Summary
Ovarian cysts are fluid-filled sacs within the ovary. The most common types are functional follicular cysts, corpus luteum cysts, and theca lutein cysts, which all develop as part of the menstrual cycle and are usually harmless and resolve on their own. Nonfunctional cysts include chocolate cysts (which are associated with endometriosis), dermoid cysts, cystadenomas, and malignant cysts (a type of ovarian cancer). Ovarian cysts are usually asymptomatic, but they can sometimes cause lower abdominal pain and predispose individuals to complications such as cyst rupture or ovarian torsion, which may require surgery. Diagnosis typically begins with workup of an adnexal mass, and is usually made with pelvic ultrasound. Management and follow-up depend on cyst size and appearance on ultrasound, the patient's menopausal status, and the presence of risk factors for ovarian tumors.
Overview
Definition
Ovarian cysts are fluid-filled sacs within the ovary.
Types
Functional ovarian cysts
Functional cysts result from a disruption in the development of follicles or the corpus luteum and often resolve on their own.
-
Follicular cyst of the ovary (most common ovarian mass in young women)
- Develops when a Graafian follicle does not rupture and release the egg (ovulation) but continues to grow
- Eventually develops into a large cyst (∼ 7 cm) lined with granulosa cells
- Associated with hyperestrogenism and endometrial hyperplasia
-
Corpus luteum cyst
- Enlargement and buildup of fluid in the corpus luteum after failed regression following the release of an ovum
- Produces progesterone, which may delay menses
- Associated with progesterone-only contraceptive pills and ovulation-inducing medication
- Common during pregnancy
-
Theca lutein cysts
- Often multiple cysts that typically develop bilaterally
- Result from exaggerated stimulation of the theca interna cells of the ovarian follicles due to excessive amounts of circulating gonadotropins such as β-hCG
- Strongly associated with gestational trophoblastic disease and multiple gestations
- Usually resolve once β-hCG levels have normalized
Nonfunctional ovarian cysts
A group of ovarian cysts that do not produce hormones.
- Chocolate cysts
- Dermoid cysts
- Cystadenoma (serous or mucinous)
- Malignant cysts (form of ovarian cancer): higher risk in postmenopausal women
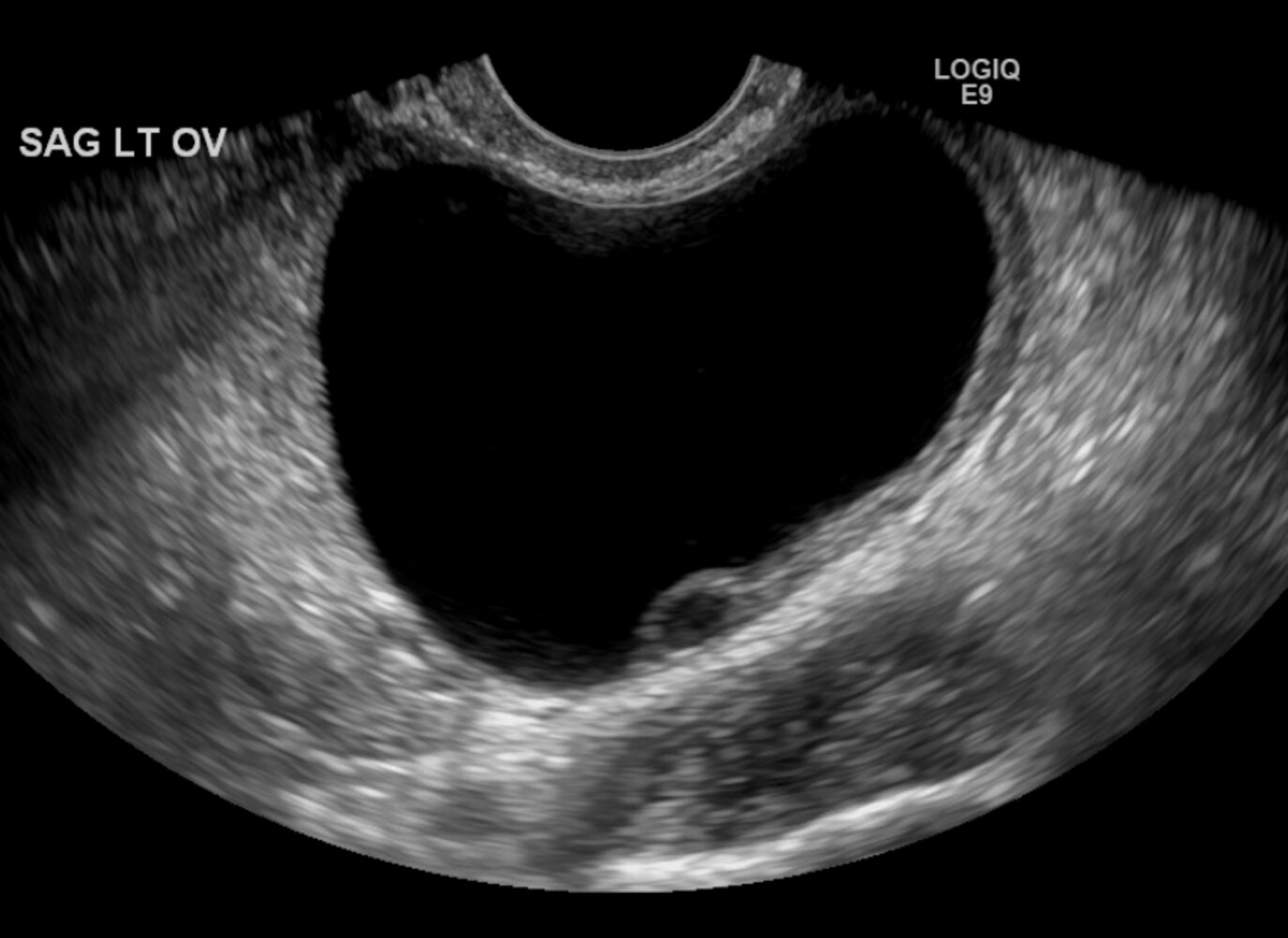
Ultrasound pelvis (left ovary; transvaginal; sagittal plane)
A rim of ovarian tissue (green overlay) is visible along the margin of a 5-cm thin-walled unilocular simple ovarian cyst.
Follicular cysts are benign functional ovarian cysts. Ovarian follicles measure < 3 cm on ultrasound whereas follicular cysts measure ≥ 3 cm.
Source: “LargeLeftOvCyst5cm.png” by James Heilman, MD, Wikimedia, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
Clinical features
- Usually asymptomatic (incidental finding)
- Can cause lower abdominal pain and lead to complications [1]
- Adnexal mass that is sometimes palpable
-
Possibly signs of the underlying cause, such as:
- Menorrhagia in endometriosis
- Hirsutism, acne, and infertility in polycystic ovary syndrome
Ovarian cancer must be ruled out in premenarchal and postmenopausal patients with an adnexal mass. [2]
Diagnosis
Approach [2][3]
- The diagnostic workup follows the approach to diagnostics for an adnexal mass, including:
- Transvaginal ultrasound with doppler to evaluate for ultrasound findings concerning for ovarian malignancy
- Consideration of ovarian tumor markers
- For acutely symptomatic patients: [4][5]
- Consider CT abdomen and pelvis with IV contrast to rule out nongynecologic causes and complications.
- Perform additional diagnostics as clinically indicated; see “Initial management of pelvic pain” and “Approach to acute abdomen.”
Exclude pregnancy in all patients of childbearing age with pelvic pain or a pelvic mass. [5]
Transvaginal ultrasound with doppler is the first-line imaging modality for symptomatic and asymptomatic patients with a suspected adnexal mass. [3]
Pelvic ultrasound findings
-
Simple cysts [6]
- Smooth lining on all sides
- Single: e.g., follicular cyst of the ovary
- Multiple: e.g., polycystic ovary syndrome
- Anechoic
- No internal flow on Doppler
-
Functional cysts
-
Corpus luteum cyst [7]
- Unilocular cyst with thick walls
- ↑ Peripheral vascularity (ring-of-fire sign)
- Small central lucency
- Intracystic echogenic debris may be present.
-
Theca lutein cysts [8]
- Bilateral multilocular cysts with thin walls
- Fluid-filled
- Solid components may be present.
-
Corpus luteum cyst [7]
- Potentially malignant cysts: ultrasound features concerning for ovarian malignancy


")
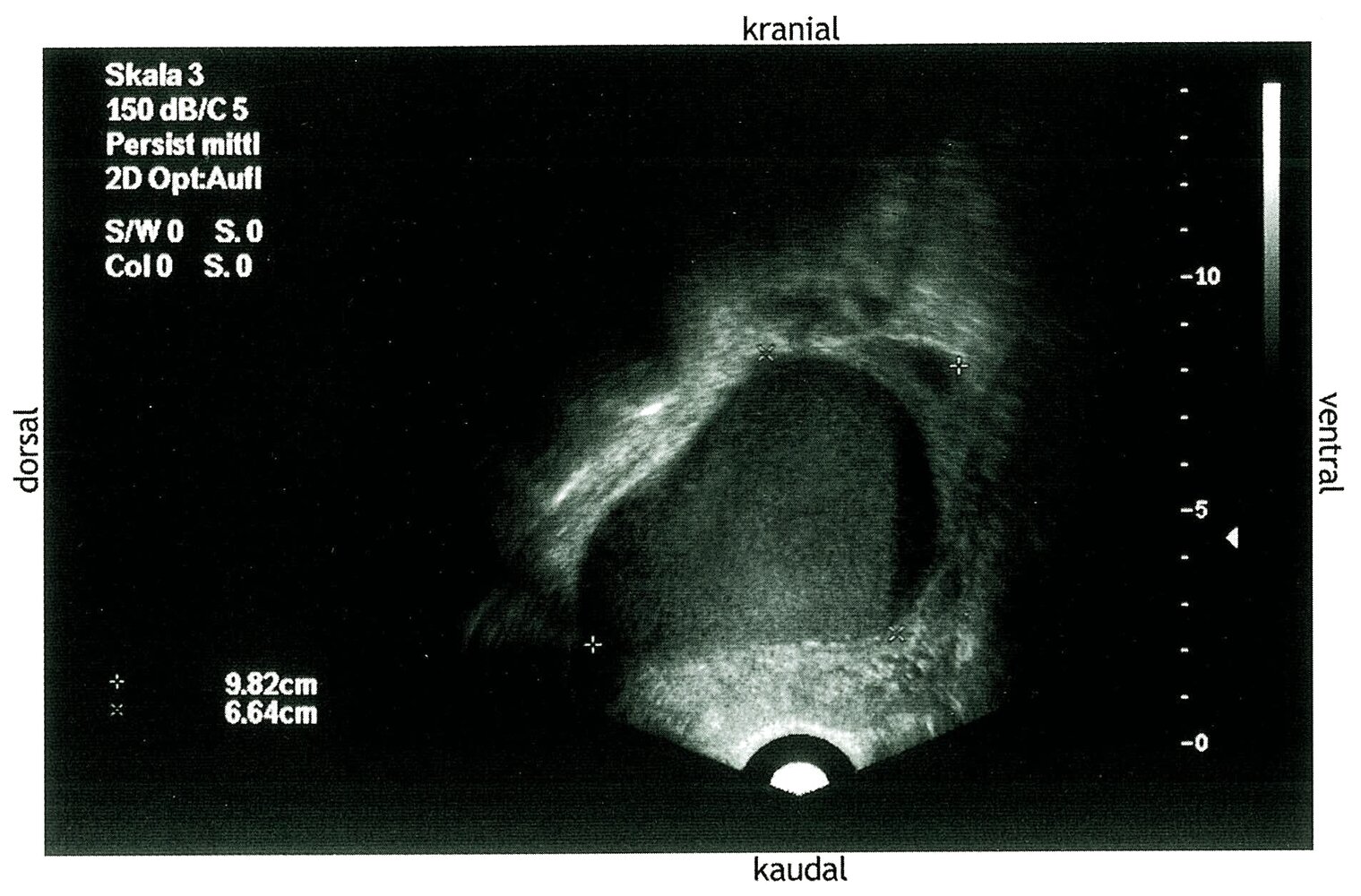
Ultrasound pelvis (transvaginal)
The right ovary (red overlay) contains a 9.8 x 6.6 cm hemorrhagic cyst with low-level echoes (pale-blue overlay) and a fluid-fluid level (dashed line). The appearance of the cyst suggests an endometrioma, or chocolate cyst, common in endometriosis.
Source: © IMPP
Ultrasound pelvis (left ovary; transvaginal; sagittal plane)
A rim of ovarian tissue (green overlay) is visible along the margin of a 5-cm thin-walled unilocular simple ovarian cyst.
Follicular cysts are benign functional ovarian cysts. Ovarian follicles measure < 3 cm on ultrasound whereas follicular cysts measure ≥ 3 cm.
Source: “LargeLeftOvCyst5cm.png” by James Heilman, MD, Wikimedia, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
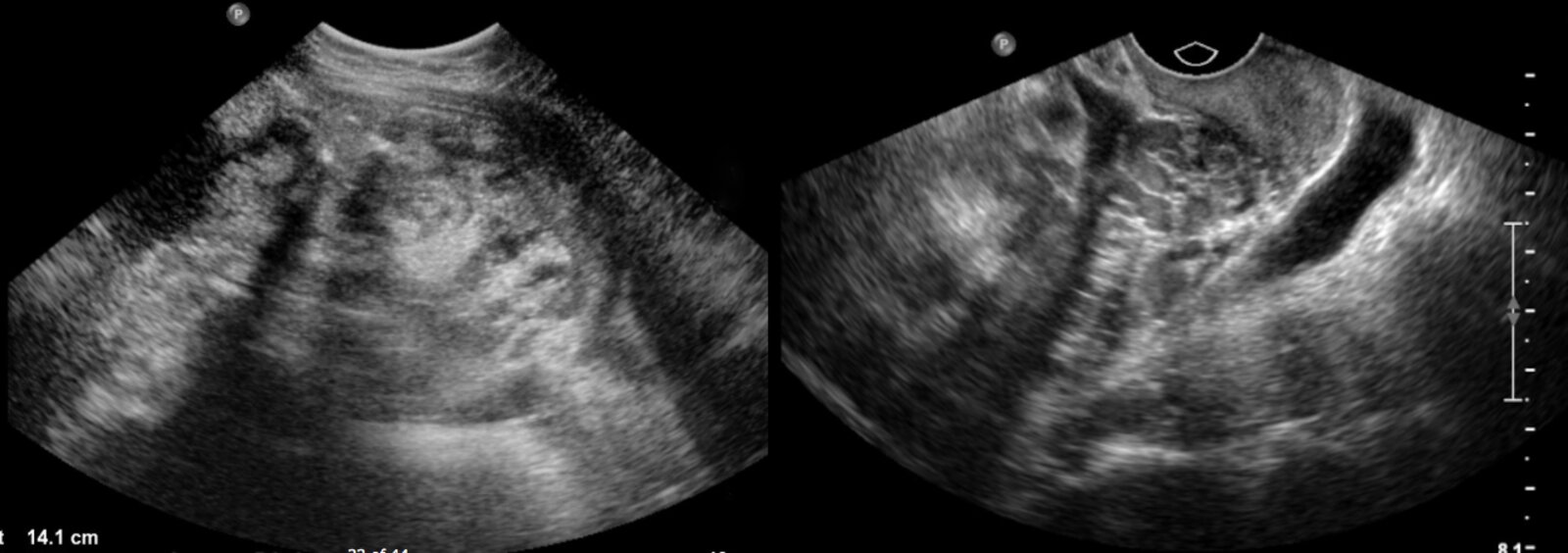
Ultrasound (left: transabdominal, longitudinal plane; right: transvaginal, transverse plane) of a female patient with a distended abdomen and 2-month-history of intermittent abdominal pain
The transabdominal image shows a large, complex abdominopelvic mass (green overlay) containing shadowing calcifications. The transvaginal image shows that part of the mass is adjacent to the bladder (B).
The ultrasound appearance is non-specific. However, real-time imaging showed superior extension from the right adnexa suggesting an ovarian origin, and the mass proved to be a teratoma. Teratomas range in appearance from predominantly cystic to predominantly solid.
C: cervix
Source: “Fig. 5 and 6, in: Ovarian Teratoma” by Laura Rubi Cuevas; Lauren Sylwanowicz, JETem, licensed under CC BY 4.0. Modifications: -asterix removed -removal of measurement on left image. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Differential diagnoses
- Ectopic pregnancy
- Tubo-ovarian abscess
- Ovarian tumors
The differential diagnoses listed here are not exhaustive.
Management
Management and follow-up are usually determined by cyst appearance and size as well as menopausal status. [5][6]
-
All patients
- Pain management: NSAIDs (first-line), opioids (only for severe cases)
- Treatment of underlying conditions such as polycystic ovary syndrome or endometriosis
- Refer for outpatient follow-up with a gynecologist.
- Consider gynecology consult prior to discharge for potentially malignant cysts.
-
Functional cysts
- Watchful waiting with repeat ultrasound
- Oral contraceptives are not routinely recommended. [9]
- Complications, large cysts, persistent painful cysts: Consider surgery.
In most patients with functional cysts, watchful waiting is recommended, as cysts often regress spontaneously.
Complications
- Ovarian torsion
- Ruptured ovarian cyst
- Hemorrhage

We list the most important complications. The selection is not exhaustive.
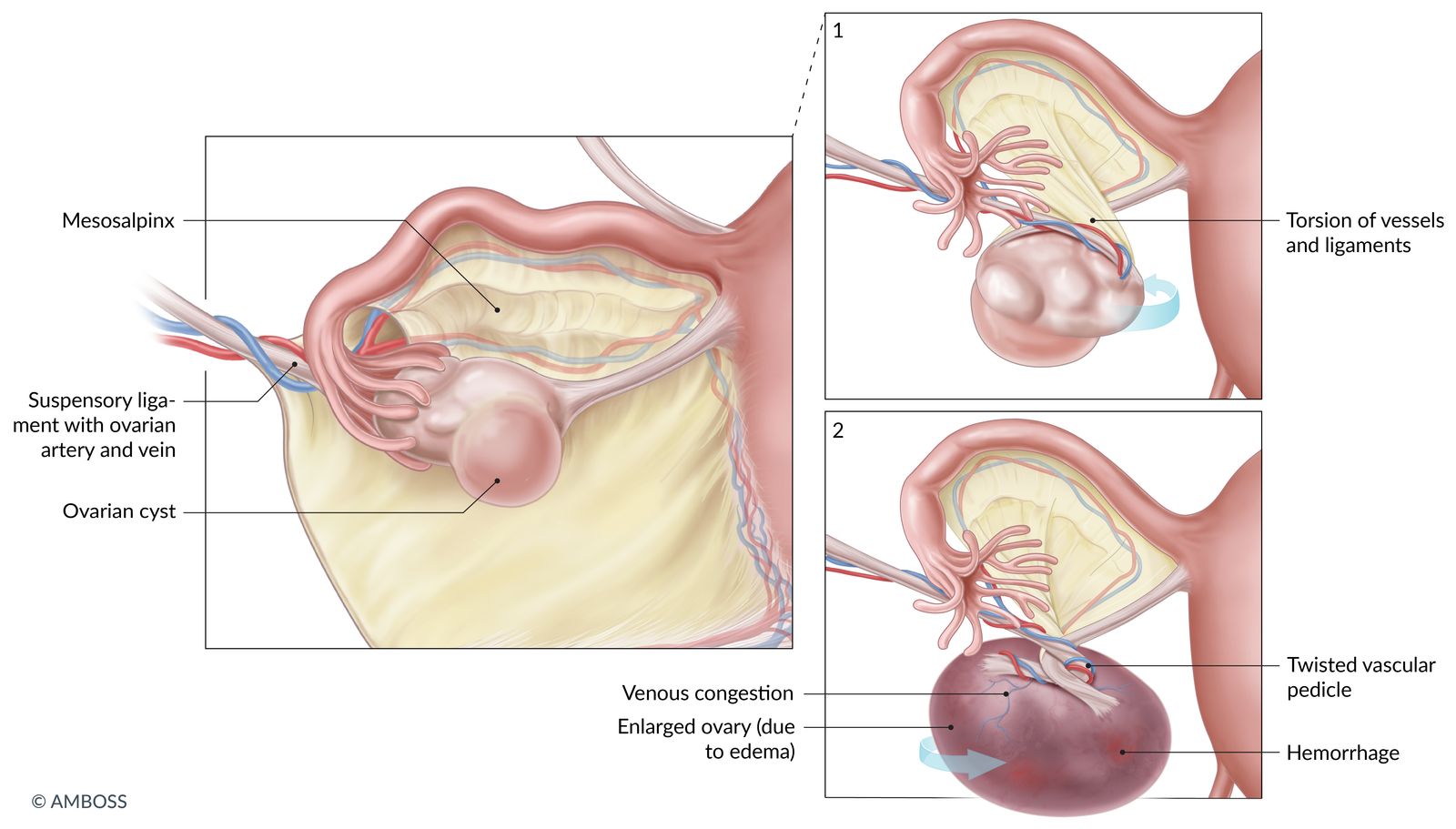
In ovarian torsion, the ovary twists around the adnexal ligaments, resulting in compression of the ovarian veins and lymphatics, consequently causing venous congestion and edema. The most important risk factor is ovarian enlargement, which can occur (e.g., due to ovarian cysts).
© AMBOSS
Ruptured ovarian cyst
Etiology [11]
- Rupture is caused by an increase in intracystic pressure.
- Most common type of ruptured cyst: corpus luteum cyst [12]
-
Risk factors
- Vigorous physical activity
- Vaginal intercourse
- Large cysts
- Reproductive age
Clinical features
- May be asymptomatic
- Sudden-onset unilateral lower abdominal pain [10]
- Possible signs of peritonitis [5]
- Possible nausea and vomiting [10]
- Minimal vaginal bleeding (spotting) may occur in some cases.
- In case of significant hemorrhage: hypovolemic shock [10]
Diagnostics [10]
Laboratory studies
- Urine or serum β-hCG: obtain in all patients to exclude intrauterine or ectopic pregnancy
- CBC: may show anemia
- Emergency preoperative diagnostics: coagulation panel, type and screen
Imaging
- POCUS/FAST: Consider in unstable patients to rapidly assess for the presence and extent of free fluid.
- Transabdominal/transvaginal pelvic ultrasound: imaging modality of choice
- Characteristic findings [10][12]
- Free fluid, most commonly in the pouch of Douglas (rectouterine pouch) [4][5]
- An adnexal mass may be visualized if the cyst is large.
- Disadvantage: cannot reliably distinguish between ruptured ovarian cyst or ruptured ectopic pregnancy in a pregnant patient. [13]
- Characteristic findings [10][12]
- CT pelvis with IV contrast: consider in nonpregnant patients if ultrasound findings are inconclusive
- Characteristic findings: pelvic hemoperitoneum [13]
Free fluid in the pouch of Douglas in a pregnant patient should raise concern for ruptured ectopic pregnancy.
Treatment [10][14][15]
-
Hemodynamically unstable patients: : emergency exploratory laparoscopy/laparotomy to obtain hemostasis
- Suturing or cauterization of the ruptured section or cystectomy
- Consider oophorectomy in intractable hemorrhage
-
Hemodynamically stable patients: conservative management with analgesics and observation
- Consider outpatient monitoring with close follow-up for patients with:
- Minimal hemoperitoneum
- Stable Hb on serial monitoring over 4–6-hours [16]
- Inpatient management if there is evidence of significant and/or ongoing hemorrhage [10]
- Monitor vital signs, hemoglobin, and hemoperitoneum size on ultrasound.
- Consider laparoscopy if there is concern for ongoing hemorrhage.
- Consider outpatient monitoring with close follow-up for patients with:
- All patients: Consider blood transfusion as needed.
Differential diagnoses
- Mittelschmerz
- Ruptured or bleeding ectopic pregnancy
- Tubo-ovarian abscess
- Ovarian torsion
- Acute appendicitis
- Diverticulitis
- See also: “Differential diagnosis of lower abdominal pain in young women.”
Acute management checklist for ruptured ovarian cyst
- Urgent OB/GYN consult
- NPO
- IV fluids (see IV fluid therapy)
- Parenteral analgesics: Opioid analgesics are preferred.
- Order emergency preoperative diagnostics and β-hCG.
- Obtain consent for blood transfusion and give emergent transfusion in suspected hemorrhagic shock.
- Hemodynamically unstable patients: emergency exploratory surgery for hemostasis
- Hemodynamically stable patients: Monitor vitals, Hb, and size of hemoperitoneum on imaging.
External Resources
- 2016 ACOG Practice Bulletin: Evaluation and Management of Adnexal Masses
- 2016 ACR Appropriateness Criteria Acute Pelvic Pain in the Reproductive Age Group
- 2019 ACR Consensus Guideline: O-RADS US Risk Stratification and Management System
- 2019 SRU Consensus Conference Update on Follow-up and Reporting of Simple Adnexal Cysts
- 2019 ACR Appropriateness Criteria: Clinically Suspected Adnexal Mass, No Acute Symptoms
References
- Shiner A, Burbos N. "Ovarian Cysts and Ovarian Cancer". InnovAiT. 5(9). :547-557. (2012)
- Hertzberg BS et al. "Ovarian cyst rupture causing hemoperitoneum: imaging features and the potential for misdiagnosis". Abdom Imaging. 24(3). :304-308. (1999)
- Bottomley C, Bourne T. "Diagnosis and management of ovarian cyst accidents". Best Pract Res Clin Obstet Gynaecol. 23(5). :711-724. (2009)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Bhosale PR et al. "ACR Appropriateness Criteria® Acute Pelvic Pain in the Reproductive Age Group". Ultrasound Q. 32(2). :108-115. (2016)
- Roche O, Chavan N, Aquilina J, Rockall A. "Radiological appearances of gynaecological emergencies". Insights Imaging. 3(3). :265-75. (2012)
- Lee JK, Bodur S, Guido R. "The management of gynecological hemoperitoneum found to be associated with a ruptured corpus luteum cyst". Gynecol Surg. 13(4). :305-311. (2016)
- Kim JH, Lee SM, Lee J-H, et al. "Successful Conservative Management of Ruptured Ovarian Cysts with Hemoperitoneum in Healthy Women". PLoS ONE. 9(3). :e91171. (2014)
- Mohamed M, Al-Ramahi G, McCann M. "Postcoital hemoperitoneum caused by ruptured corpus luteal cyst: a hidden etiology". J Surg Case Rep. 2015(10). :rjv120. (2015)
- Patel MD, Ascher SM, Horrow MM, et al. "Management of Incidental Adnexal Findings on CT and MRI: A White Paper of the ACR Incidental Findings Committee.". J Am Coll Radiol. 17(2). :248-254. (2020)
- R Eskander, M Berman, L Keder. "Practice Bulletin No. 174: Evaluation and Management of Adnexal Masses (reaffirmed 2021)". Obstet Gynecol. 128(5). :e210-e226. (2016)
- Expert Panel on GYN and OB Imaging, Patel-Lippmann KK, Wasnik AP, et al. "ACR Appropriateness Criteria® Clinically Suspected Adnexal Mass, No Acute Symptoms: 2023 Update". J Am Coll Radiol. 21(6S). :S79-S99. (2024)
- Levine D, Patel MD, Suh-Burgmann EJ, et al. "Simple Adnexal Cysts: SRU Consensus Conference Update on Follow-up and Reporting". Radiology. 293(2). :359-371. (2019)
- Bonde AA, Korngold EK, Foster BR, et al. "Radiological appearances of corpus luteum cysts and their imaging mimics". Abdom Radiol. 41(11). :2270-2282. (2016)
- Jung SI. "Ultrasonography of ovarian masses using a pattern recognition approach". Ultrasonography. 34(3). :173-182. (2015)
- Grimes DA, Jones LB, Lopez LM, Schulz KF. "Oral contraceptives for functional ovarian cysts". Cochrane Database Syst Rev. (2014)