Summary
In the US, ovarian cancer is the second most common gynecologic cancer and has the highest mortality rate of any gynecologic cancer. Incidence increases with age (peak incidence at 55–64 years of age). Genetic risk factors include mutations in the BRCA1/BRCA2 and/or mismatch repair (MMR) gene. The most common type of ovarian cancer is epithelial cell carcinoma. Symptoms of ovarian cancer are usually nonspecific (e.g., abdominal pain and distention), and over half of individuals with ovarian cancer have metastatic disease at the time of diagnosis. The diagnosis of ovarian cancer begins with workup of an adnexal mass, but tissue diagnosis is required for confirmation. Surgery is recommended for a definitive diagnosis of ovarian cancer; maximal cytoreduction should be performed to improve long-term outcomes. Most patients with ovarian cancer should receive adjuvant chemotherapy with a platinum-based agent and a taxane. Prognosis is primarily based on the disease stage, with an overall 5-year survival rate of 50%. Routine screening with CA-125 or TVUS is not recommended in individuals with an average risk.
For information about specific ovarian cancer subtypes, see “Overview of ovarian tumors.”
Epidemiology
-
Incidence [1]
- Second most common gynecologic cancer (after endometrial cancer)
- Incidence increases with age.
-
Lifetime risk
- General population: ∼ 1% [2][3]
- Individuals with genetic predisposition, e.g.:
- BRCA1-positive: 25–65% [2]
- BRCA2-positive: 10–30% [2]
- MMR gene mutation: 10% [2]
-
Age
- Peak incidence: 55–64 years of age [4]
- Women with genetic mutations are typically diagnosed at a younger age.
- Mortality: highest mortality rate of any gynecologic cancer in the US [1]
")
")
Epidemiological data refers to the US, unless otherwise specified.
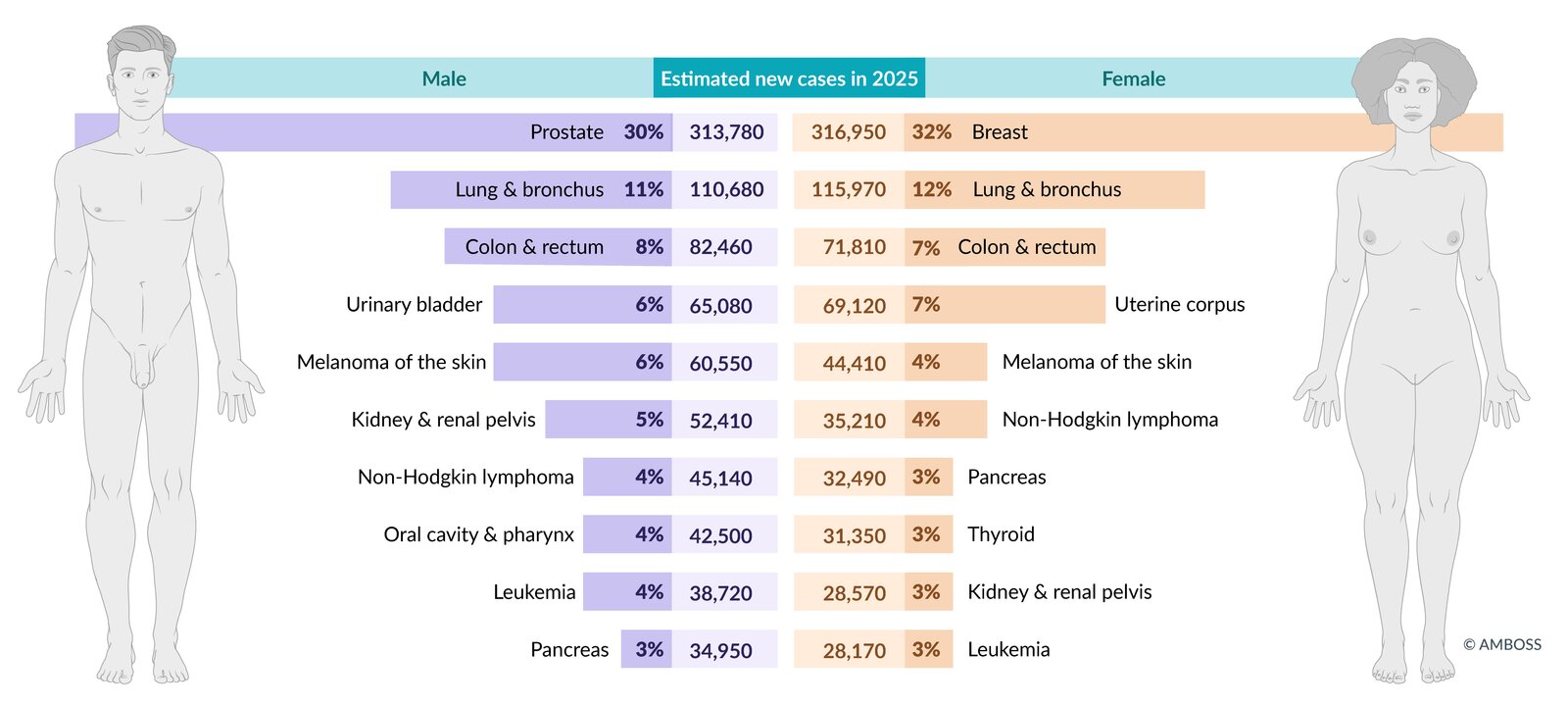
Estimated incidence of the most common cancers in the US in total figures and as a percentage of total cancer incidence (excluding non-melanoma skin cancers and in-situ carcinoma, except urinary bladder). Figures are prospective estimates of the American Cancer Society for 2025.
© AMBOSS. Data source: Cancer Facts & Figures 2024, American Cancer Society, access date 06/28/24 (https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2024/2024-cancer-facts-and-figures-acs.pdf)
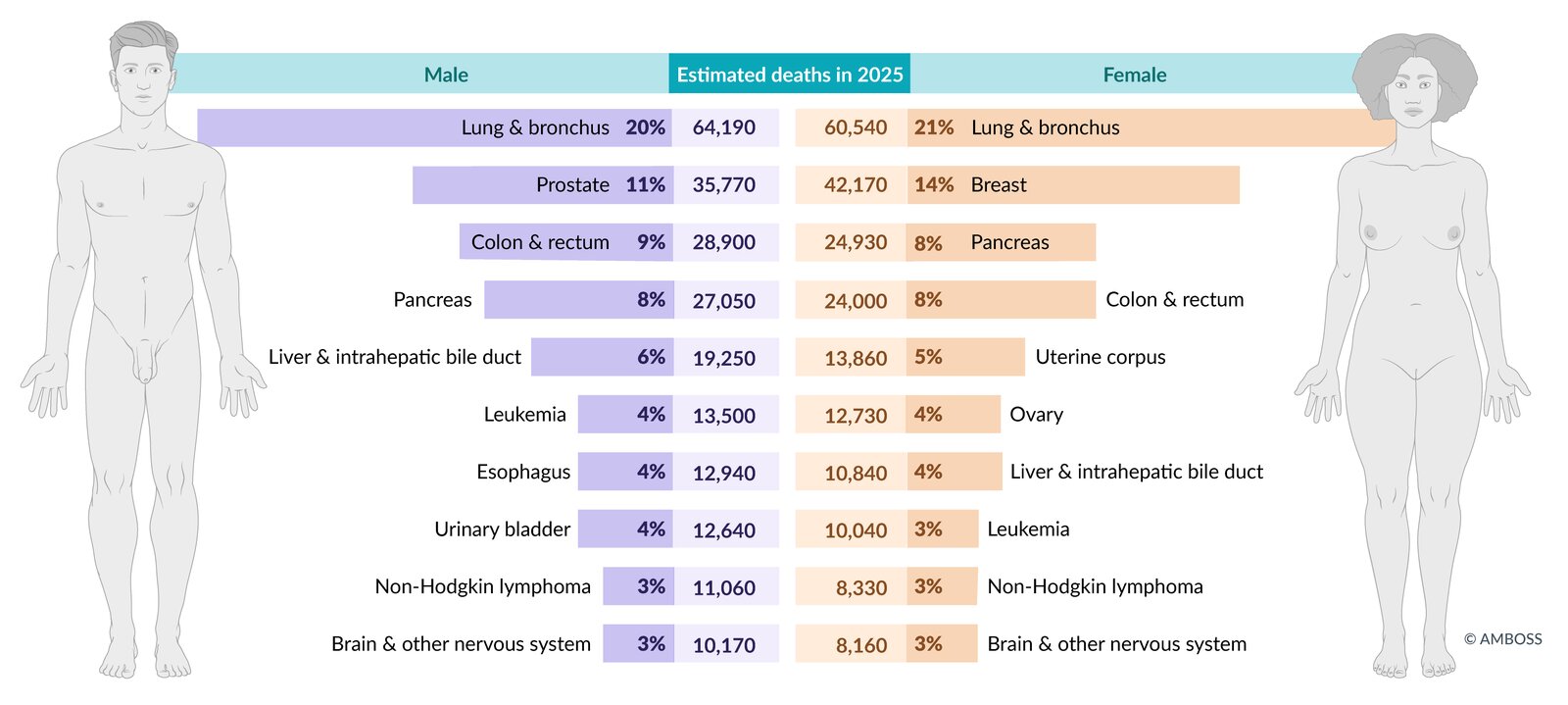
Estimated mortality from the most common cancers in the US in total figures and as a percentage of total cancer mortality. Figures are prospective estimates of the American Cancer Society for 2025.
© AMBOSS. Data source: Cancer Facts & Figures 2024, American Cancer Society, access date 06/28/24 (https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2024/2024-cancer-facts-and-figures-acs.pdf)
Etiology
Risk factors for ovarian cancer [5]
-
General
- Increasing age
- Cigarette smoking
- Asbestos exposure [6]
-
Genetic predisposition
- BRCA gene mutation
- MMR gene mutation associated with HNPCC syndrome
- Positive family history
- Ashkenazi Jewish descent [7]
-
Hormonal factors
- Elevated number of ovulatory cycles: early menarche and/or late menopause
- Nulliparity
- Endometriosis
- Hormone replacement therapy [8]
- Polycystic ovarian syndrome (PCOS) [9]
Protective factors for ovarian cancer [5]
-
Surgery
- Risk-reducing bilateral salpingo-oophorectomy (rrBSO) for high risk patients [10]
- Tubal ligation
- Hysterectomy
-
Hormonal factors
- Oral contraceptives [11]
- Breastfeeding
- Parity
Classification
For information about ovarian cancer subtypes, see “Overview of ovarian tumors.”
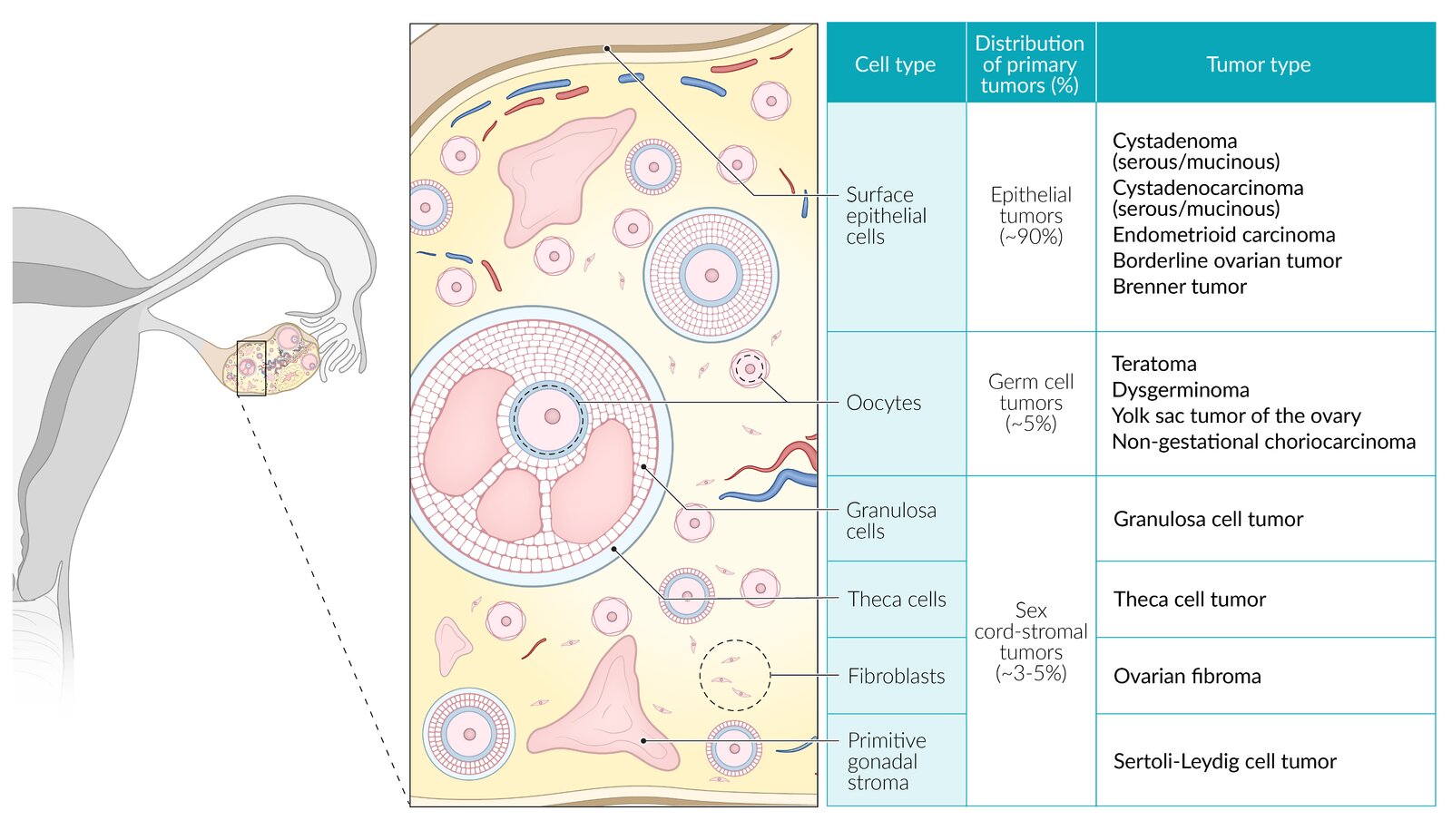
Classification of ovarian cancer
Ovarian malignancies can be either primary (i.e., arising from the different types of ovarian tissue) or secondary (i.e., metastases from other primary tumors).
Primary ovarian cancer
-
Epithelial cell tumors
- Cystadenocarcinoma (serous or mucinous)
- Clear cell tumors
- Endometrioid carcinoma
-
Germ cell tumors
- Immature teratoma
- Yolk sac tumor of the ovary (endodermal sinus tumor)
- Dysgerminoma
- Nongestational choriocarcinoma
- Sex cord tumors: granulosa cell tumor
High-grade cystadenocarcinoma is the most aggressive ovarian cancer.

Secondary ovarian cancer
Most common primary cancers: gastrointestinal tract (e.g., Krukenberg tumor), breast, and endometrium. [12]
-
Krukenberg tumor: secondary ovarian tumor that most commonly arises from metastatic spread of gastric carcinoma ; [13]
- Often bilateral
- Characteristic mucin-secreting signet ring cells on histology
- The exact route of metastatic spread (i.e., lymphatic, hematogenous, or peritoneal) is still debated.

© AMBOSS
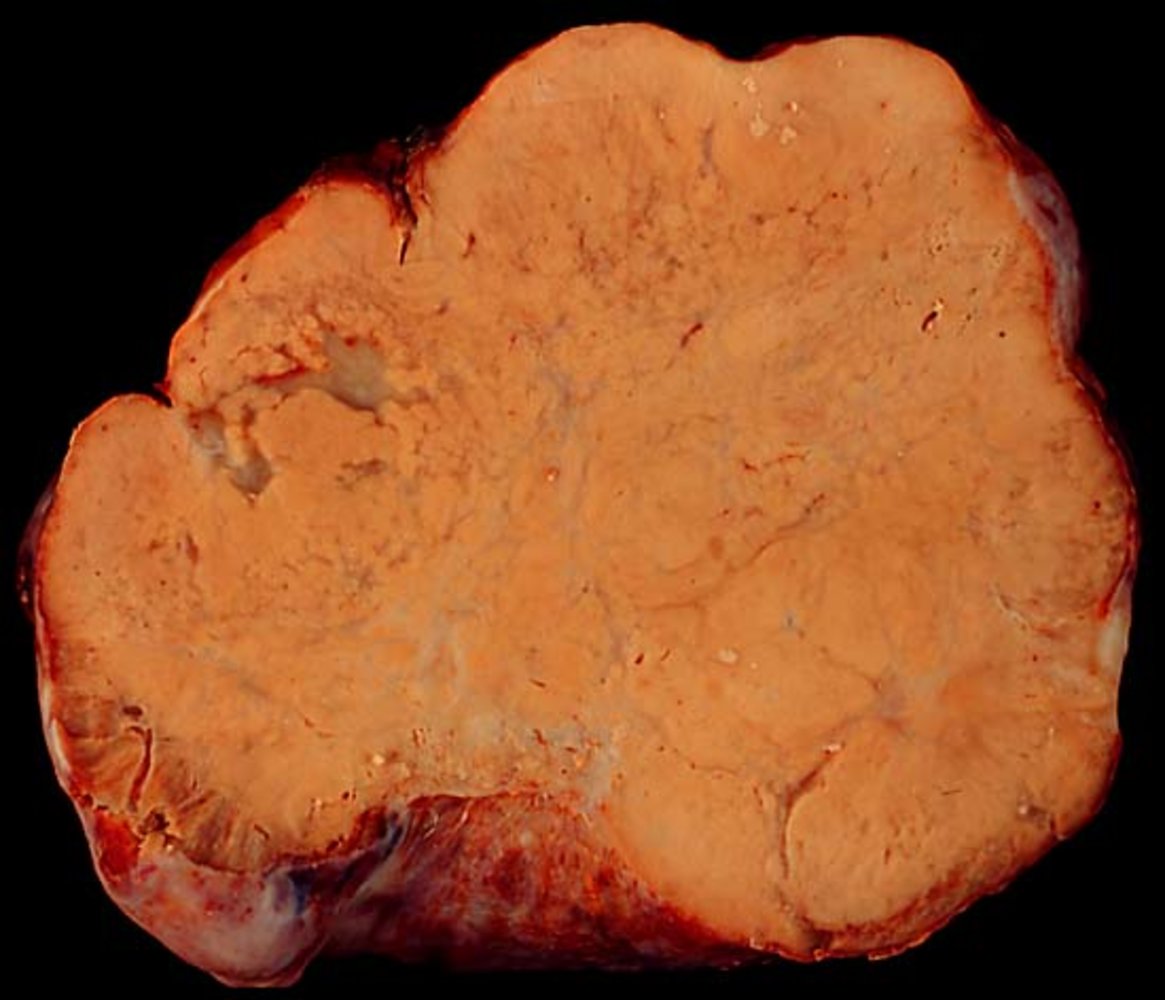
Ovarian resection specimen
The ovary appears diffusely enlarged and has a smooth surface. The heterogeneous tissue contains streaks of cystic, mucoid tissue.
Krukenberg tumors are usually secondary to gastric signet ring cell carcinoma or breast cancer.
Source: "Krukenberg Tumor.jpg", Ed Uthman, Wikipedia licensed under Public Domain
{kind=link}
Clinical features
Symptoms of ovarian cancer are usually nonspecific, which often delays the diagnosis. Early-stage ovarian cancer is usually asymptomatic. [2][8]
Abdominal and pelvic symptoms [2][8]
- Early satiety
- Abdominal distention and/or bloating
- Abdominal, pelvic, and/or lower back pain
- Changes in urination (e.g., frequency, urgency)
- Constipation
- Abnormal bleeding (rare) [14]
- Postmenopausal bleeding
- Rectal bleeding
Advanced disease [2][8]
Over half of those with ovarian cancer have metastatic disease at the time of diagnosis. [2]
-
Locally advanced disease
- Ascites
- Malignant pleural effusion (resulting in dyspnea and pleuritic chest pain)
- Bowel obstruction (resulting in severe nausea and vomiting)
-
Metastatic disease [15][16]
- Omentum: abdominal pain from infiltration of omental fat
- Liver: nausea, jaundice, ascites (see “Metastatic liver disease”)
- Distant lymph nodes: supraclavicular or inguinal lymphadenopathy
- Lung: cough, hemoptysis, chest pain (see “Lung metastases”)
- Brain: headaches, seizures, focal motor deficits (see “Brain metastases”)
- Bone: local pain and swelling, pathologic fractures (see “Bone metastases”)

Paraneoplastic syndromes [2][17]
Although rare, these syndromes may be seen in patients with ovarian cancer. [17]
- Paraneoplastic sensory neuropathy
- Paraneoplastic cerebellar degeneration
- Dermatomyositis
- Hemolytic anemia
- Leser-Trélat sign
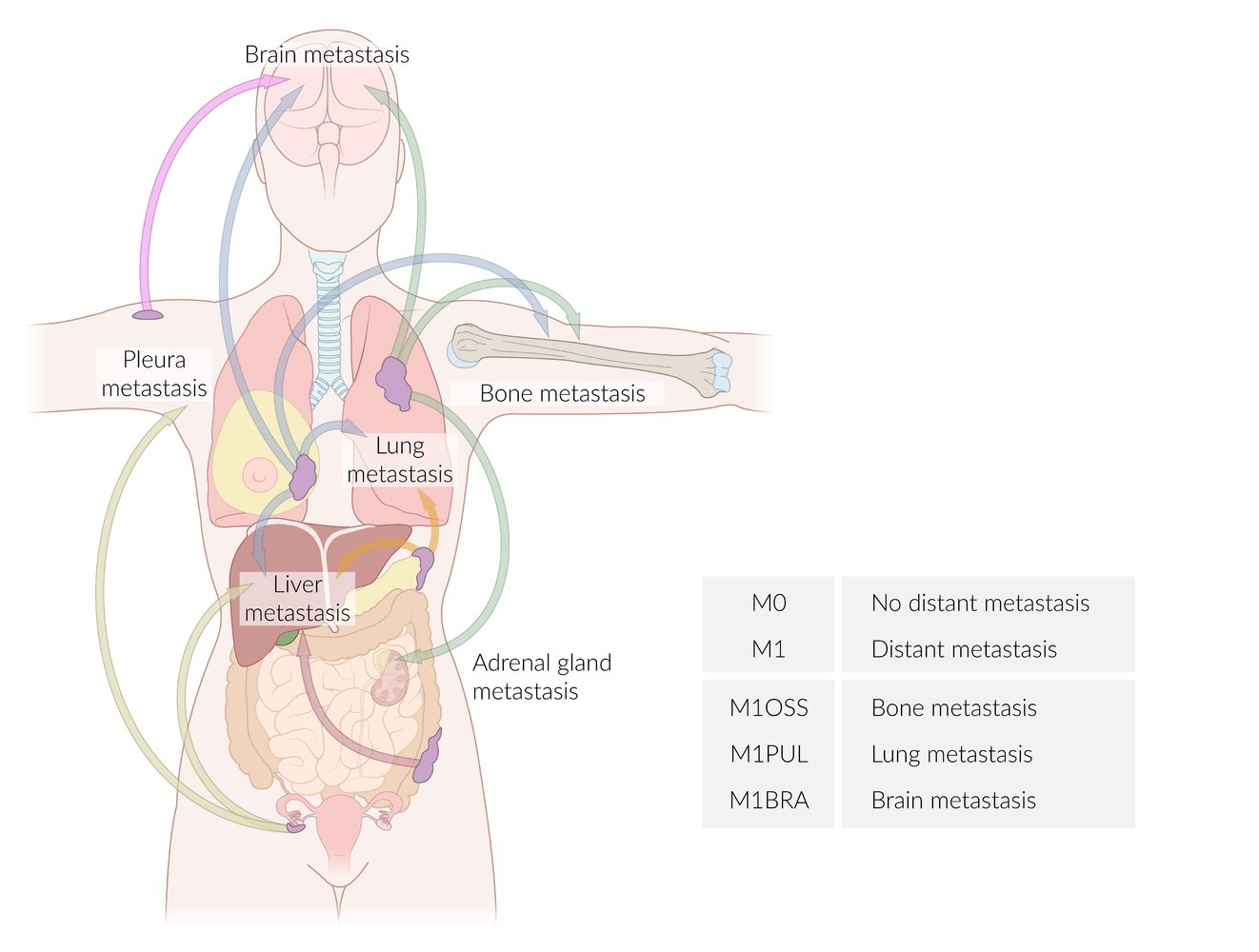
Arrows have been color-coded according to the site of the primary tumor:
Pink: skin cancer
Blue: breast cancer
Green: lung cancer
Orange: pancreatic cancer
Red: colon cancer
Lime: ovarian cancer
The table provides examples of suffixes used to specify the affected organs according to the TNM classification.
© AMBOSS
Diagnosis
General principles [2][18]
-
If ovarian cancer is suspected, follow the approach to diagnostics for an adnexal mass, including:
- Transvaginal ultrasound with doppler to evaluate for ultrasound findings concerning for ovarian malignancy
- Ovarian tumor markers (e.g., CA 125)
- Refer to gynecologic oncology for:
- Diagnostic confirmation (i.e., tissue diagnosis)
- Cross-sectional imaging for staging
Omental caking (thickening) is a radiologic finding on cross-sectional imaging that is consistent with advanced peritoneal ovarian cancer and is due to tumor infiltration of the greater omentum.
Tissue diagnosis [18]
-
Surgical biopsy
- Recommended for definitive diagnosis of ovarian cancer [8]
- Should be performed in patients with clinical, radiographic, and/or laboratory findings that suggest ovarian cancer
- Laparoscopic removal is the preferred surgical procedure.
-
Other studies
- Needle biopsy: generally avoided because of the risk of tumor seeding, which can advance the stage of disease
- Fluid cytology of ascites or pleural effusion
Fine-needle aspiration of ovarian masses is typically contraindicated when there is suspicion for malignancy because it can directly spread tumor cells to the peritoneum.
Differential diagnoses
See the following:
- “Etiology of adnexal masses”
- “Adnexal masses in pregnancy”
- “Mimics of adnexal masses”
The differential diagnoses listed here are not exhaustive.
Staging
Staging is based on the International Federation of Gynecology and Obstetrics (FIGO) and the Tumor, Node, Metastasis (TNM) classification systems.
| Staging of epithelial ovarian cancer (including fallopian tube cancer and primary peritoneal cancer) [19] | ||||
|---|---|---|---|---|
| Management approach | FIGO stage | TNM | Description | |
| Curative |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||
|
|
|
||
|
|
|
||
|
|
|
||
|
|
|
||
|
|
|
||
|
|
|
||
|
|
|
||
| Palliative |
|
|
|
|
|
|
|
||
Management
General principles
- Refer all patients to a gynecologic oncologist for ongoing management.
- Surgical staging: performed to obtain pathological specimens and evaluate the extent of cancer spread
- Surgical debulking improves long-term outcomes. [20]
- Most patients should receive adjuvant chemotherapy.
- CA-125 levels may be used to monitor disease progression and/or recurrence after treatment. [8]

Surgery [8][21][22]
For the best patient outcomes, surgical staging and debulking should be performed by a gynecologic oncologist. [23]
-
Surgical staging
- Hysterectomy with bilateral salpingo-oophorectomy
- Pelvic and paraaortic lymph node dissection
- Omentectomy
- Peritoneal cytology
-
Surgical debulking [20]
- Optimal debulking is defined as < 1 cm of residual tumor. [24]
- Used in disease stages I–III and, occasionally, stage IV
Surgical resection alone may be curative in patients with early-stage disease. [24]
Chemotherapy [8]
- Patients with ovarian cancer should receive adjuvant chemotherapy, except for those with low-grade, stage I disease.
- Common regimen: platinum-based agent (e.g., carboplatin) PLUS taxane (e.g., paclitaxel) ± bevacizumab [25]
- Adjuvant intraperitoneal chemotherapy combined with intravenous chemotherapy results in a higher survival rate than intravenous chemotherapy alone. [26]
- Neoadjuvant chemotherapy followed by interval debulking surgery can be considered in patients with advanced-stage disease and high perioperative risk. [26]
Targeted molecular therapy
-
Indications
- BRCA-positive disease [27]
- Maintenance therapy after surgical debulking and chemotherapy [28]
-
Targeted agents: oral poly (ADP-ribose) polymerase inhibitors (PARP inhibitors)
- Olaparib: first-generation oral PARP inhibitor [29]
- Niraparib: highly selective PARP1/PARP2 inhibitor [30]
- Rucaparib: inhibits PARP1, PARP2, and PARP3 [31]
Management of recurrence [32]
- Relapse within 6 months of completing chemotherapy is classified as platinum-resistant disease and can be managed with either:
- A different chemotherapy regimen
- Inclusion in clinical trials
- A focus on palliative therapy over curative therapy
- If relapse occurs > 6 months after completing initial chemotherapy:
- Treat with platinum-containing combination chemotherapy and bevacizumab or PARP inhibitors if indicated.
- Consider secondary cytoreductive surgery.
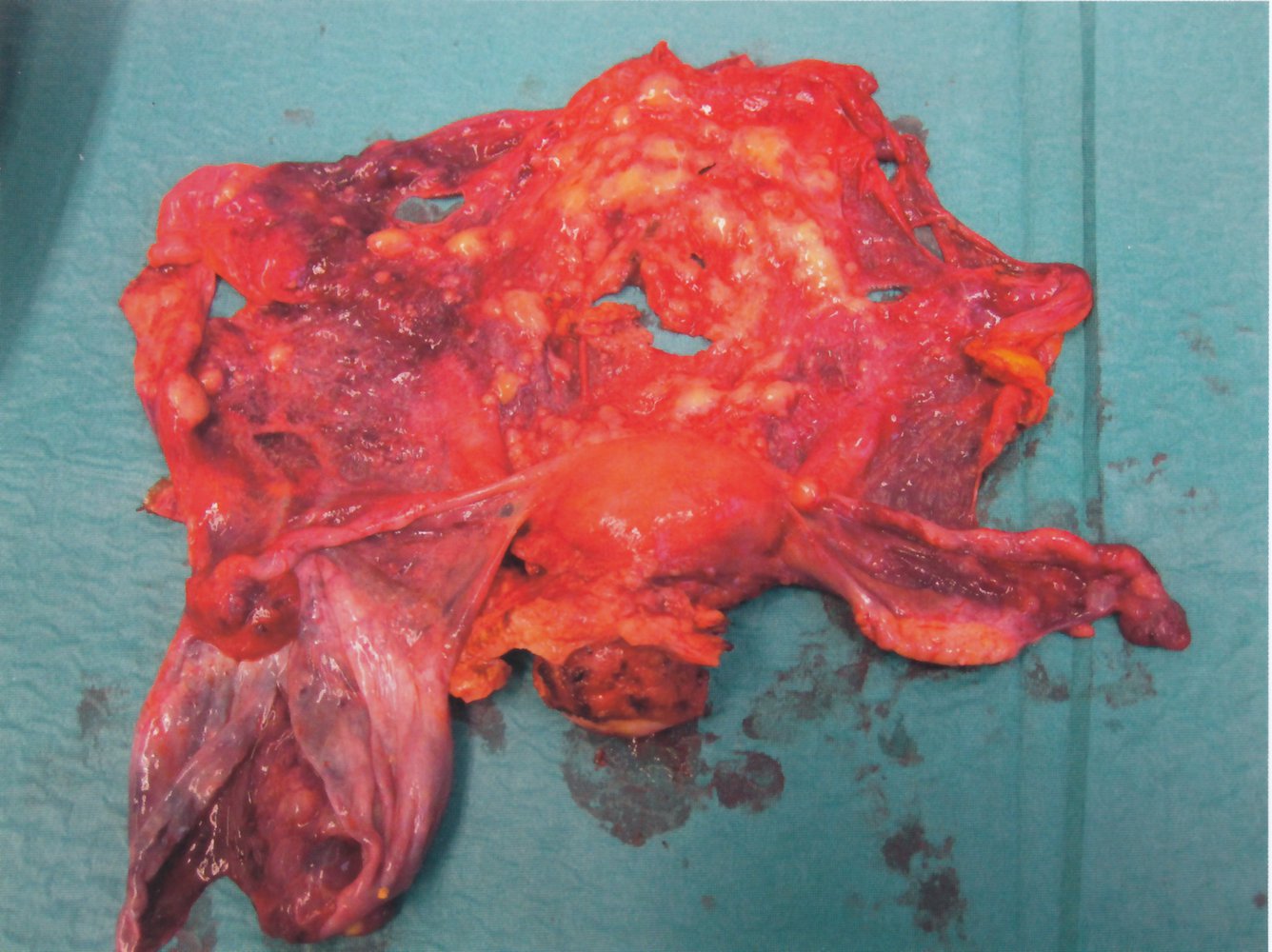
Intraoperative specimen from an en bloc pelvic resection of the uterus and uterine adnexa
The uterus and the lateral fallopian tubes (both within green dashed outline) are visible. The ovary located beneath the right fallopian tube (green arrowhead) is the normal yellow color and has a characteristic elongated shape and ridged surface. The left ovary contains a large, serous cyst (white overlay) with a gray wall, which has been opened up and, therefore, collapsed. There are nodular, solid carcinoma lesions on the inner membrane of the cyst (white arrows). Similar nodules (black arrowheads) can be identified on the peritoneum (green overlay) above the uterus, which may correspond to peritoneal carcinomatosis.
Source: © IMPP
Prognosis
-
5-year survival rates after initial diagnosis vary by disease stage. [3]
- Overall (all stages): ∼ 51%
- Localized disease (no spread): ∼ 92%
- Regional disease (spread to lymph nodes): ∼ 72%
- Distant disease (metastatic): ∼ 31%
- The lifetime risk of relapse is > 80% for patients with stage III or IV disease. [32]
Prevention
Ovarian cancer screening [33][34]
-
Indications
- Routine screening with CA-125 or transvaginal ultrasound is not recommended in individuals with an average risk of ovarian cancer. [35][36]
-
In individuals at high risk, familial risk assessment should be performed, after which genetic counseling and subsequent genetic testing for hereditary cancer syndromes (e.g., BRCA1, BRCA2, or Lynch syndrome) may be indicated. ; [37]
- Some of the tools used for familiar risk stratification include the Ontario Family History Assessment Tool, the Manchester Scoring System, the Referral Screening Tool, and the Pedigree Assessment Tool. [38]
- In patients with high-risk mutations:
- Risk-reducing bilateral salpingo-oophorectomy (rrBSO) is a preventive treatment option for patients who do not wish to conceive in the future. [39]
- Periodic screening for ovarian cancer (e.g., annual transvaginal ultrasound, pelvic exam, and CA-125 levels) is an alternative to rrBSO [40]
-
Potential benefits
- Reduction in mortality
- Diagnosis of ovarian cancer at an earlier stage
-
Potential harms
- False positives
- Psychological distress
- Morbidity or mortality from surgery
Strategies to reduce the risk of ovarian cancer
See “Protective factors” in “Etiology” above.
External Resources
References
- "Incidence and Mortality". https://cancerstatisticscenter.cancer.org/?_ga=2.248342983.1926186680.1673454593-918507681.1673454592#!/. [2023-01-01]
- Doubeni et al. "Diagnosis and Management of Ovarian Cancer". Am Fam Physician. (2016)
- "SEER Cancer Stat Facts: Ovarian Cancer". https://web.archive.org/web/20240523221806/https://seer.cancer.gov/statfacts/html/ovary.html
- "Ovarian Cancer Statistics". https://web.archive.org/web/20240120222240/https://www.cdc.gov/cancer/ovarian/statistics/index.htm. [2022-06-06]
- Brett M. R, Brett M. R, Jennifer B. P, et al. "Epidemiology of ovarian cancer: a review". Cancer Biol Med. 14(1). :9-32. (2017)
- Camargo MC, Stayner LT, Straif K, et al. "Occupational Exposure to Asbestos and Ovarian Cancer: A Meta-analysis". Environ Health Perspect. 119(9). :1211-1217. (2011)
- "Jewish Women and BRCA Gene Mutations". https://web.archive.org/web/20220928200245/https://www.cdc.gov/cancer/breast/young_women/bringyourbrave/hereditary_breast_cancer/jewish_women_brca.htm. [2021-09-27]
- Matulonis UA, Sood AK, Fallowfield L, et al. "Ovarian cancer.". Nat Rev Dis primers. 2. :16061. (2016)
- Yin W, Falconer H, Yin L, Xu L, Ye W. "Association Between Polycystic Ovary Syndrome and Cancer Risk". JAMA Oncology. 5(1). :106. (2019)
- Menon U, Karpinskyj C, Gentry-Maharaj A. "Ovarian Cancer Prevention and Screening". Obstet Gynecol. 131(5). :909-927. (2018)
- Havrilesky LJ, Moorman PG, Lowery WJ, et al. "Oral Contraceptive Pills as Primary Prevention for Ovarian Cancer". Obstet Gynecol. 122(1). :139-147. (2013)
- de Waal YRP, Thomas CMG, Oei ALM, Sweep FCGJ, Massuger LFAG. "Secondary Ovarian Malignancies". International Journal of Gynecological Cancer. 19(7). :1160-1165. (2009)
- Kubeček O, Laco J, Špaček J, et al. "The pathogenesis, diagnosis, and management of metastatic tumors to the ovary: a comprehensive review". Clin Exp Metastasis. 34(5). :295-307. (2017)
- Hamilton W, Peters TJ, Bankhead C, Sharp D. "Risk of ovarian cancer in women with symptoms in primary care: population based case-control study". BMJ. 339(aug25 2). :b2998-b2998. (2009)
- Lengyel E. "Ovarian Cancer Development and Metastasis". Am J Pathol. 177(3). :1053-1064. (2010)
- Deng K, Yang C, Tan Q, et al. "Sites of distant metastases and overall survival in ovarian cancer: A study of 1481 patients.". Gynecol Oncol. 150(3). :460-465. (2018)
- Shanbhogue AKP, Shanbhogue DKP, Prasad SR, et al. "Clinical Syndromes Associated with Ovarian Neoplasms: A Comprehensive Review". RadioGraphics. 30(4). :903-919. (2010)
- Berek JS, Renz M, Kehoe S, Kumar L, Friedlander M. "Cancer of the ovary, fallopian tube, and peritoneum: 2021 update". Int J Gynaecol Obstet. 155(S1). :61-85. (2021)
- R Eskander, M Berman, L Keder. "Practice Bulletin No. 174: Evaluation and Management of Adnexal Masses (reaffirmed 2021)". Obstet Gynecol. 128(5). :e210-e226. (2016)
- Garzon S, Laganà AS, Casarin J, et al. "Secondary and tertiary ovarian cancer recurrence: what is the best management?". Gland Surg. 9(4). :1118-1129. (2020)
- "Breast and Ovarian Cancer and Family History Risk Categories". https://web.archive.org/web/20210319030415/https://www.cdc.gov/genomics/disease/breast_ovarian_cancer/risk_categories.htm. [2020-03-25]
- "BRCA-Related Cancer: Risk Assessment, Genetic Counseling, and Genetic Testing". https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/brca-related-cancer-risk-assessment-genetic-counseling-and-genetic-testing. [2019-08-20]
- Pinsky PF, Yu K, Kramer BS, et al. "Extended mortality results for ovarian cancer screening in the PLCO trial with median 15 years follow-up". Gynecol Oncol. 143(2). :270-275. (2016)
- Jacobs IJ, Menon U, Ryan A, et al. "Ovarian cancer screening and mortality in the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): a randomised controlled trial". Lancet. 387(10022). :945-956. (2016)
- Owens DK, et al. "Risk Assessment, Genetic Counseling, and Genetic Testing for BRCA-Related Cancer". JAMA. 322(7). :652. (2019)
- "Risk Assessment, Genetic Counseling, and Genetic Testing for BRCA1/2-Related Cancer in Women: A Systematic Review for the U.S. Preventive Services Task Force [Internet]". https://www.ncbi.nlm.nih.gov/books/NBK545866/. [2019-08-01]
- Berek JS, Chalas E, Edelson M, et al. "Prophylactic and Risk-Reducing Bilateral Salpingo-oophorectomy". Obstet Gynecol. 116(3). :733-743. (2010)
- Smith RA, Manassaram-Baptiste D, Brooks D, et al. "Cancer screening in the United States, 2015: A review of current American Cancer Society guidelines and current issues in cancer screening". CA Cancer J Clin. 65(1). :30-54. (2015)
- Chi DS, Eisenhauer EL, Zivanovic O, et al. "Improved progression-free and overall survival in advanced ovarian cancer as a result of a change in surgical paradigm". Gynecol Oncol. 114(1). :26-31. (2009)
- Lheureux S, Gourley C, Vergote I, Oza AM. "Epithelial ovarian cancer". Lancet. 393(10177). :1240-1253. (2019)
- Jayson GC, Kohn EC, Kitchener HC, Ledermann JA. "Ovarian cancer". Lancet. 384(9951). :1376-1388. (2014)
- Giede KC, Kieser K, Dodge J, Rosen B. "Who should operate on patients with ovarian cancer? An evidence-based review". Gynecol Oncol. 99(2). :447-461. (2005)
- Armstrong DK, Alvarez RD, Bakkum-Gamez JN, et al. "Ovarian Cancer, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology". J Natl Compr Canc Netw. 19(2). :191-226. (2021)
- Garcia J, Hurwitz HI, Sandler AB, et al. "Bevacizumab (Avastin®) in cancer treatment: A review of 15 years of clinical experience and future outlook". Cancer Treat Rev. 86. :102017. (2020)
- Wright AA, Bohlke K, Armstrong DK, et al. "Neoadjuvant Chemotherapy for Newly Diagnosed, Advanced Ovarian Cancer: Society of Gynecologic Oncology and American Society of Clinical Oncology Clinical Practice Guideline.". J Clin Oncol. 34(28). :3460-73. (2016)
- Konstantinopoulos PA, Norquist B, Lacchetti C, et al. "Germline and Somatic Tumor Testing in Epithelial Ovarian Cancer: ASCO Guideline". J Clin Onc. 38(11). :1222-1245. (2020)
- Ledermann J, Harter P, Gourley C, et al. "Olaparib Maintenance Therapy in Platinum-Sensitive Relapsed Ovarian Cancer". N Engl J Med. 366(15). :1382-1392. (2012)
- Moore K, Colombo N, Scambia G, et al. "Maintenance Olaparib in Patients with Newly Diagnosed Advanced Ovarian Cancer". N Engl J Med. 379(26). :2495-2505. (2018)
- González-Martín A, Pothuri B, Vergote I, et al. "Niraparib in Patients with Newly Diagnosed Advanced Ovarian Cancer". N Engl J Med. 381(25). :2391-2402. (2019)
- Monk BJ, Parkinson C, Lim MC, et al. "A Randomized, Phase III Trial to Evaluate Rucaparib Monotherapy as Maintenance Treatment in Patients With Newly Diagnosed Ovarian Cancer". J Clin Oncol. 40(34). :3952-3964. (2022)
- Prat J. "Staging classification for cancer of the ovary, fallopian tube, and peritoneum". Int J Gynaecol Obstet. 124(1). :1-5. (2013)
- Khosla D, Dimri K, Pandey A, Mahajan R, Trehan R. "Ovarian granulosa cell tumor: Clinical features, treatment, outcome, and prognostic factors". North American Journal of Medical Sciences. 6(3). :133. (2014)