Summary
Lymphomas are malignancies that arise from lymphocytes and are classified as either Hodgkin lymphomas (characterized by Reed-Sternberg cells) or non-Hodgkin lymphomas (NHLs), which comprise all other types of lymphoma. NHLs are further classified according to cell type, i.e., B cells, T cells, and natural killer (NK) cells; location (nodal or extranodal); and tumor grade. Low-grade tumors originate from mature cells that have a slow growth rate and an indolent clinical course. The most common low-grade B-cell lymphoma is follicular lymphoma, while the most common low-grade T-cell lymphomas are cutaneous T-cell lymphomas, such as mycosis fungoides. High-grade tumors have a rapid growth rate and an aggressive clinical course. Certain subtypes of NHL, such as Burkitt lymphoma, are more common in children and young adults than in older adults. NHL is diagnosed by obtaining a biopsy of the affected tissue and carrying out a detailed assessment, including immunophenotyping, genetics, and molecular testing. These studies allow for the identification of specific NHL subtypes, which guides treatment. Generally, treatment involves a combination of chemotherapy and radiation therapy. Patients with high-grade NHLs and those with low-grade tumors and limited disease are treated with curative intent. Patients with advanced, low-grade tumors who experience symptoms usually receive palliative treatment.
Epidemiology
- Incidence: NHL is the most common hematopoietic neoplasm. [1]
-
Age
- The incidence of all NHLs increases with age; the peak incidence is in those aged > 50 years.
- High-grade lymphomas are most common in children and young adults (20–40 years).
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Chromosomal translocations: most commonly t(14;18)
-
Infections [2]
- EBV
- HIV
- HTLV-1
- HCV
- Helicobacter pylori: associated with gastric lymphoma, e.g., MALT lymphoma, diffuse large B-cell lymphoma (DLBCL)
- Autoimmune diseases: Hashimoto thyroiditis, rheumatoid arthritis
- Immunodeficiency: congenital immunodeficiencies, AIDS, history of chemotherapy and/or immunosuppressive therapy
- Environmental factors: aromatic hydrocarbons (e.g., benzene), radiation
Overview
B-cell lymphomas (85% of all NHLs)
| B-cell lymphomas | ||
|---|---|---|
| Grade | Lymphoma | Features |
| Indolent (low-grade) | Follicular lymphoma |
|
| Hairy cell leukemia |
|
|
| Marginal zone B-cell lymphomas (MZLs): a group of lymphomas that arise from postgerminal center B cells |
|
|
| Waldenstrom macroglobulinemia |
|
|
| Small lymphocytic lymphoma (SLL) [3] |
|
|
| Aggressive (high-grade) | Diffuse large B-cell lymphoma |
|
| Mantle cell lymphoma [6] |
|
|
| Burkitt lymphoma [7] |
|
|
| Precursor B-cell lymphoblastic lymphoma |
|
|
Burkitt lymphoma is most common in kids.
")




")



T-cell lymphomas (15% of all NHL)
| T-cell lymphomas | ||
|---|---|---|
| Grade | Lymphoma | Features |
| Indolent (low-grade) | Mycosis fungoides: most common form of cutaneous T-cell lymphoma (a type of lymphoma characterized by malignant T-cell infiltration of the skin) |
|
| Aggressive (high-grade) | Sezary syndrome (leukemic form of cutaneous T-cell lymphoma) [8] |
|
| Adult T-cell lymphoma [9] |
|
|
| Aggressive NK-cell leukemia [10] |
|
|
| Angioimmunoblastic T-cell lymphoma [11] |
|
|
| Precursor T-cell lymphoblastic lymphoma |
|
|
Think of an aggressive man to remember that the occurrence of mantle cell lymphoma is greater in men and that the disease has an aggressive course.
Hair can get TRAPped in the hairdryer: hairy cell leukemia, TRAP stain, dry tap.







Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: Prof. Dr. Karl-Anton Kreuzer, Facharzt für Innere Medizin, Hämatologie und Onkologie
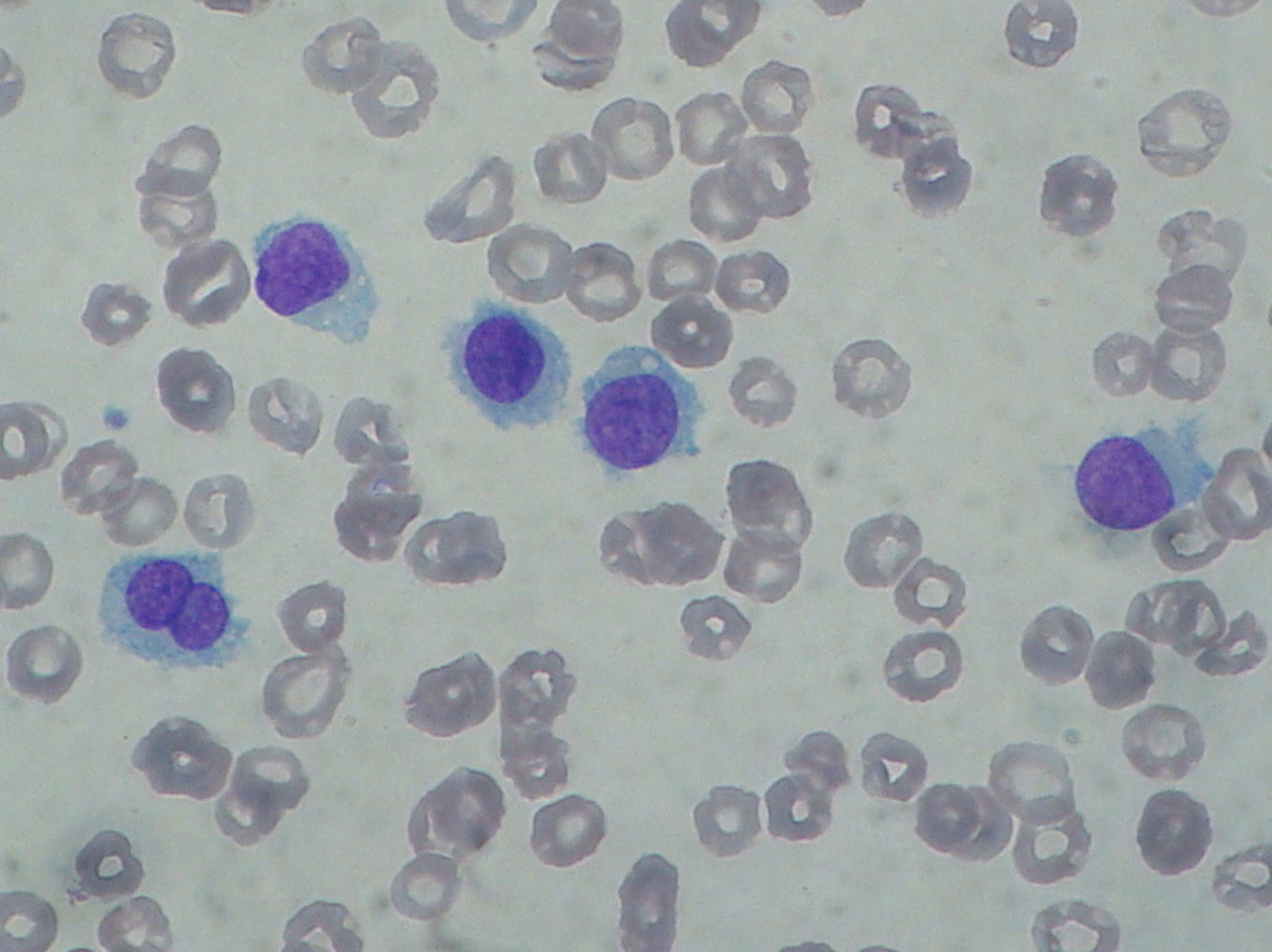
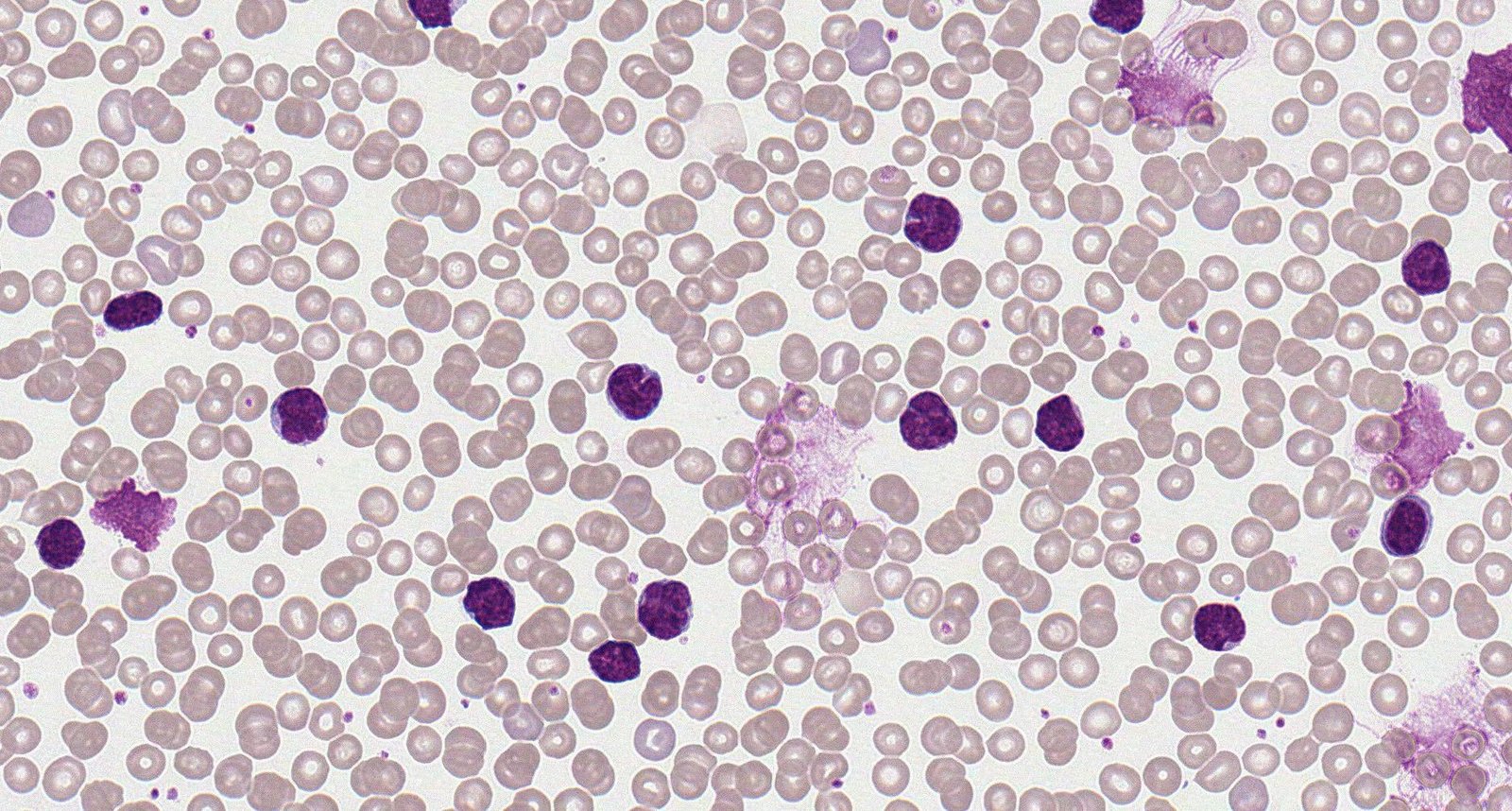
Photomicrograph of a peripheral blood smear (May-Grunwald Giemsa stain; very high magnification)
Multiple atypical lymphocytes (examples indicated by blue circles) can be seen among numerous normal erythrocytes (examples indicated by white arrowheads) in the center of the image. The cell membrane of these lymphocytes feature fine, hair-like cytoplasmic projections (examples indicated by black arrowheads) and enlarged nuclei with slightly irregular borders (examples indicated by dashed line). A binuclear cell is also present (arrow).
The presence of atypical lymphocytes with hair-like cytoplasmic projections in a peripheral blood smear indicates hairy cell leukemia. The diagnosis was confirmed on immunophenotyping.
Source: “Hairy cell leukemia smear 2009-08-20” by Paulo Henrique Orlandi Mourao, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
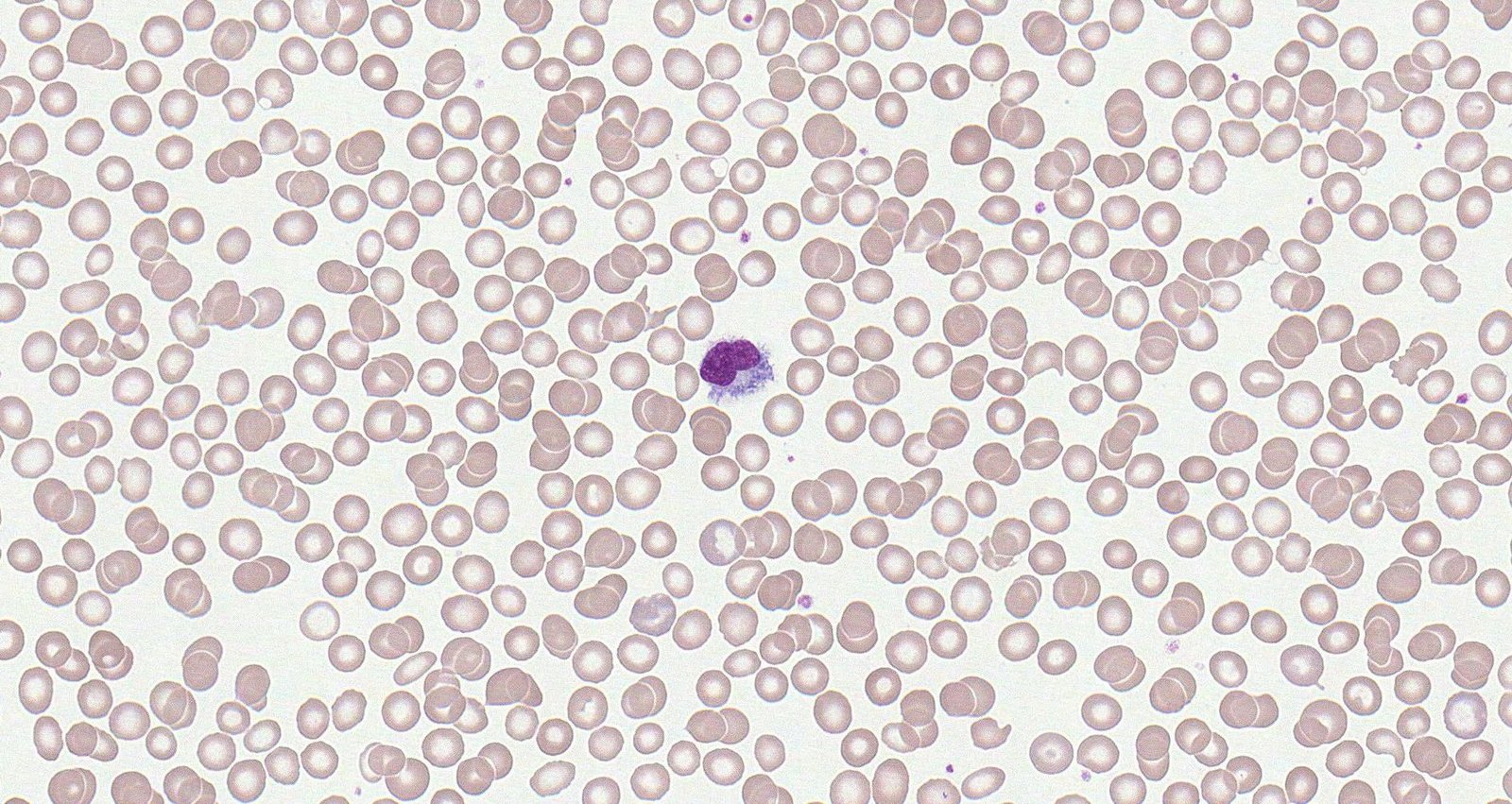
Photomicrograph of a peripheral blood smear (high magnification)
In the center of the image, a lymphocyte with an abnormal appearance is visible. Due to the villous extensions of its basophilic cytoplasm, it is referred to as a hairy cell.
This is the typical appearance of hairy cell leukemia.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: Prof. Dr. Karl-Anton Kreuzer, Facharzt für Innere Medizin, Hämatologie und Onkologie
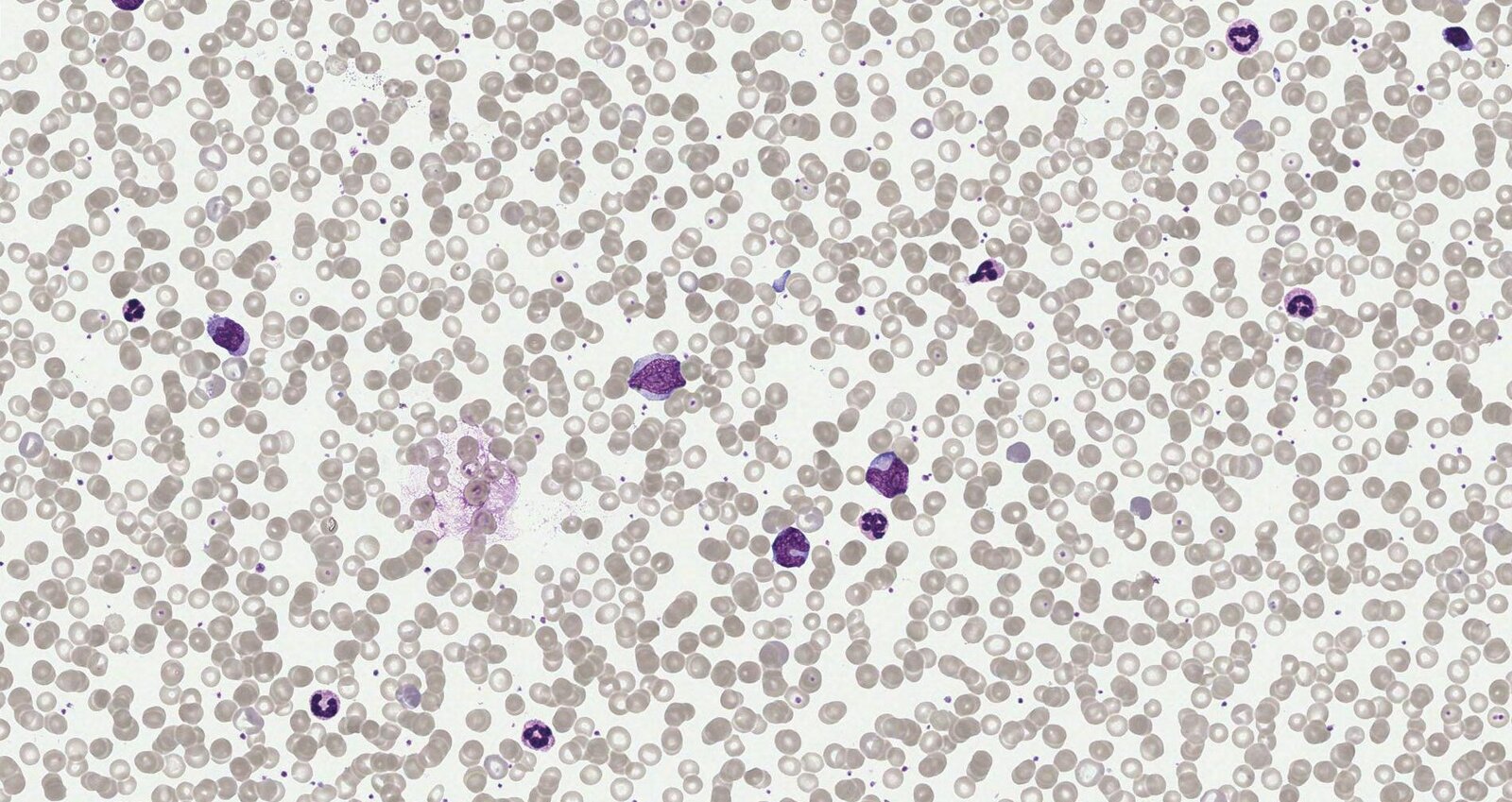
Photomicrograph of a peripheral blood smear (Giemsa stain; high magnification)
Large atypical lymphoid cells (black arrowheads) with enlarged, eccentric nuclei, vesicular chromatin, and amphophilic cytoplasm can be seen. This appearance raises suspicion for diffuse large B-cell lymphoma (DLBCL). Immunophenotyping (evaluating the expression of CD20, CD10, MUM1, and BCL6) is required to confirm the diagnosis.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: Prof. Dr. Karl-Anton Kreuzer, Facharzt für Innere Medizin, Hämatologie und Onkologie
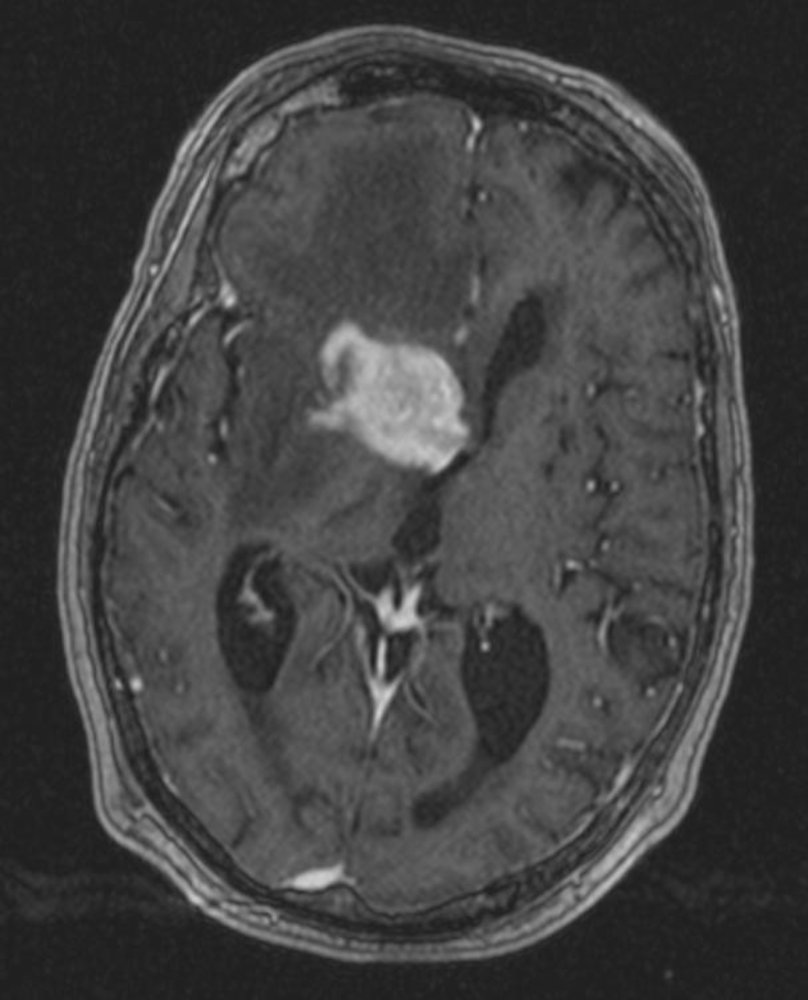
MRI head (T1-weighted; with contrast; axial plane) of a patient with primary CNS lymphoma
A mass with its epicenter in the region of the right basal ganglia shows intense contrast enhancement. There is a large amount of perilesional vasogenic edema. Mass effect has effaced the anterior horn of the right lateral ventricle and caused contralateral shift of the midline structures.
Source: “Tumor PrimaryCNSLymphoma T1Axial” by Tdvorak, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: Prof. Dr. Karl-Anton Kreuzer, Facharzt für Innere Medizin, Hämatologie und Onkologie
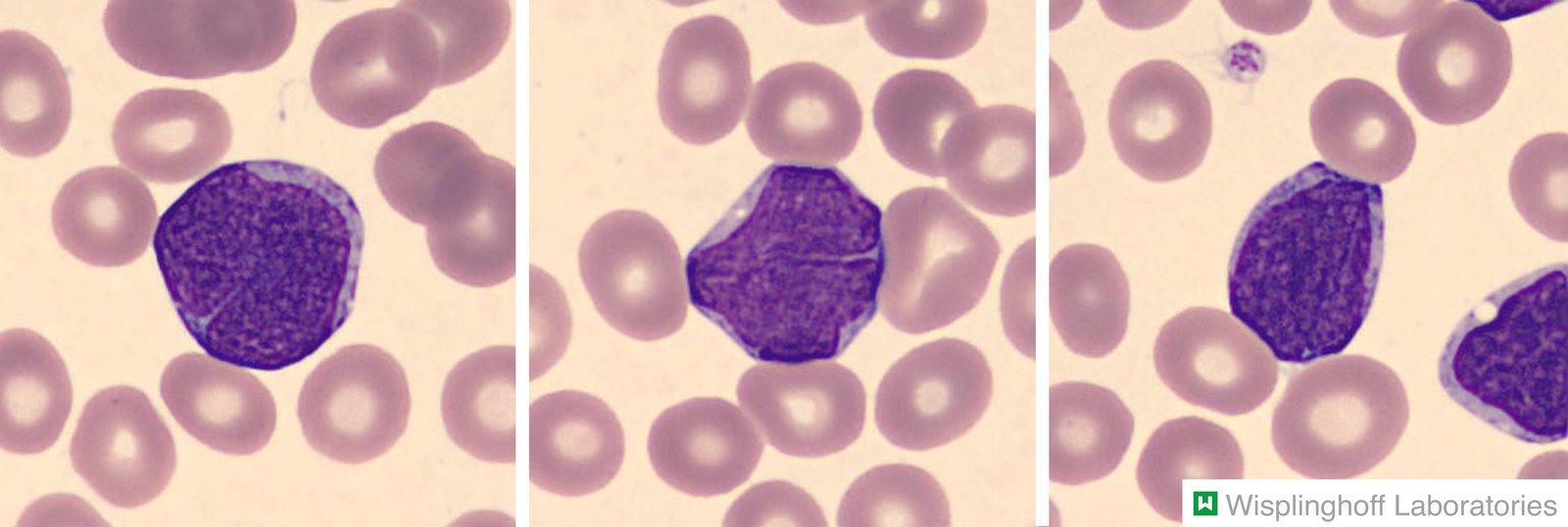
Blood smear of a 47-year-old patient with lymphadenopathy and lymphocytosis (78,000/μL).
Increased presence of lymphoblasts showing reduced cytoplasm and condensed nuclei. The diagnosis was confirmed by histological evaluation of an affected lymph node.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.

Seven-year-old boy from Nigeria
A massive swelling with central ulceration and peripheral scaling is visible above the right mandible.
The age and origin of the boy as well as the localization of the lymphoma most likely indicate the endemic form of Burkitt lymphoma (mainly found in Africa), which is associated with the Epstein Barr virus (EBV).
Source: “Large facial Burkitt's Lymphoma” by Mike Blyth, Wikimedia Commons, licensed under CC BY-SA 2.5. Modifications: Added censor bars.
{kind=link}
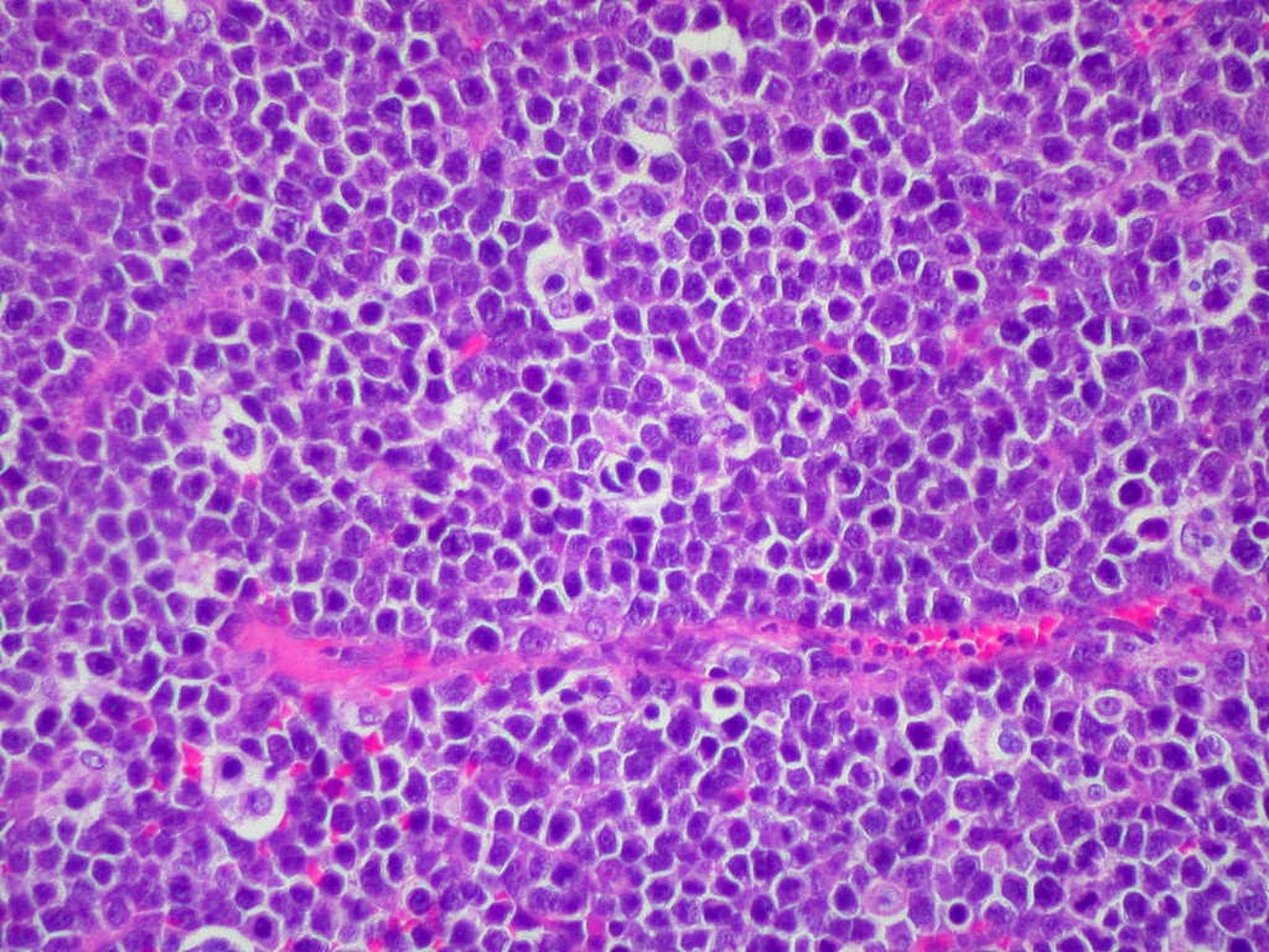
Photomicrograph of lymph node tissue (H&E stain, high magnification)
Large macrophages with clear cytoplasm (examples indicated by green overlays) are interspersed with numerous medium-sized, monomorphic neoplastic lymphocytes. This appearance is known as the starry sky pattern and is a characteristic feature of Burkitt lymphoma. Many of the lymphoma cells show mitotic activity (examples indicated by yellow overlays).
Source: “Burkitt lymphoma, H&E” by Ed Uthman, M.D., Flickr, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

Multiple partially confluent, sharply demarcated, erythematous, scaling plaques are visible on this patient's flank.
This appearance is suggestive of cutaneous lymphoma.
Source: © IMPP
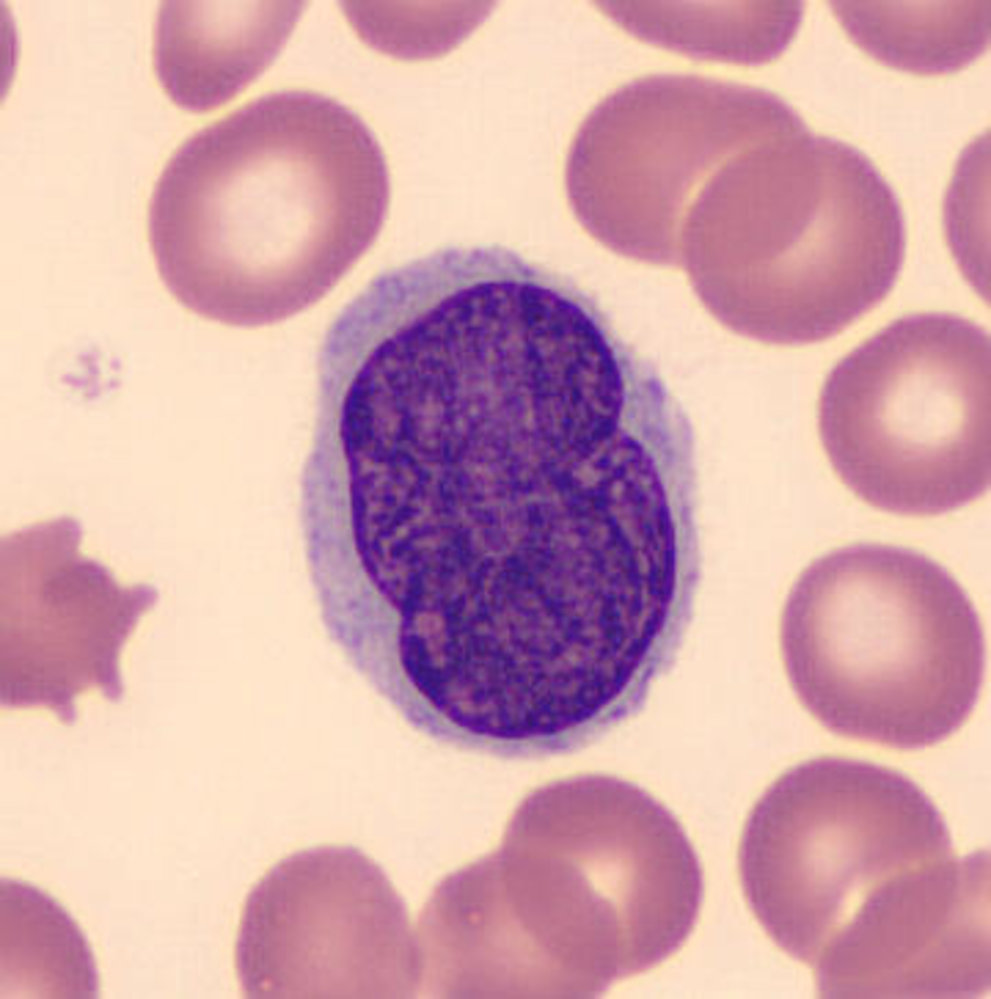
Photomicrograph of a peripheral blood smear (Giemsa staining)
In the center, there is an atypical lymphocyte. The cell is large (approximately twice the size of the surrounding erythrocytes) with light purple (basophilic) cytoplasm, and a convoluted or “brain-like” (cerebriform) dark purple nucleus.
This is the typical appearance of a Sézary cell, a lymphocyte that occurs in Sézary syndrome (a form of cutaneous T-cell lymphoma).
Source: “Hem1SezaryCell2” by EL*Falaf, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
© AMBOSS
© AMBOSS
© AMBOSS
© AMBOSS
Clinical features
-
Nodal disease: typically painless lymphadenopathy associated with fatigue and weakness (multiple noncontiguous lymph nodes may be involved) ; [12][13]
- High grade
- Rapidly growing mass/nodes
- Constitutional symptoms or B symptoms (i.e., weight loss, fever, night sweats)
- Low grade
- Slow-growing or undulant lymphadenopathy (over months or years)
- Hepatosplenomegaly
- Cytopenias: Patients may present with anemia or bleeding, or have an increased susceptibility to infections.
- High grade

-
Extranodal disease (primary or secondary): The symptoms are highly dependent on the affected tissue; B symptoms are common. [12][13]
- GI tract: e.g., early satiety, GI bleeding
- Neurological involvement: e.g., headache, focal neurologic symptoms
- Primary cutaneous NHL or secondary skin infiltration: e.g., rash, plaques, tumors, ulcers
- Thyroid involvement (rare): e.g., nodules, goiter
-
Oncologic emergencies/paraneoplastic syndromes [12][13]
- Examples include tumor lysis syndrome, hypercalcemia, spinal cord compression, superior vena cava syndrome, cardiac tamponade, lymphomatous meningitis, and a CNS mass.
- See “Oncologic emergencies” for detailed information on the management of these conditions.



A swollen superficial cervical lymph node is visible below this patient's right mandible.
Source: “Cervical lymphadenopathy right neck” by Coronation Dental Specialty Group, Wikimedia Commons, licensed under CC BY-SA 4.0. Modifications: Removed red arrows.
{kind=link}

Left upper arm, shoulder, and back with sharply demarcated, partially confluent, erythematous scaling lesions that are severely pruritic.
Source: © IMPP

Multiple, well-demarcated, partially confluent, erythematous patches are visible on the posterior thighs.
This appearance is typical of mycosis fungoides.
Source: Courtesy of Dr. Gary M. White, MD
Multiple partially confluent, sharply demarcated, erythematous, scaling plaques are visible on this patient's flank.
This appearance is suggestive of cutaneous lymphoma.
Source: © IMPP
Differential diagnoses
See ”Differential diagnosis of B symptoms”, “Enlarged lymph nodes”, and “Differential diagnosis of granulomatous disease” for more information.
Extranodal masses
- Thymoma
- Teratoma (and other germ cell tumors)
- Thyroid neoplasm
The 4 T's of anterior mediastinal masses: Thymoma, Teratoma (and other germ cell tumors), Thyroid neoplasm, and Terrible lymphoma.
Necrotizing lymphadenitis (Kikuchi-Fujimoto disease) [14]
- Etiology: unknown
-
Epidemiology
- Rare; most commonly reported in Asian population
- Sex: ♀ > ♂
- Mean age: 30 years
- Clinical features: painful cervical lymphadenopathy and fever
- Diagnostics: Lymph node biopsy shows single or multiple necrotic foci, histiocytic cellular infiltration, without granulocytic involvement.
- Treatment: typically resolves spontaneously within 1–4 months of onset without treatment
The differential diagnoses listed here are not exhaustive.
Diagnosis
Approach [15][16][17]
- Suspect NHL in patients with suggestive clinical or laboratory features.
- Confirm the diagnosis and determine the subtype via lymph node and/or tissue biopsies.
- Stage and classify the disease (see “Staging of NHL”), e.g.:
- Imaging studies: to determine the extent of the disease and detect possible CNS involvement
- Bone marrow aspiration and biopsy: to detect bone marrow involvement
The clinical presentation of patients with NHL varies (e.g., nodal symptoms, extranodal symptoms, oncologic emergencies, or paraneoplastic syndromes); therefore, clinicians must maintain a high index of suspicion to facilitate early diagnosis.
Laboratory studies [16]
-
Routine laboratory studies
- CBC: may show anemia, thrombocytopenia; WBC count may be high or low (commonly leukopenia, lymphocytosis)
- BMP: may show abnormal renal function [18]
- Serum calcium: may show hypercalcemia
- Liver chemistries: may be abnormal in patients with liver infiltration or primary hepatic lymphoma [19]
-
Markers of disease activity [16][20]
- Uric acid: usually elevated
- LDH: usually elevated
- Serum β2-microglobulin: may be elevated
- Others: CRP, ESR
-
Viral serologies
- HIV screening
- Additional studies can be suggestive of the underlying etiology (e.g., hepatitis B and C, EBV, HTLV-1).
Confirmatory diagnostics tests [13][15][17]
Histopathological studies are required to diagnose lymphoma. Large samples are preferred as intact tissue architecture is required to classify the subtype. If initial biopsy results are negative in patients with symptoms that are highly suggestive of lymphoma, consider obtaining a larger biopsy sample and repeating the studies.
Selection of biopsy sample
-
Nodal disease
- Select the most appropriate node for biopsy (e.g., a node with significant, progressive, and persistent enlargement).
- Imaging methods such as CT and PET-CT may be used to select a site (see “Staging of NHL”).
- Techniques [17]
- Preferred: excisional lymph node biopsy or core needle biopsy
- Alternative: incisional lymph node biopsy
- Avoid fine-needle aspiration biopsy.
-
Extranodal disease
- Excisional tissue biopsies are recommended.
- Biopsies frequently require guidance, e.g., with endoscopy or using ultrasound.



Histopathology and specialized studies
These studies help determine the subtype of NHL.
- Histopathology: provides a detailed morphology of individual proliferating cells and a description of the pattern of lymph node (or tissue) infiltration (e.g., nodular, diffuse)
-
Immunophenotype (e.g., flow cytometry, immunohistochemistry)
- Detects surface antigens, determines the specific cell type (B cell/T cell), and identifies specific markers
- Possible findings include:
- B-cell lymphomas: CD20 positive
- T-cell lymphomas: CD3 positive
-
Genetic studies
- Cytogenetics (karyotype, FISH): can identify chromosomal abnormalities, e.g., t(14;18) in follicular lymphoma
- Molecular testing (e.g., PCR): can detect clonality, e.g., in B-cell receptors or T-cell receptors



It is important to identify CD20-positive lymphomas, as patients may benefit from targeted therapy with CD20 antibodies (e.g., rituximab).
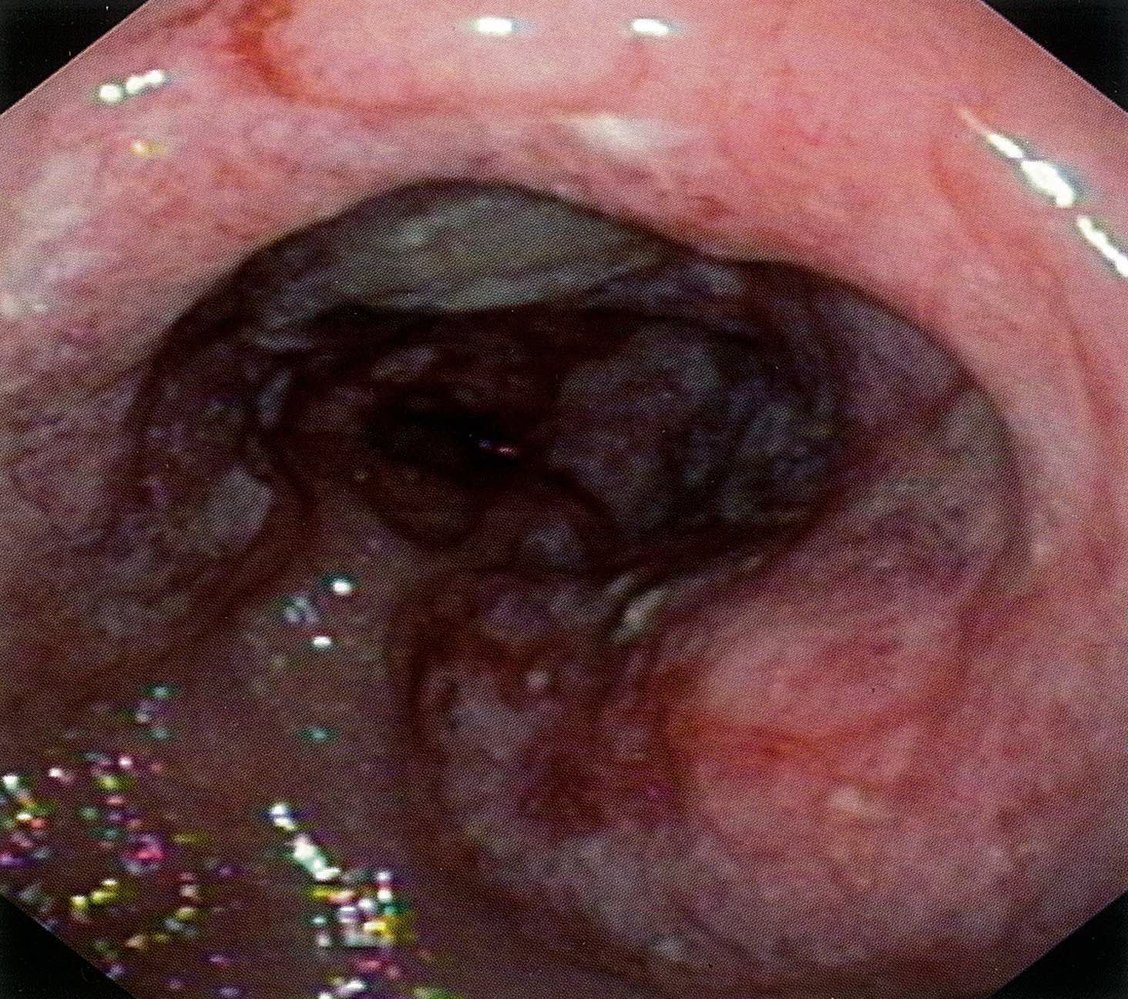
Endoscopic view of the stomach
A tumor that spans almost the entire circumference of the pyloric antrum is visible (green overlay). The surface is ulcerated and the vascular pattern is irregular.
Ulcerations in the stomach should raise suspicion of malignancy. Histopathological examination of the tumor biopsy revealed a diffuse, medium-sized B-cell lymphoma (low-grade marginal zone MALT lymphoma).
Source: © IMPP
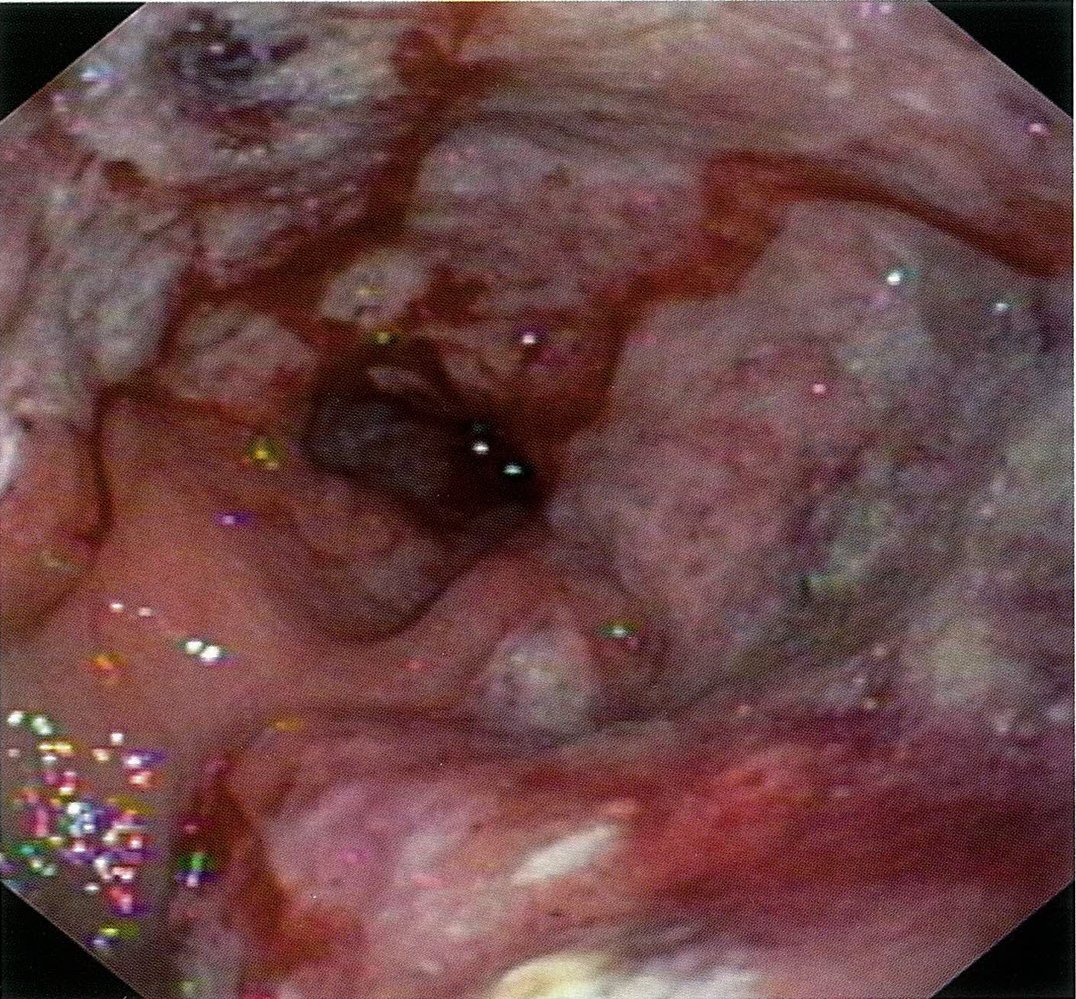
Endoscopic view of the stomach
An ulcerative tumor (green overlay) spans most of the circumference of the pyloric antrum. Consequently, narrowing of the pylorus (pyloric stenosis) is visible.
Ulcerations in the stomach should raise suspicion of malignancy. Histopathological examination of the tumor biopsy revealed a B-cell non-Hodgkin lymphoma.
Source: © IMPP

Ultrasound abdomen (liver; oblique plane) of a patient with hepatic lymphoma
A rounded mixed echogenicity hepatic mass with a hypoechoic periphery (dark green overlay) and slightly hyperechoic center (light green overlay) can be seen. Posterior acoustic enhancement can also be seen (white area).
Hepatic lymphoma does not have a characteristic ultrasound appearance. The differential includes several other pathologies, including other tumors, complicated cyst, and abscess.
L: liver parenchyma
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
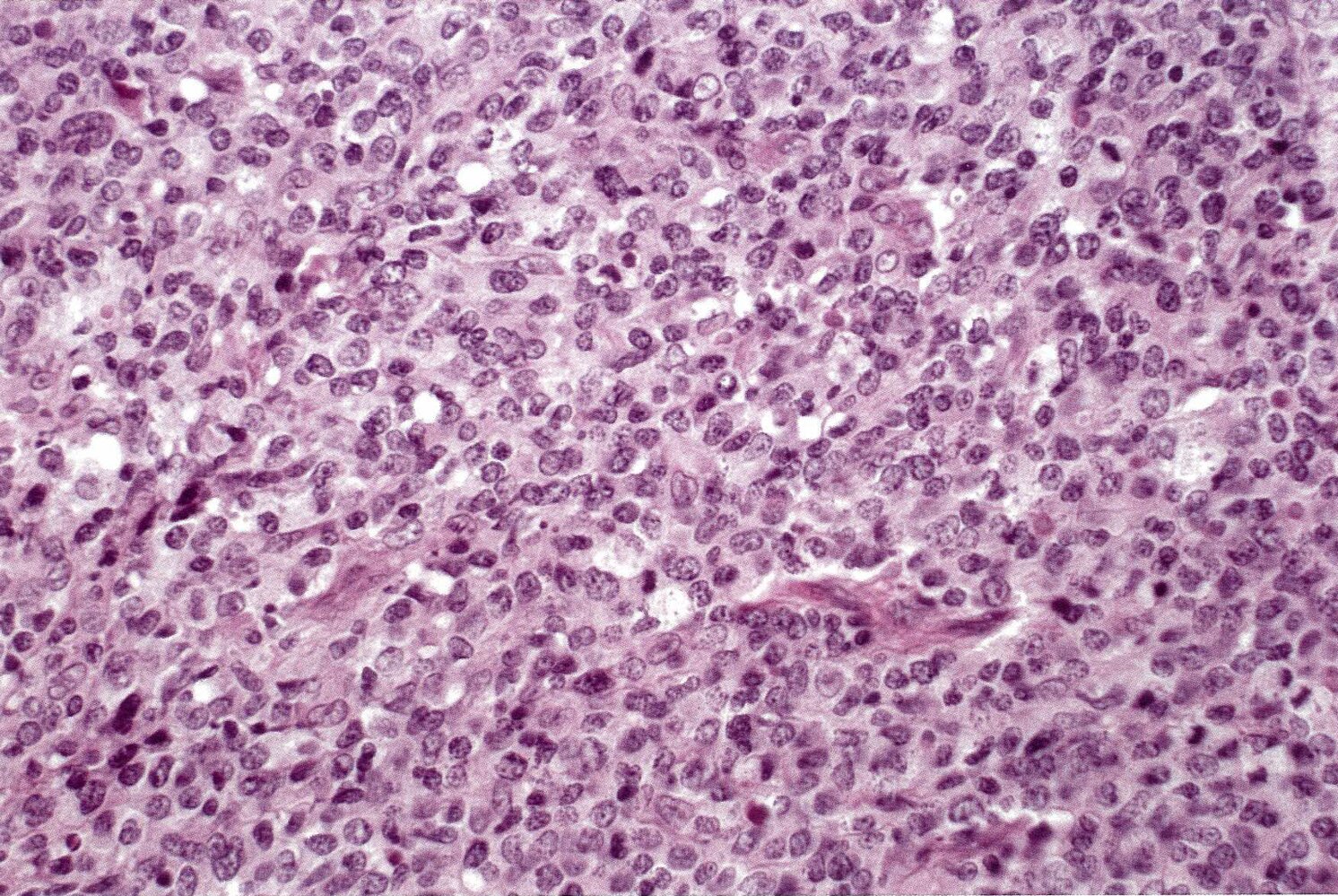
Photomicrograph of ileum tissue (H&E staining; very high magnification) showing densely arranged poorly differentiated cells.
Source: © IMPP
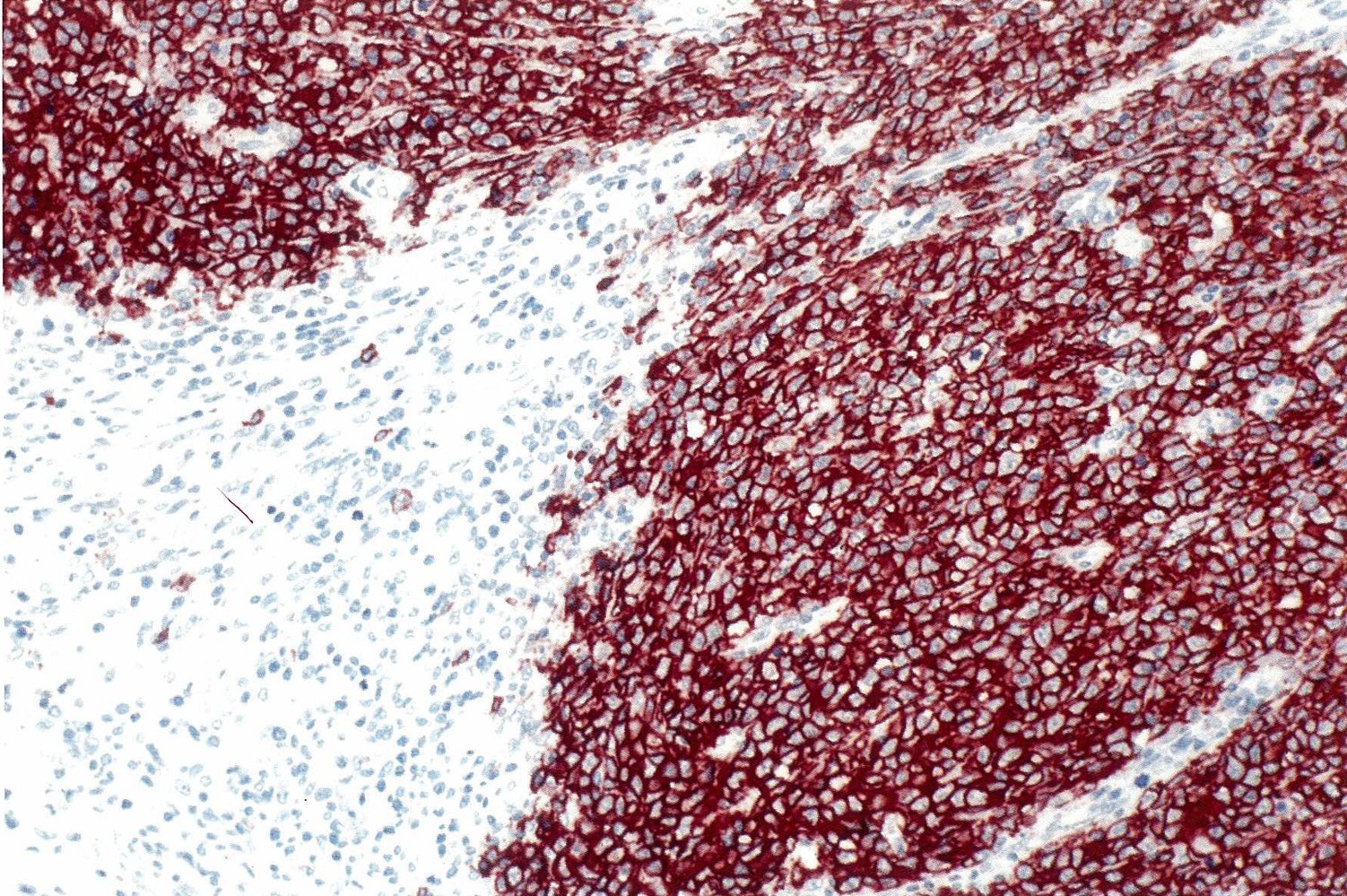
Photomicrograph of ileum tissue (CD20 immunohistochemistry stain; high magnification)
Anti-CD20 antibody has been used to selectively stain B cells (the CD20 antigen is a classic B cell surface marker).
Source: © IMPP

Photograph of a specimen resected from the ileum (longitudinal section)
The normal anatomy of the ileal wall is visible at the left and right edges of the specimen. From top to bottom at the left edge: mucosa (green overlay), submucosa (red overlay), muscularis propria (blue overlay), serosa (orange line).
Centrally a solid, white-gray mass has infiltrated the muscularis and submucosa. The mass does not originate from the mucosa, which can be seen extending intact across the upper edge of the specimen (green overlay) with no erosions or polypoid lesions; this rules out primary adenocarcinoma. Macroscopically, important differentials include lymphomas, neuroendocrine tumors, and metastases, but further testing (e.g., immunohistochemistry) was required to confirm the diagnosis of non-Hodgkin lymphoma.
Source: © IMPP
Staging and classification
Staging [15]
-
Imaging
- Indicated in all patients for staging and to assess response to therapy
- Choice of imaging modality depends on the suspected subtype of NHL (uptake of FDG varies between subtypes)
- FDG-avid NHLs (most subtypes): PET-CT
- Non-FDG-avid NHLs : CT whole body with contrast
- Bone marrow aspiration and biopsy: indicated in most newly diagnosed patients with NHL
-
Assessment of CNS involvement
- Indications
- Patients considered high-risk for CNS involvement [21]
- Primary CNS lymphoma
- Patients with neurological signs and symptoms
- Patients with HIV
-
Recommended modalities include:
- Imaging (MRI or CT brain)
- Lumbar puncture with CSF assessment (cytology; detection of EBV DNA)
- Indications


Classification [15]
-
Lugano classification is the preferred classification method for primary nodal NHL.
- Imaging is used to assess the number and location of affected lymph nodes, tumor bulk, and liver and spleen involvement.
- Bone marrow biopsy to assess bone marrow involvement
- The disease is then classified as either:
- Limited disease (stage I + II): one node or conglomerate (stage I), or ≥ 2 nodes or conglomerates on one side of the diaphragm (stage II)
- Advanced disease (stage III + IV): nodes on both sides of the diaphragm or supradiaphragmatic nodes with splenic involvement (stage III), or diffuse or disseminated disease (stage IV)
- See “Lugano classification of lymphomas” for more information.
- Previously, a version of the Cotswolds-modified Ann Arbor system was used, excluding the presence of B symptoms.
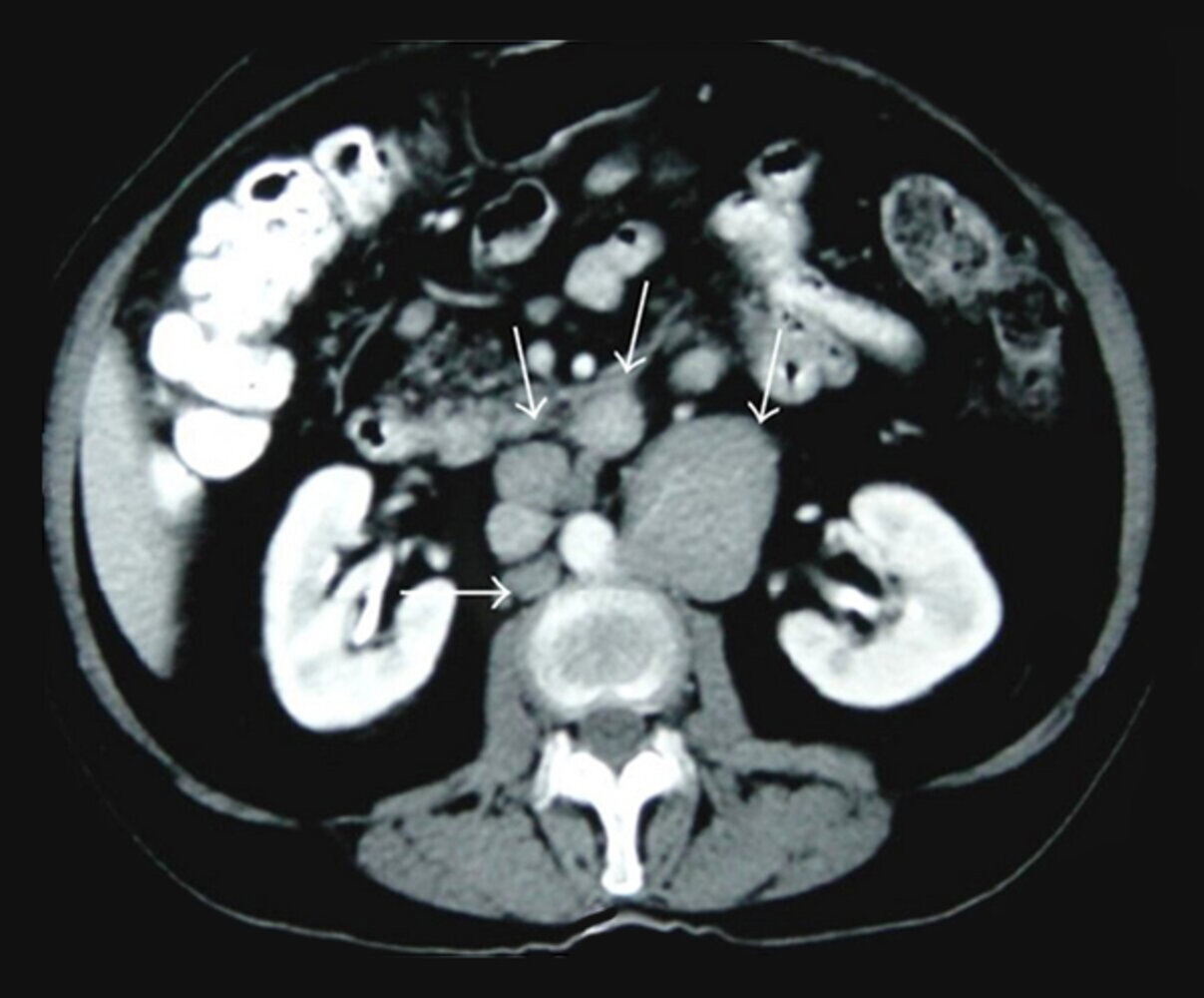
CT abdomen (with oral and IV contrast; axial plane)
Multiple enlarged lymph nodes are present in the paraaortic retroperitoneum (white arrows).
C: colon; K: kidney; A: aorta; IVC: inferior vena cava
Source: “Figure 2, in: Abdominal Manifestations of Lymphoma: Spectrum of Imaging Features” by Adonis Manzella , Paulo Borba-Filho, Giuseppe D'Ippolito and Marcella Farias, Hindawi, licensed under CC BY 3.0. Modifications: removed white frame and in-image text. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
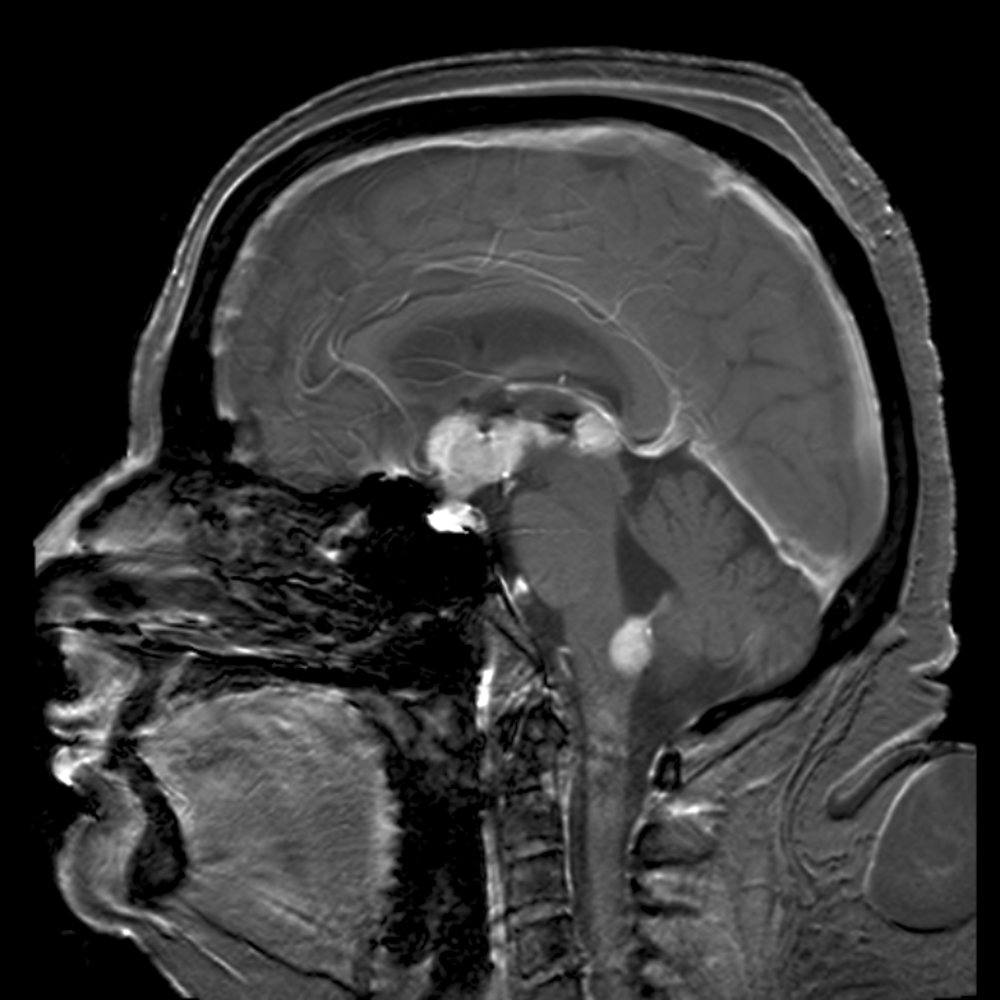
MRI brain (T1 weighted; with contrast; sagittal plane) of a patient with primary CNS lymphoma
Several rounded lesions showing intense contrast enhancement are demonstrated in the regions of the sella turcica and suprasellar space, pineal recess, and base of the fourth ventricle.
Further investigation confirmed the diagnosis of primary CNS lymphoma.
Source: “Primary central nervous system B-cell non-Hodgkin lymphoma” by Steven Fruitsmaak, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
MRI head (T1-weighted; with contrast; axial plane) of a patient with primary CNS lymphoma
A mass with its epicenter in the region of the right basal ganglia shows intense contrast enhancement. There is a large amount of perilesional vasogenic edema. Mass effect has effaced the anterior horn of the right lateral ventricle and caused contralateral shift of the midline structures.
Source: “Tumor PrimaryCNSLymphoma T1Axial” by Tdvorak, Wikimedia Commons, licensed under CC BY-SA 3.0.
Treatment
Most patients with newly diagnosed NHL require chemotherapy, radiotherapy, or both. In some patients with indolent NHLs, such as follicular lymphoma, occasionally a watch and wait strategy can be used. Consultation with a hematologist-oncologist is essential for planning and initiating treatment.
Approach [16][22]
- Perform prechemotherapy screening.
- Select treatment based on the subtype of NHL, staging, and prognosis
- Most patients will receive treatment with systemic chemotherapy and/or radiotherapy.
- Low-grade NHL (initial stages): Consider radiotherapy with curative intent.
- Low-grade NHL (advanced stages): usually palliative chemotherapy
- High-grade NHL: usually chemotherapy with curative intent
- Select patients may benefit from additional interventions, including splenectomy and hematopoietic stem cell transplantation (HSCT).
- Most patients will receive treatment with systemic chemotherapy and/or radiotherapy.
- Provide supportive treatment: see also “Principles of cancer care.”
- Adequate hydration and nutrition
- Management of chemotherapy-induced nausea and vomiting and other side effects of chemotherapy
- DVT prophylaxis
- Consider prophylaxis for tumor lysis syndrome. [23]
Prechemotherapy screening is essential in all patients receiving chemotherapy for NHL to adequately adjust chemotherapeutic doses according to patients' hepatic, renal, and cardiac function.
Medical therapy
Treatment options [22]
-
Radiotherapy
- May be curative or palliative
- Can be conventional or in form of radioimmunotherapy, in which engineered monoclonal antibodies that are specific for tumor antigens are bound to radioactive nucleotides, which results in higher doses of radiation reaching the target cancer cells and less off-target effects.
-
Systemic chemotherapy: Regimens usually include combinations of chemotherapeutic agents, steroids, and immunotherapy.
- Antifolates: high-dose methotrexate ; (in combination with leucovorin) for primary CNS lymphoma
- Alkylating agents: e.g., cyclophosphamide (C)
- Topoisomerase II inhibitors: e.g., etoposide (E), doxorubicin/hydroxydaunorubicin (H)
- Alkaloids: e.g., vincristine/oncovin (V/O)
- Steroids: e.g., prednisolone (P), dexamethasone
- Immunotherapy: e.g., rituximab (R)
- Intrathecal chemotherapy: Intrathecal methotrexate can be considered for leptomeningeal involvement.
Specific regimens [16][22]
Below is a summary of some of the common treatment regimens found in the literature for select NHL subtypes; these regimens are intended to provide an overview only and treatment decisions should be tailored to the patient and the features of the disease (e.g., specific mutations, location, extent).
CHOP is the most common regimen in NHL, with the addition of rituximab (CD20 antibody) for B-cell neoplasms (R-CHOP).
| Treatment regimens for non-Hodgkin lymphomas [16][22] | ||
|---|---|---|
| Subtype | Frequently used treatment | |
| Mature B-cell neoplasms |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Mature T-cell neoplasms |
|
|
| ||
| ||
| Cutaneous T-cell lymphoma |
|
|
Some new therapies are emerging as part of the management of certain types of NHLs, including targeted therapies (e.g., ibrutinib) and monoclonal antibodies (e.g., mogamulizumab). If available, a specialist may choose to use them depending on the individual evaluation of each patient.
Additional therapies [22][24]
-
Surgery
- Splenectomy: Consider in select patients with B-cell lymphomas with splenic involvement (e.g., splenic MZL, hairy cell leukemia).
- Surgical resection: Consider in select patients with specific NHL subtypes.
-
HSCT
- Consider in relapsing or refractory disease for some NHL subtypes, e.g., DLBCL, mantle cell lymphoma, mature T-cell lymphoma.
Prognosis
-
Typically, the prognosis of NHL is worse than that of Hodgkin lymphoma. [25]
- Low-grade lymphomas: median survival of 6–10 years
- High-grade lymphomas: survival typically several months (years in less aggressive variants)
- Indicators of poor prognosis: old age, number of involved nodal and extranodal sites, ↑ LDH, ↑ beta2 microglobulin [26]
References
- "Non-Hodgkin Lymphoma Risk Factors". https://www.cancer.org/cancer/non-hodgkin-lymphoma/causes-risks-prevention/risk-factors.html. [2020-06-09]
- Kellerman RD. "Conn's Current Therapy 2020". Elsevier. (2019). ISBN: 9780323711845
- Goldman L, Schafer AI. "Goldman-Cecil Medicine, 2-Volume Set". Elsevier. (2019). ISBN: 9780323532662
- Cheson BD, Fisher RI, Barrington SF, et al. "Recommendations for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The Lugano Classification". J Clin Oncol. (2014)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Kroft SH, Sever CE, Bagg A, et al. "Laboratory Workup of Lymphoma in Adults". Arch Pathol Lab Med. (2020)
- Li SJ, Chen HP, Chen YH, et al. "Renal involvement in non-Hodgkin lymphoma: proven by renal biopsy". PLoS ONE. 9(4). :e95190. (2014)
- Oliver Tavabie, Abid R. Suddle. "Lymphoma and hematological conditions: I. Lymphoma and liver complications of bone marrow transplant". Clinical Liver Disease. 8(1). :1-5. (2016)
- A.N. Pavlidis, J. Kalef-Ezra, L.C. Bourantas, A. Lambrou, A. Mavridis. "Serum Tumor Markers in Non-Hodgkin's Lymphomas and Chronic Lymphocytic Leukemia". Int J Biol Markers. 8(1). :14-20. (1993)
- Mahajan T, Merriman RC, Stone MJ. "Kikuchi-Fujimoto Disease (Histiocytic Necrotizing Lymphadenitis): Report of a Case with Other Autoimmune Manifestations". Baylor University Medical Center Proceedings. 20(2). :149-151. (2007)
- Caligiuri M, Levi MM, Kaushansky K, et al. "Williams Hematology, 9E". McGraw-Hill Education / Medical. (2015). ISBN: 9780071833004
- Belay Y, Yirdaw K, Enawgaw B. "Tumor Lysis Syndrome in Patients with Hematological Malignancies". Journal of Oncology. 2017. :1-9. (2017)
- Weledji EP, Orock GE. "Surgery for Non-Hodgkin's Lymphoma.". Oncology reviews. 9(1). :274. (2015)
- "Key Statistics for Non-Hodgkin Lymphoma". https://www.cancer.org/cancer/non-hodgkin-lymphoma/about/key-statistics.html. [2020-01-08]
- "Survival Rates and Factors That Affect Prognosis (Outlook) for Non-Hodgkin Lymphoma". https://www.cancer.org/cancer/non-hodgkin-lymphoma/detection-diagnosis-staging/factors-prognosis.html. [2020-01-08]
- Gayer G, Luboshitz J, Hertz M, et al. "Congenital Anomalies of the Inferior Vena Cava Revealed on CT in Patients with Deep Vein Thrombosis". American Journal of Roentgenology. 180(3). :729-732. (2003)
- "Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma (CLL/SLL)". http://www.lymphoma.org/site/pp.asp?c=bkLTKaOQLmK8E&b=6300147. [2016-12-01]
- Pasqualucci L. "The genetic basis of diffuse large B-cell lymphoma.". Curr Opin Hematol. 20(4). :336-44. (2013)
- Cerami E. "AACR Project GENIE: Powering Precision Medicine through an International Consortium". Cancer Discovery. 7(8). :818-831. (2017)
- "Mantle Cell Lymphoma". https://rarediseases.org/rare-diseases/mantle-cell-lymphoma/. [2005-01-01]
- Freedman AS, Aster JC. "Epidemiology, clinical manifestations, pathologic features, and diagnosis of Burkitt lymphoma". UpToDate. UpToDate. https://www.uptodate.com/contents/epidemiology-clinical-manifestations-pathologic-features-and-diagnosis-of-burkitt-lymphoma?source=search_result&search=burkitt%20lymphoma&selectedTitle=1~76. [2016-09-14]
- Rook AH, Olsen EA, Kuzel TM, Zic JA, Rosmarin AG. "Clinical Presentation, Pathologic Features, and Diagnosis of Sézary Syndrome". UpToDate. UpToDate. https://www.uptodate.com/contents/clinical-presentation-pathologic-features-and-diagnosis-of-sezary-syndrome. [2016-07-14]
- Matutes E. "Adult T-cell leukaemia/lymphoma". J Clin Pathol. 60(12). :1373-1377. (2006)
- Ishida F. "Aggressive NK-Cell Leukemia". Frontiers in Pediatrics. 6. (2018)
- "Angioimmunoblastic T-Cell Lymphoma". https://rarediseases.org/rare-diseases/angioimmunoblastic-t-cell-lymphoma/. [2017-07-18]
- Jingjing Ma, Qing Li, Jie Shao, et al. "Central Nervous System Involvement in Patients with Diffuse Large B Cell Lymphoma: Analysis of the Risk Factors and Prognosis from a Single-Center Retrospective Cohort Study". Cancer Manag Res. Volume 11. :10175-10185. (2019)
- Freedman AS, Friedberg DW. "Evaluation, staging, and response assessment of non-Hodgkin lymphoma". UpToDate. UpToDate. https://www.uptodate.com/contents/evaluation-staging-and-response-assessment-of-non-hodgkin-lymphoma. [2017-02-02]