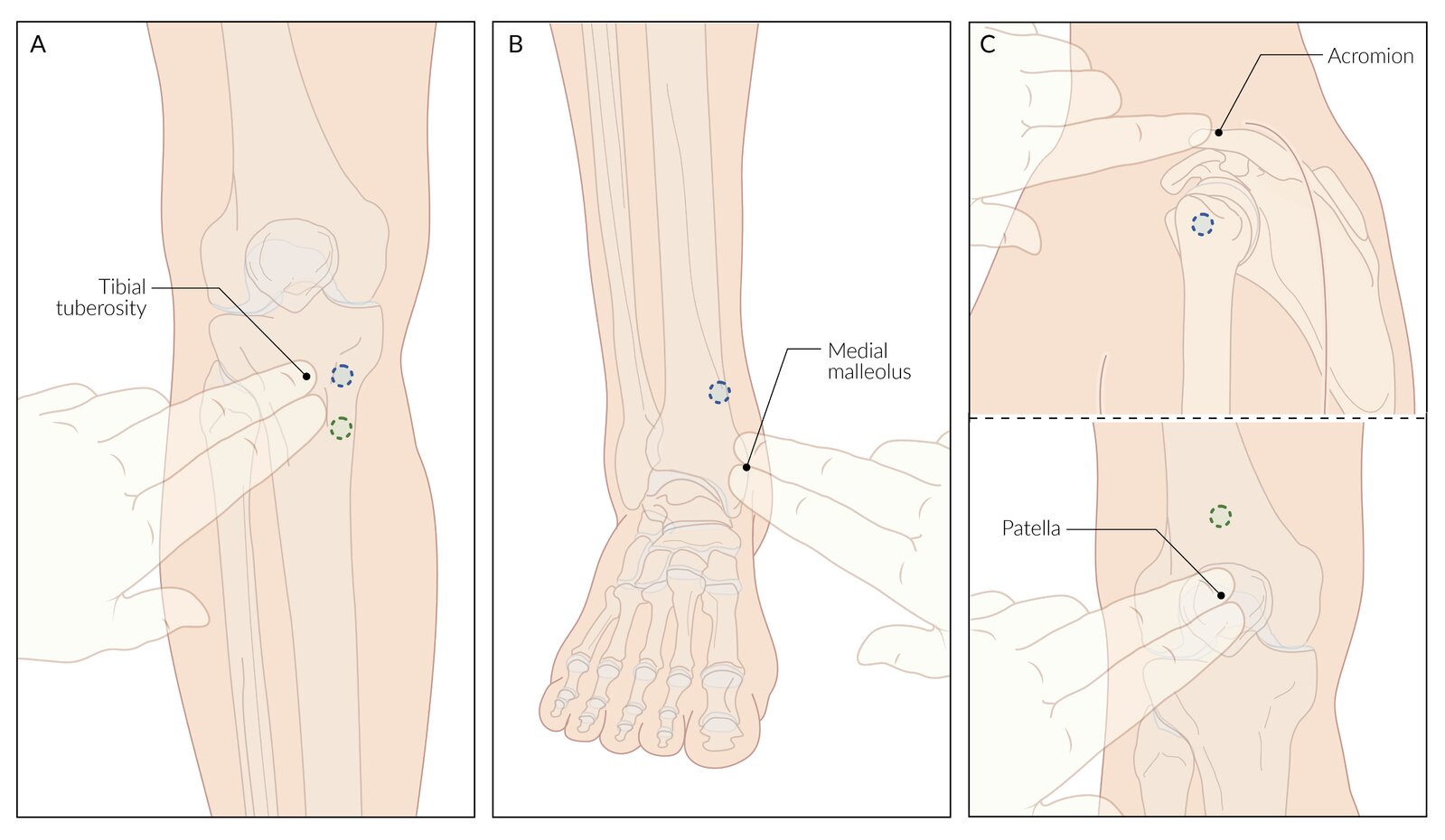
A. Proximal tibia: 1–2 cm medial and 2 cm distal to the tibial tuberosity
– The blue circle designates the most proximal acceptable location in adults.
– The green circle designates the preferred distal placement in children (to avoid the growth plate).
B. Distal tibia: 2 cm proximal to the medial malleolus
C. Other sites
– Proximal humerus (adults): greater tubercle, 2 cm distal to the acromion
– Distal femur (children): 1–2 cm proximal to the patella
© AMBOSS
© AMBOSS
Postresuscitation care
- Urgently consult neonatology or pediatrics.
- Monitor respiratory effort, heart rate, and preductal oxygen saturation continuously.
- Evaluate for hypoxic-ischemic encephalopathy (HIE), and treat perinatal HIE as indicated. [10]
- Rewarm neonates with hypothermia (< 36°C). [10]
- Monitor for neonatal hypoglycemia (blood glucose ≤ 40 mg/dL) and treat as needed. [22][23]
- Admit to neonatal ICU or monitored triage area.
Termination of resuscitation
- The decision to withhold or terminate resuscitation is individualized and based on multiple factors, including: [10]
- Family wishes
- Extremely preterm birth (i.e., < 28 weeks gestation)
- Severe congenital disease
- Availability of advanced neonatal care
- Termination of resuscitation is reasonable in newborns with no cardiac activity after 20 minutes of appropriate resuscitation. [10]
External Resources
References
- Weiner GM, Zaichkin J. "Textbook of Neonatal Resuscitation". American Academy of Pediatrics. (2016). ISBN: 9781610020251
- Yamada NK, Szyld E, Strand ML, et al. "2023 American Heart Association and American Academy of Pediatrics Focused Update on Neonatal Resuscitation: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care". Circulation. 149(1). (2024)
- Katheria AC. "Umbilical Cord Milking: A Review". Fronti Pediatr. 6. (2018)
- Jain SN, Mehendale AM. "A Review on Umbilical Cord Milking and Its Implications in Neonatal Health". Cureus. (2022)
- Phillipos E, Solevåg AL, Pichler G, et al. "Heart Rate Assessment Immediately after Birth". Neonatology. 109(2). :130-138. (2015)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Aziz K, Lee HC, Escobedo MB, et al. "Part 5: Neonatal Resuscitation: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care". Circulation. 142(16_suppl_2). (2020)
- Kariuki E, Sutton C, Leone TA. "Neonatal resuscitation: current evidence and guidelines". BJA Educ. 21(12). :479-485. (2021)
- Dawson JA, Kamlin COF, Vento M, et al. "Defining the Reference Range for Oxygen Saturation for Infants After Birth". Pediatrics. 125(6). :e1340-e1347. (2010)
- Mariani G, Dik PB, Ezquer A, et al. "Pre-ductal and Post-ductal O2 Saturation in Healthy Term Neonates after Birth". J Pediatr. 150(4). :418-421. (2007)
- Thandaveshwara D, Chandrashekar Reddy AH, Gopalakrishna MV, Doreswamy SM. "Saturation oxygenation pressure index: a non-invasive bedside measure for severity of respiratory disease in neonates on CPAP". Eur J Pediatr. 180(4). :1287-1292. (2020)
- Ho JJ, Subramaniam P, Zakarija-Grkovic I, et al. "Continuous positive airway pressure (CPAP) for apnoea of prematurity". Cochrane Database Syst Rev. (2020)
- Hawkes CP, Ryan CA, Dempsey EM. "Comparison of the T-piece resuscitator with other neonatal manual ventilation devices: A qualitative review". Resuscitation. 83(7). :797-802. (2012)
- Belting C, Rüegger CM, Waldmann AD, Bassler D, Gaertner VD. "Rescue nasopharyngeal tube for preterm infants non-responsive to initial ventilation after birth". Pediatr Res. 96(1). :141-147. (2024)
- Mani S, Pinheiro JMB, Rawat M. "Laryngeal Masks in Neonatal Resuscitation—A Narrative Review of Updates 2022". Children. 9(5). :733. (2022)
- Song ES, Jeon GW. "Updates in neonatal resuscitation: routine use of laryngeal masks as an alternative to face masks". Clin Exper Pediatr. 67(5). :240-246. (2024)
- Liu HK, Yang YN, Tey SL, et al. "Weight Is More Accurate than Gestational Age When Estimating the Optimal Endotracheal Tube Depth in Neonates". Children. 8(5). :324. (2021)
- Millin MG, Bogumil D, Fishe JN, Burke RV. "Comparing the two-finger versus two-thumb technique for single person infant CPR: A systematic review and meta-analysis". Resuscitation. 148. :161-172. (2020)
- Roberts JR. "Roberts and Hedges' Clinical Procedures in Emergency Medicine and Acute Care". Elsevier. (2018). ISBN: 9780323354783
- Cavazos-Rehg PA, Krauss MJ, Spitznagel EL, et al. "Maternal Age and Risk of Labor and Delivery Complications". Matern Child Health J. 19(6). :1202-1211. (2014)
- Edwards T, Harding JE. "Clinical Aspects of Neonatal Hypoglycemia: A Mini Review". Front Pediatr. 8. (2021)
- Adamkin DH. "Postnatal Glucose Homeostasis in Late-Preterm and Term Infants". Pediatrics. 127(3). (2011)
- "Contributor Disclosures - Neonatal resuscitation. All of the relevant financial relationships listed for the following individuals have been mitigated: Esther Welzel (illustrator, is an independent contractor for Fluentis Schweiz); Luisa Voßbeck (medical editor, was employed by GÖK Consulting GmbH through Aug 2020); Alexandra Willis (copyeditor, was an independent contractor for OPEN Health Communications through Aug 2021). None of the other individuals in control of the content for this article reported relevant financial relationships with ineligible companies. For details, please review our full conflict of interest (COI) policy"