Summary
The process of taking a history and performing a physical examination (H&P) in OB/GYN patients presents unique challenges. Because of the intimate aspect of an OB/GYN examination, it is important to establish trust and a private and relaxing setting for the patient. This article provides an overview of the possible content of the H&P of the OB/GYN patient. Depending on the patient's symptoms, additional and/or more targeted questions may also be relevant. See the “Medical history” and “Physical examination” articles for more information on general clinical examination.
Gynecologic and obstetric history
General principles
- A key difference in OB/GYN history taking is the focus on the menstrual/menopausal history and sexual history.
- Patients may be hesitant to disclose certain aspects of their gynecologic history because of the sensitive nature of the topic. In some cases, it may be due to cultural differences or even a history of abuse.
- Be empathetic and try to create a comfortable environment for each of your patients, since it will encourage them to discuss matters more openly with you.
- If you feel that the patient is uncomfortable talking about their gynecologic history, start with a social or family history in order to establish rapport with the patient.
Gynecologic history
Chief concern and history of present illness
- Begin with a brief summary of the patient's age, parity, date of last menstrual period (LMP), and any current concerns the patient may have.
- Common chief concerns in gynecology
-
Vaginal bleeding should be evaluated based on the following:
- Amount (e.g., spotting, heavy flow)
- Relation to menstrual cycle/menopause/sexual contact (e.g, intermenstrual, postmenopausal, postcoital)
-
Vaginal discharge should be evaluated based on the following:
- Color (e.g., bloody, brown, yellow, green, or gray)
- Consistency (e.g., frothy, curd-like)
- Amount
- Smell (e.g., fishy)
- Pruritic and/or erythematous vagina
-
Abdominal or pelvic pain, that can be described using the SOCRATES mnemonic:
- Site
- Onset
- Character
- Radiation
- Associations
- Time course
- Exacerbating and relieving factors
- Severity
-
Vaginal bleeding should be evaluated based on the following:
To evaluate abdominal/pelvic pain, use the SOCRATES mnemonic: Site, Onset, Character, Radiation, Associations, Time course, Exacerbating and relieving factors, Severity.
Menstrual history
- Age at menarche
- Date of last menstrual period (LMP)
- Duration, regularity, flow and associated symptoms (e.g., dysmenorrhea, mittelschmerz)
- History of intermenstrual vaginal bleeding


Menopausal history (if applicable)
- Age at onset
- History of postmenopausal uterine bleeding
- Associated symptoms (e.g., vasomotor symptoms)
- History of hormone replacement therapy
Past gynecologic history
- Previous gynecologic problems (including diseases of the breast)
- Previous gynecologic/pelvic surgeries (e.g., cervical conization, hysterectomy)
- History of sexually transmitted infections and/or pelvic inflammatory disorder
- Time and results of previous screening/diagnostic tests (e.g., Pap smear, mammography)
Past obstetric history
- See “Obstetric history” below for more information.
Sexual history
-
Opening the discussion
- Discussing a patient's health is often a sensitive matter. It is important to encourage the patient to be as descriptive as possible while remaining sensitive to the fact that they are sharing very private details of their life. Always remain empathetic and open to discussion.
- If the patient seems hesitant, explain to them that this information is vital for forming an overall picture of their health and that it is as important as other aspects of their physical and mental health.
-
Current/past sexual partners
- Discussing the patient's current/past sexual partners is an important part of taking a patient's sexual history.
- The following questions can be used:
- “Are you currently sexually active? If no, have you ever been sexually active?”
- “In recent months, how many sex partners have you had? In the past 12 months, how many sex partners have you had?”
- “Are your sex partners men, women, or both?”: If a patient answers “both,” repeat the first two questions for each specific gender.
-
Current/past sex practices
- It is necessary to ask about the patient's sexual practices to determine if they have risk factors for STIs, whether they need testing, and to guide a discussion regarding risk-reduction strategies.
- Example: “I am going to ask you a few questions to better understand if you are at risk for STIs. What kind of sexual contact do you usually engage in (genital/oral/anal)?”
-
Current/past contraception methods use
- This part of sexual history is particularly important since the use of barrier contraceptive methods can significantly reduce one's risk of STIs. Therefore, collecting this information can be very helpful in terms of assessing one's risk of developing an STI.
- Example: “Do you and your partner(s) practice any form of birth control?”
- If no, ask them why not.
- If yes, ask them which method of contraception they use and with what frequency.
- If the patient is sexually active, be sure to ask them if they are trying to conceive. If so, ask (how long they've been trying and) if they are experiencing any difficulties.
- Always give the patient the chance to ask questions about their sexual health including different types of contraception, their indications, contraindications, as well as the potential for STI transmission , and the benefit of using barrier contraceptive methods as an STI prophylaxis method.
-
History of STIs
- A history of STIs should cover the patient's previous diagnoses and/or treatments of STIs, the presence of recurrent symptoms, as well as past STI testing results.
- The following questions can be used:
- “Have you ever been diagnosed with an STI? When? What treatment did you receive?”
- “Have you ever been tested for HIV, or other STIs? Would you like to be tested?”
- “Has your current partner or any former partner ever been diagnosed or treated for an STI? Were you tested for the same STI(s)? If yes, when were you tested? What was the diagnosis? How was it treated?”
- History of postcoital vaginal bleeding
- History of sexual dysfunction (e.g., dyspareunia, low libido)
- History of sexual abuse
Transgender individuals receiving gender-affirming hormone therapy are still at risk of unintended pregnancy; see “Principles of transgender health care" for more information
The 5 Ps of a sexual history include Partners, Practices, Protection from STIs, Past history of STIs, and Prevention of pregnancy.
Medications and allergies
- Prescribed drugs
- Over-the-counter drugs
- Herbal remedies
- Allergies to drugs or environmental factors and reaction to each allergen
Enzyme-inducing medications like rifampicin, some antiepileptic drugs, some antiretrovirals, and St John's wort can reduce the efficacy of hormonal contraception. [1][2]
Family history
- Cancers of the reproductive system in the family (e.g., breast cancer and ovarian cancer with BRCA1/2 gene mutations)
- Endocrine disorders (e.g., diabetes mellitus, hypertension)
Social history
- Relationship status
- Socioeconomic status
- Occupation
- Drug and alcohol use
Review of systems
- See “Medical history” for more information on the complete review of systems.
- In the OB/GYN examination, a particular emphasis should be placed on the:
- Urogenital system (e.g., dysuria, hesitancy, urgency, incontinence, change in bowel habits, rectal bleeding)
- Abdomen (e.g., abdominal/pelvic pain)
- Breasts
- For post/perimenopausal woman, it is important to ask about menopausal symptoms (e.g., hot flashes/night sweats, vaginal dryness, abnormal bleeding, irritability, depression, mood changes).
If you feel that the patient is not comfortable talking about their gynecologic history, start with social/family history in order to establish rapport with the patient.
Obstetric history
Obstetric history taking varies based on the setting (normal prenatal checkup vs. patient presenting with a concern).
Past obstetric history (GTPAL system)
- Gravida: number of times the patient has conceived
-
Term pregnancies (≥ 37 weeks of gestation)
- Mode of delivery (e.g., normal spontaneous vaginal delivery/NSVD)
- Birth weight/gender of the baby
- Maternal/fetal perinatal complications
- Use of assisted reproductive therapies
- Preterm pregnancies (< 37 weeks of gestation)
- Abortions (elective or spontaneous before 20 weeks gestation )
- Living children or live births
- See “Clinical tasks” in the “Obstetrics and gynecology clerkship” article for more information on the GTPAL system.
GTPAL is an acronym used by doctors and nurses to sum up the obstetric history of a woman: Gravida, Term births, Preterm births, Abortions, Living children.
Current pregnancy
- Gestational age and expected day of delivery
- Beginning of prenatal care (e.g, use of folate, regular OB/GYN visits)
- History of teratogenic drug use
- History of maternal infectious diseases and immunization; See “Congenital TORCH infections” for more information.
- Prenatal diagnostic results (e.g., previous ultrasound findings)
- History of vaginal bleeding or fluid leakage during the current pregnancy
- Presence and frequency of fetal movement and uterine contractions
- Any other presenting complaints; See “Clinical signs of early pregnancy” in the “Pregnancy” article.
If the mother is not aware of previous perinatal complications, try asking her how soon she went home with the baby after the delivery.
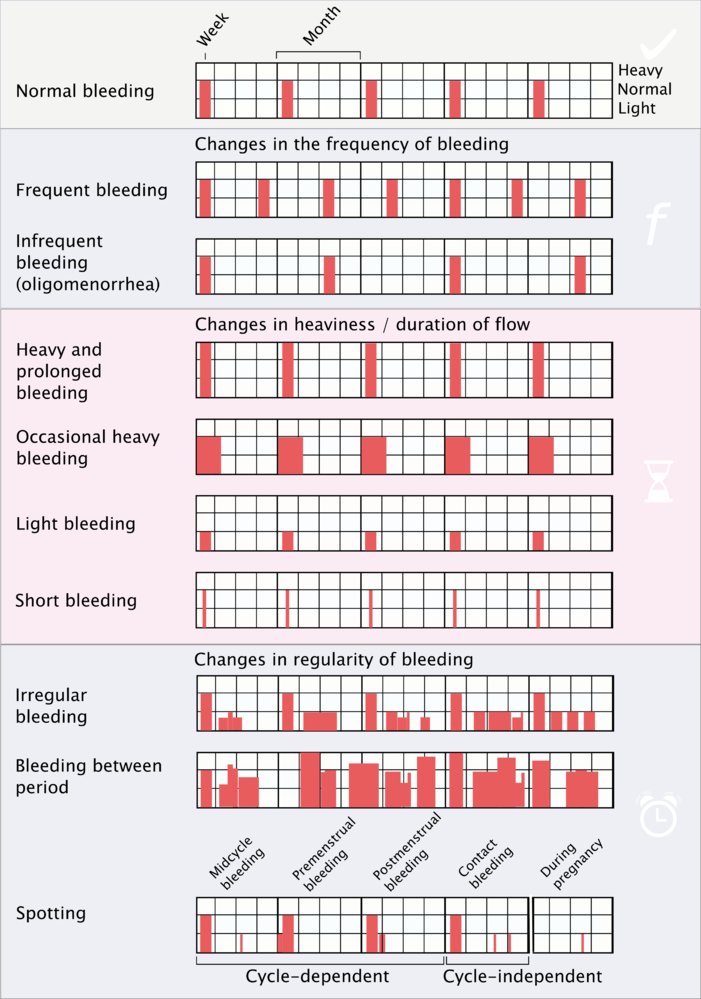
This chart provides aid for classifying the main types of menstrual irregularities based on frequency, duration, and flow of menses.
© AMBOSS
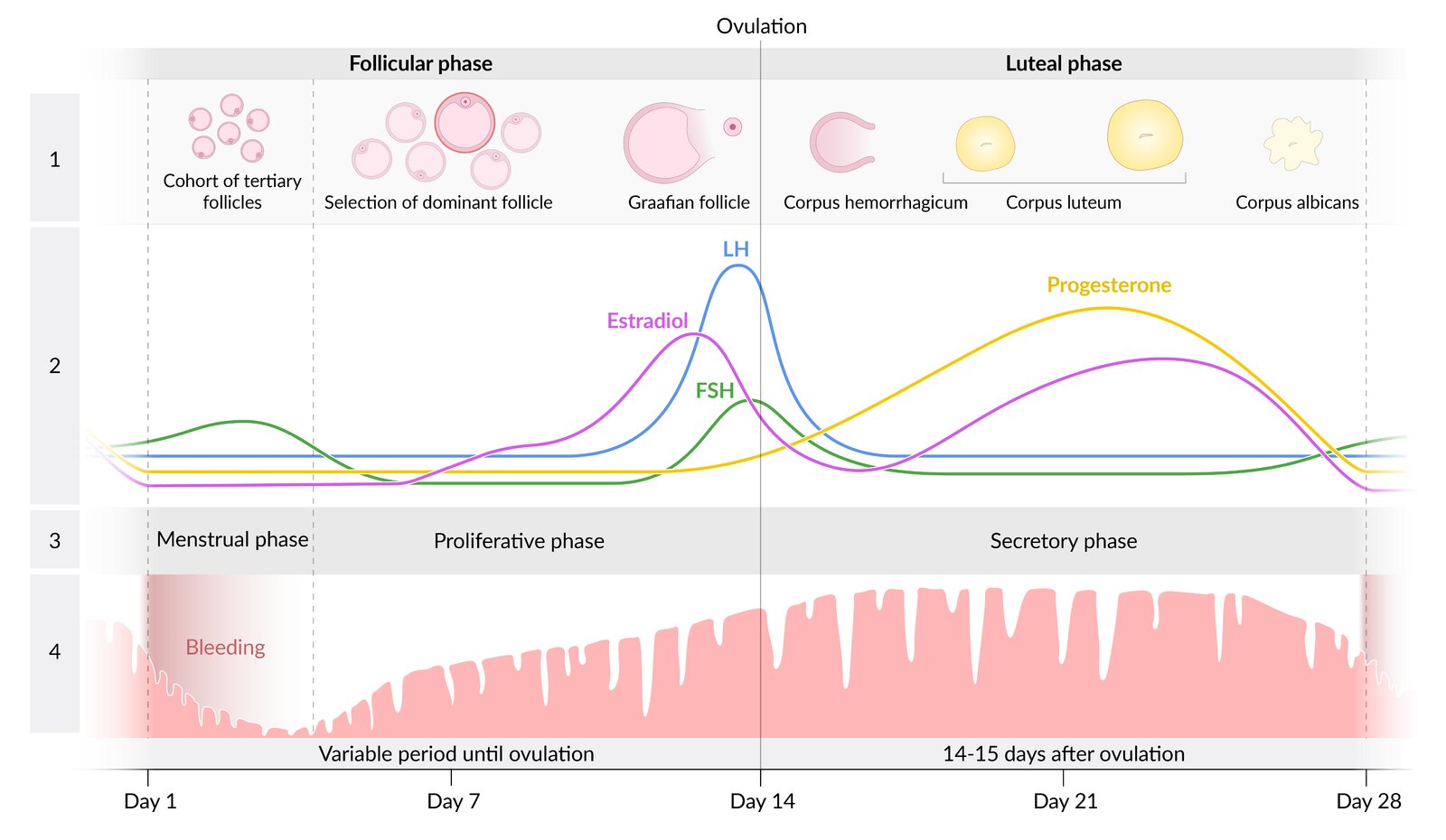
The menstrual cycle consists of two phases: the follicular and the luteal phase. The onset of menses marks the beginning of the follicular phase, which usually lasts 12–14 days but may be variable. The luteal phase begins on the day of ovulation and lasts 14 days.
During the follicular phase, FSH and LH stimulate the development of several follicles, one of which develops as the dominant follicle into the Graafian follicle. An LH surge initiates ovulation. As the oocyte reaches the fallopian tube, the ruptured follicle transforms into the corpus luteum, which produces progesterone. If no pregnancy occurs, the corpus luteum regresses and the progesterone level drops. This drop induces vasospasms in the uterine spiral arteries, ischemia, and sloughing off of the functional endometrial layer, which leads to menstrual bleeding (menstrual phase). During the proliferative phase, the endometrium is built up again in preparation for oocyte implantation during the secretory phase.
1: stages of follicle development; 2: hormone levels; 3: phases of the endometrial cycle; 4: development of the endometrium during the cycle
© AMBOSS
Gynecologic examination
Preliminary considerations
Because of the sensitive nature of this physical examination, patients are often anxious, which can further complicate the exam itself. It is important to make sure the patient feels comfortable prior to proceeding.
- Always begin by explaining the procedure, the tools being used (e.g., speculum), why the examination is being done, and what you are looking for.
- Ask the patient how they feel and give them a chance to clarify any concerns they have with you.
- Let the patient know that they are still in control throughout the process. Assure them that you will not proceed if they are in pain or distress. Asking questions such as, “Is this painful in any way?” or “Are you alright with me proceeding?” will give the patient the feeling that they can stop the process if needed and help them relax.
- Explain what a chaperone is and whether the patient would like to have one present during their examination.
- See “Physical examination” and “Diagnostic procedures in gynecology” articles for more information.
Instruments and equipment
- Gynecologic exam: gloves, lubricant, vaginal speculum, cervicovaginal swab, paper towels
- Obstetric exam: measuring tape, Pinard stethoscope or doppler transducer, ultrasound gel, paper towels

Breast examination [3][4]
Preparation
- Before proceeding to breast examination, ask the patient what part of the menstrual cycle they are currently in.
- Ask the patient about any specific concerns (e.g., detected mass during breast self-examination).
- After explaining the details of the procedure and obtaining the patient's verbal consent, invite the patient to get undressed.
- The patient should be sitting upright during the examination.
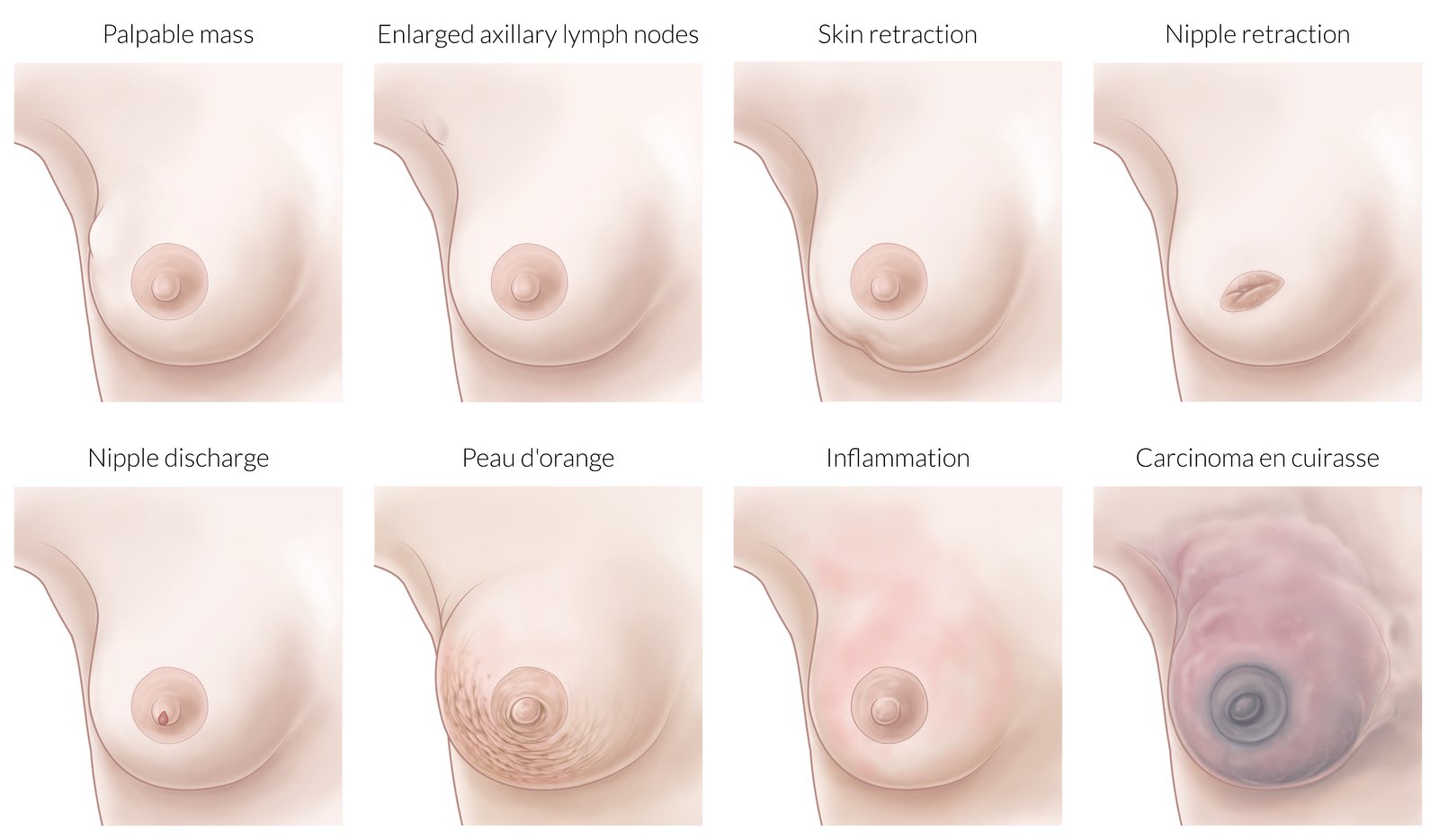
Breast inspection
- Evaluate the breasts' symmetry and shape (e.g., swelling, breast masses).
- Check for any changes in skin color or texture (e.g., redness, peau d'orange, mamillary eczema, ulcerations).
- Evaluate the presence of nipple discharge.





Breast palpation
- The dominant hand should be used for palpation while the other hand provides support.
- A thorough tactile evaluation can be achieved with the following:
- Circular movements starting at the nipple and moving towards the periphery or vice-versa
- Vertical palpation of linear segments
- Palpation of each of the four breast quadrants
- Apply light pressure at first to scan for superficial changes and then proceed to deeper palpation of each of the breasts.
- Gently squeeze the sides of the nipple to detect the presence of any discharge.
Even though breast self-examination is not the most accurate tool for breast cancer screening, it still remains an important tool for breast health promotion and disease prevention in women [5].


Lymph node palpation
- The palpation of the regional lymph nodes should be performed in the following three positions:
- The patient lets their arms hang loosely at their sides.
- The patient rests their hands on the hips.
- The patient crosses their arms behind the head.
- The following lymph nodes should be evaluated for size, tenderness, mobility, and firmness:
- Axillary nodes (most common site of lymphatic spread from breast cancer)
- Infraclavicular and supraclavicular nodes

Pelvic exam [6]


Preparation
- After explaining the details of the procedure and obtaining the patient's verbal consent, ask the patient to empty their bladder.
- Allow the patient to remove all clothes and underwear below the waist in privacy, and provide sheets for cover if necessary.
- Ask the patient to lay back in the lithotomy position on the examination chair.
- Ensure that all the equipment and instruments used during the procedure are warmed.
External genital exam
- Check the vulva for any abnormalities (e.g., swelling, irritation, ulcers, warts).
- Examine the skin for the presence of scars, discoloration, and hair distribution.
- Inspect the vaginal introitus for discharge or swelling.
- Ask the patient to perform the Valsalva maneuver and examine the vaginal introitus for organ prolapse or urinary incontinence.
- Palpate the labia majora for any masses or tenderness.




Bimanual pelvic exam
- Lubricate the index and middle fingers of one hand and slowly insert them into the vaginal canal.
- Use the other hand to simultaneously palpate the abdomen.
- This procedure allows for palpation of both the uterus and adnexa (e.g., their localization, size, tenderness during manipulation, presence of masses).

Rectovaginal pelvic exam [7]
- Lubricate the index and middle fingers of one hand and slowly insert them into the vaginal canal and rectum respectively.
- Use the other hand to push the uterus posteriorly by pressing on the anterior abdominal wall.
- This procedure allows for the palpation of the rectovaginal septum, cul-de-sac tenderness, or masses.
- The rectovaginal exam is usually reserved for patients with suspected pelvic masses (e.g., colorectal cancer).

Sterile speculum exam[8]
- Before proceeding to the speculum exam, remind the patient about the procedure and ensure they are comfortable before beginning.
- Choose the appropriately sized speculum and lubricate it. [9]
- Separate the labia majora with the index and middle fingers and gently introduce the speculum inside the vaginal canal with the blades facing down and the handle pointing to the side.
- After fully advancing the speculum, carefully rotate it to 90° so that the blades are in a horizontal position, with the handle pointing down.
- Only after the speculum has been placed in its final position, remove the fingers and slowly open the speculum.
- Lock the screws on the speculum after getting a good visualization of the cervix.
- Inspect the cervix and the cervical os for the following:
- Position (e.g., anteriorly displaced cervix in a patient with a retroverted uterus)
- Color (e.g., ectocervical reddening due to the development of cervical ectropion )
- Abnormal discharge (e.g., mucopurulent discharge in gonococcal cervicitis)
- Erosions and ulcerations (e.g., HSV infection)
- Hemorrhages (e.g., strawberry cervix in trichomoniasis)
- Cervical masses (e.g., polyps, cervical cancer)
- Take a cervical swab/Pap smear if necessary.
- Loosen the screws, close the speculum partially , and slowly return it to its original position at insertion (i.e., with the blades facing down and the handle pointing to the side). [9]
- Carefully extract the speculum and inspect the vaginal introitus.
If the view of the cervix is obscured during a speculum exam by prolapse of the vaginal walls, a condom with the tip cut off may be rolled over the speculum to help keep them retracted while the speculum is open. [9]






")
After the procedure
- Inform the patient that the procedure is over and allow them to get dressed in privacy.
- Provide paper towels to the patient if needed.
- Dispose of the used equipment and wash your hands.
- Summarize and discuss the results of the exam with the patient.
Ask the patient to empty their bladder before proceeding to the pelvic exam.
Do not open the speculum until it has been fully inserted in the vaginal canal and placed in its final position. Do not extract the speculum in its fully open position.

The Cusco speculum is a self-retaining speculum used to examine the vagina and cervix and to obtain smears for microbiological or histological examination. The lubricated speculum is inserted into the vagina in a closed position. The speculum retracts the anterior and posterior vaginal walls and can be fixed in an open position with the help of the screws on the handle, avoiding the need for an assistant to complete the examination. The speculum is partially extracted in the open position to avoid injury to the cervix.
Source: “Speculum en métal” by Ceridwen, Wikimedia Commons, licensed under CC BY-SA 2.0.
{kind=link}
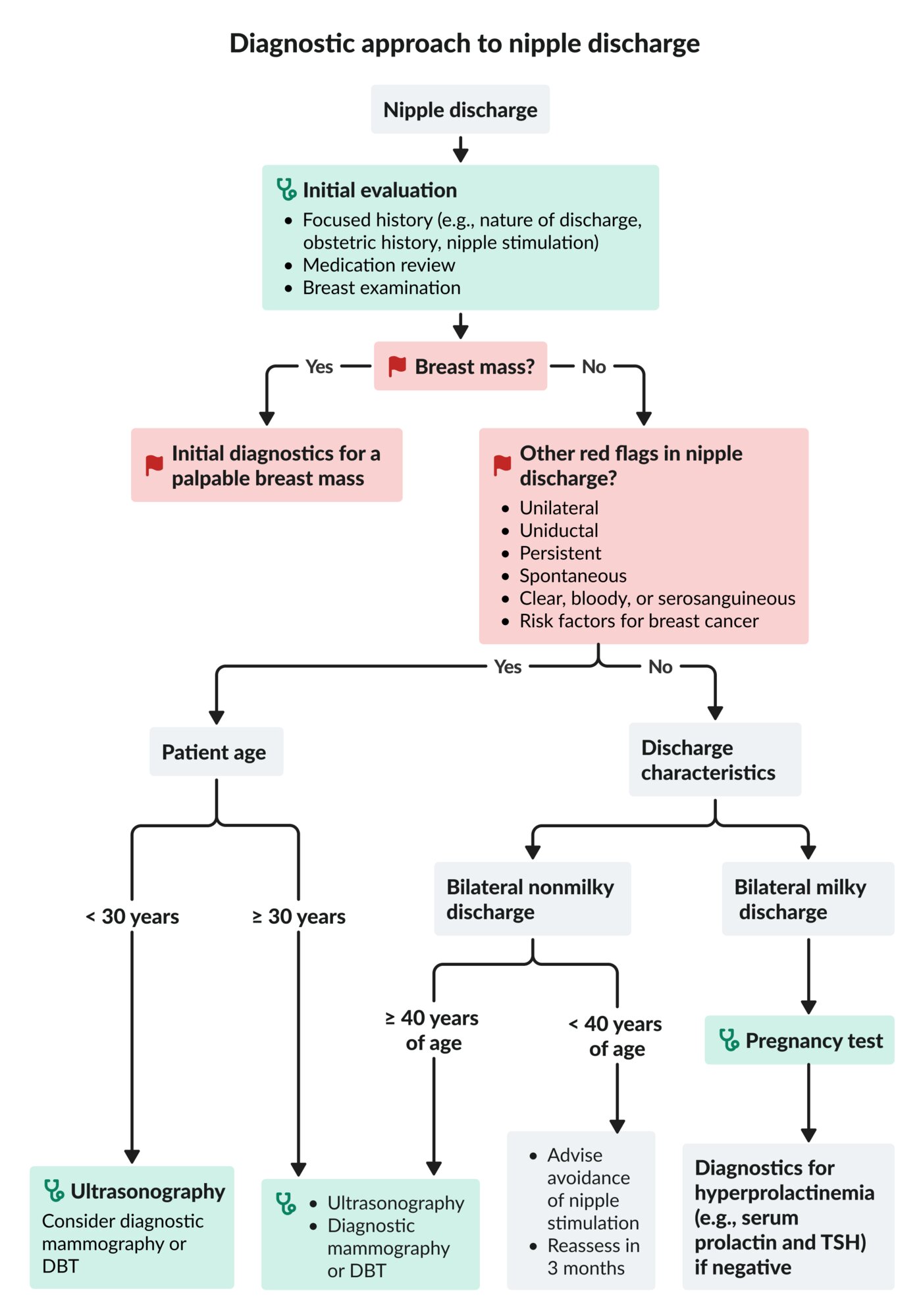
DBT: digital breast tomosynthesis
TSH: thyroid-stimulating hormone
© AMBOSS

The right breast is swollen and shows diffuse erythema that extends over most of its surface. Conspicuous hair follicles produce the typical orange peel appearance (peau d'orange). The nipple is also markedly retracted.
Edematous swelling, orange peel appearance, and nipple retraction are all caused by blockage of lymphatic channels. The swelling and erythema distinguish inflammatory breast cancer from locally advanced breast cancer.
Source: “Figure 1. in: What is inflammatory breast cancer? Revisiting the case definition.” by Paul H. Levine, Ladan Zolfaghari, Heather Young, Muhannad Hafi, Timothy Cannon, Chitra Ganesan, Carmela Veneroso, Rachel Brem and Mark Sherman, MDPI, licensed under CC BY 3.0.

Extensive, sharply demarcated erythema can be seen on the left breast. Cracked skin at the lower edge of the areola is also visible.
Source: © IMPP

An erythematous, scaling rash with irregular borders and erosion of the nipple is visible on the left breast of a female patient. The pathology extends beyond the areola region.
These findings are typical of Paget's disease of the breast, a rare type of ductal carcinoma that is often accompanied by nipple discharge. Age-appropriate imaging and biopsy are required for diagnosis.
Source: “Figure 1a, in: Paget’s disease of the breast: clinical, imaging and pathologic findings: a review of 16 patients” by M. Muttarak, B. Siriya, P. Kongmebhol et al., Biomedical Imaging and Intervention Journal, licensed under CC BY-SA 3.0. Further notes: Original publication available at: https://web.archive.org/web/20120905132437/http://www.biij.org/2011/2/e16/e16.pdf
© AMBOSS
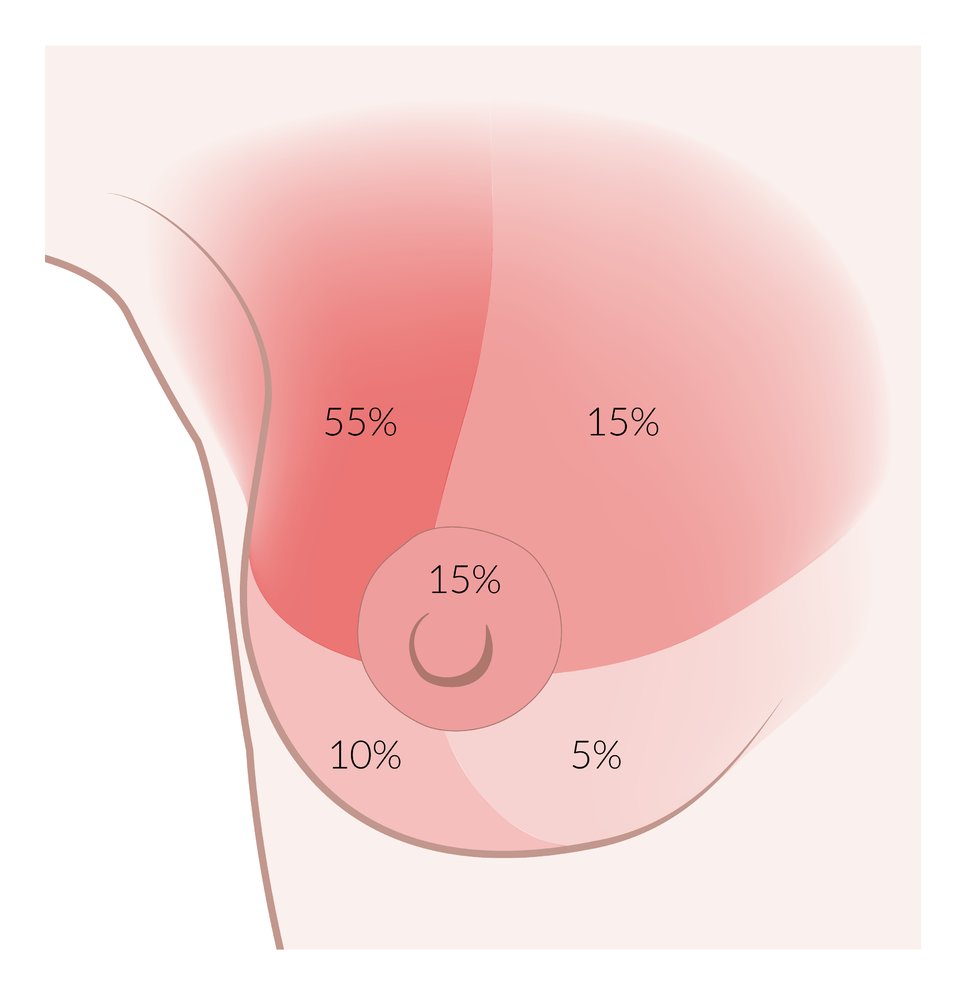
∼ 55%: upper outer quadrant
∼ 10–15%: upper inner quadrant
∼ 10–15%: nipple
∼ 10–15%: lower outer quadrant
∼ 5%: lower inner quadrant
© AMBOSS
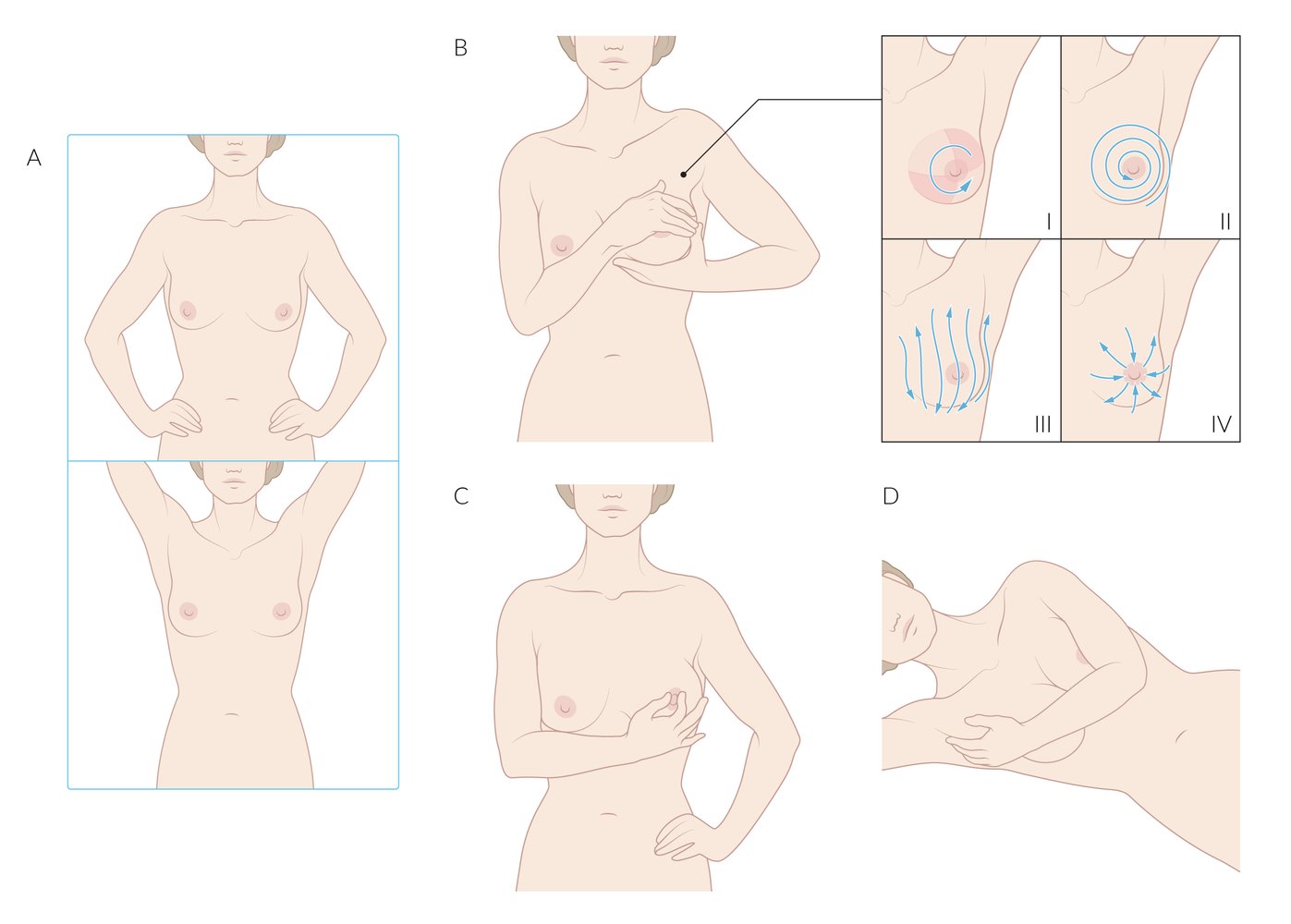
Breast self-examination (BSE) is a screening method for breast abnormalities (primarily signs of breast cancer) that involves the following technique:
A) Inspection: Look at the breasts directly in a mirror, with the arms at the sides, then raised above the head. Inspect the shape of each breast and look for changes in skin texture (e.g., dimpling, puckering, orange peel texture).
B) Palpation of the breast tissue using one of the four patterns depicted to cover all breast tissue
C) Palpation of the nipple: Squeeze the nipple gently and inspect for discharge (milky or bloody).
D) Palpation of axillary breast tissue: While standing or lying down, palpate the axillary tail of the breast, which extends into the axilla.
Note: The efficacy of routine BSE is still the subject of ongoing debate and, as such, is no longer recommended. Various studies have shown that it does not help reduce deaths from breast cancer but does lead to higher rates of biopsies of benign masses (unnecessary surgical biopsies). However, these studies have been criticized for employing inadequate BSE techniques and thereby introducing bias. In addition, many women continue to regard BSE as an important part of their health maintenance.
© AMBOSS
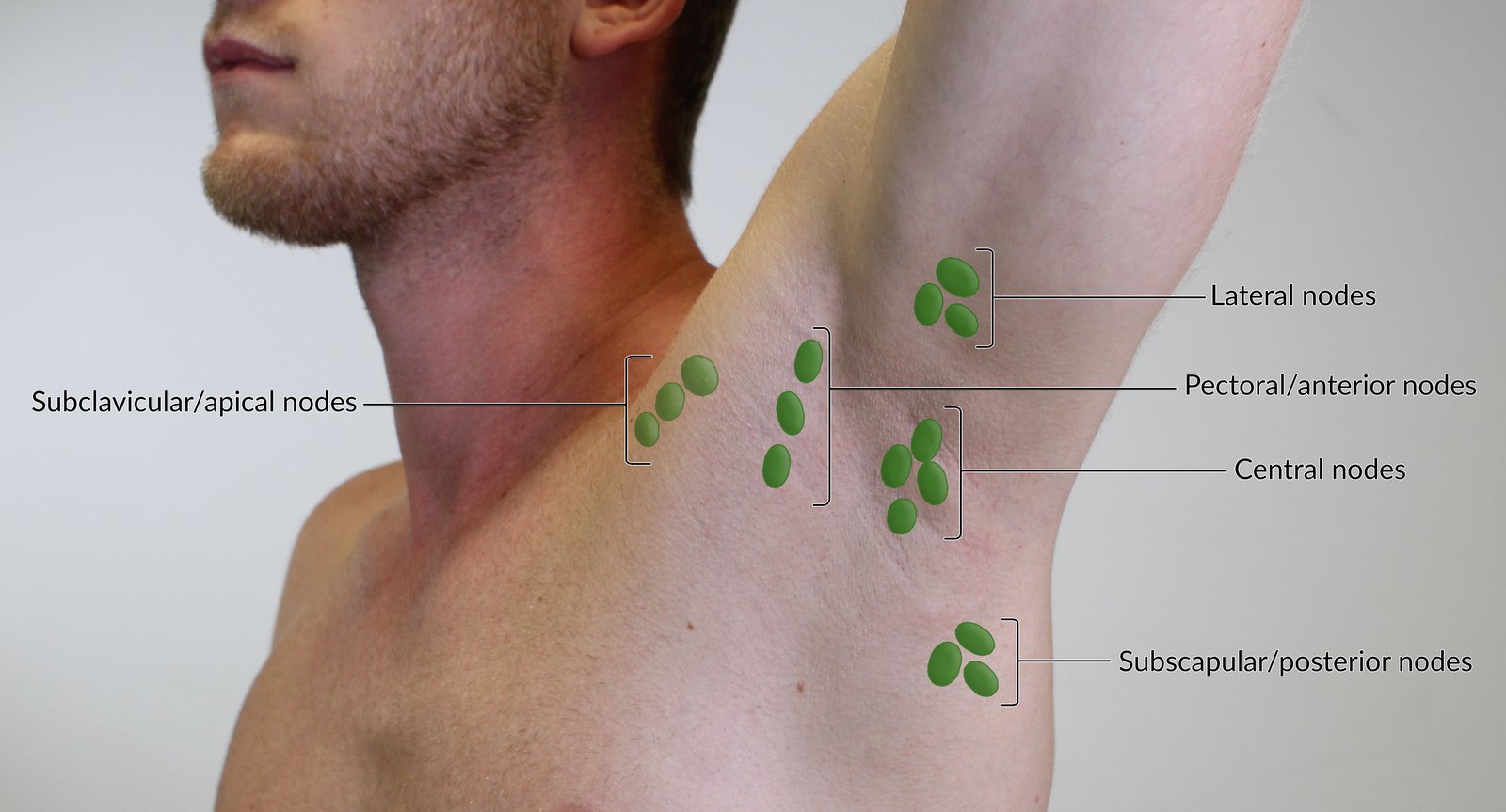
The lateral nodes drain most of the arm and shoulder and are palpable near the proximal humerus. The pectoral or anterior nodes drain the thoracic wall and parts of the thorax and are palpable in the anterior axillary line. The subscapular or posterior nodes drain the posterior thoracic wall and parts of the arm and are palpable in the posterior axillary line.
All these lymph nodes drain into the central nodes, which are palpable at the base of the axilla. Before entering the venous system, lymph from the central nodes passes through the subclavicular or apical nodes before entering the venous system. Therefore, these nodes should also be palpated in the examination.
For educational purposes, the lymph nodes are depicted enlarged.
© AMBOSS
© AMBOSS
© AMBOSS

An irregular, sclerotic white plaque with a reddened, inflammatory edge localized to the vulva and perianal region is visible. The labia minora and majora are hard to distinguish from one another because of atrophy and sclerosis; the vaginal opening is markedly narrowed.
Source: "ID#: 15553", Susan Lindsley, Centers for Disease Control and Prevention (CDC) licensed under Public Domain

Purulent discharge can be seen on this patient's vulva on external genital examination.
Source: “SOA-gonorroe-female” by SOA-AIDS Amsterdam, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

The cervix can be seen visibly protruding out of the vaginal introitus of this older postmenopausal patient. Note that the labia are thin and atrophic, a normal postmenopausal change.
Source: "Uterine_prolapse", Mikael Häggström, Wikimedia Commons licensed under Public Domain
{kind=link}

Vaginal introitus of a woman presenting with painless swelling of her right labia
There is a small fluid-filled cyst visible as a translucent gray mass at the posterolateral aspect (8 o'clock position) of the vaginal introitus, distending the right labia minora. There are no signs of inflammation.
Source: “Bartholincyst2011” by Medimage, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
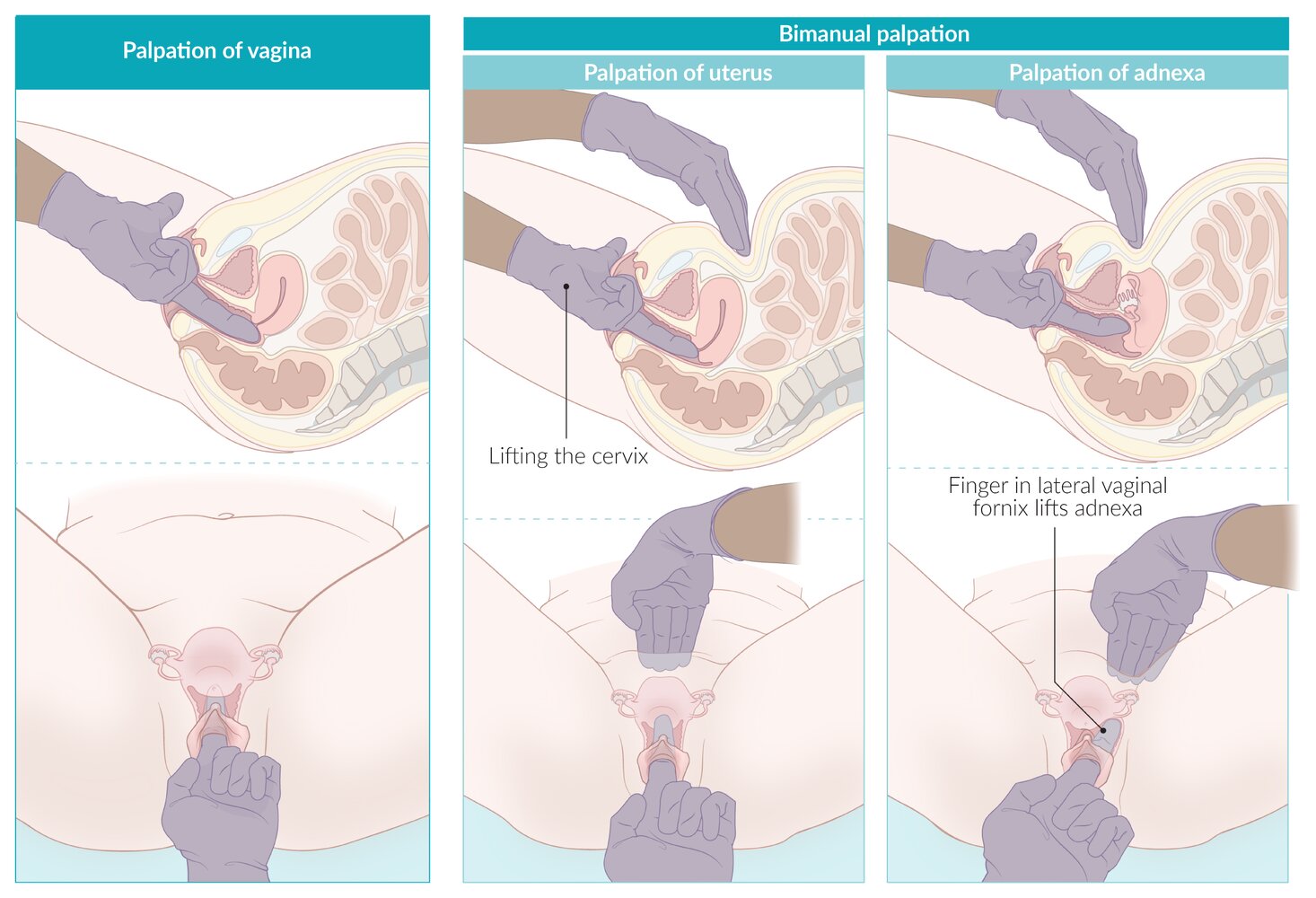
– Lubricate the index and middle fingers (or the index finger only if more size-appropriate) of one hand and slowly insert them into the vaginal canal. Place the other hand on the patient's abdomen for external pelvic palpation.
– With the inserted fingers, palpate the vaginal walls for any irregularities or masses (asking the patient to strain can make a uterine prolapse, cystocele, or rectocele more pronounced) and assess position, consistency and any tenderness of the cervix.
– Palpate the uterus bimanually, using the inserted fingers on the cervix to lift the uterus toward the abdominal examining hand. Assess uterine position, size, consistency, mobility, and any tenderness.
– Palpate the adnexa bimanually, placing the inserted fingers into each lateral vaginal fornix in turn and lifting upwards toward the abdominal examining hand, assessing for masses or tenderness. Note that the normal adnexa are frequently impalpable.
© AMBOSS
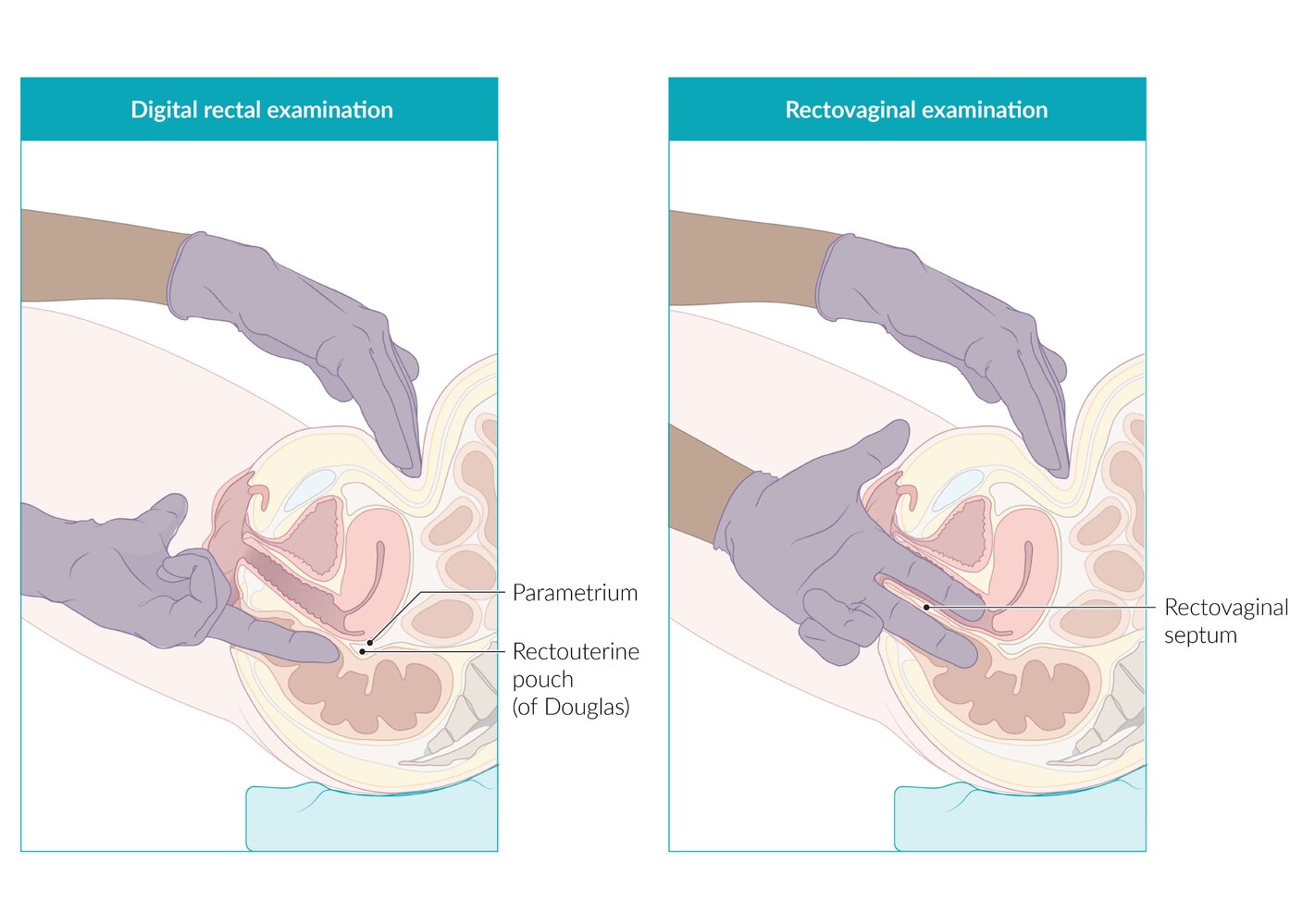
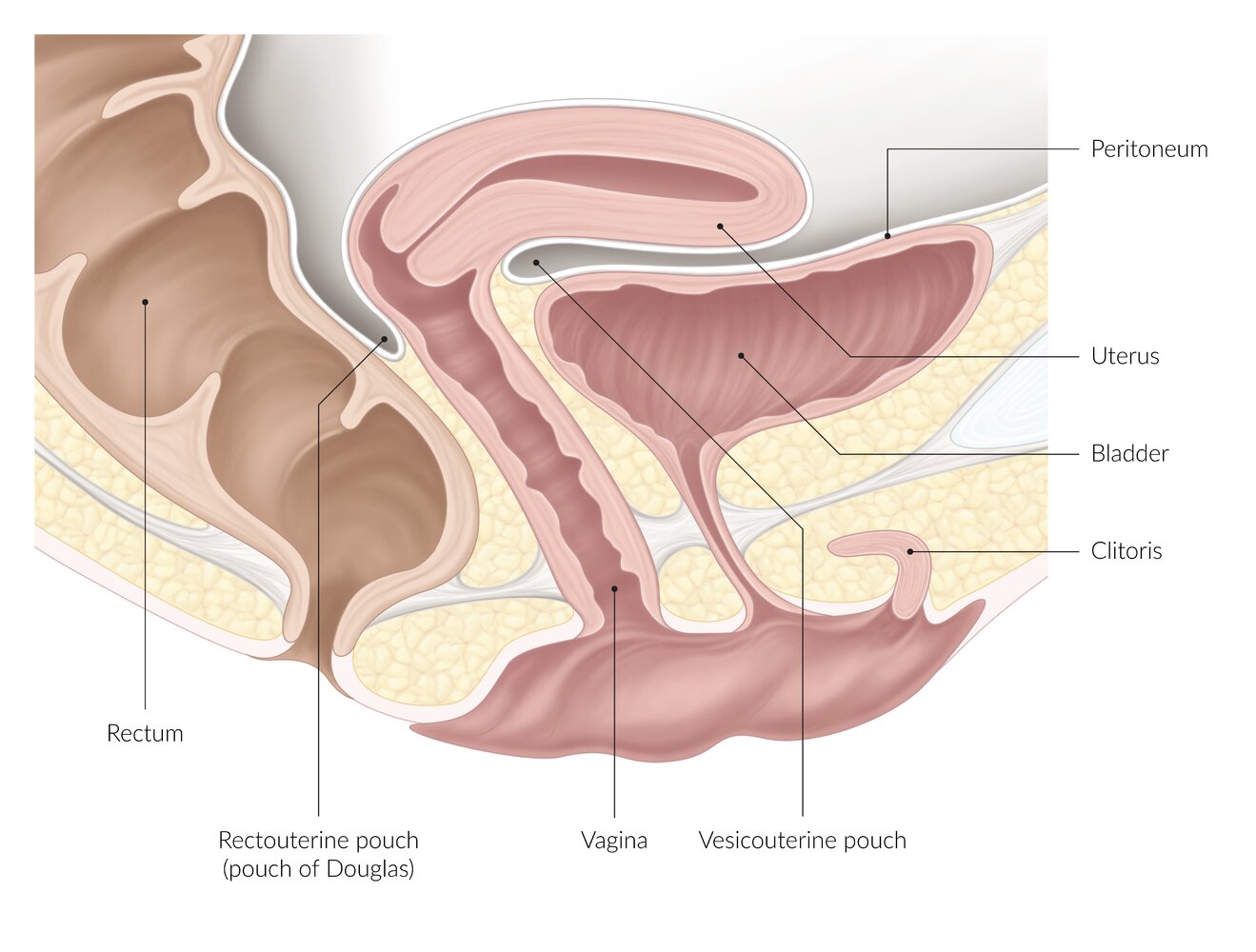
Bimanual rectovaginal examination is helpful in evaluating the rectouterine pouch (pouch of Douglas), rectovaginal septum, and adnexa:
– Lubricate the index and middle fingers of one hand and slowly insert them into the vagina and rectum. Ask the patient to bear down while inserting the fingers.
– Press on the anterior abdominal wall with the other hand to push the uterus posteriorly; use the fingers in the vagina and rectum to palpate for tenderness or masses.
Bimanual digital rectal examination can be used instead of the vaginal bimanual examination if the latter is contraindicated (rectal examination alone is less accurate), or as an additional examination, e.g., for pathologies in the rectouterine pouch (pouch of Douglas):
– Lubricate the index finger of one hand and slowly insert it into the rectum. Palpate the rectum, pelvic walls, uterus, and adnexa between the inserted finger and the hand examining the abdomen.
© AMBOSS
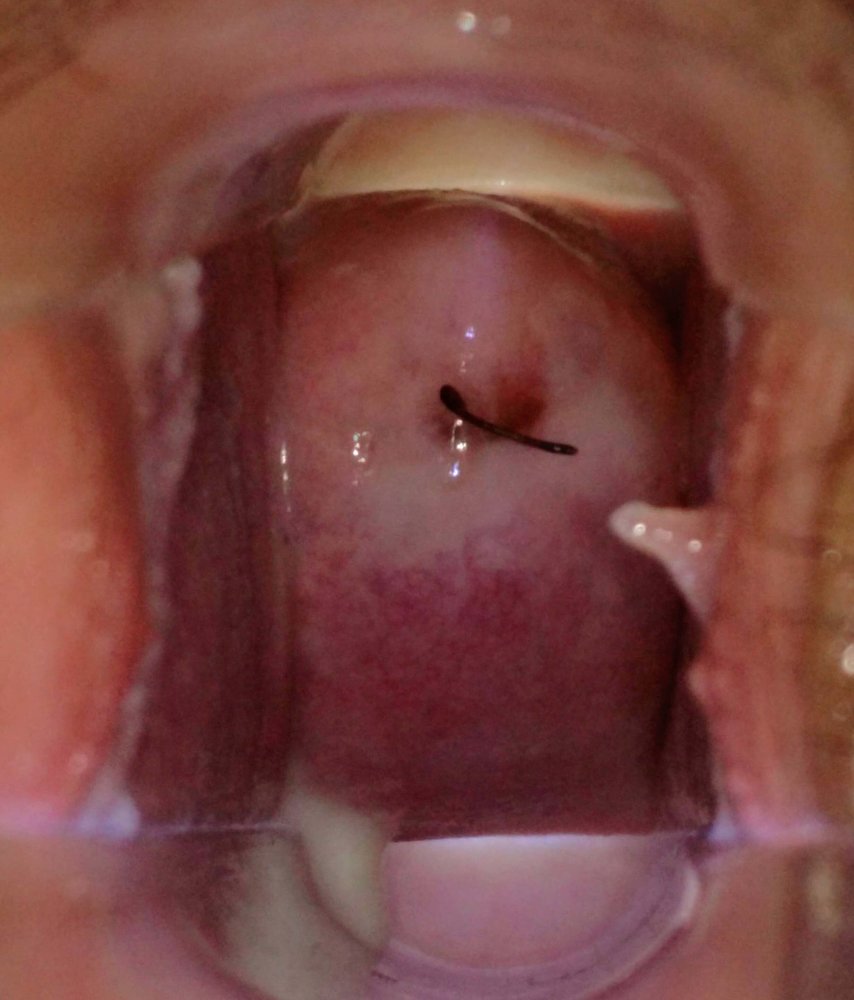
Speculum view
The fornix and cervix appear unremarkable. The black strings noted at the cervical os are the strings of an intrauterine device (IUD). Physiologic, milky-white vaginal discharge pooled in the vaginal fornix (leukorrhea) is also seen.
Source: “Normal cervix and vaginal discharge” by VeeBabzel, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}
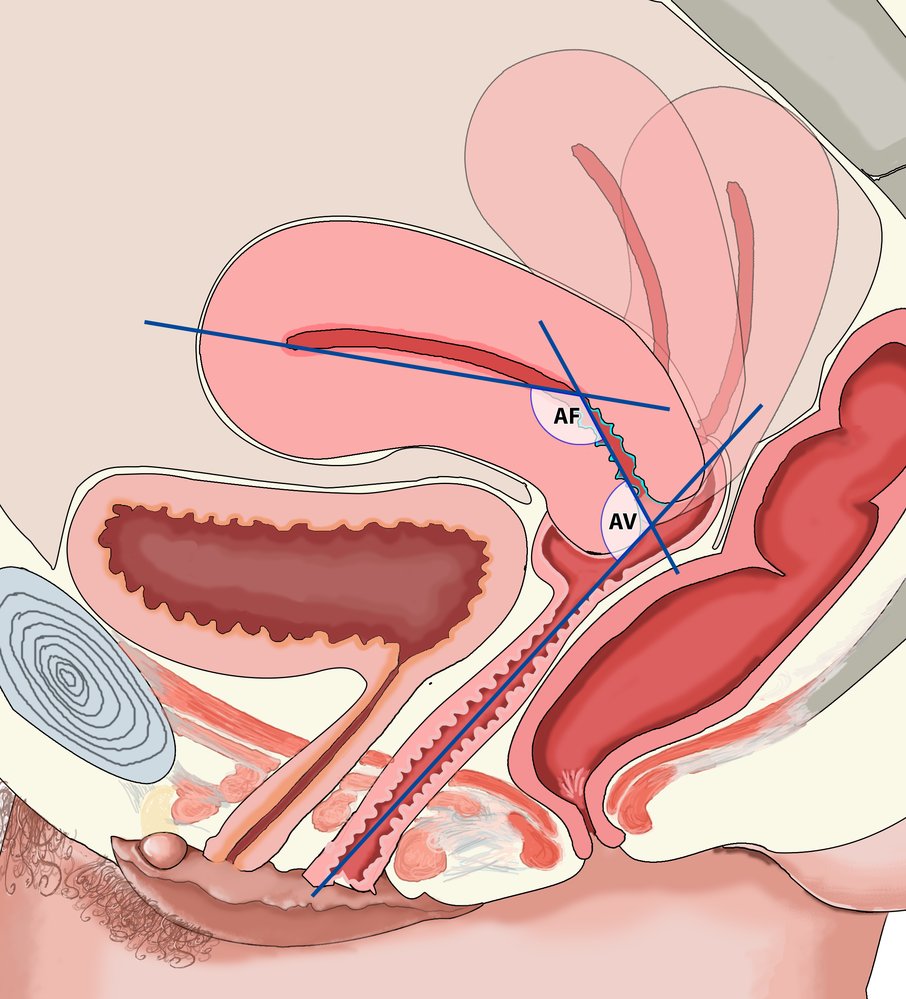
The uterus is usually anteverted by 90° and anteflexed by 120°:
- Version is the angle between the long axis of the cervix and the long axis of the vagina (AV).
- Flexion is the angle between the long axis of the body and the long axis of the cervix (AF).
- Retroflexion, which is also shown here, is a physiological variation.
© AMBOSS
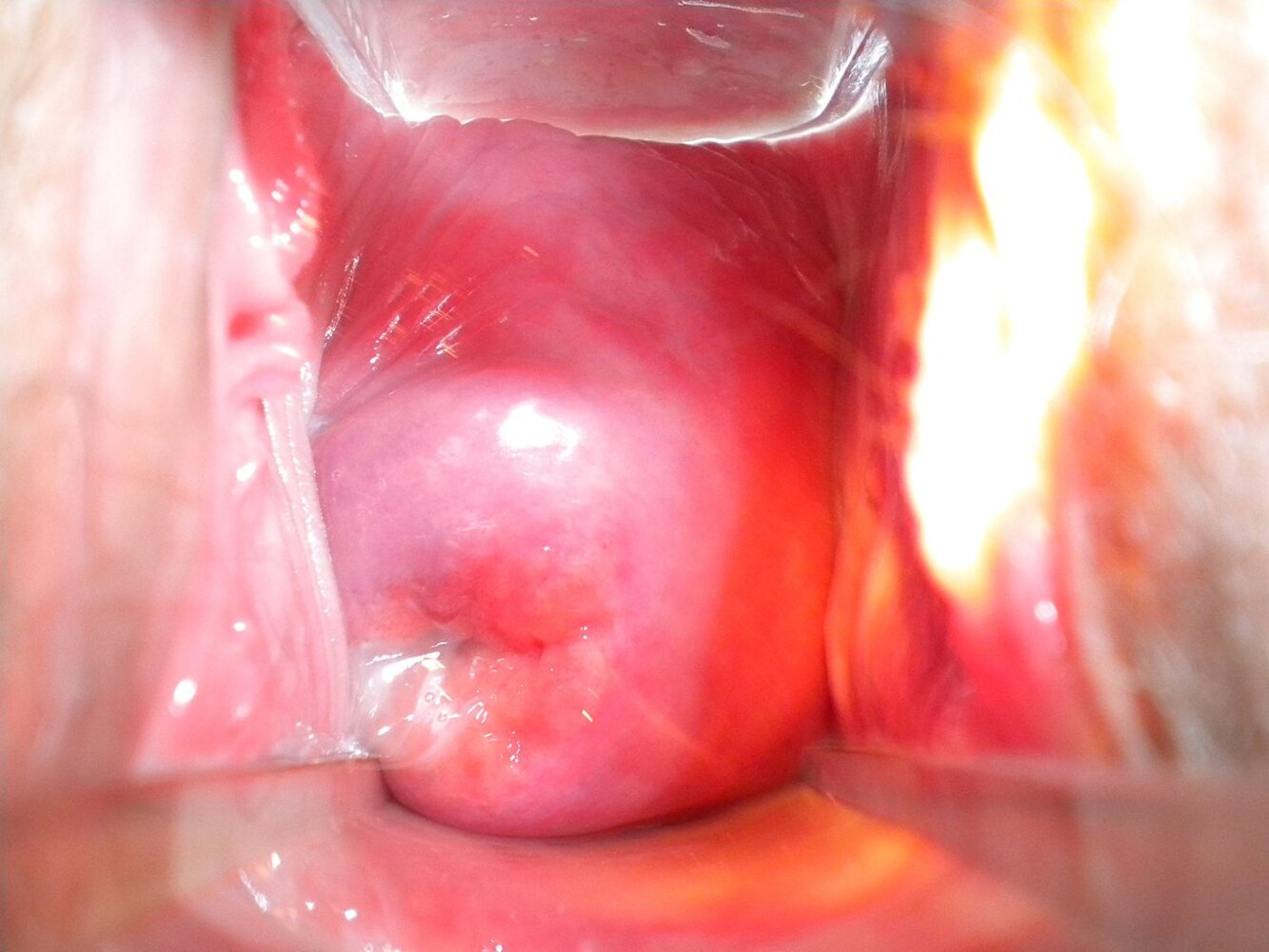
Speculum view of the cervix
- The external os of the cervix is visible as a transverse slit (indicating that this patient has had a previous vaginal delivery).
- The reddish mucosa surrounding the os is the endocervix (green overlay), which is lined with columnar epithelium.
- The pale pink mucosa surrounding the endocervix is the ectocervix (blue overlay), which is lined with nonkeratinizing squamous epithelium.
- The junction of the pink and red mucosa is known as the squamocolumnar junction (SCJ) and is usually located at the border of the external os.
- Vaginal secretions can be seen in the lower left area of the cervix.
This eversion of the endocervix onto the ectocervix is known as cervical ectropion (cervical erosion). It is a physiological response of the cervical mucosa to estrogen and is seen in pregnancy, women taking OCPs, and during the ovulatory phase of the menstrual cycle.
Source: "Cervix uteri, breastfeeding woman after 2 births.jpg", Ep11904, Wikimedia commons licensed under Public Domain
{kind=link}
The surface of the cervix is covered with yellowish-white, purulent discharge. The external os of the uterus is inflamed and red.
These findings are consistent with gonorrhea.
Source: "ID#: 4087", CDC, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
© AMBOSS
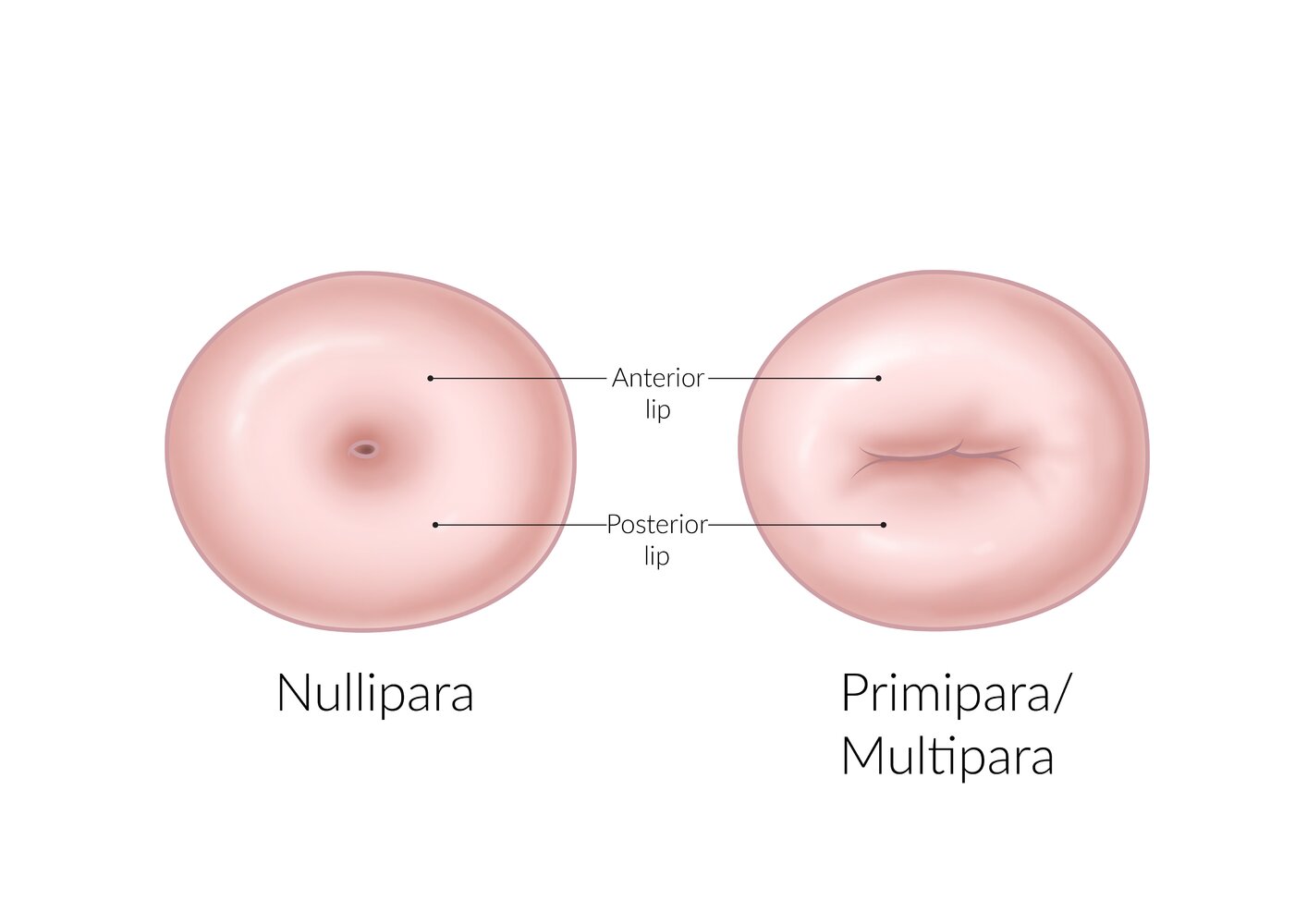
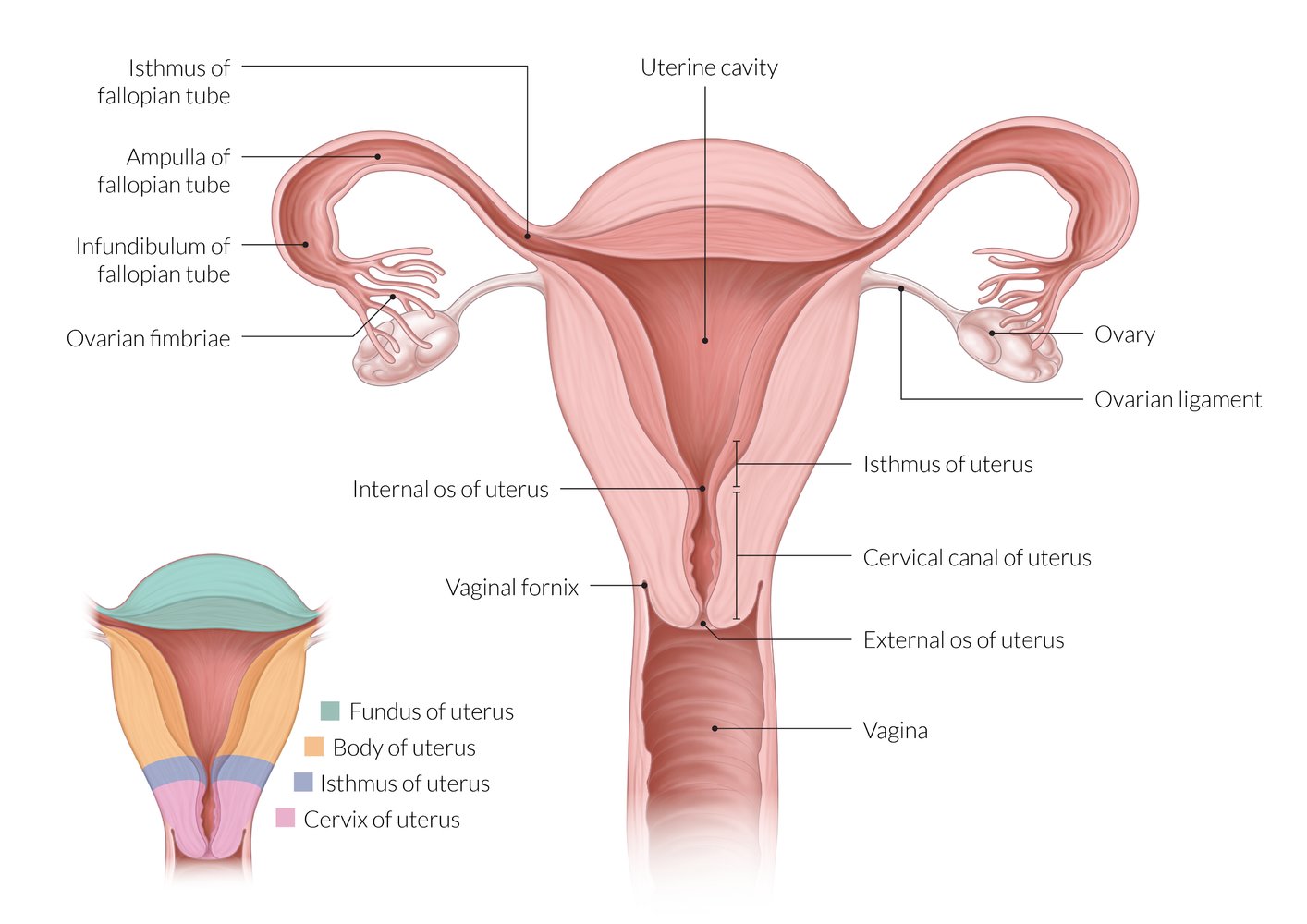
In nulliparous women, the external os of the cervix is a circular aperture. After childbirth, the external os becomes a transverse slit.
© AMBOSS

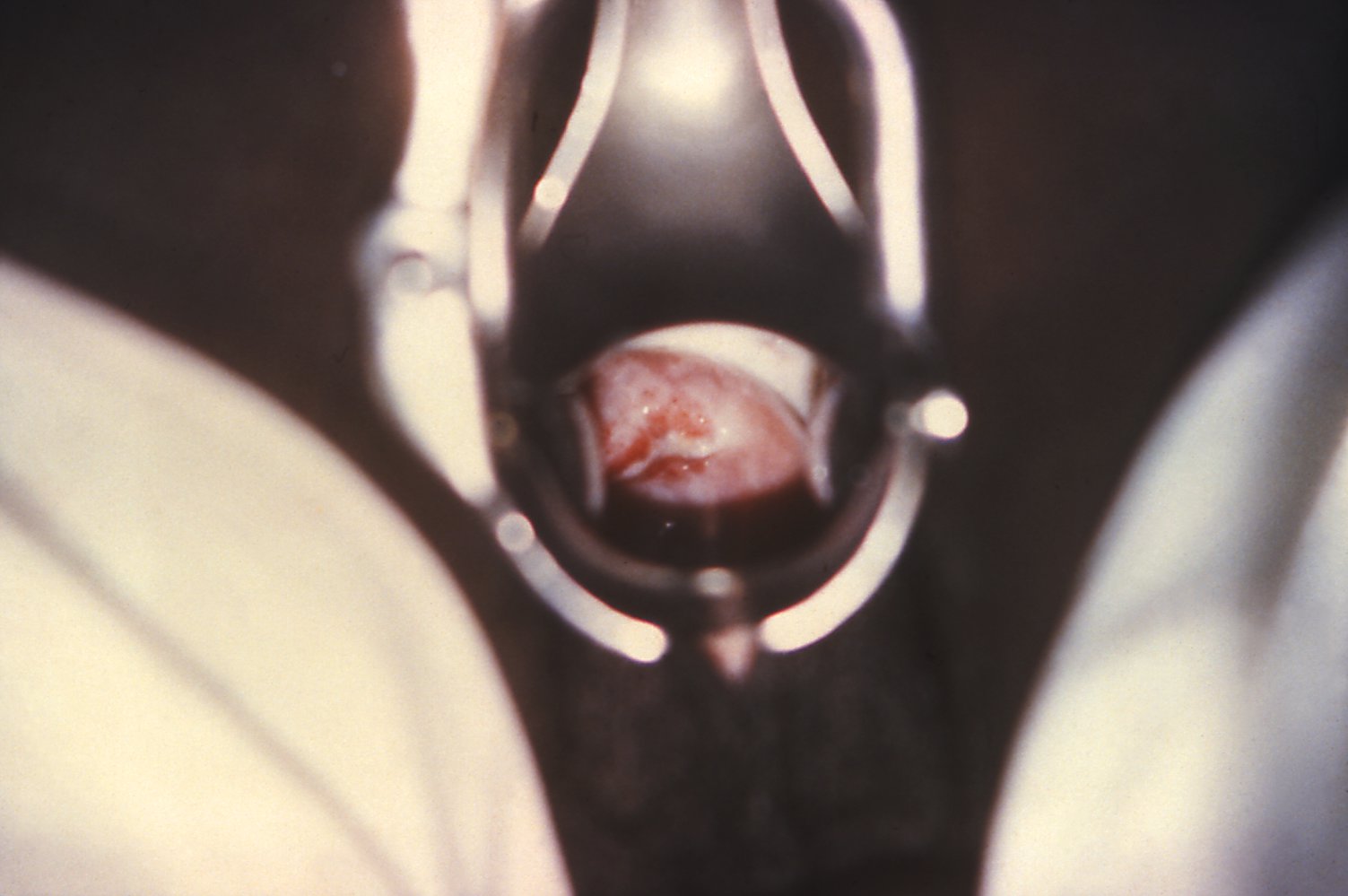
Colposcopy with application of acetic acid
The external os of the cervix is circular and the mucosa is smooth and pale pink.
These findings are characteristic of a normal ectocervix in a nulliparous woman.
Source: “Fig. 1, in: VIA and Challenges of a Single Visit Approach in Malawi” by Haeok Lee, Mary Sue Makin, Jasintha T Mtengezo, and Address Malata, Published in clinmed - international library, licensed under CC BY 4.0.
Obstetric examination
See “Prenatal care” and “Childbirth” for more information.
References
- Dhanjal MK. "Contraception in women with medical problems". Obstet Med. 1(2). :78-87. (2008)
- Thurman AR, Anderson S, Doncel GF. "Effects of hormonal contraception on antiretroviral drug metabolism, pharmacokinetics and pharmacodynamics". Am J Reprod Immunol. 71(6). :523-30. (2014)
- "The Breast Exam". https://stanfordmedicine25.stanford.edu/the25/BreastExam.html
- "Examination of Breast: Palpation". http://www.meddean.luc.edu/lumen/meded/medicine/pulmonar/pd/pstep31.htm
- Armin J, Torres CH, Vivian J, Vergara C, Shaw SJ. "Breast self-examination beliefs and practices, ethnicity, and health literacy: Implications for health education to reduce disparities". Health Educ J. 73(3). :274-284. (2013)
- "The Pelvic Exam". https://stanfordmedicine25.stanford.edu/the25/PelvicExam.html
- Bates CK, Carroll N, Potter J. "The Challenging Pelvic Examination". Journal of General Internal Medicine. 26(6). :651-657. (2011)
- Secor RM, DNP RM, FNP-BC RM, et al. "Fast Facts About the Gynecologic Exam". Springer Publishing Company. (2017). ISBN: 9780826196095
- "Cervix: Speculum exam". http://www.meddean.luc.edu/lumen/meded/medicine/pulmonar/pd/pstep68.htm