Summary
Osteoarthritis is a disabling joint disease characterized by degeneration of the joint complex (articular cartilage, subchondral bone, and synovium) that can have various causes, most notably advanced age and overuse. It mainly affects weight-bearing joints and joints that are heavily used, such as the hip, knee, hands, and vertebrae. Despite the widespread view that osteoarthritis is a condition caused exclusively by degenerative “wear and tear” of the joints, newer research indicates that there are various causes, including preexisting joint abnormalities, genetics, local inflammation, mechanical forces, and biochemical processes that are promoted by proinflammatory mediators and proteases. Major risk factors for osteoarthritis include advanced age, obesity, previous injuries, and asymmetrically stressed joints. In early-stage osteoarthritis, patients typically report a reduced range of motion, joint stiffness, and pain that is aggravated with heavy use. As the disease advances, persistent pain may also be present during the night and/or at rest. The diagnosis is predominantly based on clinical features and supported by radiological findings, as classic radiographic features of osteoarthritis do not always correlate with the patient's clinical symptoms or appearance. If lifestyle changes (e.g., moderate exercise, weight loss) fail to improve symptoms, pharmacotherapy is typically used for the management of active osteoarthritis. If these measures do not improve the patient's quality of life, surgical procedures such as arthroplasty may be necessary.
See also “Osteoarthritis of the hip and knee” for more specific information.





© AMBOSS

© AMBOSS

© AMBOSS

© AMBOSS
Epidemiology
- Prevalence: most common joint disorder in the USA, affecting more than 20 million adults [1]
- Incidence: increases with age
- Sex: : ♀ > ♂, especially in patients older than 50 years
- Incidence rates in specific joints: knee > hip > hand [1]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Modifiable risk factors [1]
- Obesity
- Excessive joint loading or overuse (mechanical stress)
-
Nonmodifiable risk factors [1]
- Age (> 55 years)
- Family history
- History of joint injury (especially anterior cruciate ligament injury), trauma, and/or surgery
- Anatomic factors causing asymmetrical joint stress
- Hemophilic hemarthroses and deposition diseases that stiffen cartilage
- Sex (See “Epidemiology” above.)
- Neuromuscular weakness
- Infections
- Inflammatory disorders
Classification
Osteoarthritis can be classified according to the underlying cause: [2]
-
Idiopathic OA
- No identifiable underlying cause
- Can be localized or generalized
- Genetic factors of causation have been implicated, but not definitively proven.
-
Secondary OA
- Hemochromatosis
- Wilson disease
- Ehlers-Danlos syndrome
- Diabetes
- Avascular necrosis
- Congenital disorders of joints
- Alkaptonuria
- Joint trauma
Pathophysiology
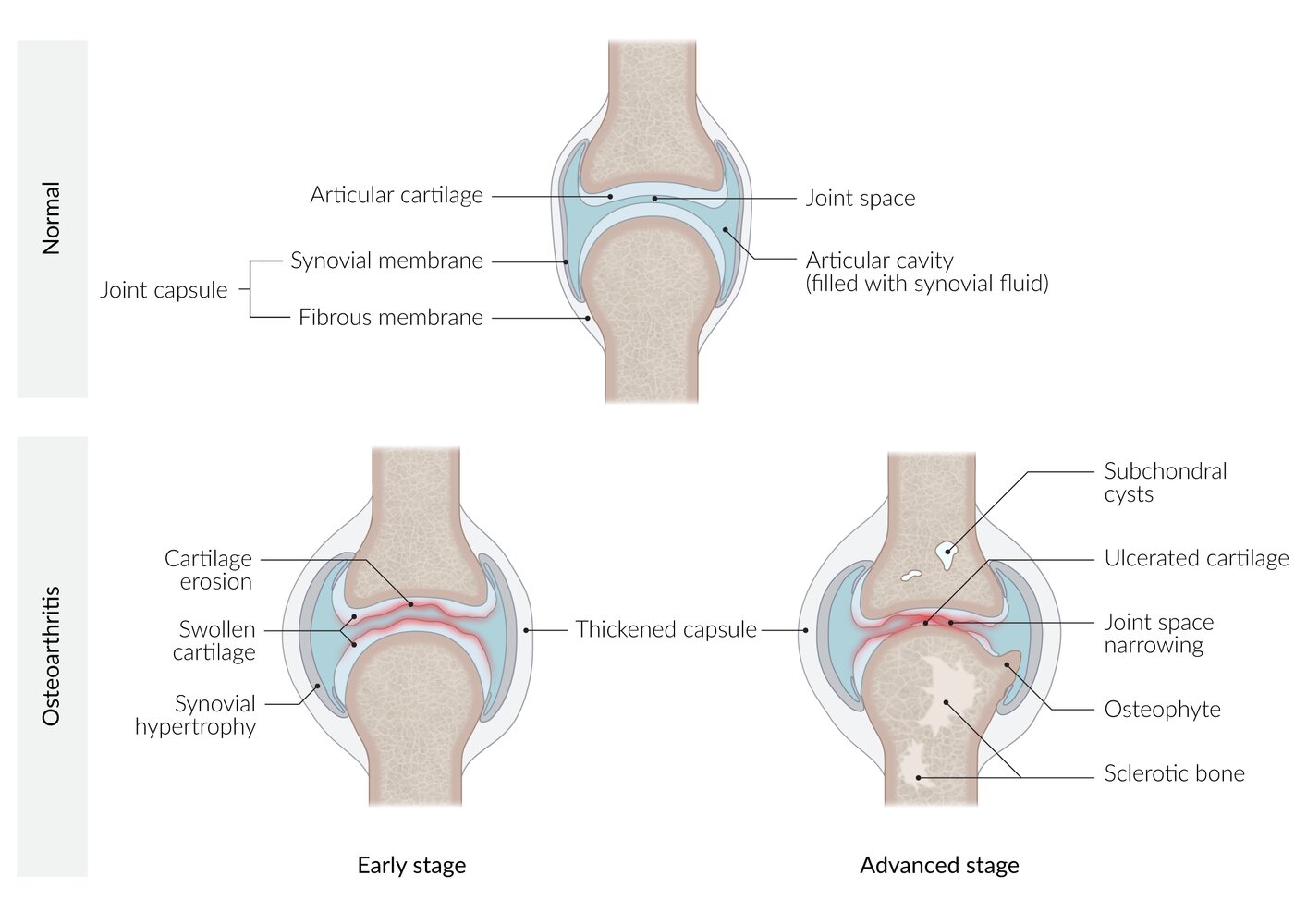
Chronic mechanical stress on the joints and age-related decrease in proteoglycans → cartilage loses elasticity and becomes friable → degeneration and inflammation of cartilage ; → joint space narrowing and thickening and sclerosis of the subchondral bone [3][4]

© AMBOSS
Clinical features
Common clinical findings [5][6][7][8]
- Pain during or after exertion (e.g., at the end of the day) that is relieved with rest
- Pain in both complete flexion and extension
- Crepitus on joint movement
- Joint stiffness and restricted range of motion
- Morning joint stiffness usually lasting < 30 minutes
- Possible formation of varus deformity if the knee is affected
- Joints are usually asymmetrically involved, as opposed to rheumatoid arthritis.
- Findings in late-stage disease: constant pain (including at night) and a more severely restricted range of motion than during the early stages
Joint-specific findings [5]
- Heberden nodes: pain and nodular thickening on the dorsal sides of the distal interphalangeal joints, ♀ > ♂
- Bouchard nodes: pain and nodular thickening on the dorsal sides of the proximal interphalangeal joints , ♀ > ♂
- Rhizarthrosis: osteoarthritis of the first carpometacarpal joint, between the trapezium and the first metacarpal bone
- Hallux rigidus: osteoarthritis of the first metatarsophalangeal joint, between the first metatarsal and the first proximal phalanx; characterized by hypertrophy of the sesamoid bones
- See also “Clinical features” in “Osteoarthritis of the hip and knee.”







")



In contrast to rheumatoid arthritis, osteoarthritis can affect the distal interphalangeal joints.

X-ray left knee (AP view)
Marked medial compartment narrowing (red lines and arrowheads) is accompanied by subchondral sclerosis (green overlay) and osteophyte formation (red overlay).
Source: © IMPP

X-ray knees (AP standing view)
Marked bilateral medial compartment joint space narrowing is accompanied by surface irregularity (indicated by red lines), subchondral sclerosis (example indicated by green overlay), and prominent osteophytes (examples indicated by arrowheads). Subluxation of the medial femoral condyles is also seen (indicated by dashed arrows). The lateral compartments show only mild degenerative changes.
Source: “Fig. 3A, in: Arthroscopic cartilage regeneration facilitating procedure for osteoarthritic knee” by Lyu SR, Hsu CC, Lin CW, BMC Musculoskeletal Disorders, licensed under CC BY 2.0. Modifications: Image is cropped, letter "A" is removed, date removed, round metal BBs removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
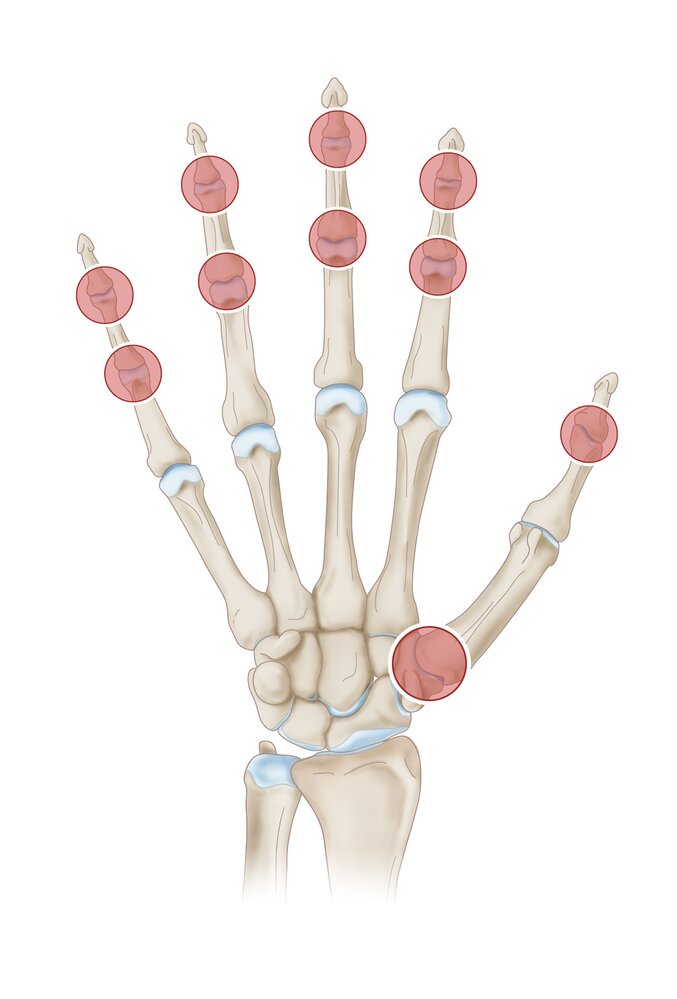
Osteoarthritis of the hand affects especially the distal interphalangeal joints (Heberden nodes), proximal interphalangeal joints (Bouchard nodes), and the first carpometacarpal joint, between the trapezoid and the first metacarpal (Rhizarthrosis).
© AMBOSS

Nodular thickening of the distal interphalangeal joints (DIPJ) and proximal interphalangeal joints (PIPJ) can be seen.
This appearance is characteristic of bony swellings caused by osteophyte formation in osteoarthritis. At the DIPJ these are called “Heberden nodes” (best seen here on the right middle finger and both index fingers), and at the PIPJ they are called “Bouchard nodes” (best seen here on the right middle finger).
Source: © IMPP

There is nodular thickening of the distal interphalangeal joint of the index finger (Heberden node), with mild ulnar deviation of the distal phalanx.
Source: © IMPP

There is nodular thickening of the distal interphalangeal joint of the second to 5th digits (Heberden nodes), with mild radial deviation of the distal phalanx of digits 3 and 5.
Source: © IMPP

X-ray right hand (PA view)
Typical features of osteoarthritis are visible at the first carpometacarpal joint (green circle), including joint space narrowing (blue line), subchondral sclerosis (increase in bone density; green overlay), and marginal osteophytes. A subchondral cyst (geode; red overlay) has formed at the base of the first metacarpal (MC1). Findings of early osteoarthritis also involve several other joints of the hand and wrist (indicated by red arrows).
T: Trapezium
Source: © IMPP

X-ray hand (PA view)
Advanced degenerative changes can be seen at the first carpometacarpal joint (trapeziometacarpal joint), including joint space narrowing (green line), subchondral sclerosis (indicated by yellow overlay), subchondral cysts (examples indicated by blue overlay), and osteophytes (example indicated by red overlay). Similar features of osteoarthritis (examples indicated by red outlines) involve several intercarpal and interphalangeal joints and the sesamoid articulations of the first metacarpophalangeal joint.
Source: © IMPP

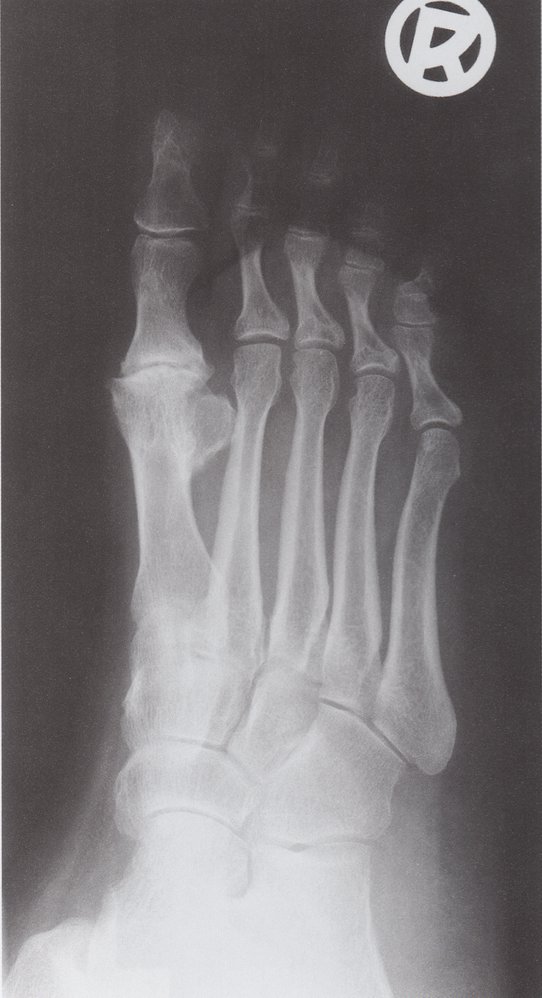
X-ray anterior foot (bilateral; AP view)
Advanced degenerative changes can be seen at the left first metatarsophalangeal (MTP) joint and sesamoid articulations (indicated by red lines), with prominent MTP joint osteophytes (yellow overlay), subchondral sclerosis (green overlay), and joint space narrowing (blue line). There is lesser involvement of the right first MTP joint. No articular erosions can be seen.
Source: © IMPP
X-ray right foot (oblique view)
Advanced degenerative changes involve the metatarsophalangeal joint, with subchondral sclerosis (red overlay), osteophytosis (green circles), and irregular joint space narrowing (indicated by blue line). Degenerative changes also involve the sesamoid bones (arrowheads).
Source: © IMPP
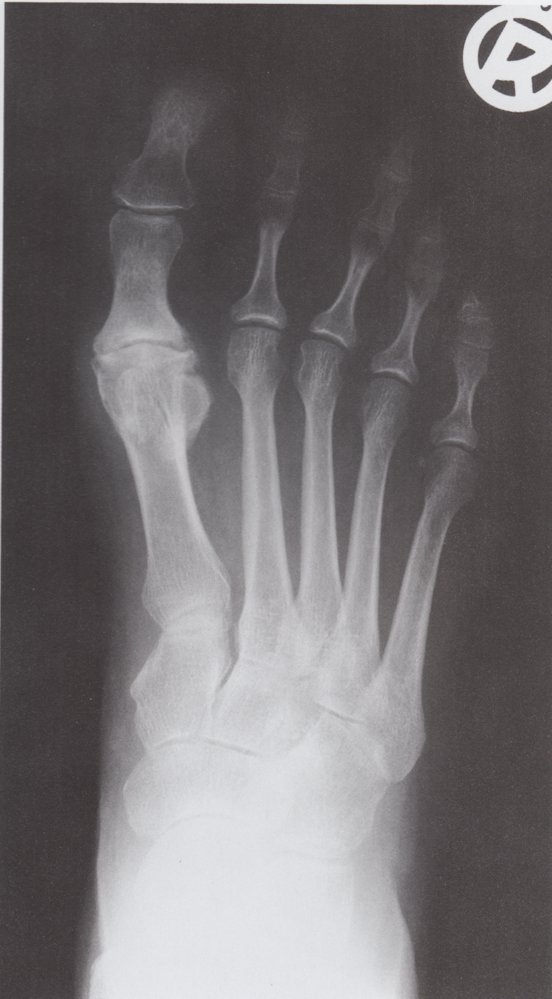
X-ray right foot (dorsoplantar/AP view)
Advanced degenerative changes involve the first metatarsophalangeal joint, with subchondral sclerosis (red overlay), osteophytosis (green circle), and irregular joint space narrowing (indicated by blue line). Degenerative changes also involve the sesamoid bones (arrowheads).
Source: © IMPP

There is nodular thickening of the distal interphalangeal joint (Heberden node).
Source: © IMPP
Diagnosis
Approach
-
Osteoarthritis is a clinical diagnosis
- Consider the diagnosis in patients ≥ 45 years of age with typical clinical features. [7]
- There are no specific diagnostic criteria. [9]
- If there is clinical doubt, consider imaging and additional testing to:
- Support the clinical diagnosis with radiological evidence of joint degeneration [1]
- Rule out differential diagnoses [7][10]
- Invasive procedures are not routinely recommended, but may be helpful in select circumstances, for example:
- Uncertain diagnosis
- Assessing cartilage damage
- Ruling out septic arthritis
- Procedures with dual diagnostic and therapeutic purposes.
Osteoarthritis is often diagnosed based on the patient's history and the presence of typical clinical features. Radiographic signs often do not correlate with the patient's reported symptoms or clinical findings; therefore, imaging is usually used to support the diagnosis.
Imaging [7][10]
The presence of at least one of the radiological signs of osteoarthritis, in addition to typical clinical features, supports the diagnosis of osteoarthritis.
First-line modality: plain radiography of affected joints
- Indications
- Suspected fracture
- To rule out inflammatory arthritis
- Uncertain diagnosis
- Consideration: Multiple views are typically more accurate than a single view.
Other imaging modalities
Other modalities may be indicated if the diagnosis remains uncertain after radiography.
-
MRI
- Indications
- Suspicion of a cartilage or meniscal tear to determine if knee surgery is required
- To rule out or confirm differential diagnoses (e.g., avascular necrosis, femoroacetabular impingement)
- Disadvantages: expensive, not as widely available as other imaging modalities, and the contrast can cause hypersensitivity or kidney injury
- Indications
-
Ultrasonography
- Indications
- Joint swelling: to differentiate from inflammatory arthritis
- Joint interventions (e.g., aspiration, injection): to guide the needle
- Disadvantages: A skilled technician is required, and subchondral bone lesions cannot be visualized.
- Indications
- Computed tomography : may offer improved visualization of osteophytes and subchondral cysts, particularly in the hip joint, compared with radiography and MRI
Radiological signs of osteoarthritis [1]
- Irregular joint space narrowing
- Subchondral sclerosis: a dense area of bone (visible on x-ray) just below the cartilage zone of a joint that forms as a result of a compressive load on the joint
- Osteophytes (bone spurs): spurs or densifications that develop on the edges of the joint, increasing its surface area
- Subchondral cyst: a fluid-filled cyst that develops on the surface of a joint due to local bone necrosis induced by the joint stress caused by osteoarthritis


Further investigations
- Laboratory testing: Inflammatory markers (e.g., erythrocyte sedimentation rate, C-reactive protein) are usually normal in osteoarthritis.
- Arthrocentesis: Synovial fluid analysis usually does not show the presence of inflammation (white blood cell count < 2000/mm3). [11]
- Arthroscopy: may show a thickened capsule, synovial hypertrophy, and/or ulcerated cartilage
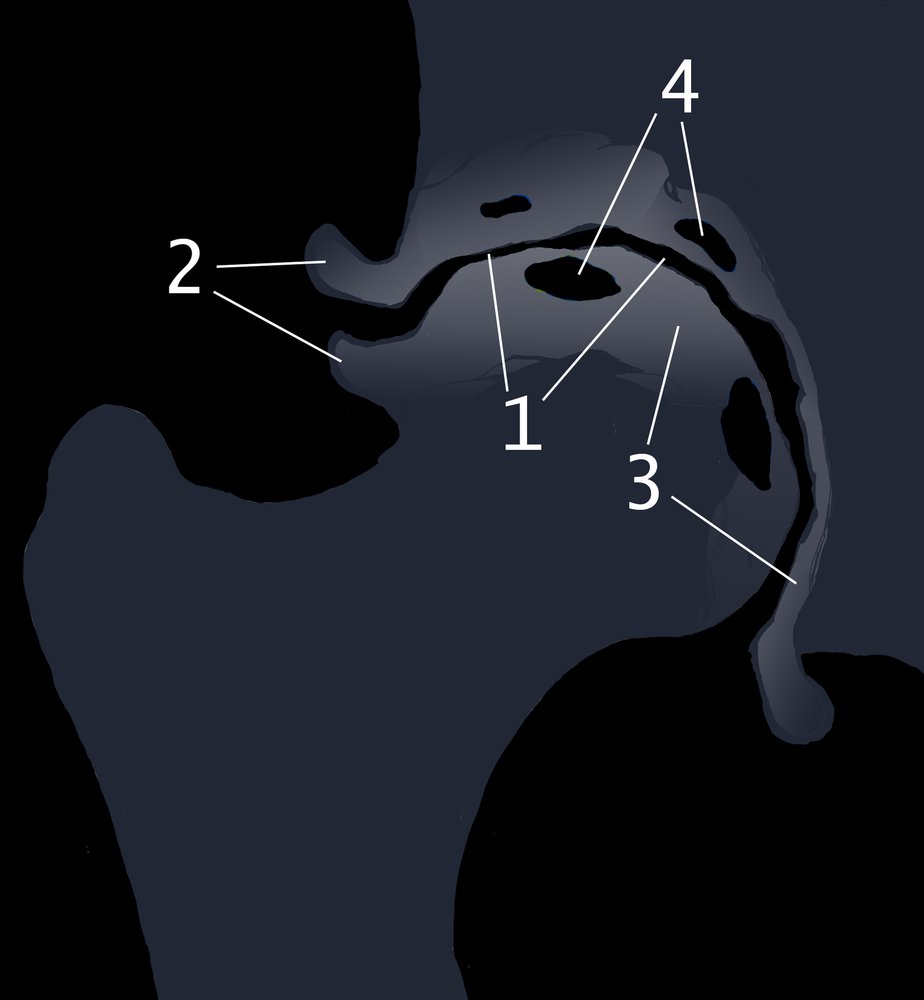
AP view
Findings of osteoarthritis include irregular joint space narrowing (1), osteophytes (2), subchondral sclerosis (3), and subchondral cyst formation (4).
© AMBOSS
X-ray anterior foot (bilateral; AP view)
Advanced degenerative changes can be seen at the left first metatarsophalangeal (MTP) joint and sesamoid articulations (indicated by red lines), with prominent MTP joint osteophytes (yellow overlay), subchondral sclerosis (green overlay), and joint space narrowing (blue line). There is lesser involvement of the right first MTP joint. No articular erosions can be seen.
Source: © IMPP
X-ray right hand (PA view)
Typical features of osteoarthritis are visible at the first carpometacarpal joint (green circle), including joint space narrowing (blue line), subchondral sclerosis (increase in bone density; green overlay), and marginal osteophytes. A subchondral cyst (geode; red overlay) has formed at the base of the first metacarpal (MC1). Findings of early osteoarthritis also involve several other joints of the hand and wrist (indicated by red arrows).
T: Trapezium
Source: © IMPP

X-ray right knee (AP view)
Marked lateral compartment narrowing (indicated by white lines and arrows) is accompanied by subchondral sclerosis (green overlay) and osteophyte formation (red overlay). Tibial spine osteophytes (example indicated by yellow overlay) are also visible.
This image was created by AMBOSS and is licensed under CC BY-SA 3.0. It is based on the image “Roe-Gonarthrose” by J. Lengerke, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
X-ray knees (AP standing view)
Marked bilateral medial compartment joint space narrowing is accompanied by surface irregularity (indicated by red lines), subchondral sclerosis (example indicated by green overlay), and prominent osteophytes (examples indicated by arrowheads). Subluxation of the medial femoral condyles is also seen (indicated by dashed arrows). The lateral compartments show only mild degenerative changes.
Source: “Fig. 3A, in: Arthroscopic cartilage regeneration facilitating procedure for osteoarthritic knee” by Lyu SR, Hsu CC, Lin CW, BMC Musculoskeletal Disorders, licensed under CC BY 2.0. Modifications: Image is cropped, letter "A" is removed, date removed, round metal BBs removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Differential diagnoses
See “Differential diagnoses of inflammatory arthritis.”
The differential diagnoses listed here are not exhaustive.
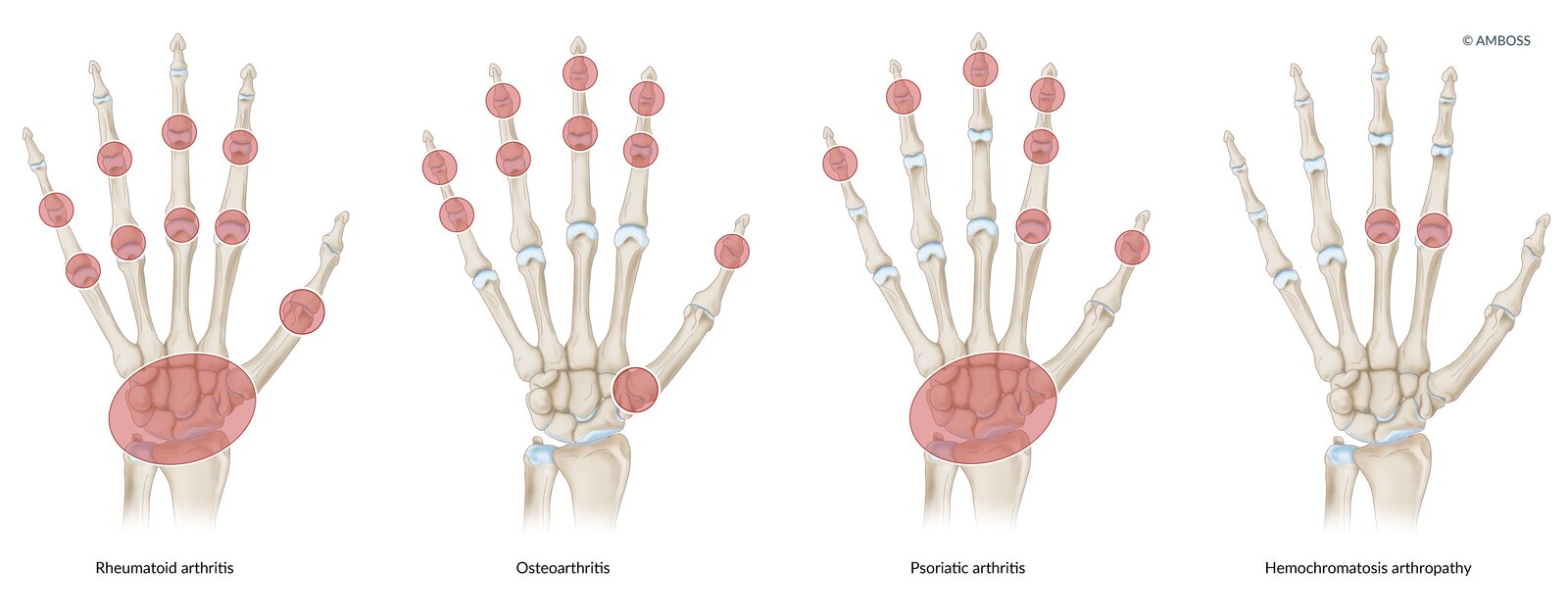
Rheumatoid arthritis: symmetrical swelling of metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints
Osteoarthritis: PIP, distal interphalangeal (DIP), and first carpometacarpal (CMC) joints
Psoriatic arthritis: DIP and MCP joints, or whole digit (dactylitis)
Hemochromatosis: symmetrical arthropathy of the MCP joint of the second and third digits
© AMBOSS
Treatment
Treatment recommendations are consistent with the 2019 American College of Rheumatology (ACR) management guidelines for osteoarthritis of the hand, hip, and knee. [12]
Approach [12][13]
- Follow a stepwise approach to treatment: Start with nonpharmacological management, followed by pharmacological and/or surgical treatment if needed.
- Nonpharmacological management: e.g., exercise and weight loss
-
Pharmacotherapy
- First line: e.g., topical or oral NSAIDs
- Second line: e.g., acetaminophen or intraarticular glucocorticoid injections
- Surgical management: e.g., complete or partial joint replacement (arthroplasty) using an endoprosthesis
- Individualize treatment based on patient preferences, comorbidities, treatment goals, and available resources.
- Consider referral to physical therapy or occupational therapy.
Nonpharmacological management
- Educate patients about the disease and self-management techniques.
-
Exercise: indicated in all patients, especially those with osteoarthritis of the hip and knee
- Formulate a specific exercise plan, taking into account patient preference and availability.
- There is no clear evidence that one form of exercise is superior to another.
- Tai chi offers benefits that are comparable to physical therapy in patients with osteoarthritis of the knee. [14]
- Weight loss: indicated in overweight and obese patients [15]
- Supportive devices (e.g., a cane or knee brace): Consider for patients with osteoarthritis of the hip and knee who are experiencing joint instability and pain when weight is placed on the joint.
- Other symptomatic therapy: e.g., acupuncture, kinesiology taping, or heat/cold therapy
Pharmacotherapy [12][13]
Pharmacotherapy for osteoarthritis should be consistent with the WHO pain ladder. See “Treatment of pain” for dosages and important considerations.
-
NSAIDs (e.g., ibuprofen): first-line treatment option
- Topical analgesics: preferred initial therapy for patients with osteoarthritis of the knee because of the lack of systemic absorption
- Oral analgesics: recommended for hip osteoarthritis or if there is inadequate relief with topical NSAIDs
- Acetaminophen: an option for patients who are unable to tolerate oral NSAIDs; less effective than NSAIDs
-
Opioids (e.g., tramadol): short-term use for patients who cannot tolerate or have had insufficient relief with NSAIDs
- Tramadol is the preferred opioid for patients with osteoarthritis of the knee, hip, and/or hand
- If all other oral medication options are ineffective, consider nontramadol opioids. [12]
- Use opioids sparingly because of the risk of dependence and severe adverse effects.
- Intraarticular glucocorticoid injection: local, short-term relief in patients with osteoarthritis of the hip and knee
- Other treatments: conditionally recommended for specific joints [12]
- Osteoarthritis of the knee: topical capsaicin
- Osteoarthritis of the knee, hip, and/or hand: duloxetine
Pharmacotherapy should only be used as a short-term treatment in symptomatic patients; long-term therapy is associated with many adverse effects.
Surgical management [16][17]
Modalities
Surgery is typically indicated if conservative measures fail.
-
Arthroscopy
- Indications: patients with meniscus or cartilage damage, or femoroacetabular impingement
- Procedures: debridement and lavage
-
Osteotomy: realigns joints to relieve pain and potentially delay disease progression
- Indication: young patients (typically ≤ 60 years of age) with single compartment arthritis
- Procedures: tibial osteotomy for varus alignment; femoral osteotomy for valgus deformity
-
Arthrodesis
- Indication: patients with advanced, therapy-resistant osteoarthritis of the wrist and/or ankle
- Procedure: surgical fusion of the two bones that form the joint in a functional position; can be performed arthroscopically
-
Arthroplasty
- Indication: patients who have experienced inadequate relief using conservative measures
- Procedure: complete or partial replacement of a joint using an endoprosthesis
- Risks: infection, blood clot (e.g., deep vein thrombosis, pulmonary embolism), dislocation, implant failure [16]
- See also “Treatment” in “Osteoarthritis of the hip and knee” and “Complications after osteosynthesis/arthroplasty.”
Perioperative considerations
- Follow measures to prevent surgical site infection. [18]
- Perioperative antibiotic prophylaxis: Cefazolin is recommended for patients undergoing total joint replacement. [19]
- Postoperative considerations [20][21]
- Initiate VTE prophylaxis after total hip or knee joint replacement. [22]
- Refer patients for physical therapy. [20][21]
- Antibiotics are not routinely recommended prior to dental work in patients with a history of joint replacement. [23]
- Individuals with comorbidities may be less likely to experience symptomatic improvement postoperatively.
After total joint replacement, patients should receive aspirin or an anticoagulant (e.g., a direct oral anticoagulant or low molecular weight heparin) for VTE prophylaxis. [22]
Related One-Minute Telegram
- One-Minute Telegram 72-2023-2/3: Metformin may defend against osteoarthritis
Interested in the newest medical research, distilled to just one minute? Sign up for the One-Minute Telegram in the “Tips and links” below.
External Resources
References
- Litwic A, Edwards MH, Dennison EM, Cooper C. "Epidemiology and burden of osteoarthritis". Br Med Bull. 105(1). :185-199. (2013)
- Altman R, Asch E, Bloch D, et al. "Development of criteria for the classification and reporting of osteoarthritis: Classification of osteoarthritis of the knee". Arthritis & Rheumatism. 29(8). :1039-1049. (1986)
- Liu-Bryan R, Terkeltaub R. "Emerging regulators of the inflammatory process in osteoarthritis". Nat Rev Rheumatol. (2014)
- Lane NE, Brandt K, Hawker G et al. "OARSI-FDA initiative: defining the disease state of osteoarthritis". Osteoarthritis Cartilage. (2011)
- Marshall M, Watt FE, Vincent TL, Dziedzic K. "Hand osteoarthritis: clinical phenotypes, molecular mechanisms and disease management". Nature Reviews Rheumatology. 14(11). :641-656. (2018)
- Hawker GA, Stewart L, French MR, et al. "Understanding the pain experience in hip and knee osteoarthritis – an OARSI/OMERACT initiative". Osteoarthritis and Cartilage. 16(4). :415-422. (2008)
- Wang X, Oo WM, Linklater JM. "What is the role of imaging in the clinical diagnosis of osteoarthritis and disease management?". Rheumatology. 57(suppl_4). :iv51-iv60. (2018)
- Michael JW-P, Schlüter-Brust KU, Eysel P. "The Epidemiology, Etiology, Diagnosis, and Treatment of Osteoarthritis of the Knee". Deutsches Aerzteblatt Online. 107(9). :152-162. (2010)
- Aggarwal R, Ringold S, Khanna D, et al. "Distinctions between diagnostic and classification criteria?". Arthritis Care Res (Hoboken). 67(7). :891-7. (2015)
- Wenham CYJ, Grainger AJ, Conaghan PG. "The role of imaging modalities in the diagnosis, differential diagnosis and clinical assessment of peripheral joint osteoarthritis". Osteoarthritis and Cartilage. 22(10). :1692-1702. (2014)
- Bhavsar TB, Sibbitt WL, Band PA, et al. "Improvement in diagnostic and therapeutic arthrocentesis via constant compression". Clin Rheumatol. 37(8). :2251-2259. (2017)
- Kolasinski SL, Neogi T, Hochberg MC, et al. "2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee". Arthritis Care Res (Hoboken). 72(2). :149-162. (2020)
- Paterson KL, Gates L. "Clinical Assessment and Management of Foot and Ankle Osteoarthritis: A Review of Current Evidence and Focus on Pharmacological Treatment". Drugs Aging. 36(3). :203-211. (2019)
- Wang C, Schmid CH, Iversen MD, et al. "Comparative Effectiveness of Tai Chi Versus Physical Therapy for Knee Osteoarthritis". Ann Intern Med. 165(2). :77-86. (2016)
- Messier SP, Resnik AE, Beavers DP, et al. "Intentional Weight Loss in Overweight and Obese Patients With Knee Osteoarthritis: Is More Better?". Arthritis Care & Research. 70(11). :1569-1575. (2018)
- Katz JN, Earp BE, Gomoll AH. "Surgical management of osteoarthritis". Arthritis Care & Research. 62(9). :1220-1228. (2010)
- De l’ Escalopier N, Anract P, Biau D. "Surgical treatments for osteoarthritis". Annals of Physical and Rehabilitation Medicine. 59(3). :227-233. (2016)
- Myers TG, Lipof JS, Chen AF, Ricciardi BF. "Antibiotic Stewardship for Total Joint Arthroplasty in 2020". J Am Acad Orthop Surg. 28(18). :e793-e802. (2020)
- Bratzler DW, Dellinger EP, Olsen KM, et al. "Clinical practice guidelines for antimicrobial prophylaxis in surgery.". Am J Health Syst Pharm. 70(3). :195-283. (2013)
- "Management of Osteoarthritis of the Hip Evidence-Based Clinical Practice Guideline". https://www.aaos.orog/oahcpg. [2017-03-13]
- "Surgical Management of Osteoarthritis of the Knee Evidence Based Clinical Practice Guideline". https://www.aaos.org/smoakcpg. [2015-09-04]
- Anderson DR et al. "American Society of Hematology 2019 guidelines for management of venous thromboembolism: prevention of venous thromboembolism in surgical hospitalized patients". Blood Adv. 3(23). :3898-3944. (2019)
- Sollecito TP, Abt E, Lockhart PB, et al. "The use of prophylactic antibiotics prior to dental procedures in patients with prosthetic joints". J Am Dent Assoc. 146(1). :11-16.e8. (2015)