Summary
Overweight and obesity are characterized by an accumulation of excess body fat (adiposity) associated with the risk of developing weight-related complications. Multiple underlying factors (e.g., genetics, hormonal changes, lifestyle behaviors, medical conditions, medication use) ultimately result in prolonged excess energy intake relative to energy expenditure. Body mass index (BMI) and waist circumference are used to diagnose and classify overweight and obesity and to estimate the risk of weight-related complications. Clinical evaluation and diagnostic studies are used to assess for contributing causes of overweight and obesity and weight-related complications (e.g., hypertension, cardiovascular disease, dyslipidemia, diabetes), and a clinical severity assessment of obesity should be performed. Management focuses on weight loss and preventing or improving weight-related complications and should be individualized based on shared decision-making. Management options include lifestyle changes (dietary changes, increased physical activity, and/or behavioral interventions), pharmacotherapy, and bariatric surgery. Interventions are often performed concurrently.
Epidemiology
- Sex: ♀ > ♂
-
Prevalence (adults)
- Overweight: ∼ 30% [1]
- Obesity (all classes): ∼ 40% [1][2]
- Class 3 obesity: ∼ 9% [1][2]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Overweight and obesity are caused by prolonged excess energy intake relative to energy expenditure. Contributing factors include: [3][4][5]
-
Genetic and epigenetic predisposition
- Genes that regulate appetite and satiety, genetic syndromes [4]
- Maternal obesity during pregnancy [4]
-
Excessive caloric intake
- High-calorie foods and unhealthy eating habits
- Dysregulated eating: emotional eating, eating disorders (e.g., binge-eating disorder) [5]
- Low caloric expenditure: sedentary lifestyle, excessive screen use, physical inactivity [4]
- Socioeconomic factors: food insecurity, social determinants of health
- Hormonal conditions: hypothyroidism, hypercortisolism
- Medications: corticosteroids, antipsychotics, anticonvulsants, antidepressants, antihyperglycemics [5][6]
Chronic sleep deprivation can lead to obesity through multiple mechanisms (e.g., increased caloric intake, sedentary lifestyle, and hormonal imbalance). [4][5]
Classification
Body mass index [7][8][9][10]
Lower cutoffs for BMI are used in individuals of Asian descent. [7][8][9][11]
| BMI classification for overweight and obesity [7][8][9][10] | ||||||
|---|---|---|---|---|---|---|
| Adults (absolute BMI) | Children aged 2–17 years (BMI percentile for age and sex) [4][12] | |||||
| Overweight |
|
|
||||
| Class 1 obesity |
|
|
||||
| Class 2 obesity |
|
|
||||
| Class 3 obesity |
|
|
||||
There is a direct relationship between increasing BMI and increasing risk of ASCVD, type 2 diabetes (T2DM), and all-cause mortality. [15]
To determine class 2 or class 3 obesity in children, use the adult BMI cutoff if it is lower than the pediatric BMI percentile for age and sex cutoff. [4]
")
")
")
")
")
Clinical severity
In patients with confirmed obesity, use a clinical severity classification system for obesity for risk stratification.
American Association of Clinical Endocrinology [10]
- Stage 1 obesity: no weight-related complications
- Stage 2 obesity: ≥ 1 weight-related complication of mild to moderate severity
- Stage 3 obesity: ≥ 1 severe weight-related complication
The severity of each weight-related complication should be determined on an individual basis and based on clinical judgement. [10]
Lancet Diabetes and Endocrinology Commission [16]
- Preclinical obesity: excess adiposity without the features of clinical obesity
-
Clinical obesity diagnostic criteria
- Organ or tissue dysfunction due to obesity
- AND/OR substantial limitation of ADLs due to obesity
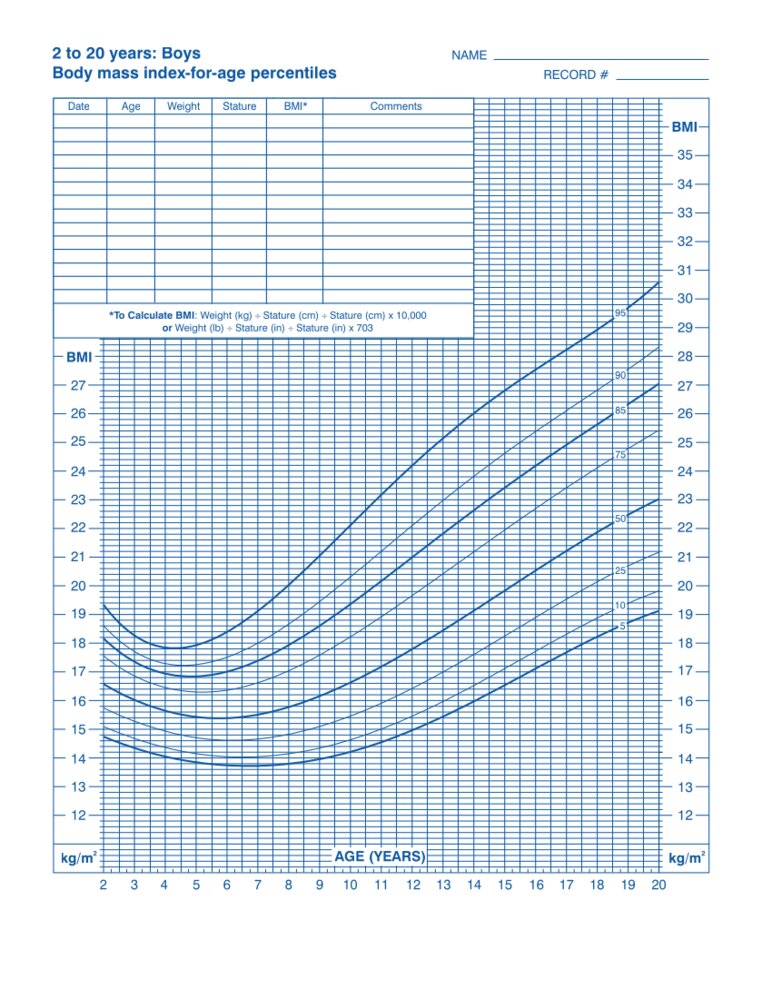
This image is an adaptation. Source of original image: CDC. Original title: “2 to 20 years: Boys; Body mass index-for-age percentiles”. Created by: Centers for Disease Control and Prevention, National Center for Health Statistics. Licensed under Public Domain. Modifications to original image: CDC logo removed by request.
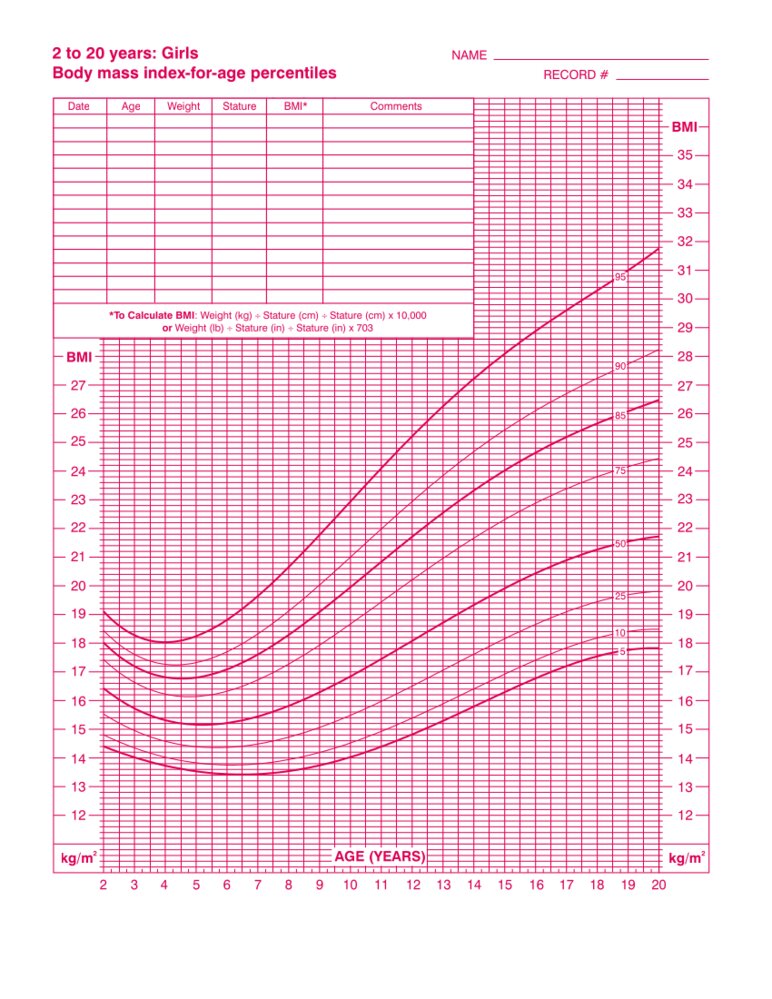
This image is an adaptation. Source of original image: CDC. Original title: “2 to 20 years: Girls; Body mass index-for-age percentiles”. Created by: Centers for Disease Control and Prevention, National Center for Health Statistics. Licensed under Public Domain. Modifications to original image: CDC logo removed by request.
This image is an adaptation. Source of original image: Centers for Disease Control and Prevention, Atlanta. Original title: “Boys: Ages 2–20 Years Body Mass Index-for-age Percentiles Printable Chart”. Created by: National Center for Health Statistics in collaboration with National Center for Chronic Disease Prevention and Health Promotion. Licensed under Public Domain. Modifications to original image: CDC logo removed upon request.
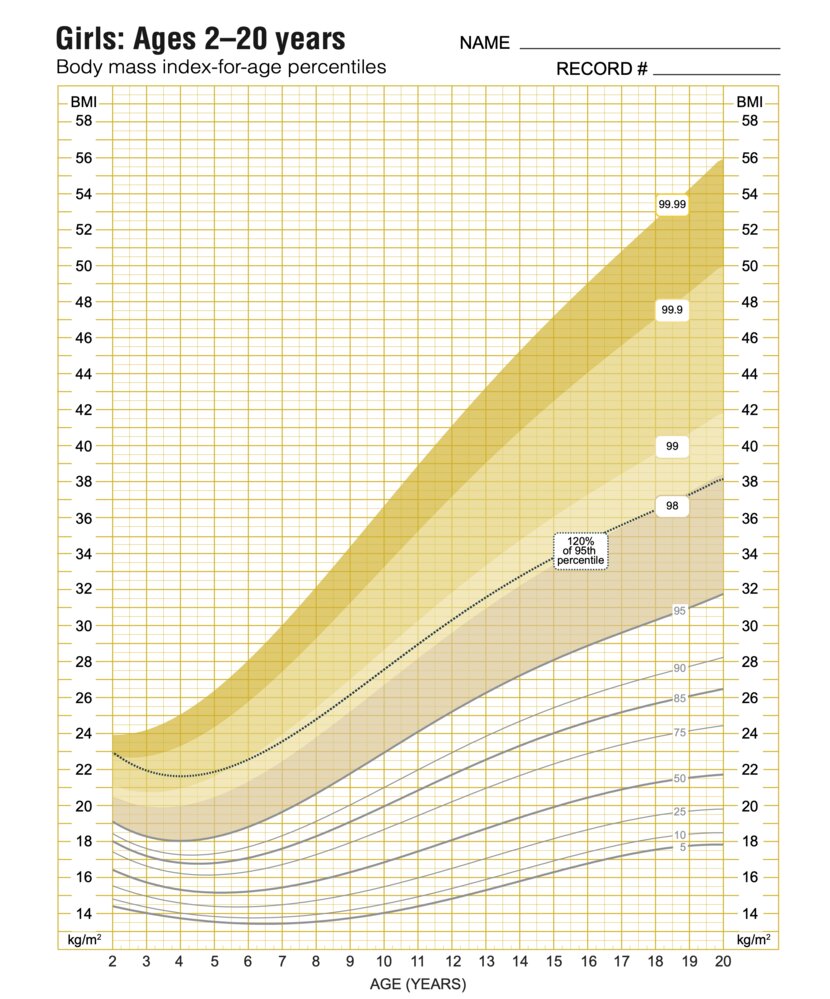
This image is an adaptation. Source of original image: Centers for Disease Control and Prevention, Atlanta. Original title: “Girls: Ages 2–20 Years Body Mass Index-for-age Percentiles Printable Chart”. Created by: National Center for Health Statistics in collaboration with National Center for Chronic Disease Prevention and Health Promotion. Licensed under Public Domain. Modifications to original image: CDC logo removed upon request.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Clinical features
-
Characteristic findings [10]
- Increased BMI
- Increased waist circumference
-
Associated features [16]
- Fatigue and poor exercise tolerance
- Body pains
- Reduced functional mobility (may negatively impact activities of daily living)
- Clinical features of weight-related complications
Diagnosis
Overweight and obesity in children and overweight and obesity in pregnancy (including preconception care) are addressed separately.
Approach [3][10][15][17]
- Address any acute problems and obtain the patient's permission before discussing weight. [18][19][20]
- Assess BMI classification for overweight and obesity, typically at routine health maintenance visits.
- BMI ≤ 40 kg/m2: Perform an anthropometric assessment to confirm that elevated BMI represents excess adiposity. [10][16]
- Perform a clinical evaluation and studies for weight-related complications to assess for:
- Causes of excess adiposity
- Weight-related complications, including metabolic syndrome
- Perform additional studies in select patients as indicated.
- Determine the clinical severity of obesity.
In individuals with BMI > 40 kg/m2, excess adiposity can be reasonably assumed without anthropometric measurements. [16]
Screening for metabolic syndrome is performed as part of the routine initial evaluation in patients with obesity. [10]
Anthropometric assessment [10][15][16][21]
The anthropometric assessment for overweight and obesity includes the following:
- Measurements of abdominal obesity [15][21]
- Waist circumference
- Waist-to-height ratio
- Assessment for increased or decreased muscle mass and edema
- If physical examination is inconclusive, consider imaging (e.g., DEXA, MRI) to better assess body composition.
Clinical evaluation [3][10][22]
The clinical evaluation for overweight and obesity includes a history, review of symptoms, and physical examination.
History
- Weight-related history: weight trends, prior attempts at weight loss
- Personal or family history of weight-related complications
- Medications associated with weight gain
- Dietary habits and level of physical activity
- Social determinants of health that may be barriers to a healthy diet and/or physical activity [18]
- Experience of weight-related bias and stigma [18]
Review of symptoms
- Sleep: insufficient sleep time, poor quality of sleep, clinical features of obstructive sleep apnea
- Symptoms of asthma
- Symptoms of hypothyroidism
- Joint or back pain
- Clinical features of GERD
- Psychological conditions: symptoms of depression, anxiety disorders, clinical features of eating disorders
- Female patients: abnormal vaginal bleeding, infertility, urinary incontinence
- Male patients: decreased libido, erectile dysfunction
Physical examination
- Vital signs: to assess for bradycardia, tachycardia, elevated blood pressure
- Thyroid examination: to assess for goiter or nodules
- Skin examination: to assess for acanthosis nigricans , hirsutism, skin striae, intertrigo, signs of chronic venous insufficiency, acrochordons
- Female patients: clinical features of PCOS
- Male patients: clinical features of male hypogonadism
Use an appropriately sized blood pressure cuff; extended cuffs may be necessary. [13]

")
Studies for weight-related complications [3][10][16][22]
Routine studies
- AST and ALT, and platelets
- Fasting plasma glucose and hemoglobin A1C (see “Diagnostics for diabetes” for interpretation of results) [10][22][23][24]
- Lipid panel
- Serum creatinine (to calculate estimated GFR)
- May consider obtaining:
- CBC [10]
- CMP
- Urinalysis and urine albumin-to-creatinine ratio
- ECG
Further studies
- Obtain studies to evaluate for weight-related complications based on clinical suspicion, e.g.:
- Diagnostics for hypothyroidism
- Diagnostics for obstructive sleep apnea
- Diagnostics for GERD
- Diagnostics for PCOS
- Diagnostics for amenorrhea
- Diagnostics for male hypogonadism
- Diagnostics for MASLD [3][4]
- History of obesity < 5 years of age and/or early hyperphagia: genetic testing for monogenic disorders or syndromic obesity[10]

The back of the neck of an individual with obesity
Dark, velvety, thickened patches are present.
These findings are consistent with acanthosis nigricans (also called pseudoacanthosis nigricans when associated with obesity).
Source: © IMPP

Multiple dark-colored pedunculated papules are visible.
Source: “Molluscum pendulum- acrochordon - cervical” by Grook Da Oger, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
Management
Overweight and obesity in children and overweight and obesity in pregnancy (including preconception care) are addressed separately.
Approach [3][10][13][15][16]
- Provide collaborative patient-centered care. [18][19][20]
- Address any acute problems and obtain the patient's permission before discussing weight.
- Focus on specific health outcomes rather than BMI and weight alone.
- Individualize management using shared decision-making.
-
Address modifiable risk factors, including:
- Modifiable risk factors for cardiovascular disease
- Underlying conditions or medications associated with weight gain [6]
- Set weight-loss goals.
- Overweight without weight-related complications: maintain or lose weight (based on patient preference)
- All other patients: Long-term weight loss of ≥ 5–15% is recommended. [10][13]
- Initiate appropriate interventions.
- All patients: Recommend lifestyle modifications and refer to multidisciplinary specialists as needed.
- Indications for weight-loss medications: Offer pharmacotherapy in addition to lifestyle modifications; use shared decision-making to determine treatment. [15][25][13][16][10]
- Indications for bariatric surgery: Recommend a bariatric surgery evaluation.
- Provide ongoing management.
- Assess progress toward weight-loss goals and modify therapy as needed.
- Periodically assess other medications for possible dose reduction. [13][15]
- After long-term weight-loss goal is achieved: Recommend a weight maintenance program for ≥ 1 year. [13][25]
A trial of lifestyle modifications alone is not required before initiating pharmacotherapy in patients with indications for weight-loss medications. [10][13][16]
Loss of ≥ 5% of body weight is considered clinically significant (i.e., decreases the risk or mitigates the effects of some weight-related complications). [10][13][25]
Medications associated with weight changes
| Medications associated with weight changes [3][5] | |||
|---|---|---|---|
| Promote weight gain | Mild or no effect on weight gain | May promote weight loss | |
| Antihyperglycemic agents |
|
|
|
| Antihypertensives |
|
|
|
| Antidepressants |
|
|
|
| Antipsychotics and mood stabilizers |
|
|
|
| Anticonvulsants |
|
|
|
| Contraceptives |
|
|
|
| Anti-inflammatory agents |
|
|
|
Lifestyle interventions
General principles [3][6][15]
- Lifestyle interventions can lead to weight loss, increase insulin sensitivity, and reduce cardiovascular risk factors.
- To support the implementation of dietary and physical activity changes:
- Refer to a multicomponent behavioral intervention program.
- Address barriers related to social determinants of health (e.g., food insecurity). [18]
- Lifestyle modifications without pharmacotherapy
- Advise patients on weight-loss goals.
- Initial goal: ≥ 2.5% weight loss at 1 month [26]
- Long-term goal: 5–10% weight loss at 6 months [13][15]
- Base frequency of follow-up on patient need (e.g, every 4–6 weeks initially). [19]
- Advise patients on weight-loss goals.
Dietary changes [6][10][17]
- Provide general counseling on nutrition.
- Various dietary approaches that result in a caloric deficit may be effective for weight loss.
- Refer to a dietitian for specific caloric and energy deficit recommendations. [6][15]
- Recommend sufficient protein intake during weight loss to prevent muscle loss.
- Most patients: ≥ 1.2 g/kg/day
- Patients with CKD: See "Protein and energy consumption in CKD."
Physical activity [6][10][27][28]
-
Provide counseling on regular exercise.
- No specific form of physical activity is recommended over another for weight loss.
- Encourage gradually increasing quantity and/or intensity of activity as tolerated to meet recommendations and weight-loss goals. [27][28]
- Encourage an increase in nonsedentary activities.
- Additional guidance: exercise coach or physical therapy referral
Behavioral interventions [6][10][17][25]
- Offer referral for to a multicomponent behavioral intervention program, if available.
- Interventions may include:
- Goal setting
- Self-monitoring of weight
- Identification of weight-gain triggers
- Development of self-management skills
- Stress reduction and healthy coping skills
- Support groups and psychological counseling (e.g., cognitive behavioral therapy, intensive behavioral therapy)
- Counseling on sleep hygiene
Pharmacotherapy
General principles [5][10][13][25][29]
- Offer pharmacotherapy in conjunction with lifestyle modifications to patients with indications for weight-loss medications.
- BMI ≥ 30 kg/m2
- BMI ≥ 27 kg/m2 and at least one weight-related complication
- Choose a medication based on:
- Indications and contraindications
- Patient preference (including cost considerations)
- Weight-loss goals [10][13]
- Follow-up
- Frequency: monthly for 3–6 months, and then less frequently [6][13][15]
- Titrate medications gradually to improve tolerance.
- Monitor for adverse effects (e.g., cholelithiasis and mood disorders).
- Assess progress toward weight-loss goals, and adjust treatment as needed.
- After 3 months on maximum tolerated dose: If weight loss is < 5%, change to an alternative medication.[10][25]
- Long-term: If not meeting individualized goals, consider changing to an alternative medication and/or referral to an obesity specialist.
- Long-term use of medications is typically required for sustained weight loss.
Medications
| Pharmacotherapy for weight loss [10][13][25][29] | |||
|---|---|---|---|
| Drug class | Examples | Indications | Considerations |
| Nutrient-stimulated hormone-based medications |
|
|
|
| Centrally acting medications |
|
|
|
| Lipase inhibitors |
|
|
|
Due to the teratogenicity risk, advise patients who can become pregnant to use contraception while taking pharmacotherapy for obesity. [6][25][32]
Tirzepatide has the highest efficacy in terms of total weight loss compared to other weight-loss drugs.[13]
Orlistat reversibly inhibits gastric and pancreatic lipase, resulting in a decrease in fat breakdown and absorption, and can cause gastrointestinal side effects.
Metabolic and bariatric surgery
-
Indications for bariatric surgery [33]
- Class 2 obesity or class 3 obesity
-
Class 1 obesity with either of the following:
- T2DM
- Lack of improvement following nonsurgical interventions
- Average weight loss with bariatric surgery: > 20% [6][13]
- See “Bariatric surgery” for additional information.
Complications
-
Cardiometabolic [34]
- Hypertension, cardiovascular disease (ASCVD)
- Atrial fibrillation
- Cardiomyopathy and congestive heart failure [35][36]
- Insulin resistance: prediabetes, T2DM
- Dyslipidemia
- PCOS
- MASLD, MASH: increased risk of liver cirrhosis and liver malignancy
-
Respiratory
- Obstructive sleep apnea (OSA)
- Obesity hypoventilation syndrome
- Asthma [26]
-
Musculoskeletal
- Osteoarthritis
- Chronic back pain [37]
- Slipped capital femoral epiphysis and Blount disease (especially in children) [4]
-
Reproductive and genitourinary [38]
- Chronic kidney disease [35]
- Menstrual dysfunction and/or ovulatory dysfunction
- Adverse events during pregnancy: e.g., gestational hypertension, preterm labor, and pregnancy loss (see “Overweight and obesity in pregnancy”) [39]
- Urinary incontinence
- Infertility [13]
- Erectile dysfunction [40]
- Male hypogonadism
-
Gastrointestinal [41]
- Cholelithiasis, cholecystitis
- GERD
- Colonic diverticulosis
-
Malignancies [42][43]
- Hepatocellular carcinoma
- Colorectal cancer
- Breast cancer
- Endometrial cancer
- Renal cancer [44]
-
CNS
- Idiopathic intracranial hypertension
- Dementia
-
Psychological [18]
- Anxiety
- Depression
- Internalized weight bias and/or stigma
- Eating disorders
-
Other
- Disability causing limitation of activities of daily living
- Inflammatory skin diseases, intertrigo
- Lymphedema
- Thromboembolism, including portal vein thrombosis [45][46]
- Gout [47]
The co-occurence of central obesity, T2DM or prediabetes, hypertension, and dyslipidemia is known as metabolic syndrome. [48]
We list the most important complications. The selection is not exhaustive.
Prevention
- All patients
- Provide counseling on nutrition and counseling on regular exercise at each routine wellness visit.
- Recommend avoidance of weight gain to prevent weight-related complications.
- Patients with overweight or normal weight with a history of overweight or obesity
- Recommend self-monitoring of weight.
- Recommend lifestyle interventions for overweight and obesity if weight is trending up.
- See also “Primary prevention strategies for adult health.”
Special patient groups
Overweight and obesity in children [4]
- Children with overweight or obesity are at increased risk of obesity and weight-related complications as adults.
- Prevalence of obesity in individuals 12–19 years of age: ∼ 20% [49]
Diagnostics
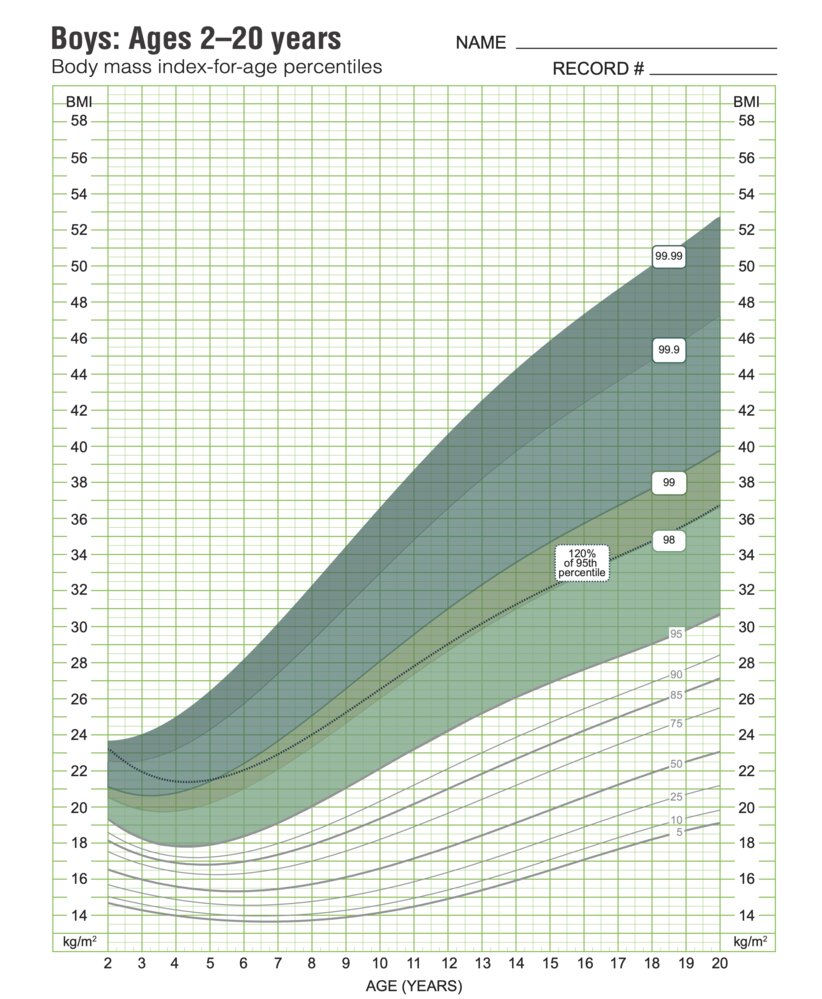
- Assess BMI at all well-child visits in children ≥ 2 years of age; extended growth charts are available.
- Perform a clinical evaluation for overweight and obesity, including a musculoskeletal examination.
- Routine laboratory testing: at baseline and, if normal, may repeat every 2 years or sooner based on risk [50]
- 2–9 years of age with obesity: Consider a fasting lipid panel (see “Pediatric dyslipidemia screening”).
-
≥ 10 years of age
- All: fasting lipid panel
- Overweight with risk factors for T2DM: hyperglycemia testing
- Overweight with risk factors for MASLD: ALT
- Obesity: hyperglycemia testing and ALT
- Additional testing [50][51]
- Decreased linear growth: Obtain endocrine evaluation.
- Either of the following: Refer for genetic testing.
- Class 2 obesity or higher at ≤ 5 years of age with hyperphagia and/or a family history of class 2 obesity or higher
- Developmental delay or other syndromic features
Suspect genetic causes of obesity in children with class 2 obesity or higher at ≤ 5 years of age with hyperphagia and/or other syndromic features. [4][50]
Management [4][52][53]
-
Lifestyle interventions
- Initiate or refer to intensive health behavior and lifestyle treatment starting at 6 years of age. [4][53]
- Provide counseling on nutrition; no specific diet is recommended. [54]
- Provide counseling on regular exercise.
- Provide counseling on sleep hygiene.
- Use motivational interviewing to promote behavioral change.
-
Pharmacotherapy: Weight-loss drugs are typically managed by a specialist.
- 8–11 years of age: Pharmacotherapy may be considered off-label.
-
FDA-approved for long-term use in children ≥ 12 years of age with obesity
- GLP-1 agonists: liraglutide, semaglutide [4]
- Orlistat
- Phentermine/topiramate extended release
-
FDA-approved for short-term use in children > 16 years of age
- With overweight and weight-related complications or with obesity: phentermine
- With obesity and no improvement with lifestyle interventions: diethylpropion
- Bariatric surgery: Refer all patients ≥ 13 years of age with class 2 obesity and higher to a surgical center for evaluation. [33][55]
Overweight and obesity in pregnancy [32]
Preconception
- Recommend waiting to attempt conception until:
- 12–24 months after bariatric surgery [38]
- ≥ 2 months after discontinuation of GLP-1 agonists [56]
-
Preconception counseling should include:
- Discussion of obesity-related complications in pregnancy [38]
- Recommendation for weight loss before conception [32]
- See “Preconception care” for additional information.
Pregnancy
- At the initial prenatal visit, perform prenatal screening for comorbidities, e.g.:
- Diabetes screening for overweight with risk factors for T2DM or obesity
- Screening for OSA
- Studies for weight-related complications (if not already obtained)
- Assess for other risk factors for VTE; see “Prevention of DVT in pregnancy and postpartum.” [57]
- For post-bariatric surgery patients, consider: [58]
- Studies for micronutrient deficiencies (e.g., thiamine, folate, vitamin B12) early in pregnancy
- Alternative hyperglycemia tests if a malabsorptive procedure was performed
- A multivitamin in addition to a prenatal vitamin (limit daily vitamin A intake to 5000 IU)
- Early dietitian referral
-
Weight management
- Encourage lower recommended weight gain during pregnancy.
- Overweight: 15–25.0 lb (6.8–11.3 kg)
- Obesity: 11–20 lb (5–9.1 kg)
- Pharmacotherapy and bariatric surgery are contraindicated.
- Encourage lower recommended weight gain during pregnancy.
- Counsel patients with obesity that prenatal ultrasound has decreased sensitivity in detecting fetal abnormalities.
- Consider earlier antepartum fetal surveillance based on prepregnancy BMI classification. [59]
- Class 2 obesity: weekly starting at 34 0/7 weeks' gestation
- Class 3 obesity: weekly starting at 37 0/7 weeks' gestation
- See “Prenatal care” for additional information.
Obesity-related complications during pregnancy include maternal complications (e.g., pregnancy loss, gestational diabetes, preeclampsia, cesarean delivery, postpartum hemorrhage) and fetal complications (e.g., neural tube defects, hydrocephalus, anatomic abnormalities). [32]
Delivery and postpartum [32]
- Individualize the decision for vaginal or cesarean delivery, and for induction of labor.
- Consult anesthesiology prior to labor or in early labor.
- For patients with obesity who undergo cesarean delivery, consider postpartum DVT prophylaxis with LMWH in addition to routine pneumatic compression devices. [57]
- See “Postpartum care” for additional information.
Pharmacotherapy for obesity is contraindicated during pregnancy and breastfeeding due to the risk of adverse effects in the fetus or infant. [25]
This image is an adaptation. Source of original image: Centers for Disease Control and Prevention, Atlanta. Original title: “Boys: Ages 2–20 Years Body Mass Index-for-age Percentiles Printable Chart”. Created by: National Center for Health Statistics in collaboration with National Center for Chronic Disease Prevention and Health Promotion. Licensed under Public Domain. Modifications to original image: CDC logo removed upon request.
Related One-Minute Telegram
- One-Minute Telegram 132-2025-2/3: Peer coaching for weight loss in US veterans
- One-Minute Telegram 121-2025-3/3: The weight is over: study shows intermittent fasting beats daily caloric restriction for weight loss
- One-Minute Telegram 111-2024-1/3: Timing meals to trim body weight
- One-Minute Telegram 109-2024-2/3: A weight off your shoulders: tirzepatide’s dual impact on sleep apnea and weight
- One-Minute Telegram 103-2024-1/3: Bariatric surgery yields greater weight loss and lower mortality than GLP-1RAs in individuals with obesity and diabetes
- One-Minute Telegram 88-2023-1/3: Semaglutide in the absence of diabetes: slimming the risk of CVD
- One-Minute Telegram 57-2022-2/3: Intermittent fasting effective for weight loss
- One-Minute Telegram 50-2022-3/3: A new drug combination to treat obesity in adolescents
- One-Minute Telegram 15-2020-2/4: What is the risk factor in COVID-19, obesity or its comorbidities?
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- 2025 AACE Consensus Statement: Algorithm for the Evaluation and Treatment of Adults with Obesity/Adiposity-Based Chronic Disease
- 2025 ACC Expert Consensus Statement on Medical Weight Management for Optimization of Cardiovascular Health
- 2025 ADA Standards of Care in Diabetes: Obesity and Weight Management for the Prevention and Treatment of Type 2 Diabetes
- 2025 USPSTF Recommendation Statement: Interventions for High Body Mass Index in Children and Adolescents
- 2023 AAP Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents With Obesity
- 2022 AGA Clinical Practice Guideline on Pharmacological Interventions for Adults With Obesity
- 2022 ASMBS/IFSO Statement: Indications for Metabolic and Bariatric Surgery
- 2021 ACOG Practice Bulletin No. 230 (reaffirmed 2025): Obesity in Pregnancy
- 2018 USPSTF Recommendation Statement: Weight Loss to Prevent Obesity-Related Morbidity and Mortality in Adults
- 2015 Endocrine Society Guideline for the Pharmacological Management of Obesity
- 2013 AHA/ACC/TOS Guideline for the Management of Overweight and Obesity in Adults
- One-Minute Telegram
References
- Curry SJ, Krist AH, et al. "Behavioral Weight Loss Interventions to Prevent Obesity-Related Morbidity and Mortality in Adults". JAMA. 320(11). :1163. (2018)
- Jensen MD, Ryan DH, Apovian CM, et al. "2013 AHA/ACC/TOS Guideline for the Management of Overweight and Obesity in Adults". Circulation. 129(25 suppl 2). :S102-S138. (2013)
- Keating MK, Woodruff RK, Saner EM. "Management of Obesity: Office-Based Strategies". Am Fam Physician. 110(2). :145-156. (2024)
- Nadolsky K, Garvey W, Agarwal M, et al. "American Association of Clinical Endocrinology Consensus Statement: Algorithm for the Evaluation and Treatment of Adults with Obesity/Adiposity-Based Chronic Disease – 2025 Update". Endocr Pract. 31(11). :1351-1394. (2025)
- Nadolsky K, Addison B, Agarwal M, et al. "American Association of Clinical Endocrinology Consensus Statement: Addressing Stigma and Bias in the Diagnosis and Management of Patients with Obesity/Adiposity-Based Chronic Disease and Assessing Bias and Stigmatization as Determinants of Disease Severity". Endocr Pract.. 29(6). :417-427. (2023)
- Elmaleh-Sachs A, Schwartz JL, Bramante CT, et al. "Obesity Management in Adults". JAMA. 330(20). :2000. (2023)
- Yanovski SZ, Yanovski JA. "Approach to Obesity Treatment in Primary Care". JAMA Intern Med. 184(7). :818. (2024)
- Rubino F, Cummings DE, Eckel RH, et al. "Definition and diagnostic criteria of clinical obesity". Lancet Diabetes Endocrinol. 13(3). :221-262. (2025)
- NHLBI Obesity Task Force. "Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults-The Evidence Report". Obes Res. 6 Suppl 2. :51S-209S. (1998)
- Burridge K, Christensen SM, Golden A, et al. "Obesity history, physical exam, laboratory, body composition, and energy expenditure: An Obesity Medicine Association (OMA) Clinical Practice Statement (CPS) 2022". Obes Pillars. 1. :100007. (2022)
- Gilbert O, Gulati M, Gluckman TJ, et al. "2025 Concise Clinical Guidance: An ACC Expert Consensus Statement on Medical Weight Management for Optimization of Cardiovascular Health". J Am Coll Cardiol. (2025)
- US Preventive Services Task Force., Davidson KW, Barry MJ, et al. "Screening for Prediabetes and Type 2 Diabetes: US Preventive Services Task Force Recommendation Statement". JAMA. 326(8). :736-743. (2021)
- ElSayed NA, McCoy RG, et al. "2. Diagnosis and Classification of Diabetes: Standards of Care in Diabetes—2025". Diabetes Care. 48(Supplement_1). :S27-S49. (2024)
- Hampl SE, Hassink SG, Skinner AC, et al. "Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents With Obesity". Pediatrics. 151(2). (2023)
- Garvey WT, Mechanick JI, Brett EM, et al. "American Association of Clinical Endocrinologists and American College of Endocrinology Comprehensive Clinical Practice Guidelines for Medical Care of Patients with Obesity". Endocr Pract. 22(Supplement 3). :1-203. (2016)
- Powell-Wiley TM, Poirier P, Burke LE, et al. "Obesity and Cardiovascular Disease: A Scientific Statement From the American Heart Association". Circulation. 143(21). (2021)
- Tune JD, Goodwill AG, Sassoon DJ, Mather KJ. "Cardiovascular consequences of metabolic syndrome". Transl Res. 183. :57-70. (2017)
- Perrone-Filardi P, Paolillo S, Costanzo P, et al. "The role of metabolic syndrome in heart failure". Eur Heart J. 36(39). :2630-2634. (2015)
- Shiri R, Karppinen J, Leino-Arjas P, Solovieva S, Viikari-Juntura E. "The Association Between Obesity and Low Back Pain: A Meta-Analysis". Am J Epidemiol. 171(2). :135-154. (2009)
- Penzias A, Azziz R, Bendikson K, et al. "Obesity and reproduction: a committee opinion". Fertil Steril. 116(5). :1266-1285. (2021)
- Shin D, Song WO. "Prepregnancy body mass index is an independent risk factor for gestational hypertension, gestational diabetes, preterm labor, and small- and large-for-gestational-age infants". J Matern Fetal Neonatal Med. 28(14). :1679-86. (2015)
- Besiroglu H, Otunctemur A, Ozbek E. "The Relationship Between Metabolic Syndrome, Its Components, and Erectile Dysfunction: A Systematic Review and a Meta-Analysis of Observational Studies". J Sex Med. 12(6). :1309-1318. (2015)
- Camilleri M, Malhi H, Acosta A. "Gastrointestinal Complications of Obesity". Gastroenterology. 152(7). :1656-1670. (2017)
- Micucci C, Valli D, Matacchione G, Catalano A. "Current perspectives between metabolic syndrome and cancer". Oncotarget. 7(25). :38959-38972. (2016)
- Gallagher EJ, LeRoith D. "Epidemiology and Molecular Mechanisms Tying Obesity, Diabetes, and the Metabolic Syndrome With Cancer". Diabetes Care. 36(Supplement_2). :S233-S239. (2013)
- Kim LH, Doan P, He Y, et al. "A Systematic Review and Meta-Analysis of the Significance of Body Mass Index on Kidney Cancer Outcomes". J Urol. 205(2). :346-355. (2021)
- Blokhin IO, Lentz SR. "Mechanisms of thrombosis in obesity". Curr Opin Hematol. 20(5). :437-444. (2015)
- Bureau C, Laurent J, Robic MA, et al. "Central obesity is associated with non-cirrhotic portal vein thrombosis". J Hepatol. 64(2). :427-432. (2016)
- Qaseem A, Harris RP, Forciea MA. "Management of Acute and Recurrent Gout: A Clinical Practice Guideline From the American College of Physicians". Ann Intern Med. 166(1). :58. (2016)
- Grundy SM, Cleeman JI, Daniels SR, et al. "Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement". Circulation. 112(17). :2735-2752. (2005)
- "Prevalence of Overweight, Obesity, and Severe Obesity Among Adults Aged 20 and Over: United States, 1960–1962 Through 2017–2018". https://web.archive.org/web/20250409154524/https://www.cdc.gov/nchs/data/hestat/obesity-adult-17-18/obesity-adult.htm. [2021-02-08]
- "Obesity and Severe Obesity Prevalence in Adults: United States, August 2021–August 2023"
- Stierman B, Afful J, Carroll MD, et al. "National Health and Nutrition Examination Survey 2017-March 2020 Prepandemic Data Files-Development of Files and Prevalence Estimates for Selected Health Outcomes.". Natl Health Stat Report. (2021)
- Cuda SE, Censani M. "Assessment, differential diagnosis, and initial clinical evaluation of the pediatric patient with obesity: An Obesity Medical Association (OMA) Clinical Practice Statement 2022". Obes Pillars. 1. :100010. (2022)
- Styne DM, Arslanian SA, Connor EL, et al. "Pediatric Obesity—Assessment, Treatment, and Prevention: An Endocrine Society Clinical Practice Guideline". J Clin Endocrinol Metab. 102(3). :709-757. (2017)
- Moore TH, Phillips SM, Heslehurst N, et al. "Interventions to prevent obesity in children under 2 years old". Cochrane Database Syst Rev. 2024(9). (2022)
- Nicholson WK, Silverstein M, et al. "Interventions for High Body Mass Index in Children and Adolescents". JAMA. 332(3). :226. (2024)
- National Heart, Lung, and Blood Institute. "Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents: Summary Report". Pediatrics. 128(Supplement). :S213-S256. (2011)
- Pratt JSA, Browne A, Browne NT, et al. "ASMBS pediatric metabolic and bariatric surgery guidelines, 2018". Surg Obes Relat Dis. 14(7). :882-901. (2018)
- Eisenberg D, Shikora SA, Aarts E, et al. "2022 American Society of Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO) Indications for Metabolic and Bariatric Surgery". Obes Surg. 33(1). :3-14. (2022)
- American College of Obstetricians and Gynecologists. "Obesity in Pregnancy Practice Bulletin Number 230". Obstet Gynecol.. 137(6). :e128-e144. (2021)
- Minis E, Stanford FC, Mahalingaiah S. "Glucagon-like peptide-1 receptor agonists and safety in the preconception period". Curr Opin Endocrinol Diabetes Obes. 30(6). :273-279. (2023)
- ACOG. "ACOG Practice Bulletin No. 196: Thromboembolism in Pregnancy". Obstetrics & Gynecology. 132(1). :e1-e17. (2018)
- ACOG. "ACOG Practice Bulletin No. 105: Bariatric Surgery and Pregnancy (reaffirmed 2025)". Obstetrics & Gynecology. 113(6). :1405-1413. (2009)
- ACOG. "Indications for Outpatient Antenatal Fetal Surveillance (reaffirmed 2024)". Obstetrics & Gynecology. 137(6). :e177-e197. (2021)
- Grunvald E, Shah R, Hernaez R, et al. "AGA Clinical Practice Guideline on Pharmacological Interventions for Adults With Obesity". Gastroenterology. 163(5). :1198-1225. (2022)
- Cornier M-A, Després J-P, Davis N, et al. "Assessing Adiposity: A Scientific Statement From the American Heart Association". Circulation. 124(18). :1996-2019. (2011)
- "The Asia-Pacific Perspective: Redefining Obesity and its Treatment". https://web.archive.org/web/20250409151530/https://iris.who.int/bitstream/handle/10665/206936/0957708211_eng.pdf. [2000-02-01]
- Li Z, Daniel S, Fujioka K, Umashanker D. "Obesity among Asian American people in the United States: A review". Obesity. 31(2). :316-328. (2023)
- WHO. "Obesity: preventing and managing the global epidemic. Report of a WHO consultation.". World Health Organ Tech Rep Ser. 894. :i-xii, 1-253. (2000)
- "Growth Chart Training : Using the WHO Growth Charts Case Example 4: Transitioning from the WHO Weight-for-Length Chart to the CDC BMI-for-Age Chart at Age 2 Years". https://web.archive.org/web/20230207180111/https://www.cdc.gov/nccdphp/dnpao/growthcharts/who/examples/example4.htm. [2022-01-13]
- Kwan TW, Wong SS, Hong Y, et al. "Epidemiology of Diabetes and Atherosclerotic Cardiovascular Disease Among Asian American Adults: Implications, Management, and Future Directions: A Scientific Statement From the American Heart Association". Circulation. 148(1). :74-94. (2023)
- ElSayed NA, McCoy RG, et al. "8. Obesity and Weight Management for the Prevention and Treatment of Type 2 Diabetes: Standards of Care in Diabetes–2025". Diabetes Care. 48(Supplement_1). :S167-S180. (2024)
- Apovian CM, Aronne LJ, Bessesen DH, et al. "Pharmacological Management of Obesity: An Endocrine Society Clinical Practice Guideline". J Clin Endocrinol Metab. 100(2). :342-362. (2015)
- Jakicic JM, Apovian CM, Barr-Anderson DJ, et al. "Physical Activity and Excess Body Weight and Adiposity for Adults. American College of Sports Medicine Consensus Statement". Med Sci Sports Exerc. 56(10). :2076-2091. (2024)
- "Physical activity guidelines for Americans 2nd edition 2018". https://web.archive.org/web/20250517061526/https://odphp.health.gov/sites/default/files/2019-09/Physical_Activity_Guidelines_2nd_edition.pdf. [2018-01-01]
- Gudzune KA, Kushner RF. "Medications for Obesity". JAMA. 332(7). :571. (2024)
- Kittleson MM, Benjamin EJ, Blumer V, et al. "2025 ACC Scientific Statement on the Management of Obesity in Adults With Heart Failure". J Am Coll Cardiol. (2025)
- Kushner RF, Almandoz JP, Rubino DM. "Managing Adverse Effects of Incretin-Based Medications for Obesity". JAMA. (2025)