Summary
Pancreatic and hepatic surgeries are indicated in the management of malignant/symptomatic benign tumors and traumatic lacerations of the liver and pancreas. The choice of surgery depends on the location, size, and extent of the malignancy/injury. Depending on the extent of resection, pancreatic surgeries for malignancy include enucleation (for islet cell tumors), partial pancreatic resections (distal pancreatectomy, central pancreatectomy, pancreaticoduodenectomy/Whipple procedure), and total pancreatectomy. Chronic pancreatitis patients with a dilated main pancreatic duct (> 5 mm), not responding to conservative therapy, are candidates for lateral pancreaticojejunostomy with/without resection of the pancreatic head. Complications of pancreatic surgeries include anastomotic leaks, pancreatic ascites/fistula, and exocrine/endocrine insufficiency. Depending on which segments of the liver are removed, hepatic resections include right/left hepatectomy, right/left lobectomy, and segmentectomy. Wedge resections of the liver are performed for small, peripherally located lesions. Other complications of hepatic resections include liver failure, hemorrhage, hemobilia, and bile leaks.
Pancreatic surgery
Anatomy of the pancreas
- See “Pancreas.”
Types of pancreatic surgeries
| Overview of pancreatic surgery types [1][2] | |||
|---|---|---|---|
| Type | Indications | Surgical procedure | |
| Pancreatic resections | Pancreaticoduodenectomy (Whipple procedure) |
|
|
| Pylorus-preserving pancreaticoduodenectomy (modified Whipple procedure) |
|
|
|
| Distal pancreatectomy (with/without splenectomy) |
|
|
|
| Central pancreatectomy [5] |
|
|
|
| Total pancreatectomy [6] |
|
|
|
| Enucleation [7] |
|
|
|
| For acute pancreatitis | Debridement of pancreatic parenchyma (Pancreatic necrosectomy) [8] |
|
|
| For chronic pancreatitis | Duodenum-preserving pancreatic head resection (Beger procedure) [9] |
|
|
| Lateral pancreaticojejunostomy + resection of the pancreatic head (Frey procedure) |
|
|
|
| Lateral pancreaticojejunostomy (Puestow procedure) |
|
|
|
| For pancreatic pseudocysts | Pseudocyst-gastrostomy (cystogastrostomy) Pseudocyst-duodenostomy (cystoduodenostomy) Pseudocyst-jejunostomy (cystojejunostomy) |
|
|
| For pancreatic fistulae | Fistulojejunostomy Pancreatic resection (e.g., distal pancreatectomy for distal duct disruption) [3] |
|
|

")
Complications
- Delayed gastric emptying/gastroparesis (most common) [13][14]
-
Pancreaticojejunostomy anastomotic leak/pancreatic ductal disruption → leakage of pancreatic secretions into the abdominal cavity which leads to:
- Hyperchloremic acidosis
- Pancreatic fistula
- Pancreatic pseudocyst
- Pancreatic ascites
- Hepaticojejunostomy anastomotic leak → biliary peritonitis
- Exocrine pancreatic insufficiency [14]
- Endocrine pancreatic insufficiency (diabetes mellitus) and lifelong dependence on insulin
- Small bowel obstruction: herniation, volvulus, anastomotic stricture
- Intraabdominal abscess or sepsis
- Gastrointestinal hemorrhage
- If the duodenum is resected: iron deficiency anemia
Suspect a pancreaticojejunostomy anastomotic leak in a patient with hyperchloremic acidosis (loss of bicarbonate) and high levels of amylase in abdominal secretions.
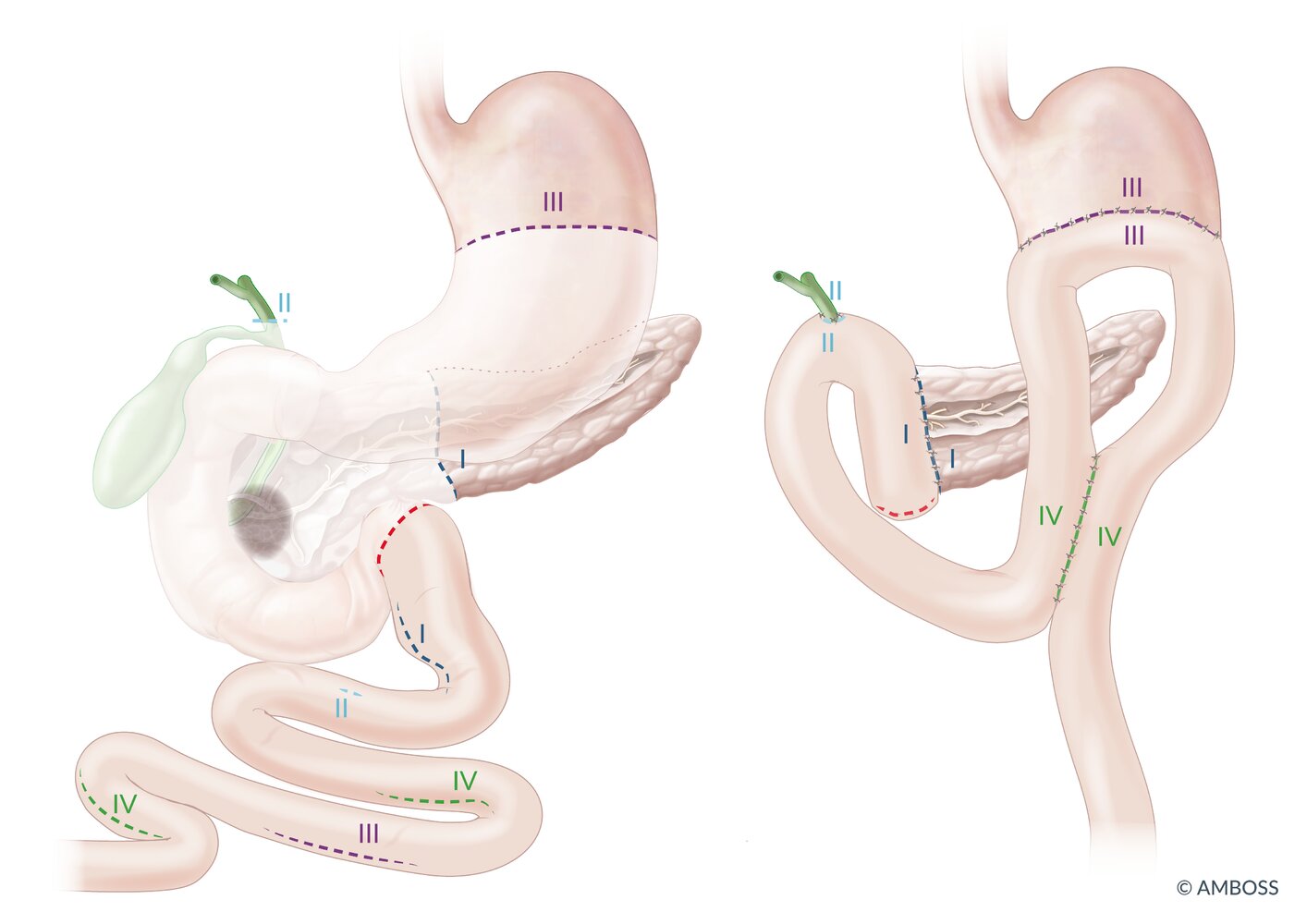
(1) Preoperative situation: The grey mass represents a tumor in the pancreatic head. The structures depicted as transparent are resected.
- Distal stomach (antrum and pylorus)
- Entire duodenum
- ∼ 15 cm of the proximal jejunum
- The pancreatic head with the distal pancreatic duct
- The gall bladder and the CBD
(2) Post-operative situation: Four anastomoses are created.
- Pancreaticojejunostomy (I)
- Hepaticojejunostomy (II; common hepatic duct is sutured to the jejunum)
- Gastrojejunostomy (III)
- Enteroenterostomy (IV; between the afferent and efferent jejunal loop)
The blind proximal end of the jejunum is closed (red line).
© AMBOSS
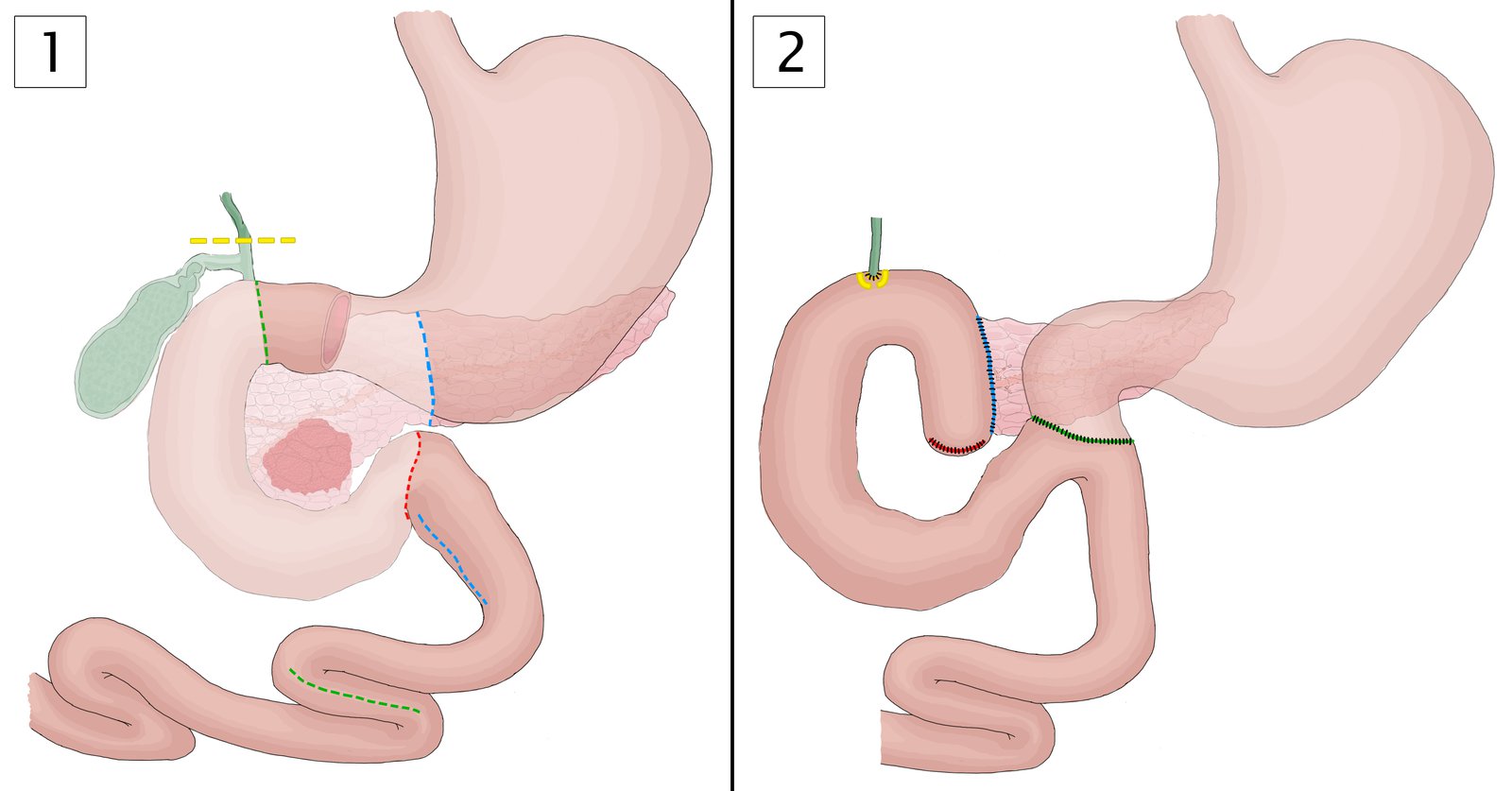
The Transverso-Longmire procedure is a modification of the Whipple procedure that preserves the gastric antrum, the pylorus, and a small part of the duodenum to provide a more physiologic stomach emptying.
Image 1 outlines the preoperative situation and allows for a direct comparison with the postoperative situation in image 2. Organs to be resected are shown in lighter colors (1).
Green to red line:
- Partial duodenectomy preserving the proximal duodenum including the pylorus (1)
→ End-to-side duodenojejunostomy and blind ending of proximal jejunum (2)
Blue line:
- Resection of pancreatic head (1)
→ End-to-side pancreaticojejunostomy (2)
Yellow line:
- Resection of gall bladder and bile duct
→ Hepaticojejunostomy
© AMBOSS
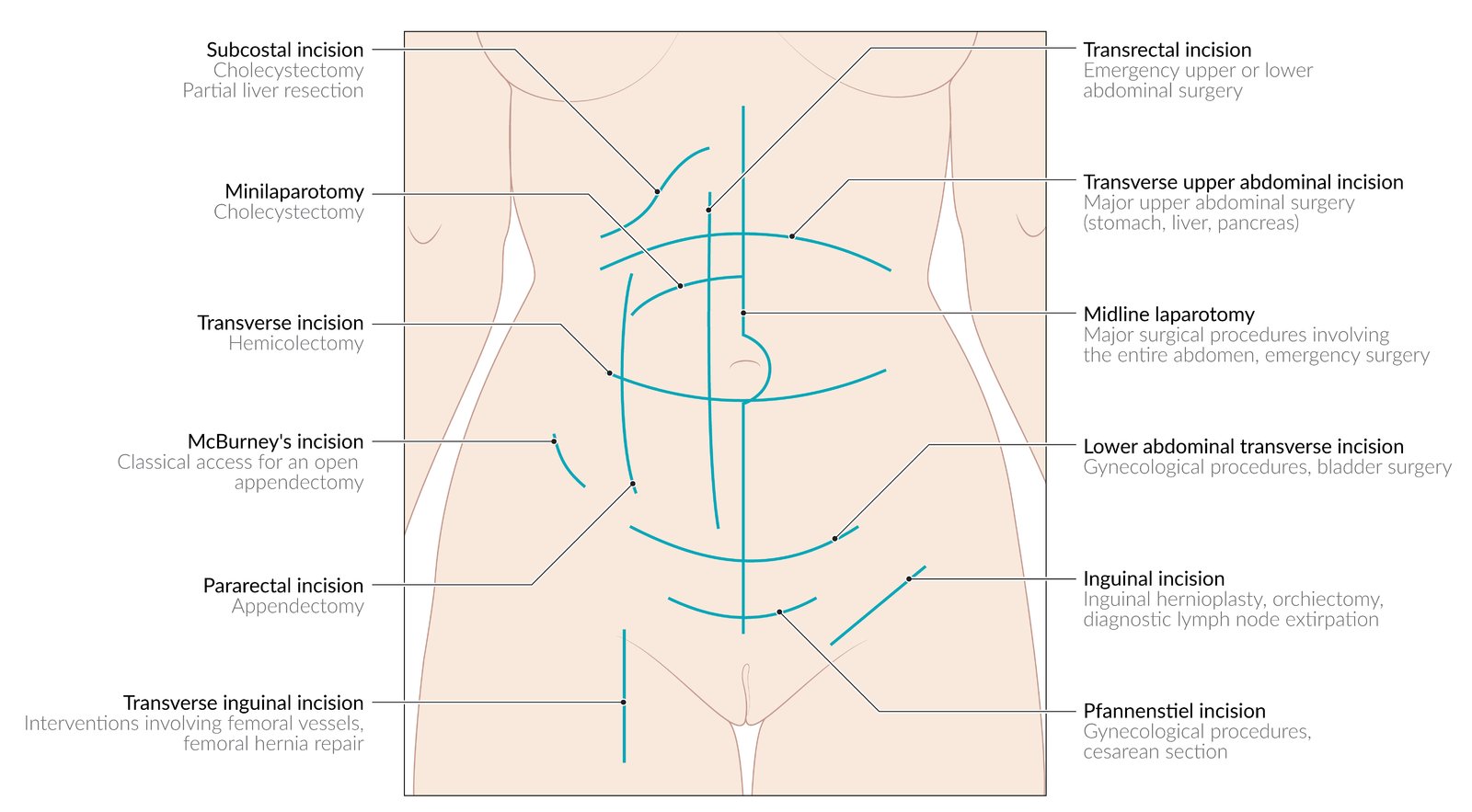
The choice of incision site depends on the indication for and urgency of surgery.
© AMBOSS
Hepatic surgery
Anatomy of the liver
- See “Liver.”
General principles of hepatic surgery
- Access: laparotomy (transverse, midline or subcostal incisions) or laparoscopy
- Pringle maneuver: temporary occlusion of the hepatic artery and portal vein by clamping of the free edge of the lesser omentum (hepatoduodenal ligament) in order to control vascular inflow to the liver or to reduce hemorrhage
- Cholecystectomy is routinely performed as part of all major hepatic resections to allow for easier dissection during the surgery.
- Cavitron ultrasonic surgical aspirator (CUSA): uses ultrasonic waves to vaporize only the liver cells while sparing the biliary radicles and blood vessels

Types of liver resections [15]
| Overview of liver resection types | ||||
|---|---|---|---|---|
| Type | Indications | Contraindications | Surgical procedure | |
| Anatomical resections | Right hepatectomy (right hemihepatectomy) |
|
|
|
| ||||
| Left hepatectomy |
|
|||
| Left lobectomy |
|
|||
| Segmental resection |
|
|||
| Non-anatomical resection | Wedge resection |
|
|
|
Complications
- Hemorrhage
- Hemobilia [18][19]
- Bile leak
- Liver failure
Before performing extensive hepatic resections the future liver remnant (FLR) needs to be calculated (using CT images), as patients with insufficient FLR postresection, can develop liver failure.
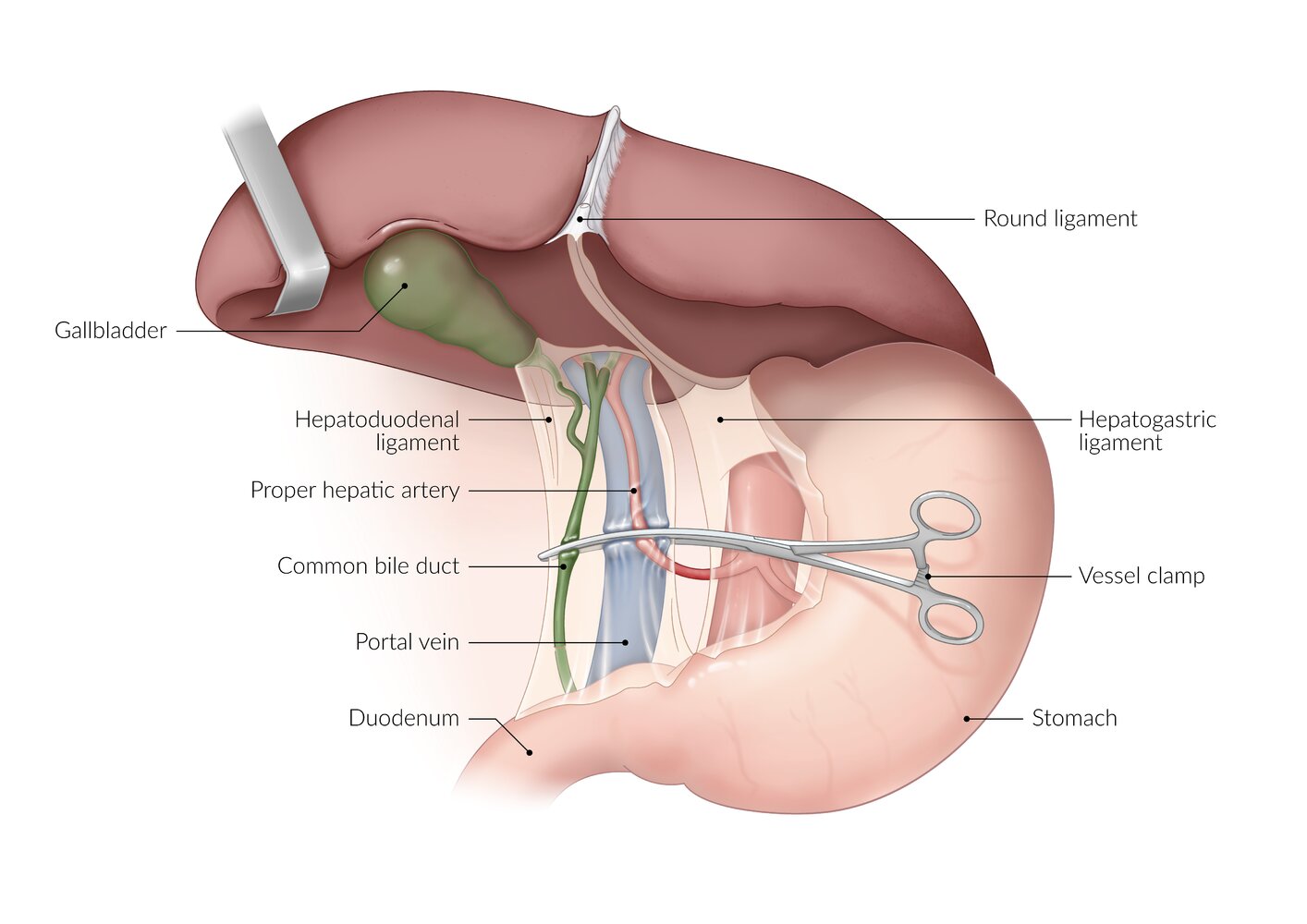
© AMBOSS
Related One-Minute Telegram
- One-Minute Telegram 139-2026-3/3: Small steps for the Whipple: laparoscopic vs. open approach
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- de Virgilio C, Frank PN, Grigorian A. "Surgery: A Case Based Clinical Review". Springer. (2015). ISBN: 9781493917259
- Noorani A, Rangelova E, Del chiaro M, Lundell LR, Ansorge C. "Delayed Gastric Emptying after Pancreatic Surgery: Analysis of Factors Determinant for the Short-term Outcome". Front Surg. 3. :25. (2016)
- Holzheimer RG, Mannick JA, Sayek I, Onat D, Lerut T. "Surgical Treatment: Evidence-Based and Problem-Oriented". W. Zuckschwerdt Verlag GmbH.. (2001). ISBN: 9783886037148
- Bachmann J, Michalski CW, Martignoni ME, Büchler MW, Friess H. "Pancreatic resection for pancreatic cancer". HPB. 8(5). :346-351. (2006)
- Christein JD, Smoot RL, Farnell MB. "Central pancreatectomy: a technique for the resection of pancreatic neck lesions". Arch Surg. 141(3). :293-299. (2006)
- Kulu Y, Schmied BM, Werner J, et al. "Total pancreatectomy for pancreatic cancer: indications and operative technique". HPB. 11(6). :469-475. (2009)
- "Laparoscopic Pancreatic Surgery". http://www.surgery.usc.edu/divisions/tumor/pancreasdiseases/web%20pages/pancreas%20resection/LAP%20PANCREATIC%20SURGERY.html. [2017-04-09]
- "Surgery for Acute Pancreatitis". http://www.surgery.usc.edu/divisions/tumor/pancreasdiseases/web%20pages/PANCREATITIS/surgery-acute%20panc.html. [2017-04-09]
- "Surgery for Chronic Pancreatitis". http://www.surgery.usc.edu/divisions/tumor/pancreasdiseases/web%20pages/PANCREATITIS/surgery-chronic%20pancreatit.html. [2017-04-09]
- Köninger J, Friess H, Müller M, Büchler MW. "Duodenum preserving pancreatic head resection in the treatment of chronic pancreatitis". Rocz Akad Med Bialymst. 49. :53-60. (2004)
- Strobel O, Büchler MW, Werner J. "[Duodenum-preserving pancreatic head resection: technique according to Beger, technique according to Frey and Berne modifications].". Chirurg. 80(1). :22-7. (2009)
- Nair RR, Lowy AM, Mcintyre B, et al. "Fistulojejunostomy for the management of refractory pancreatic fistula". Surgery. 142(4). :636-642. (2007)
- Malleo G, Crippa S, Butturini G, et al. "Delayed gastric emptying after pylorus-preserving pancreaticoduodenectomy: validation of International Study Group of Pancreatic Surgery classification and analysis of risk factors". HPB. 12(9). :610-618. (2010)
- Tejedor L, Serrablo A. "Postoperative Pancreatic Biliary Surgical Complications". J Gastroenterol Hepatol Res. 2(7). :661-671. (2013)
- Aragon RJ, Solomon NL. "Techniques of hepatic resection.". J Gastrointest Oncol. 3(1). :28-40. (2012)
- Letoublon C, Morra I, Chen Y, et al. "Hepatic arterial embolization in the management of blunt hepatic trauma: indications and complications". J Trauma. 70(5). :1032-1036. (2011)
- Ribero D, Chun YS, Vauthey JN. "Standardized liver volumetry for portal vein embolization". Semin Intervent Radiol. 25(2). :104-109. (2008)
- Zaydfudim VM, Angle JF, Adams RB. "Current Management of Hemobilia". Curr Surg Rep. 2. :54. (2014)
- Galun D, Basarić D, Lekić N, et al. "[Hemobilia].". Acta Chir Iugosl. 54(1). :41-5. (2007)