Summary
A number of conditions affect the breasts, including disorders of breast development (e.g., congenital anomalies, breast hypertrophy), fibrocystic breast changes, inflammatory conditions (e.g., mastitis, mammary ductal ectasia), benign neoplasms (e.g., fibroadenoma, phyllodes tumor), breast cancer, and breast cysts. Mastalgia is a common symptom that is often caused by an underlying benign etiology. This article provides a brief overview of common breast conditions. Each condition is detailed in the respective articles.
See also “Palpable breast mass” and “Nipple discharge.”
Benign neoplasms
| Overview of benign neoplasms of the breast | ||||
|---|---|---|---|---|
| Disorder | Epidemiology | Clinical features | Diagnostics | Management |
| Fibroadenoma [1][2][3] |
|
|
|
|
| Phyllodes tumor [1][4] |
|
|
|
|
| Intraductal papilloma [5] |
|
|
|
|
| Lobular carcinoma in situ (LCIS) [6][7][8][9] |
|
|
|
|
Benign breast conditions most commonly affect women between the third and fifth decades of life.
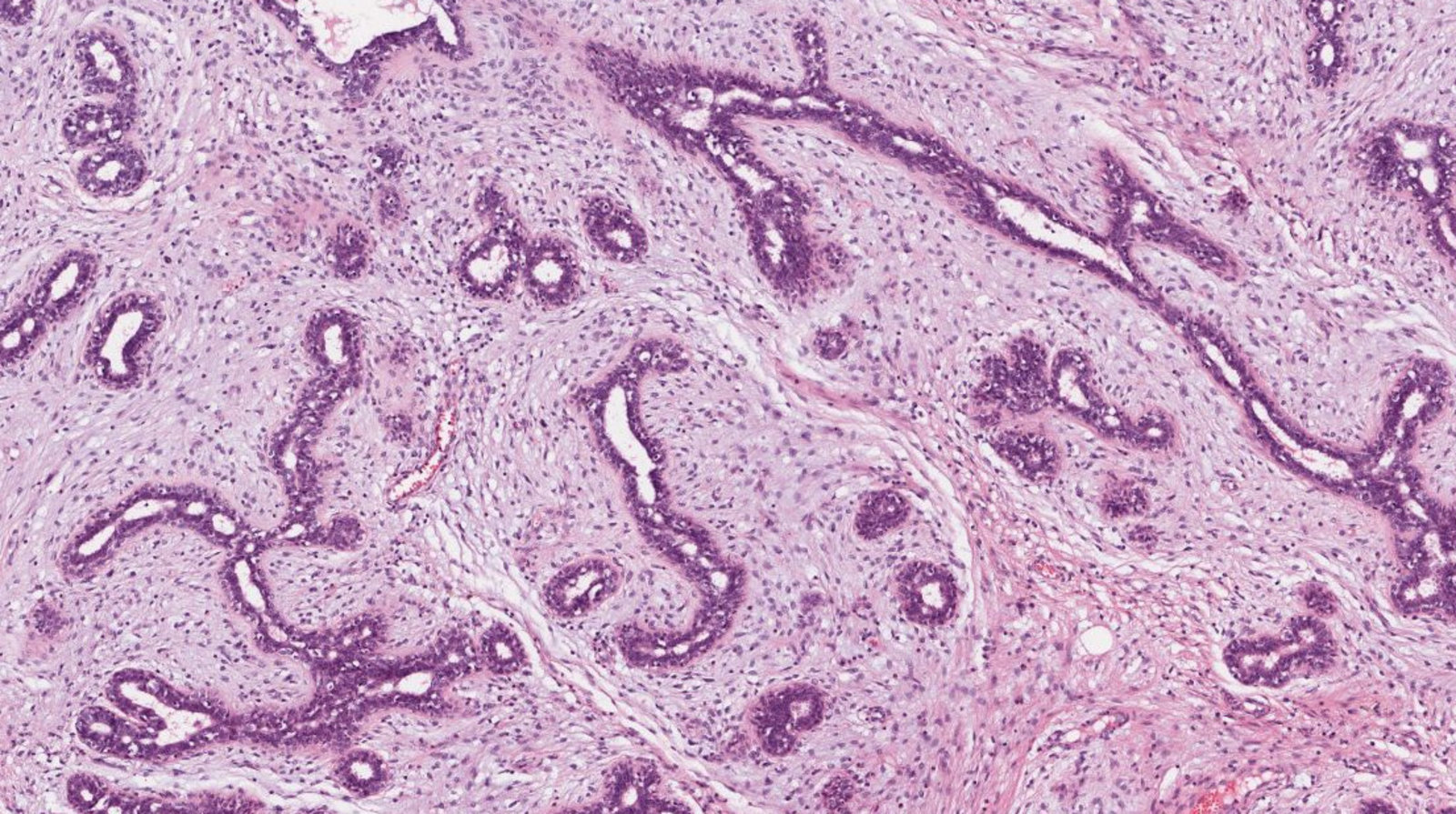
Photomicrograph of breast tissue (H&E stain; 200x magnification)
Compressed glandular spaces, i.e., epithelial component of fibroadenoma (green overlay) and stromal component of fibroadenoma (red overlay), are visible.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
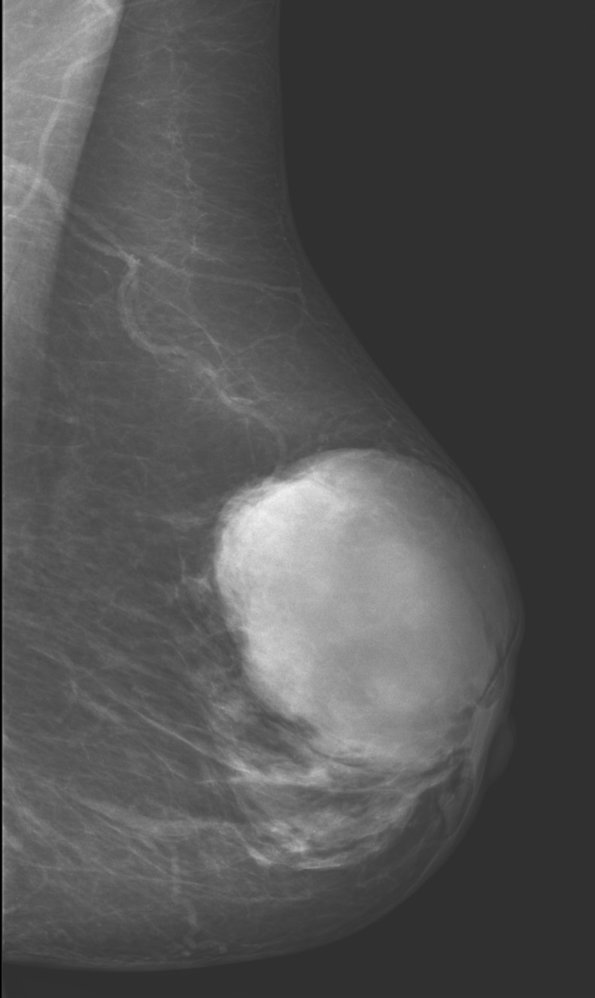
Mammography (left breast; mediolateral oblique view)
A large, high-density mass with a circumscribed, slightly lobulated margin is seen in the upper anterior breast.
Histopathology confirmed a phyllodes tumor.
Source: “Phylloidestumor der Mamma - Mammographie” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
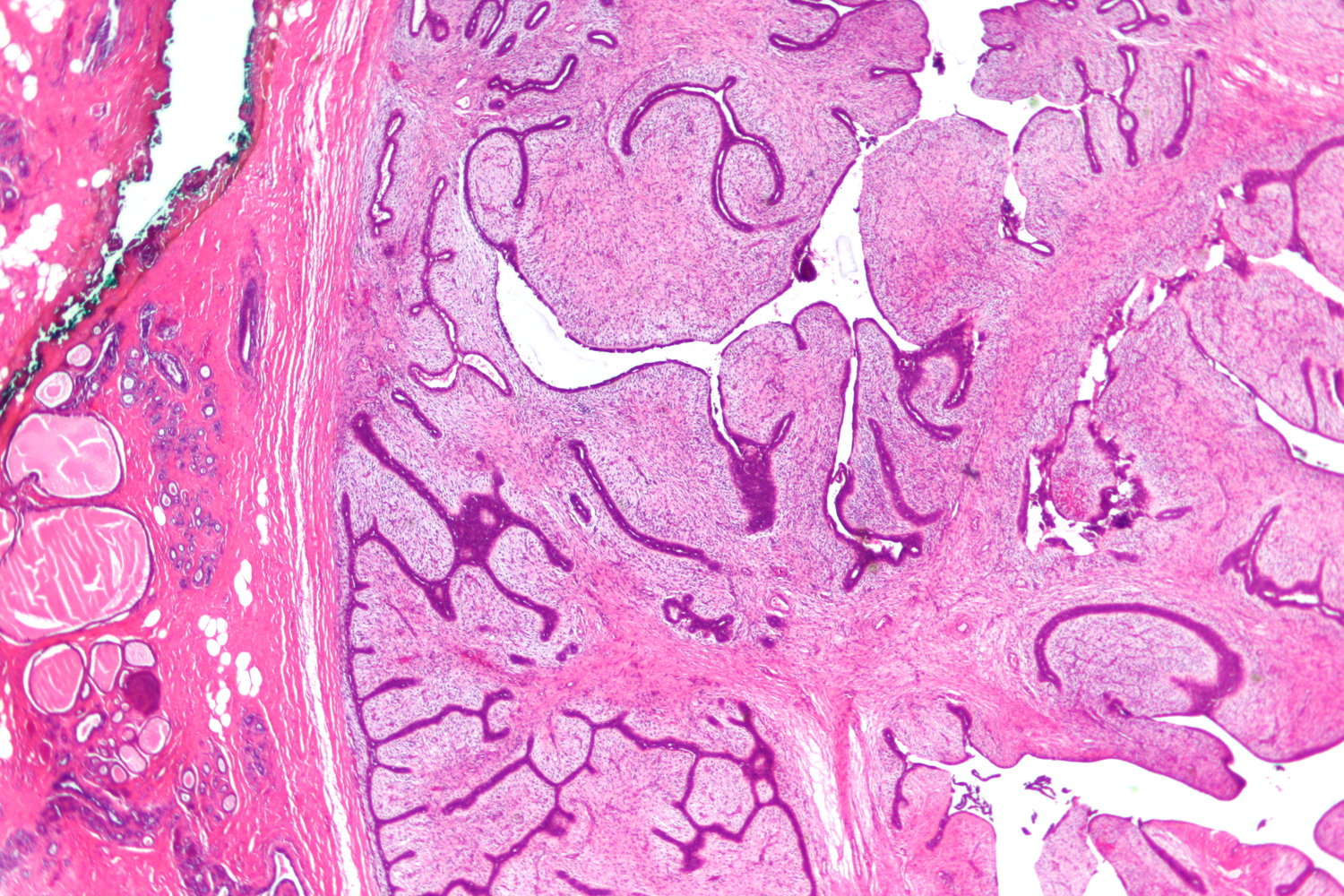
Photomicrograph of a breast tissue specimen (H&E stain; low magnification)
A hypercellular stroma (example indicated by blue overlay) is visible in the right half of the image. Several clefts or slit-like spaces (examples indicated by black dashed line) lined by darker stained epithelial cells are visible within the stroma, giving it a leaf-like appearance. These are characteristic features of a phyllodes tumor.
Normal breast tissue is visible in the left half of the image.
Source: “Phyllodes tumour - very low mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

Ultrasound breast
A well-defined solitary mass (blue overlay) is seen within a dilated mammary duct.
The main differential diagnoses are intraductal papilloma, ductal carcinoma (especially papillary carcinoma), and inspissated secretions. Secretions do not show vascularity on color Doppler. Intraductal papilloma may show a vascular stalk. Ductal carcinoma cannot always be reliably distinguished from intraductal papilloma by ultrasound.
Source: “Ultrasound image, intraductal papilloma” by Nevit Dilmen, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Malignant neoplasms
| Overview of malignant neoplasms of the breast | |||
|---|---|---|---|
| Clinical features | Breast imaging | Biopsy | |
| Invasive ductal carcinoma |
|
|
|
| Invasive lobular carcinoma |
|
||
| Inflammatory breast cancer |
|
|
|
| Paget disease of the breast |
|
|
|
Cysts and fibrocystic changes
| Overview of breast cysts and fibrocystic breast changes | ||||
|---|---|---|---|---|
| Disorder | Epidemiology | Clinical features | Diagnostics | Management |
| Fibrocystic breast changes [1][10] |
|
|
|
|
| Breast cysts [1][17][18] |
|
|
|
|
| Galactocele |
|
|
|
|
Benign inflammatory disorders
| Overview of benign inflammatory disorders of the breast | ||||
|---|---|---|---|---|
| Epidemiology | Clinical features | Diagnostics | Management | |
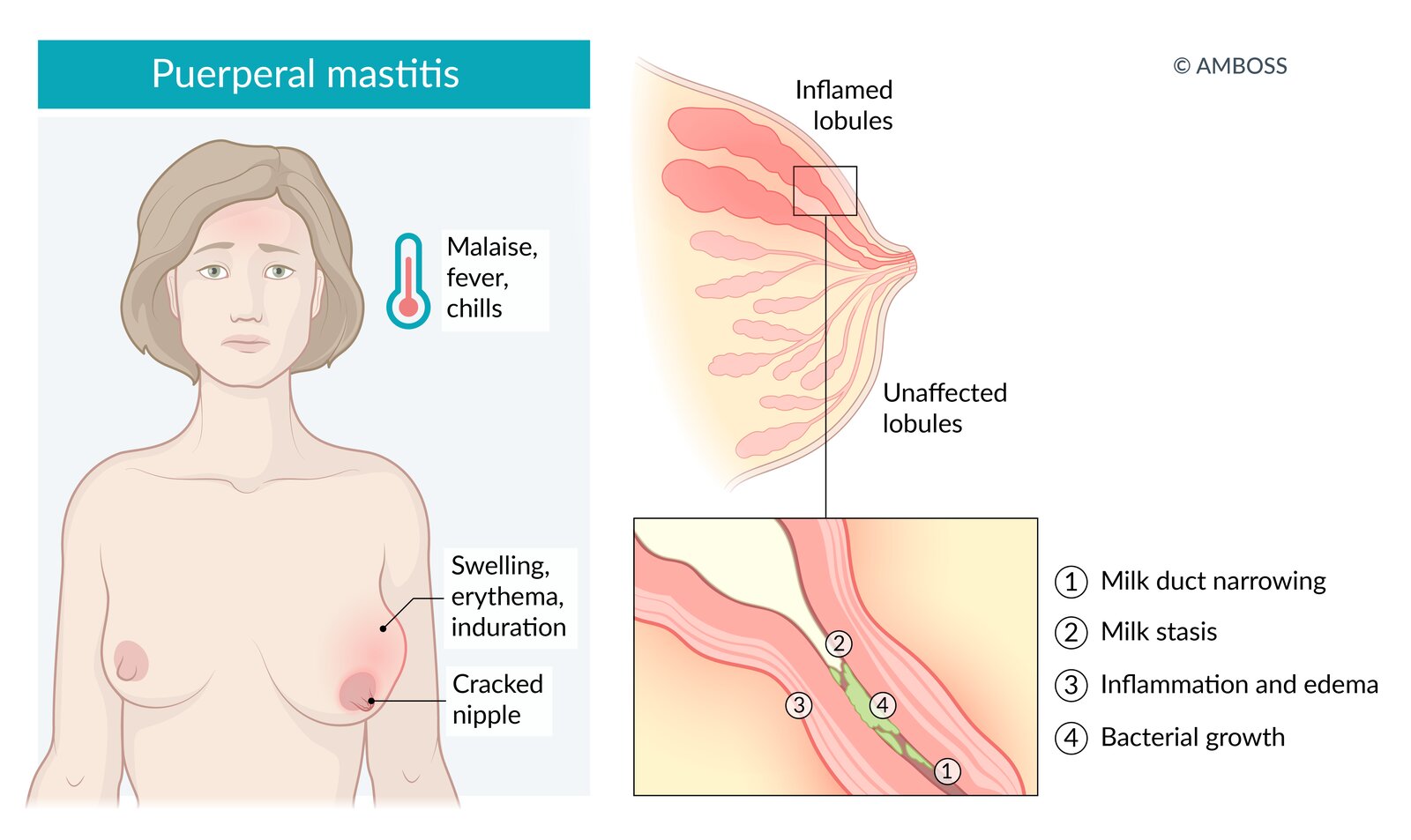
| Mastitis |
|
|
|
|
| Breast abscess |
|
|
|
|
| Fat necrosis of the breast |
|
|
|
|
| Mammary duct ectasia |
|
|
|
|
| Mondor disease of the breast |
|
|
|
|
© AMBOSS
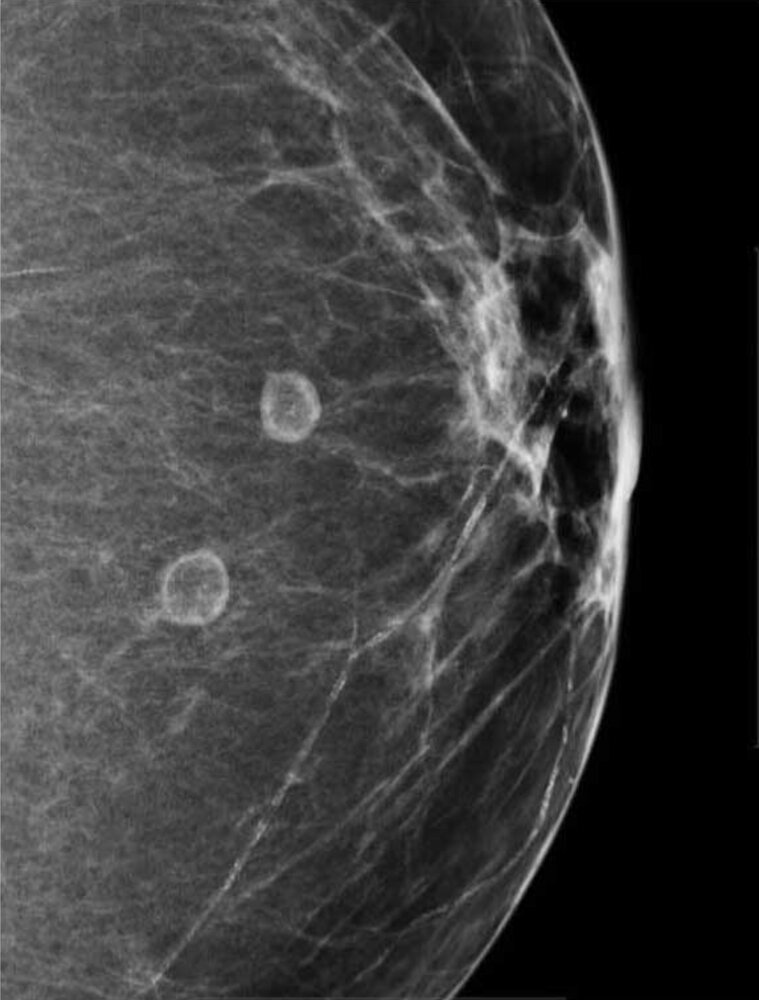
Mammography (left breast; mediolateral oblique projection)
Two circumscribed round masses can be seen in the fatty tissue of the breast. They have a thin radiopaque rim, which may indicate calcifications in the cyst wall.
These findings are typical of oil cysts, which result from benign fat necrosis.
Source: “Figure 5, in: Fat Necrosis of the Breast: A Pictorial Review of the Mammographic, Ultrasound, CT, and MRI Findings with Histopathologic Correlation” by William D. Kerridge, Oleksandr N. Kryvenko, Afua Thompson, Biren A. Shah, Hindawi, licensed under CC BY 3.0.
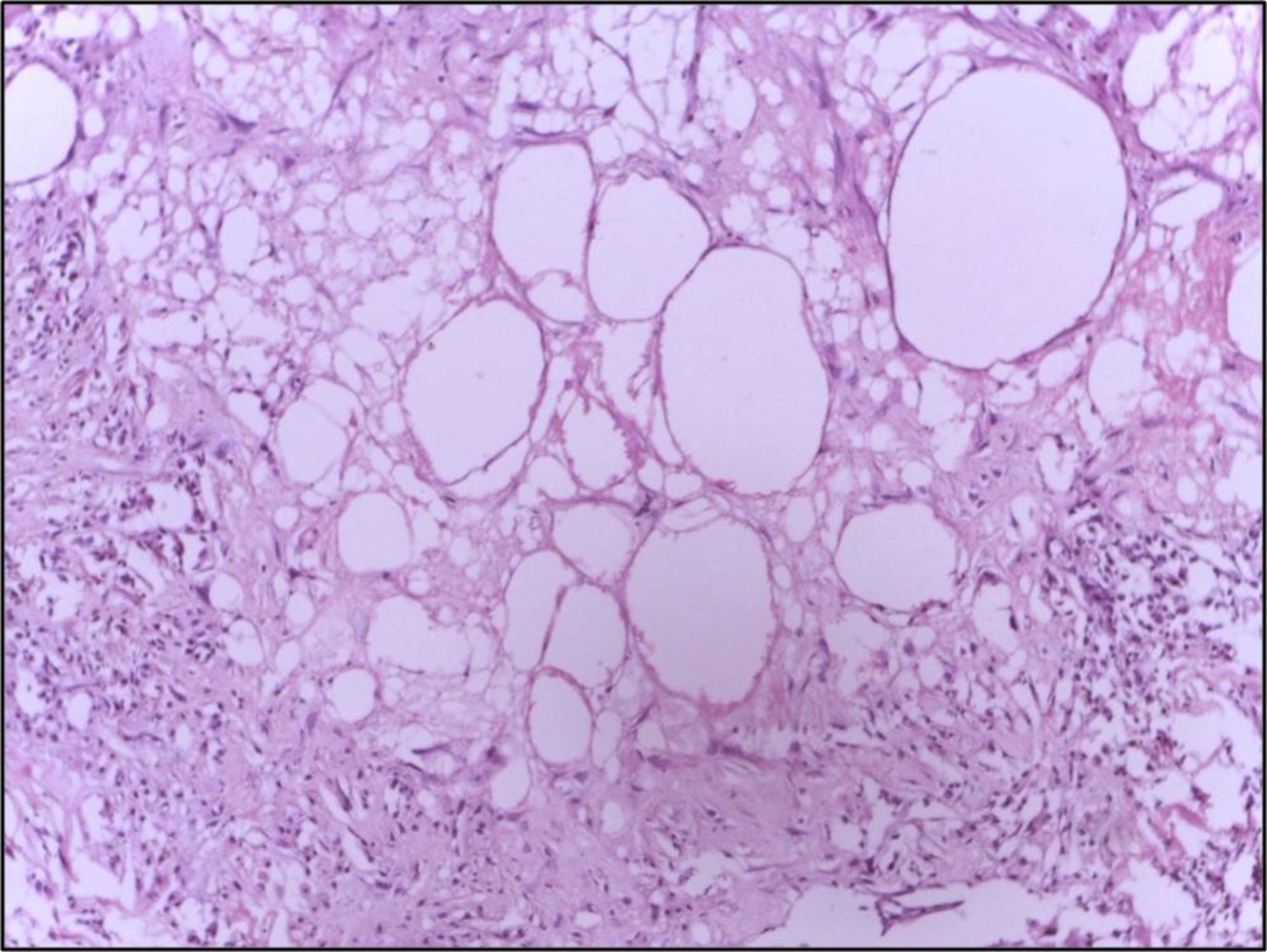
Photomicrograph of breast lesion (H&E stain; medium magnification)
Necrotic adipocytes (examples indicated by yellow overlay) are visible as adipocytes with indistinct, irregular borders and absent nuclei. Unstained, lipid-filled cystic spaces are visible in the center of the image (green overlay). An inflammatory infiltrate is present (example indicated by arrowhead).
These findings are characteristic of fat necrosis of the breast. At a higher magnification, cholesterol clefts, foam cells, and multinucleated giant cells would also be visible.
Source: “Breast tissue showing fat necrosis” by Department of Pathology, Calicut Medical College, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
Mastalgia
| Overview of mastalgia | ||||
|---|---|---|---|---|
| Disorder | Epidemiology | Clinical features | Diagnostics | Management |
| Cyclical mastalgia [1][32][35] |
|
|
|
|
| Noncyclical mastalgia [1][32][35] |
|
|
||
Disorders of breast development
| Overview of breast development disorders | ||||
|---|---|---|---|---|
| Disorder | Epidemiology | Clinical features | Diagnostics | Management |
| Congenital anomalies of the breast |
|
|
|
|
| Breast hypertrophy [38][39][40] |
|
|
|
|
| Gynecomastia [41][42][43] |
|
|
|
|
External Resources
References
- ACOG. "Practice Bulletin No. 164 Diagnosis and management of benign breast disorders". Obstetrics & Gynecology. 127(6). :e141-e156. (2016)
- Salzman B, Collins E, Hersh L. "Common Breast Problems". Am Fam Physician. 99(8). :505-514. (2019)
- Holbrook AI, Moy L, Akin EA, et al. "ACR Appropriateness Criteria Breast Pain". Journal of the American College of Radiology. 15(11). :S276-S282. (2018)
- Kopkash K, Yao K. "The surgeon’s guide to fibroadenomas". Ann Breast Surg. 4. :25-25. (2020)
- Rao R, Ludwig K, Bailey L, et al. "Select Choices in Benign Breast Disease: An Initiative of the American Society of Breast Surgeons for the American Board of Internal Medicine Choosing Wisely® Campaign". Ann Surg Oncol. 25(10). :2795-2800. (2018)
- Simpson A, Li P, Dietz J. "Diagnosis and management of phyllodes tumors of the breast". Ann Breast Surg. 5. :8-8. (2021)
- Calvillo KZ, Portnow LH. "Intraductal papillomas of the breast". Ann Breast Surg. 5. :24-24. (2021)
- Wong SM, Stout NK, Punglia RS, et al. "Breast cancer prevention strategies in lobular carcinoma in situ: A decision analysis". Cancer. 123(14). :2609-2617. (2017)
- King TA, Pilewskie M, Muhsen S, et al. "Lobular Carcinoma in Situ: A 29-Year Longitudinal Experience Evaluating Clinicopathologic Features and Breast Cancer Risk". Journal of Clinical Oncology. 33(33). :3945-3952. (2015)
- Thomas PS. "Diagnosis and Management of High-Risk Breast Lesions". Journal of the National Comprehensive Cancer Network. 16(11). :1391-1396. (2018)
- Wen HY, Brogi E. "Lobular Carcinoma In Situ". Surg Pathol Clin. 11(1). :123-145. (2018)
- Kulkarni D, Dixon JM. "Congenital Abnormalities of the Breast". Women's Health. 8(1). :75-88. (2012)
- Borsuk D, Caouette-Laberge L. "Congenital Anomalies of the Breast". Seminars in Plastic Surgery. 27(01). :036-041. (2013)
- Perdikis G, Dillingham C, Boukovalas S, et al. "American Society of Plastic Surgeons Evidence-Based Clinical Practice Guideline Revision: Reduction Mammaplasty". Plast Reconstr Surg. 149(3). :392e-409e. (2022)
- Jones K, Pruthi S. "Nonsurgical Management of Fibroadenoma and Virginal Breast Hypertrophy". Semin Plast Surg. 27(01). :062-066. (2013)
- Fonseca CC, Veiga DF, Garcia E da S, et al. "Breast Hypertrophy, Reduction Mammaplasty, and Body Image". Aesthet Surg J. 38(9). :972-979. (2018)
- Narula HS, Carlson HE. "Gynaecomastia—pathophysiology, diagnosis and treatment". Nat. Rev. Endocrinol.. 10(11). :684-698. (2014)
- Kanakis GA, Nordkap L, Bang AK, et al. "EAA clinical practice guidelines—gynecomastia evaluation and management". Andrology. 7(6). :778-793. (2019)
- Dickson G. "Gynecomastia". Am Fam Physician. 85(7). :716-22. (2012)
- Mitchell KB, Johnson HM, Rodríguez JM, et al. "Academy of Breastfeeding Medicine Clinical Protocol #36: The Mastitis Spectrum, Revised 2022". Breastfeed Med. 17(5). :360-376. (2022)
- Moy L, Heller SL, Bailey L, et al. "ACR Appropriateness Criteria ® Palpable Breast Masses". J Am Coll Radiol. 14(5). :S203-S224. (2017)
- Trop I, Dugas A, David J, et al. "Breast Abscesses: Evidence-based Algorithms for Diagnosis, Management, and Follow-up". RadioGraphics. 31(6). :1683-1699. (2011)
- diFlorio-Alexander RM, Slanetz PJ, Moy L, et al. "ACR Appropriateness Criteria® Breast Imaging of Pregnant and Lactating Women". J Am Coll Radiol. 15(11). :S263-S275. (2018)
- Guirguis MS, Adrada B, Santiago L, Candelaria R, Arribas E. "Mimickers of breast malignancy: imaging findings, pathologic concordance and clinical management". Insights Imaging. 12(1). (2021)
- Khan TV, Ramirez M. "Management of Common Breastfeeding Problems". Clinical Lactation. 8(4). :181-188. (2017)
- Amir LH. "ABM Clinical Protocol #4: Mastitis, Revised March 2014". Breastfeed Med. 9(5). :239-243. (2014)
- Pluguez-Turull CW, Nanyes JE, Quintero CJ, et al. "Idiopathic Granulomatous Mastitis: Manifestations at Multimodality Imaging and Pitfalls". RadioGraphics. 38(2). :330-356. (2018)
- Spencer JP. "Management of mastitis in breastfeeding women". Am Fam Physician. 78(6). :727-731. (2008)
- Cho SH, Park SH. "Mimickers of Breast Malignancy on Breast Sonography". Journal Ultrasound Med. 32(11). :2029-2036. (2013)
- Boakes E, Woods A, et al. "Breast Infection: A Review of Diagnosis and Management Practices". Eur J Breast Health. (2018)
- Kerridge WD, Kryvenko ON, Thompson A, Shah BA. "Fat necrosis of the breast: a pictorial review of the mammographic, ultrasound, CT, and MRI findings with histopathologic correlation". Radiol Res Pract. 2015. :1-8. (2015)
- Warren R, Degnim A. "Uncommon Benign Breast Abnormalities in Adolescents". Semin Plast Surg. 27(01). :026-028. (2013)
- Dodelzon K, Katzen JT. "Evaluation of Palpable Breast Abnormalities". J Breast Imaging. 1(3). :253-263. (2019)
- Choe AI, Kasales C, Mack J, Al-Nuaimi M, Karamchandani DM. "Fibrocystic Changes of the Breast: Radiologic–Pathologic Correlation of MRI". J of Breast Imaging. 4(1). :48-55. (2021)
- Choe J, Chikarmane SA, Giess CS. "Nonmass Findings at Breast US: Definition, Classifications, and Differential Diagnosis". RadioGraphics. 40(2). :326-335. (2020)
- Goldbach AR, Tuite CM, Ross E. "Clustered Microcysts at Breast US: Outcomes and Updates for Appropriate Management Recommendations". Radiology. 295(1). :44-51. (2020)
- Rinaldi P, Ierardi C, Costantini M, et al. "Cystic Breast Lesions". J Ultrasound Med. 29(11). :1617-1626. (2010)
- Maimone S, Ocal IT, Robinson KA, Wasserman MC, Maxwell RW. "Characteristics and Management of Male Breast Parenchymal Cysts". J Breast Imaging. 2(4). :330-335. (2020)
- Pleasant V. "Management of breast complaints and high-risk lesions". Best Practice & Research Clinical Obstetrics & Gynaecology. 83. :46-59. (2022)
- Bevers TB, Helvie M, Bonaccio E, et al. "Breast Cancer Screening and Diagnosis, Version 3.2018, NCCN Clinical Practice Guidelines in Oncology". Journal of the National Comprehensive Cancer Network. 16(11). :1362-1389. (2018)
- Clark HR, Merchant KA, Omar LA, Compton LM, Hayes JC. "Breast Lesions in Women Aged Younger than 30 Years: Clinical Presentation, Diagnosis, and Management". J Breast Imaging. 2(1). :72-80. (2020)
- Kieturakis AJ, Wahab RA, Vijapura C, Mahoney MC. "Current Recommendations for Breast Imaging of the Pregnant and Lactating Patient". American Journal of Roentgenology. 216(6). :1462-1475. (2021)
- Vashi R, Hooley R, Butler R, Geisel J, Philpotts L. "Breast Imaging of the Pregnant and Lactating Patient: Physiologic Changes and Common Benign Entities". AJR Am J Roentgenol .. 200(2). :329-336. (2013)
- "Non-cancerous Breast Conditions". https://www.cancer.org/cancer/breast-cancer/non-cancerous-breast-conditions.html. [2017-02-18]
- "Fibrocystic breast disease". https://medlineplus.gov/ency/article/000912.htm. [2014-04-11]
- "Mastitis". http://www.mayoclinic.org/diseases-conditions/mastitis/basics/definition/con-20026633. [2015-06-12]
- Zendehdel M, Niakan B, Keshtkar A, Rafiei E, Salamat F. "Subtypes of Benign Breast Disease as a Risk Factor for Breast Cancer: A Systematic Review and Meta-Analysis Protocol.". Iranian journal of medical sciences. 43(1). :1-8. (2018)
- Tan PH, Lai LM, Carrington EV, et al. "Fat necrosis of the breast—A review". The Breast. 15(3). :313-318. (2005)