Summary
Osteoporosis is a skeletal condition in which the loss of bone mineral density (BMD) leads to decreased bone strength and increased susceptibility to fractures. Postmenopausal women and older adults are often affected, as an abrupt decrease in estrogen and age-related processes play a key role in the development of osteoporosis. Additional risk factors include physical inactivity, a diet low in calcium and vitamin D, smoking, and alcohol consumption. Osteoporosis usually remains asymptomatic until the first occurrence of a fragility fracture (typically following minor trauma). Patients may also present with thoracic hyperkyphosis and height loss secondary to multiple vertebral compression fractures. Diagnostic evaluation includes BMD assessment (e.g., dual-energy x-ray absorptiometry), fracture risk assessment, and workup for common causes of secondary osteoporosis. Fractures are usually confirmed through conventional x-ray. Pharmacotherapy is indicated in patients who fulfill the diagnostic criteria for osteoporosis. Bisphosphonates, which inhibit bone resorption and can significantly decrease the risk of fractures, are the preferred first-line treatment. Nonbisphosphonates are indicated in patients who are unable to take bisphosphonates and those in whom bisphosphonate therapy has been unsuccessful. Prevention mainly comprises of adequate calcium and vitamin D intake and regular physical activity with strengthening exercises to maintain or even increase bone mass and improve balance, thereby reducing the risk of falls and fragility fractures. High-risk individuals should be offered screening for osteoporosis and pharmacotherapy should be initiated in those with osteopenia at a high risk of fractures.
Definitions
- Osteoporosis: loss of trabecular and cortical bone mass which leads to bone weakness and increased susceptibility to fractures
- Osteopenia: decreased bone strength but less severe than osteoporosis
Epidemiology
- Sex: ♀ > ♂ (∼ 4:1)
- Age of onset: 50–70 years
- Demographics: higher incidence in individuals of Asian, Hispanic, and northern European ancestry [1]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Primary osteoporosis (most common)
-
Type I (postmenopausal osteoporosis): postmenopausal women [2][3]
- Estrogen stimulates osteoblasts and inhibits osteoclasts.
- The decreased estrogen levels following menopause lead to increased bone resorption.
- Type II (senile osteoporosis): gradual loss of bone mass as patients age (especially > 70 years)
-
Idiopathic osteoporosis
- Idiopathic juvenile osteoporosis [4]
- Idiopathic osteoporosis in young adults [5]
Secondary osteoporosis
-
Drug-induced/iatrogenic
- Most commonly due to systemic long-term therapy with corticosteroids (e.g., in patients with autoimmune disease) [3]
-
Long-term therapy involving: [6]
- Anticonvulsants (e.g., phenytoin, carbamazepine)
- L-thyroxine
- Anticoagulants (e.g., heparin)
- Proton pump inhibitors
- Aromatase inhibitors (e.g., anastrozole, letrozole)
- Immunosuppressants (e.g., cyclosporine, tacrolimus)
- Androgen deprivation therapy (ADT)
- Endocrine/metabolic: hypercortisolism, hypogonadism, hyperthyroidism, hyperparathyroidism, renal disease
- Multiple myeloma
Additional risk factors [7]
- Excessive alcohol consumption
- Cigarette smoking
- Immobilization or inadequate physical activity
- Malabsorption (e.g., celiac disease), malnutrition (e.g., diet low in calcium and vitamin D), anorexia [8]
- Low body weight
- Family history of osteoporosis
- Personal history of fracture
Clinical features
- Mostly asymptomatic
-
Fragility fractures: pathological fractures that are caused by everyday-activities (e.g., bending over, sneezing) or minor trauma (e.g. falling from standing height) [9]
- Common locations of major osteoporotic fractures: vertebral (most common) > femoral neck > distal radius (Colles fracture) > other long bones (e.g., humerus)
-
Vertebral compression fractures
- Commonly asymptomatic but may cause acute back pain and possible point tenderness without neurological symptoms
- Multiple fractures can lead to decreased height and thoracic kyphosis.
- See “Vertebral fractures” for more information.

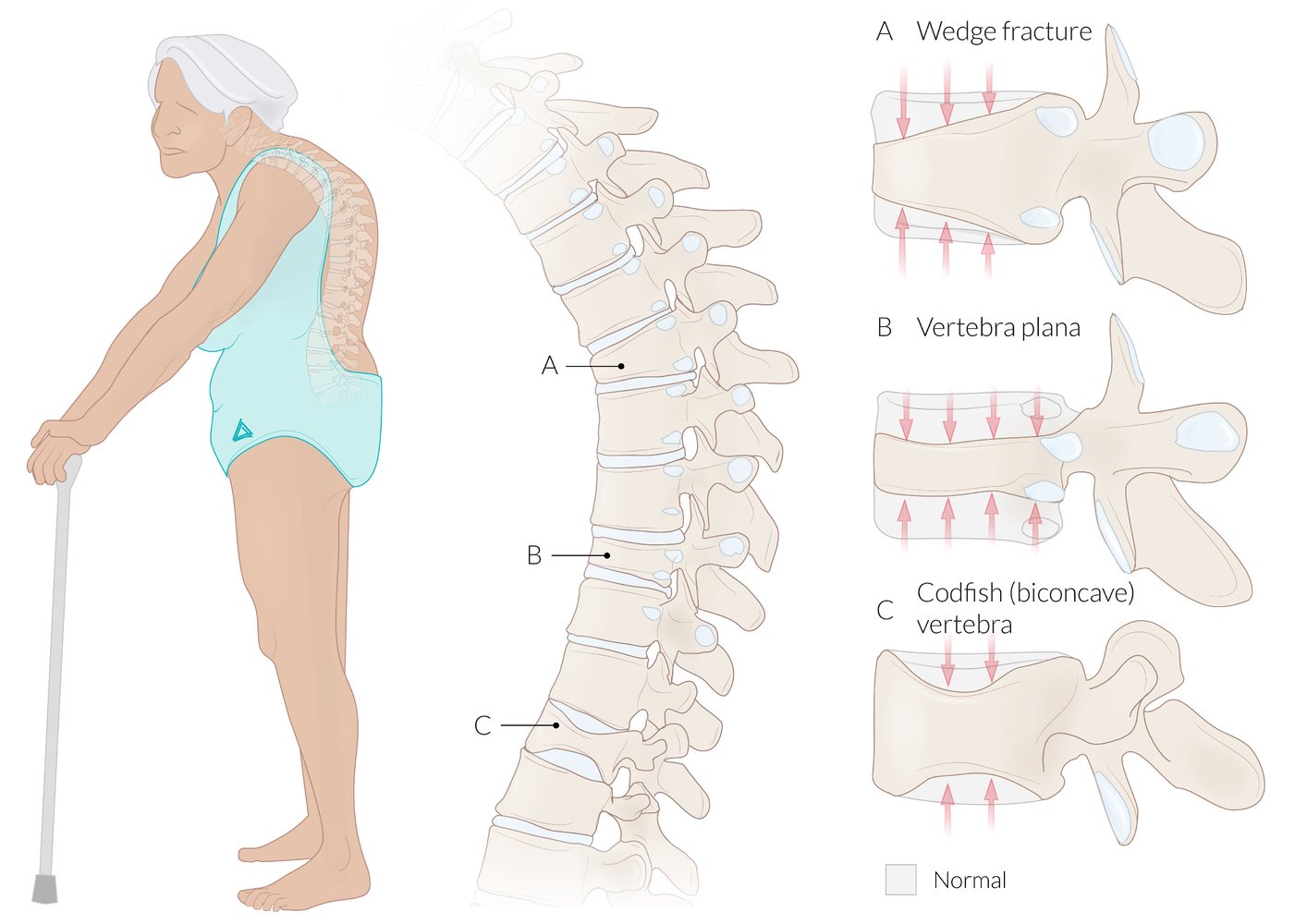
(A) Wedge fracture: characterized by a loss of height, predominantly of the anterior part of the vertebral body. Wedge fractures are common in individuals with osteoporosis, and they can lead to a kyphotic deformity of the spine (gibbus) if multiple vertebrae are involved.
(B) Vertebra plana: an advanced compression fracture where there is a loss of height of the entire vertebral body, both anteriorly and posteriorly. Vertebra plana is also referred to as a pancake or coin-on-edge vertebra.
(C) Codfish vertebra: characterized by loss of height of the central part of the vertebral body, resulting in a biconcave vertebral body that resembles fish vertebrae.
© AMBOSS
Screening
Indications [10]
- Screening is recommended in:
- Women ≥ 65 years of age
- Postmenopausal women < 65 years of age with ≥ 1 risk factor for osteoporosis
- Individuals with a history of low-trauma fracture after 50 years of age [11]
- There is insufficient evidence to recommend routine screening for osteoporosis in men; consider screening:
- Younger men with risk factors for osteoporosis (e.g., long-term corticosteroid use; ADT for prostate cancer) [12][13]
- Men ≥ 70 years of age [7][12][14]
The majority of screening and prevention recommendations are for women; consult an endocrinologist for men with suspected osteoporosis.
Modality [10]
- ≥ 65 years of age: BMD assessment; DXA of lumbar spine and hips is preferred. [10][11][15]
-
< 65 years of age
- Stratify patients using an osteoporosis risk assessment tool, e.g., FRAX.
- For patients with a clinically significant risk of osteoporosis, obtain BMD assessment.
Further management
- If the diagnostic criteria for osteoporosis are fulfilled, start treatment for osteoporosis.
- For all other patients: [16]
- Optimize bone health and discuss fall prevention.
- For high-risk individuals : Start pharmacotherapy for osteoporosis prevention. [11]
- Reassess BMD at regular intervals.
- There is a paucity of data on the value and optimal timing of repeating the BMD assessment.
- Determine the need for and frequency of screening intervals on an individual basis based on the initial BMD (T-score) and development of new risk factors for osteoporosis or fractures.
| Suggested frequency of osteoporosis screening [16] | |
|---|---|
|
T-score (in SD) |
Intervals |
| -2.0 to -2.4 | within 3 years |
| -1.5 to -1.9 | 3–5 years |
| -1.0 to -1.4 | 5–10 years |
| > -1.0 | > 10 years |
Short-interval (within 2–3 years) reassessment of BMD in individuals who do not fulfill the diagnostic criteria for osteoporosis is not routinely recommended. [7][16]
Diagnosis
Approach [11]
Osteoporosis is typically identified during screening in high-risk individuals (see “Screening for osteoporosis”).
- Assess BMD and estimate the risk of major osteoporotic fracture.
- The diagnosis is confirmed if any of the following diagnostic criteria for osteoporosis are fulfilled. [11]
- T-score ≤ -2.5 standard deviations (SDs) on dual-energy x-ray absorptiometry (DXA)
- T-score -1 to -2.5 SD in patients at increased risk of major osteoporotic fracture
- History of a major osteoporotic fragility fracture (regardless of BMD)
-
Once confirmed:
- Consider screening all patients for common causes of secondary osteoporosis.
- Evaluate high-risk patients for vertebral fractures.
- Consider bone turnover markers (BTMs) to assess fracture risk and monitor treatment response.
Osteoporosis is diagnosed in patients with a T-score ≤ -2.5 SD and/or a fragility fracture. [11]
Bone mineral density (BMD) assessment [11][15]
Indications
- Evaluation of suspected osteoporosis
- Screening for osteoporosis in asymptomatic high-risk individuals
Preferred modality: dual-energy x-ray absorptiometry
DXA measures BMD; at the lumbar spine and hip/femoral neck using two x-ray beams. Findings are represented in terms of BMD scores that compare results to a reference population.
| BMD scores [11][15] | |
|---|---|
| Postmenopausal women and men > 50 years of age |
|
| All other individuals |
|
DXA evaluates bone quantity. The trabecular bone score uses data from DXA images to evaluate bone quality and may sometimes be used to further stratify fracture risk. [17]

Alternatives [15]
These studies are most commonly used when conventional DXA is unavailable.
- Peripheral DXA: measures BMD at the distal forearm
-
Quantitative computed tomography
- Provides a volumetric measurement of BMD at the lumbar spine and hip
- Can measure density of trabecular bone
- May be superior to DXA in patients with: [15]
- Very tall or very short stature
- Significant degenerative disk disease
- BMI > 35 kg/m2
- Close monitoring of trabecular bone density changes (e.g., chronic glucocorticoid use, parathyroid hormone therapy)
Fracture risk assessment [11]
- Several calculators are used to estimate fracture risk during the diagnostic workup or screening for osteoporosis.
- FRAX (commonly used; see “Tips and Links”): estimates the 10-year probability of a major osteoporotic fracture [11][14]
Laboratory studies [7][11]
Consider screening all patients with newly diagnosed osteoporosis for common causes of secondary osteoporosis and potential contraindications for certain pharmacotherapy.
-
Routine studies
- CBC, CMP, PTH, phosphate, and serum 25-hydroxyvitamin D
- 24-hour urine to measure calcium, creatinine, and sodium levels
-
Additional studies
- Evaluate for specific etiologies of secondary osteoporosis as guided by clinical assessment (e.g., celiac antibodies, TSH, myeloma screen).
- Consider BTMs to assess fracture risk and monitor treatment response. [11][18]
-
Findings
- Primary osteoporosis: Serum calcium, phosphate, and parathyroid hormone (PTH) levels are usually normal
- Secondary osteoporosis: See “Laboratory findings in common bone disorders” and/or relevant articles for details.
Treat vitamin D deficiency and ensure at least 2 weeks of recommended daily intake of calcium before obtaining 24-hour urine calcium. [11]
Screening for vertebral fractures [11][15][19][20]
Vertebral fractures are common in patients with osteoporosis, asymptomatic in up to two-thirds of cases, and associated with a high risk of future fractures.
-
Indications: T-score ≤ -1.0 in individuals with one or more of the following [11][19]
- Women ≥ 70 years of age or men ≥ 80 years of age
- Height loss of ≥ 4 cm (> 1.5 inches)
- Undocumented (self-reported) prior vertebral fracture
- Kyphosis
- Recent long-term glucocorticoid therapy
-
Modalities [11][15]
- Vertebral fracture assessment (VFA): uses DXA to assess for vertebral fractures
- Lateral thoracic and lumbar spine x-ray
-
Supportive findings (on x-ray)
- Increased radiolucency and cortical thinning [21]
- Vertebral compression fractures




Imaging for other skeletal fractures [11][22]
-
Indications
- Symptoms of fracture (e.g., pain, limited mobility)
- Thigh or groin pain in patients on long-term (∼ 5 years) bisphosphonate therapy [23]
-
Modalities
- First line: plain x-ray
- Second-line : Consider MRI or CT.
-
Supportive findings
- Radiographic signs of a fracture
- Atypical femoral fractures: Transverse noncomminuted fracture of the subtrochanteric region or shaft of the femur [24]
- Increased radiolucency (on x-ray/CT) and cortical thinning [21]


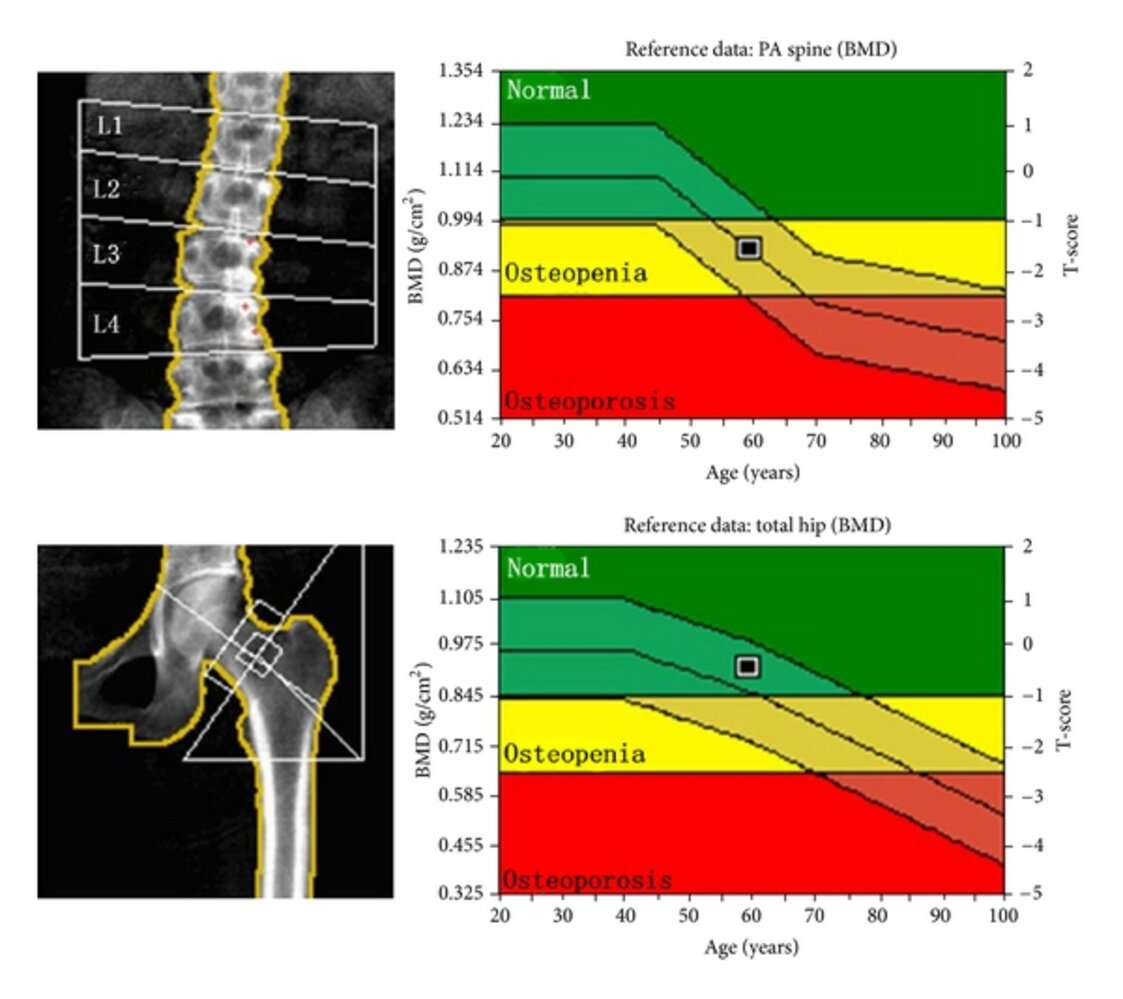
Dual-energy x-ray absorbtiometry (DXA) scan of a 59-year-old female patient
The T-scores are -1.6 for the lumbar spine (top image) and -0.5 for the femoral neck (bottom image). The graph indicates the T-score values for osteopenia (-1 to -2.5) and osteoporosis (≤ -2.5); since the lower T-score is used for diagnostic categorization, this patient meets the criteria for osteopenia. The three lines on the graph indicate the 90th, 50th, and 10th percentile for bone density of the reference population over time.
BMD: bone mineral density
T-score: the difference in standard deviations between the patient's BMD and the BMD of a young adult female reference mean
Source: “Fig. 2, in: Comparison of QCT and DXA: Osteoporosis Detection Rates in Postmenopausal Women” by Na Li, Xin-min Li, Li Xu, Wei-jie Sun, Xiao-guang Cheng, Wei Tian, International Journal of Endocrinology, licensed under CC BY 3.0.

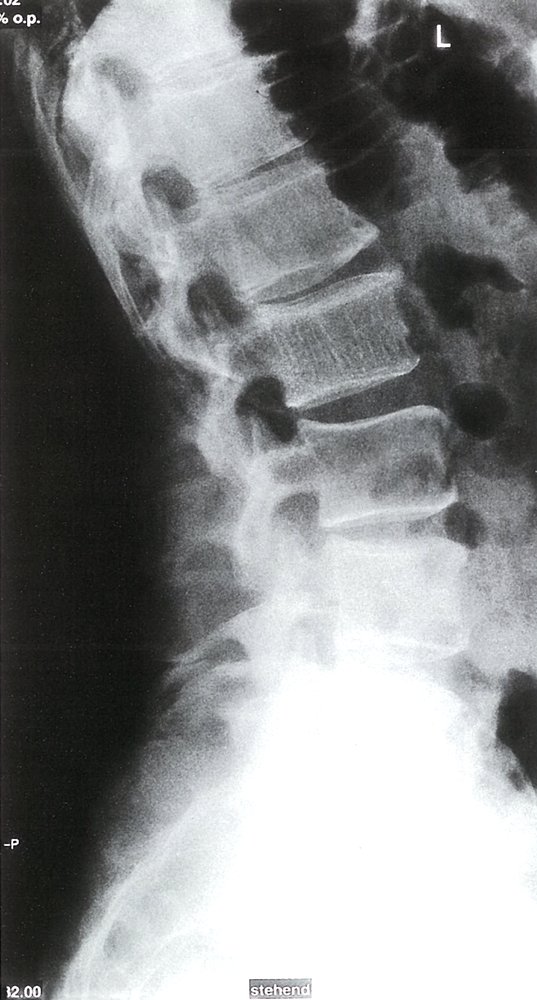
X-ray lumbar spine (lateral view) of a patient with osteoporosis
The vertebrae have a low-density appearance as a result of the loss of trabecular bone, and the cortical outline (example indicated by white line) of each vertebra appears accentuated. Other findings that may be seen on a spine radiograph in osteoporosis include an accentuated trabecular pattern and biconcave or compressed vertebral configuration.
Source: “Fig. 1, in: Imaging Findings and Evaluation of Metabolic Bone Disease” by Anish A. Patel, Rohit Ramanathan, Joshua Kuban et al., Hindawi, licensed under CC BY 3.0. Modifications: Flipped the image to face left Deleted letter L. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
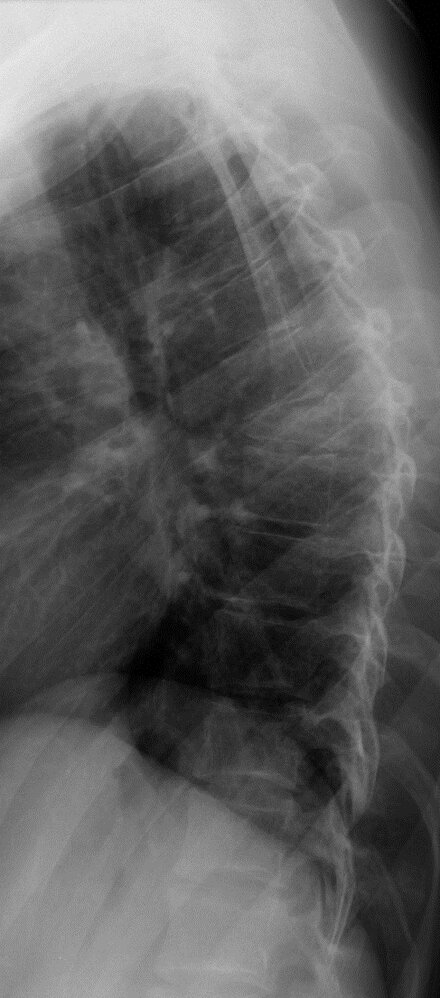
X-ray thoracic spine (lateral view) of a patient with osteoporosis
There is an insufficiency fracture of the T7 vertebral body, which is anteriorly wedged (green overlay) and accompanied by anterior subluxation (arrow) of the T6 vertebral body.
Wedge compression deformities are frequently osteoporotic, although alternatively may be pathologic (secondary to a focal bone lesion) or traumatic.
Red dashed outlines: normal vertebrae
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.

X-ray lumbar spine (lateral view)
There is a chronic compression deformity (red dimension line) of the L4 vertebral body, with displacement (red overlay) toward the spinal canal beyond the posterior vertebral lines of L3 and L5 (white dotted line). Exuberant anterior osteophyte formation is visible at L3–4 (red dotted lines).
Source: © IMPP

MRI lumbar spine (left: STIR image; right: T1-weighted; sagittal plane)
Compression deformities of the T8, T10, and L4 vertebrae (green overlays) are visible. The T8 and T10 fractures are hyperintense on the STIR image, indicating that they are recent. The compressed superior endplate of L4 is iso- to hypointense, indicating an old or chronic deformity. The hypointense appearance of the L2–3 intervertebral disc (green circle) on the STIR image indicates disc degeneration.
Source: © IMPP

X-ray right femur (AP view) of a patient with multiple myeloma treated with intravenous bisphosphonate therapy
An oblique fracture is seen in the subtrochanteric region of the right femur (indicated by arrows).
Atypical femoral fractures (AFFs; bisphosphonate-related proximal femoral fractures) are uncommon stress or insufficiency fractures, occurring in the femoral shaft.
Source: “Fig. 1b, in: Bilateral Atypical Femoral Fractures in a Patient with Multiple Myeloma Treated with Intravenous Bisphosphonate Therapy” by Ichiro Tonogai; Tomohiro Goto; Daisuke Hamada et al., Case Reports in Orthopedics, licensed under CC BY 4.0. Modifications: - cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
Pathology
- Thin, disconnected trabecular structures
- Attenuated, pitted cortical bone
- Increased osteoclast number and activity
Differential diagnoses
- Osteomalacia
- Hyperparathyroidism
- Metastases
- Multiple myeloma
- Intraosseous hemangioma


The differential diagnoses listed here are not exhaustive.
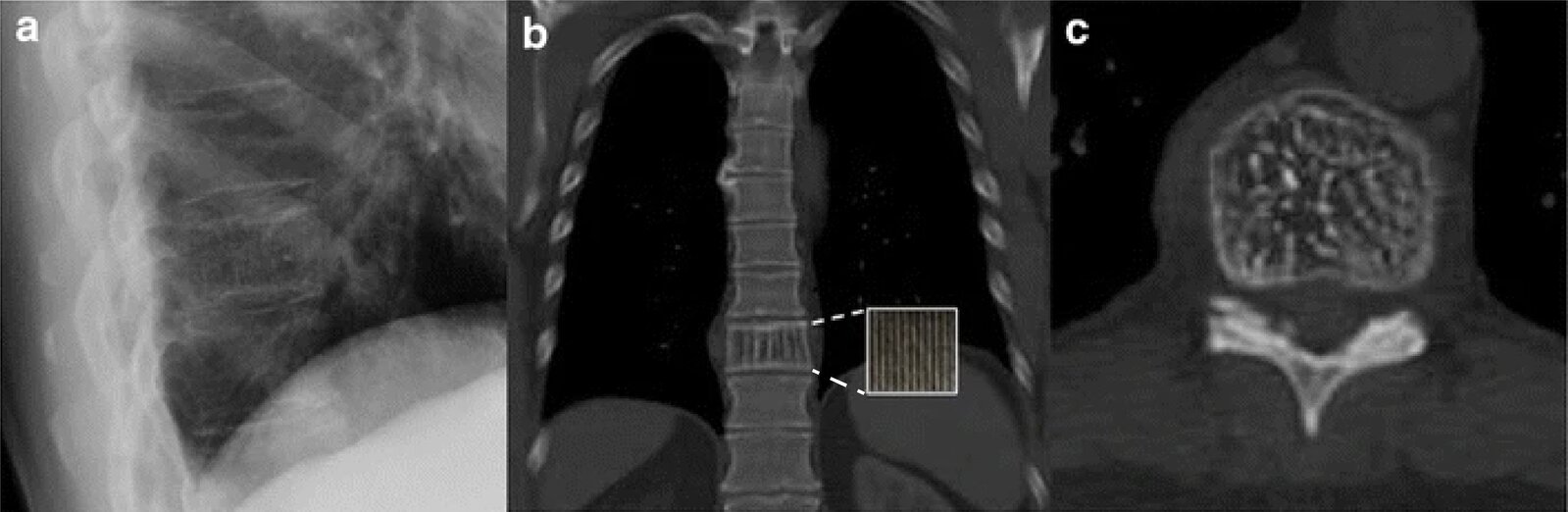
X-ray chest (A: lateral view) and CT chest (without contrast; B: coronal plane; C:axial plane)
The T10 vertebral body (green dashed outline) has a vertically striated (corduroy) appearance (examples indicated by yellow overlay) on both the lateral radiograph and the coronal CT section and a dotted (salt and pepper) appearance (examples indicated by red overlay) on the axial CT section.
Vertebral hemangiomas often have a characteristic imaging appearance. Vertical striations are the result of thickening of the bony trabeculae and produce a dotted appearance if imaged en face.
Source: “Fig 1, In: The clothes maketh the sign” by Buckley B, Chan VO, Mitchell DP et al., SpringerLink, licensed under CC BY 4.0. Modifications: Adjusted the dashed line of the zoom box. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Standing X-ray of the lumbar spine: L2 shows hypertrophic sclerosis of the vertical trabeculae, which indicates an intraosseous hemangioma.
Source: © IMPP
Treatment
Approach [7][11]
- All patients: Optimize bone health.
- Older patients: Assess for and manage risk factors for falls. [7][25]
- Discuss fall prevention strategies.
- Identify and manage risk factors for falls using the CDC STEADI algorithm for falls.
- Recommend individual and/or group exercise interventions that incorporate strength and balance training.
- Refer to physical and/or occupational therapy as needed.
- Start pharmacotherapy in the following situations:
- Diagnostic criteria for osteoporosis fulfilled
- Patients with osteopenia at increased risk of major osteoporotic fracture in the next 10 years
- See also “Introduction to geriatrics” for general information on the prevention of falls in older individuals.
Pharmacotherapy for osteoporosis [11][26][27]
Indications [11]
- Treatment: patients who fulfill any of the diagnostic criteria for osteoporosis
- Prevention: patients with osteopenia and an increased probability of a major osteoporotic fracture in the next 10 years (as determined on a clinical risk assessment tool such as the FRAX)
General principles [11]
- Bisphosphonates are preferred first-line agents.
- Consider nonbisphosphonates as first-line alternatives in certain situations or as second-line agents if bisphosphonate therapy is unsuccessful or not tolerated.
- Combination therapy with agents of different classes is currently not recommended.
-
Agents approved for osteoporosis treatment in men [12]
- Alendronate, risedronate, zoledronic acid, and teriparatide
- Denosumab is approved for men receiving ADT for prostate cancer.
-
Agents approved for glucocorticoid-induced osteoporosis [7][11][28]
- Bisphosphonates, denosumab, and teriparatide
- Teriparatide may be more effective at preventing vertebral fractures in this patient group than the other agents.
Bisphosphonates for osteoporosis [7][11]
- Indications: : preferred initial treatment in all patients [7][11][23][28]
- Mechanism of action: inhibition of osteoclasts, which are involved in bone resorption
-
Agents: The following are approved for both prevention and treatment of osteoporosis.
- Alendronate [7][11]
- Risedronate [7][11]
- Ibandronate (only FDA-approved for postmenopausal women) [7][11]
- Zoledronic acid [7][11]
-
Adverse effects [7][29]
- Osteonecrosis of the jaw
- Atypical femoral fractures
- Esophagitis
- Hypocalcemia
- See also “Contraindications to bisphosphonate therapy” and “Duration of pharmacotherapy for osteoporosis.”
Oral bisphosphonates should be taken in the morning with plenty of water at least 30 minutes before food and other medication, and the patient should maintain an upright position for at least 30 minutes after intake to prevent esophagitis. [14]
Alendronate, risedronate, and zoledronic acid reduce hip, vertebral, and nonvertebral fracture risk; ibandronate reduces vertebral fracture risk only. [7]
Nonbisphosphonates [7][11][23]
-
General indications
- Alternative first-line agents in patients with contraindications to bisphosphonate therapy
- Second-line agents in those who do not improve with bisphosphonates or are unable to tolerate bisphosphonate therapy (e.g., due to adverse effects)
- Specific indications: detailed below
| Nonbisphosphonates for the treatment of osteoporosis [7][11][23] | |||
|---|---|---|---|
| Specific indications [11][12] | Mechanism of action | Potential adverse effects | |
| Denosumab [7][11] |
|
|
|
PTH and PTH-related protein analogues
|
|
|
|
| Romosozumab [33] |
|
|
|
| Raloxifene [7] |
|
|
|
| Calcitonin [11] |
|
|
|
| Hormonal therapy |
|
|
|
Estrogen is not approved for the treatment of osteoporosis in women; if estrogen is prescribed to a patient with a uterus, it should always be combined with progesterone therapy to reduce the risk of endometrial hyperplasia. [11][23]


Monitoring and follow-up [11][14][23]
- Regularly review patients to assess for problems with adherence; see “Managing chronic conditions.”
- Consider BTMs to assess treatment efficacy and adherence. [11]
- Measure height yearly; if there is a ≥ 2 cm height loss, repeat imaging for vertebral fractures.
- Obtain DXA every 1–2 years for patients on treatment to monitor response. [11]
- Markers of improvement: stable or increasing BMD, no new fractures, normal or low BTMs
- If there is inadequate improvement : [11]
- Consider alternative agents or reevaluate for secondary osteoporosis.
- Consider referral to a clinical endocrinologist or osteoporosis specialist, if available.
| Duration of pharmacotherapy for osteoporosis [11] | ||
|---|---|---|
| Duration of therapy | Additional considerations | |
| Bisphosphonates |
|
|
| Abaloparatide, teriparatide |
|
|
| Romosozumab |
|
|
| Denosumab |
|
|
The benefits of nonbisphosphonates are lost rapidly after discontinuation; initiate another treatment for osteoporosis after cessation. [11][14]
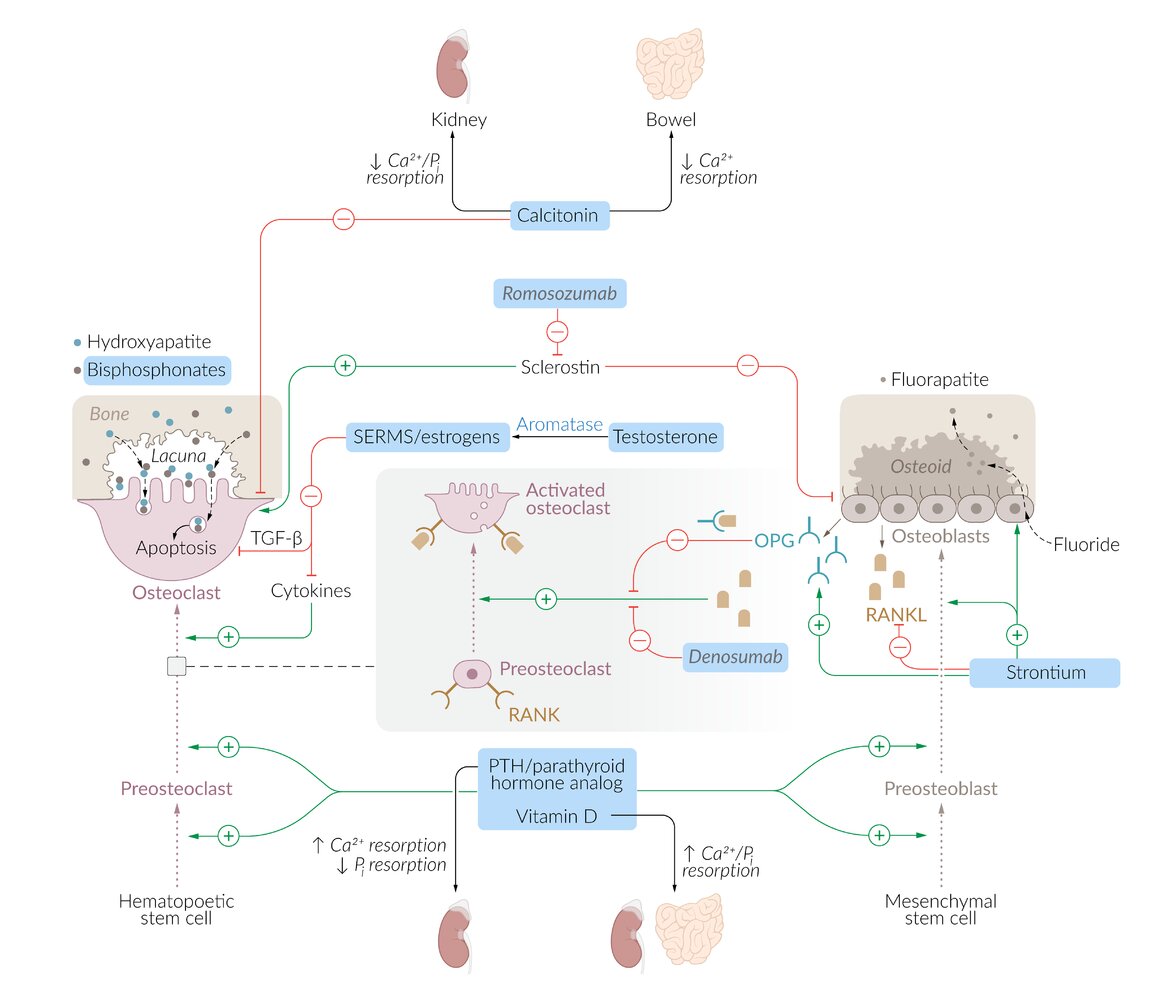
– Calcitonin: inhibits osteoclast activity and reduces renal and gastrointestinal resorption of calcium
– Romosozumab: a monoclonal antibody that binds sclerostin, promoting bone formation and inhibiting bone resorption
– Selective estrogen receptor modulators (SERMs; e.g., raloxifene) and estrogens: suppress chemical mediators (e.g., cytokines, TGFb), resulting in inhibition of osteoclast bone resorption and promotion of osteoclast apoptosis
– Bisphosphonates (alendronate, risedronate): inhibit osteoclast activity and, therefore, bone resorption
– RANKL inhibitors (denosumab): bind to RANKL, preventing it from activating osteoclasts via the RANK receptor
– Strontium: activates osteoblasts and stimulates them to produce osteoprotegerin (OPG), which inhibits RANK-RANKL binding
– PTH/parathyroid analogs (teriparatide): promote both osteoblast and osteoclast activity but with the net result of increased bone mass
– Vitamin D: increases absorption of calcium and phosphate from the gastrointestinal tract
© AMBOSS

The underlying bone is exposed in a tooth gap, and the surrounding gums are inflamed, swollen, and erythematous.
These findings, together with a history of long-term therapy with antiresorptive medications (e.g., bisphosphonates or RANKL inhibitors), are highly suggestive of medication-related osteonecrosis of the jaw. Dental surgery and pressure points from dentures are common triggers for such lesions.
Source: “Stage 2 MRONJ” by Coronation Dental Specialty Group, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}

Teeth of a 65-year-old patient 3 weeks after a tooth extraction; medication history included bisphosphonates and denosumab.
On the left mandible, a 2.5–3 cm area of the alveolar process surrounding the extraction site is completely exposed and appears necrotic.
In patients with a history of long-term therapy with antiresorptive medications (e.g., bisphosphonates or RANKL inhibitors such as denosumab), this appearance is highly suggestive of medication-related osteonecrosis of the jaw. Common triggers for such lesions include dental surgery and pressure points from dentures.
Source: “Fig. 2, in: Denosumab Related Osteonecrosis of the Jaw with Spontaneous Necrosis of the Soft Palate: Report of a Life Threatening Case” by Qaisi M, Hargett J, Loeb M, Brown J, Caloss R, Case Reports in Dentistry, licensed under CC BY 4.0.
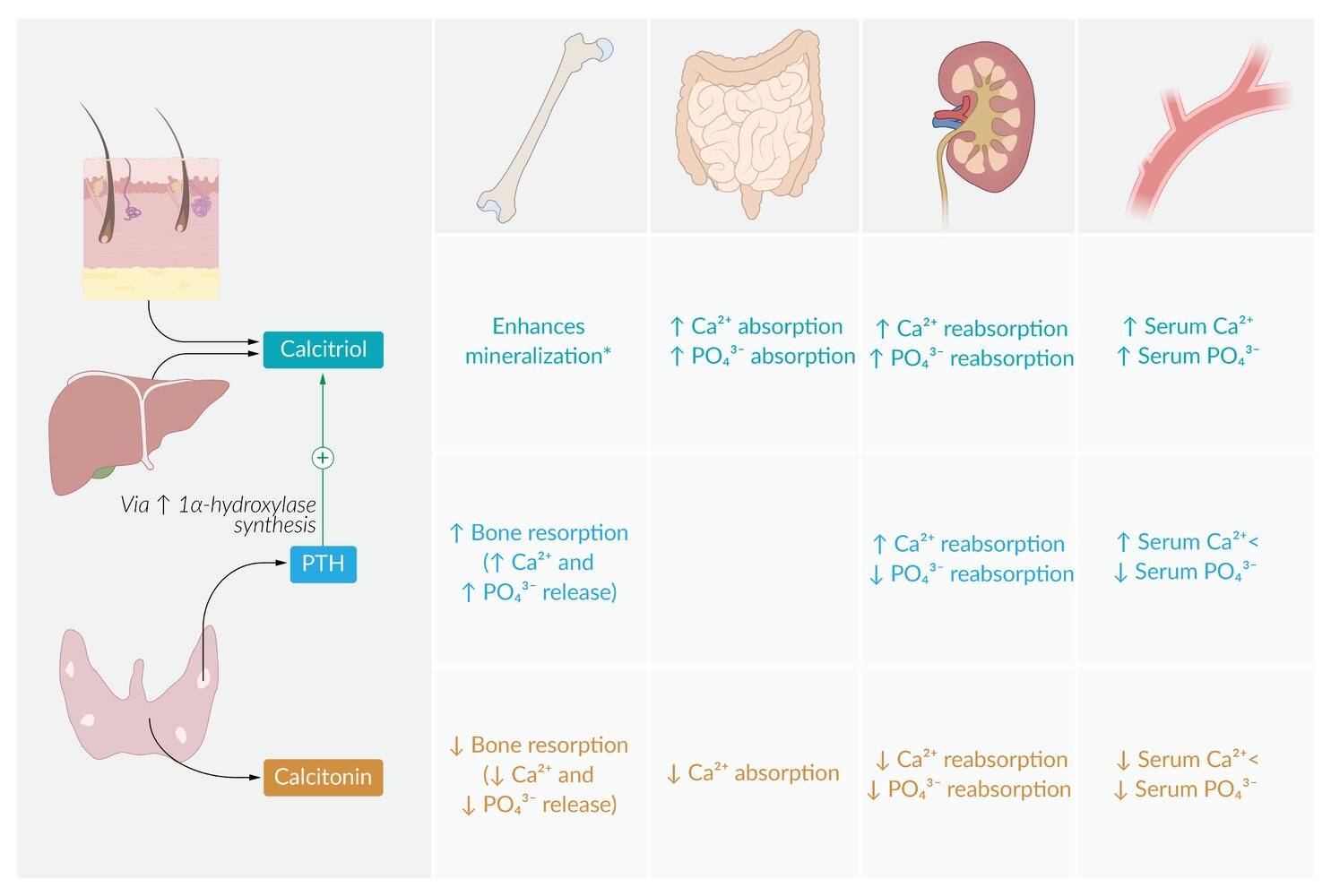
When serum calcium levels decrease, parathyroid chief cells secrete parathyroid hormone (PTH), which regulates calcium levels via the following mechanisms:
1. PTH activates osteoclasts, which degrade bone, thereby releasing calcium and phosphate.
2. In the kidneys, PTH stimulates calcium reabsorption in the distal tubule and decreases phosphate reabsorption in the proximal tubule.
3. PTH increases the expression of 1α-hydroxylase in the kidneys, an enzyme required to synthesize calcitriol. Calcitriol, in turn, stimulates renal and intestinal reabsorption of both calcium and phosphate. In contrast to PTH, calcitriol promotes the mineralization of bone using calcium and phosphate.
© AMBOSS
Prevention
General measures [7][14]
-
Optimize calcium and vitamin D intake.
- Recommended daily intake of calcium: 1000–1200 mg [14]
- Recommended daily intake of vitamin D: 800–1000 IU [14]
- Treat vitamin D deficiency.
- Encourage physical activity, including strength (resistance) and balance training.
- Avoidance or minimization of the following:
- Tobacco use: See “Counseling on smoking cessation.”
- Excessive alcohol consumption: See “Counseling on alcohol abuse.”
- Glucocorticoid use; see also “Measures to prevent complications of steroid therapy” [38]
Pharmacotherapy for osteoporosis prevention [39]
- Indication: individuals with osteopenia who are at high risk for osteoporotic fractures [11]
- Preferred agents: bisphosphonates (see “Bisphosphonates for osteoporosis” for dosages) [11]
- Alternatives for postmenopausal women in whom bisphosphonates are inappropriate or who desire pharmacotherapy for management of menopause symptoms [11][40][41]
- Raloxifene [11]
- Consider estrogen or conjugated estrogen/bazedoxifene; see “Hormone replacement therapy” for dosages and details.
Related One-Minute Telegram
- One-Minute Telegram 115-2025-2/3: Bone up on the updated USPSTF recommendations for osteoporosis screening to prevent fragility fractures
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- Sign up for the One-Minute Telegram
- 2025 USPSTF Recommendation on Screening for Osteoporosis to Prevent Fractures
- 2023 ACP Living Guideline for the Pharmacologic Treatment of Primary Osteoporosis or Low Bone Mass
- 2022 ACR Appropriateness Criteria® Osteoporosis and Bone Mineral Density
- 2020 AACE/ACE Clinical Practice Guidelines for the Diagnosis and Treatment of Postmenopausal Osteoporosis
- 2020 Pharmacological Management of Osteoporosis in Postmenopausal Women: An Endocrine Society Guideline Update
- 2018 EAA Clinical Guideline on Management of Bone Health in the Andrological Outpatient Clinic
- 2012 Osteoporosis in Men: An Endocrine Society Clinical Practice Guideline
- FRAX ®Fracture Risk Assessment Tool
References
- "Percentage of Adults Aged 65 and Over With Osteoporosis or Low Bone Mass at the Femur Neck or Lumbar Spine: United States, 2005–2010". https://web.archive.org/web/20200723075407/https://www.cdc.gov/nchs/data/hestat/osteoporsis/osteoporosis2005_2010.htm
- Karlamangla AS, Burnett-Bowie SAM, Crandall CJ. "Bone Health During the Menopause Transition and Beyond". Obstet Gynecol Clin North Am. 45(4). :695-708. (2018)
- Pouresmaeili F, Kamali Dehghan B, Kamarehei M, Yong Meng G. "A comprehensive overview on osteoporosis and its risk factors". Ther Clin Risk Manag. Volume 14. :2029-2049. (2018)
- "Juvenile Osteoporosis". https://www.bones.nih.gov/health-info/bone/bone-health/juvenile/juvenile-osteoporosis. [2018-10-01]
- Rozenberg S, Bruyère O, Bergmann P, et al. "How to manage osteoporosis before the age of 50". Maturitas. 138. :14-25. (2020)
- Panday K, Gona A, Humphrey MB. "Medication-induced osteoporosis: screening and treatment strategies". Ther Clin Risk Manag. 6(5). :185-202. (2014)
- Jeremiah MP, Unwin BK, Greenawald MH, Casiano VE. "Diagnosis and Management of Osteoporosis". Am Fam Physician. 92(4). :261-8. (2015)
- Rogerson D. "Vegan diets: practical advice for athletes and exercisers". J Int Soc Sports Nutr. 14(1). (2017)
- Piccirilli E, Cariati I, Primavera M, et al. "Augmentation in fragility fractures, bone of contention: a systematic review". BMC Musculoskelet Disord. 23(1). (2022)
- Camacho PM, Petak SM, Binkley N, et al. "American Association of Clinical Endocrinologists/American College of Endocrinology Clinical Practice Guidelines for the Diagnosis and Treatment of Postmenopausal Osteoporosis—2020 Update". Endocr Pract. 26(Supp 1). :1-46. (2020)
- Joseph SY, Nidhi GK, Michael GF et al. "Osteoporosis and Bone Mineral Density". J Am Coll Radiol. (2022)
- Harvey NC, Glüer CC, Binkley N, et al. "Trabecular bone score (TBS) as a new complementary approach for osteoporosis evaluation in clinical practice.". Bone. 78. :216-24. (2015)
- Cosman F, de Beur SJ, LeBoff MS, et al. "Clinician’s Guide to Prevention and Treatment of Osteoporosis". Osteoporos Int. 25(10). :2359-2381. (2014)
- Bauer DC. "Clinical Use of Bone Turnover Markers". JAMA. 322(6). :569-570. (2019)
- Ward RJ, Roberts CC, Bencardino JT, et al. "ACR Appropriateness Criteria ® Osteoporosis and Bone Mineral Density". J Am Coll Radiol. 14(5S). :S189-S202. (2017)
- McCarthy J, Davis A. "Diagnosis and Management of Vertebral Compression Fractures.". Am Fam Physician. 94(1). :44-50. (2016)
- Tegola L, Mattera M, Cornacchia S, Cheng X, Guglielmi G. "Diagnostic imaging of two related chronic diseases: Sarcopenia and Osteoporosis.". J Frailty Sarcopenia Falls. 3(3). :138-147. (2018)
- Guglielmi G, Muscarella S, Bazzocchi A. "Integrated Imaging Approach to Osteoporosis: State-of-the-Art Review and Update". RadioGraphics. 31(5). :1343-1364. (2011)
- Eastell R, Rosen CJ, Black DM, et al. "Pharmacological Management of Osteoporosis in Postmenopausal Women: An Endocrine Society* Clinical Practice Guideline". J Clin Endocrinol Metab. 104(5). :1595-1622. (2019)
- Shane E, Burr D, Abrahamsen B, et al. "Atypical Subtrochanteric and Diaphyseal Femoral Fractures: Second Report of a Task Force of the American Society for Bone and Mineral Research". J Bone Miner Res. 29(1). :1-23. (2013)
- Nicholson WK, Silverstein M, et al. "Interventions to Prevent Falls in Community-Dwelling Older Adults". JAMA. (2024)
- Qaseem A, Hicks LA, Etxeandia-Ikobaltzeta I, et al. "Pharmacologic Treatment of Primary Osteoporosis or Low Bone Mass to Prevent Fractures in Adults: A Living Clinical Guideline From the American College of Physicians". Ann Intern Med. 176(2). :224-238. (2023)
- Qaseem A, Cooney TG, Shamliyan TA, et al. "Pharmacologic Treatment of Primary Osteoporosis or Low Bone Mass to Prevent Fractures in Adults: A Living Clinical Guideline From the American College of Physicians (Version 1: Update Alert 1: Surveillance Note 1)". Ann Intern Med. (2025)
- Watts NB, Adler RA, Bilezikian JP, et al. "Osteoporosis in Men: An Endocrine Society Clinical Practice Guideline". J Clin Endocrinol Metab. 97(6). :1802-1822. (2012)
- Chotiyarnwong P, McCloskey EV. "Pathogenesis of glucocorticoid-induced osteoporosis and options for treatment". Nat. Rev. Endocrinol.. 16(8). :437-447. (2020)
- Kennel KA, Drake MT. "Adverse Effects of Bisphosphonates: Implications for Osteoporosis Management". Mayo Clinic Proceedings. 84(7). :632-638. (2009)
- Dubois EA, Rissmann R, Cohen AF. "Denosumab". Br J Clin Pharmacol. 71(6). :804-806. (2011)
- Hodsman AB, Bauer DC, Dempster DW, et al. "Parathyroid Hormone and Teriparatide for the Treatment of Osteoporosis: A Review of the Evidence and Suggested Guidelines for Its Use". Endocr Rev. 26(5). :688-703. (2005)
- Thompson JC, Wanderman N, Anderson PA, Freedman BA. "Abaloparatide and the Spine: A Narrative Review". Clin Interv Aging. 15. :1023-1033. (2020)
- Shoback D, Rosen CJ, Black DM, et al. "Pharmacological Management of Osteoporosis in Postmenopausal Women: An Endocrine Society Guideline Update". The Journal of Clinical Endocrinology & Metabolism. 105(3). :587-594. (2020)
- Cummings SR, Eckert S, Krueger KA, et al. "The Effect of Raloxifene on Risk of Breast Cancer in Postmenopausal Women". JAMA. 281(23). :2189. (1999)
- Knopp-Sihota JA, Newburn-Cook CV, Homik J, Cummings GG, Voaklander D. "Calcitonin for treating acute and chronic pain of recent and remote osteoporotic vertebral compression fractures: a systematic review and meta-analysis". Osteoporos Int. 23(1). :17-38. (2011)
- Naot D, Musson DS, Cornish J. "The Activity of Peptides of the Calcitonin Family in Bone". Physiol Rev. 99(1). :781-805. (2019)
- Manolagas SC, O’Brien CA, Almeida M. "The role of estrogen and androgen receptors in bone health and disease". Nat Rev Endocrinol. 9(12). :699-712. (2013)
- Nicholson WK, Silverstein M, et al. "Screening for Osteoporosis to Prevent Fractures". JAMA. (2025)
- Choksi P, Gay BL, Reyes-Gastelum D, Haymart MR, Papaleontiou M. "Understanding Osteoporosis Screening Practices in Men: A Nationwide Physician Survey". Endocr Pract. 26(11). :1237-1243. (2020)
- Leslie WD, Crandall CJ. "Serial Bone Density Measurement for Osteoporosis Screening". JAMA. 326(16). :1622. (2021)
- Buckley L, Humphrey MB. "Glucocorticoid-Induced Osteoporosis". N Engl J Med. 379(26). :2547-2556. (2018)
- "Approach to the Poisoned Patient"
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins—Gynecology. "ACOG Practice Bulletin No. 141: Management of Menopausal Symptoms (reaffirmed 2024)". Obstet Gynecol. 123(1). :202-16. (2014)
- Stuenkel CA, Davis SR, Gompel A, et al. "Treatment of Symptoms of the Menopause: An Endocrine Society Clinical Practice Guideline". J Clin Endocrinol Metab. 100(11). :3975-4011. (2015)