Summary
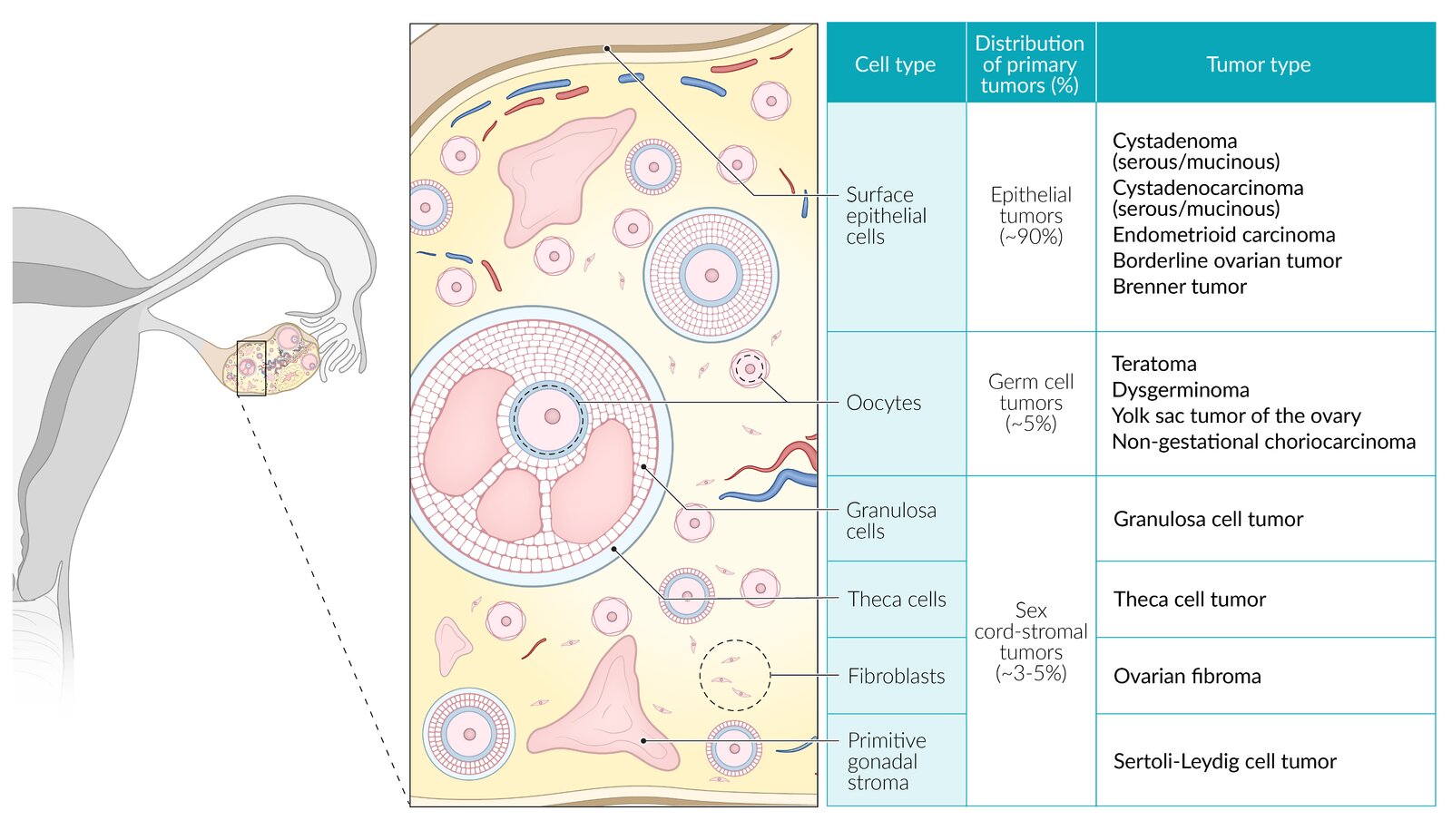
The ovaries consist of different types of tissue (epithelial, germ cells, and sex cord tissue), which may give rise to benign or malignant tumors. Epithelial ovarian tumors are the most common tumor subtype.
For information about ovarian cancer, see “Ovarian cancer.”
Classification of ovarian tumors
Classification of ovarian tumors
-
Epithelial ovarian tumors
- Arise from ovarian surface epithelium
- Most commonly benign
-
Germ cell ovarian tumors
- Arise from the primordial germ cells (e.g., oocytes)
- Can be benign or malignant
-
Sex cord and stromal ovarian tumors
- Arise from sex cord cells (e.g., Sertoli or granulosa cells) or stromal cells (e.g., fibroblasts or primitive gonadal stroma)
- Can be benign or malignant

© AMBOSS
Epithelial ovarian tumors
-
Frequency [3]
- Most common benign and malignant ovarian tumor subtype
- Epithelial tumors account for ∼ 90% of all ovarian malignancies
-
Histological classification
- Benign: lack hyperproliferative and invasive behavior
- Borderline ovarian tumors: a histopathological term that describes an ovarian tumor of low malignant potential that expresses cytologic features of malignancy without frank invasion
- Malignant: evidence of invasion
-
Clinicopathological classification [4]
-
Type I ovarian tumors: low-grade, indolent tumors that typically manifest as large, unilateral, cystic neoplasms
- Histologic subtypes include low-grade serous, endometrioid, clear cell, mucinous carcinomas, and malignant Brenner tumors
- Account for ∼ 10% of ovarian cancer deaths
- Associated with low levels of chromosomal instability
- p53 mutations are uncommon.
-
Type II ovarian tumors: high-grade, aggressive tumors that typically involve both ovaries and are diagnosed at an advanced stage
- Histologic subtypes include high-grade serous, carcinosarcoma, and undifferentiated carcinoma
- Account for ∼ 90% of ovarian cancer deaths
- Associated with high levels of chromosomal instability
- p53 mutations are common
-
Type I ovarian tumors: low-grade, indolent tumors that typically manifest as large, unilateral, cystic neoplasms
| Types of epithelial ovarian tumors | ||||||||
|---|---|---|---|---|---|---|---|---|
| Type | Cystadenoma | Brenner tumor[5] | Cystadenocarcinoma | Endometrioid carcinoma [3][6] | Clear cell tumors [3][7] | |||
| Ovarian serous cystadenoma | Ovarian mucinous cystadenoma | Serous | Mucinous [8] | |||||
| Classification |
|
|
||||||
| Epidemiology |
|
|
|
|
|
|
||
| ||||||||
| Clinical features |
|
|
|
|||||
| Ultrasound appearance |
|
|
|
|
|
|
||
|
|
|||||||
| Pathology | Gross examination |
|
|
|
|
|
|
|
| Histology |
|
|
|
|
|
|
|
|
| Tumor marker |
|
|||||||
CA-125 is used as a tumor marker for epithelial ovarian cancer but can also be elevated in endometriosis, cirrhosis, and malignancies (e.g., uterine leiomyoma).
Most ovarian tumors are benign, not malignant.

Source: “Mucinous Cystadenocarcinoma of the Ovary” by Ed Uthman, Flickr, licensed under CC BY 2.0.
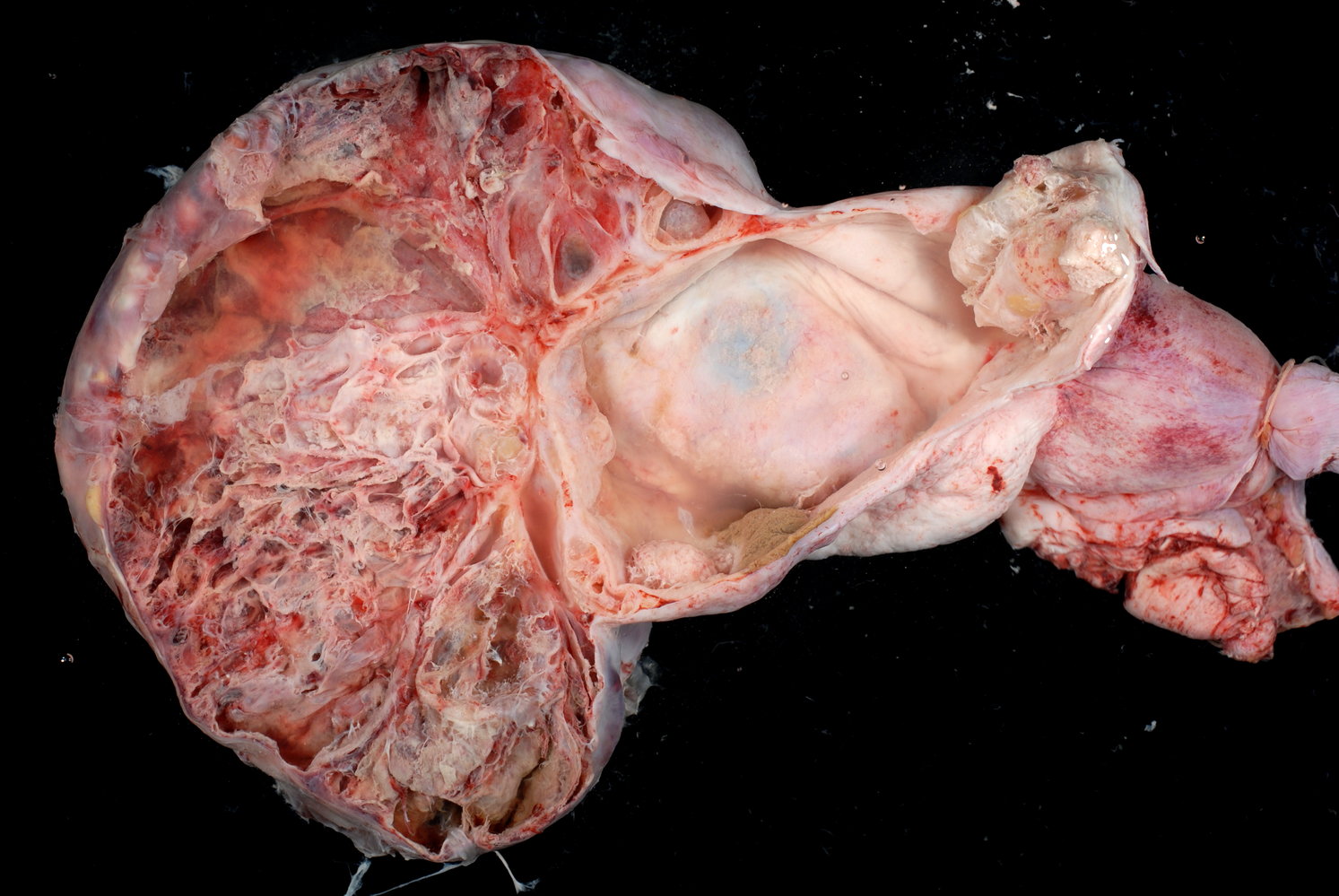
Macroscopic specimen of a right ovary (longitudinal section)
The ovary is significantly enlarged and completely transformed into a multilocular cyst. The ovarian surface is smooth on all sides (examples indicated by arrows). The cysts have partly smooth (examples indicated by green overlay) and partly polypoid raised inner walls (examples indicated by black lines) and were found to contain mucinous contents. In some areas, the cyst walls are noticeably thickened (examples indicated by blue overlay).
Histological examination revealed a mucinous borderline tumor of the ovary.
Source: “Proliferating Mucinous Tumor of the Ovary (1)” by Ed Uthman, Flickr, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Histopathology slide of the ovary (H&E stain)
In addition to papillary tumor cells, there are two Psammoma bodies located in the lower left corner of the image (red overlay). Psammoma bodies are concentric, lamellar calcifications, which are characteristic for serous tumors of the ovary.
Source: © IMPP
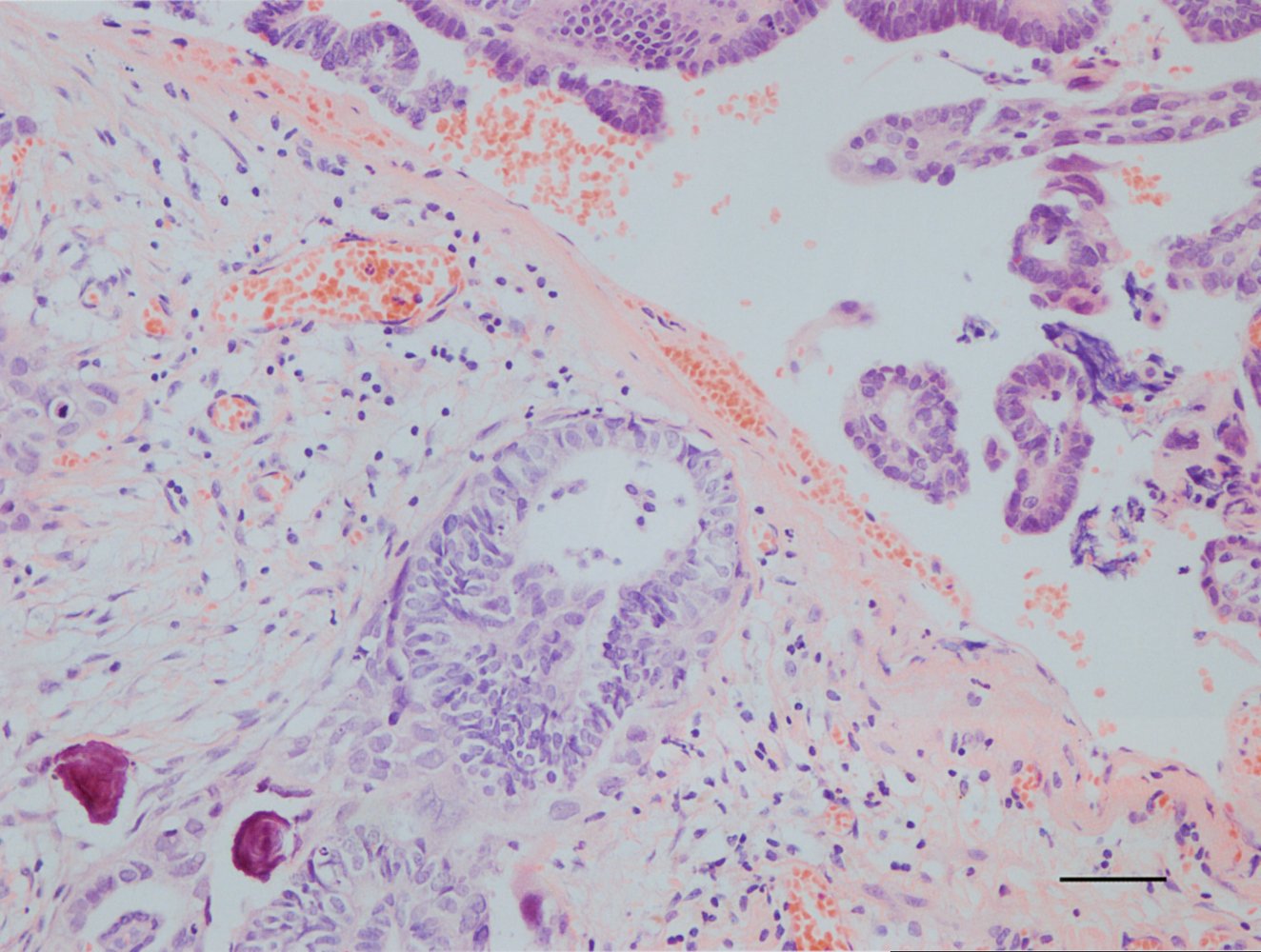
Photomicrograph of an ovarian tissue specimen (H&E stain; high magnification)
A cyst (green overlay) lined by a single layer of columnar mucinous epithelium (white dashed line) is visible. The nuclei can be seen at the basal aspect of the cells (black arrow) with mucinous vacuoles visible apically. No cytologic atypia is visible.
This appearance is typical of an ovarian mucinous cystadenoma.
Source: “Ovarian_mucinous_cystadenoma_-_a2_--_intermed_mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
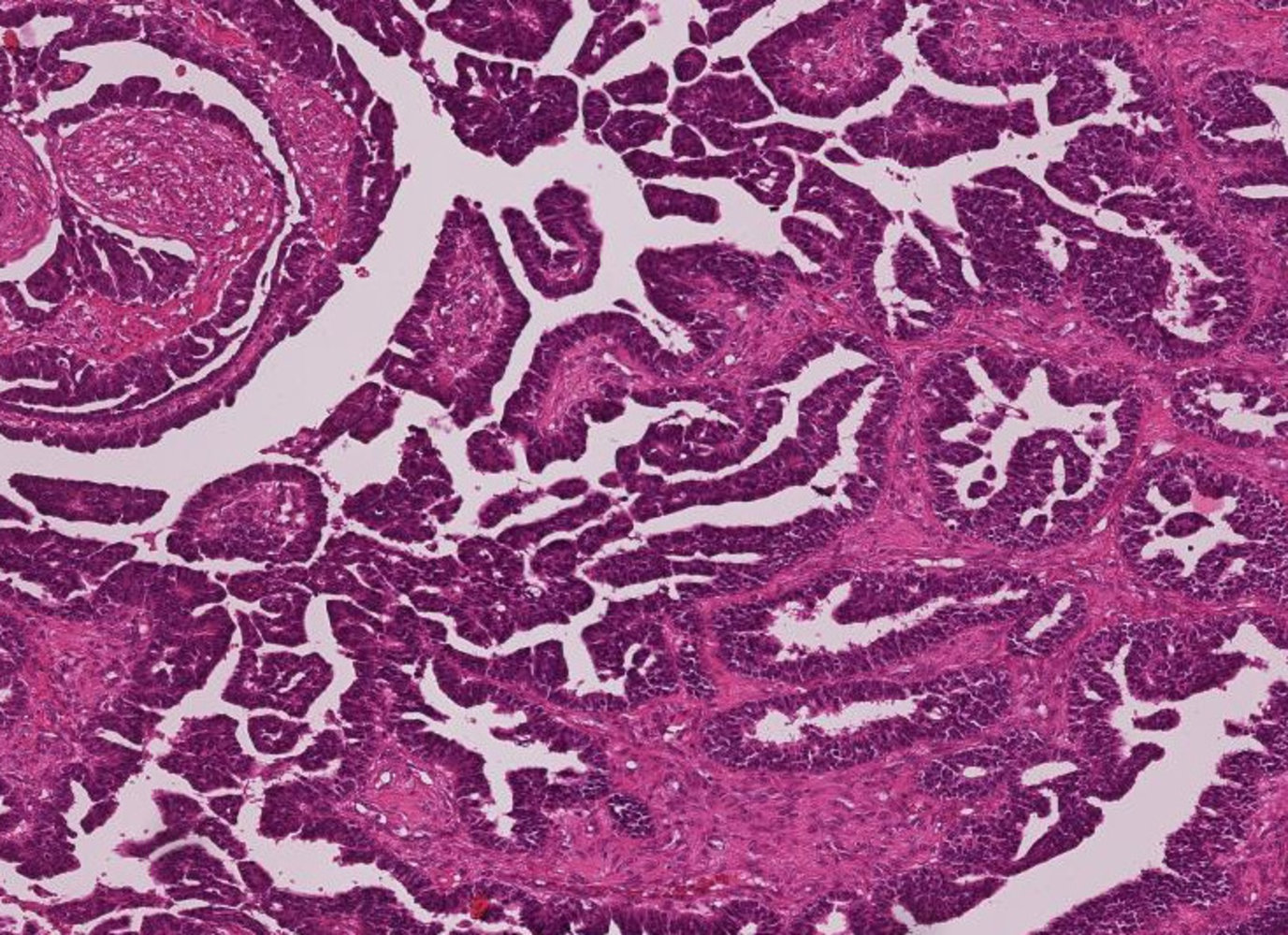
Photomicrograph of specimen from an ovarian cystic mass (H&E stain, medium magnification):
The carcinoma has a complex papillary architecture, with stromal cores lined by atypical, intensely staining (serous) epithelial cells. At higher magnification, these cells show hyperchromatic (dark blue staining), pleomorphic nuclei that often contain mitotic or apoptotic figures.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
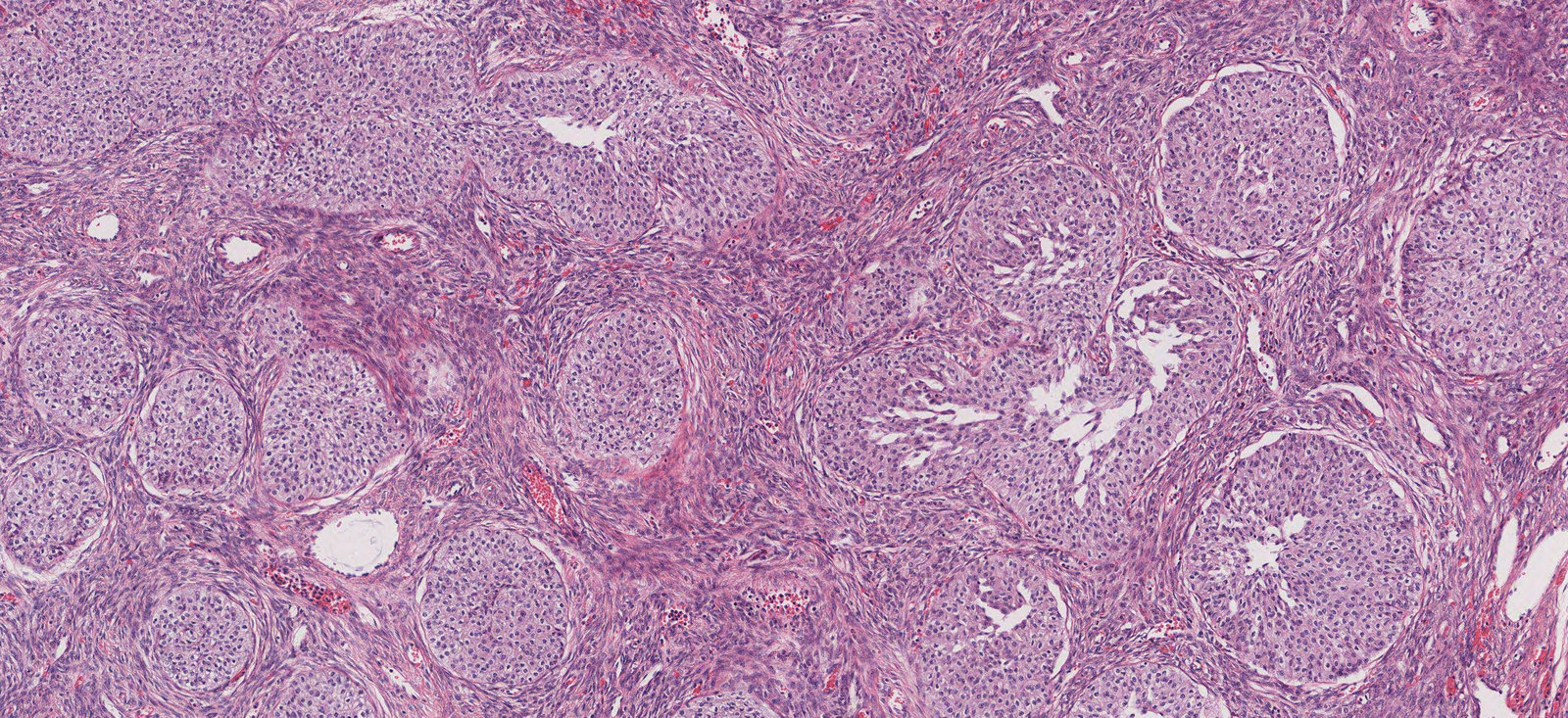
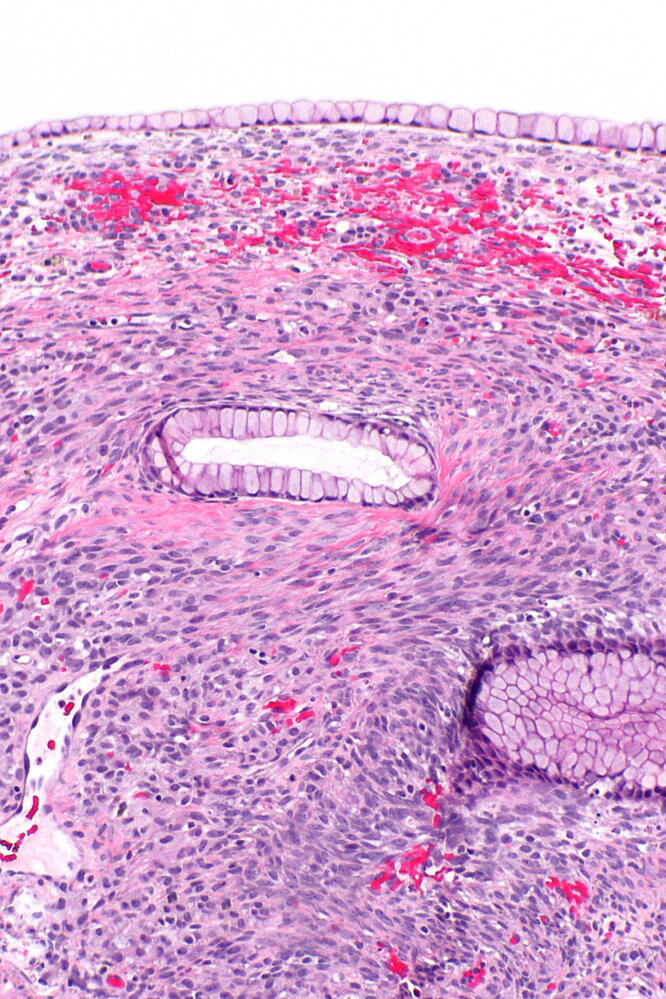
Photomicrograph of ovary tissue (H&E stain; 300x magnification)
Circular aggregations of tumor cells forming nests (examples indicated by green overlays) are visible throughout the specimen. These nests appear to be embedded in fusiform stroma (white overlay).
These findings are characteristic of a benign type of epithelial tumor known as a Brenner tumor.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie

Anatomical specimen of the ovary
The ovary is enlarged (11 cm in diameter). There are multiple chambered cysts that were filled mainly with mucinous secretions. Histological examination is needed to rule out malignancy (adenocarcinoma).
Source: “Ovarian Mucinous Cystadenoma” by Ed Uthman, MD, Flickr, licensed under CC BY 2.0.
Ovarian germ cell tumors
- Frequency: ∼ 5% of all ovarian tumors [3]
-
Subtypes are determined by structural differentiation
- Extraembryonic differentiation: yolk sac tumor
- Somatic differentiation: teratoma
- No differentiation: dysgerminoma
| Types of ovarian germ cell tumors | |||||||
|---|---|---|---|---|---|---|---|
| Type | Teratoma | Yolk sac tumor of the ovary (endodermal sinus tumor) [11] | Dysgerminoma [12] | Nongestational choriocarcinoma [13] | Embryonal carcinoma of the ovary | ||
| Dermoid cysts (mature cystic teratoma) | Struma ovarii (mature teratoma) [14] | Immature teratoma [15] | |||||
| Classification |
|
|
|||||
| Epidemiology |
|
|
|
|
|
|
|
| Clinical features |
|
|
|
|
|||
|
|
||||||
| Ultrasound appearance |
|
|
|
|
|
|
|
| Histopathology |
|
|
|
|
|
|
|
| Tumor markers |
|
|
|
|
|
||
|
|
||||||
| Risk of malignant transformation |
|
|
|
||||
")





Resection specimen of a mature teratoma of the ovary
This sebaceous and solid ovarian tumor contains skin, fat, hair, and cartilage.
Mature teratomas can derive from all three embryological germ layers.
Source: © IMPP
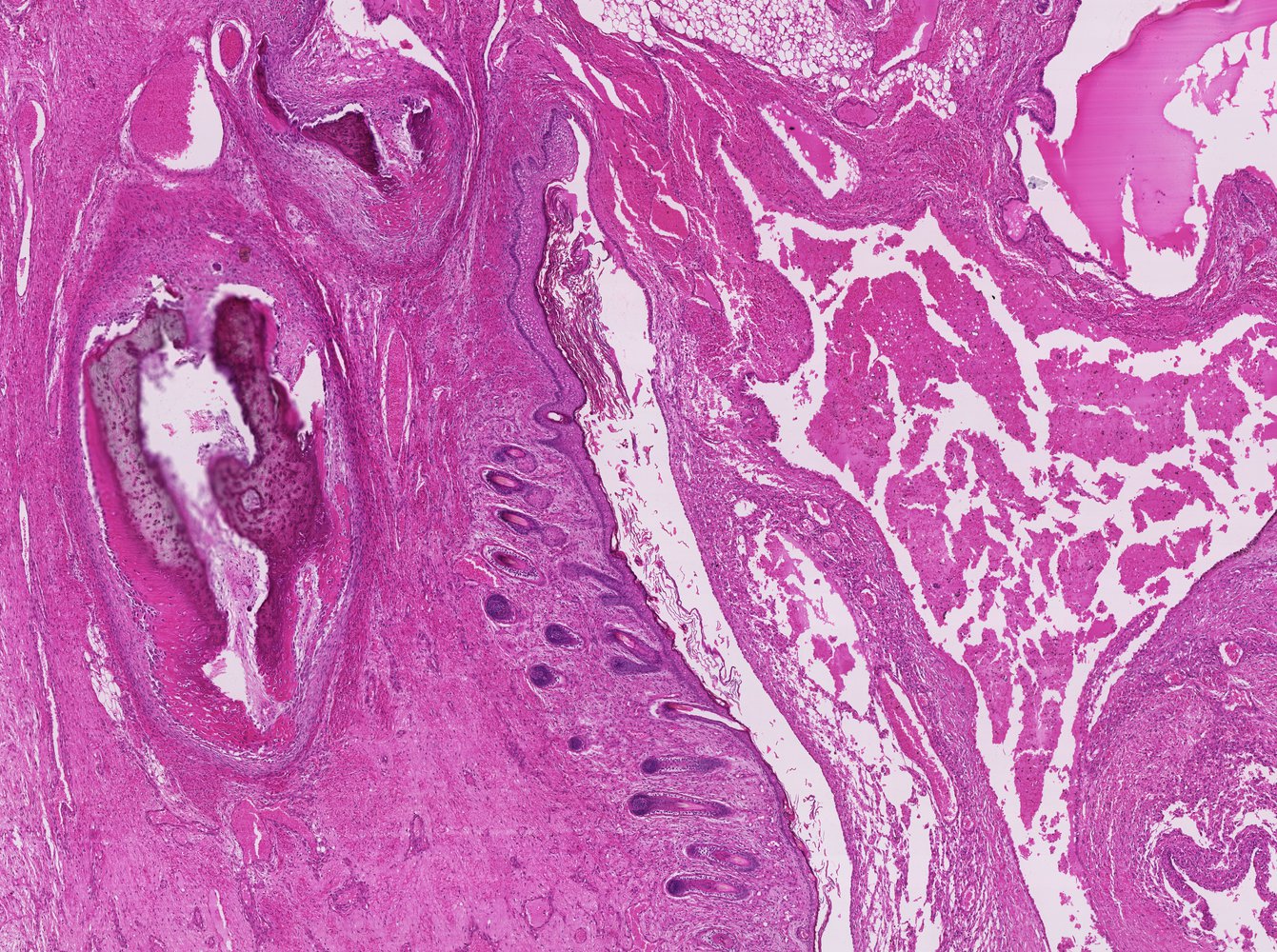
Photomicrograph of ovary tissue (H&E stain; low magnification)
On the left is an area of dark-pink-stained bone matrix with embedded osteocytes and osteoblasts in the periphery of the aggregation. Various purple-stained hair follicles can be seen from the center to the bottom of the image.
These findings are consistent with a mature teratoma.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
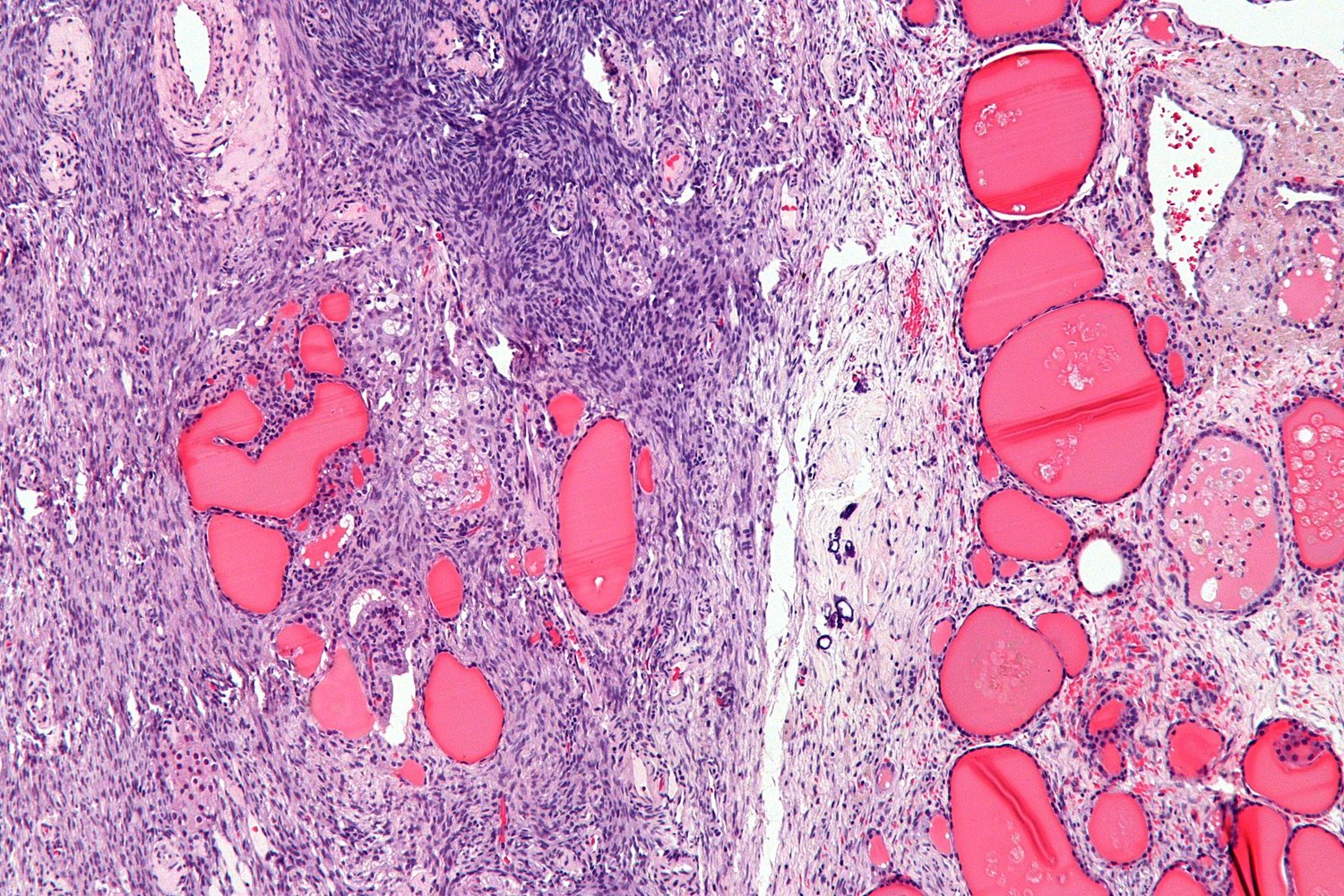
Photomicrograph of ovarian tissue specimen (H&E stain; low magnification)
Teratoma with endodermal differentiation into thyroid tissue. Numerous thyroid follicles (examples indicated by green overlay) filled with colloid and lined by simple flat/cuboidal epithelium are visible. Normal ovarian stroma (OS) is visible on the left and in the center of the image.
Source: “Struma ovarii - intermed mag” by Michael Bonert ("Nephron"), Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
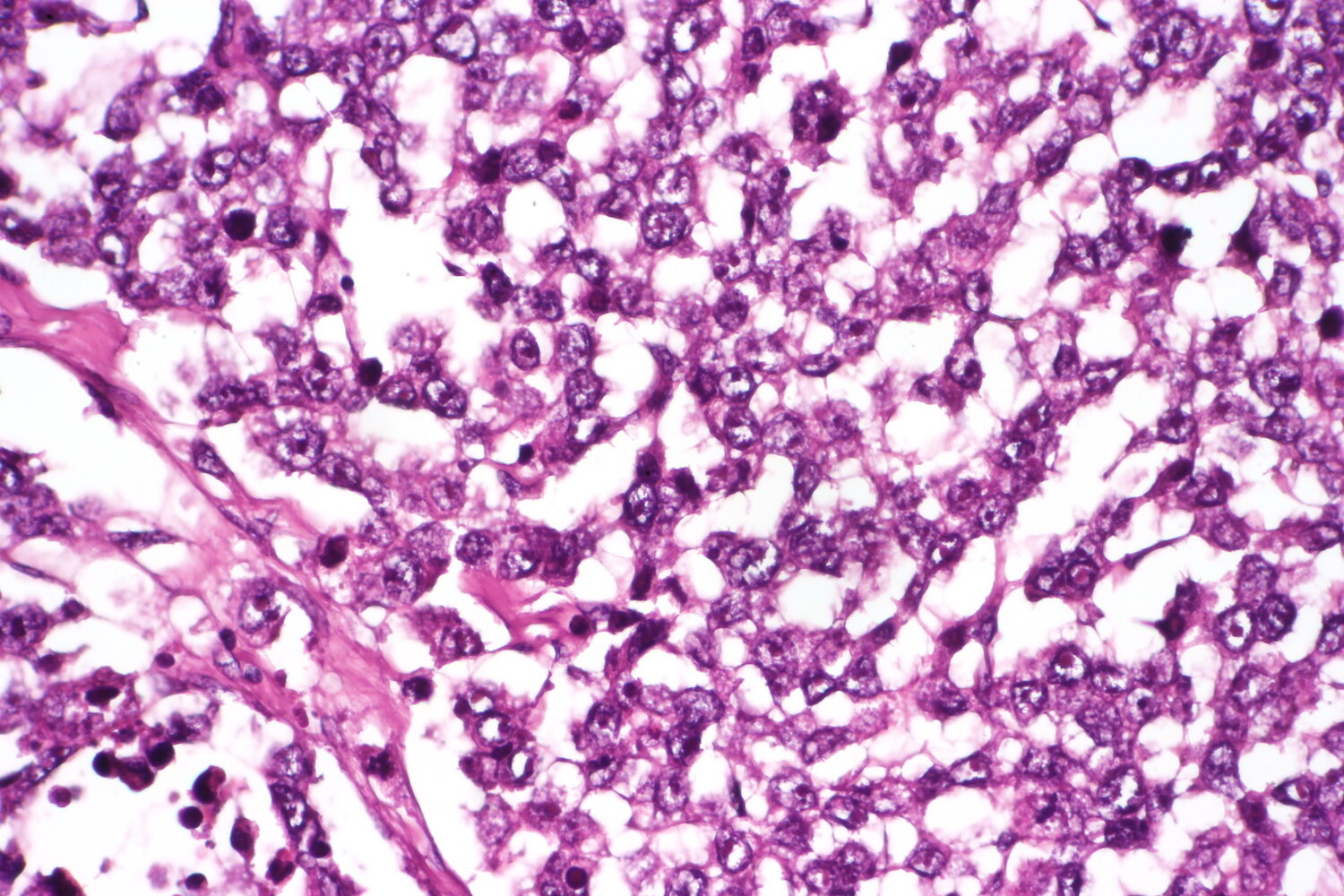
Photomicrograph of a testicular tumor sample (H&E stain; very high magnification)
A central blood vessel (red overlay) is surrounded by tumor cells (blue overlay) with enlarged nuclei and coarse chromatin, resulting in a glomerulus-like appearance (Schiller-Duval body).
Schiller-Duval bodies are a classic finding in yolk sac tumors. The diagnosis was confirmed by immunohistochemical findings (positive for α-fetoprotein and glypican 3).
Source: “Yolk sac tumor schiller duval body” by Jensflorian, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
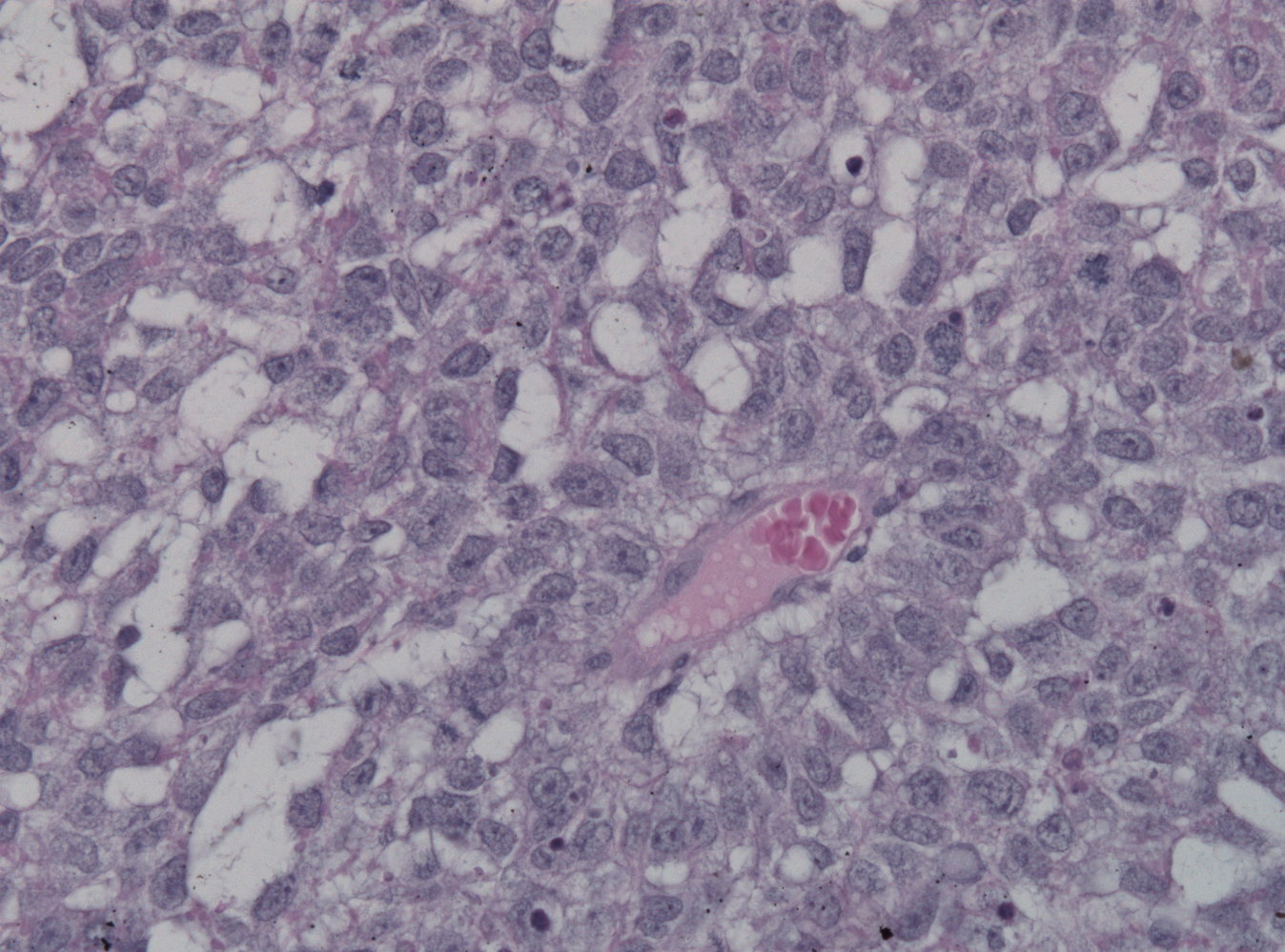
Photomicrograph of an ovary tissue specimen (H&E stain; high magnification)
Sheets of uniform cells with a fried-egg appearance (large nucleus and clear cytoplasm) are visible throughout (examples indicated by green overlay). These sheets of cells are separated by fibrous septa with lymphocytic infiltration.
These findings are consistent with dysgerminoma.
Source: “Dysgerminoma, very high mag.2” by CoRus13, Wikimedia Commons, licensed under CC0 1.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
Sex cord-stromal tumors of the ovary
- Frequency: < 5% of all ovarian tumors [25]
| Types of sex cord-stromal tumors of the ovary | |||||
|---|---|---|---|---|---|
| Type | Ovarian fibroma [26] | Theca cell tumor (thecoma) [27] | Sertoli-Leydig cell tumor [28][29][30][31] | Granulosa cell tumor [28][32][33] | |
| Classification |
|
|
|
||
| Epidemiology |
|
|
|
||
| Clinical features |
|
|
|
|
|
| Ultrasound appearance |
|
|
|
|
|
| Pathology | Gross examination |
|
|
|
|
| Histology |
|
|
|
|
|
| Tumor markers |
|
|
|||
Call-Exner bodies are characteristic of Granulosa cell tumors: “Call your Ex and Grandparents!”

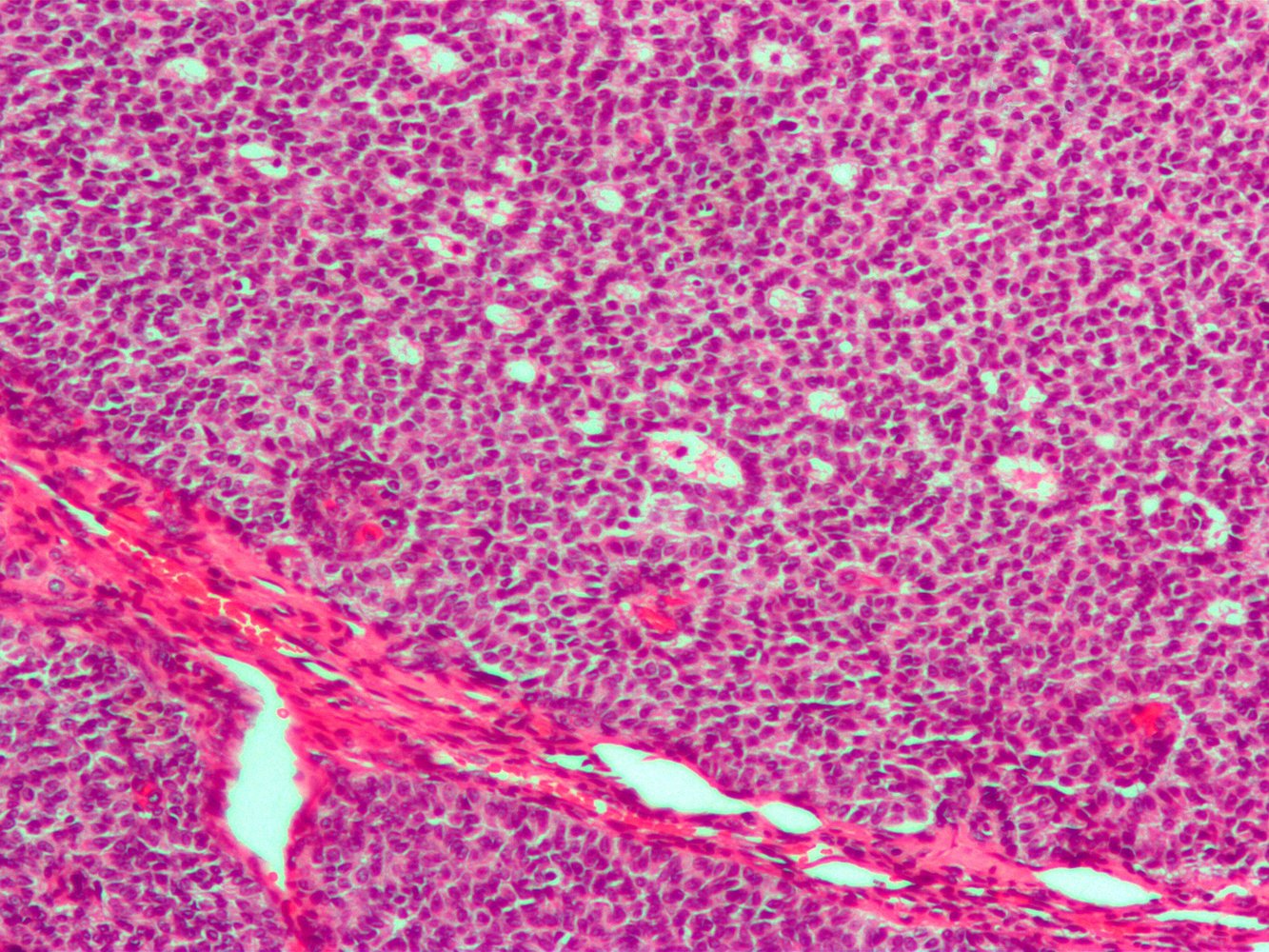
Photomicrograph of an ovary tissue sample (H&E stain; low magnification)
Granulosa cells (blue overlay) are arranged in clusters around multiple central cavities (Call-Exner bodies, yellow overlay). The characteristic grooved, “coffee-bean” appearance can be seen in some nuclei.
This is the typical histological appearance of granulosa cell tumors, although the absence of Call-Exner bodies in such tumors is not uncommon and does not rule out the diagnosis.
Source: “Granulosa cell tumour2” by Nephron, WIkimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
References
- "Ovarian Cancer Including Fallopian Tube Cancer and Primary Peritoneal Carcinoma Version 1.2020". https://www.nccn.org/professionals/physician_gls/pdf/ovarian.pdf. [2020-03-11]
- Meinhold-Heerlein I, Fotopoulou C, Harter P, et al. "The new WHO classification of ovarian, fallopian tube, and primary peritoneal cancer and its clinical implications.". Arch Gynecol Obstet. 293(4). :695-700. (2016)
- Torre LA, Trabert B, DeSantis CE, et al. "Ovarian cancer statistics, 2018". CA Cancer J Clin. 68(4). :284-296. (2018)
- Kurman RJ, Shih IeM. "The Dualistic Model of Ovarian Carcinogenesis: Revisited, Revised, and Expanded.". Am J Pathol. 186(4). :733-47. (2016)
- Dierickx I, Valentin L, Van Holsbeke C, et al. "Imaging in gynecological disease (7): clinical and ultrasound features of Brenner tumors of the ovary". Ultrasound in Obstetrics & Gynecology. 40(6). :706-713. (2012)
- Moro F, Magoga G, Pasciuto T, et al. "Imaging in gynecological disease (13): clinical and ultrasound characteristics of endometrioid ovarian cancer". Ultrasound in Obstetrics & Gynecology. 52(4). :535-543. (2018)
- Pozzati F, Moro F, Pasciuto T, et al. "Imaging in gynecological disease (14): clinical and ultrasound characteristics of ovarian clear cell carcinoma". Ultrasound in Obstetrics & Gynecology. 52(6). :792-800. (2018)
- Babaier A, Ghatage P. "Mucinous Cancer of the Ovary: Overview and Current Status". Diagnostics. 10(1). :52. (2020)
- Wentzensen N, Poole EM, Trabert B, et al. "Ovarian Cancer Risk Factors by Histologic Subtype: An Analysis From the Ovarian Cancer Cohort Consortium". J Clin Oncol. 34(24). :2888-2898. (2016)
- Smith JW, Kemeny N, Caldwell C, et al. "Pseudomyxoma peritonei of appendiceal origin. The memorial sloan-kettering cancer center experience". Cancer. 70(2). :396-401. (1992)
- Anfelter P, Testa A, Chiappa V, et al. "Imaging in gynecological disease (17): ultrasound features of malignant ovarian yolk sac tumors (endodermal sinus tumors)". Ultrasound in Obstetrics & Gynecology. 56(2). :276-284. (2020)
- Guerriero S, Testa AC, Timmerman D, et al. "Imaging of gynecological disease (6): clinical and ultrasound characteristics of ovarian dysgerminoma". Ultrasound in Obstetrics & Gynecology. 37(5). :596-602. (2011)
- Mascilini F, Moro F, Di Grazia FM, et al. "Clinical and ultrasound features of non‐gestational ovarian choriocarcinoma". Ultrasound in Obstetrics & Gynecology. 52(1). :121-123. (2017)
- Weinberger V, Kadlecova J, Minář L, et al. "Struma ovarii – ultrasound features of a rare tumor mimicking ovarian cancer". Medical Ultrasonography. 20(3). :355. (2018)
- Abdullahi Idle S, Hayes K, Ross J. "Ultrasound features of immature ovarian teratomas: Case series and review of literature". Ultrasound. 28(2). :82-90. (2020)
- Comerci JT Jr, Licciardi F, Bergh PA, Gregori C, Breen JL. "Mature cystic teratoma: a clinicopathologic evaluation of 517 cases and review of the literature.". Obstet Gynecol. 84(1). :22-8. (1994)
- M.Roth L, Talerman A. "The enigma of struma ovarii". Pathology. 39(1). :139-146. (2007)
- Smith HO, Berwick M, Verschraegen CF, et al. "Incidence and Survival Rates for Female Malignant Germ Cell Tumors". Obstet Gynecol. 107(5). :1075-1085. (2006)
- Kurman RJ, Norris HJ. "Endodermal sinus tumor of the ovary.A clinical and pathologic analysis of 71 cases". Cancer. 38(6). :2404-2419. (1976)
- Kawai M, Kano T, Kikkawa F, et al. "Seven tumor markers in benign and malignant germ cell tumors of the ovary". Gynecol Oncol. 45(3). :248-253. (1992)
- Levato F, Martinello R, Campobasso C, Porto S. "LDH and LDH isoenzymes in ovarian dysgerminoma.". Eur J Gynaecol Oncol. 16(3). :212-5. (1995)
- Ihara T, Ohama K, Satoh H, et al. "Histologic grade and karyotype of immature teratoma of the ovary". Cancer. 54(12). :2988-2994. (1984)
- Gershenson DM, Del Junco G, Herson J, Rutledge FN. "Endodermal sinus tumor of the ovary: the M. D. Anderson experience.". Obstet Gynecol. 61(2). :194-202. (1983)
- Park J-Y, Kim D-Y, Kim J-H, et al. "Malignant transformation of mature cystic teratoma of the ovary: Experience at a single institution". Eur J Obstet Gynecol Reprod Biol. 141(2). :173-178. (2008)
- Quirk JT, Natarajan N. "Ovarian cancer incidence in the United States, 1992–1999". Gynecol Oncol. 97(2). :519-523. (2005)
- Paladini D, Testa A, Van Holsbeke C, et al. "Imaging in gynecological disease (5): clinical and ultrasound characteristics in fibroma and fibrothecoma of the ovary". Ultrasound in Obstetrics and Gynecology. 34(2). :188-195. (2009)
- "Ovarian thecoma". https://radiopaedia.org/articles/ovarian-thecoma
- Lim D, Oliva E. "Ovarian sex cord-stromal tumours: an update in recent molecular advances". Pathology. 50(2). :178-189. (2018)
- Zanotti KM. "The clinical manifestations and diagnosis of Sertoli-Leydig cell tumors of the ovary.". CME Journal of Gynecologic Oncology. 7. :129-133. (2002)
- Young RH, Scully RE. "Ovarian Sertoli - Leydig cell tumors". Am J Surg Pathol. 9(8). :543-569. (1985)
- Demidov VN, Lipatenkova J, Vikhareva O, et al. "Imaging of gynecological disease (2): clinical and ultrasound characteristics of Sertoli cell tumors, Sertoli–Leydig cell tumors and Leydig cell tumors". Ultrasound in Obstetrics and Gynecology. 31(1). :85-91. (2007)
- Young RH. "Sex cord-stromal tumors of the ovary and testis: their similarities and differences with consideration of selected problems". Mod Pathol. 18(S2). :S81-S98. (2005)
- Van Holsbeke C, Domali E, Holland TK, et al. "Imaging of gynecological disease (3): clinical and ultrasound characteristics of granulosa cell tumors of the ovary". Ultrasound in Obstetrics and Gynecology. 31(4). :450-456. (2008)
- Tanaka YO, Tsunoda H, Kitagawa Y, et al. "Functioning Ovarian Tumors: Direct and Indirect Findings at MR Imaging". RadioGraphics. 24(suppl_1). :S147-S166. (2004)
- Brun J-L. "Demons syndrome revisited: A review of the literature". Gynecol Oncol. 105(3). :796-800. (2007)