Summary
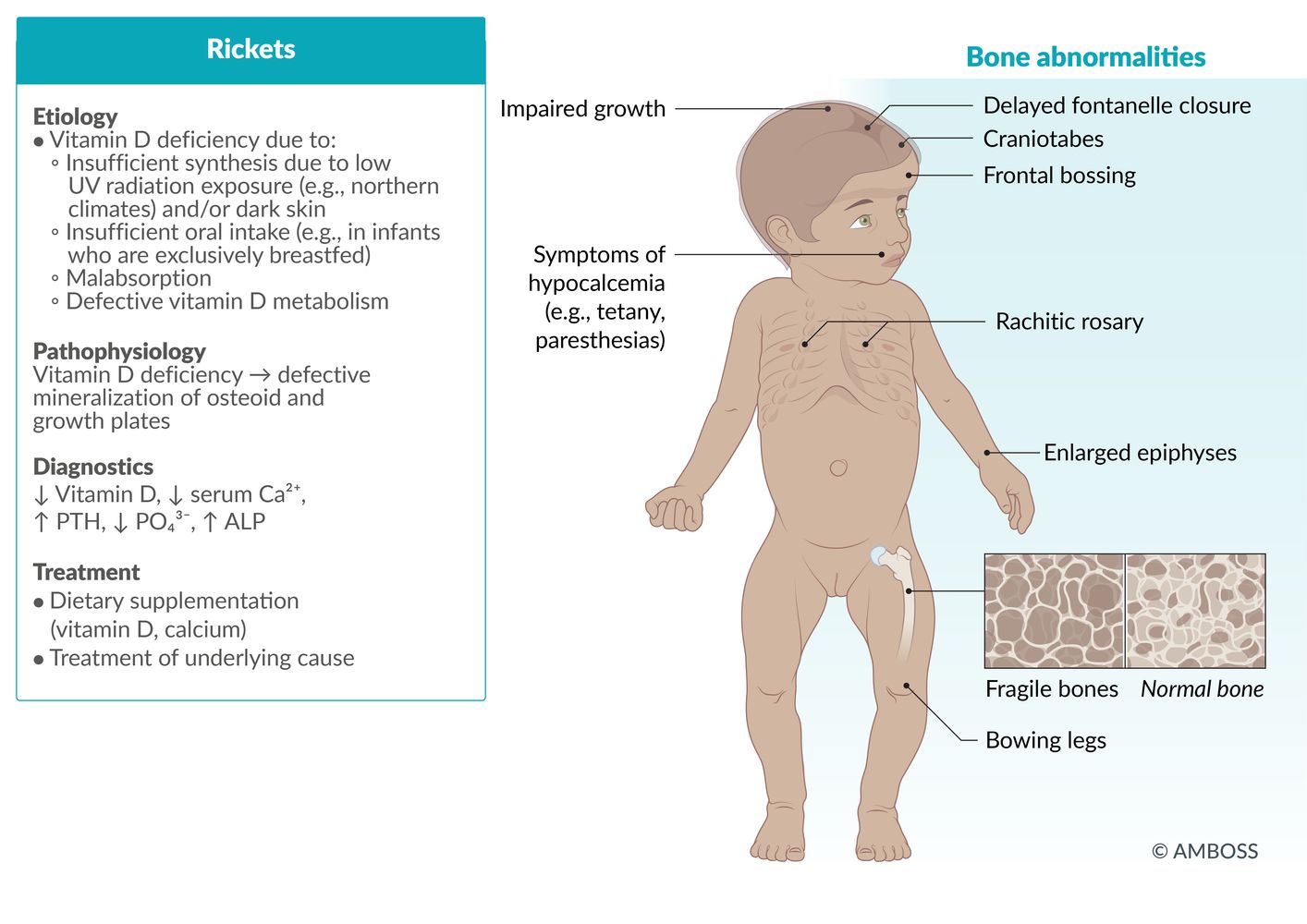
Osteomalacia and rickets are disorders of bone mineralization. In osteomalacia, remodeling of preexisting bone is defective; in rickets, new bone formation is defective. Osteomalacia can affect individuals of any age, whereas rickets can only occur in children with open growth plates. Osteomalacia and rickets are caused by insufficient calcium, phosphate depletion, and/or direct inhibition of bone mineralization. The most common cause of both disorders is vitamin D deficiency. Patients with osteomalacia usually present with bone pain and tenderness, while patients with rickets exhibit bone deformities and impaired growth. Over time, both conditions may lead to bowing of the long bones and/or pathological fractures. The diagnosis involves a combination of clinical history, abnormal laboratory studies, and, in many cases, imaging. Treatment, which is directed at the underlying cause, most commonly involves treatment of vitamin D deficiency and ensuring sufficient calcium intake.
Etiology
| Overview of etiologies of rickets and osteomalacia | |
|---|---|
| Mechanism | Underlying causes |
| Insufficient calcium (calcipenic rickets) [1] |
|
| Phosphate deficiency (phosphopenic rickets) [1] |
|
| Direct inhibition of bone mineralization [1] |
|
Vitamin D deficiency is the most common cause of both osteomalacia and rickets. Vitamin D-independent causes (i.e., hypophosphatemia, hypocalcemia, medication-induced) and hereditary causes are less common. [2]
Pathophysiology
The causes of osteomalacia and rickets involve at least one of the following mechanisms: [1][5]
-
Calcipenic rickets
- ↓ Calcium → ↑ PTH levels → ↓ phosphate → impaired bone mineralization [1][5]
- See “Calcium homeostasis.”
- Phosphopenic rickets: ↓ phosphate → impaired bone mineralization
- Direct inhibition of mineralization → impaired bone mineralization
Impaired bone mineralization can affect both existing bone matrix (osteomalacia) and, if growth plates are still open, new bone formation (rickets). [1]
Low phosphate is present in both calcipenic and phosphopenic forms of osteomalacia and rickets. [1][5]
Clinical features
Osteomalacia [5]
- Occurs in adults and children
- Bone pain and tenderness
- Pathologic fractures
-
Myopathy (predominantly proximal)
- Muscle weakness causing waddling gait and difficulty walking
- Spasms
- Cramps
- Symptoms of hypocalcemia
- Severe osteomalacia: bone deformities, e.g., bowing of the lower limbs
Osteomalacia and rickets may be asymptomatic. [6][7]
Rickets [1]
- Only occurs in children (growth plates have not fused)
-
Bone deformities
- Bowing, primarily of the long bones
-
Distention of the bone-cartilage junctions
- Rachitic rosary: bead-like distention of the bone-cartilage junctions in the ribs
-
Marfan sign
- Distention of the epiphyseal plate of the distal tibia with widening and cupping of the metaphysis
- Gives appearance of a double medial malleolus on inspection and palpation of the ankle
- Widened wrists
- Craniotabes: softening of the skull
- Deformities of the knee, especially genu varum [1]
- Increased risk of fracture
-
Harrison groove
- A depression of the thoracic outlet
- Caused by muscles pulling along the costal insertion of the diaphragm
- Impaired growth
- Symptoms of hypocalcemia including seizures in infants
- Late closing of fontanelles
- Delayed walking (> 18 months)
- Cardiomyopathy
Osteomalacia is defective mineralization of existing bone and can occur in individuals with open or closed growth plates. Rickets is defective mineralization of new bone formation and, therefore, only occurs in children with open growth plates (i.e., before the end of puberty). [8]


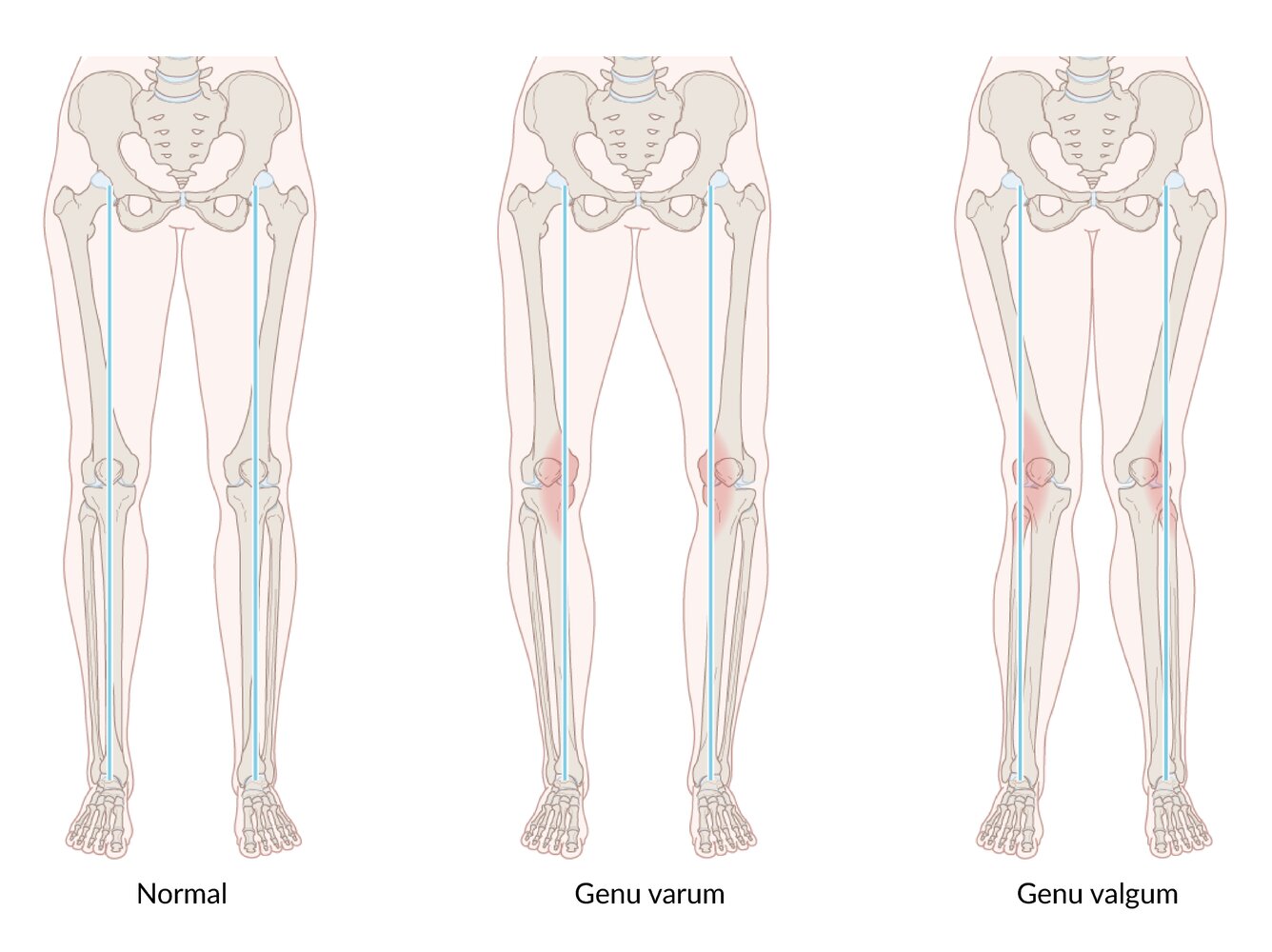
The mechanical axis of the lower extremity runs from the midpoint of the femoral head and the midpoint of the ankle joint. Physiologically, this line passes through the midpoint of the knee joint. In genu varum (bow legs), the mechanical axis passes medial to the knee joint, causing maximum mechanical strain on the medial aspect of the knee. In genu valgum (knock knees), the mechanical axis passes lateral to the knee joint, causing maximum mechanical strain on the lateral aspect of the knee.
© AMBOSS
© AMBOSS
Subtypes and variants
Vitamin D-dependent rickets type 1 [1][3][9]
-
Pathophysiology
- Autosomal recessive mutation in the 25-hydroxyvitamin-D-1α-hydroxylase gene [1]
- Leads to impaired conversion of inactive vitamin D to the active form, 1,25‑dihydroxyvitamin D3 (calcitriol)
-
Clinical features
- Early onset of rickets (in infancy)
- Muscle weakness
- Growth faltering
- Hypotonia
- Pathological fractures
-
Diagnostics [1][9][10]
- Normal or elevated plasma 25-OH
- Low or undetectable 1,25(OH)2D
- Hypocalcemia, hypophosphatemia, and elevated ALP
- Elevated parathyroid hormones
- Treatment: calcitriol supplementation
Vitamin D-dependent rickets type 2 [1][4][9]
- Pathophysiology: : An autosomal recessive mutation in the vitamin D receptor gene causes end-organ resistance to vitamin D.
-
Clinical features
- Early onset of rickets (in infancy)
- Growth faltering
- Alopecia
-
Diagnostics [1][9][10]
- Normal or elevated plasma 25-OH
- Extremely elevated plasma 1,25(OH)2D
- Hypocalcemia, hypophosphatemia, elevated ALP
- Elevated parathyroid hormones
-
Treatment [1][9]
- Very high-dose vitamin D therapy [9]
- Refractory disease: elemental calcium
Diagnosis
General principles [1][5][11]
- Diagnosis is based on characteristic laboratory and imaging findings.
- The choice of imaging depends on whether osteomalacia or rickets is suspected.
- If there is diagnostic uncertainty, refer patients to endocrinology for advanced studies.
Diagnostic scoring systems for osteomalacia that include clinical history, biochemical results, and radiological imaging findings have been proposed, but they have not yet been validated. [5]
Laboratory studies [1][5][12]
- Obtain the studies listed in the table below.
- Common laboratory findings in vitamin D deficiency include ↓ Ca, ↓ phosphorus, ↑ PTH, and ↑ ALP).
- If findings are not consistent with osteomalacia/rickets, see “Laboratory evaluation of bone disease.”
| Laboratory findings in osteomalacia and rickets by etiology [1][5][12] | ||
|---|---|---|
| Test | Calcipenic rickets | Phosphopenic rickets |
| Calcium, serum |
|
|
| Phosphorus, serum [1] |
|
|
| Calcium, urine |
|
|
| Phosphorus, urine |
|
|
| ALP |
|
|
| Parathyroid hormone (PTH) |
|
|
| Serum 25-OH (vitamin D levels) |
|
|
PTH is elevated in calcipenic rickets but is typically normal in phosphopenic rickets. [1]
Imaging
Modalities [1][12][13]
-
X-rays
- Children with open growth plates: x-rays of wrists and knees to evaluate for rickets
- Adults and children with closed growth plates: Consider x-rays of ribs, scapulae, or pelvis. [5][14]
- Additionally, in osteomalacia, consider:
- DEXA
- Bone scintigraphy
Imaging findings in osteomalacia and/or rickets [1][12][13]
-
General
-
Evidence of bone loss [15]
- ↓ Bone mineral density (i.e., osteopenia or osteoporosis)
- Thinned cortical bone
- Pathological fractures
-
Looser zones (pseudofractures), which are transverse radiolucent bands that represent insufficiency stress fractures seen in osteomalacia and severe rickets; typical features include: [13][15][16]
- Multiple and symmetrical
- Perpendicular to the periosteal surface
- Most often occur in the ribs, scapulae, pubic rami, and medial cortex of long bones
-
Evidence of bone loss [15]
-
Additional findings in rickets may include:
- Epiphyseal plate widening
- Metaphyseal cupping, stippling, and fraying
- Bone bowing (e.g., genu varum )
- Chest x-ray: prominent costochondral junctions of the ribs (i.e., rachitic rosary)
- X-ray skull: persistently widened suture lines (i.e., open fontanelles), occipital flattening, and a more squared appearance
- X-ray spine: spinal curvature
-
Additional findings in osteomalacia may include increased uptake on bone scintigraphy. [15]
- Occurs as a result of increased bone turnover
- May mimic metastatic cancer
Advanced studies [1][5][15]
-
Indications
- Diagnostic uncertainty
- Rare etiologies suspected e.g.:
- Tumor-induced osteomalacia
- Vitamin D-dependent rickets type I or type II
-
Potential studies
- Serum 1,25(OH)2D levels
- FGF23 levels
- Iliac bone biopsy with tetracycline labeling

X-ray of the right leg and ankle joint of an elderly patient (AP view)
Multiple transverse, radiolucent lines with sclerotic margins (example indicated by white arrow) can be seen extending into the bone from the cortical surface of the tibia and fibula. Diffuse demineralization (osteopenia) of the tibia and fibula is evidenced by their radiolucent appearance and the bowing of the fibular shaft.
The radiolucent lines are pseudofractures, known as Looser zones, which are typically seen in patients with osteomalacia and rickets.
Source: “Figure 1, in: Severe Osteomalacia Related to Long-Term Intravenous Drug Abuse” by Leslie Gamache, Mark R. Burge, Journal of Investigative Medicine, licensed under CC BY 3.0.

X-ray of the left forearm (PA view) of a 2-year-old child with rickets from vitamin D deficiency
There is generalized osteopenia as a result of deficient mineralization. Growth plate widening and metaphyseal cupping and flaring seen earlier in the disease have progressed to an irregular disorganized appearance of the distal radius and ulna. The radius and ulna are shortened and bowed.
Source: © IMPP
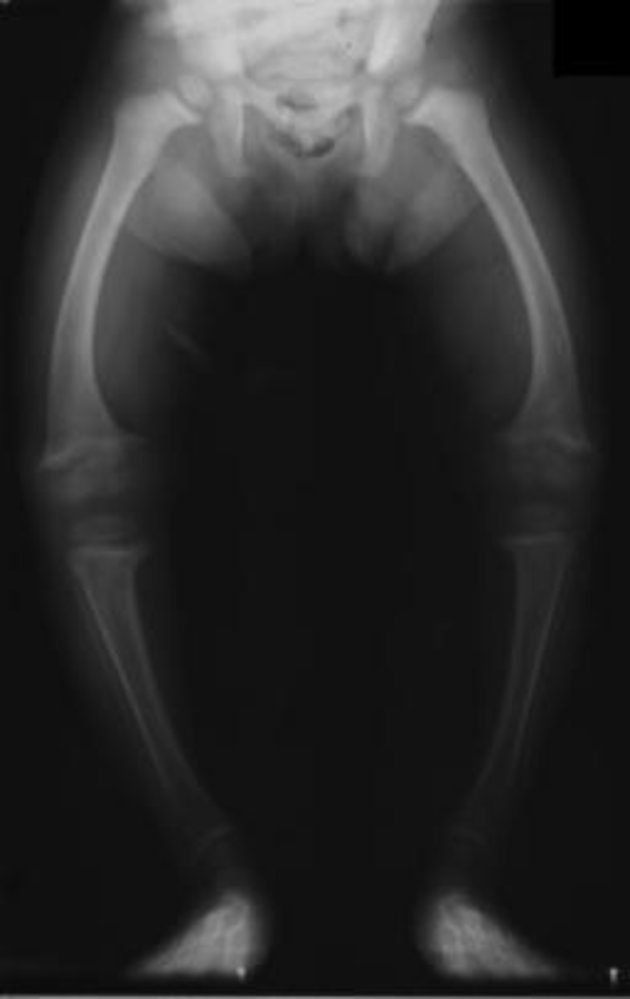
X-ray legs (AP view) of a 2-year-old child with rickets
Deficiency in mineralization has resulted in bowing of the legs (genu varum; indicated by dashed lines). Excess nonmineralized osteoid at the metaphyseal zones of provisional calcification has produced widening of the epiphyseal growth plate (examples indicated by green overlay) along with metaphyseal splaying (examples indicated by red lines), cupping (yellow line), and fraying (examples indicated by blue overlay).
Source: “Anteroposterior (AP) view of the legs in a 2 year old child with rickets.” by Michael L. Richardson, Wikimedia Commons, licensed under CC BY-SA 1.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 1.0.
{kind=link}

X-ray chest (AP view) of a child.
There are prominent nodular costochondral junctions (black arrows) on the right side of the chest due to the expansion of the anterior ribs.
These findings are referred to as rachitic rosary because of their resemblance to beads on a rosary.
Source: “RicketsChestXray.jpg” by Frank Gaillard, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Differential diagnoses
Differential diagnoses of osteomalacia [17][18]
- Bone metastases
- Osteoporosis
- Paget disease of bone
- Hyperparathyroidism
- Renal osteodystrophy
Differential diagnoses of rickets [19]
- Osteoglophonic dysplasia with dwarfism
- Osteogenesis imperfecta
- Neurofibromatosis
- McCune-Albright syndrome
- Child abuse/neglect
- Congenital pseudarthrosis of the tibia
Congenital pseudarthrosis of the tibia [20]
- Definition: unilateral anterolateral bowing of the lower third of the tibia and possibly fibula associated with neurofibromatosis type I
-
Clinical features
- Bowing of the tibia
- Pseudoarthrosis of the lower leg
- Fractures of the tibia and fibula are possible.
- Clinical features of neurofibromatosis type I
-
Treatment
- Orthoses
- Osteotomy to excise pseudoarthrosis
- Bone graft
- Internal or external fixation

The differential diagnoses listed here are not exhaustive.

X-ray lower right leg (left: AP view; right: lateral view) of a child with neurofibromatosis type I (NF1)
Sclerosis and anterolateral bowing of the tibial diaphysis are seen (green overlay), with a bony defect along the anterior tibial cortex (arrow). Also present is a displaced distal fibular fracture with overriding fragments (red overlay).
The radiographic findings are consistent with congenital tibial pseudoarthrosis, a rare dysplasia that can manifest in infancy or childhood and has a strong association with NF1. Radiographs may show anterolateral tibial bowing with or without bony heterogeneity and discontinuity. MRI with perfusion sequences can provide a more detailed assessment of the soft tissues, the periosteum, and vascular defects in the bone.
Source: © IMPP
Treatment
General principles [1][5][12]
- Treat any acute electrolyte abnormalities, e.g.:
- Calcium repletion for severe and/or symptomatic hypocalcemia
- Phosphate repletion
- Review diet and medication list to look for reversible etiologies of osteomalacia and rickets.
- Determine underlying etiology and refer to a specialist for further management, e.g.:
- Endocrinology for treatment of vitamin D deficiency or other metabolic bone disease
- Nephrology for treatment of underlying renal disease
- Fully complete treatment for underlying osteomalacia before treating other metabolic bone diseases (e.g., osteoporosis). [6][15]
- For bone deformities that persist despite medical management, refer to orthopedics for surgical correction. [21]
Treatment of vitamin D-associated osteomalacia and rickets [1][12][15]
-
Pharmacological therapy
- Treatment doses of vitamin D [5][11][22]
- Adequate daily intake of calcium [5][11][12]
- Calcitriol may be required for selected indications. [1][5]
-
Ongoing management
- Monitoring for clinical features of vitamin D toxicity (uncommon at typical treatment doses) [11]
- Follow-up x-rays and laboratory studies to ensure resolution of abnormalities [1][15]
- Target serum 25(OH)D: > 30 ng/mL [5]
- Target PTH level: normal [5]
- Maintenance dosing of vitamin D for prevention of vitamin D deficiency
In patients with malabsorption, vitamin D and calcium doses may need to be increased or given via alternative routes (i.e., IM/IV). [5][11]
Prevention
- Prevention of vitamin D deficiency [1]
- Adequate dietary calcium [1]
Sun exposure is not recommended to prevent vitamin D deficiency because of the risk of skin cancer. [23]
External Resources
References
- Carpenter TO, Shaw NJ, Portale AA, et al. "Rickets". Nat Rev Dis Primers. 3(1). (2017)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Yan Y, Calikoglu AS, Jain N. "Vitamin D-Dependent Rickets Type 1: A Rare, but Treatable, Cause of Severe Hypotonia in Infancy". J Child Neurol. 26(12). :1571-1575. (2011)
- Inamdar P, Bellad R, Herekar V. "Vitamin D-dependent rickets type 2: Alopecia responding to 1,25 hydroxy Vitamin D". Journal of the Scientific Society. 43(3). :155. (2016)
- Minisola S, Colangelo L, Pepe J, et al. "Osteomalacia and Vitamin D Status: A Clinical Update 2020". JBMR Plus. 5(1). (2020)
- Jha S, Chapman M, Roszko K. "When Low Bone Mineral Density and Fractures Is Not Osteoporosis". Curr Osteoporos Rep. 17(5). :324-332. (2019)
- Misra M, Pacaud D, Petryk A, Collett-Solberg PF, Kappy M. "Vitamin D Deficiency in Children and Its Management: Review of Current Knowledge and Recommendations". Pediatrics. 122(2). :398-417. (2008)
- Uday S, Högler W. "Nutritional Rickets and Osteomalacia in the Twenty-first Century: Revised Concepts, Public Health, and Prevention Strategies". Curr Osteoporos Rep. 15(4). :293-302. (2017)
- Munns CF, Shaw N, Kiely M, et al. "Global Consensus Recommendations on Prevention and Management of Nutritional Rickets". J Clin Endocrinol Metab. 101(2). :394-415. (2016)
- World Health Organization. "Nutritional rickets: a review of disease burden, causes, diagnosis, prevention and treatment". World Health Organization. (2019). ISBN: 9789241516587
- Chang CY, Rosenthal DI, Mitchell DM, et al. "Imaging Findings of Metabolic Bone Disease". Radiographics. 36(6). :1871-1887. (2016)
- Fukumoto S, Ozono K, Michigami T, et al. "Pathogenesis and diagnostic criteria for rickets and osteomalacia — Proposal by an expert panel supported by Ministry of Health, Labour and Welfare, Japan, The Japanese Society for Bone and Mineral Research and The Japan Endocrine Society [Opinion]". Endocr J. 62(8). :665-671. (2015)
- Bhan A, Rao AD, Rao DS. "Osteomalacia as a Result of Vitamin D Deficiency". Endocrinol Metab Clin North Am. 39(2). :321-331. (2010)
- Gentile C, Chiarelli F. "Rickets in Children: An Update". Biomedicines. 9(7). :738. (2021)
- Burgener FA, Kormano M, Pudas T. "Differential Diagnosis in Conventional Radiology". Thieme. (2011). ISBN: 9783131620736
- Bilezikian, JP. "Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism". John Wiley & Sons. (2018). ISBN: 9781119266570
- Michałus I, Rusińska A. "Rare, genetically conditioned forms of rickets: Differential diagnosis and advances in diagnostics and treatment". Clin Genet. 94(1). :103-114. (2018)
- Eisenberg KA, Vuillermin CB. "Management of Congenital Pseudoarthrosis of the Tibia and Fibula". Curr Rev Musculoskelet Med. 12(3). :356-368. (2019)
- Blaney SM, Giardino AP, Orange JS, et al. "Rudolph's Pediatrics, 23rd Edition". McGraw-Hill Education / Medical. (2018). ISBN: 9781259588594
- Kennel KA, Drake MT, Hurley DL. "Vitamin D Deficiency in Adults: When to Test and How to Treat". Mayo Clinic Proceedings. 85(8). :752-758. (2010)
- Wagner CL, Greer FR. "Prevention of Rickets and Vitamin D Deficiency in Infants, Children, and Adolescents". Pediatrics. 122(5). :1142-1152. (2008)
- Levine MA. "Diagnosis and Management of Vitamin D Dependent Rickets". Front Pediatr. 8. (2020)
- American Academy of Pediatrics. "Textbook of Pediatric Care". American Academy of Pediatrics. (2016). ISBN: 9781610020473