Quick guide
Diagnostic approach
- ABCDE survey
- Targeted clinical evaluation
- CBC
- BMP
- Urinalysis
- β-hCG in patients who can become pregnant
- Nonpregnant adults: CT abdomen and pelvis without contrast
- Children and pregnant adults: US abdomen and pelvis
Red flag features
- Intractable pain
- Inability to tolerate PO
- Signs of sepsis (e.g., fever)
- Acute renal failure
- Solitary kidney
- Kidney transplant
Management checklist
- NPO if the need for anesthesia is anticipated
- Analgesia (e.g., ketorolac )
- Antiemetics (e.g., ondansetron )
- IV fluid therapy for dehydration
- Consider medical expulsive therapy (e.g., tamsulosin ).
- Treat concomitant UTI, if present.
- Provide a urine strainer for stone collection.
- Consult urology urgently if red flag features are present.
Summary
Nephrolithiasis encompasses the formation of all types of urinary calculi in the kidney, which may be deposited along the entire urogenital tract, from the renal pelvis to the urethra. Risk factors include low fluid intake and high-sodium, high-purine, low-potassium diets, which can raise the calcium, uric acid, and oxalate levels in the urine and thereby promote stone formation. Urinary stones are most commonly composed of calcium oxalate. Less common stones are composed of uric acid, struvite (due to infection with urease-producing bacteria), calcium phosphate, or cystine. Nephrolithiasis manifests as sudden-onset colicky flank pain that may radiate to the groin, testes, or labia, commonly called renal or ureteric colic, and it is usually associated with hematuria. Diagnostics include spiral CT without contrast in nonpregnant adults and/or ultrasound of the abdomen and pelvis to detect the stone, as well as urinalysis to assess for concomitant urinary tract infection (UTI) and serum BUN and creatinine to evaluate kidney function. Small stones that do not require urgent urological intervention can be managed with symptomatic treatment and a trial of medical expulsive therapy to promote spontaneous passage. If spontaneous passage appears unlikely or fails because of the size or location of the stone, first-line urological interventions include shock wave lithotripsy, ureterorenoscopy, and, in patients with large kidney stones, percutaneous nephrolithotomy. The most important preventive measure is adequate hydration. In addition, the analysis of passed stones may provide information to guide dietary changes and/or medical therapy (e.g., thiazide diuretics, urine alkalinization) that can prevent future stone formation.
Epidemiology
- Sex: ♂ > ♀ [1]
- Peak incidence: 45–70 years [1]
-
Risk factors for nephrolithiasis
- Low fluid intake, dehydration
- Prolonged immobilization
- Dietary factors, e.g.,
- Diets high in sodium and/or low in calcium
- Excessive animal protein intake (increases the risk of calcium oxalate stones)
- Ketogenic diet (increases the risk of uric acid stones)
- Supplements (e.g., calcium, vitamin D, and vitamin C supplementation)
- Medications (e.g., antiepileptic drugs, corticosteroids, loop diuretics, carbonic anhydrase inhibitors)
- Postcolectomy and/or postileostomy
- Personal or family history
- See also:
- “Overview of kidney stones” for type-specific risk factors
- “Risk factors for pediatric nephrolithiasis” for additional factors in children
Epidemiological data refers to the US, unless otherwise specified.
Classification
Overview of kidney stones
| Types | Incidence | Etiology/associated findings | Urine pH | Crystal appearance | Radiopacity | |
|---|---|---|---|---|---|---|
| Calcium oxalate stones |
|
|
|
|
|
|
| Uric acid stones |
|
|
|
|
|
|
| Struvite stones |
|
|
|
|
|
|
| Calcium phosphate stones |
|
|
|
|
|
|
| Cystine stones |
|
|
|
|
||
| Xanthine stones |
|
|
|
|
||
Urine alkalizers (e.g., potassium citrate) prevent stones that form in acidic urine. Urine acidifiers (e.g., cranberry juice, betaine) prevent stones that form in alkaline urine.





Calcium oxalate stones [3]
-
Types
- Calcium oxalate monohydrate (whewellite): brown or black calculi
- Calcium oxalate dihydrate (weddellite): light yellow calculi
-
Etiology
- Hypercalciuria: presence of elevated calcium levels in the urine
-
Hyperoxaluria: presence of elevated oxalate levels in the urine
- Dehydration
- Increased intake of dietary oxalate
-
Increased intestinal absorption of oxalate, e.g., due to fatty acid malabsorption (e.g., Crohn disease, ulcerative colitis, short bowel syndrome)
- Calcium normally binds oxalate to form calcium oxalate, which is excreted via feces.
- In conditions associated with fatty acid malabsorption due to impaired bile acid reabsorption, calcium preferentially binds free fatty acids, leading to excess free oxalate and, therefore, to increased oxalate absorption.
- Vitamin C supplements
- Ethylene glycol poisoning [4]
- Pyridoxine deficiency [5]
- Obesity
- Hypocitraturia: decreased level of citrate in the urine
- Hyperuricosuria: increased urinary excretion of uric acid
- Develop in persistently acidic urine
-
Diagnosis
- Urine microscopy: dumbbell-shaped or octahedron-shaped crystals
- X-ray (or CT): radiopaque stones
-
Treatment [6][7]
- Hydration
- Dietary modification
- Reduced intake of salt (mainly sodium) and animal protein
- Reduced intake of oxalate-rich foods and supplemental vitamin C
- Calcium intake should not be restricted (restriction increases risk of hyperoxaluria, and thereby, the risk for osteoporosis)
- Thiazide diuretics for recurrent calcium-containing stones with idiopathic hypercalciuria (i.e., no hypercalcemia)
- Urine alkalinization (e.g., with potassium citrate)
- Possibly citrate supplementation
Crohn disease leads to increased oxalate absorption via malabsorption of fatty acids, which can ultimately cause nephrolithiasis.


Uric acid stones
-
Etiology
-
Hyperuricemia and hyperuricosuria
- Gout
- High cell turnover (e.g., tumor lysis syndrome, myelodysplastic syndrome)
- Diabetes mellitus, metabolic syndrome
- Chronic diarrhea
- ↓ Urine volume; , e.g., due to dehydration (often seen in desert climates)
- Develop in persistently acidic urine [8]
-
Hyperuricemia and hyperuricosuria
-
Diagnosis
- Urine microscopy: rhomboid/needle-shaped crystals
- X-ray: radiolucent stones
- CT: can be visible but are usually only minimally visible (not as visible as calcium stones)
- US and/or intravenous pyelogram may also be helpful in diagnosis
-
Treatment
- Hydration
- Oral chemolitholysis (e.g., potassium citrate) via urine alkalinization
- Low-purine diet
- Allopurinol
Uricosuric agents (e.g., probenecid) increase the excretion of uric acid, which can accelerate the formation of stones.
Uric acid stones are radiolUcent (x-ray negative).
Struvite stones (magnesium ammonium phosphate stones)
-
Etiology
-
Upper UTI with urease-producing bacteria such as Proteus mirabilis, Klebsiella, Staphylococcus saprophyticus, and/or Pseudomonas
- These bacteria convert urea to ammonia → elevated ammonia causing alkaline urine → precipitation of the ammonium magnesium phosphate salt → crystal and stone formation
- Can form very large stones that fill the entire renal pelvis and calyces (staghorn calculi)
- Use of indwelling catheter increases risk
- Develop in persistently alkalic urine
-
Upper UTI with urease-producing bacteria such as Proteus mirabilis, Klebsiella, Staphylococcus saprophyticus, and/or Pseudomonas
-
Diagnosis
- Urine microscopy: rectangular prisms (coffin lid-appearance) indicate struvite stones
-
X-ray (or CT)
- Weakly radiopaque stones
- Possibly staghorn calculi
-
Treatment
- Antibiotic treatment of urinary tract infections
- Hydration
- Urine acidification
- Usually require surgical stone removal
Urinary tract infections can lead to the formation of struvite stones, but struvite stones also increase the risk of urinary tract infections.


Calcium phosphate stones [3]
-
Types
- Carbonate apatite
- Brushite
-
Etiology
- Hyperparathyroidism (brushite)
- Type 1 renal tubular acidosis (brushite)
- Upper urinary tract infections (carbonate apatite)
- Develop in persistently alkalic urine
-
Diagnosis
- Urine microscopy: wedge-shaped crystals
- X-ray (or CT): radiopaque stones
-
Prevention
- Hydration
- Thiazide diuretics
- Diet low in sodium
- Urine acidification (carbon apatite stones)
Cystine stones [9]
-
Etiology
- Autosomal recessive defect in cystine-reabsorbing PCT transporter → impaired proximal renal tubular absorption of dibasic amino acids → cystinuria → cystine stone formation (as cystine is poorly soluble)
- Develop in persistently acidic urine
- Clinical features: recurrent kidney stones (manifesting with e.g., flank pain) starting in childhood
-
Diagnosis
- Urine microscopy: hexagonal crystals
-
X-ray (or CT)
- Weakly radiopaque stones
- Possibly staghorn calculi
- Positive cyanide nitroprusside test
-
Prevention
- Hydration
- Diet low in sodium
- Urine alkalinization
- Chelating agents (e.g., penicillamine) for refractory cases
- Tiopronin
To remember that cystine crystals are hexagonal, think “The Cystine Chapel has six sides.”
Xanthine stones
-
Etiology: xanthinuria
- Hereditary deficiency of xanthine oxidase → failure to convert xanthine to uric acid
- Allopurinol
-
Diagnosis
- Urine microscopy: amorphous crystals
- Urine pH: plays little role in diagnosis [10]
- X-ray: radiolucent stones (require further evaluation with CT, US, and/or intravenous pyelogram)
- Treatment: reduced dietary intake of purines
2,8-Dihydroxyadenine stones
- Etiology: increased urinary 2,8-dihydroxyadenine concentration due to hereditary deficiency of adenine phosphoribosyltransferase
- Treatment: allopurinol OR febuxostat
Ammonium urate stones
- Etiology: urinary tract infection, malabsorption, hypokalemia
-
Treatment
- Antibiotic treatment of UTI as indicated
- Urine acidification
Drug-induced stones
Can be caused by:
- Crystallization of drug compounds in the urine, which is most commonly associated with:
- Acyclovir
- Indinavir
- Sulfonamides
- Fluoroquinolones
- Ceftriaxone
- Stone formation due to alterations in urine composition, which are most commonly associated with:
- Acetazolamide
- Furosemide
- Topiramate
- Vitamin D, vitamin A
- Aluminium magnesium hydroxide
- Calcium
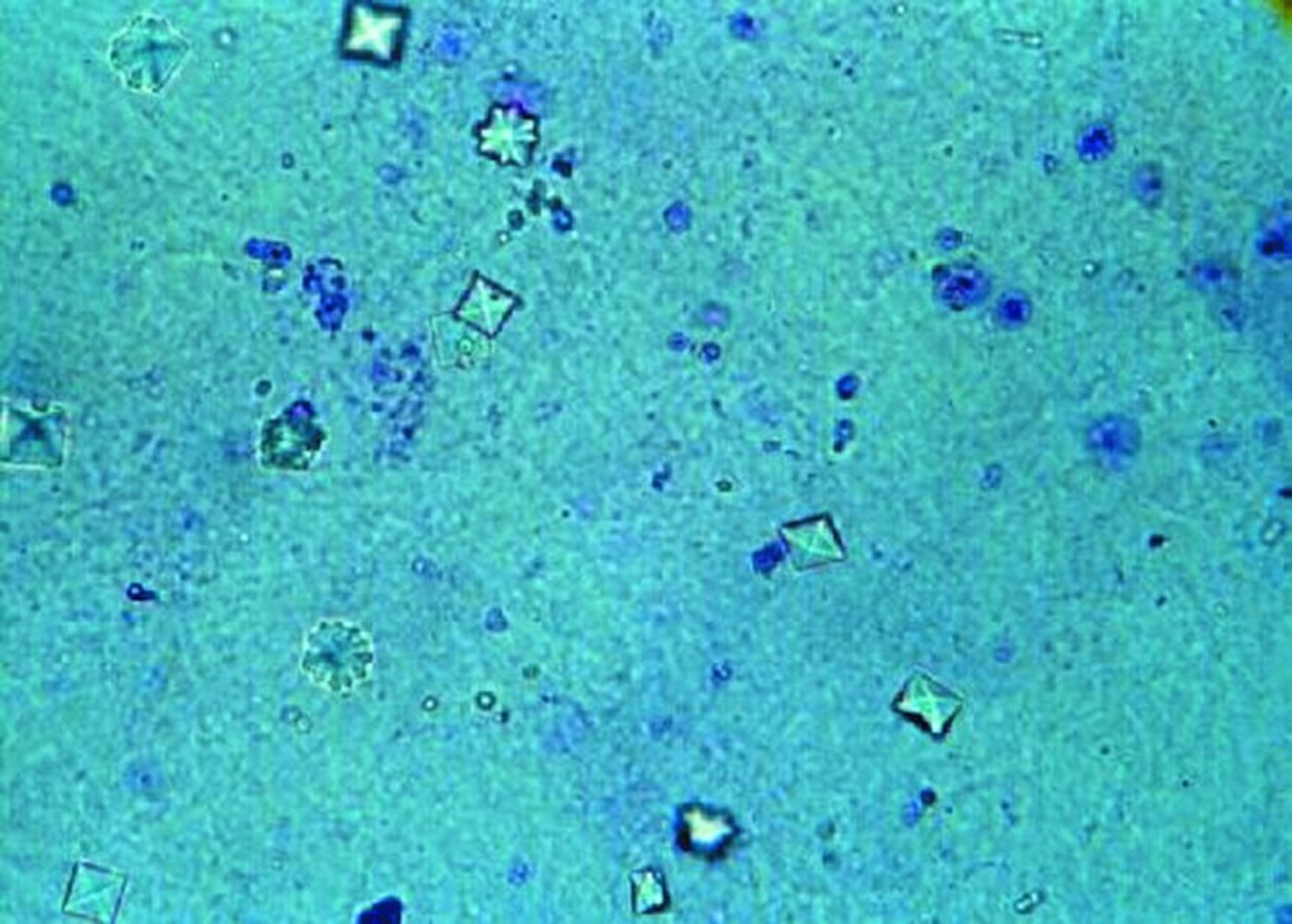
Photomicrograph of a urine sample (urine sediment wet mount, intermediate magnification)
Multiple envelope-shaped crystals can be seen (cf. illustration; examples indicated by yellow overlay) throughout the sample. These are composed of calcium oxalate dihydrate and have an octahedral structure.
Source: "The micrograph shows calcium oxalate crystals in urine. These small crystals can develop to form renal stones. (NASA)", NASA/JSC, NASA licensed under Public Domain Further notes: NASA CC: https://www.nasa.gov/multimedia/guidelines/index.html
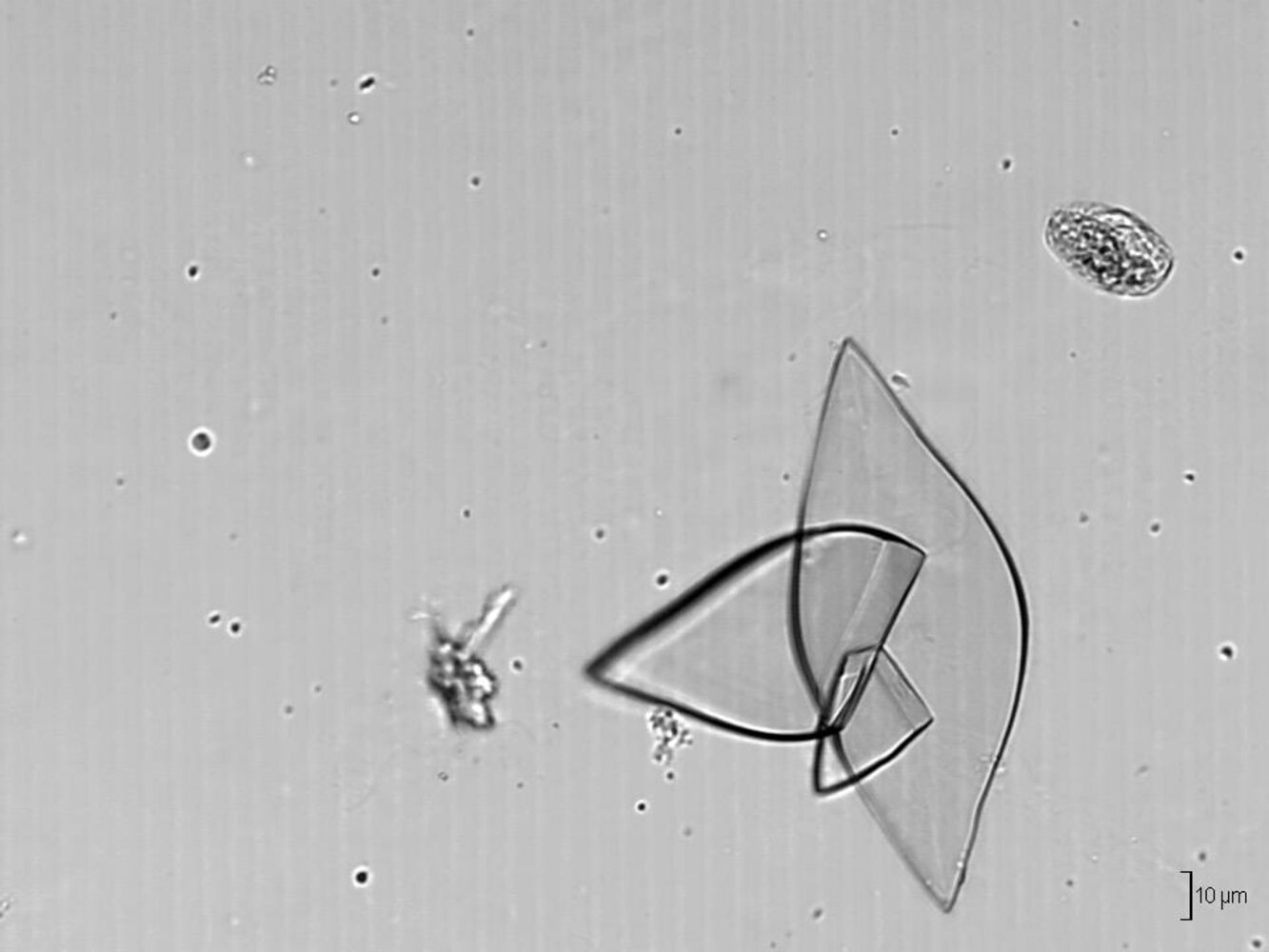
Photomicrograph of a urine sample with a pH of 5 (phase contrast microscopy; high magnification)
Multiple crystals of varying sizes and shapes can be seen (blue overlay).
Their diamond-shaped (rhomboid) form is one of the characteristic appearances of uric acid crystals, which only form in urine samples with a pH < 5.5 and are typically seen in patients with gout or in healthy individuals on a high-purine diet. Uric acid crystals may also appear barrel-shaped and needle-shaped (not seen in this image).
Source: “Uric acid crystals (urine) - Ürik asit kristalleri (idrar) - 03.png” by Doruk Salancı, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
_-_%C3%9Crik_asit_kristalleri_(idrar)_-_03.png){kind=link}

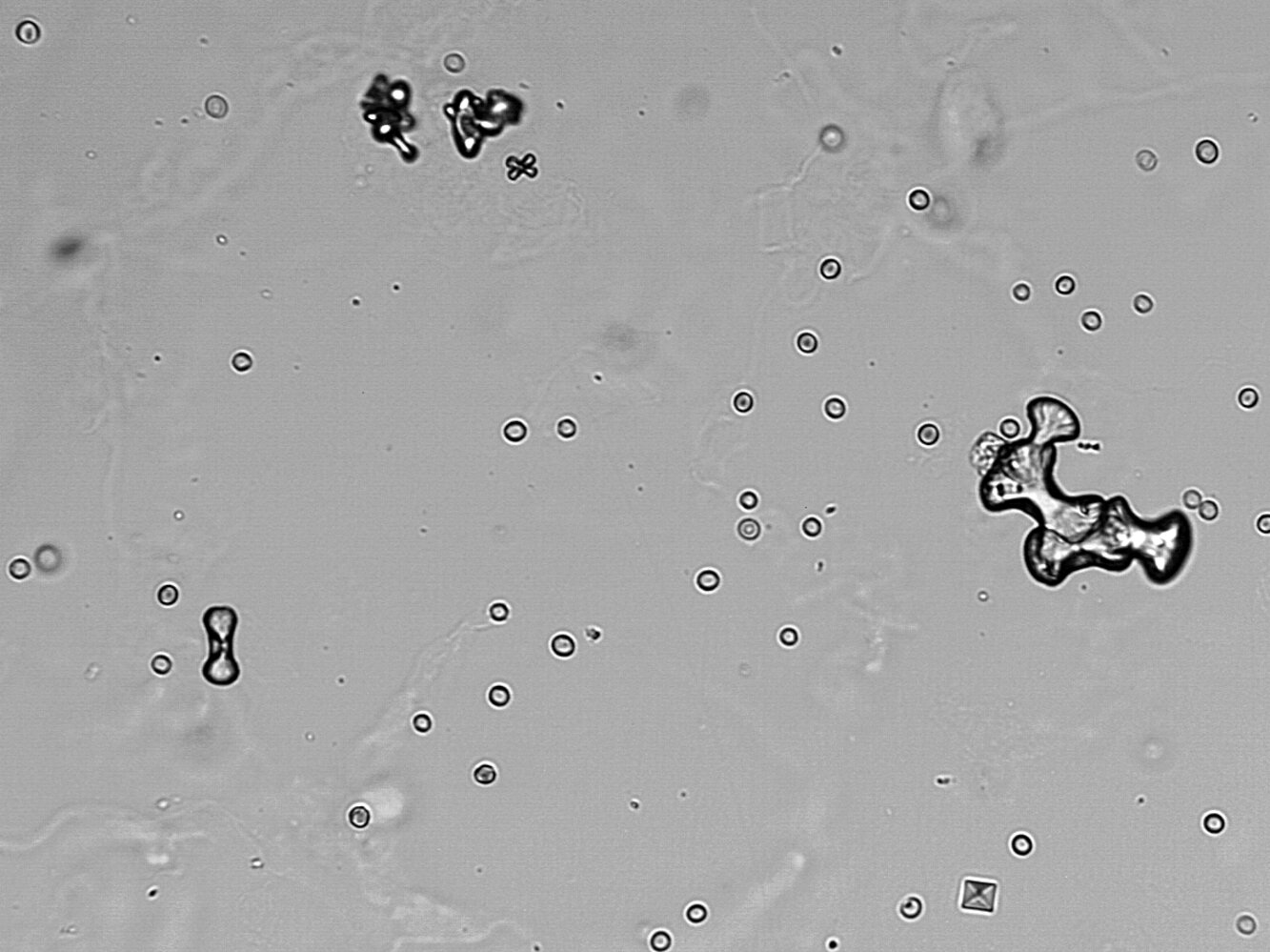
Photomicrograph of a canine urine sample
Sample shows clear, euhedral, rectangular prism crystals (struvite crystals with their characteristic coffin-lid appearance (cf. illustration); examples indicated by green overlay) composed of magnesium, ammonium, and phosphate. In humans, struvite crystals are only seen in upper urinary tract infections caused by urease-producing organisms (e.g., Proteus or Klebsiella species).
Source: “Struvite crystals dog with scale 1” by Joel Mills, Wikimedia Foundation, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

Photomicrograph showing crystals with the appearance of wedge-shaped prisms (can also be described as blunt-ended needles), some bound together forming a rosette.
Source: “vvv calcium phosphate rosette” by Cayla Devine, Flickr, licensed under CC BY 2.0.
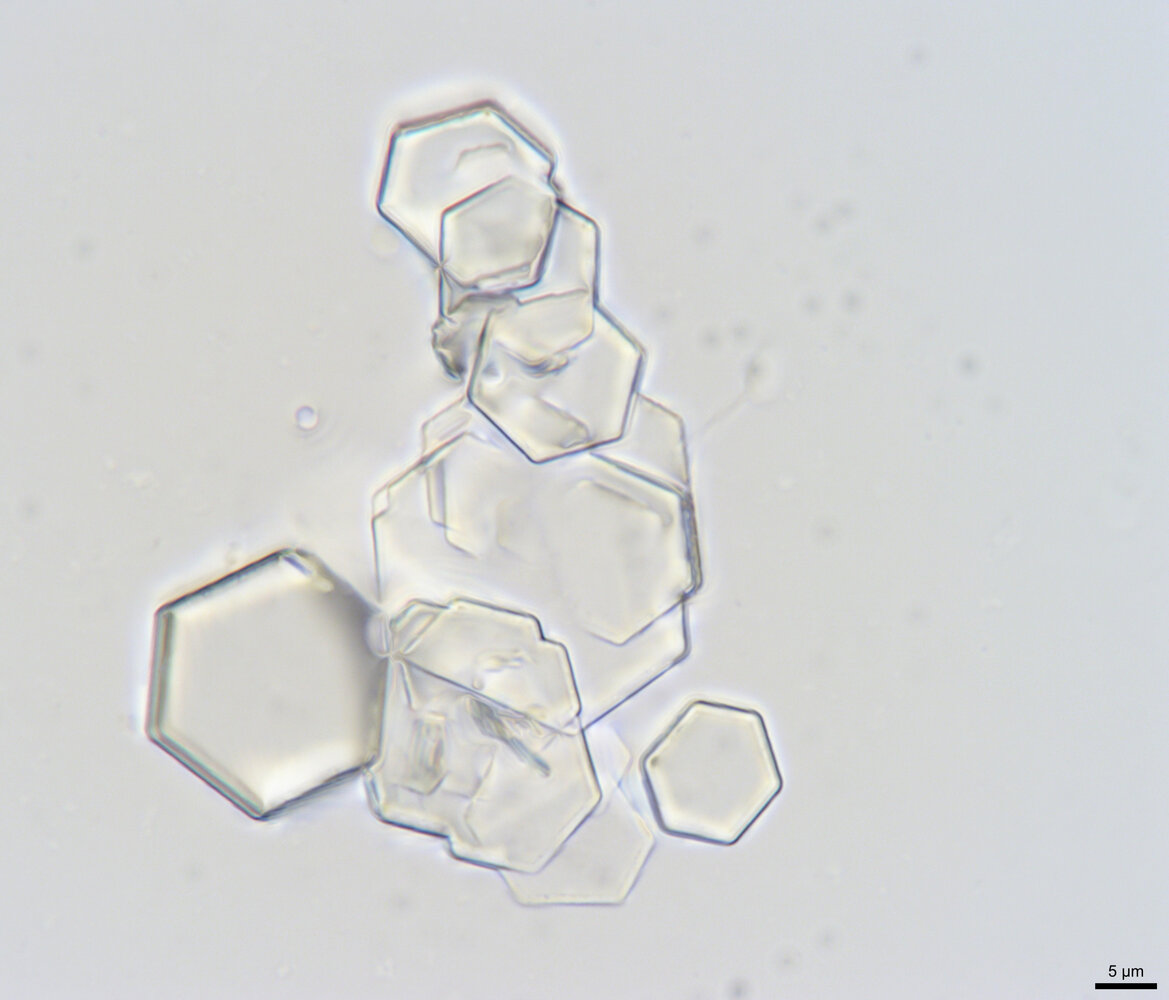
Photomicrograph of cystine crystals from a canine urine sample (1000x magnification)
A clump of multiple, clear, hexagon-shaped crystals is visible.
This is the characteristic appearance of cystine crystals.
Source: “Cystine Crystals in Canine Urine Sediment.jpg” by Lance Wheeler, Wikimedia Commons, licensed under CC BY-SA 4.0. Modifications: Image was cropped..
{kind=link}
Urine microscopy
Clumps of dumbbell-shaped calcium oxalate monohydrate crystals can be seen (yellow overlay). An envelope-shaped (octahedral) calcium oxalate dihydrate crystal (black arrowhead) and multiple erythrocytes (examples indicated by white arrowheads) are also present.
Calcium oxalate stones are the most common type of kidney stones.
Source: “Calcium oxalate crystals (urine) - kalsiyum oksalat kristalleri (idrar)” by Doruk Salancı, Wikimedia commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
_-_kalsiyum_oksalat_kristalleri_(idrar)_-_02.png){kind=link}

© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.

X-ray abdomen (AP view)
A large branching structure is seen within the renal pelvis and several enlarged calyces (green overlay). The appearance is typical of a struvite staghorn calculus. The term “staghorn calculus” is used when at least two calyces are involved, giving rise to the appearance of a stag's antlers.
Struvite calculi are caused by urease-producing bacteria. Calcium carbonate precipitates with struvite to form large calculi that are radiographically visible and conform to the renal collecting system.
Severe lumbar rotatory scoliosis is also seen on the radiograph.
P: renal pelvis; VB: vertebrae
Source: “Staghorn Kidney Stone 08779” by Nevit Dilmen, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

Clinical features
Stones usually form in the collecting ducts of the kidneys but may be deposited along the entire urogenital tract from the renal pelvis to the urethra. Their localization and size determine the specific symptoms. Small kidney stones may also be asymptomatic and detected incidentally. [11]
-
Severe unilateral and colicky flank pain (renal colic) ; [12]
- Radiates anteriorly to the lower abdomen, groin, labia, testicles, or perineum
- Paroxysmal or progressively worsening [13]
- The area around the kidneys may be tender on percussion (costovertebral angle tenderness)
- Hematuria
- Nausea, vomiting, and reduced bowel sounds
- Dysuria, frequency, and urgency
- Passage of gravel or a stone
- Patients are usually unable to sit still and move around frequently (opposed to patients with peritonitis, who usually prefer to lie still)
Depending on the location of the stone, nephrolithiasis may resemble conditions such as appendicitis or testicular torsion.


© AMBOSS
Diagnosis
Approach [14][15][16]
-
Clinical suspicion: Consider nephrolithiasis in patients with unilateral colicky flank pain associated with nausea, vomiting, and/or hematuria.
- See “Approach to the management of acute abdominal pain” for the general evaluation of patients with flank pain.
- For patients presenting with hematuria, see also “Diagnostics” in “Hematuria.”
-
Initial diagnostics
- Laboratory studies: CBC, BMP, urinalysis , β-hCG
- Imaging studies: CT abdomen and pelvis without contrast preferred if imaging is indicated
-
Further evaluation
- Determine stone composition.
- Identify metabolic risk factors with a dietary history and laboratory studies.
Laboratory studies [14][15]
- CBC: ↑ WBC count [17]
-
BMP
- Typically within normal limits
- Elevated BUN and creatinine suggest an acute kidney injury.
Laboratory studies are not necessary for the diagnosis of nephrolithiasis, but they may help narrow the differential diagnosis and identify complicating factors (e.g., acute kidney injury, UTI).
Urinalysis [15][17]
- Nonspecific findings of nephrolithiasis
- Gross or microscopic hematuria
- Crystalluria
- Nonspecific urinalysis findings of UTI, e.g., positive leukocyte esterase or nitrites, leukocyturia, bacteriuria
- Findings suggestive of stone composition
- Alkaline urine (pH > 7.5–8) suggests struvite stones associated with urease-producing organisms. [18][19]
- Acidic urine (pH < 4.5–5.5) may indicate uric acid stones. [20]
Imaging studies [21][22][23]
- Recommendations in this section are consistent with the 2015 American College of Radiology (ACR) appropriateness criteria for acute-onset flank pain with suspicion of stone disease. [21]
- In general, an initial presentation suspicious for nephrolithiasis requires confirmatory CT imaging.
- Imaging is also indicated for acute flank pain of uncertain etiology, e.g., to rule out AAA.
- Routine CT is controversial in adults < 55 years of age with uncomplicated presentations of renal colic , especially those with a history of nephrolithiasis. [21][24][25][26]
CT abdomen and pelvis without contrast and ultrasound of the abdomen and pelvis are the preferred diagnostic tests for nephrolithiasis in patients for whom imaging is indicated.
CT abdomen and pelvis without IV contrast
CT has the highest accuracy of the imaging modalities to identify kidney stones.
- Type: low-dose, helical (spiral) CT without contrast
- Indication: first-line for nonpregnant patients with suspected nephrolithiasis
-
CT findings in nephrolithiasis [21]
- Calculus size , location, density , and degree of obstruction
- Hydronephrosis and/or hydroureter
- Perinephric fat stranding
Hydronephrosis and/or hydroureter without calculi may suggest a recently passed kidney stone. [21]
The addition of IV contrast may help to differentiate ureteral stones from phleboliths and increases the likelihood of detecting alternative causes of abdominal pain (e.g., appendicitis, diverticulitis). However, IV contrast reduces the sensitivity for kidney stones to ∼ 80% compared to > 95% in CT without contrast. [21]
")
")

Ultrasound abdomen and pelvis
- Indications: suspected nephrolithiasis in patients for whom radiation exposure should be minimized (e.g., pregnant patients, pediatric patients, those with recurrent stones)
- Findings
- Obstructive uropathy (e.g., hydronephrosis, hydroureter, perinephric fluid) [21]
- Stone: hyperechoic signal with acoustic shadowing [17]
- Twinkle artifact: intense multicolored signal behind a stone seen when using color Doppler technique
- Absence of ureteral jet : suggests an obstructing stone


X-ray kidney, ureter, and bladder (KUB)
- Indications: follow-up for previously identified radiopaque stones after the initiation of treatment
- Findings: radiographic densities (e.g., stones, phleboliths, vascular calcifications)
Because KUB sensitivity is proportional to stone size, it is usually only suitable for larger stones.
MR urography [21]
- Indications
- Suspected nephrolithiasis in patients for whom radiation exposure should be minimized (e.g., pregnant patients)
- High clinical suspicion for nephrolithiasis despite inconclusive or negative CT findings
- Findings: similar to CT
Intravenous pyelogram (IVP)
- Indications: rarely indicated given the broad availability of CT
- Findings
- Provides a complete outline of the urinary tract system
- Size and location of stone, degree of obstruction

Metabolic evaluation for nephrolithiasis [14][16][27]
For initial episodes of nephrolithiasis, patients should undergo a limited metabolic evaluation to rule out underlying systemic disorders and guide preventative therapy. This workup is typically unnecessary following repeat visits for renal colic where the underlying etiology is already known.
- Dietary history: fluid intake, protein, calcium, sodium, fruits, vegetables, high-oxalate foods, over-the-counter supplements
- Laboratory studies: BMP , serum calcium and phosphorous , serum uric acid , serum magnesium, urinalysis
- Stone composition analysis [28]
-
24-hour urine profile
- Measures saturation of stone-forming salts and other parameters, such as total volume, pH, and creatinine
- Dietary changes, medical therapies, or additional testing may be recommended based on the results.
Provide patients with a first-time diagnosis of nephrolithiasis with a urine strainer at the time of discharge to collect passed stones for compositional analysis during their follow-up.
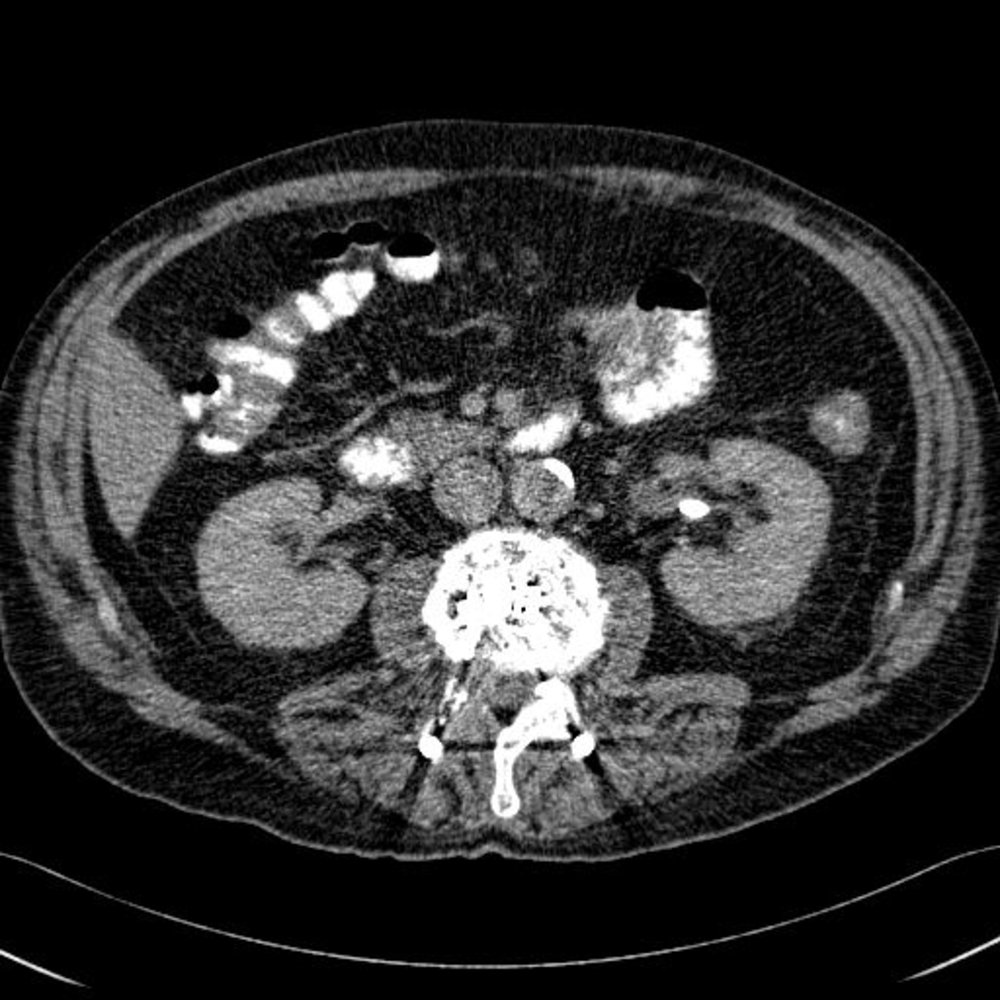
CT abdomen (with oral contrast; axial plane)
The calcific density (circled) in the left renal pelvis is a calculus. There is no dilatation of the renal pelvis to indicate obstruction. Atherosclerotic calcification (red arrowhead) of the abdominal aorta is seen. Metal streak artifacts (examples indicated by green overlay) over the spine are caused by an internal spinal fixator (white arrows).
A: aorta; IVC: inferior vena cava; K: kidney; L: liver
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.

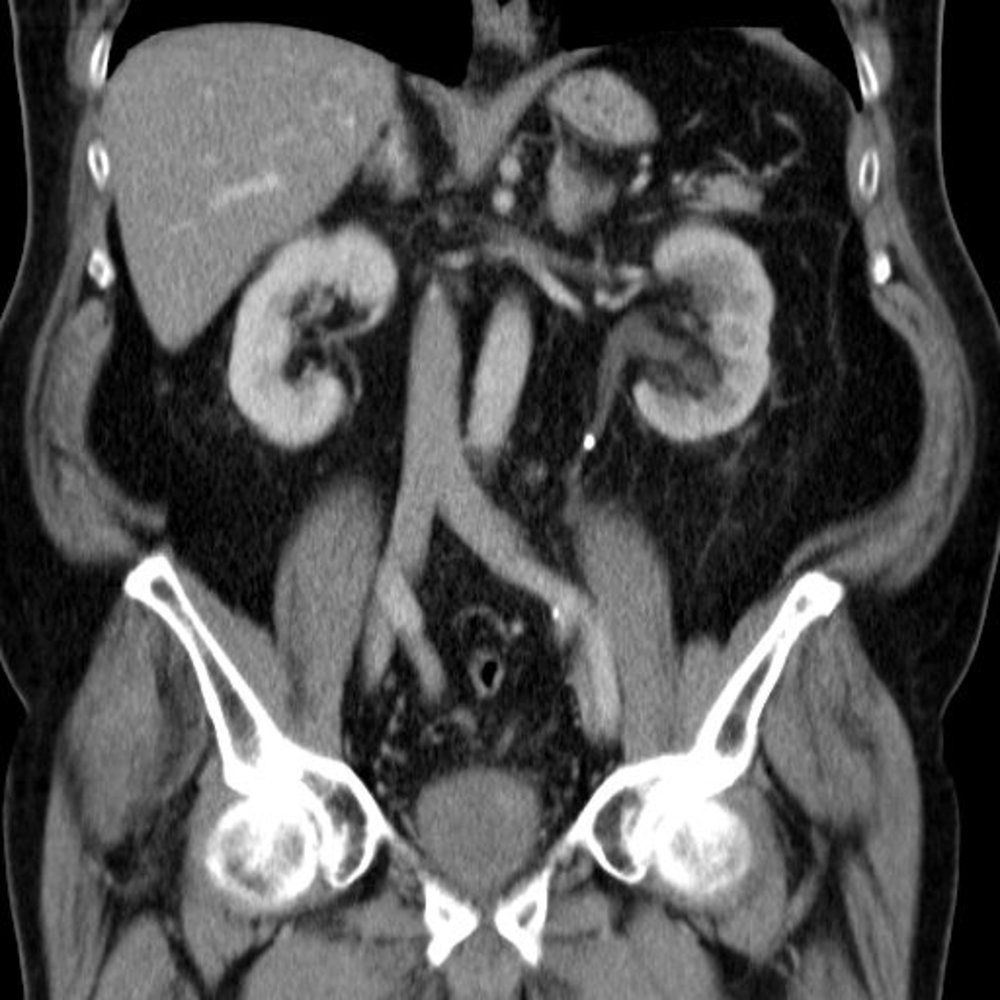
CT abdomen (with oral contrast; coronal plane)
A nonobstructive hyperdense calculus (red circle) is present in the left renal pelvis. Atherosclerotic calcifications (red arrowheads) of the abdominal aorta (red overlay) are also seen. Metal streak artifacts (white arrows) between the aorta and inferior vena cava (blue overlay) are caused by an internal spinal fixator.
K and dashed lines: kidney; Li: liver, Lu: lung; PM: psoas major muscle; S: stomach with oral contrast; UB: urinary bladder
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.
CT abdomen (with contrast; coronal plane)
The left renal collecting system (green overlay) is dilated to the level of a hyperdense calculus (yellow overlay) within the proximal third of the ureter. The left renal parenchyma shows less enhancement than the right renal parenchyma as a result of impaired excretion from ureteral obstruction.
Blue overlay: inferior vena cava; red overlay: abdominal aorta
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.

Ultrasound left kidney (longitudinal plane)
The calyces (green overlay) are dilated and have lost their normal cup-shaped appearance. Flattening of papillae and blunting of fornices can be seen. Where visible, the renal cortical parenchyma is not thinned.
RP: renal parenchyma; Arrowheads: hyperechoic renal sinus
Source: “Ultrasonographic picture taken from a patient with left ureteral stone with hydronephrosis, created in Taiwan” by morning2k, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

Ultrasound kidney (longitudinal plane; imaged from flank)
A left lower pole renal calculus is seen as a hyperechoic structure (red overlay) with posterior acoustic shadowing (green overlay).
Posterior acoustic shadowing is an ultrasound artifact that occurs when beam penetration is severely impeded by a structure with a high attenuation coefficient (e.g., calculus, bone, dense fibrous tissue).
Our great thanks to Albertinen Krankenhaus, Hamburg, Germany, for kindly providing this case. Further notes: removal of in-image text
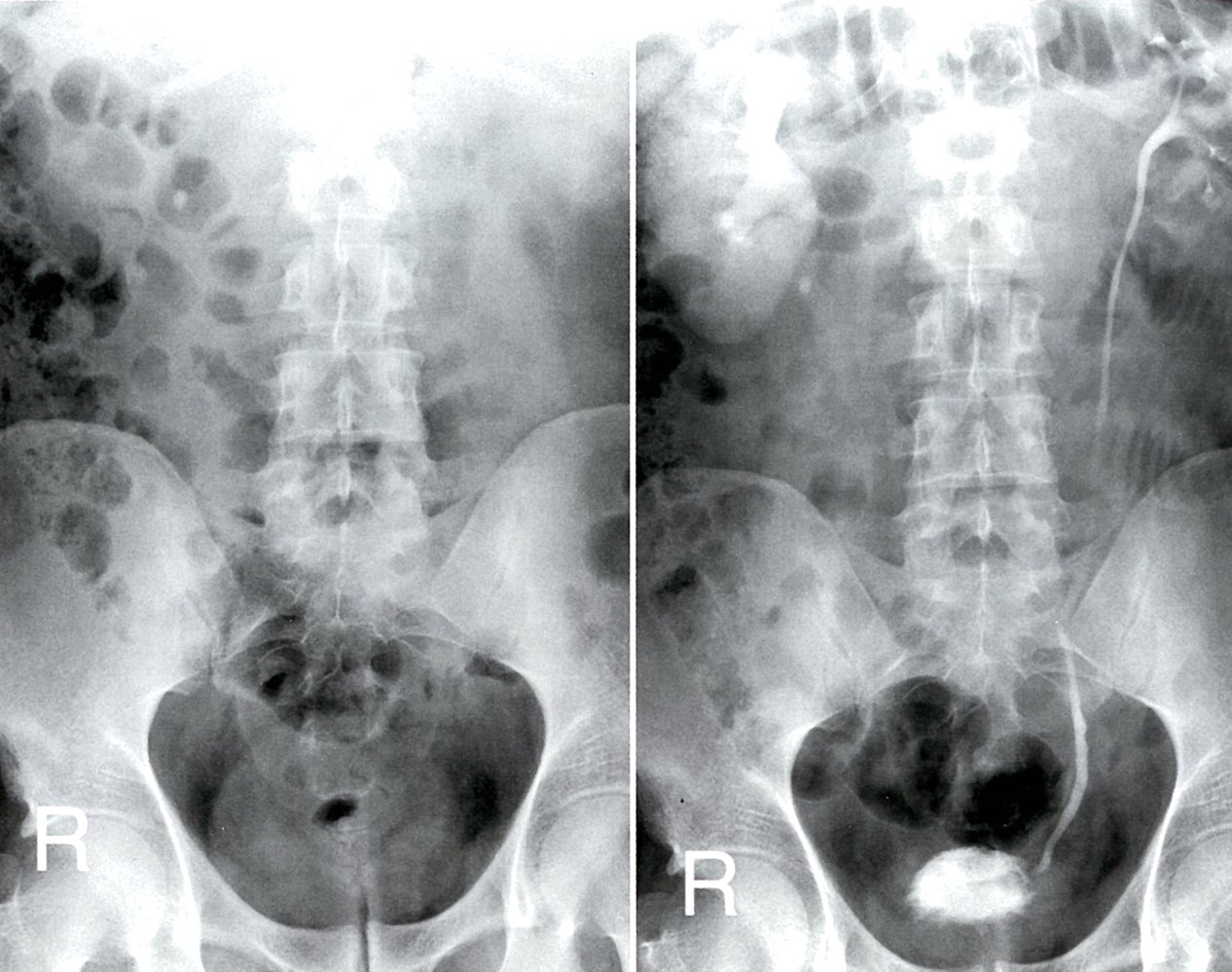
Excretory urography (AP view; left: pre-contrast; right: 2.5 hours post-contrast)
A calcification medial to the lower pole of the right kidney on the pre-contrast radiograph (red overlay) is shown post-contrast to be an obstructing proximal ureteral calculus (UC; red overlay). The right kidney is enlarged, with persistent enhancement (green overlay). There is pelvicaliectasis and poor contrast-filling of the right ureter (region indicated by dashed lines). The left renal collecting system is normal (purple overlay).
RP: renal pelvis, U: ureter; UB: urinary bladder
Source: © IMPP
Differential diagnoses
-
Pain
- Causes of acute abdomen (See “Differential diagnoses of acute abdominal pain.”)
- Causes of acute back pain (E.g., see “Nonspinal causes of acute back pain.”)
- Causes of testicular pain (See “Differential diagnosis of scrotal pain.”)
-
Other findings or clinical features
- Causes of hydronephrosis (See “Upper urinary tract obstruction.”)
- Urinary tract infection: cystitis or pyelonephritis
- See also “Hematuria.”
The differential diagnoses listed here are not exhaustive.
Treatment
Recommendations in this section are consistent with the 2016 American Urological Association (AUA) guideline on the surgical management of kidney stones and the 2019 AUA guideline on the medical management of kidney stones. [14][29]
Approach [22][29]
- Initiate symptomatic management prior to confirmatory imaging for patients with renal colic.
-
Consult urology urgently for interventional treatment in the following cases:
- Uncontrolled symptoms (e.g., intractable pain, inability to tolerate PO)
- Large stones (> 10 mm)
- Infected kidney stones (e.g., signs of sepsis in combination with high-grade obstruction)
- Acute renal failure
- Solitary kidney or kidney transplant with obstruction
-
Attempt a trial of conservative management for patients with small (≤ 10 mm), uncomplicated stones.
- Offer medical expulsive therapy in addition to symptomatic treatment.
- Treat concomitant UTI, if present.
- Interventional treatment is indicated if conservative management is unsuccessful after 4–6 weeks.
- Disposition: Most patients with uncomplicated nephrolithiasis can be treated successfully with conservative management during an emergency department visit of a few hours.
- Admit patients requiring urgent urology consult and intervention.
- Ensure outpatient urology follow-up for all patients eligible for discharge (e.g., no indications for urgent urology consult, resolved symptoms, no complications).
- Tailor recurrence prevention measures to the type of stone; see “Prevention of nephrolithiasis.”
The larger the stone, the less likely it is to pass spontaneously.
Obstructing nephrolithiasis with suspected infection requires urgent urology consultation and management. [29]
Symptomatic management [17][22]
-
Analgesia
- First-line: NSAIDs, e.g., ketorolac [30]
- Second-line: opioids, e.g., morphine
- Antiemetics, e.g., ondansetron (off-label)
- Intravenous fluids for dehydration
Conservative management [22][29]
- Initiate medical expulsive therapy (MET).
-
First-line: tamsulosin (alpha blocker, off-label) [29]
- Relieves ureter muscle spasms
- Promotes the passage of ureteral stones ≤ 10 mm
- Reduces the need for analgesics
- Alternative: nifedipine; (calcium-channel blocker, currently not routinely recommended)
-
First-line: tamsulosin (alpha blocker, off-label) [29]
- Provide antibiotic treatment if urinalysis indicates a UTI; for specific recommendations, see:
- “Antibiotic treatment of complicated lower UTI”
- “Empiric antibiotic therapy for complicated pyelonephritis”
Interventional management [29]
Overview
The choice of interventional treatment is based on the size and location of the stone, suspected infection, and shared decision-making.
- Infected stones: ureteral stenting or percutaneous nephrostomy to relieve obstruction; delayed definitive management
-
Ureteral stones
- Ureterorenoscopy (URS): first-line for mid- or distal ureter stones
- OR extracorporeal shockwave lithotripsy (ESWL)
- Renal stones > 20 mm OR lower renal pole stones > 10 mm: percutaneous nephrolithotomy (PCNL)
Procedures
| Urological interventions for nephrolithiasis [29][31] | ||
|---|---|---|
| Intervention | Description | Indications |
| Extracorporeal shock wave lithotripsy (ESWL) |
|
|
| Ureterorenoscopy (URS) |
|
|
| Percutaneous nephrolithotomy (PCNL) |
|
|
| Ureterolithotomy |
|
|
The need for follow-up imaging after conservative or interventional management depends on the symptoms, stone type, and intervention modality.
Complications
- Recurrent urinary tract infections → risk of pyelonephritis, urosepsis, and perinephric abscess
- Urinary obstruction → inflammation of the kidney and hydronephrosis → permanent glomerular damage if left untreated
- Acute kidney injury [11]
We list the most important complications. The selection is not exhaustive.
Prognosis
- Stone size and location determine the likelihood of spontaneous passage: Stones ≤ 5 mm tend to pass spontaneously, while stones ≥ 10 mm are unlikely to do so, especially if located in the pyelon or proximal ureter. [8]
- 50% of patients may have a new episode of nephrolithiasis within 10 years. [1]
Prevention
- Hydration: sufficient fluid intake (i.e., to maintain urine output of ≥ 2.5 L/day for adults; > 30 mL/kg/day for children) [27][32]
-
Diet [27][32]
-
For calcium stones [27]
- Reduce consumption of salt.
- Avoid overconsumption of animal protein.
- Reduce consumption of oxalate-rich foods and supplemental vitamin C (for oxalate stones). [33][34]
- Calcium intake should not be restricted (restriction increases risk of hyperoxaluria, and thereby, the risk for osteoporosis)
- For uric acid stones: low in purine
- For cystine stones: low in sodium
-
For calcium stones [27]
-
Pharmacotherapy (chemoprophylaxis) [35]
-
Calcium stones
- Thiazide diuretics for recurrent calcium-containing stones with idiopathic hypercalciuria (i.e., no hypercalcemia) [27][36]
- Allopurinol in the case of high urine uric acid
- Uric acid stones: allopurinol
- Cystine stones: tiopronin, D-penicillamine
- Struvite stones: antibiotic treatment for UTI
-
Calcium stones
-
Change urinary pH: depends on stone composition
-
Urine alkalinization: a treatment regimen to raise urinary pH to 6.5–7.5
- Achieved via diet rich in fruits and vegetables or supplementation of potassium citrate
- Used to prevent recurrence of calcium oxalate, uric acid, and cystine stones
-
Urine acidification: a treatment regimen to lower the urinary pH to ≤ 7
- Achieved via intake of cranberry juice or betaine or a diet rich in dairy products, grains, or meat
- Used to prevent recurrence of calcium phosphate and struvite stones
-
Urine alkalinization: a treatment regimen to raise urinary pH to 6.5–7.5
Low calcium diets increase the risk of calcium-containing stone formation because they increase oxalate reabsorption.
Special patient groups
The approach to nephrolithiasis in pregnant individuals and children is largely similar to that in adults, with a few modifications.
Nephrolithiasis in pregnancy
- Epidemiology: ∼ 1:3000 pregnancies [37][38]
-
Risk factors
- ↑ Calcium excretion, ↓ excretion of magnesium and citrate
- ↑ Urine pH
- Urinary stasis due to hormonal changes (e.g., due to increased progesterone levels)
- Late pregnancy: ↓ fluid intake resulting from ↓ bladder capacity due to altered position and increasing size of uterus
- Clinical features: similar to clinical features of nephrolithiasis in nonpregnant adults
-
Diagnostics
- Renal ultrasonography is preferred.
- Inconclusive renal ultrasonography: Consider MR urography without IV contrast or low-dose CT without IV contrast.
-
Treatment
- Focuses on pain control because the majority of stones pass spontaneously (for details on analgesia during pregnancy, see “Overview of analgesics to avoid during pregnancy”)
- Surgical interventions are similar to those for nonpregnant individuals (see “Conservative management” and “Interventional management” in “Treatment”).
Nephrolithiasis in children
Epidemiology
- Incidence: approx. 1% of children annually [32]
-
Incidence is rising, particularly in : [27][32][39][40]
- Children aged 12–19 years
- ♀ > ♂
- African American population
Common types of kidney stones in children
- Calcium oxalate stone (40–60%) [39]
- Calcium phosphate stone (10–20%) [39]
- Struvite stone (∼ 10%) [32]
- Uric acid stone (< 5%) [32]
Risk factors for nephrolithiasis in children [27][32][39]
- See “Risk factors for nephrolithiasis” for factors common in children and adults (e.g., low fluid intake, dietary factors, medications).
-
Risk factors specific to children include:
- Congenital anomalies of the kidneys and urinary tract
- Pediatric UTI
- Metabolic abnormalities (e.g., hypercalciuria, hypocitraturia) [27][32]
- Medical comorbidities (e.g., pediatric inflammatory bowel disease, cystic fibrosis)
Clinical features [41]
- Similar to clinical features of nephrolithiasis in adults (i.e., renal colic, hematuria, dysuria, nausea, vomiting) [32][39]
- Nonspecific symptoms and poorly localized pain are more common in young children. [27]
- Features of the underlying etiology or risk factor may be present. [32]
Diagnostics [27][32]
Routine studies
-
Laboratory studies [27]
- Urinalysis, CBC, BMP
- Urine culture if pediatric UTI is identified or suspected
- Metabolic evaluation for nephrolithiasis for all patients [27][32]
-
Imaging [24][27][42][43]
- Preferred initial modality: ultrasound kidneys and bladder
- Alternatives
- Ultra-low-dose or low-dose CT abdomen and pelvis without IV contrast
- KUB x-ray
- Findings: similar to those in adults; see “Diagnosis of nephrolithiasis” for details.
Additional studies
Perform as needed to evaluate for an underlying risk factor for pediatric nephrolithiasis; examples include: [32]
- Voiding cystourethrogram for posterior urethral valves and vesicoureteric reflux
- Evaluation for inborn errors of metabolism (e.g., cystinuria, hereditary xanthinuria)
Treatment [27][32][39][43]
- Administer appropriate pediatric pain management and encourage oral hydration. [43]
- Consult or refer to pediatric urology for management, which may include:
- Observation with or without medical expulsive therapy for uncomplicated ureteric stones ≤ 10 mm [27][32][43]
- Interventional management (e.g., ESWL, PCNL, URS) is required for larger or complicated kidney stones. [27][32][43]
- Treat concomitant UTI, if present; see “Treatment of pediatric UTI.”
- Disposition [27]
- Uncomplicated nephrolithiasis: Consider discharge after acute pain management.
- Admit patients with infection, severe symptoms, renal disease or renal anomalies, and planned interventional management.
- Address risk factors for pediatric nephrolithiasis to prevent recurrence: See “Prevention of nephrolithiasis.”
- Follow-up [27]
- Repeat metabolic evaluation for nephrolithiasis after initiating dietary and/or pharmacological interventions to prevent recurrence.
- Consider screening ultrasound for recurrent stone(s) every 6 months for 2 years until normal levels on 24-hour urine profile are achieved.
Related One-Minute Telegram
- One-Minute Telegram 71-2023-3/3: NOSTONE left unturned
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- Preminger GM, Curhan GC. "The first kidney stone and asymptomatic nephrolithiasis in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/the-first-kidney-stone-and-asymptomatic-nephrolithiasis-in-adults. [2016-11-18]
- Manissorn J, Fong-ngern K, Peerapen P, Thongboonkerd V. "Systematic evaluation for effects of urine pH on calcium oxalate crystallization, crystal-cell adhesion and internalization into renal tubular cells". Scientific Reports. 7(1). (2017)
- Curhan GC, Goldfarb S, Lam AQ. "Risk Factors for Calcium Stones in Adults". UpToDate. UpToDate. https://www.uptodate.com/contents/risk-factors-for-calcium-stones-in-adults. [2018-05-16]
- Cristoforo Pomara, Carmela Fiore, Stefano D'Errico, Irene Riezzo, Vittorio Fineschi. "Calcium oxalate crystals in acute ethylene glycol poisoning: a confocal laser scanning microscope study in a fatal case". Clinical Toxicology. (2008)
- Pietro Manuel Ferraro, Eric N. Taylor, Giovanni Gambaro, and Gary C. Curhan. "Vitamin B6 Intake and the Risk of Incident Kidney Stones". Urolithiasis. (2017)
- Gary C Curhan. "Prevention of recurrent calcium stones in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/prevention-of-recurrent-calcium-stones-in-adults. [2020-05-18]
- Gary C Curhan. "Risk factors for calcium stones in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/risk-factors-for-calcium-stones-in-adults. [2020-02-13]
- "Kidney Stones". https://www.auanet.org/education/kidney-stones.cfm. [2016-07-01]
- Worcester E, Goldfarb S, Lam AQ. "Cystine Stones". UpToDate. UpToDate. https://www.uptodate.com/contents/cystine-stones. [2015-08-20]
- Grases F, Costa-Bauza A, Roig J, Rodriguez A. "Xanthine urolithiasis: Inhibitors of xanthine crystallization". PLoS ONE. 13(8). :e0198881. (2018)
- Curhan GC, Aronson MD, Preminger GM. "Diagnosis and acute management of suspected nephrolithiasis in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/diagnosis-and-acute-management-of-suspected-nephrolithiasis-in-adults?source=search_result&search=nephrolithiasis%20adult&selectedTitle=1~150#H2698242. [2015-11-11]
- Asif Sharfuddin, Sumit Kumar. "Renal colic: Keys to diagnosis and management". Nephrology. (2002)
- Stephen W. Leslie; Hussain Sajjad; Patrick B. Murphy.. "Renal Calculi". StatPearls. (2020)
- Pearle MS, Goldfarb DS, Assimos DG et al. "Medical management of kidney stones: AUA guideline.". J Urol. 192(2). :316-324. (2014)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Fontenelle LF, Sarti TD. "Kidney Stones: Treatment and Prevention.". Am Fam Physician. 99(8). :490-496. (2019)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Wilson ML, Gaido L. "Laboratory Diagnosis of Urinary Tract Infections in Adult Patients". Clin Infect Dis. 38(8). :1150-1158. (2004)
- Flores-Mireles et al. "Urinary tract infections: epidemiology, mechanisms of infection and treatment options". Nature Reviews Microbiology. 13(5). :269-284. (2015)
- Wiederkehr MR, Moe OW. "Uric Acid Nephrolithiasis: A Systemic Metabolic Disorder". Clin Rev Bone and Miner Metab. 9(3-4). :207-217. (2011)
- "American College of Radiology ACR Appropriateness Criteria® Acute Onset Flank Pain-Suspicion of Stone Disease". https://acsearch.acr.org/docs/69362/Narrative/. [2015-01-01]
- Gottlieb M, Long B, Koyfman A. "The evaluation and management of urolithiasis in the ED: A review of the literature". Am J Emerg Med. 36(4). :699-706. (2018)
- Mayans L. "Nephrolithiasis.". Prim Care. 46(2). :203-212. (2019)
- Moore CL, Carpenter CR, Heilbrun ME, et al. "Imaging in Suspected Renal Colic: Systematic Review of the Literature and Multispecialty Consensus". Journal of the American College of Radiology. (2019)
- Schoenfeld EM, Houghton C, Patel PM, et al. "Shared Decision Making in Patients With Suspected Uncomplicated Ureterolithiasis: A Decision Aid Development Study". Academic Emergency Medicine. 27(7). :554-565. (2020)
- Doty E, DiGiacomo S, Gunn B, Westafer L, Schoenfeld E. "What are the clinical effects of the different emergency department imaging options for suspected renal colic? A scoping review". JACEP Open. 2(3). (2021)
- Bowen DK, Tasian GE. "Pediatric Stone Disease". Urol Clin North Am. 45(4). :539-550. (2018)
- Viljoen A, Chaudhry R, Bycroft J. "Renal stones.". Ann Clin Biochem. 56(1). :15-27. (2019)
- "Surgical Management of Stones: American Urological Association/Endourological Society Guideline". https://web.archive.org/web/20220201221114/https://www.auanet.org/guidelines/guidelines/kidney-stones-surgical-management-guideline. [2016-05-27]
- Davenport K, Waine E. "The Role of Non-Steroidal Anti-Inflammatory Drugs in Renal Colic". Pharmaceuticals (Basel). 3(5). :1304-1310. (2010)
- McAninch JW, Lue TF. "Smith and Tanagho's General Urology, 19th Edition". McGraw-Hill Education / Medical. (2020). ISBN: 9781259834332
- BUTLER E. "Symptomatic nephrolithiasis complicating pregnancy". Obstetrics & Gynecology. 96(5). :753-756. (2000)
- Ordon M, Dirk J, Slater J, et al. "Incidence, Treatment, and Implications of Kidney Stones During Pregnancy: A Matched Population-Based Cohort Study". Journal of Endourology. 34(2). :215-221. (2020)
- Cao B, Daniel R, McGregor R, Tasian GE. "Pediatric Nephrolithiasis". Healthcare (Basel). 11(4). (2023)
- Hernandez JD, Ellison JS, Lendvay TS. "Current Trends, Evaluation, and Management of Pediatric Nephrolithiasis". JAMA pediatrics. 169(10). :964-70. (2015)
- Tasian GE, Ross ME, Song L, et al. "Annual Incidence of Nephrolithiasis among Children and Adults in South Carolina from 1997 to 2012". Clin J Am Soc Nephrol. 11(3). :488-96. (2016)
- Walls R, MD R, Hockberger R, et al. "Rosen's Emergency Medicine: Concepts and Clinical Practice". Elsevier. 1. (2022). ISBN: 9780323757898
- Expert Panel on Pediatric Imaging:, Dillman JR, Rigsby CK, et al. "ACR Appropriateness Criteria(®) Hematuria-Child". J Am Coll Radiol. 15(5S). :S91-S103. (2018)
- Lee JY, Andonian S, Bhojani N, et al. "Canadian Urological Association guideline: Management of ureteral calculi". Can Urol Assoc J.. 15(12). :E676-E690. (2021)
- Knight J, Madduma-Liyanage K, Mobley JA, Assimos DG, Holmes RP. "Ascorbic acid intake and oxalate synthesis". Urolithiasis. 44(4). :289-297. (2016)
- Assimos DG. "Vitamin C supplementation and urinary oxalate excretion.". Rev Urol. 6(3). :167. (2004)
- Stephenson A, Eggener SE, Bass EB, et al. "Diagnosis and Treatment of Early Stage Testicular Cancer: AUA Guideline". J Urol. 202(2). :272-281. (2019)
- Matlaga BR, Shah OD, Assimos DG. "Drug-induced urinary calculi". Rev Urol. 5(4). :227-31. (2003)