Summary
Nipple discharge can be physiological or pathological. Physiological discharge is typically bilateral, multiductal, with a milky appearance; causes include lactation and galactorrhea. Pathological discharge is typically unilateral, uniductal, nonmilky, and spontaneous. Although most causes of pathological nonmilky nipple discharge are benign (e.g., intraductal papilloma, mammary duct ectasia), malignancy is an important consideration. The diagnostic approach to nipple discharge is based on clinical evaluation findings, including characteristics of the discharge and patient age. Further evaluation with imaging is required for all patients with red flags in nipple discharge. Treatment depends on the underlying cause.
Nipple discharge in male individuals is not addressed in this article.
Classification
-
Physiological nipple discharge [1]
- Bilateral discharge from multiple ducts
- Typically milky; may be green or clear
- Usually provoked (i.e., after nipple stimulation or expression)
-
Pathological nipple discharge [1]
- Unilateral discharge that typically originates from a single duct
- Nonmilky; may be clear, bloody, or serosanguineous
- Usually spontaneous (i.e., occurs without nipple stimulation or expression)
Etiology
Physiological nipple discharge [1][2][3]
- Lactation: discharge related to pregnancy or breastfeeding
-
Galactorrhea
- Discharge unrelated to pregnancy or breastfeeding
-
Caused by physiological, pharmacological, pathological or idiopathic hyperprolactinemia: ; [4][5][6]
- Endocrine disorders (e.g., hypothyroidism, prolactinomas)
- Medications (e.g., dopamine antagonists, TCAs)
- Chronic nipple stimulation (e.g., piercings, tight clothing)
- See “Etiology of hyperprolactinemia” for details.
Pathological nipple discharge [1][2][3]
-
Benign breast conditions
- Intraductal papilloma (most common) [7]
- Mammary duct ectasia
- Fibrocystic breast changes
- Breast abscess
- Malignancy (5–15% of cases): most commonly ductal carcinoma in situ [7]
Intraductal papilloma is the most common cause of pathological nipple discharge accounting for up to 58% of cases. [7]
Clinical evaluation
Focused history [1][2]
- Nature of discharge (e.g., color, laterality, spontaneous vs. provoked)
- Obstetric history (e.g., time since last pregnancy and breastfeeding)
- Medication review for drugs that can cause galactorrhea (see “Etiology of hyperprolactinemia”)
- Nipple stimulation (e.g., from tight-fitting clothing or during sexual activity)
Focused examination [1][2]
Perform a clinical breast examination to assess for:
- Palpable breast mass
- Visible nipple discharge (spontaneous or after expression)
- Characteristics of nipple discharge (e.g., color, involvement of single or multiple ducts)
Red flags in nipple discharge [1][2]
The following are red flag features for malignancy.
-
Characteristics of pathological nipple discharge
- Unilateral
- Uniductal
- Persistent
- Spontaneous
- Clear, bloody, or serosanguineous
- Breast mass
- Risk factors for breast cancer (e.g., advanced age, positive family history)
Diagnosis
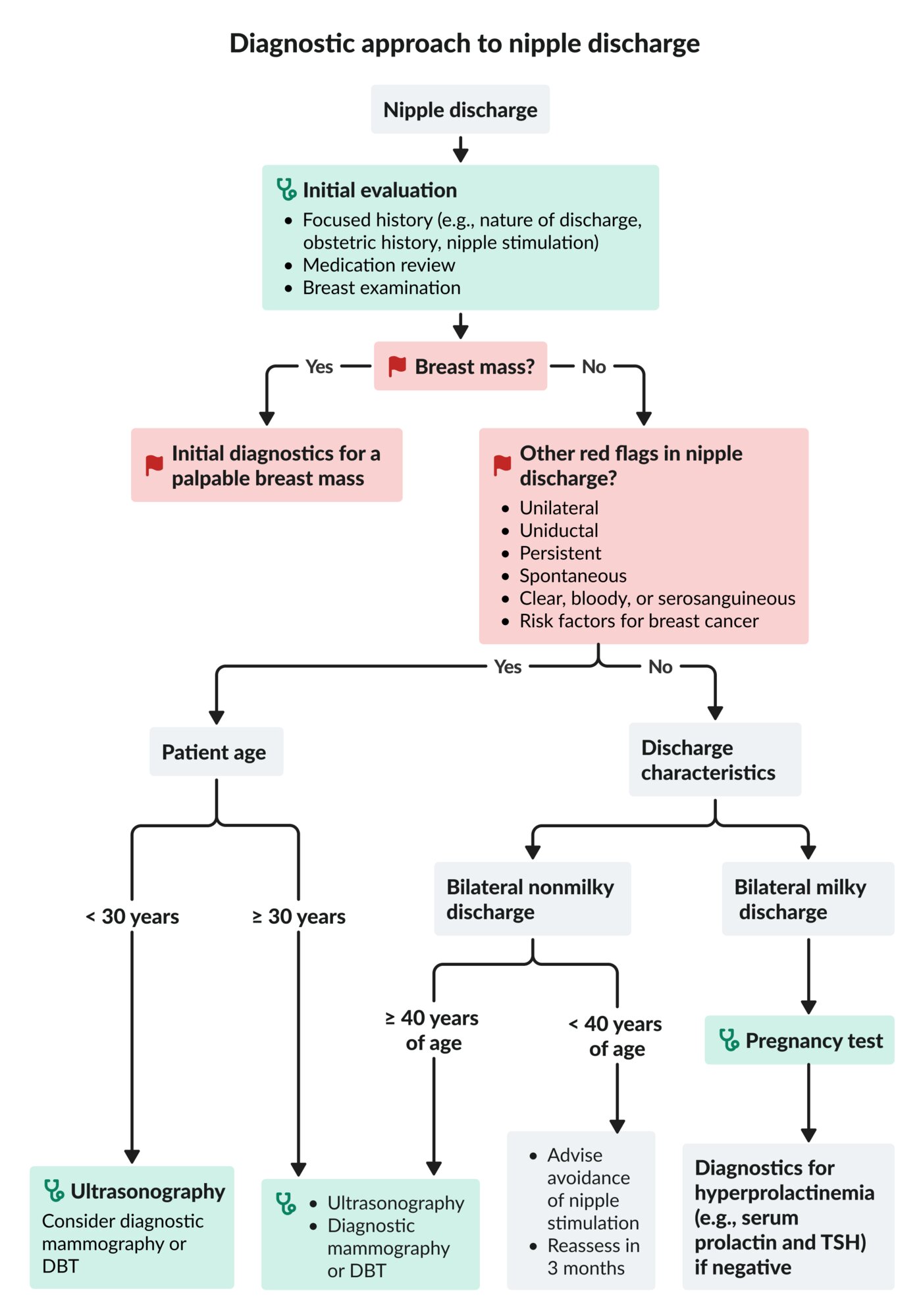
Initial diagnostic approach [1][2][3]
Perform a focused clinical evaluation in all patients, including for red flags in nipple discharge.
Presence of red flags
- Breast mass: Obtain initial diagnostics for a palpable breast mass and manage accordingly.
-
Other red flags in nipple discharge
-
Patients ≥ 30 years of age ; [2][3]
- Ultrasonography
- AND diagnostic mammography or digital breast tomosynthesis (DBT)
-
Patients < 30 years of age
- Ultrasonography
- Consider diagnostic mammography or DBT. [1]
-
Patients ≥ 30 years of age ; [2][3]
No red flags
Perform evaluation based on the characteristics of the discharge.
-
Bilateral milky discharge
- All patients: pregnancy test
- If pregnancy test is negative, perform diagnostics for hyperprolactinemia (e.g., serum prolactin and TSH levels).
-
Nonmilky discharge
- Patients aged ≥ 40 years [1]
- Ultrasonography
- AND diagnostic mammography or DBT
- Patients aged < 40 years: Advise avoidance of nipple stimulation and reassess in 3 months.
- Patients aged ≥ 40 years [1]
Additional studies [1][2][3]
-
Indications
- Diagnostic uncertainty
- Follow-up of abnormal findings on initial imaging
- Preprocedural planning
-
Modalities
- Breast MRI
- Ductography
- Breast biopsy
Biopsy is necessary if imaging findings are concerning for malignancy (e.g., BI-RADS 4 or 5). [2]

DBT: digital breast tomosynthesis
TSH: thyroid-stimulating hormone
© AMBOSS
Common causes
| Common causes of nipple discharge [1][2] | |||
|---|---|---|---|
| Distinguishing clinical features | Diagnostic findings | Management | |
| Pregnancy and breastfeeding |
|
|
|
| Galactorrhea |
|
|
|
| Intraductal papilloma |
|
|
|
| Mammary duct ectasia |
|
|
|
| Breast cancer |
|
|
|
| Fibrocystic breast changes |
|
|
|
| Breast abscess |
|
|
|
Treatment
Treatment is based on the underlying cause; see “Common causes of nipple discharge.” [1][2]
-
Physiological nipple discharge
- Lactation: Advise patients that milky discharge may continue for one year after the end of pregnancy or breastfeeding.
-
Galactorrhea
- Physiological hyperprolactinemia: Advise avoidance of nipple stimulation and reassess in 3 months.
- Pathological or pharmacological hyperprolactinemia: See “Treatment of hyperprolactinemia.”
-
Pathological nipple discharge
- Concern for malignancy: Management is based on biopsy results; consult appropriate specialists.
-
For all other patients (e.g., with BI-RADS 1–3 on imaging), consider either:
- Duct excision
- Clinical and imaging surveillance for 24 months [1][2]
External Resources
References
- Salzman B, Collins E, Hersh L. "Common Breast Problems". Am Fam Physician. 99(8). :505-514. (2019)
- ACOG. "Practice Bulletin No. 164 Diagnosis and management of benign breast disorders". Obstetrics & Gynecology. 127(6). :e141-e156. (2016)
- "ACR Appropriateness Criteria® Evaluation of Nipple Discharge"
- Samperi I, Lithgow K, Karavitaki N. "Hyperprolactinaemia". J Clin Med. 8(12). :2203. (2019)
- Bruehlman RD, Winters S, McKittrick C. "Galactorrhea: Rapid Evidence Review". Am Fam Physician. 106(6). :695-700. (2022)
- Peña KS, Rosenfeld JA. "Evaluation and treatment of galactorrhea". Am Fam Physician. 63(9). :1763-70. (2001)
- Gupta D, Mendelson EB, Karst I. "Nipple Discharge: Current Clinical and Imaging Evaluation". AMJ Am J Roentgenol. 216(2). :330-339. (2021)
- Eiada R, Chong J, Kulkarni S, Goldberg F, Muradali D. "Papillary Lesions of the Breast: MRI, Ultrasound, and Mammographic Appearances". AJR Am J Roentgenol. 198(2). :264-271. (2012)
- Calvillo KZ, Portnow LH. "Intraductal papillomas of the breast". Ann Breast Surg. 5. :24-24. (2021)
- Ferris-James DM et al. "Imaging Approaches to Diagnosis and Management of Common Ductal Abnormalities". RadioGraphics. 32(4). :1009-1030. (2012)
- Choe J, Chikarmane SA, Giess CS. "Nonmass Findings at Breast US: Definition, Classifications, and Differential Diagnosis". RadioGraphics. 40(2). :326-335. (2020)
- Cheung H, Parker EU, Yu M, Kilgore MR, Lam DL. "Radiologic and Pathologic Correlation for Benign Breast Processes". Curr Breast Cancer Rep. 13(4). :381-397. (2021)
- Cho SH, Park SH. "Mimickers of Breast Malignancy on Breast Sonography". Journal Ultrasound Med. 32(11). :2029-2036. (2013)
- Trop I, Dugas A, David J, et al. "Breast Abscesses: Evidence-based Algorithms for Diagnosis, Management, and Follow-up". RadioGraphics. 31(6). :1683-1699. (2011)