Summary
Osteoarthritis of the hip and knee is characterized by joint degeneration, which can lead to functional impairment. Although the exact etiology is unknown, risk factors include older age, overuse of the joint, obesity, previous injuries, and asymmetrically stressed joints. Patients often present with joint stiffness and pain, which can progress to severe pain and functional limitation. Osteoarthritis is a clinical diagnosis, supported by radiological findings. Initial management includes nonpharmacological measures such as weight loss, physical therapy, and the use of assistive devices (e.g., canes, braces), and short-term pharmacotherapy for pain management. If conservative measures do not improve the patient's quality of life and joint destruction is severe, surgical procedures such as arthroplasty may be indicated.
For more general information on osteoarthritis, see the respective article.
Epidemiology
The risk of developing hip and knee osteoarthritis increases with age. [1][2]
- Age: Peak incidence at initial diagnosis is 50–60 years of age.
- Sex: ♀ > ♂, especially in patients older than 50 years
Osteoarthritis is the most common disease of the hip joint in adults.
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- See “Etiology” in osteoarthritis. [3]
- Primary osteoarthritis: idiopathic
-
Secondary osteoarthritis
- Hip osteoarthritis due to Legg-Calvé-Perthes disease, slipped capital femoral epiphysis, developmental dysplasia of the hip, hemochromatosis, gout, stiffened ipsilateral knee joint
- Knee osteoarthritis due to genu valgum, genu varum, cruciate ligament rupture, meniscal tear
Clinical features
See also "Clinical features of osteoarthritis.” [4]
-
Hip osteoarthritis
- Pain in the groin area and above the greater trochanter
- Increased contracture in the flexor, external rotation, and adduction position → antalgic gait
- Early signs: limited and painful internal rotation of the hip joint
- Pain on palpation: greater trochanter, groin
- Positive Thomas test
- Function: test for hip flexion contracture
- Position: supine
- Procedure: Examiner passively flexes the hip joint opposite to the affected side to a maximum to compensate lumbar lordosis.
- Positive test: If flexion contracture is present, the ipsilateral leg will simultaneously flex independently as a reflex.
-
Knee osteoarthritis
- Function-limiting knee pain
- Knee swelling which increases on activity
- Mechanical instability, locking, catching sensation
- In case of patello-femoral osteoarthritis: positive Patellar grind test (pain on movement of the patella)
- Cartilage damage usually begins medially and may lead to genu varum (bowing of legs)
Walking downhill is painful with knee osteoarthritis, whereas walking uphill is painful with hip osteoarthritis!
Diagnosis
Osteoarthritis is a clinical diagnosis. Diagnostic studies may be indicated if there is clinical uncertainty or to exclude alternative diagnoses (see “Diagnosis of osteoarthritis” and “Differential diagnoses of inflammatory arthritis”). [5]
Plain radiography [5]
-
Patient position: Obtain multiple views (e.g., anteroposterior, lateral) of the affected joints, if possible. [6]
- Hip: Patient may be weight-bearing or non-weight-bearing.
- Knee: Patient should be standing.
-
Supportive findings
- Radiological signs of osteoarthritis [5]
- Standing views of the knee may show: [6]
- Joint space narrowing
- Uneven pressure distribution: e.g., patella lateralization, genu valgum, genu varum
X-rays may appear normal in the early stages of osteoarthritis. The absence of radiological signs of osteoarthritis does not rule out osteoarthritis. [5]






Additional studies [5]
Consider to rule out complications and alternative diagnoses (e.g., fractures, infection), and for surgical planning. [5][6]
-
Imaging
- MRI, ultrasound, or CT scan of the affected joint
- See “Other imaging modalities” and “Further investigations” in “Diagnostics of osteoarthritis.”
- Laboratory studies: usually normal in osteoarthritis [7]
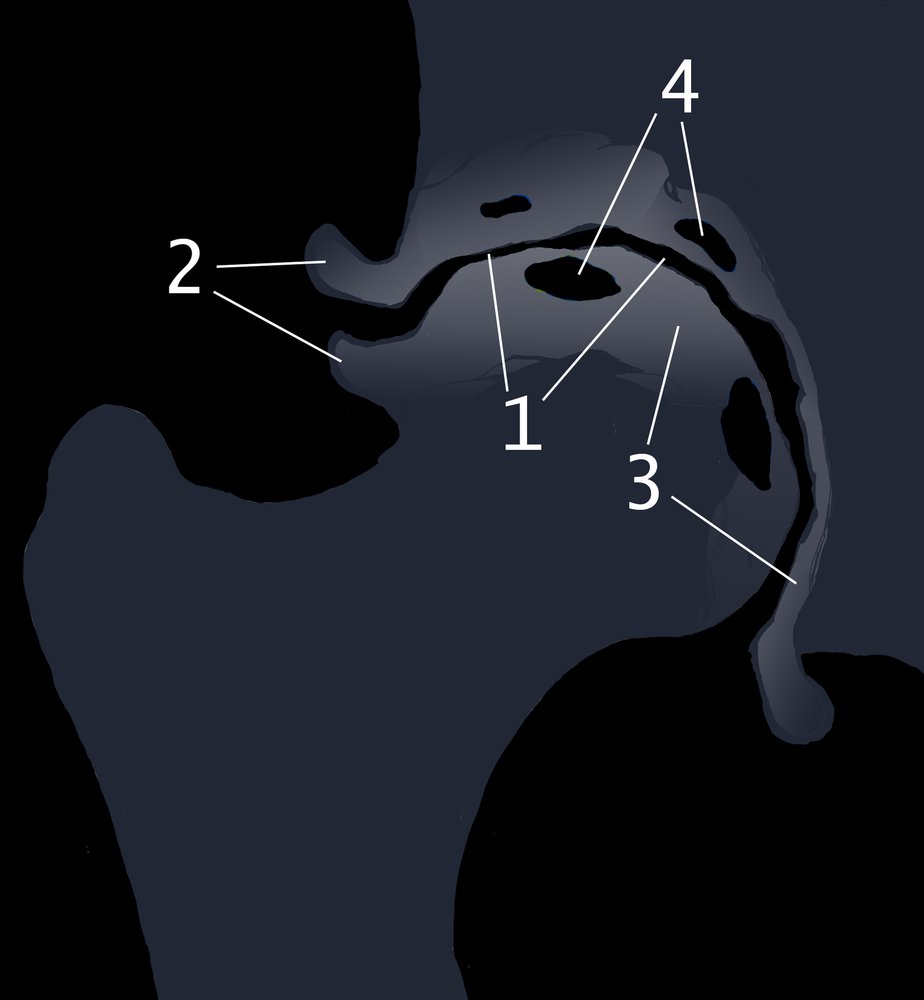
AP view
Findings of osteoarthritis include irregular joint space narrowing (1), osteophytes (2), subchondral sclerosis (3), and subchondral cyst formation (4).
© AMBOSS

X-ray pelvis (AP view)
Marked narrowing of the weight-bearing regions of the acetabulofemoral joint spaces (yellow lines) is accompanied by femoral head and acetabular sclerosis (green overlay), subchondral cyst formation (examples indicated by white dashed outlines), and osteophytes (examples indicated by red overlay). The femoral heads show superolateral migration and loss of normal sphericity.
Source: © IMPP

X-ray left knee (AP view)
Marked medial compartment narrowing (red lines and arrowheads) is accompanied by subchondral sclerosis (green overlay) and osteophyte formation (red overlay).
Source: © IMPP

X-ray right knee (AP view)
Marked lateral compartment narrowing (indicated by white lines and arrows) is accompanied by subchondral sclerosis (green overlay) and osteophyte formation (red overlay). Tibial spine osteophytes (example indicated by yellow overlay) are also visible.
This image was created by AMBOSS and is licensed under CC BY-SA 3.0. It is based on the image “Roe-Gonarthrose” by J. Lengerke, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

X-ray of the knee, lateral view: joint space narrowing in the tibiofemoral joint and retropatellar, subchondral sclerosis
Source: © IMPP
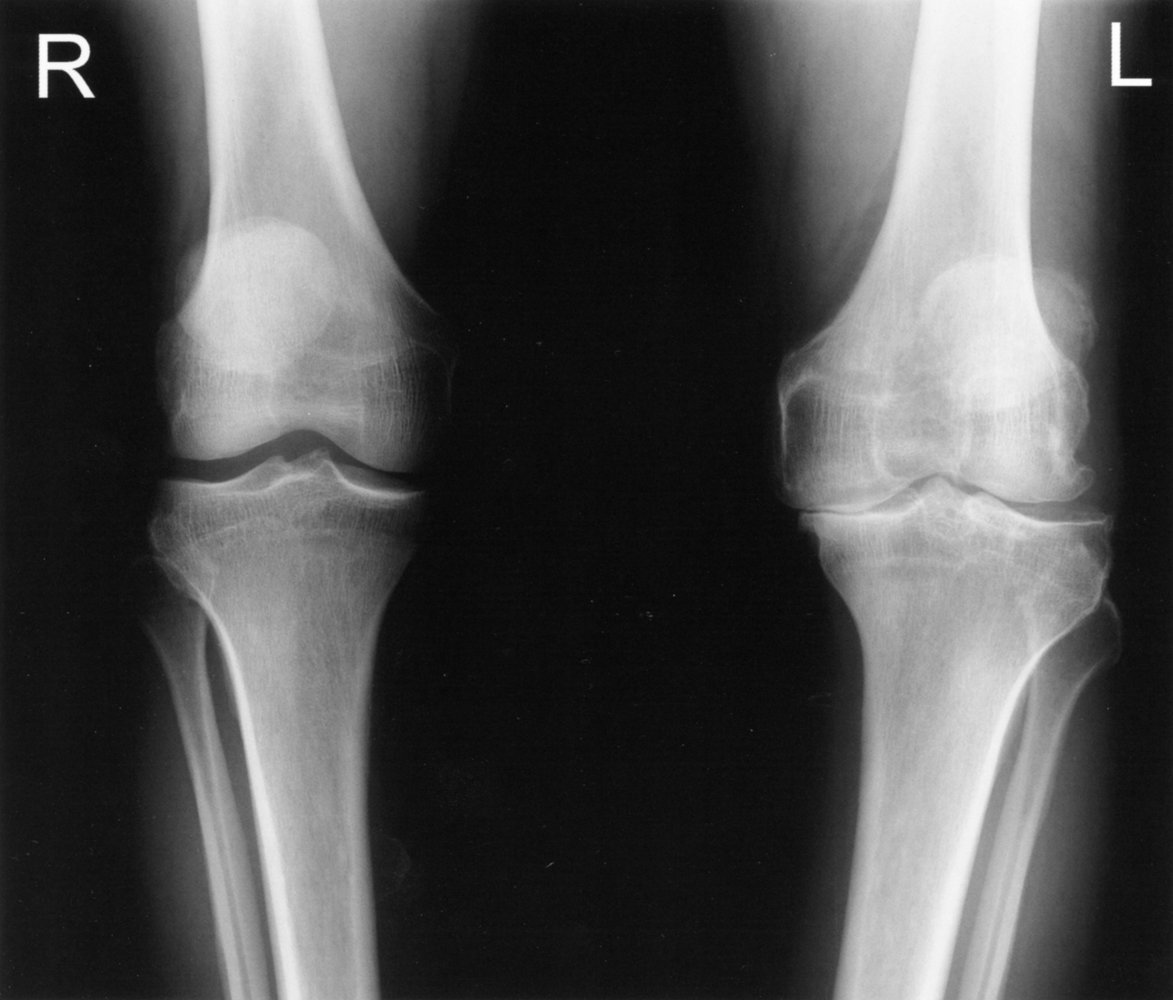
X-ray knees (AP view)
Advanced degenerative changes of the left knee are seen, with marked medial compartment narrowing, surface irregularity (indicated by red line), subchondral sclerosis (example indicated by green overlay), and osteophytes (red overlay). Additional findings include a subchondral cyst (blue overlay) at the lateral edge of the tibia and medial subluxation of the femur (indicated by dashed arrows). Only small intercondylar eminence osteophytes are seen on the right (yellow arrowheads).
Source: © IMPP
Treatment
Approach [8][9]
- Recommend nonpharmacological management for all patients (see “Management of osteoarthritis”).
- Initiate pharmacological therapy for pain management, as needed.
- Indications for referral to orthopedic surgery include:
- Persistent symptoms despite multiple trials of conservative management [5]
- Symptoms associated with radiographic evidence of osteonecrosis or moderate-to-severe osteoarthritis [9]
Conservative management [5][10]
-
Nonpharmacological management [8][10]
- Weight loss (if overweight or obese) and exercise are recommended for all patients.
- Physical therapy and use of assistive devices (e.g., cane, knee braces) may help improve pain and mobility.
- There is limited evidence to support the routine use of oral supplements (e.g., fish oil, vitamin D, glucosamine, chondroitin sulfate) or orthotic insoles. [5][8][10][11]
-
Pharmacotherapy [5]
- First line: NSAIDs
- Patients who cannot tolerate or do not improve with NSAIDs: See “Management of osteoarthritis” for alternative agents.
-
Intraarticular glucocorticoid injection: Consider for local, short-term relief in patients with osteoarthritis of the hip and knee.
- Intraarticular triamcinolone or methylprednisolone [12]
- Use ultrasound to guide hip joint injections.
- Risks: cartilage loss, joint space infection
- Intraarticular hyaluronic acid: may be considered for osteoarthritis of the knee [8][11][13]
Pharmacotherapy should only be used as a short-term treatment in symptomatic patients; long-term therapy is associated with many adverse effects.
Surgery
Arthroplasty
- Total or partial joint replacement may be considered for advanced joint destruction with pain and functional impairment not adequately controlled by conservative management. [5]
- Type of surgery depends on the joint involved and the extent of involvement; indications include:
-
Total hip arthroplasty
- Primary and secondary osteoarthritis of the hip
- Femoral neck fracture in patients with concomitant osteoarthritis [14][15]
- Total knee replacement: osteoarthritis of one or more compartments of the knee joint [16][17]
- Partial knee replacement: isolated osteoarthritis of one or two compartments of the knee joint [6][16][17]
-
Total hip arthroplasty
- See also “Complications after arthroplasty.”
Patients undergoing total joint replacement should receive perioperative antibiotic prophylaxis and VTE prophylaxis. Early postoperative physiotherapy can reduce the duration of hospitalization and improve pain and function. See “Perioperative considerations” in “Treatment of osteoarthritis” for details. [18]
Osteotomy
- May be considered to delay the development or worsening of osteoarthritis in young individuals (< 60 years of age) with unicompartmental osteoarthritis (e.g., due to trauma) [10][16][19]
- Types and indications include:
- High tibial osteotomy: osteoarthritis of the medial compartment of the knee and associated genu varus
- Low femoral osteotomy: osteoarthritis of the lateral compartment of the knee and associated genu valgum
- Hip osteotomy: hip dysplasia and no significant osteoarthritis
Arthroscopy
- Consider for osteoarthritis and a concomitant meniscal tear that does not respond to conservative management [10][19]
Related One-Minute Telegram
- One-Minute Telegram 60-2022-3/3: Yoga improves function in knee OA (but only if you actually do it).
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- One-Minute Telegram
- 2021 American Academy of Orthopaedic Surgeons Evidence-Based Clinical Practice Guideline: Management of Osteoarthritis of the
- Knee (Non-Arthroplasty)
- 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee
- 2015 American Academy of Orthopaedic Surgeons Evidence-Based Clinical Practice Guideline: Surgical Management of Osteoarthritis of the Knee
References
- Litwic A, Edwards MH, Dennison EM, Cooper C. "Epidemiology and burden of osteoarthritis". Br Med Bull. 105(1). :185-199. (2013)
- "Arthritis - Arthritis Basics - Arthritis Types - Osteoarthritis". https://web.archive.org/web/20170502141746/https://www.cdc.gov/arthritis/basics/osteoarthritis.htm. [2017-02-02]
- West SG. "Rheumatology Secrets". Hanley & Belfus. (2002). ISBN: 9781560534747
- Magee DJ. "Orthopedic Physical Assessment - E-Book". Elsevier Health Sciences. (2014). ISBN: 9781455709755
- Katz JN, Arant KR, Loeser RF. "Diagnosis and Treatment of Hip and Knee Osteoarthritis". JAMA. 325(6). :568. (2021)
- Jennings JM, Kleeman-Forsthuber LT, Bolognesi MP. "Medial Unicompartmental Arthroplasty of the Knee". J Am Acad Orthop Surg. 27(5). :166-176. (2019)
- Sinusas K. "Osteoarthritis: diagnosis and treatment.". Am Fam Physician. 85(1). :49-56. (2012)
- Kolasinski SL, Neogi T, Hochberg MC, et al. "2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee". Arthritis Care Res (Hoboken). 72(2). :149-162. (2020)
- Hannon CP, Goodman SM, Austin MS, et al. "2023 American College of Rheumatology and American Association of Hip and Knee Surgeons Clinical Practice Guideline for the Optimal Timing of Elective Hip or Knee Arthroplasty for Patients With Symptomatic Moderate‐to‐Severe Osteoarthritis or Advanced Symptomatic Osteonecrosis With Secondary Arthritis for Whom Nonoperative Therapy Is Ineffective". Arthritis Care & Research. 75(11). :2227-2238. (2023)
- "Management of Osteoarthritis of the Knee (Non-Arthroplasty) Evidence-Based Clinical Practice Guideline". https://www.aaos.org/oak3cpg. [2021-08-31]
- "Management of Osteoarthritis of the Hip Evidence-Based Clinical Practice Guideline". https://www.aaos.orog/oahcpg. [2017-03-13]
- Douglas RJ. "Corticosteroid injection into the osteoarthritic knee: drug selection, dose, and injection frequency". Int J Clin Pract. 66(7). :699-704. (2012)
- Trojian TH, Concoff AL, Joy SM, et al. "AMSSM Scientific Statement Concerning Viscosupplementation Injections for Knee Osteoarthritis". Clin J Sport Med. 26(1). :1-11. (2016)
- "American Academy of Orthopaedic Surgeons Management of Hip Fractures in Older Adults Evidence-Based Clinical Practice Guideline". https://www.aaos.org/hipfxcpg. [2021-12-03]
- Schmitz PP, van Susante JLC, Somford MP. "Low conversion rates toward total hip arthroplasty after hemiarthroplasty in patients under 75 years of age". Eur J Orthop Surg Traumatol. 29(8). :1687-1691. (2019)
- "Surgical Management of Osteoarthritis of the Knee Evidence Based Clinical Practice Guideline". https://www.aaos.org/smoakcpg. [2015-09-04]
- Rönn K, Reischl N, Gautier E, Jacobi M. "Current Surgical Treatment of Knee Osteoarthritis". Arthritis. 2011. :1-9. (2011)
- Anderson DR et al. "American Society of Hematology 2019 guidelines for management of venous thromboembolism: prevention of venous thromboembolism in surgical hospitalized patients". Blood Adv. 3(23). :3898-3944. (2019)
- Katz JN, Earp BE, Gomoll AH. "Surgical management of osteoarthritis". Arthritis Care & Research. 62(9). :1220-1228. (2010)