Summary
Osteomyelitis is an infection of the bone; it occurs following hematogenous (seeded from a remote source) or exogenous (expansion from nearby tissue) spread of pathogens, most commonly Staphylococcus aureus. Individuals are at increased risk of osteomyelitis following trauma, placement of surgical implants or hardware, or if they are immunosuppressed or have poor tissue perfusion. Osteomyelitis can be either acute or chronic and manifests with signs of local inflammation, including swelling, pain, redness, and warmth. Systemic signs, such as fever and chills, are more common in acute infection. Diagnosis is supported via laboratory tests, imaging, and/or biopsy. In most cases, antibiotic therapy should be delayed until culture results are obtained, so as to better tailor treatment. Empiric antibiotic therapy for osteomyelitis is reserved for patients with signs of sepsis or rapidly progressing infections. Surgery may be necessary to remove necrotic bone, abscesses, infected foreign bodies, or fistulae. Osteomyelitis in adults often assumes a chronic course and requires prolonged treatment, whereas children typically make a quick and full recovery.
The diagnosis and management of vertebral osteomyelitis are described in “Spinal infections.”
Definitions
- Osteitis: a general term for inflammation of the bone
- Osteomyelitis: infection of the bone
Epidemiology
- Incidence: ∼ 20 per 100,000 [1]
-
Hematogenous osteomyelitis
- More common in children and adolescents
- Incidence is increasing in adults, driven by a rise in vertebral osteomyelitis [2]
- Exogenous osteomyelitis: more common in adults
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Routes of infection [3]
- Hematogenous osteomyelitis: (endogenous osteomyelitis): caused by hematogenous dissemination of a pathogen
-
Exogenous osteomyelitis: caused by a spread of bacteria (typically multiple pathogens) from the surrounding environment [4]
- Posttraumatic: infection following deep injury (penetrating injury, open fractures, severe soft tissue injury)
-
Contiguous: spread of infection from adjacent tissue
- Secondary to infected foot ulcer in patients with diabetes
- Iatrogenic (e.g., postoperative infection of a prosthetic joint implant)
Risk factors for osteomyelitis [5]
-
Local
- Poor tissue perfusion
- Open fractures
- Severe soft tissue injury
-
Systemic
- Immunosuppression
- Systemic diseases (e.g., diabetes mellitus, atherosclerosis)
- IV drug use
- Microbial: highly virulent pathogens
Pathogens
| Most common pathogens causing osteomyelitis [5] | ||
|---|---|---|
| Pathogens | Commonly affected groups | |
| Staphylococcus aureus (most common cause) |
|
|
| Staphylococcus epidermidis |
|
|
| Streptococci |
|
|
| Pseudomonas aeruginosa |
|
|
| Enterobacteriaceae | Salmonella |
|
| Klebsiella |
|
|
| Mycobacterium tuberculosis |
|
|
| Pasteurella multocida |
|
|
| Fungi (e.g., Candida) |
|
|
Clinical features
Acute osteomyelitis and subacute osteomyelitis [5]
- Onset: within days or weeks; associated with acute bone inflammation
- Duration: < 2 weeks (acute) or 2–6 weeks (subacute) [3][8]
- Symptoms: pain at the site of infection; in patients with peripheral neuropathy the pain may be mild or absent
- Possible localized findings: point tenderness, swelling, redness, warmth
- Possible systemic findings: malaise, fever, chills
Features of underlying disease (e.g., peripheral neuropathy, signs of peripheral arterial disease) may be seen in both acute and chronic osteomyelitis.
Chronic osteomyelitis
- Onset: develops slowly (over months or years) following acute infection
- Associated with: avascular bone necrosis and sequestrum formation (necrotic bone fragment that has become detached from the original bone) [9]
- Duration: typically > 6 weeks
- Symptoms: recurrent pain lasting weeks to months, maybe cyclical [3]
-
Possible localized findings
- Swelling, redness
- Deformity
- Impaired healing of overlying wounds
- Local sinus tract formation, perhaps draining pus
- Positive probe-to-bone test [10]
- Systemic findings: typically absent; may include low-grade fever, malaise
A positive probe-to-bone test is strongly suggestive of osteomyelitis, especially in diabetic patients with risk factors for osteomyelitis. [10][11]
The symptoms of chronic osteomyelitis may be subtle and the diagnosis may only become apparent when late complications occur (e.g., pathological fracture, loosening of implants). [12]
Diagnosis
The following recommendations are for nonvertebral osteomyelitis; diagnostics for vertebral osteomyelitis are detailed separately in “Spinal infections.”
Approach [5][10]
- Signs of sepsis present: Start management of sepsis without waiting for diagnostic test results.
- Routine studies: CBC, inflammatory markers, blood cultures, and an x-ray; choice of further imaging depends on patient characteristics.
- Suspected hematogenous osteomyelitis : Consider additional studies (e.g., urine culture, chest x-ray) based on clinical presentation.
- Imaging findings and blood cultures inconclusive: Consider bone biopsy with cultures to confirm the diagnosis.
In stable patients, defer antibiotics until blood cultures and/or bone biopsy have been taken. Do not delay antibiotic administration in patients with signs of sepsis.
Laboratory studies [10]
-
Routine studies
- CBC: thrombocytosis, possible leukocytosis [5]
- Inflammatory markers: ↑ CRP, ↑ ESR (sensitive but not specific) [12]
-
Blood cultures
- May be positive in hematogenous osteomyelitis (see “Causative pathogens in osteomyelitis”)
- Typically negative in exogenous osteomyelitis
-
Additional studies (as needed)
- Features of sepsis present: full diagnostic workup for sepsis
- Purulent wounds/sinuses: Consider culture of purulent material. [10]
Imaging
Routine imaging [10][13][14]
-
X-ray: low sensitivity and specificity for osteomyelitis ; [15]
- Indication: initial evaluation as can also exclude differential diagnoses of osteomyelitis
- Characteristic findings
- Acute osteomyelitis: typically no pathological findings [5]
- Subacute/chronic osteomyelitis: bone destruction, sequestrum formation, periosteal reactions [15]
-
MRI with and without IV gadolinium: most sensitive study [15]
- Indications
- Suspected acute osteomyelitis (evidence of inflammation can be seen ≤ 5 days after onset of infection)
- Negative x-ray but high clinical suspicion [13]
- Evaluation of the extent of osteomyelitis
- Characteristic findings [15]
- Acute/subacute osteomyelitis: cortical destruction, bone marrow inflammation, soft-tissue involvement
- Chronic osteomyelitis: fibrotic scarring of the marrow
- Disadvantages [15]
- Unable to differentiate infection from inflammation (e.g., in postoperative patients)
- Surgical hardware may decrease image quality.
- Indications
X-ray is the recommended initial imaging modality because it is inexpensive and can rule out differential diagnoses; however, it may miss acute osteomyelitis as findings are typically visible only 10–14 days after symptom onset. [10][13]




Imaging in special circumstances [15]
-
Contraindications to MRI
- Adults: CT with contrast [15][16]
- Children: ultrasound
- Recent surgery or fracture: labeled leukocyte scintigraphy [5][10]
- Surgical hardware (affecting MRI image quality): triple-phase bone scintigraphy
- Suspected overlying abscess (potentially requiring drainage): ultrasound
Bone biopsy [10][14]
- Indications: imaging findings and blood culture inconclusive
- Options: include MRI/CT-guided needle and open biopsy
- Timing: before administering antibiotic therapy, when feasible [17]
-
Send specimens for:
- Gram staining and cultures
- Histology
Bone biopsy with cultures is the confirmatory test for osteomyelitis and should be performed unless there are characteristic imaging features of osteomyelitis and positive blood cultures.
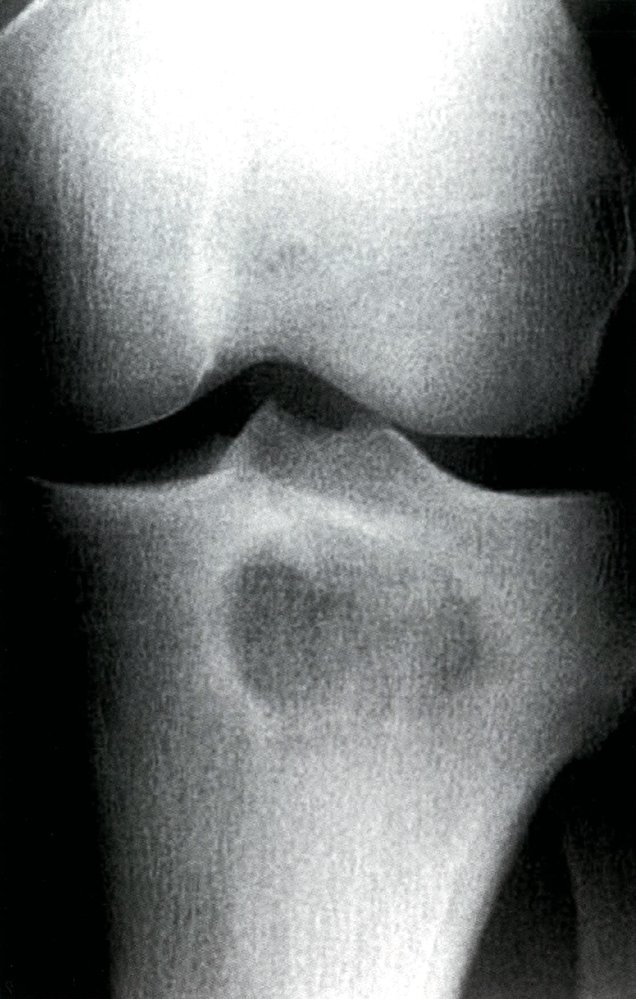
X-ray left knee (AP view) of a patient with clinically suspected osteomyelitis
The lytic lesion (circled green) seen in the proximal tibia has a partially sclerotic margin (green-shaded area). In conjunction with clinical suspicion, this appearance is compatible with subacute or chronic osteomyelitis (Brodie abscess). Differential diagnoses include various malignant and benign bone lesions.
Brodie abscesses typically occur at the ends of tubular bones. They may occur in the metaphysis or epiphysis and can cross an epiphyseal plate. The margins of a Brodie abscess may be sclerotic or nonsclerotic.
Source: © IMPP

X-ray left foot (dorsoplantar view)
Marked bony destruction (examples indicated by green overlay) involving multiple metatarsals and phalanges is accompanied by deformities and solid periosteal reaction (examples indicated by red overlay). Degenerative changes, particularly involving the great toe metatarsophalangeal joint, are also visible (indicated by arrowheads).
Source: “OsteomylitisWorse” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}

X-ray leg (left; AP view) of a child
A fragment of bone (green overlay) has separated from adjacent bone and is surrounded by a lucent rim (red outline).
A bony sequestrum is devascularized bone that may be seen in the setting of chronic osteomyelitis. A sequestrum may act as a nidus for ongoing infection.
Source: “Bony sequestrum in a child femur” by Sarindam7, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: Arrow removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
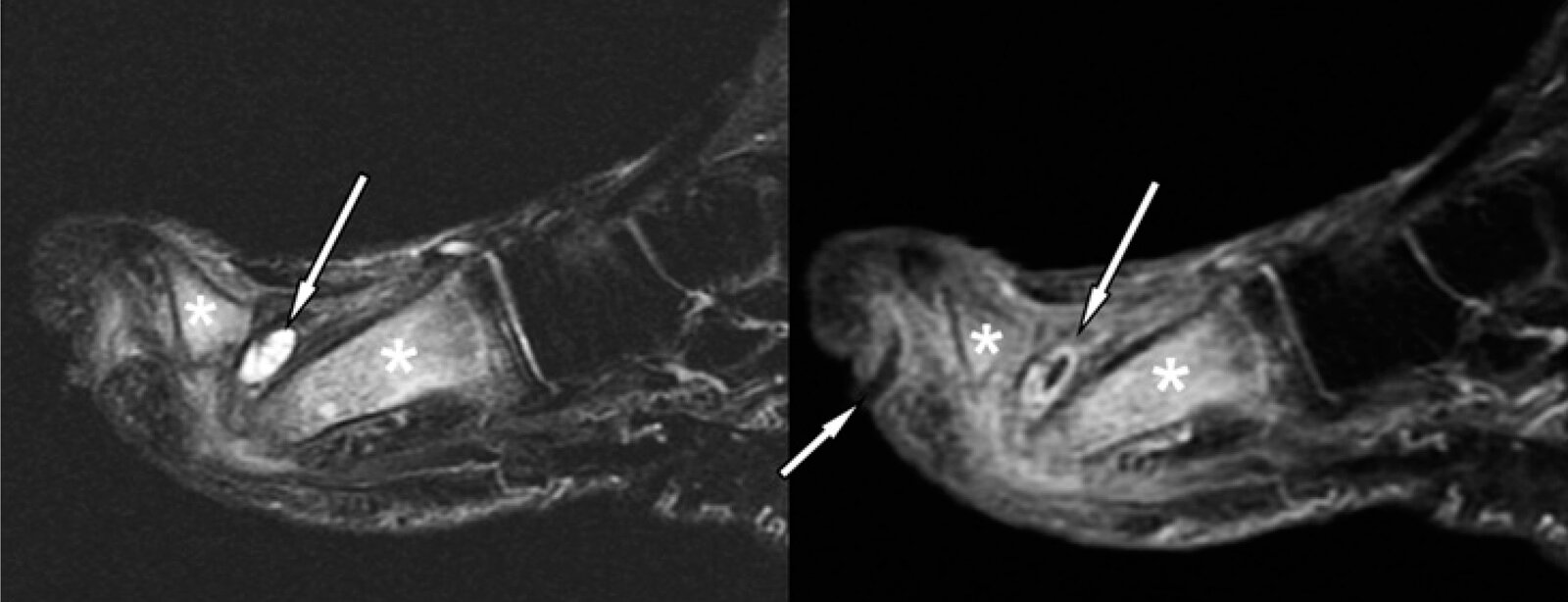
MRI foot (sagittal plane; fat-suppressed; left: T2-weighted; right: T1-weighted post-contrast) of a patient with diabetes
On the plantar surface of the first toe (great toe; big toe) an ulcer is visible, from which a peripherally-enhancing (hyperintense) sinus tract (right, short arrow) extends toward the interphalangeal joint.
An abscess dorsal to the head of the first metatarsal is seen as a hyperintense fluid collection on the T2-weighted sequence (left, long arrow) and as a peripherally-enhancing collection on the post-contrast T-1 weighted sequence (right, long arrow).
The first metatarsal (right asterisk on both images) and proximal phalanx (left asterisk on both images) show hyperintense edema (left) and contrast enhancement (right) indicative of osteomyelitis.
Source: “Fig. 3, in: Diabetic Foot Infections: The Diagnostic Challenges” by Lauri C, Leone A, Cavallini M, Signore S, Giurato L, Uccioli L, Journal of Clinical Medicine, licensed under CC BY 4.0.
Differential diagnoses
-
Septic arthritis
- Infection of the joint (in contrast to osteomyelitis, involvement of the metaphysis is rare)
- May occur secondary to osteomyelitis in infants
- Bone tumors (e.g., Ewing sarcoma, osteoid osteoma)
- Avascular bone necrosis
- Benign bone tumors (e.g., bone cyst)
- Fracture
The differential diagnoses listed here are not exhaustive.
Treatment
The following recommendations are for the treatment of nonvertebral osteomyelitis. For treatment of vertebral osteomyelitis, see “Treatment of spinal infections.”
Approach
- All patients
- Admit for IV antibiotics; consult infectious disease specialists to help guide choice of antibiotics. [16]
- Signs of sepsis or severe or rapidly progressing infection: Administer empiric antibiotic therapy for osteomyelitis.
- All other patients: Administer pathogen-directed antibiotic therapy for osteomyelitis once cultures are available.
- Provide pain management and supportive treatment to optimize bone healing.
- Consider trending inflammatory markers to monitor response to therapy. [18][19]
- Admit for IV antibiotics; consult infectious disease specialists to help guide choice of antibiotics. [16]
- Hematogenous osteomyelitis: Identify and treat the underlying infection.
- Consultations
- Relevant specialists for management of comorbidities (e.g., diabetic foot, sickle cell disease)
- Surgeons (orthopedic or vascular) to determine the need for surgery based on: [20]
- Extent of disease
- Presence of surgical hardware
- Patient comorbidities
Acute hematogenous osteomyelitis can typically be treated with antibiotic therapy alone. Management of acute osteomyelitis due to contiguous spread and chronic osteomyelitis usually requires surgical debridement of infected tissue. [18][21]
Antibiotic therapy [5][18][21]
- Empiric antibiotic therapy is rarely required.
- Start most patients directly on pathogen-directed antibiotics based on culture results.
- Consider switching to oral antibiotics after an initial IV course.
- Duration of therapy is normally 4–8 weeks. [10][18][21]
- Rarely, patients who are unsuitable for surgery remain on long-term suppressive antibiotic therapy. [18]
When indicated, obtain a bone biopsy preferably before administering antibiotic therapy to maximize diagnostic yield. [17]
Empiric antibiotic therapy for osteomyelitis
- Indications
- Signs of sepsis
- Severe or rapidly progressing infection
- Consider in diabetic foot osteomyelitis.
-
Empiric regimens for adults should cover: [22]
- S. aureus; (e.g., with vancomycin )
-
AND gram-negative bacilli, including Pseudomonas; recommended regimens include: ; [18]
- Meropenem
- OR cefepime PLUS metronidazole
- For empiric regimens in children, see “Osteomyelitis in children.”
Avoid giving vancomycin with piperacillin-tazobactam; while the combination provides cover against both S. aureus and Pseudomonas, it has a high risk of nephrotoxicity. [22]
Pathogen-directed antibiotics
| Pathogen-directed antibiotic therapy for osteomyelitis [5][10][18][21] | ||||
|---|---|---|---|---|
| Pathogen | First-line | Alternative | ||
| Staphylococcus spp. | Methicillin-susceptible S. aureus (MSSA) |
|
|
|
| Methicillin-resistant S. aureus (MRSA) [24] |
|
|
||
| Enterococcus spp. | Penicillin-susceptible |
|
|
|
| Penicillin-resistant |
|
|
||
| Enterobacteriaceae | Quinolone-sensitive |
|
|
|
| Quinolone-resistant |
|
|||
| Pseudomonas aeruginosa |
|
|
||
| Beta-hemolytic streptococci |
|
|
||
| Anaerobes |
|
|
||
| ||||
Supportive therapy [21]
- Treat patient factors that affect healing, e.g.:
- Optimize nutrition.
- Treat anemia.
- Manage coexisting medical comorbidities (e.g., diabetes).
- Treat any associated decubitus ulcers.
- Manage pain with analgesia, immobilization of affected area, and physiotherapy.
Surgery [21][25]
- Manage patient factors that may have impacted healing prior to surgery (e.g., anemia, poor nutrition).
- The decision for surgery should be made in consultation with infectious disease specialists.
- The choice of procedure depends on site of infection, presence of hardware, and patient factors (e.g., comorbidities).
- Continue antibiotic therapy after surgery, even if bone has been successfully debrided.
| Potential surgical interventions in osteomyelitis [10][21] | |
|---|---|
| Surgical intervention | |
| Chronic osteomyelitis |
|
| Acute osteomyelitis refractory to antibiotic treatment | |
| Infected prosthetic joint or foreign body |
|
| Posttraumatic osteomyelitis |
|
| Overlying abscess |
|
| Poor wound healing or limb ischemia |
|
Subtypes and variants
Brodie abscess
- Definition: subacute osteomyelitis characterized by an intraosseous abscess; commonly affects the distal femur and proximal tibia
- Pathophysiology: hematogenous seeding of a distant infectious focus → subacute or chronic pyogenic infection of the bone → fibrous and granulation tissue formation around pyogenic focus → localized abscess
-
Clinical features
- Frequently asymptomatic or only mild symptoms
- Localized pain
- Diagnostics: well-circumscribed, thick-walled cystic lesion in the metaphysis and epiphysis of long bones on x-ray and contrast-enhanced MRI
- Treatment: surgical drainage and antibiotics
Complications
-
Infectious
- Abscess
- Sequestrum
- Recurrent or chronic osteomyelitis
- Pyarthrosis: infiltration of nearby joints
- Sinus tracts
- Cellulitis
- Sepsis
-
Mechanical
- Progressive destruction of bone
- Pathological fractures
- Pseudarthrosis, abnormal bone healing
- Malignant: development of Marjolin ulcer [3]

We list the most important complications. The selection is not exhaustive.

Erythematous, purulent, ulcerating tumor with multiple sites of petechial bleeding on the elbow, distal upper arm, and proximal forearm.
Source: "Marjolin ulcer", Raj d0509, Wikimedia Foundation licensed under Public Domain
{kind=link}
Special patient groups
Osteomyelitis in children [10][19][27]
Overview [10]
- Most common form: acute hematogenous osteomyelitis
- Epidemiology: typically occurs in children < 5 years of age (♂:♀ 2:1) [28]
-
Risk factors
- In neonates: bacteremia
- Children > 3 months: immunodeficiency, sickle cell disease
- Common pathogens include:
- Staphylococcus aureus
- Group A Streptococcus
- Kingella kingae spp. (typically in children < 5 years of age) [10][29]
- Most commonly affected areas: metaphyses of the long bones (femur, tibia, humerus)
Clinical features [28]
- Fever
-
Limb pain, which may manifest as:
- Limp
- Reduced range of movement
- Refusal to use the limb (pseudoparalysis)
- In infants, multiple sites may be affected.
Diagnostics
- Similar to diagnostics for osteomyelitis in adults
Management of osteomyelitis in children [10][19]
Stable patients
- Most children can be managed with antibiotic therapy alone. [10]
- Initiation of antibiotics can be delayed up to 72 hours to allow tailoring of antibiotics to culture results.
- Duration of antibiotic therapy: 3–4 weeks [10][19]
- Consider referral for incision and drainage in patients with an abscess ≥ 2 cm in size.
Signs of sepsis in children or rapidly progressive infection
- Obtain blood cultures and start immediate empiric antibiotics.
- Urgent consultation with infectious diseases specialist for choice of empiric antibiotics; if a specialist is unavailable the following antibiotics are IDSA-recommended:
- Low prevalence MRSA area : cefazolin OR an antistaphylococcal agent (e.g., nafcillin , oxacillin ) [19]
- High prevalence MRSA area : options include clindamycin OR vancomycin [19]
- Urgent referral for debridement of infected bone and/or drainage of any abscess. [19]
Complications [27]
- Similar to those seen in adults (see “Complications”)
- The following are more common in children
- Increased risk of septic arthritis [28]
- Impaired growth and long-term limb deformity
- Pyomyositis [28]
- DVT and PE [27]
Maintain a high index of suspicion for osteomyelitis in children; delayed diagnosis and treatment can have detrimental effects on bone development, affecting growth and causing severe long-term impairment.
Prognosis
-
Acute osteomyelitis
- Quick, full recovery is common in children who receive appropriate antimicrobial treatment [30]
- Acute osteomyelitis in adults often transforms into chronic osteomyelitis.
-
Chronic osteomyelitis
- Difficult to cure
- Often requires repeated surgical and antibiotic treatment (over years to decades)
- In patients with diabetes or vascular insufficiency, the probability of complete resolution is particularly low. [31]
External Resources
References
- Kremers HM, Nwojo ME, Ransom JE, et al. "Trends in the epidemiology of osteomyelitis: a population-based study, 1969 to 2009". J Bone Joint Surg Am. 97(10). :837-45. (2015)
- Nickerson EK, Sinha R. "Vertebral osteomyelitis in adults: an update". Br Med Bull. 117(1). :121-138. (2016)
- Panteli M, Giannoudis PV. "Chronic osteomyelitis: what the surgeon needs to know". EFORT Open Rev. 1(5). :128-135. (2016)
- Hotchen AJ, McNally MA, Sendi P. "The Classification of Long Bone Osteomyelitis: A Systemic Review of the Literature". J Bone Jt Infect. 2(4). :167-174. (2017)
- Bury DC, Rogers TS, Dickman MM. "Osteomyelitis: Diagnosis and Treatment". Am Fam Physician. 104(4). :395-402. (2021)
- Allison DC, Holtom PD, Patzakis MJ, Zalavras CG. "Microbiology of bone and joint infections in injecting drug abusers". Clin Orthop Relat Res. 468(8). :2107-12. (2010)
- Olson ME, Horswill AR. "Staphylococcus aureus osteomyelitis: bad to the bone". Cell Host Microbe. 13(6). :629-31. (2013)
- Helm C, Huschart E, Kaul R, et al. "Management of Acute Osteomyelitis: A Ten-Year Experience". Infect Dis Rep. 8(3). :6350. (2016)
- Lew DP, Waldvogel FA. "Osteomyelitis". The Lancet. 364(9431). :369-379. (2004)
- Schmitt SK. "Osteomyelitis". Infect Dis Clin North Am. 31(2). :325-338. (2017)
- Lam K, van Asten SAV, Nguyen T, La Fontaine J, Lavery LA. "Diagnostic Accuracy of Probe to Bone to Detect Osteomyelitis in the Diabetic Foot: A Systematic Review". Clinical Infectious Diseases. 63(7). :944-948. (2016)
- Walter G, Kemmerer M, Kappler C, Hoffmann R. "Treatment algorithms for chronic osteomyelitis". Dtsch Arztebl Int. 109(14). :257-64. (2012)
- Niels van der, Diederik P.J. Smeeing, Roderick M. Houwert, et al. "Brodie's Abscess: A Systematic Review of Reported Cases". J Bone Jt Infect. 4(1). :33-39. (2019)
- Expert Panel on Musculoskeletal Imaging:., Beaman FD, von Herrmann PF, et al. "ACR Appropriateness Criteria® Suspected Osteomyelitis, Septic Arthritis, or Soft Tissue Infection (Excluding Spine and Diabetic Foot)". J Am Coll Radiol. 14(5S). :S326-S337. (2017)
- Walker EA, Beaman FD, Wessell DE, et al. "ACR Appropriateness Criteria® Suspected Osteomyelitis of the Foot in Patients With Diabetes Mellitus". J Am Coll Radiol. 16(11). :S440-S450. (2019)
- Pineda C, Espinosa R, Pena A. "Radiographic Imaging in Osteomyelitis: The Role of Plain Radiography, Computed Tomography, Ultrasonography, Magnetic Resonance Imaging, and Scintigraphy". Sem Plast Surg. 23(02). :080-089. (2009)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Hirschfeld CB, Kapadia SN, Bryan J, et al. "Impact of diagnostic bone biopsies on the management of non-vertebral osteomyelitis: A retrospective cohort study". Medicine (Baltimore). 98(34). :e16954. (2019)
- Fraimow HS. "Systemic Antimicrobial Therapy in Osteomyelitis". Seminars in Plastic Surgery. 23(02). :090-099. (2009)
- Woods et al. "Clinical Practice Guideline by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America: 2021 Guideline on Diagnosis and Management of Acute Hematogenous Osteomyelitis in Pediatrics". J Pediatric Infect Dis Soc. 10(8). :801-844. (2021)
- Marais LC, Ferreira N, Aldous C, Sartorius B, Le Roux T. "A modified staging system for chronic osteomyelitis". J Orthop. 12(4). :184-92. (2015)
- Rao N, Ziran BH, Lipsky BA. "Treating Osteomyelitis: Antibiotics and Surgery". Plastic & Reconstructive Surgery. 127. :177S-187S. (2011)
- Kolinsky DC, Liang SY. "Musculoskeletal Infections in the Emergency Department". Emerg Med Clin North Am. 36(4). :751-766. (2018)
- Rybak MJ, Lomaestro BM, Rotschafer JC, et al. "Vancomycin Therapeutic Guidelines: A Summary of Consensus Recommendations from the Infectious Diseases Society of America, the American Society of Health‐System Pharmacists, and the Society of Infectious Diseases Pharmacists". Clin Infect Dis. 49(3). :325-327. (2009)
- Liu C, Bayer A, Cosgrove SE et al. "Clinical Practice Guidelines by the Infectious Diseases Society of America for the Treatment of Methicillin-Resistant Staphylococcus Aureus Infections in Adults and Children". Clin Infect Dis. 52(3). :e18-55. (2011)
- Lipsky et al. "2012 Infectious Diseases Society of America Clinical Practice Guideline for the Diagnosis and Treatment of Diabetic Foot Infections". Clin Infect Dis. 54(12). :e132-e173. (2012)
- Le Saux N, Howard A, Barrowman NJ, et al. "Shorter courses of parenteral antibiotic therapy do not appear to influence response rates for children with acute hematogenous osteomyelitis: a systematic review". BMC Infect Dis. 2. :16. (2002)
- Berendt AR, Peters EJG, Bakker K, et al. "Diabetic foot osteomyelitis: a progress report on diagnosis and a systematic review of treatment". Diabetes Metab Res Rev. 24(S1). :S145-S161. (2008)
- Gornitzky AL, Kim AE, O’Donnell JM, Swarup I. "Diagnosis and Management of Osteomyelitis in Children". JBJS Rev. 8(6). :e19.00202-e19.00202. (2020)
- Thakolkaran N, Shetty AK. "Acute Hematogenous Osteomyelitis in Children". Ochsner J. 19(2). :116-122
- Yagupsky P. "Outbreaks of Kingella kingae infections in daycare facilities". Emerg Infect Dis. 20(5). :746-53. (2014)