Summary
Childbirth begins with the onset of labor, which consists of contractions that lead to progressive cervical dilation and effacement, eventually resulting in the birth of the infant and expulsion of the placenta. The process of normal childbirth depends on a high degree of anatomical and physiological compatibility between the mother and child. The birth canal is the passage consisting of the mother's bony pelvis and soft tissues through which a fetus passes during vaginal delivery. Fetal orientation during childbirth is described in terms of lie, presenting part, position, attitude of the presenting part, and station. The clinical status of the mother and fetus should be consistently monitored during labor and delivery. Obstetric analgesia should be offered, and prophylaxis for neonatal GBS infection should be given during labor if indicated. While vaginal delivery is typically preferred, cesarean delivery may be indicated under certain circumstances. Complications of normal vaginal delivery include perineal lacerations, hemorrhage, nerve injuries, and coccydynia.
See “Abnormal labor and delivery” for intrapartum complications and their management.
Orientation in utero
For the management of fetal malpresentation, see “Obstructed labor.”
Fetal lie
- Definition: relation of the fetal long axis to the long axis of the maternal uterus
-
Types
- Longitudinal lie: fetus is in the same axis (most common)
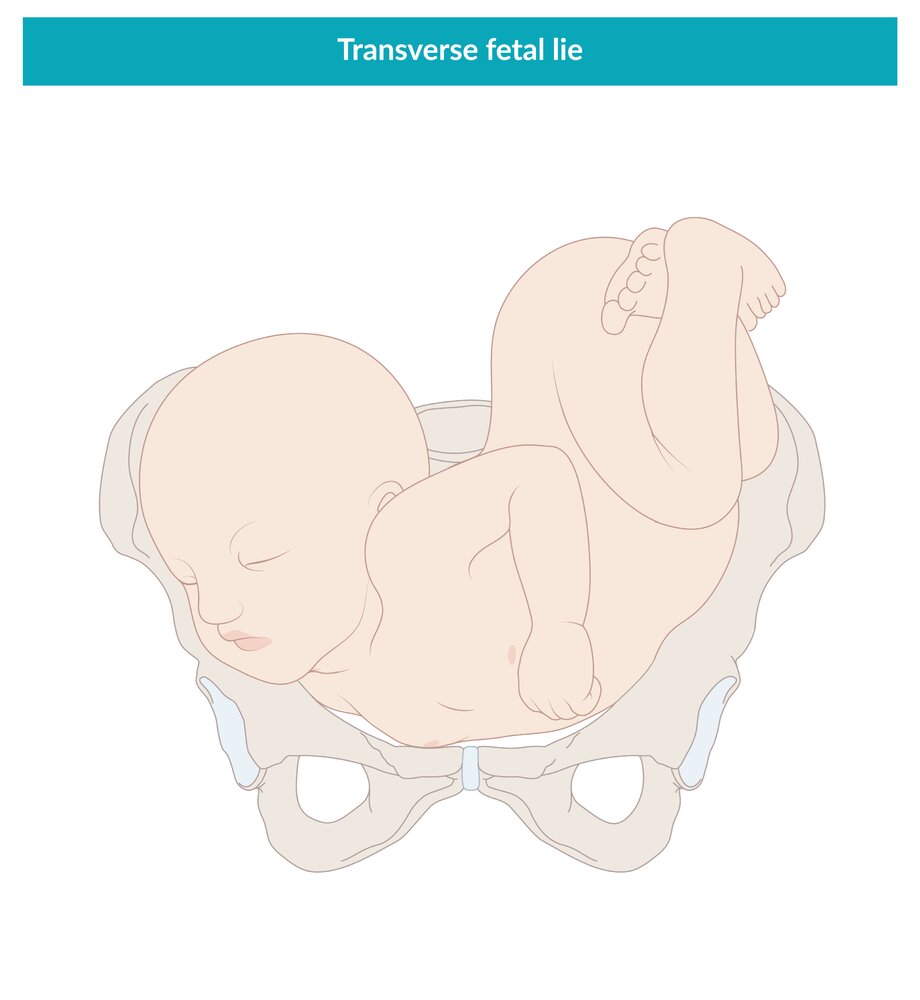
- Transverse lie: fetus is at a 90° angle
- Oblique lie: fetus is at a 45° angle


Fetal presentation
- Definition: part of the fetus that overlies the maternal pelvic inlet
-
Types
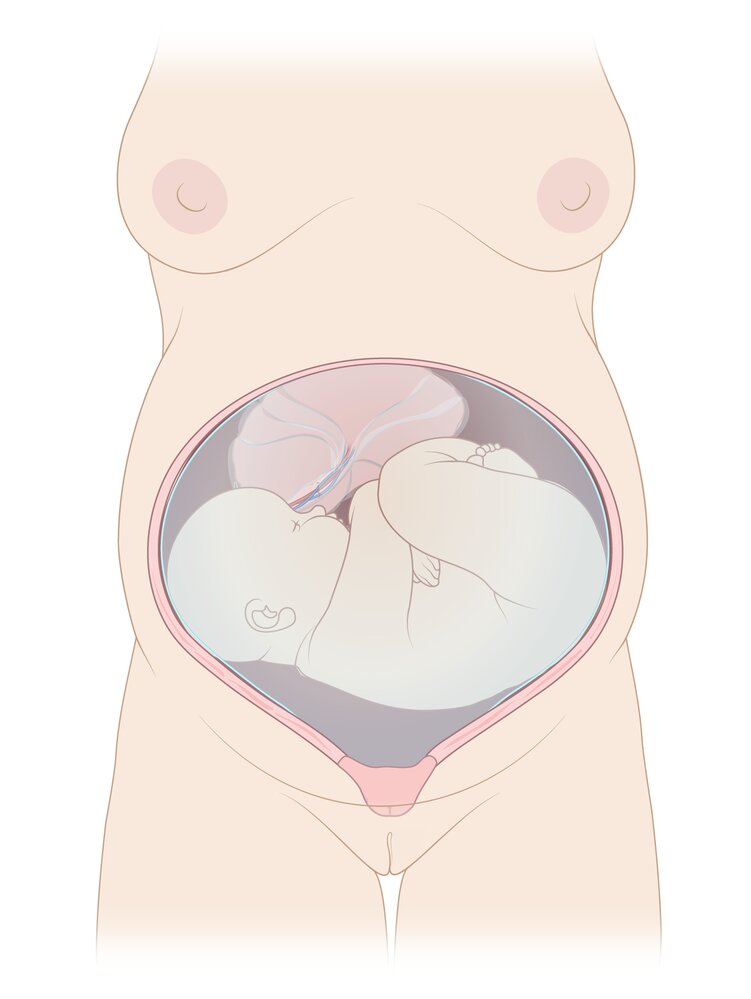
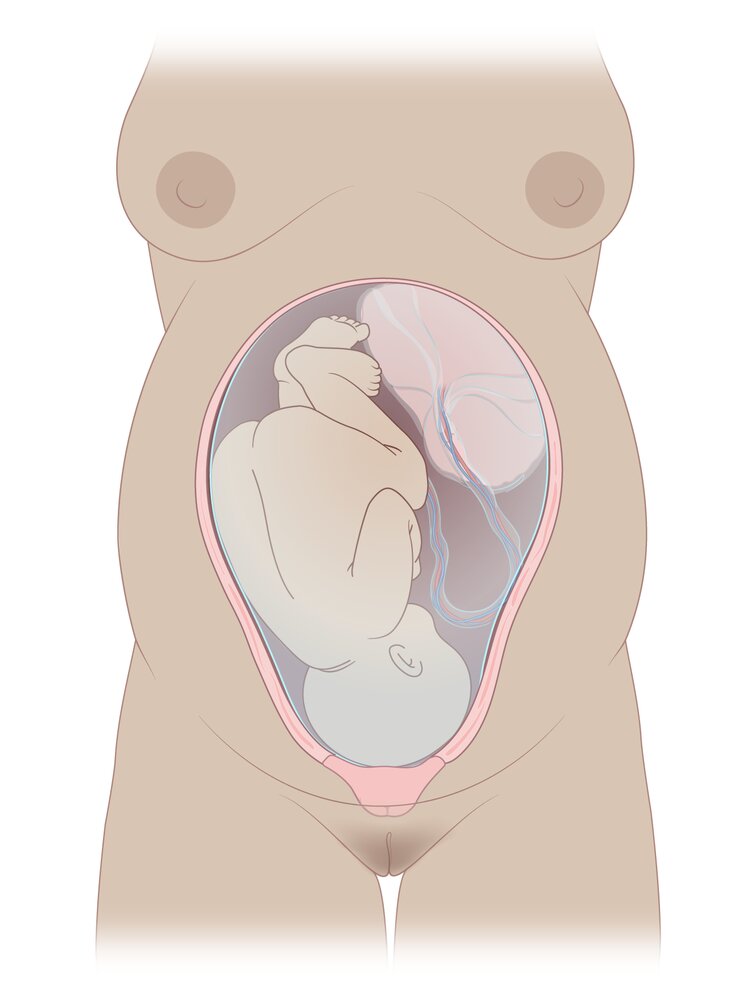
- Cephalic presentation: head (most common)
-
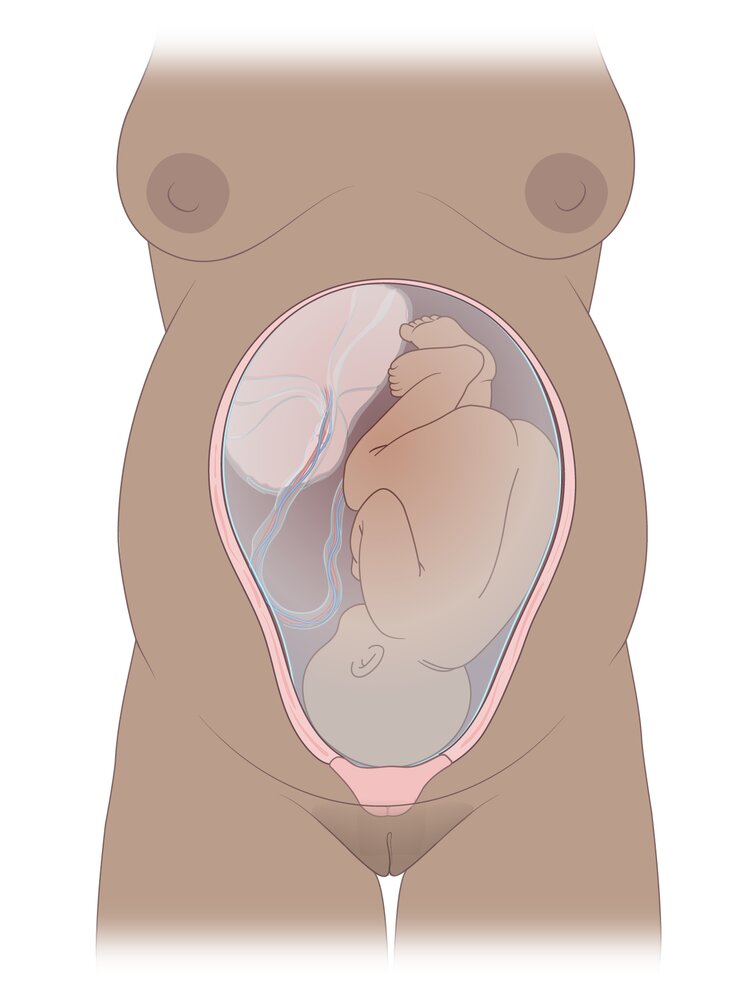
Breech presentation: buttocks or feet
- Frank breech: flexed hips and extended knees (buttocks presenting)
- Complete breech: thighs and legs flexed (cannonball position)
- Single footling breech: hip of one leg is flexed and the knee of the other is extended (one foot presenting)
- Double footling breech: both thighs and legs are extended (feet presenting)
- Compound presentation: ≥ 1 anatomical presenting part (e.g., cephalic or breech presentation with presentation of an extremity)
- Shoulder presentation: shoulder presentations combined with a transverse or oblique lie
")
")





Fetal position
- Definition: relationship and orientation (i.e., fetal occiput pointing towards maternal left or right) of the presenting fetal part to the maternal pelvis
-
Types
-
Occiput anterior position: Fetal occiput points towards maternal symphysis pubis; fetus faces downwards.
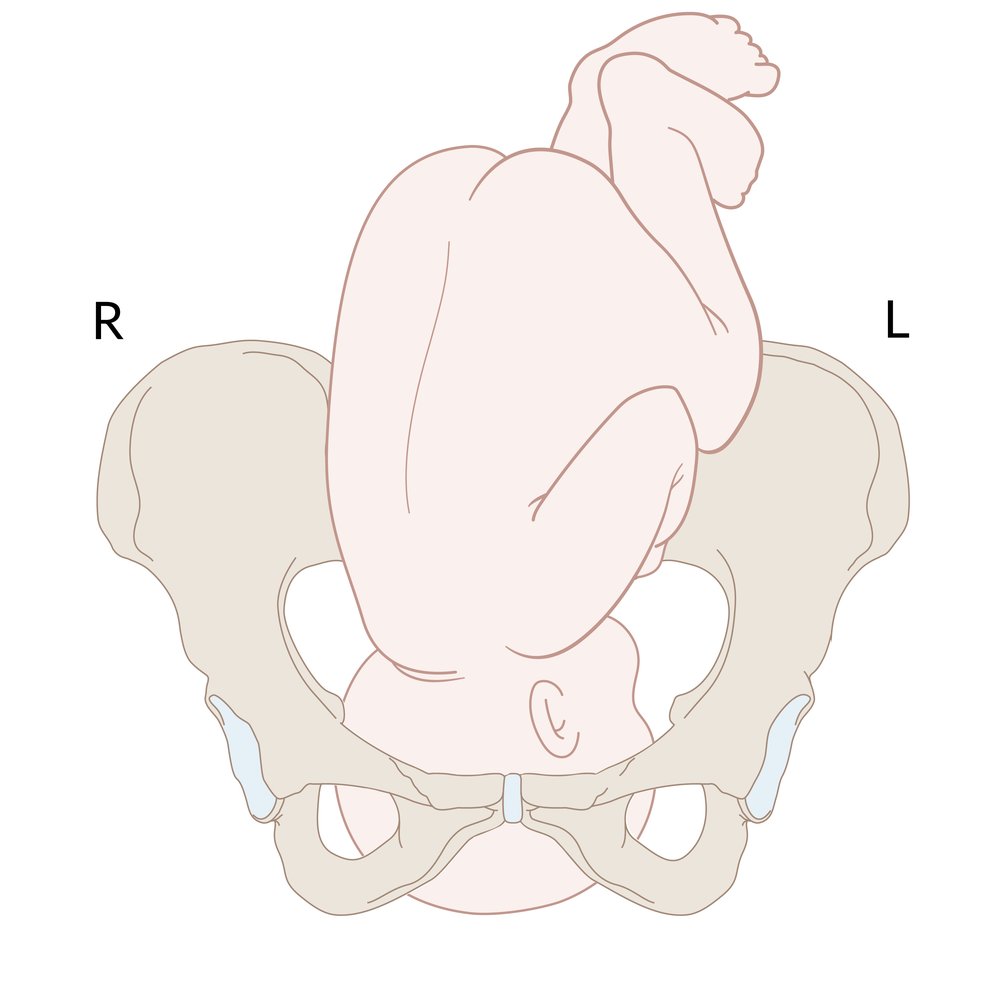
- Left occiput anterior (LOA): Fetal back faces the maternal left, anterior fontanelle faces the maternal right, sagittal suture lies in the right oblique diameter (most common position).
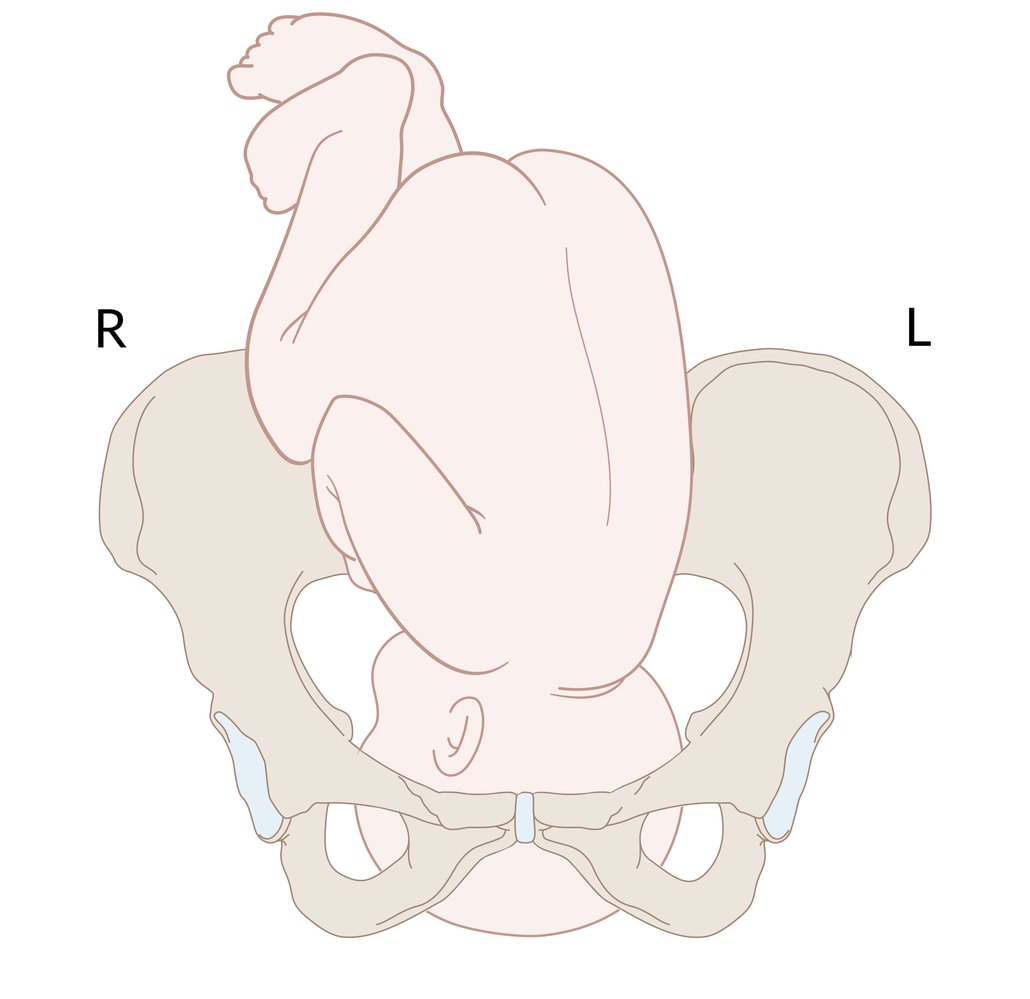
- Right occiput anterior (ROA): Fetal back faces the maternal right, anterior fontanelle faces the maternal left, sagittal suture lies in the left oblique diameter.
- Occiput posterior position: Fetal occiput points towards the maternal sacral promontory with face to pubis symphysis; the fetus faces upward
- Sacrum in breech presentation
- Mentum (chin) in extended cephalic (face) presentation
-
Occiput anterior position: Fetal occiput points towards maternal symphysis pubis; fetus faces downwards.







Fetal attitude [1]
- Definition: degree of extension/flexion of the fetal head during cephalic presentation
-
Types
- Vertex presentation (maximally flexed); most common attitude
- Brow presentation (partially extended)
-
Face presentation (maximally extended)
- Mentum anterior face presentation : Spontaneous vaginal delivery is possible .
- Mentum posterior face presentation
- Forehead presentation (partially flexed; military attitude): Spontaneous vaginal delivery is possible .
Station (Obstetrics) [2]
- Definition: measurement (in cm) of the presenting part above and below the maternal ischial spine
| Station | Description |
|---|---|
| 0 | The presenting part is at the level of the ischial spines |
| -1, -2, -3 | 1, 2, and 3 cm above the level of the ischial spines, respectively |
| +1, +2, +3 | 1, 2, and 3 cm below the level of the ischial spines, respectively |
-
Engagement (Obstetrics)
- When the widest transverse diameter of the head (presenting part) passes through the pelvic inlet
- Use the rule of fifths: engagement is clinically identified when ≤ 2/5 of the fetal head are felt above the symphysis pubis through the maternal abdomen

Synclitism
- Definition: parallelism between the pelvic plane and the plane of the fetal head
- In asynclitism, the sagittal suture is in the transverse diameter of the pelvic inlet and not between the symphysis pubis and sacral promontory.
-
Anterior asynclitism (Naegele obliquity)
- The sagittal suture is positioned towards the sacral promontory
- Spontaneous vaginal delivery possible
-
Posterior asynclitism (Litzmann obliquity)
- The sagittal suture is positioned towards the symphysis pubis
- Normal vaginal delivery is impossible. → premature cesarean delivery
-
Anterior asynclitism (Naegele obliquity)
")
")
© AMBOSS
The fetus is shown in the transverse lie, a malpresentation in which the fetal long axis is perpendicular to the uterine long axis.
© AMBOSS
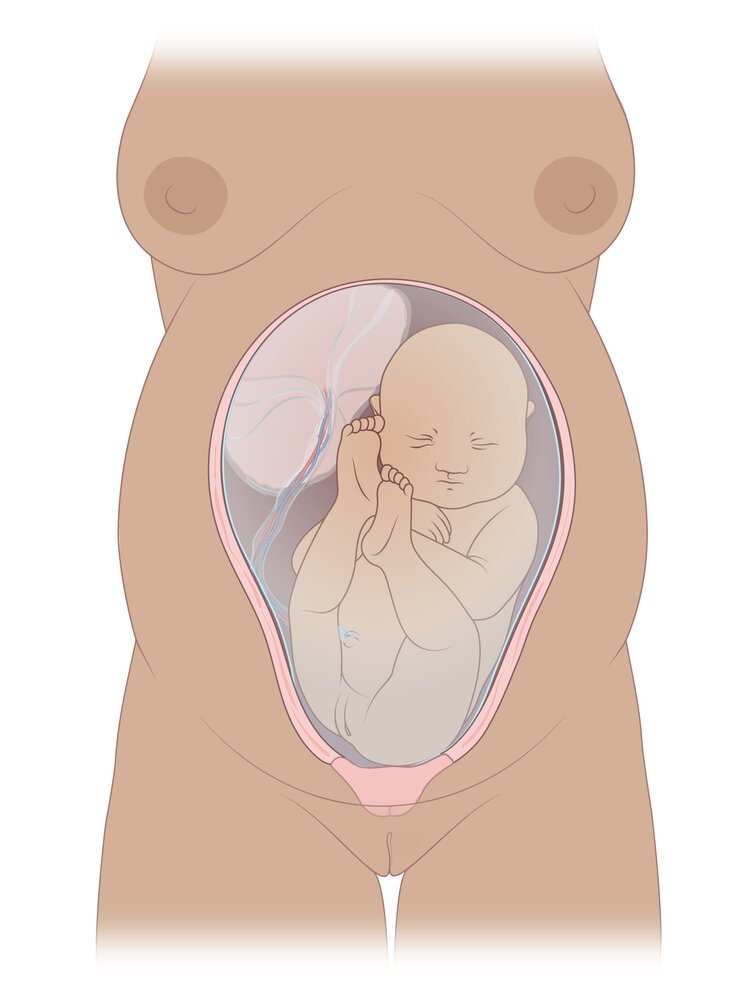
The fetus is shown in the cephalic presentation, in which the head lies closest to the cervix. Cephalic presentation can be further subdivided based on the position of the fetal occiput, in this case, anterior, and towards the mother's right side: right occiput anterior.
© AMBOSS
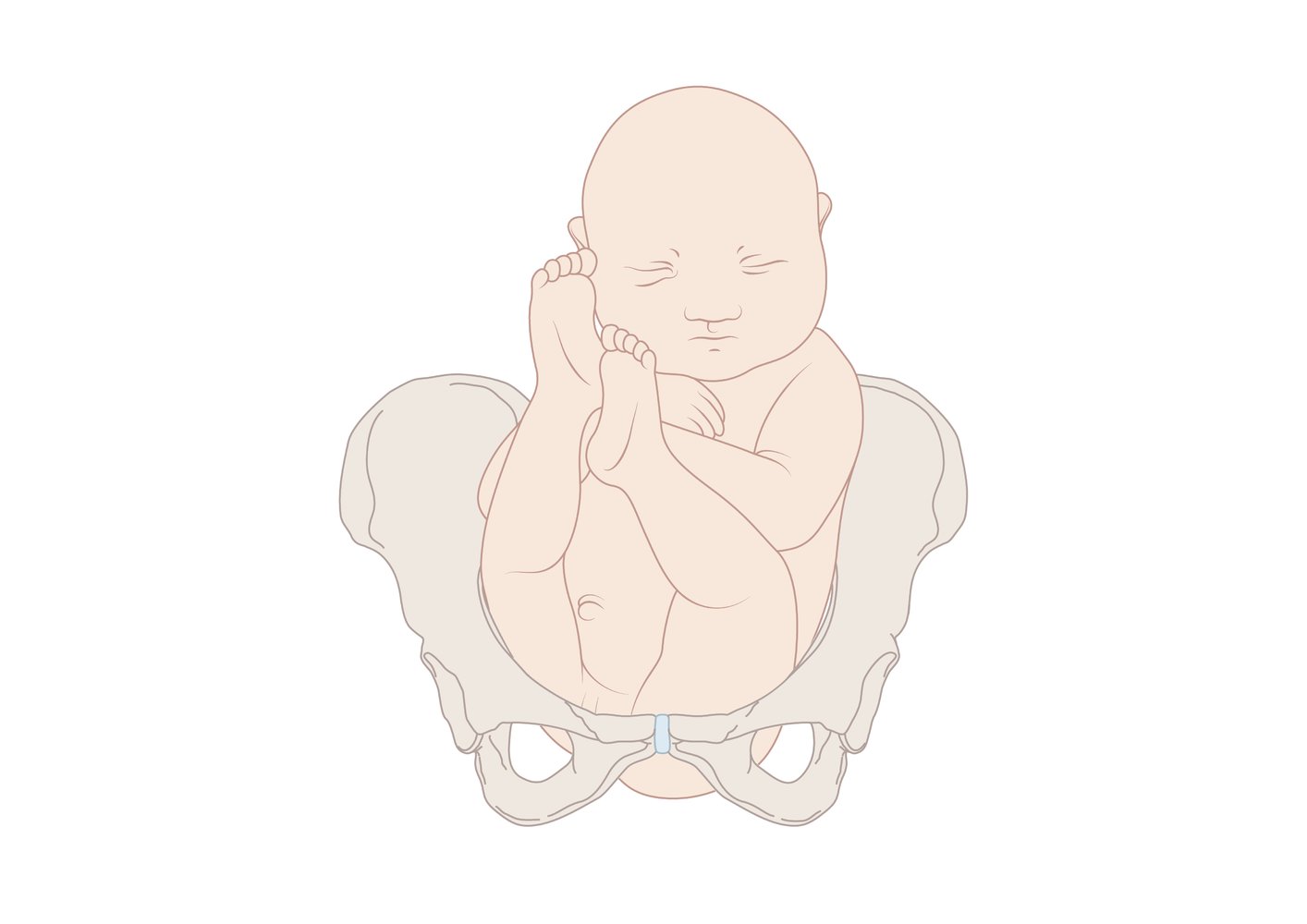
The fetus is shown in the cephalic presentation, in which the head lies closest to the cervix. Cephalic presentation can be further subdivided based on the position of the fetal occiput, in this case, anterior, and towards the mother's left side: left occiput anterior.
© AMBOSS
The fetus is shown in the breech presentation, in which the buttocks or feet lie closest to the cervix.
© AMBOSS
This malpresentation is characterized by flexed hips and extended knees. The buttocks of the baby are directed towards the birth canal.
© AMBOSS
Both hips and knees are flexed with the feet close to the buttocks.
© AMBOSS

Variant of breech presentation: one foot/leg is stretched to be delivered first.
© AMBOSS

Variant of breech presentation: both feet/legs are stretched to be delivered first.
© AMBOSS
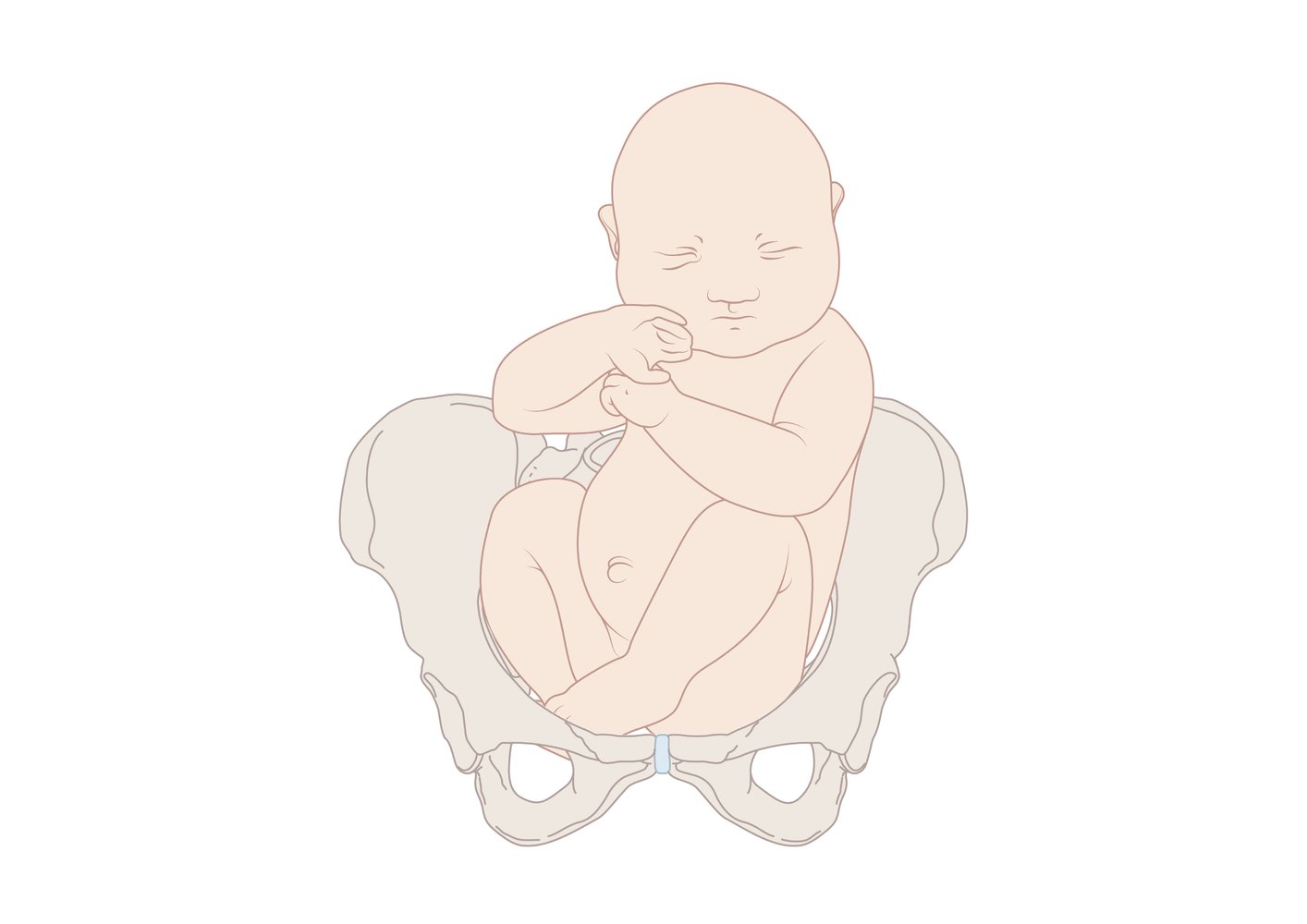
The occiput anterior fetal position is a cephalic presentation, in which the fetus is face down, facing the mother's spine. This is the ideal position for childbirth and, accordingly, the most common type of presentation. The fetus presents with a flexed neck, which extends during delivery. The shoulders then rotate before delivery is completed.
© AMBOSS
The occiput posterior position is a cephalic presentation, in which the fetus is face up, facing the mother's abdomen. This position of the head results in a larger presenting diameter, which often makes delivery more difficult. In order to complete delivery in this presentation, the fetal head must undergo maximal flexion. This is followed by extension of the head and shoulder rotation before delivery is completed.
© AMBOSS
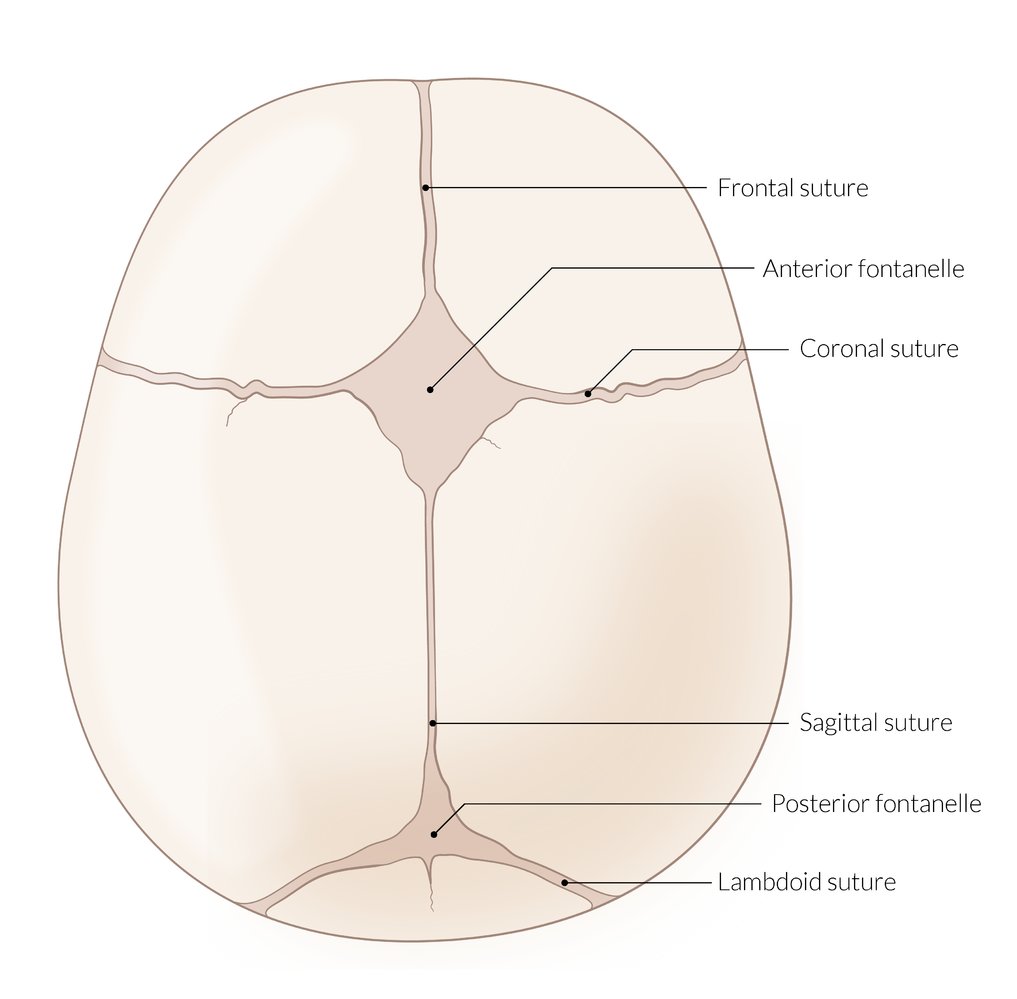
Skull of an infant (cranial view)
Anterior fontanelle: diamond-shaped structure located at the junction of the frontal, sagittal, and coronal sutures between the two frontal and two parietal bones. Normally closes between 12–18 months of age.
Posterior fontanelle: triangular-shaped structure located at the junction of the sagittal and lambdoid sutures between the occipital and two parietal bones. Normally closes between 2–3 months of age.
© AMBOSS
The child's back faces towards the mother's left.
© AMBOSS
The child's back faces towards the mother's right.
© AMBOSS
The occiput faces the symphysis. From the obstetrician's perspective with the mother in the supine position, the child faces the ground during birth.
© AMBOSS
The occiput faces the promontory. From the obstetrician's perspective with the mother in the supine position, the child faces the ceiling during birth.
© AMBOSS
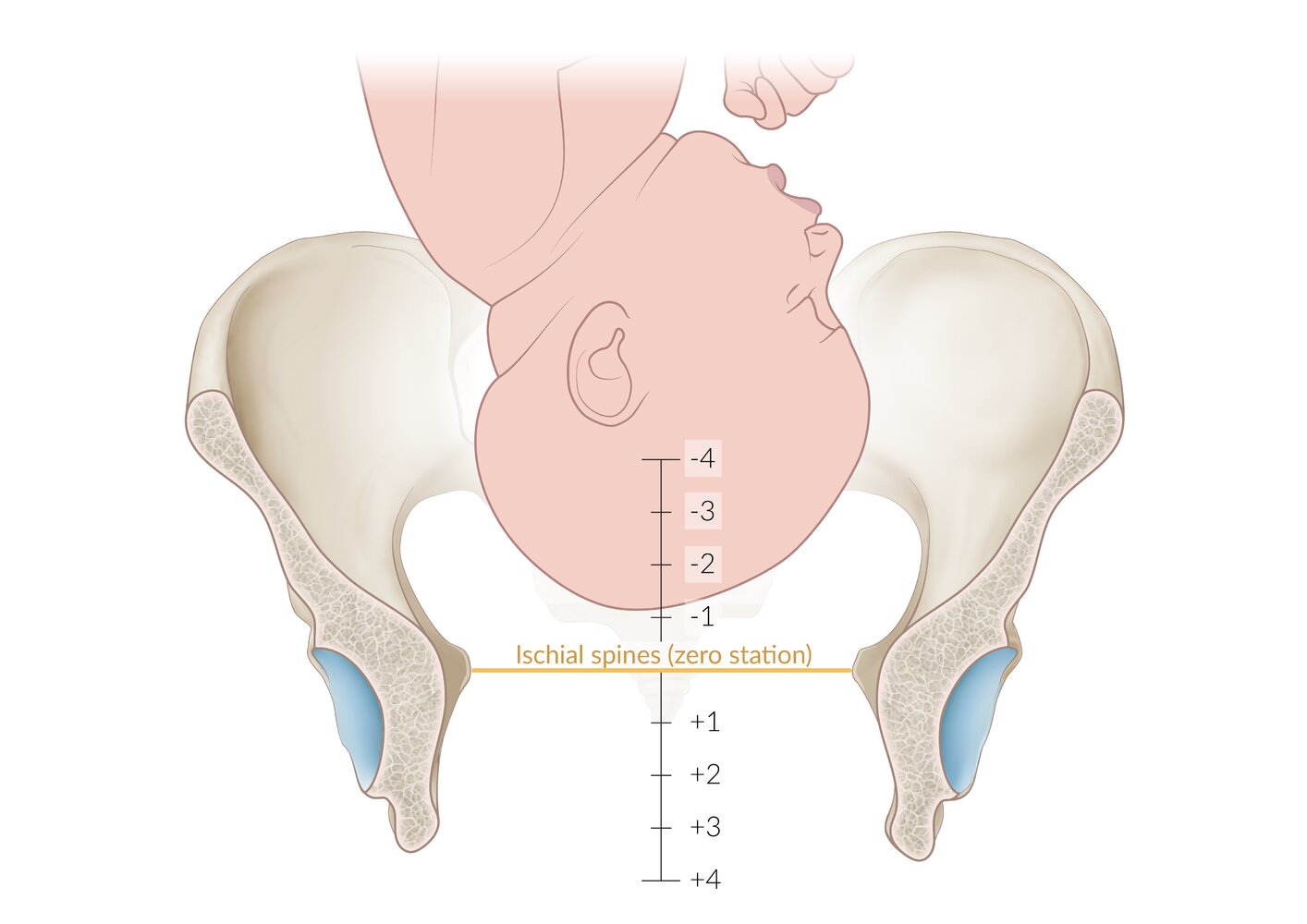
Illustration of a fetal head within the female pelvis
The scale shows the pelvic division according to de Lee in centimeter steps from –4 to +4, with the line connecting the ischial spines (interspinous plane; ISP) equating to the zero station. In this case, the presenting part is located slightly above ISP-1.
© AMBOSS
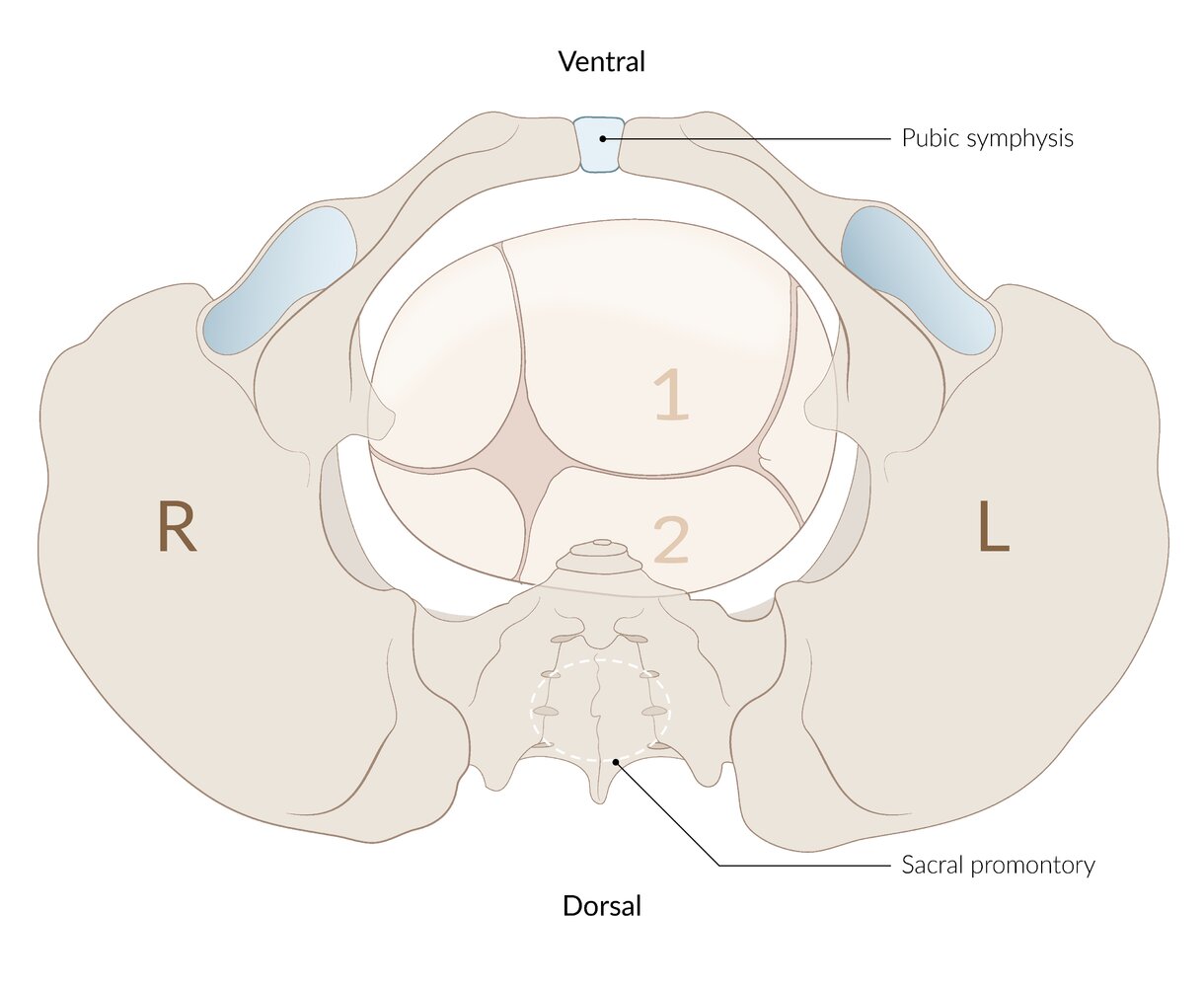
From the obstetrician's perspective with the mother in the supine position, the sagittal suture is inclined towards the promontory so that the anterior parietal bone (1) presents first. (2 = posterior parietal bone)
© AMBOSS
From the obstetrician's perspective with the mother in the supine position, the sagittal suture is inclined towards the symphysis so that the posterior parietal bone (2) presents first (1 = anterior parietal bone).
© AMBOSS
Normal spontaneous labor
Obstetric contractions (uterine muscle contractions) [3][4]
| Overview of obstetric contractions [1][5] | |||
|---|---|---|---|
| Time | Characteristics | ||
| Uterine contractions during pregnancy | Alvarez-waves |
|
|
| Braxton Hicks contractions (false labor) |
|
|
|
| Prelabor |
|
|
|
| Labor | Stage 1: cervical dilation and effacement |
|
|
| Stage 2: fetal expulsion |
|
|
|
| Stage 3: placental expulsion or afterbirth |
|
|
|
| Afterpains |
|
|
|
False labor only requires reassurance.
Rupture of membranes (ROM)
- Definition: the rupture of the amniotic sac followed by the release of amniotic fluid
- Spontaneous rupture of membranes: : ROM that usually occurs at the onset of labor and is unprovoked by health practitioners
- Artificial rupture of membranes (amniotomy): A procedure in which the amniotic sac is ruptured in order to release amniotic fluid.
- Delayed rupture of membranes: ROM that occurs during fetal expulsion, after cervical dilation and effacement
-
Abnormal rupture of membranes
- Premature rupture of membranes (PROM)
- Preterm premature rupture of membranes (PPROM)
- Prolonged rupture of membranes
- Clinical features: sudden “gush” of pale yellow or clear fluid from the vagina (may also be a constant leaking sensation)
-
Diagnostics
- Consider sterile speculum examination if the diagnosis is uncertain.
- Suggestive findings include pooling, positive litmus test or nitrazine test, and ferning.
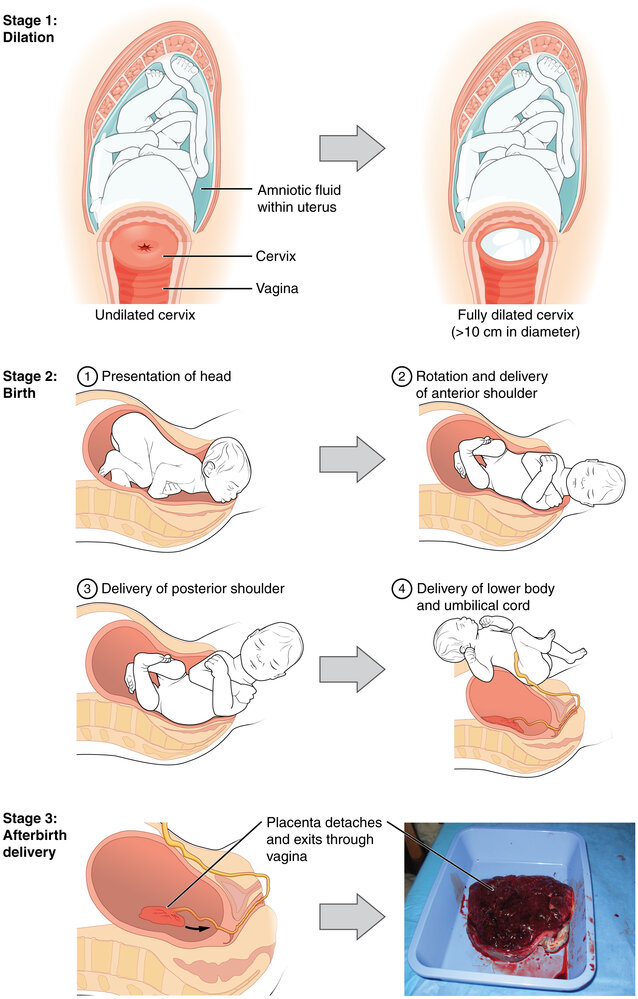
Stages of labor [3][4][6]
| Overview of the stages of labor | |||||
|---|---|---|---|---|---|
| Stage | Characteristics | Duration | Clinical features | ||
| Nulliparous patients | Multiparous patients | ||||
| First stage of labor | Latent phase of labor |
|
|
|
|
| Active phase of labor |
|
|
|
||
| Second stage of labor |
|
|
|
|
|
| Third stage of labor |
|
|
|
||
| Fourth stage of labor |
|
|
|
||
Management of labor by stage
-
First stage of labor
- Analgesia upon request
- Fetal heart rate monitoring
-
Determine fetal position via abdominal (see Leopold maneuvers) and pelvic (palpation of fetal sutures/fontanelles) examination.
- If the fetal position cannot be determined by examination, perform ultrasound.
- Regular assessment of cervical dilation and descent of the fetal head
- In case of heavier bleeding but normal maternal vital signs and fetal heart tracing (e.g., increased bloody show), delivery should proceed as planned with frequent observation.
-
Second stage of labor
- Help the mother to find comfortable and safe positions.
- Guide the delivery of the fetus through the vaginal canal (See “Mechanics of childbirth” for expected fetal movements).
- Clamp the umbilical cord after no less than 30–60 seconds. [10]
- See “Delivery of the infant” in “Manually assisted vaginal delivery” for detailed instructions.
-
Third stage of labor
-
Active management of the third stage of labor (reduces the risk of postpartum hemorrhage)
- Oxytocin reduces blood loss by inducing stronger uterine contractions.
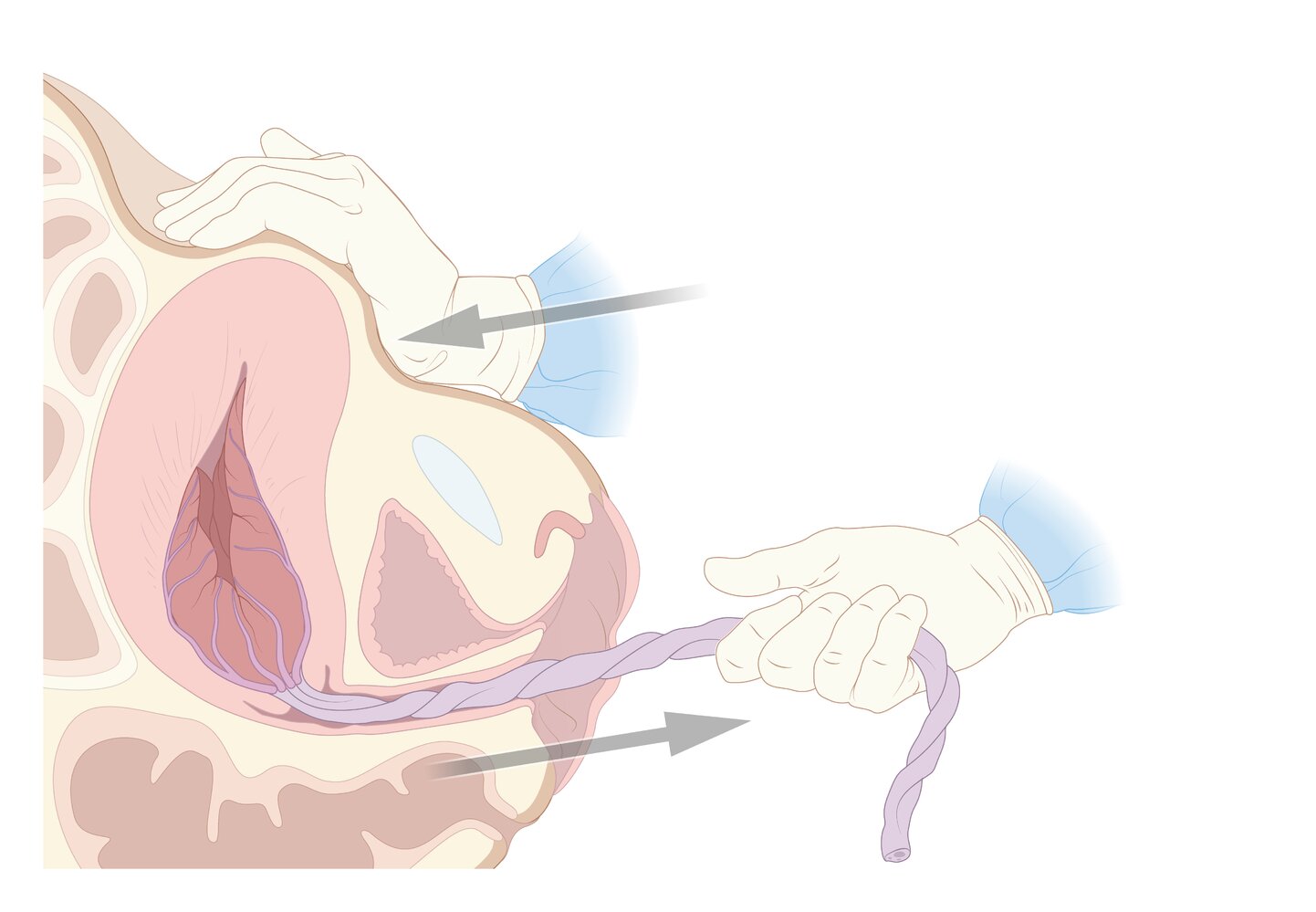
- Controlled cord traction (Brandt-Andrews maneuver) if placenta is not delivered spontaneously
- See “Delivery of the placenta” in “Manually assisted vaginal delivery” for detailed instructions.
- Examine the placenta to confirm completeness (regular surface with complete cotyledons), which should also consist of the umbilical cord, complete amniotic membranes, and three blood vessels (one vein, two arteries).
- Repair any obstetric lacerations.
-
Active management of the third stage of labor (reduces the risk of postpartum hemorrhage)
- Fourth stage of labor: Monitoring to rule out postpartum hemorrhage or preeclampsia

")
")
Normal mechanics of childbirth [1]
Adaptation to the different forms of the pelvic region requires a great deal of rotation.
-
Engagement, descent, and increased flexion (occur simultaneously)
- The head engages below the plane of the pelvic inlet.
- The presenting part begins to descend into the birth canal.
- The chin of the fetus moves towards its chest.
- Internal rotation: The fetal head rotates by 90° (two 45° steps) in the midpelvis, from a transverse to anterior-posterior position.
- Extension: The fetal head, lying behind the symphysis pubis bone and the pelvic floor, acts upwards and forwards.
- Restitution: The fetal head rotates 45° in the opposite direction as it passes through the pelvic outlet.
- External rotation: The anterior shoulder rotates 45° anteriorly as it meets the maternal pelvic floor. This action is transmitted to the head which also rotates 45°, placing the head in its original transverse position.
- Expulsion: Delivery of the head, anterior shoulder followed by the posterior shoulder, and the body




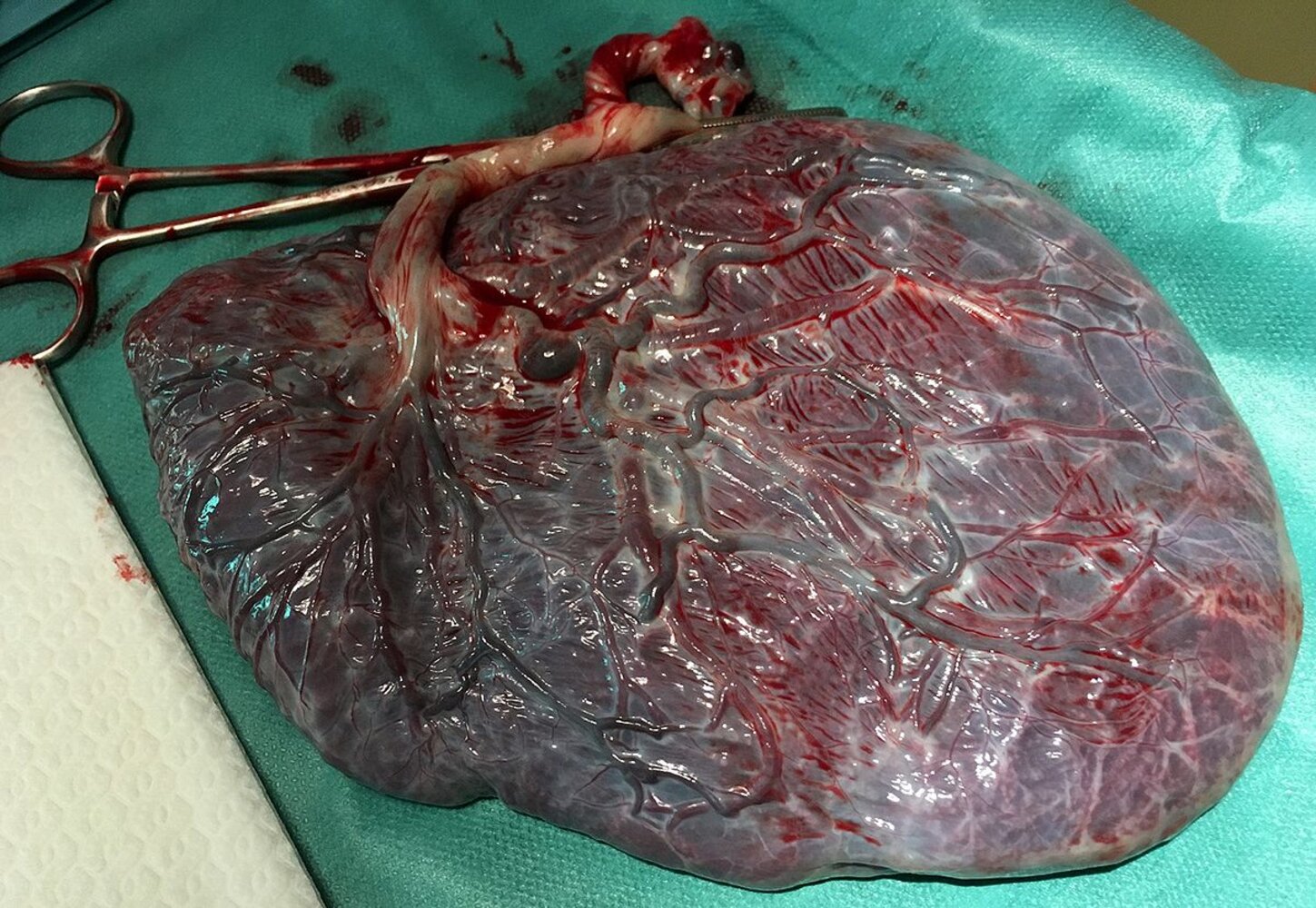
Photograph of the fetal side (chorionic plate) of a placenta immediately after delivery
Size and shape of the placenta are unremarkable. The umbilical vessels are visible on the organ's surface, covered by the amnion. The clamped umbilical cord can be seen to the upper left of the image. It typically attaches centrally to the chorionic plate (from the image it appears that the placenta is not fully spread out, but it cannot be ruled out that it attaches off-center here).
Source: “Placenta human newborn” by Eolic, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}
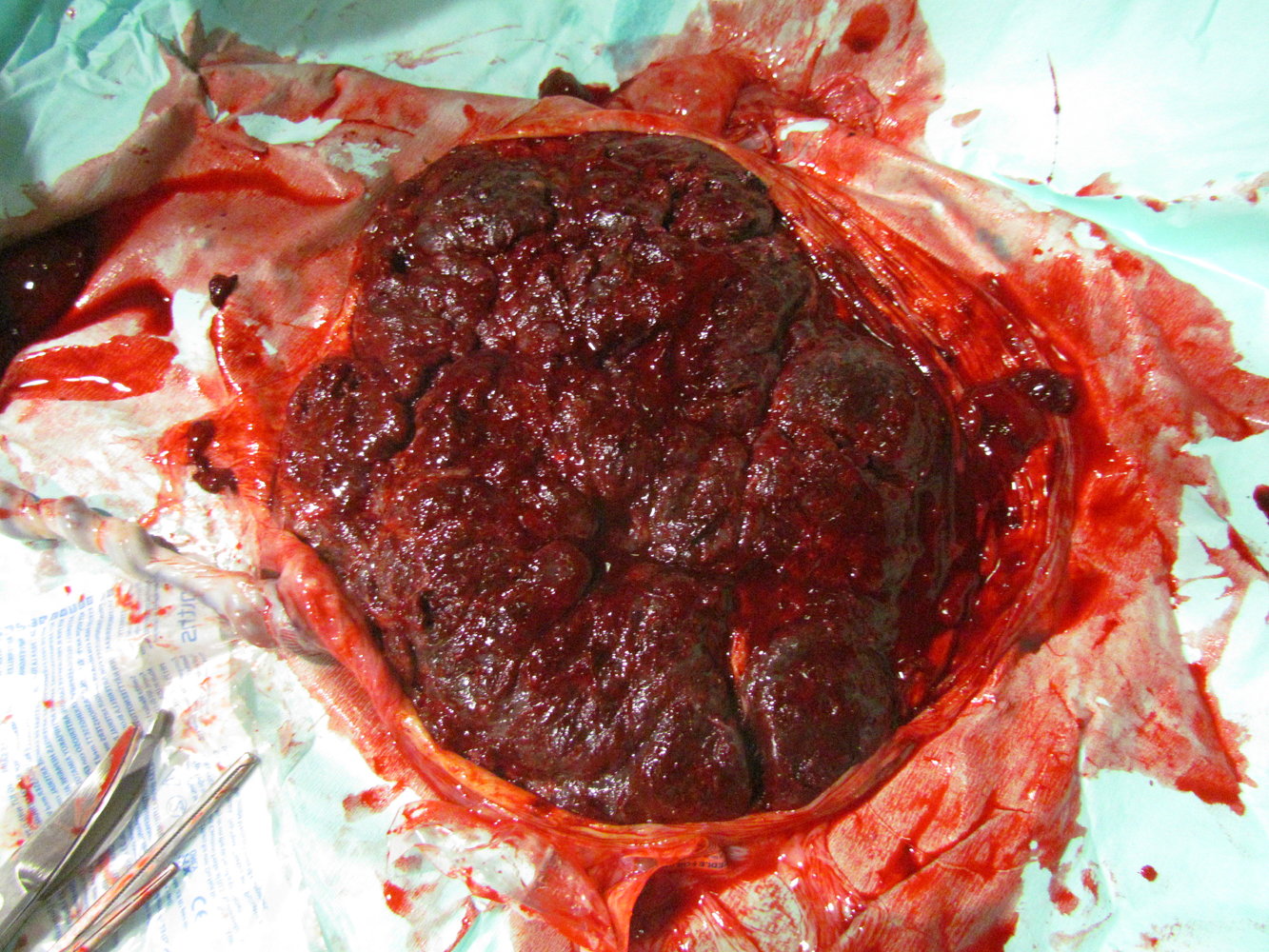
Photograph of the maternal side (basal plate) of a placenta immediately after delivery
Folds of amnion are visible at the margins of the placenta. The basal plate itself is divided into 15–30 macroscopically distinct areas (cotyledons) by the placental septa. After delivery, placental completeness should be confirmed by checking that all cotyledons are present (to exclude retained placental tissue).
Source: “Human placenta 01” by תמרה דהן - דולה, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
Source: “2920 Stages of Childbirth-02” by OpenStax College, Wikimedia Commons, licensed under CC BY 4.0.
{kind=link}
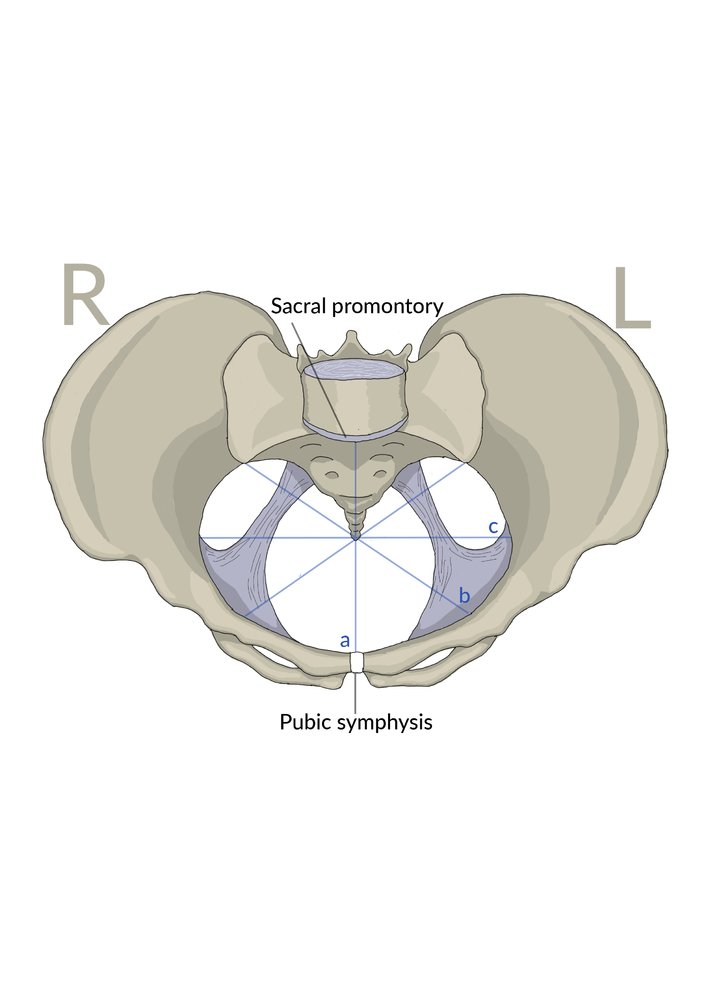
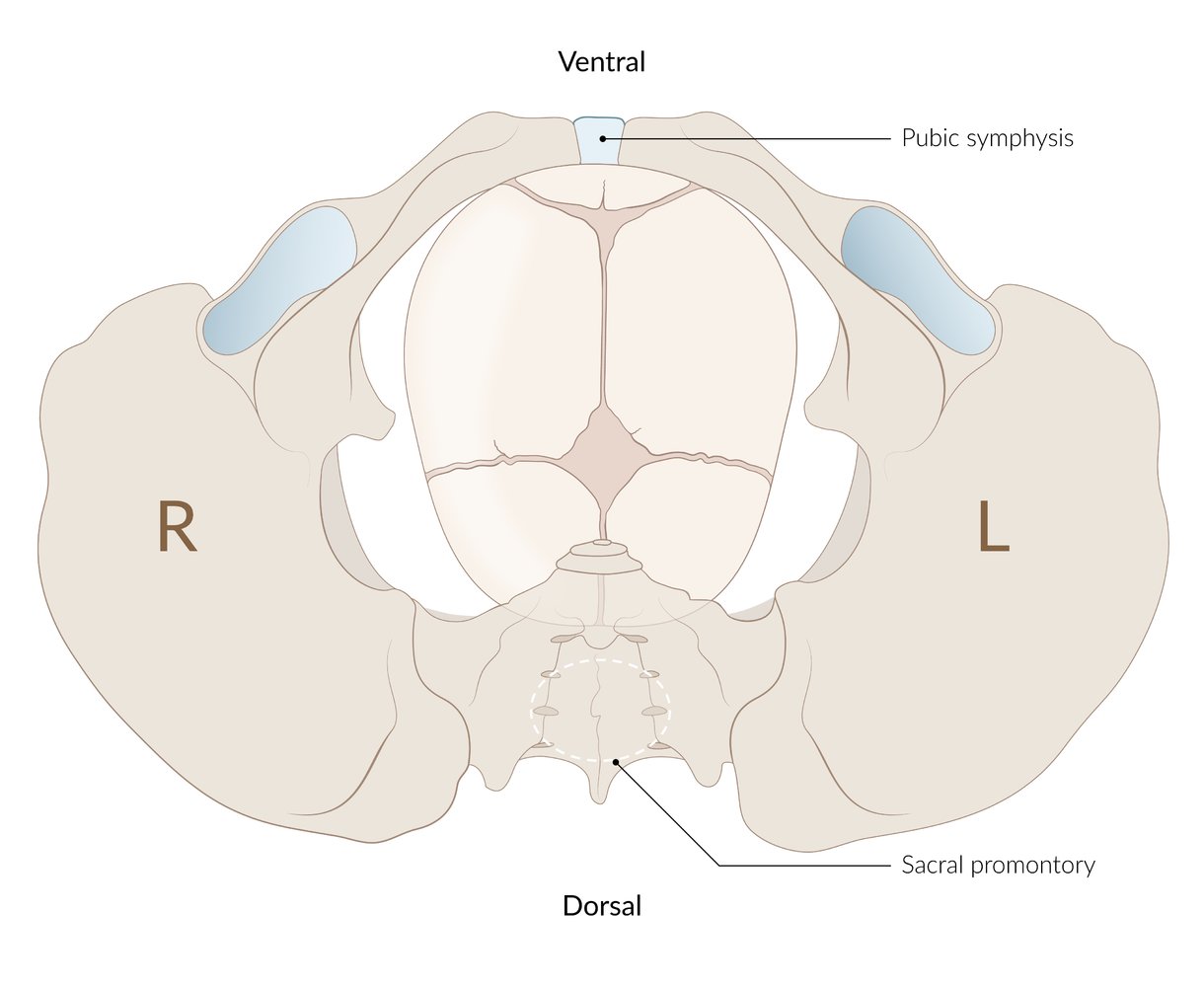
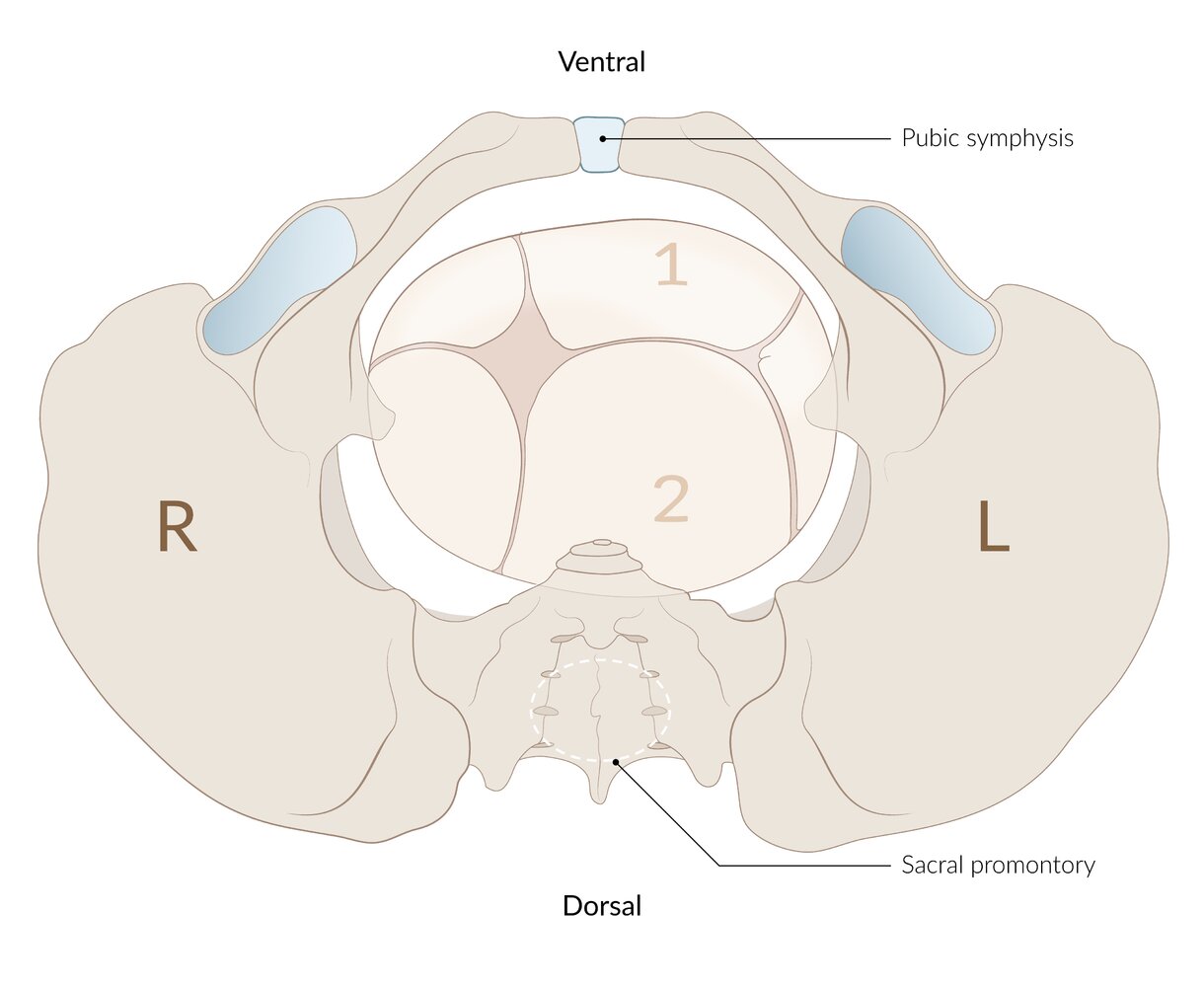
The plane of the pelvic inlet has an oval shape that is widest at the transverse diameter (C; ∅ 13 cm). The plane of the pelvic outlet is delimited by the sacrotuberous ligaments and has an oval shape that is rotated by 90° in relation to the plane of the pelvic inlet. This requires a 90° rotation of, first, the head and then the shoulders during birth. (A = true conjugate, ∅ 11 cm; B = oblique diameter, ∅ 12 cm)
© AMBOSS
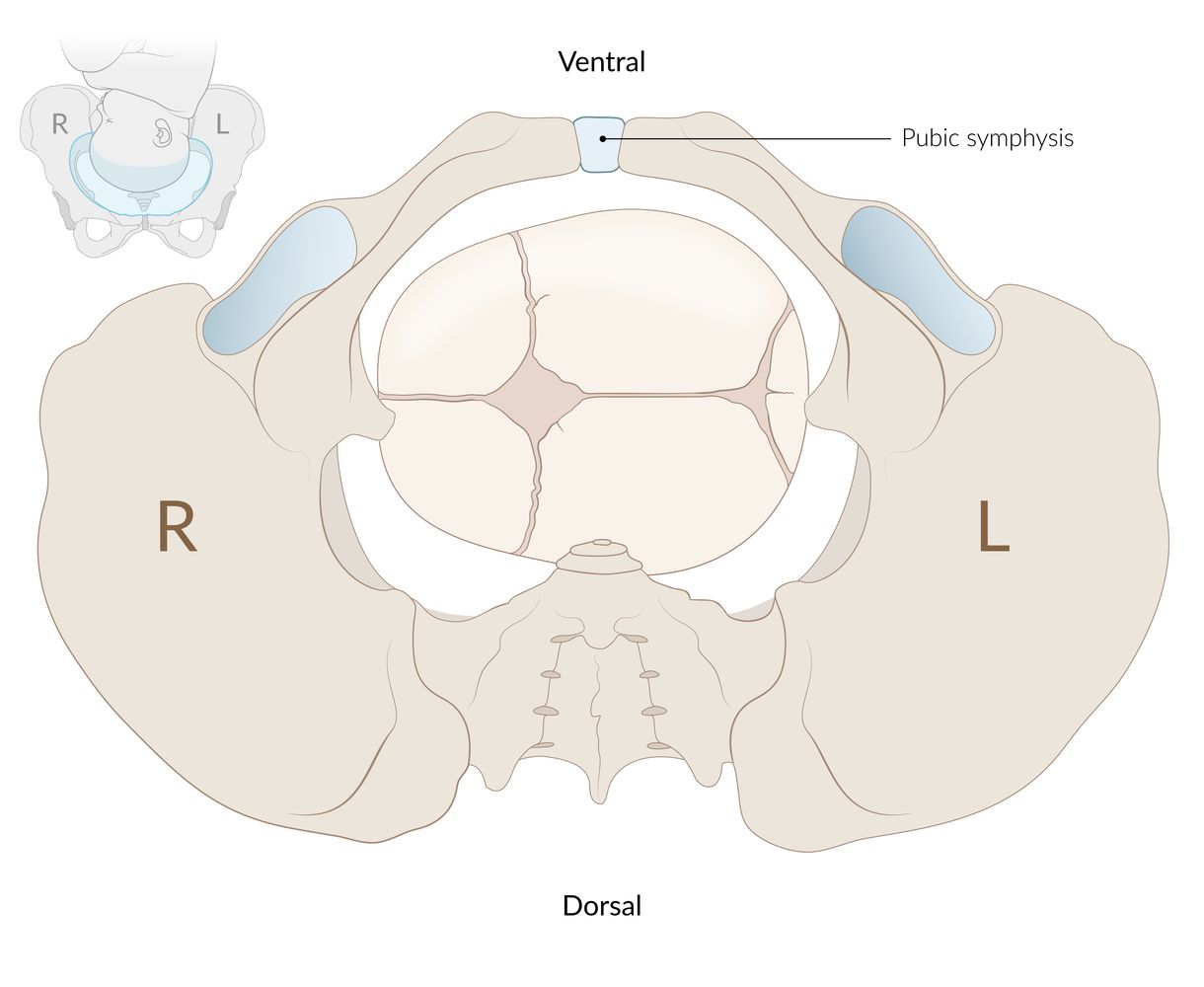
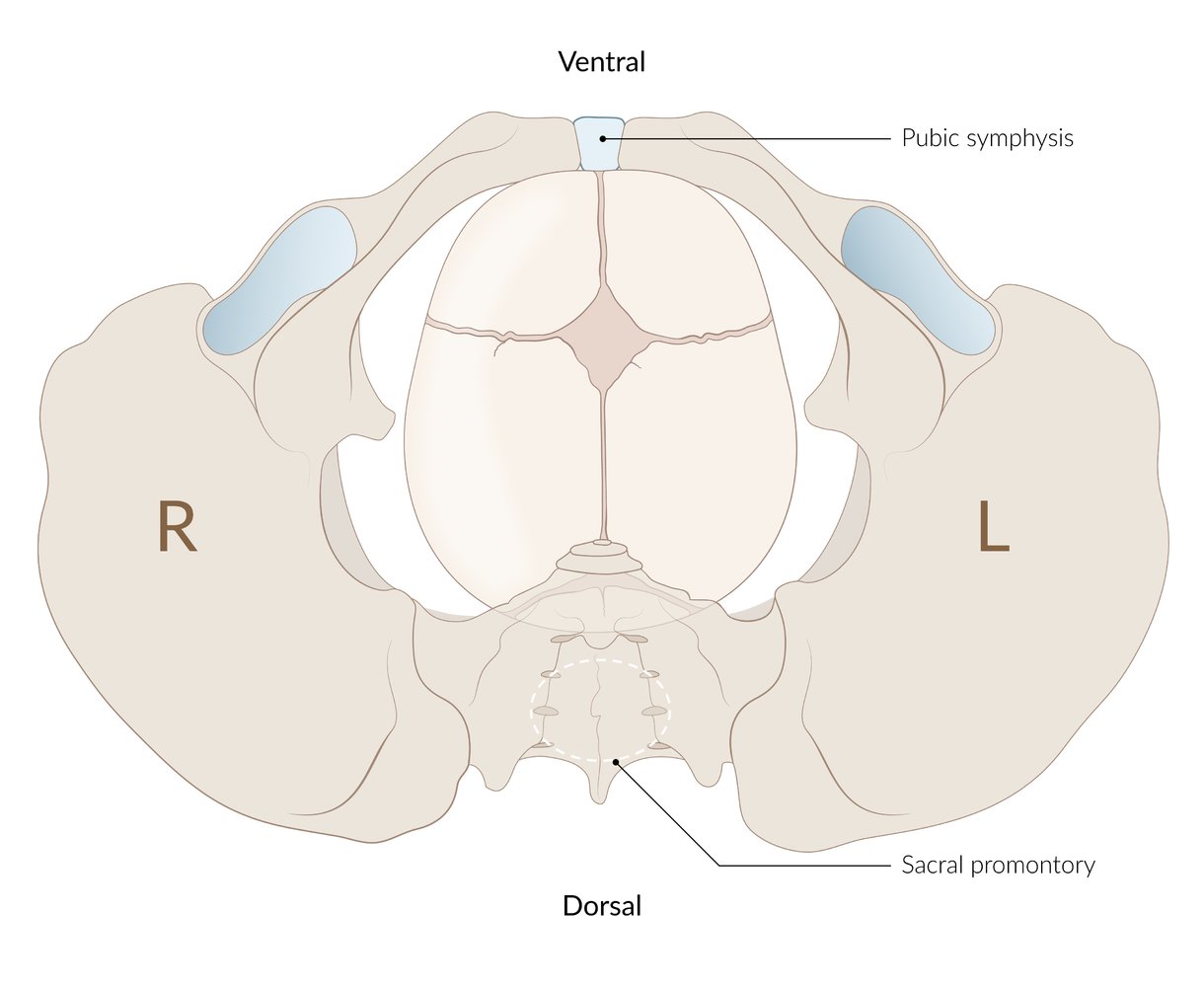
During normal vaginal births, the sagittal suture of the fetal head (arrow) lies transverse to the plane of the pelvic inlet, thus enabling passage through the plane.
© AMBOSS
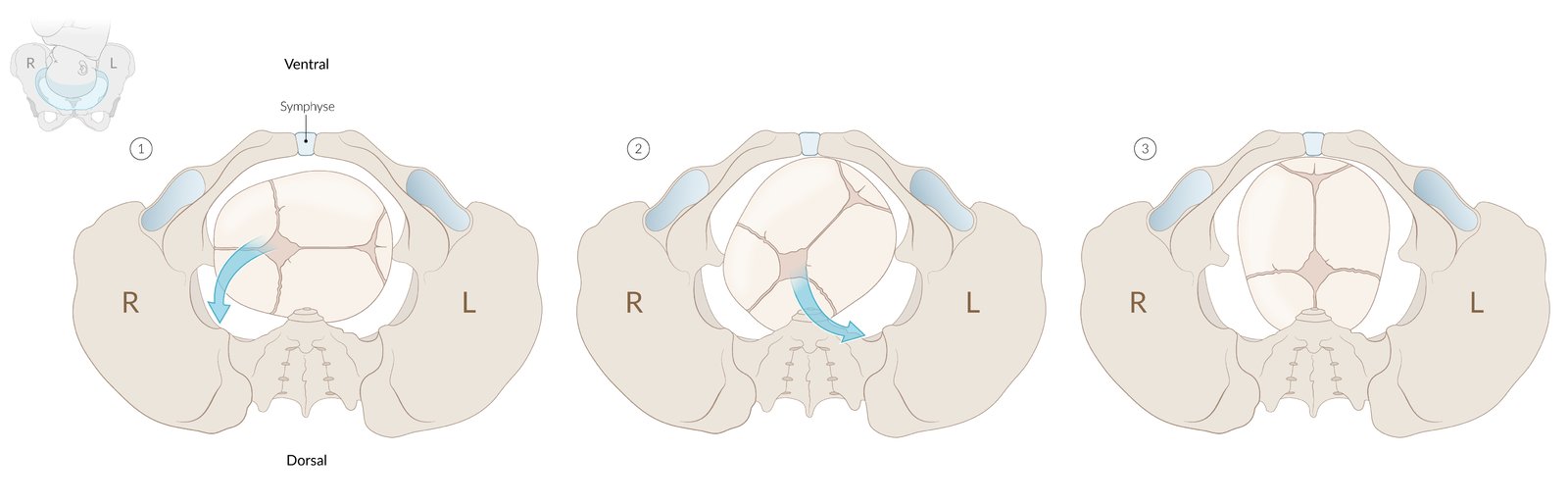
From the obstetrician's perspective: (1) Plane of the pelvic inlet: left occiput transverse position; 45° counterclockwise rotation. (2) Sagittal suture lies in the left oblique diameter; 45° counterclockwise rotation. (3) Plane of the pelvic outlet: occiput anterior position.
© AMBOSS
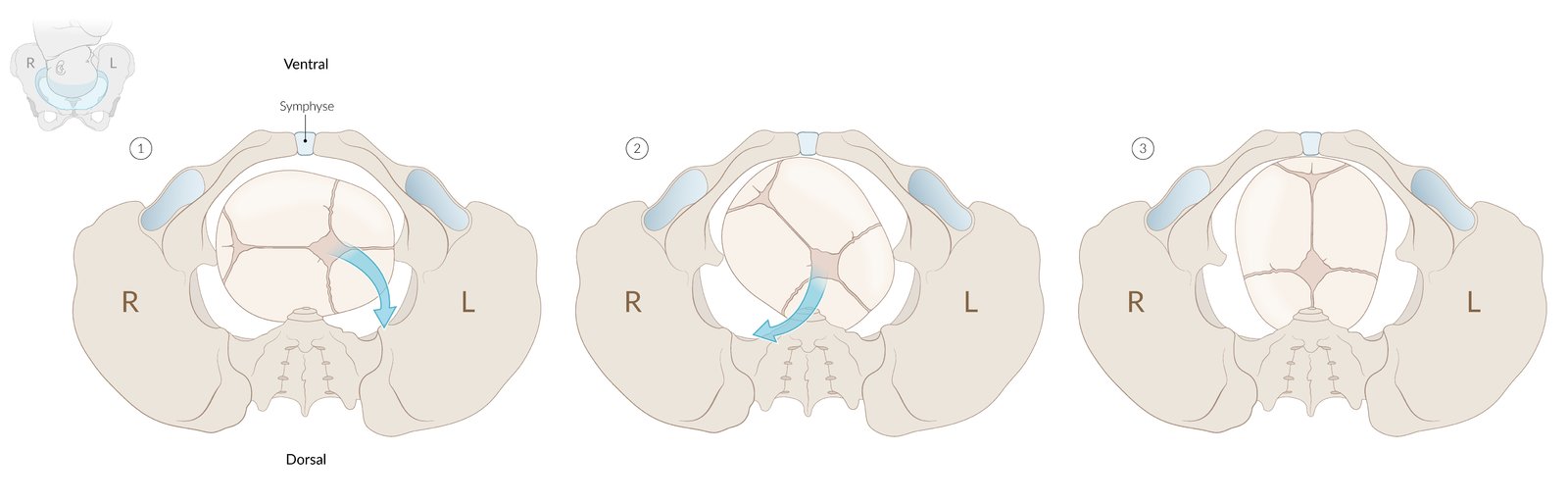
From the obstetrician's perspective: (1) Plane of the pelvic inlet: right occiput transverse position; 45° clockwise rotation. (2) Sagittal suture lies in the right oblique diameter; 45° clockwise rotation. (3) Plane of the pelvic outlet: occiput anterior position.
© AMBOSS
Manually assisted vaginal delivery
The following describes the uncomplicated delivery of an infant in the occiput anterior position, the most common fetal presentation. Begin active management of labor as soon as crowning occurs. [11][12][13]

Preparation
- Help the mother into the most comfortable position. [14]
- Cleanse the vulvar and perineal area.
- Don PPE.
Delivery of the infant
Delivery of the head
- Support the perineum with a warm compress. [15]
- Once the vaginal introitus is distended ≥ 5 cm, apply gentle pressure to the fetal occiput with one hand.
- Lift the fetal chin by applying upward pressure through the perineum with the other hand.
- Support the head during passage through the vaginal introitus.
- Check for a nuchal umbilical cord and, if present, slip it over the fetal head.
Delivery of the shoulders
- Assist delivery of the shoulders, if not delivered spontaneously.
- Hold the fetal head with both hands and apply gentle downward traction.
- Once the anterior shoulder appears below the symphysis pubis, apply gentle upward traction until the posterior shoulder is free.
Delivery of the body and immediate care of the newborn
- Apply gentle long-axis traction, if necessary, without placing fingers under the axillae.
- Once delivered, wipe the face and mouth to clear the airway. [11][12][16]
- Quickly dry the infant to prevent hypothermia and stimulate crying. [15]
- If necessary, initiate neonatal resuscitation.
- Initiate skin-to-skin contact, e.g., by placing the infant on the mother's abdomen.
Clamping the umbilical cord
- Delay clamping by at least 30–60 seconds after delivery (unless immediate neonatal resuscitation is required). [10][15]
- Place two Kelly clamps 6–8 cm from the abdominal insertion and cut the cord between them.

Delivery of the placenta
- Palpate the uterine fundus and monitor for signs of placental separation.
- Once placental separation occurs, ask the patient to bear down to expel the placenta.
- If the placenta is not expelled with maternal effort, apply controlled umbilical cord traction.
- Administer oxytocin to prevent postpartum hemorrhage. [13][17][18]
Never apply forceful traction to the umbilical cord, as this may result in uterine inversion or separation of the cord from the placenta. [12]

Immediate postpartum care [11]
- Monitor for postpartum hemorrhage and eclampsia.
- Palpate the fundus regularly to assess uterine tone.
- Check maternal blood pressure and pulse every 15 minutes for the first two hours after birth.
- Assess the placenta, membranes, and umbilical cord for completeness and anomalies.
- Inspect for and repair perineal lacerations.
- See also “Postpartum care,” “The newborn infant,” and “Infant nutrition and breastfeeding” as needed.
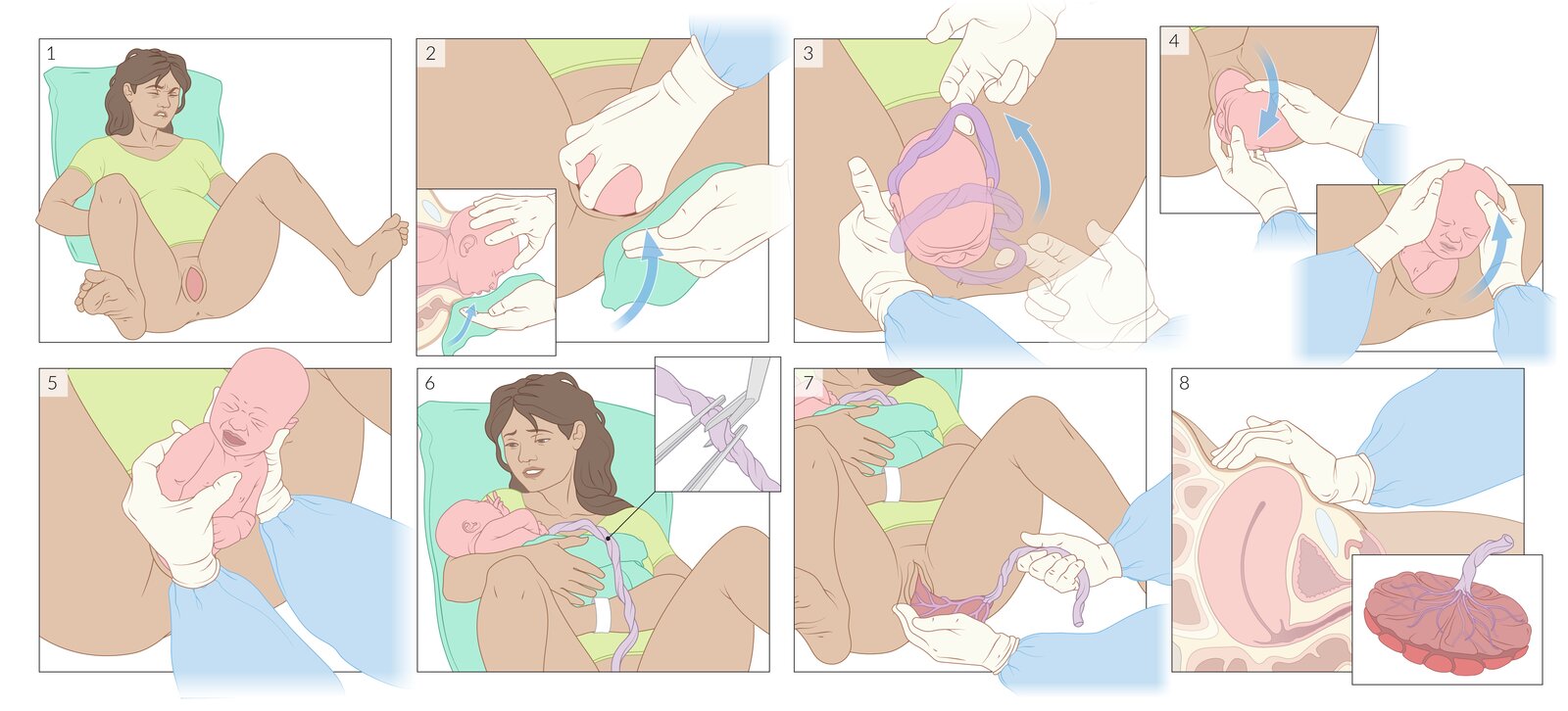
1. Once crowning occurs, the mother is helped into a comfortable position and the vulvar and perineal area are cleansed (not shown).
2. Gentle pressure on the fetal head is applied with one hand to control the rate of expulsion. The fetal chin is lifted with the other hand by applying upward pressure through the perineum.
3. If a nuchal cord is present, it is gently slipped over the fetal head.
4. Gentle downward traction is applied on the fetal head until the anterior shoulder is free, then gentle upward traction until the posterior shoulder is free.
5. The fetal body is supported with both hands and a gentle longitudinal traction is applied if necessary. The fingers should not be placed in the fetal axillae.
6. The infant is placed on the mother's abdomen and gently dried with a towel. After waiting at least 30–60 seconds, the umbilical cord is cut between two Kelly clamps placed 6–8 cm from the abdominal insertion.
7. Once signs of uterine separation have occurred, the mother is asked to bear down to expel the placenta.
8. In the immediate postpartum period, uterine tone should be assessed regularly. The placenta, membranes, and umbilical cord should be evaluated for completeness and anomalies.
© AMBOSS

Source: “Untitled - panoramio - Pedro Martha (19)” by Pedro Martha, Wikimedia Commons, licensed under CC BY 3.0. Modifications: image cropped.
.jpg){kind=link}
© AMBOSS
Photograph of the fetal side (chorionic plate) of a placenta immediately after delivery
Size and shape of the placenta are unremarkable. The umbilical vessels are visible on the organ's surface, covered by the amnion. The clamped umbilical cord can be seen to the upper left of the image. It typically attaches centrally to the chorionic plate (from the image it appears that the placenta is not fully spread out, but it cannot be ruled out that it attaches off-center here).
Source: “Placenta human newborn” by Eolic, Wikimedia Commons, licensed under CC BY-SA 4.0.
Photograph of the maternal side (basal plate) of a placenta immediately after delivery
Folds of amnion are visible at the margins of the placenta. The basal plate itself is divided into 15–30 macroscopically distinct areas (cotyledons) by the placental septa. After delivery, placental completeness should be confirmed by checking that all cotyledons are present (to exclude retained placental tissue).
Source: “Human placenta 01” by תמרה דהן - דולה, Wikimedia Commons, licensed under CC BY-SA 3.0.
Intrapartum fetal monitoring
Electronic fetal heart rate monitoring [19][20]
- Description: widely used diagnostic tool during 3rd trimester and labor to detect signs of fetal distress
-
Procedure
- Determination of the fetal heart rate (FHR), presence of acceleration or deceleration by Doppler ultrasound, recording beats per minute (bpm) in the upper curve (cardiogram)
-
During birth, the FHR may be monitored internally via an electrode that is attached to the fetal head (fetal scalp electrode monitoring).
- Rupture of the membranes must have occurred or an amniotomy performed
- Used when external monitoring is difficult (e.g., maternal obesity, polyhydramnios, multiple gestations)
- Mechanoelectrical measurement of uterine contractions via a pressure transducer, recording in the lower curve in kPa (tocodynagraph)
-
Indications
- During labor
- Admission in the labor ward
- In every case of complication during pregnancy or delivery, such as impending preterm birth, abnormalities of the fetal heart, multiple pregnancy, suspected placental insufficiency, uterine bleeding, tocolysis
Fetal heart rate [21][22][23]
- In CTG, the FHR is designated as the baseline or basal heart rate and is normally 110–160 bpm.
-
Tachycardia
- Mild tachycardia: FHR of 160–180 bpm for > 10 minutes
- Severe tachycardia: FHR of ≥180 bpm for > 10 minutes
- Causes: stress, hypotension, maternal fever; , medication (e.g., betamimetics for the treatment of tocolysis), chorioamnionitis, fetal arrhythmias, fetal anemia, hypoxia
-
Bradycardia
- Mild bradycardia: FHR of < 110 bpm for > 3 minutes
- Severe bradycardia: FHR of < 100 bpm for > 3 minutes
- Causes: supine hypotensive syndrome, fetal heart defects; , central nervous system anomalies, severe hypoxia
- Methods to assess FHR: Nonstress test (NST) and contraction stress test (CST); are performed during the third trimester of pregnancy to measure FHR reactivity to fetal movements and FHR reactivity in response to uterine contractions respectively. See nonstress test and contraction stress test in “Prenatal care” for details.



Fetal heart rate (FHR) tracing
| Fetal heart rate tracing categories | |||
|---|---|---|---|
| Category I FHR tracing | Category II FHR tracing | Category III FHR tracing | |
| Characteristics |
|
|
|
| Interpretation |
|
|
|
| Management |
|
|
|
Fetal heart rate variability [24]
On CTG, variability of FHR is represented by the oscillation of the FHR around the baseline and is determined by measuring the amplitude between the highest and lowest turning point of the FHR curve.
| Overview of fetal heart rate variability | ||
|---|---|---|
| Type | Oscillation amplitude | Causes |
| Moderate variability |
|
|
| Absent variability |
|
|
| Minimal variability |
|
|
| Marked variability |
|
|
| Sinusoidal variability |
|
|
| Pseudosinosoidal variability |
|
|
 showing different types of FHR baseline variability")
 with normal findings")


Acceleration (CTG) [23]
- Description: a normal temporal increase in the FHR from the baseline by > 15 bpm for more than 15 seconds but less than 10 minutes if the gestational age is > 32 weeks, or by > 10 bpm for more than 10 seconds if the gestational age is < 32 weeks
-
Interpretation
- The presence of > 2 accelerations within a span of 20 minutes indicates a reactive fetal heart rate tracing.
- If the acceleration lasts longer than 10 minutes, it should be considered a baseline change in the fetal heart rate.
Decelerations (CTG) [19][25][26][27][28]
- Description: a temporary decline in the FHR of > 15 bpm for a maximum duration of 3 minutes
| Overview of types of fetal deceleration | |||
|---|---|---|---|
| Type | Etiology | Characteristics | Measures |
| Early deceleration |
|
|
|
| Late deceleration |
|
|
|
| Variable deceleration |
|
|
|
| Prolonged deceleration |
|
|
|
Consider umbilical cord compression or umbilical cord prolapse in patients with recurrent variable decelerations (≥ 50% of contractions).
| MNEMONIC for etiology of fetal HR alterations: VEAL CHOP | |
|---|---|
| Variable decelerations | → Cord compression/prolapse |
| Early decelerations | → Head compression |
| Accelerations | → OK |
| Late decelerations | → Placental insufficiency/Problem |
 showing early decelerations")
 showing late decelerations")
 showing intermittent variable decelerations")
 showing recurrent variable decelerations")
 variability")

Interpretation
-
Nonreassuring fetal status
-
Characteristic changes in the fetal heart rate (FHR) in response to fetal hypoxia and metabolic acidosis
- Fetal tachycardia (FHR > 160–180/min)
- Fetal bradycardia (FHR < 110/min)
- Loss of baseline variability
- Recurrent variable decelerations and/or late decelerations
- A nonreassuring tracing requires intrauterine resuscitation and/or immediate delivery (cesarean or, if imminent, vaginal delivery).
-
Characteristic changes in the fetal heart rate (FHR) in response to fetal hypoxia and metabolic acidosis
-
Reassuring fetal status
- A fetal heart tracing that shows a good beat to beat variability (> 6 bpm), > 2 accelerations within a 20 minute period, and no evidence of fetal distress (e.g., fetal bradycardia, fetal tachycardia, late or variable decelerations, sinusoidal pattern)
- Indicates fetal well-being.
Management
See “Intrauterine resuscitation” for details.
- Initial management includes repositioning of the mother, supplemental O2, fluids, and delayed active pushing in the second stage of labor.
- Consider amnioinfusion, tocolytics, and emergency cesarean delivery if initial measures are unsuccessful.
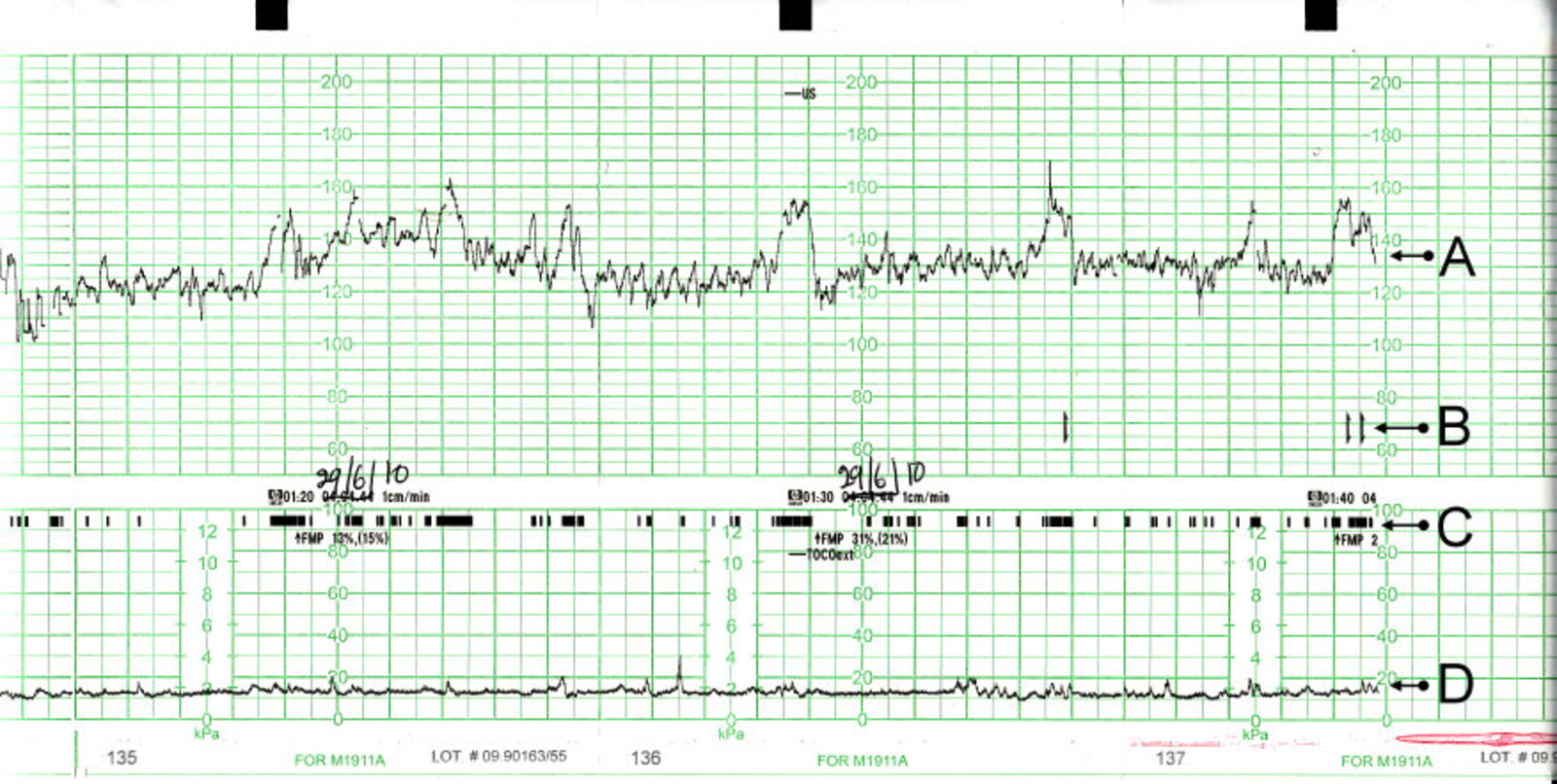
CTG with normal findings (in a woman not in labor), including several accelerations.
(A) Fetal heart rate (FHR)
(B) Fetal movements felt by mother (signalled by pressing a button)
(C) Fetal movements recorded by instruments
(D) Uterine contractions
Source: “CTG Output” by PhantomSteve, Wikimedia Foundation, licensed under CC BY-SA 3.0.
{kind=link}
20 minute cardiotocogram (CTG) section
Upper blue trace: fetal heart rate in beats per minute (bpm)
Middle trace (black bars; light blue overlay): fetal movement recording
Lower blue trace: maternal contractions in mmHg
The baseline fetal heart rate of 175 bpm (dashed red line overlay) is above the normal range (110-160 bpm; light green overlay). Fetal heart rate variability (oscillation of the trace around the baseline) is below the normal (moderate variability) range of 6-25 bpm.
Fetal movements are sparse. There are two contractions visible ∼ 9 minutes apart.
© AMBOSS
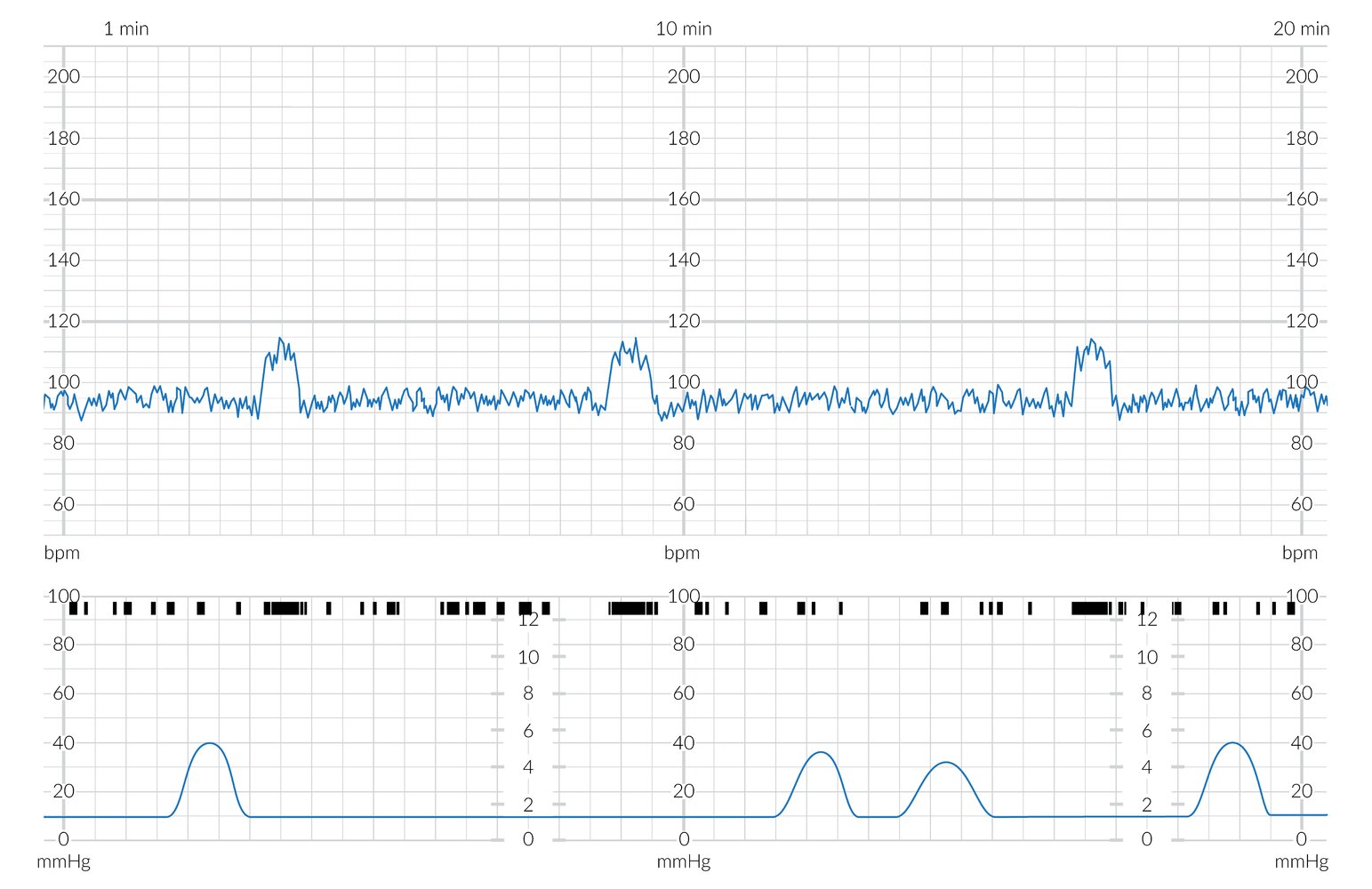
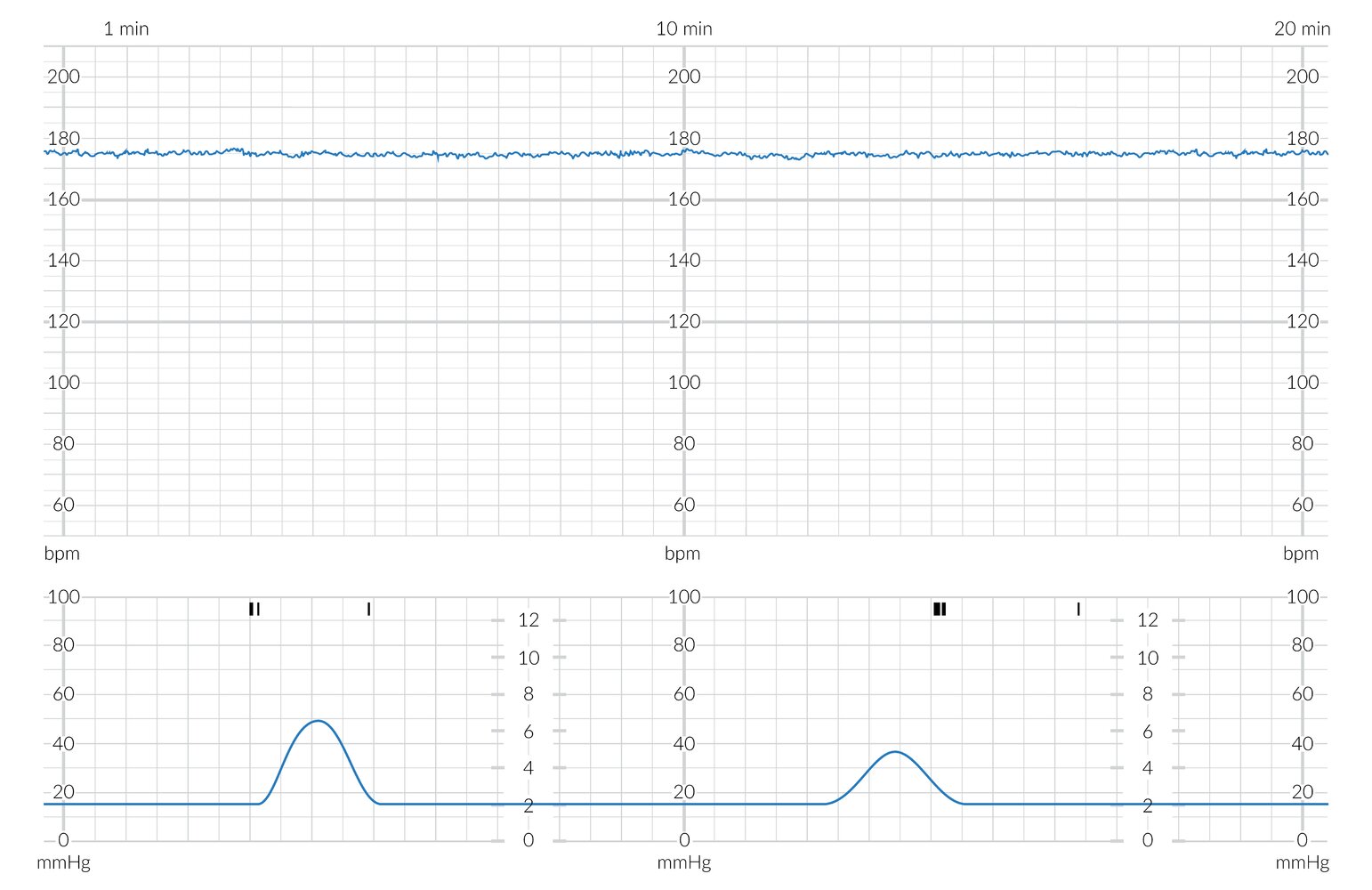
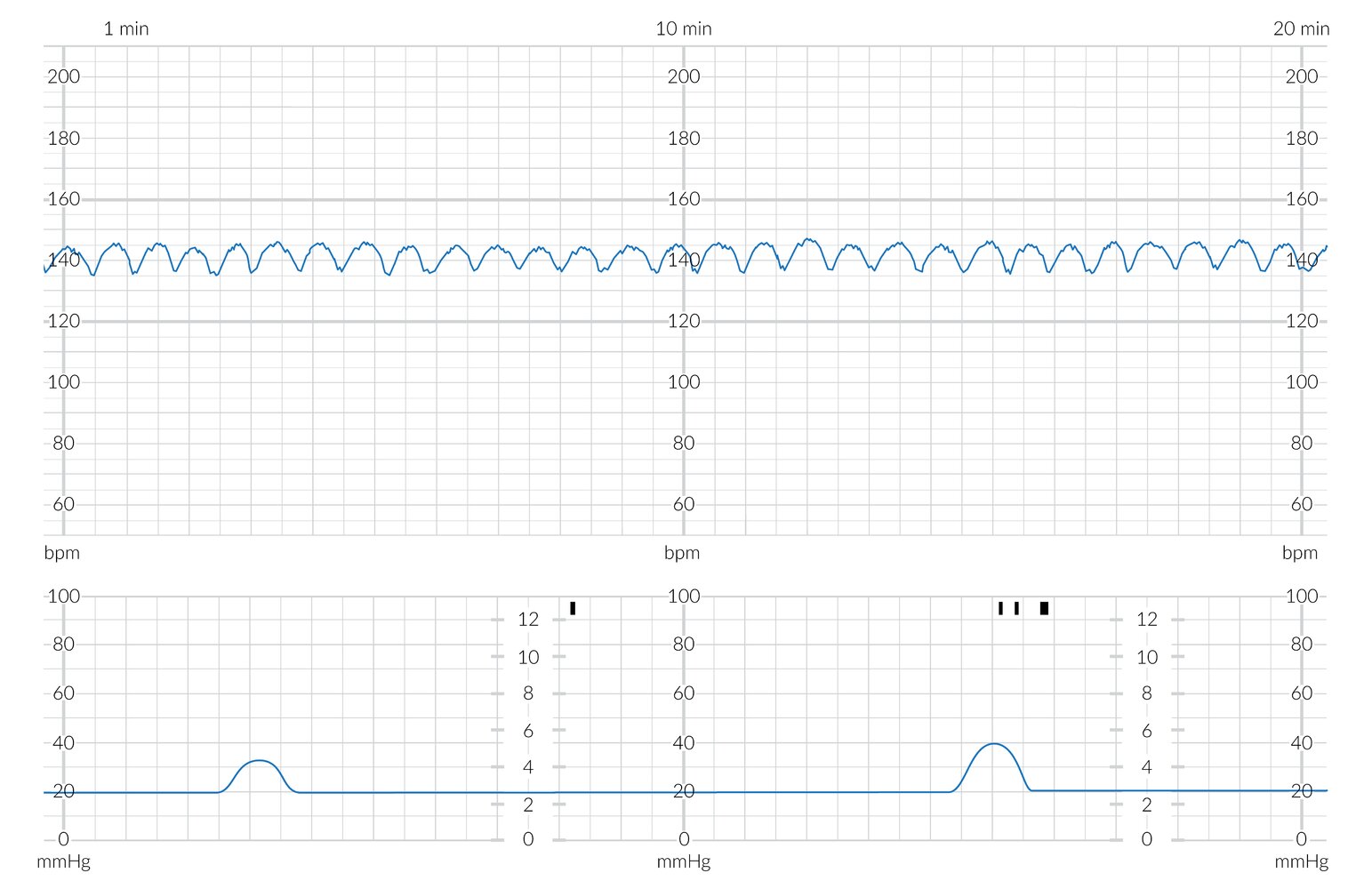
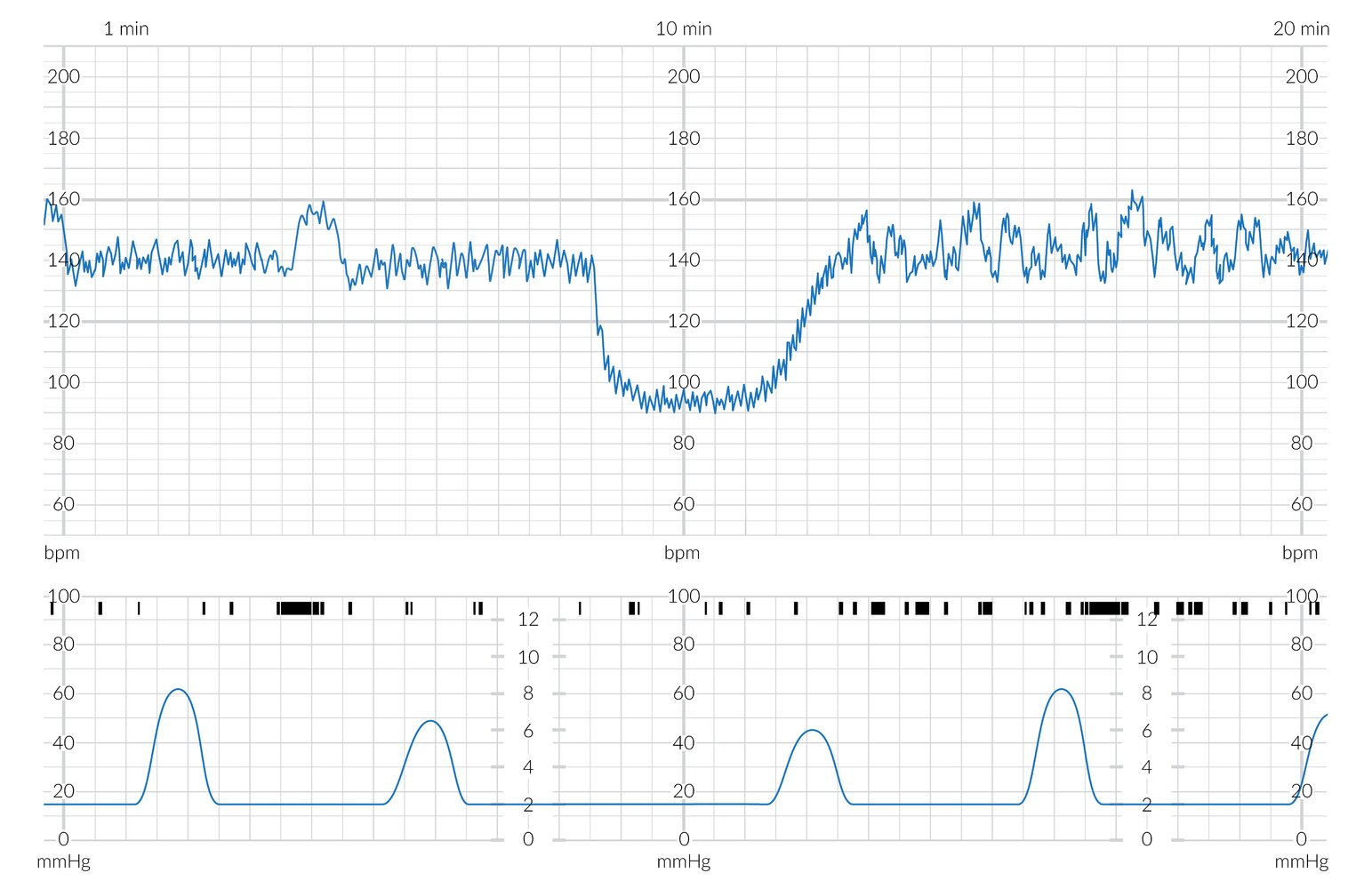
20 minute cardiotocogram (CTG) section
Upper blue trace: fetal heart rate (FHR) in beats per minute (bpm)
Middle trace (black bars; light blue overlay): fetal movement recording
Lower blue trace: maternal contractions in mmHg
The baseline FHR of 95 bpm (dashed red line overlay) is below the normal range (110-160 bpm; light green overlay). FHR variability (oscillation of the trace around the baseline) is within the normal (moderate variability) range of 6-25 bpm. There are three FHR accelerations (green arrow overlay), which coincide with periods of increased fetal movement.
While the FHR in itself is pathologically low, in the context of normal variability a FHR of 90-99 may possibly represent a normal variant.
© AMBOSS
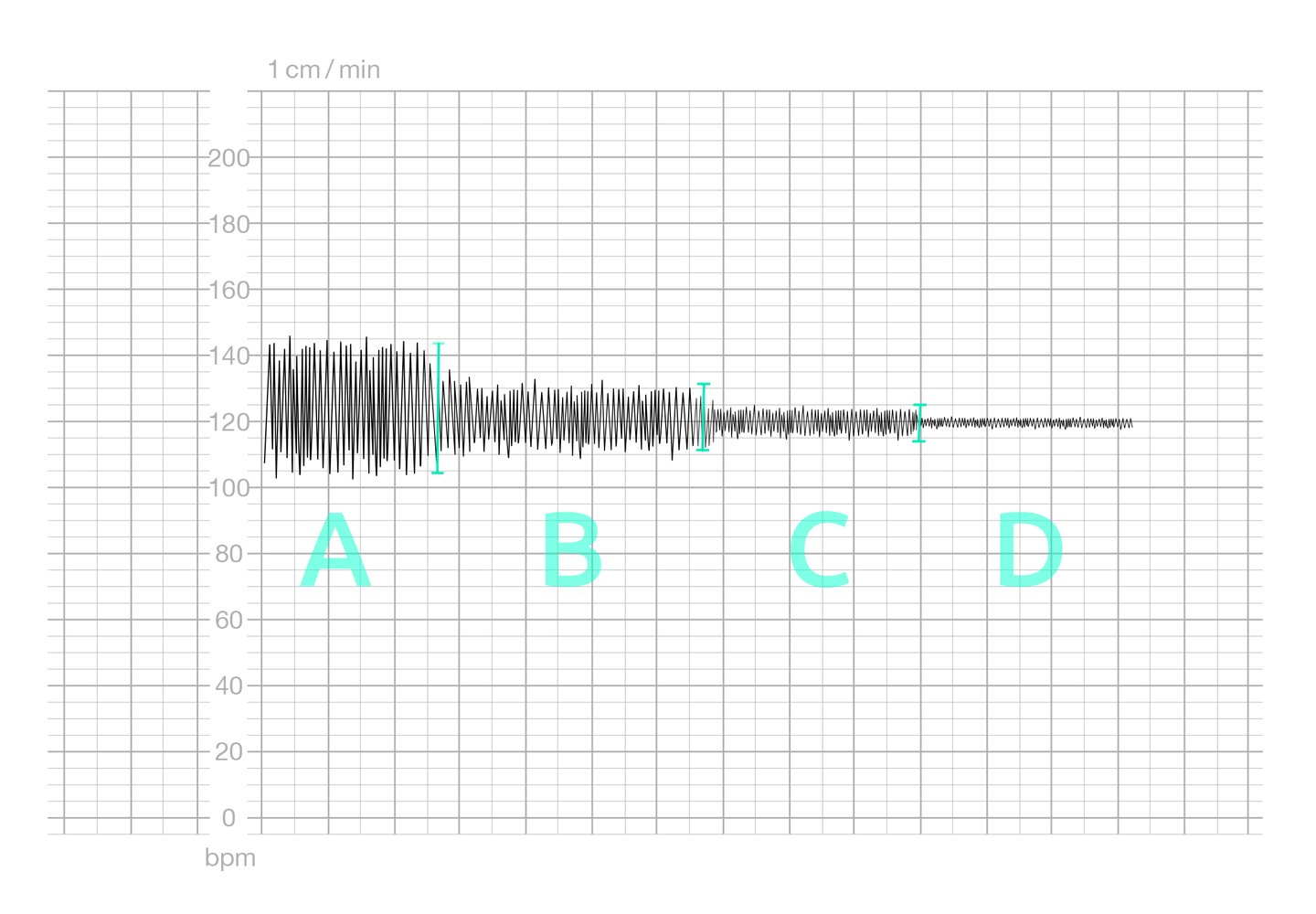
The baseline fetal heart rate (FHR) is displayed on the Y-axis (approx. 120–130/min, which is within normal limits).
CTG also conveys information about the variability of FHR oscillations, which is an indication of fetal movement. Variability of FHR is classified as follows:
(A) Marked: amplitude > 25/min
(B) Moderate: amplitude 6–25/min
(C) Minimal: amplitude 0–5/min
(D) Absent: amplitude undetectable
© AMBOSS
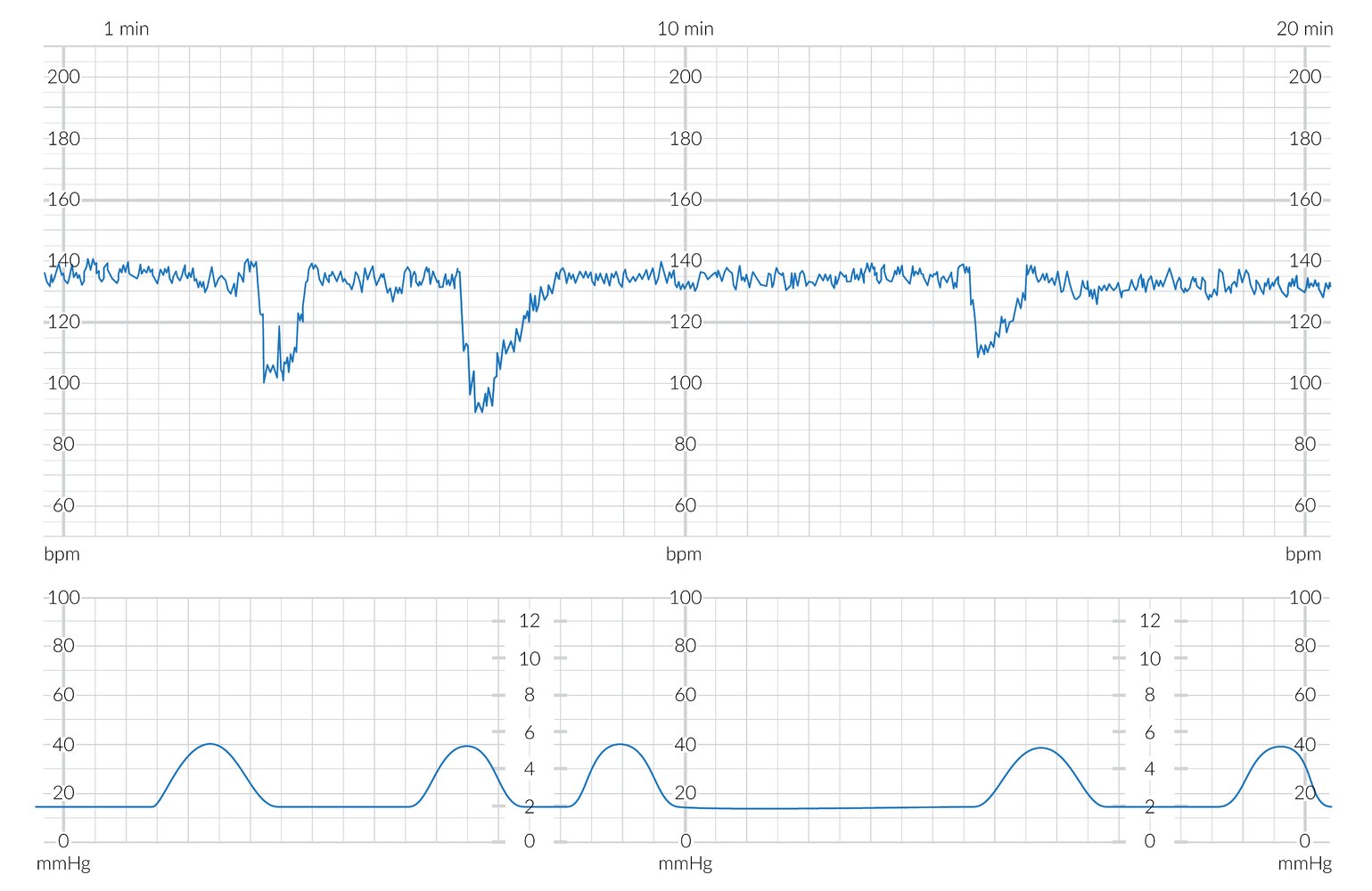
The upper blue tracing shows the fetal heart rate (FHR) in beats per minute (bpm) with a baseline of approx. 135 bpm (green dashed line overlay). The FHR lies within the normal range (green shading overlay) and shows moderate variability (~10 bpm; normal range 6–25 bpm).
The lower blue tracing shows the maternal uterine contractions (in mm Hg). The black markings above this tracing show fetal movements (blue shading overlay).
There are three FHR accelerations (green arrow overlay), which coincide with periods of increased fetal movement.
© AMBOSS
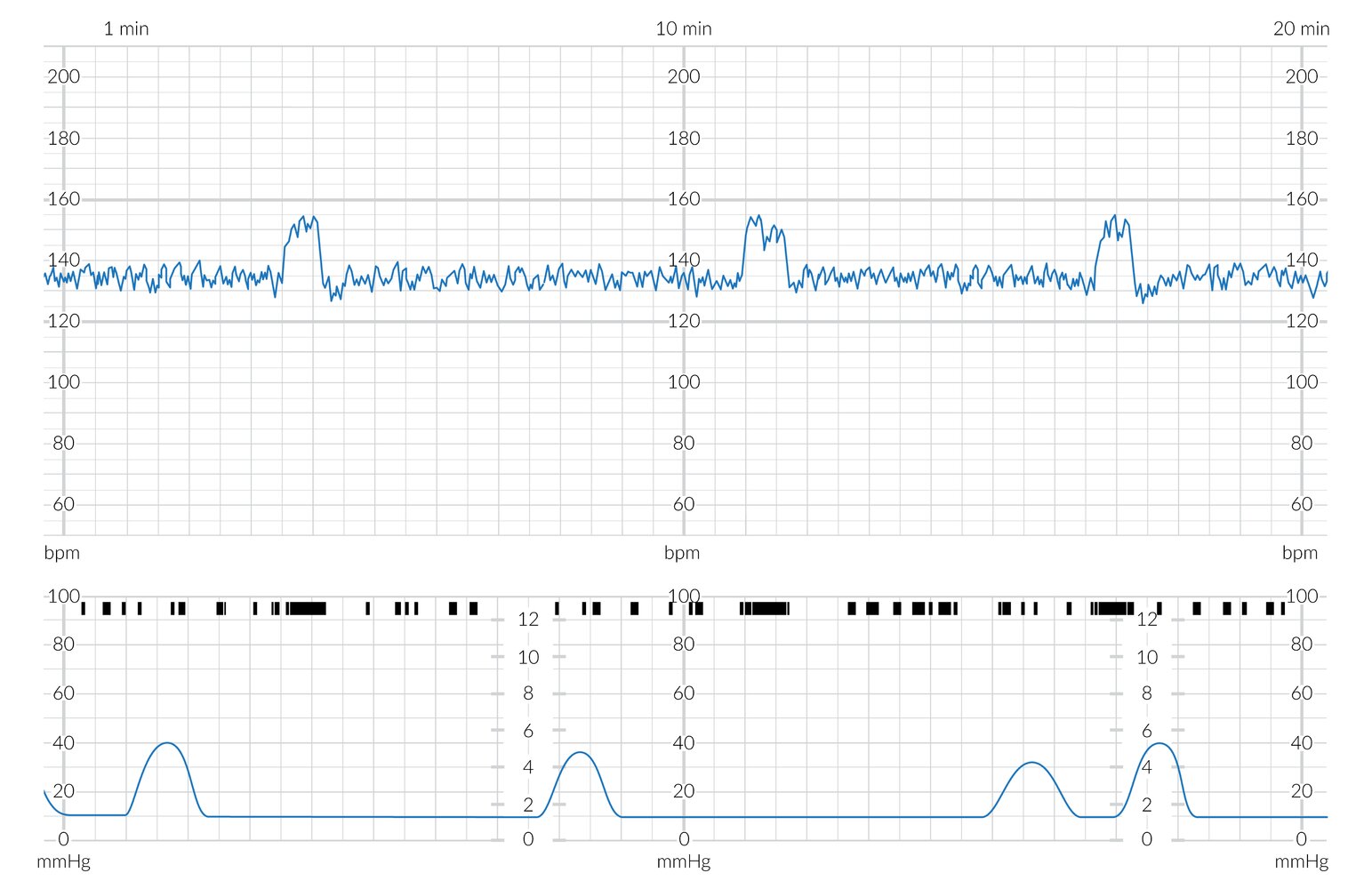
20 minute cardiotocogram (CTG) section
Upper blue trace: fetal heart rate in beats per minute (bpm)
Middle trace (black bars; light blue overlay): fetal movement recording
Lower blue trace: maternal contractions in mmHg
The baseline fetal heart rate of 135 bpm (dashed green line overlay) is within the normal range (110-160 bpm; light green overlay). However, fetal heart rate variability (oscillation of the trace around the baseline) is outside the normal (moderate variability) range of 6-25 bpm.
Fetal movements are unremarkable. Contractions are largely regular and around 6 minutes apart.
© AMBOSS
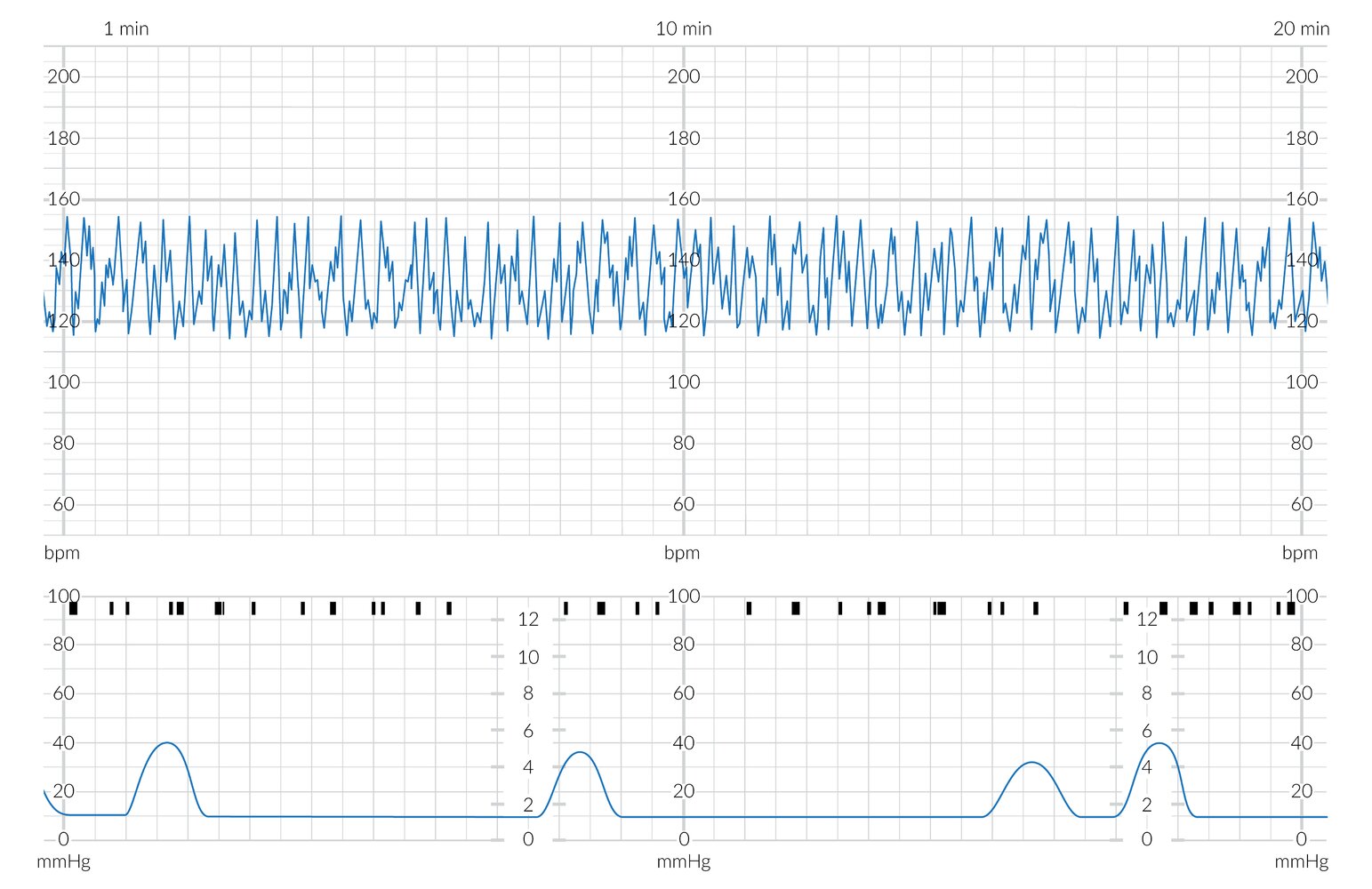
20 minute cardiotocogram (CTG) section
Upper blue trace: fetal heart rate in beats per minute (bpm)
Middle trace (black bars; light blue overlay): fetal movement recording
Lower blue trace: maternal contractions in mmHg
The baseline fetal heart rate of 140 bpm (dashed green line overlay) is within the normal range (110-160 bpm; light green overlay). However, the oscillation is smooth and regular, resembling a sinus wave (rather than the spiky and slightly irregular appearance of a normal trace).
Fetal movements are sparse. There are two contractions visible ∼ 10 minutes apart.
This is a highly concerning CTG suggestive of severe fetal anemia or hypoxia.
© AMBOSS
The upper blue tracing shows the fetal heart rate (FHR) in beats per minute (bpm) with a baseline of approx. 130 bpm (green dashed line overlay). The FHR baseline lies within the normal range (green shading overlay) and shows moderate variability (~10 bpm; normal range 6–25 bpm).
The lower blue tracing shows the maternal uterine contractions (in mm Hg). The black markings above this tracing show fetal movements (blue shading overlay).
Contractions and decelerations begin and end together (red dashed line overlay), with the peaks of the contractions coinciding with the nadirs of the decelerations (red arrow overlay). The decelerations are gradual, with ≥ 30 s from onset to nadir. These findings are characteristic of early decelerations.
© AMBOSS
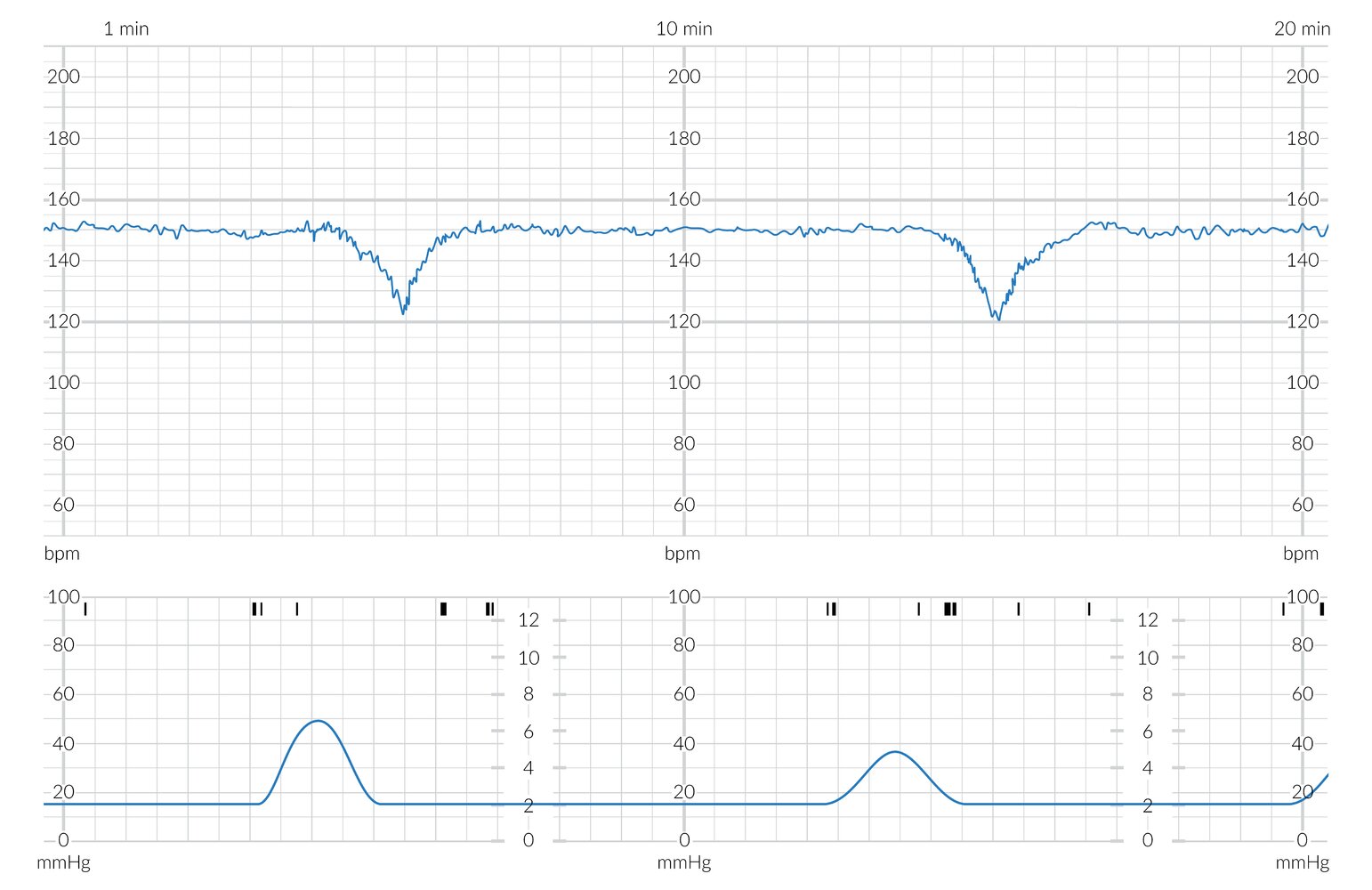
The upper blue tracing shows the fetal heart rate (FHR) in beats per minute (bpm) with a baseline of approx. 150 bpm (green dashed line overlay). The FHR lies within the normal range (green shading overlay) and shows minimal variability (< 6 bpm; normal range 6–25 bpm).
The lower blue tracing shows the maternal uterine contractions (in mm Hg). The black markings above this tracing show fetal movements (blue shading overlay).
The decelerations begin after the peaks of the uterine contractions (red dashed line overlay). These are gradual, with ≥ 30 s from onset to nadir (red arrow overlay). These findings are characteristic of late decelerations.
© AMBOSS
The upper blue tracing shows the fetal heart rate (FHR) in beats per minute (bpm), with a baseline of approx. 135 bpm (green dashed line overlay). The FHR baseline lies within the normal range (green shading overlay) and exhibits moderate variability (∼ 10 bpm; normal range 6–25 bpm).
The lower blue tracing shows maternal uterine contractions (in mm Hg). The black markings above this tracing show fetal movements (blue shading overlay).
The two decelerations visible are abrupt, with < 30 s from onset to nadir (red arrow overlay). They moreover vary in their shape and their temporal relation to the uterine contractions (dashed red line overlay). These findings are characteristic of variable decelerations. As the decelerations here occur with < 50 % of uterine contractions over a 20-minute time period, they are termed intermittent variable decelerations.
© AMBOSS
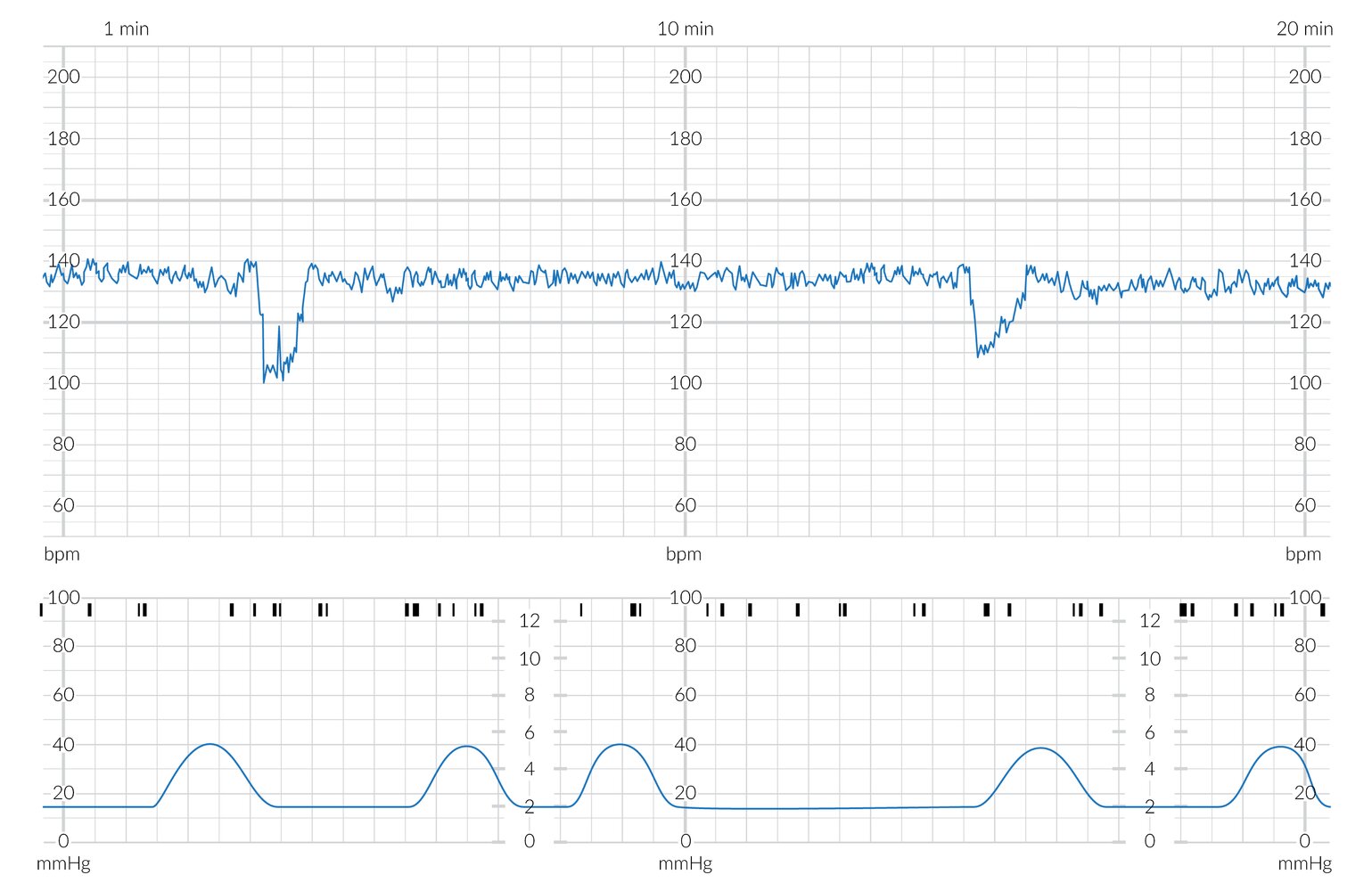
The upper blue tracing shows the fetal heart rate (FHR) in beats per minute (bpm), with a baseline of approx. 136 bpm (dashed green line overlay). The FHR baseline lies within the normal range (green shading overlay) and shows moderate variability (∼ 10 bpm; normal range 6–25/minute). The lower blue tracing shows the maternal uterine contractions (in mm Hg).
The three decelerations visible are abrupt, with < 30 s from onset to nadir (red arrow overlay), and vary in their shape and their temporal relation to the uterine contractions (dashed red line overlay). These findings are characteristic of variable decelerations. As the decelerations here occur with ≥ 50% of uterine contractions over a 20-minute time period, they are termed “recurrent variable decelerations.” This pattern is concerning for umbilical cord compression/prolapse. If persistent, it may prompt considering emergency cesarean delivery.
© AMBOSS
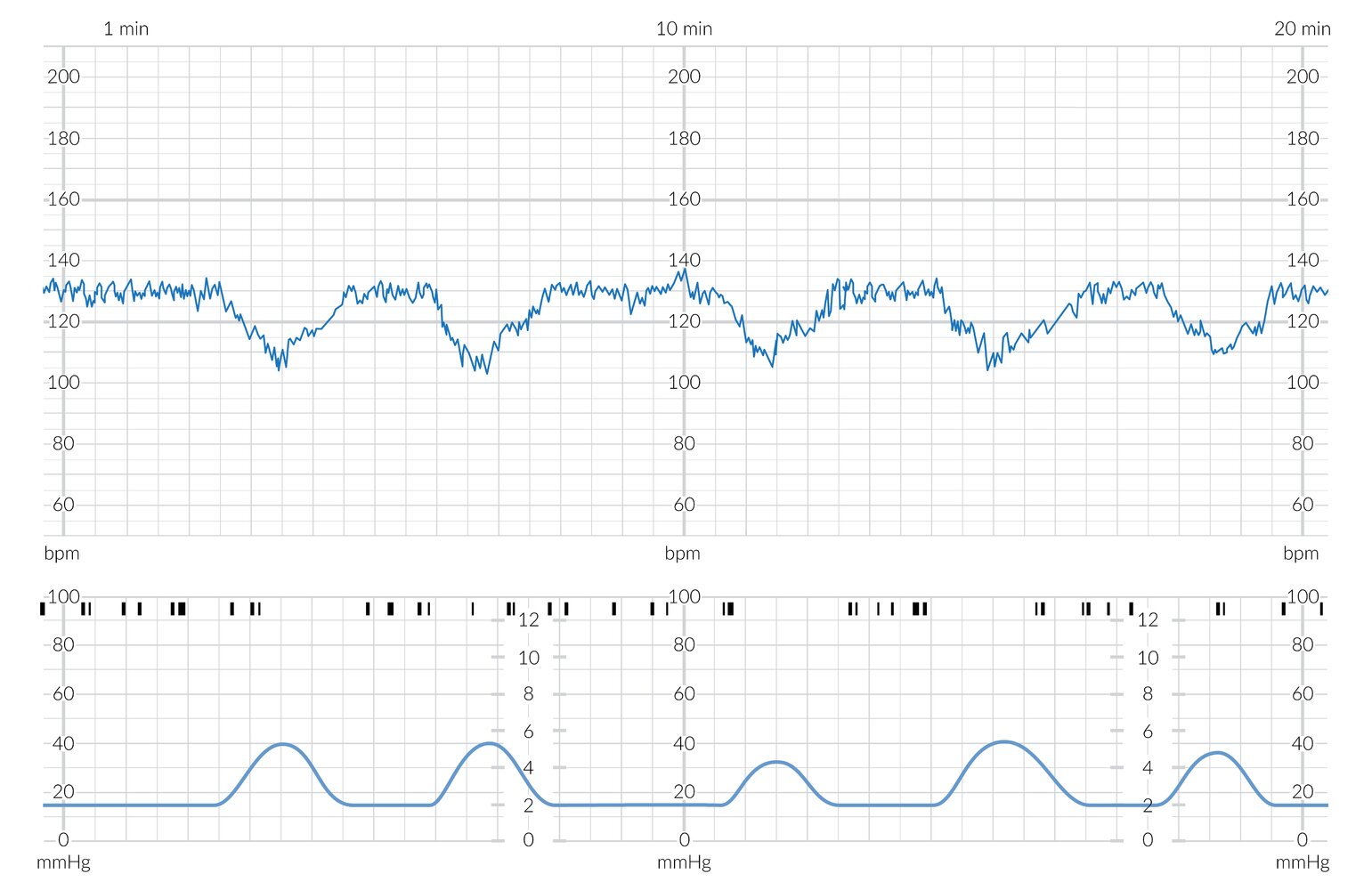
20 minute cardiotocogram (CTG) section
Upper blue trace: fetal heart rate (FHR) in beats per minute (bpm)
Middle trace (black bars; light blue overlay): fetal movement recording
Lower blue trace: maternal contractions in mmHg
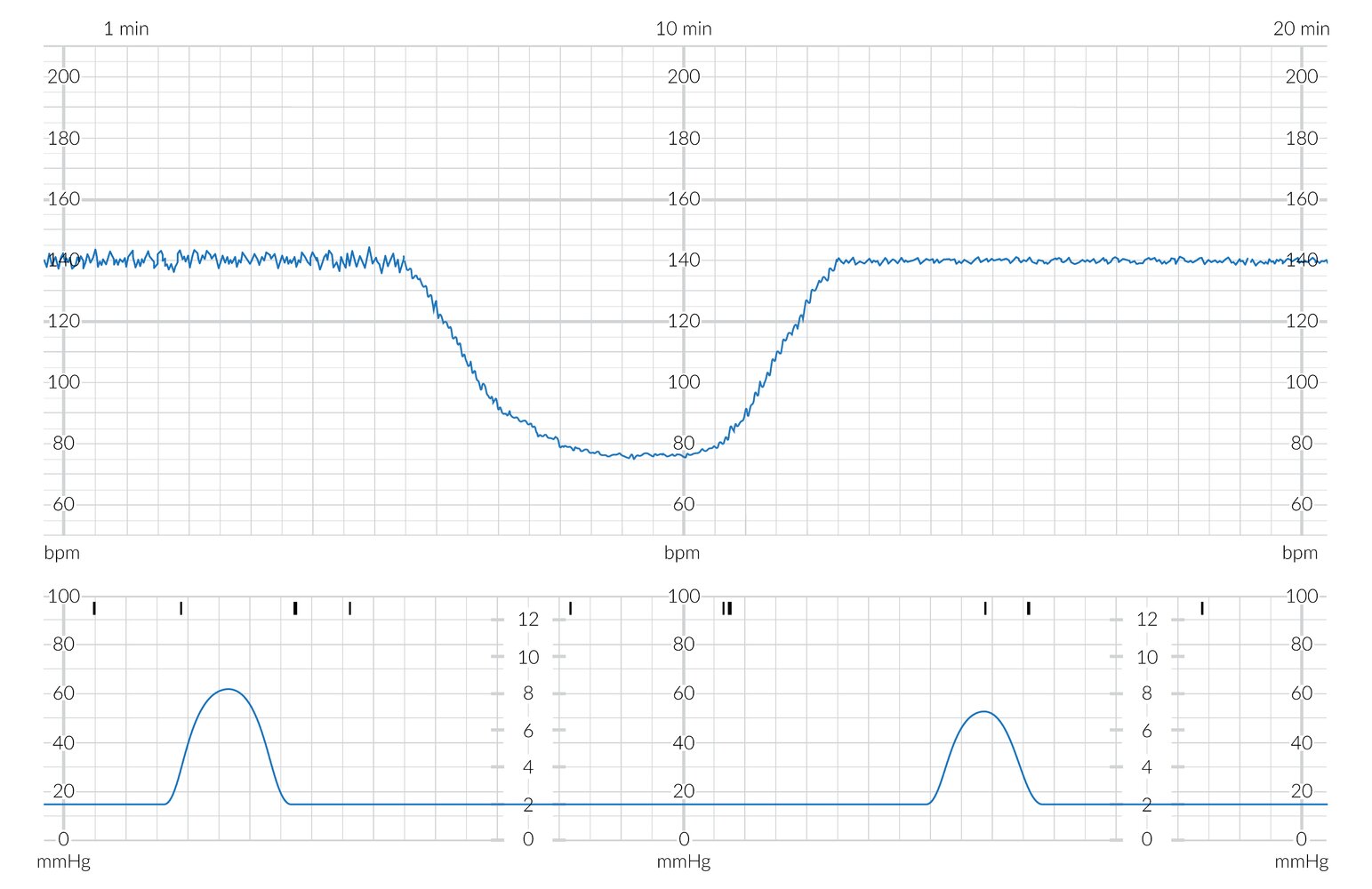
The baseline fetal heart rate of 140 bpm (dashed green line overlay) is within the normal range (110-160 bpm; light green overlay). FHR variability (oscillation of the trace around the baseline) is also normal at ∼15 bpm. Fetal movements are unremarkable. Contractions are largely regular at a rate of ∼2-3 every 10 minutes. There is an unremarkable acceleration and a prolonged deceleration. The deceleration lasts ∼4 minutes and does not have an obvious temporal relation to a contraction. During the deceleration, variability reduces to ∼10 bpm but remains within the normal (moderate variability) range of 6-25 bpm.
This is a concerning CTG that should prompt intrauterine resuscitation and, if the FHR pattern does not improve, emergency cesarean delivery.
© AMBOSS
20 minute cardiotocogram (CTG) section
Upper blue trace: fetal heart rate (FHR) in beats per minute (bpm)
Middle trace (black bars; light blue overlay): fetal movement recording
Lower blue trace: maternal contractions in mmHg
The baseline fetal heart rate of 140 bpm (dashed green line overlay) is within the normal range (110-160 bpm; light green overlay). FHR variability (oscillation of the trace around the baseline) is initially at ∼10 bpm, within the normal (moderate variability) range of 6-25 bpm. There is a prolonged deceleration lasting ∼7 minutes, with no obvious temporal relation to a contraction. During the deceleration, variability pathologically drops below 6 bpm. Fetal movements are sparse. There are two contractions visible ∼ 10 minutes apart.
This is a highly concerning CTG that should prompt emergency cesarean delivery.
© AMBOSS
Complications of delivery
Life-threatening complications
- Prolonged second stage of labor
- Obstructed labor, e.g., due to shoulder dystocia
- Umbilical cord complications, including nuchal umbilical cord
- Uterine rupture
- Uterine inversion
- Postpartum hemorrhage
- Amniotic fluid embolism
- See also “Abnormal labor and delivery.”
Perineal lacerations
- Definition: tear of the perineal area due to significant or rapid stretching forces during labor and delivery
- Epidemiology: most common obstetric injury of the pelvic floor
-
Risk factors [30]
- Macrosomia
- Forceps delivery
- No previous delivery
- Prolonged second stage of labor
- Occiput posterior delivery
- Rapid delivery of head in breech presentation
- Head extension before crowning
- Lack of perineal elasticity (e.g., perineal edema)
-
Classification ; [1][31]
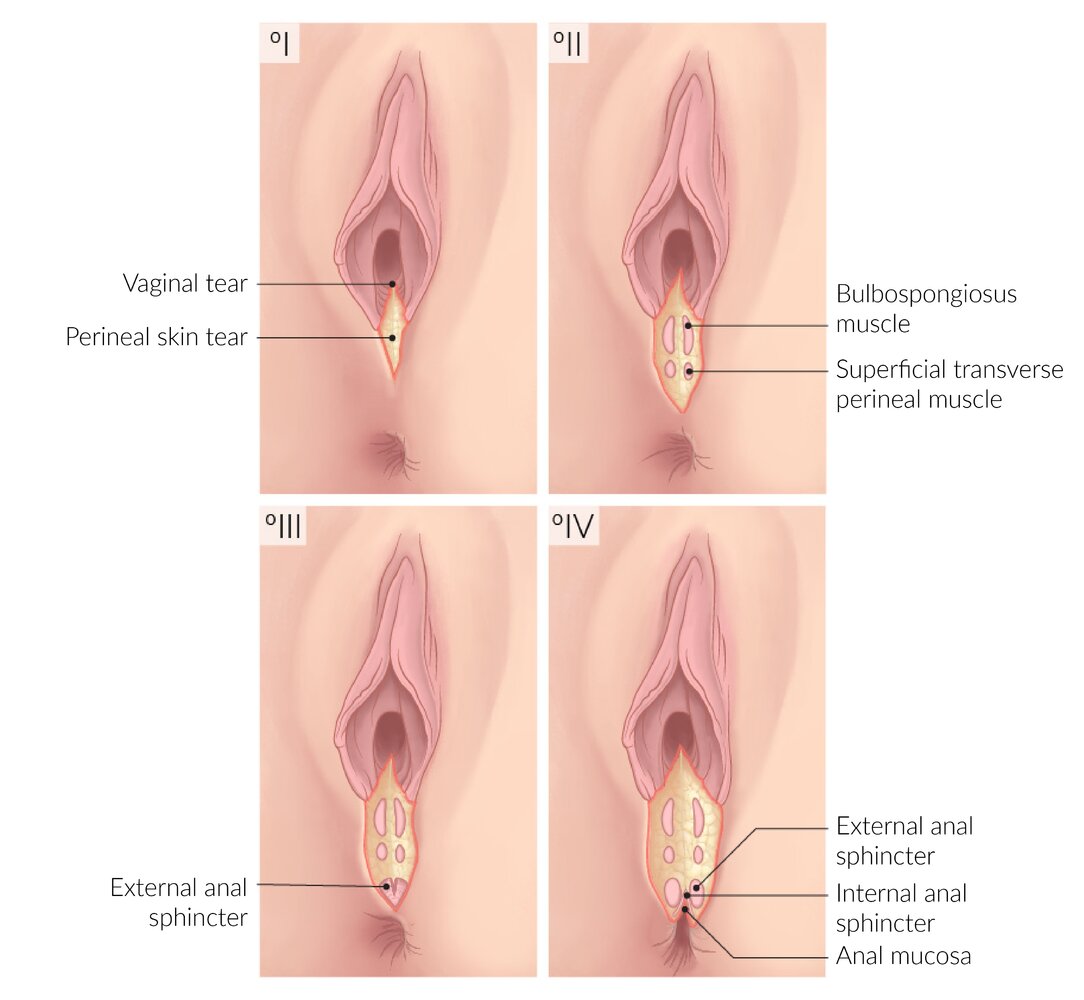
- First degree: cutaneous to subcutaneous tissue tear (skin, fourchette, posterior vaginal wall) with no involvement of the perineal muscles
- Second degree: first-degree lacerations plus laceration of the perineal muscles without involvement of the anal sphincter
-
Third degree: second-degree lacerations plus involvement of the external anal sphincter (may lead to fecal incontinence due to sphincter involvement)
- A: < 50% of the external anal sphincter is torn.
- B: > 50% of the external anal sphincter is torn.
- C: external and internal anal sphincters are torn.
- Fourth degree: third-degree lacerations plus lacerations of the anterior wall of the anal canal or rectum
-
Clinical features: symptoms of a missed perineal laceration (occult perineal laceration) may manifest immediately or up to years after delivery ; [32]
- Perineal edema/hematoma, dysuria
- Symptoms of pelvic floor dysfunction (e.g., fecal/flatus incontinence, pelvic organ prolapse)
- Signs of infection (e.g., foul-smelling discharge, fever, persisting pain)
-
Diagnosis
-
Digital rectal examination findings
- A palpable defect
- Decreased anal sphincter tone and/or asymmetric sphincter contractions
- Endoanal ultrasonography: to evaluate the integrity of the internal and external anal sphincter
-
Digital rectal examination findings
-
Treatment
- First and second degree: Minor tears (e.g., superficial, hemostatic lacerations) are left to the clinician’s discretion to determine if suturing is required. [33]
- Conservative: e.g., NSAIDs, sitz baths
- Suture: local anesthesia and laceration closure using surgical glue or continuous sutures
- Third and fourth degree
- Regional or general anesthesia may be used.
- Reconstructive surgery to repair the anal sphincters and mucosa
- Reconstruction of the distal rectovaginal septum and the perineal body
- First and second degree: Minor tears (e.g., superficial, hemostatic lacerations) are left to the clinician’s discretion to determine if suturing is required. [33]
-
Complications [34]
- Primarily associated with third- and fourth-degree lacerations.
-
Complications include:
- Pain and dyspareunia
- Rectovaginal fistulae
- Hemorrhage
- Infection
- Wound dehiscence
- Prevention: application of warm compress to perineum during delivery
Complications of fourth-degree lacerations include rectovaginal fistulae.


Obstetric nerve injuries [35]
Acute nerve injury can occur during childbirth due to compression, transection, traction, or vascular injury to the nerve.
| Obstetric nerve injuries | ||
|---|---|---|
| Nerve | Clinical features | Risk factors |
| Lumbar radiculopathy |
|
|
| Lateral femoral cutaneous nerve injury |
|
|
| Femoral nerve injury |
|
|
| Common peroneal nerve injury |
|
|
| Pudendal nerve injury |
|
|
Coccydynia
- Etiology: injury to the coccyx during childbirth as a result of internal and external pressure on the coccyx during labor and delivery
-
Clinical features
- Pain and tenderness of the coccyx, esp. when sitting or leaning back
- Pain may suddenly increase when the patient is changing from a sitting to a standing position.
- Pain may also occur during defecation or sexual intercourse.
- Physical examination: palpation of the coccyx elicits pain
- Diagnosis: clinical
-
Management
- Protection (e.g., sitting on Donut or wedge cushions)
- Analgesics (e.g., NSAIDs)
- Local heat or cooling according to patient preference
- Exacerbating factors (e.g., sitting on hard surfaces, cycling) should be avoided if possible.
- Prognosis: resolves spontaneously in the majority of patients (> 90%) [36]
Postpartum retroperitoneal hematoma
- Epidemiology: rare (∼ 1:1000) [37]
-
Etiology: injury to branches of the internal iliac artery (most commonly, uterine artery)
- Most commonly due to:
- Laceration of a uterine artery during hysterotomy or uterine rupture
- Extension of a paravaginal hematoma into the retroperitoneal space
- Other: pelvic or abdominal injury, anticoagulation, rupture of an aneurysm of the abdominopelvic vasculature
- Most commonly due to:
-
Clinical features
- Signs of hemodynamic instability (e.g., tachycardia, hypotension)
- Usually painless (unless caused by pelvic or abdominal injury)
- Diagnostics: imaging (e.g., sonography, CT)
-
Management
- Prompt laparotomy
- Alternatively: selective arterial embolization
First degree: cutaneous to subcutaneous tissue tear (skin, fourchette, posterior vaginal wall) with no involvement of the perineal muscles
Second degree: first-degree lacerations plus laceration of the perineal muscles without involvement of the anal sphincter
Third degree: second-degree lacerations plus involvement of the external anal sphincter
Fourth degree: third-degree lacerations plus lacerations of the anterior wall of the anal canal or rectum
© AMBOSS
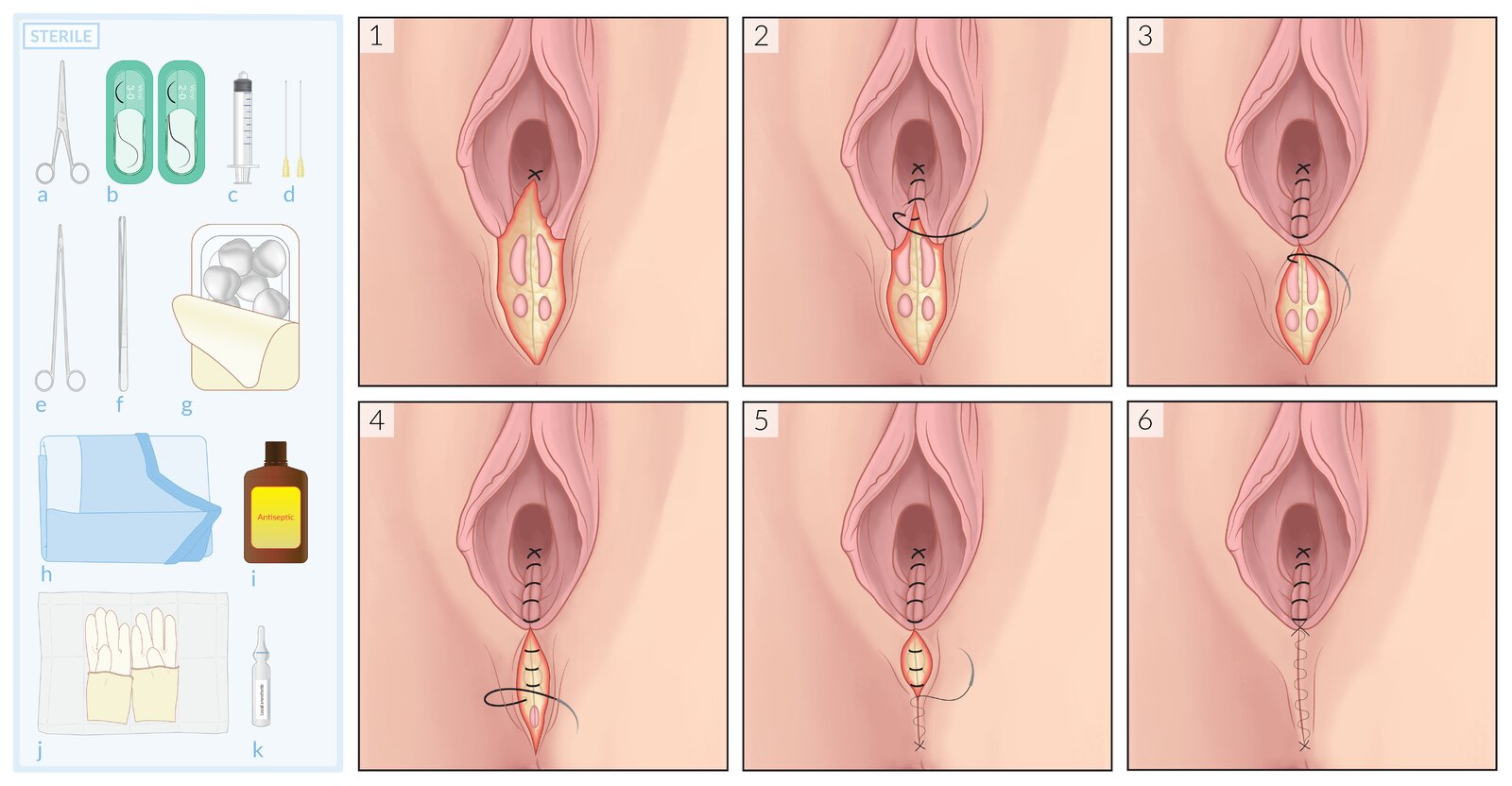
Before beginning surgical repair, it is necessary to confirm that the perineal tear is a second-degree laceration and does not extend into the external anal sphincter. The procedure is then performed under local anesthesia (may not be required with an epidural) following surgical field disinfection.
Materials (left):
a: Scissors
b: Suture material (3-0 and 2-0)
c: Syringe for local anesthetic
d: Needles for drawing up and injecting local anesthetic
e: Needle holder
f: Forceps
g: Surgical swabs
h: Surgical drapes
i: Antiseptic
j: Sterile gloves
k: Local anesthetic
Procedure (right):
1) Placement of an anchoring suture cranial to the upper end of the laceration
2) Closure of vaginal mucosa and rectovaginal fascia up to the hymenal ring, using a running suture
3 & 4) The same running suture may be continued to close the perineal muscles (shown here). Alternatively, the vaginal suture may be tied off proximal to the hymenal ring, and a new running suture or interrupted sutures may be used to close the perineal muscles (not shown here).
5 & 6) If further approximation of the skin is required, this can be achieved using running subcuticular sutures.
© AMBOSS
Planned home birth
-
Statistics
- In the US, approx. 1% of births per year are home births.
- 75% of these home births are planned.
-
Indications
- There is insufficient evidence to determine what makes a good candidate for a home birth.
- Home births can be considered in individuals with no contraindications.
- Patients who would like to plan a home birth should be advised about the benefits and risks of home birth compared to hospital delivery in order to make an informed decision.
-
Advantages compared to hospital delivery
- Lower risk of maternal interventions (e.g., induction or augmentation of labor, episiotomy, cesarean delivery)
- Lower risk of certain maternal complications (e.g., vaginal or perineal lacerations, peripartum or postpartum infections)
- Lower costs
- Familiar environment for the mother
-
Disadvantages compared to hospital delivery
- Higher risk of perinatal death for both the mother and fetus
- Higher risk of neurological complications for the newborn
-
Contraindications
-
Absolute contraindications
- Fetal malpresentation (e.g., breech presentation)
- Multiple gestation pregnancy
- Previous cesarean delivery
-
Relative contraindications
- Any other risk factor for a complicated pregnancy (see “High-risk pregnancies”)
- No means for safe and timely transport to a nearby hospital or accredited birth center
- Lack of access to home-birth provider services (e.g., certified professional midwife, certified nurse midwife, obstetrician, family medicine physician)
-
Absolute contraindications
References:[38]
Obstetric analgesia
This guidance pertains to analgesia for normal spontaneous vaginal delivery. Analgesic considerations may differ for assisted vaginal delivery and cesarean delivery.
General principles [39][40]
- Discuss analgesic options during counseling related to peripartum care.
- Nonpharmacological and pharmacological strategies may be used alone or in combination.
- Consult anesthesia early for any of the following:
- If difficulty administering anesthesia is anticipated (e.g., due to obesity, anatomic abnormalities of head or neck)
- Comorbidities in the mother (e.g., spinal cord injury, cardiomyopathy, coagulopathy, opioid use disorder) [41]
- Obstetric complications (e.g., placenta accreta)
- See “Postpartum pain management” for analgesia after birth.
Nonpharmacological strategies [39][42]
- Upright positioning (e.g., walking, sitting, squatting, kneeling) [43][44]
- Water immersion: during first stage of labor for uncomplicated pregnancies between 37 and 41 6/7 weeks' gestation [45][46]
- Support companion (e.g., a doula) throughout labor [13][47]
- Other strategies: limited evidence of benefit, but low risk [48]
- Lumbosacral massage
- Relaxation techniques (e.g., breathing, music, mindfulness) [13]
- Hypnosis [49]
- Warm showers
Use of a continuous support companion during labor can improve maternal outcomes (e.g., reduced need for analgesics during labor, shorter duration of labor, and lower rates of cesarean delivery) and neonatal outcomes (e.g., higher neonatal Apgar scores). [13][47]
Pharmacological strategies [39][40]
Neuraxial anesthesia is the most effective pharmacological option. Systemic analgesia is available for patients who prefer noninvasive options. [39]
Neuraxial anesthesia
- Most effective and most commonly used option [39]
- May be offered during any stage of labor [50]
- Modalities: typically include a local anesthetic ± an opioid [40][51]
- Epidural anesthesia
- Combined spinal and epidural anesthesia (walking epidural) [40]
- Dural puncture epidural anesthesia [39][52]
- Single-injection spinal anesthesia [40][51]
- Contraindications: See “Regional anesthesia” for details.
- See “Complications of neuraxial anesthesia.”
Neuraxial anesthesia does not increase the risks of assisted vaginal delivery or cesarean delivery. [39]
Systemic analgesia
- Nitrous oxide
- Opioids, e.g., fentanyl, butorphanol, morphine (IM or IV)
- Acetaminophen (oral or IV)
- Sedatives, e.g., benzodiazepines
- Antihistamines, e.g., promethazine
Patients on opioid agonist therapy for opioid use disorder in pregnancy often require multiple pharmacological strategies to achieve adequate peripartum pain control. [39][53]
Local anesthesia
- Paracervical block: during first stage of labor [54]
- Pudendal block: during second stage of labor and for perineal laceration repairs
External Resources
- 2020 ACOG Committee Opinion No. 814: Delayed Umbilical Cord Clamping After Birth
- 2018 WHO Recommendations: Intrapartum Care for a Positive Childbirth Experience
- 2017 ACOG Committee Opinion No. 687: Approaches to Limit Intervention During Labor and Birth
- 2021 AAFP`Review on Pain Management in Labor
- 2019 ACOG Committee Opinion No. 209: Obstetric Analgesia and Anesthesia (reaffirmed 2024)
References
- Smith A, Laflamme E, Komanecky C. "Pain Management in Labor". Am Fam Physician. 103(6). :355-364. (2021)
- ACOG. "ACOG Practice Bulletin No. 209: Obstetric Analgesia and Anesthesia". Obstet Gynecol. 133(3). :e208-e225. (2019)
- The American College of Obstetricians and Gynecologists. "Committee Opinion No. 711: Opioid Use and Opioid Use Disorder in Pregnancy". Obstetrics & Gynecology. 130(2). :e81-e94. (2017)
- ACOG. "ACOG Committee Opinion No. 766: Approaches to Limit Intervention During Labor and Birth". Obstet Gynecol. 133(2). :e164-e173. (2019)
- Lawrence A, Lewis L, Hofmeyr GJ, Styles C. "Maternal positions and mobility during first stage labour". Cochrane Database Syst Rev. (2013)
- Gupta JK, Sood A, Hofmeyr GJ, Vogel JP. "Position in the second stage of labour for women without epidural anaesthesia". Cochrane Database Syst Rev. 2017(5). (2017)
- ACOG. "Committee Opinion No. 679 Summary: Immersion in Water During Labor and Delivery". Obstet Gynecol. 128(5). :1198-1199. (2016)
- Papile LA, Baley JE, et al. "Immersion in Water During Labor and Delivery". Pediatrics. 133(4). :758-761. (2014)
- Bohren MA, Hofmeyr GJ, Sakala C, Fukuzawa RK, Cuthbert A. "Continuous support for women during childbirth". Cochrane Database Syst Rev. 2017(8). (2017)
- World Health Organization. "WHO Recommendations on Intrapartum Care for a Positive Childbirth Experience". World Health Organization. (2018). ISBN: 9789241550215
- AAP Committee on Fetus and Newborn; ACOG Committee on Obstetric Practice. "Guidelines for Perinatal Care, 8th edition". American College of Obstetricians and Gynecologists, American Academy of Pediatrics. (2017). ISBN: 9781934984697
- Madden K, Middleton P, Cyna AM, Matthewson M, Jones L. "Hypnosis for pain management during labour and childbirth". Cochrane Database Syst Rev. 2016(5). (2016)
- ACOG. "First and Second Stage Labor Management". Obstet Gynecol. 143(1). :144-162. (2024)
- American Society of Anesthesiologists. "Practice Guidelines for Obstetric Anesthesia". Anesthesiology. 124(2). :270-300. (2016)
- Toledano RD, Leffert L. "What’s New in Neuraxial Labor Analgesia". Curr Anesthesiol Rep. 11(3). :340-347. (2021)
- ACOG. "Committee Opinion No. 711 Summary: Opioid Use and Opioid Use Disorder in Pregnancy". Obstet Gynecol. 130(2). :488-489. (2017)
- Novikova N, Cluver C. "Local anaesthetic nerve block for pain management in labour". Cochrane Database Syst Rev. 2015(9). (2012)
- Committee on Obstetric Practice. "Committee Opinion No. 697: Planned Home Birth". Obstet Gynecol. 129(4). :e117-e122. (2017)
- Callahan TL, Caughey AB. "Blueprints Obstetrics and Gynecology". Lippincott Williams&Wilki. (2013). ISBN: 9781451117028
- Madara B, Avery CT, Pomarico-Denino V, Wagner L. "Quick Look Nursing: Obstetric and Pediatric Pathophysiology". Jones & Bartlett Learning. (2008). ISBN: 9780763741174
- Dudenhausen JW, Obladen M. "Practical Obstetrics". Walter de Gruyter GmbH & Co KG. (2014). ISBN: 9783110276114
- Beckmann CRB. "Obstetrics and Gynecology". Lippincott Williams & Wilkins. (2010). ISBN: 0781788072
- "Nation's Ob-Gyns Take Aim at Preventing Cesareans". https://www.acog.org/About-ACOG/News-Room/News-Releases/2014/Nations-Ob-Gyns-Take-Aim-at-Preventing-Cesareans. [2014-02-19]
- ACOG. "Obstetric care consensus no. 1: safe prevention of the primary cesarean delivery". Obstet Gynecol. 123(3). :693-711. (2014)
- "The stages of labour and birth". https://www.nhs.uk/pregnancy/labour-and-birth/what-happens/the-stages-of-labour-and-birth/. [2020-03-20]
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine - Concepts and Clinical Practice". Elsevier Health Sciences. (2013). ISBN: 9780323390163
- ACOG Committee. "Delayed Umbilical Cord Clamping After Birth". Obstet Gynecol. 136(6). :e100-e106. (2020)
- Mikolajczyk RT, Zhang J, Troendle J, Chan L. "Risk factors for birth canal lacerations in primiparous women". Am J Perinatol. 25(5). :259-264. (2013)
- Goh R, Goh D, Ellepola H. "Perineal tears – A review". Australian Journal of General Practice. 47(1-2). :35-38. (2018)
- Ozyurt S, Aksoy H, Gedikbasi A, et al. "Screening occult anal sphincter injuries in primigravid women after vaginal delivery with transperineal use of vaginal probe: a prospective, randomized controlled trial". Arch Gynecol Obstet. 292(4). :853-9. (2015)
- Lallemant M, D'Antona A, Vidal C, et al. "Conservative management versus systematic suture of isolated vaginal or first-degree perineal tears after delivery: A preliminary randomized efficacy trial". Birth. (2022)
- Lewicky-Gaupp C, Leader-Cramer A, Johnson LL, Kenton K, Gossett DR. "Wound complications after obstetric anal sphincter injuries". Obstet Gynecol. 125(5). :1088-1093. (2015)
- "Obstetrical Nerve Injury"
- Lirette LS, Chaiban G, Tolba R, Eissa H. "Coccydynia: an overview of the anatomy, etiology, and treatment of coccyx pain". Ochsner J. 14(1). :84-7
- Redondo Villatoro A, Azcona Sutil L, Vargas Gálvez D, Carmona Domínguez E, Cabezas Palacios MN. "Diagnosis and Management of Postpartum Retroperitoneal Hematoma: A Report of 3 Cases". American Journal of Case Reports. 23. (2022)
- Arulkumaran S, Regan L, Papageorghiou A, Farquharson D, Monga A. "Oxford Desk Reference: Obstetrics and Gynaecology". Oxford University Press. (2011). ISBN: 9780199552214
- Afors K, Chandraharan E. "Use of continuous electronic fetal monitoring in a preterm fetus: Clinical dilemmas and recommendations for practice". J Pregnancy. 2011. :1-7. (2011)
- Feinstein N, Torgersen KL, Atterbury J, et al. "Fetal Heart Monitoring, Principles and Practices". Kendall/Hunt. (1993). ISBN: 9780757500596
- "ACOG Practice Bulletin Number 106, July 2009 - Intrapartum Fetal Heart Rate Monitoring: Nomenclature, Interpretation, and General Management Principles"
- Ayres-de-Campos D, Spong CY, Chandraharan E. "FIGO consensus guidelines on intrapartum fetal monitoring: Cardiotocography". Int J Gynaecol Obstet. 131(1). :13-24. (2015)
- Macones GA, Hankins GD, et al. "The 2008 National Institute of Child Health and Human Development workshop report on electronic fetal monitoring: update on definitions, interpretation, and research guidelines". Obstet Gynecol. (2008)
- "Intrapartum Care: Care of Healthy Women and Their Babies During Childbirth - NICE Clinical Guidelines, No. 190". https://www.ncbi.nlm.nih.gov/books/NBK328270/#__NBK328270_dtls__. [2014-12-01]
- Bailey RE. "Intrapartum fetal monitoring". Am Fam Physician. 80(12). :1388-1396. (2009)
- Chang KSG. "Family Medicine". Lippincott Williams & Wilkins. (2007). ISBN: 9781405104951
- Kennedy BB, Ruth DJ, Martin EJ. "Intrapartum Management Modules". Lippincott Williams & Wilkins. (2009). ISBN: 9780781781688
- Maharaj D. "Intrapartum Fetal Resuscitation: A Review". The Internet Journal of Gynecology and Obstetrics. 9(2). (2007)
- Leveno K, Bloom S, Casey B, et al. "Williams Obstetrics". McGraw-Hill Education Ltd. 25th. (2018). ISBN: 9781259644320
- Roberts JR. "Roberts and Hedges' Clinical Procedures in Emergency Medicine and Acute Care". Elsevier. (2018). ISBN: 9780323354783
- Committee on Obstetric Practice. "Committee Opinion No. 687: Approaches to Limit Intervention During Labor and Birth". Obstet Gynecol. 129(2). :e20-e28. (2017)
- Dresang LT, Yonke N. "Management of Spontaneous Vaginal Delivery". Am Fam Physician. 92(3). :202-8. (2015)
- Kelleher J, Bhat R, Salas AA, et al. "Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial". Lancet. 382(9889). :326-330. (2013)
- Dahlke JD, Mendez-Figueroa H, Maggio L, et al. "Prevention and management of postpartum hemorrhage: a comparison of 4 national guidelines". Am J Obstet Gynecol. 213(1). :76.e1-76.e10. (2015)
- Committee on Practice Bulletins-Obstetrics. "Practice Bulletin No. 183: Postpartum Hemorrhage". Obstetrics & Gynecology. 130(4). :e168-e186. (2017)
- Buchmann EJ, Guidozzi F. "Level of fetal head above brim: comparison of three transabdominal methods of estimation, and interobserver agreement". J Obstet Gynaecol. 27(8). :787-790. (2007)