Summary
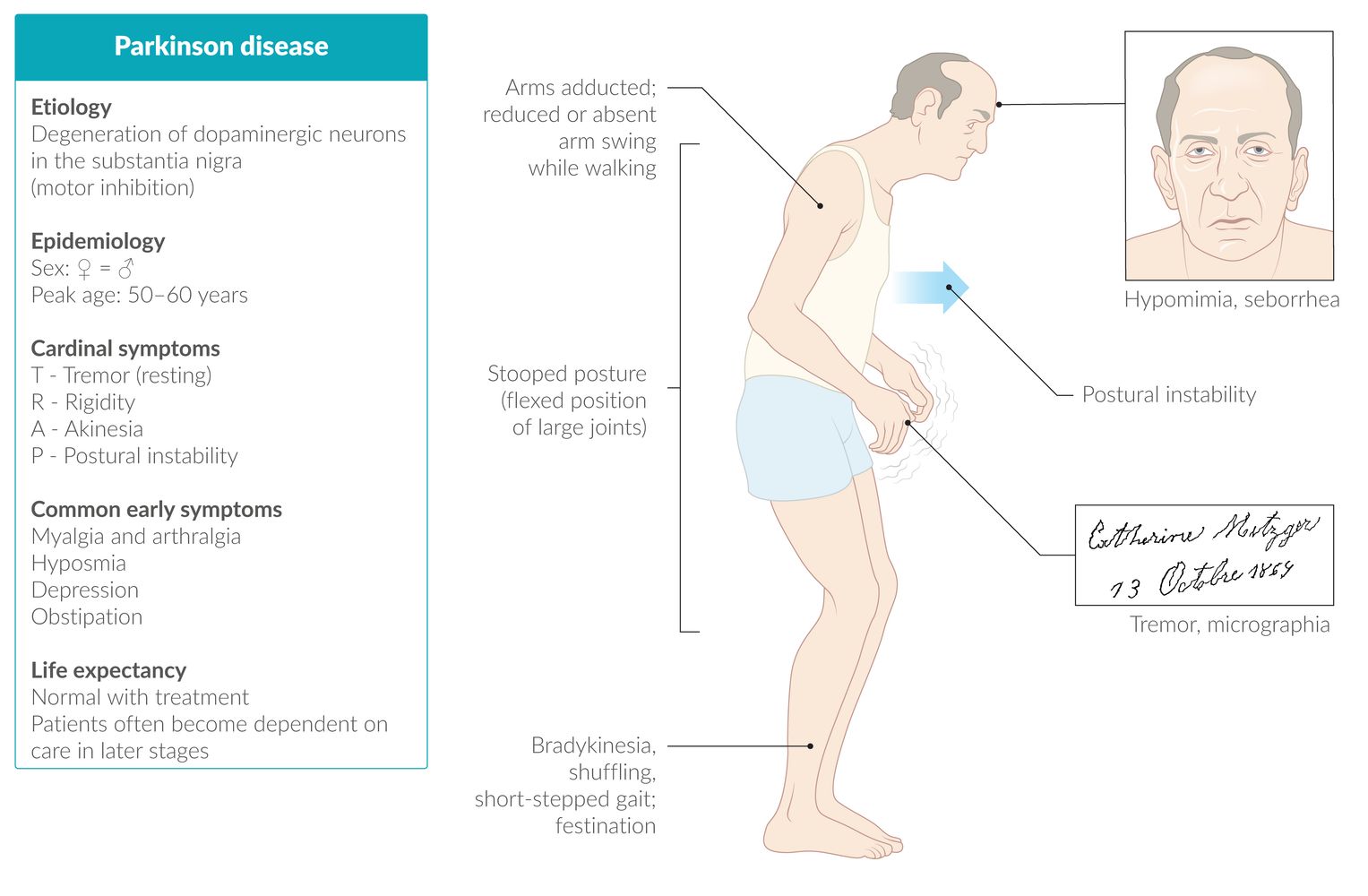
Parkinson disease (PD) is a neurodegenerative condition that involves the progressive depletion of dopaminergic neurons in the basal ganglia, particularly the substantia nigra. The disease most commonly manifests at approx. 60 years of age. PD is predominantly considered an idiopathic disease but genetic factors play a role in approx. 10–15% of cases and, accordingly, familial clustering has been observed. A core clinical feature of PD is parkinsonism, a syndrome that comprises bradykinesia along with resting tremor and/or rigidity. Postural instability is a common finding in later stages of PD. Parkinsonism that results from medication, intoxication, or traumatic brain injury is referred to as secondary parkinsonism. Parkinsonism due to neurodegenerative disorders other than PD is called atypical parkinsonism and manifests with features that are not characteristic of PD, such as vertical gaze palsy in progressive supranuclear palsy and apraxia and agnosia in corticobasal degeneration. The diagnosis is clinical; diagnostic testing may be considered to rule out alternative diagnoses. There is currently no cure for PD. Symptomatic treatment includes physical therapy and, depending on patient factors and individual symptoms, certain medications (e.g., levodopa, dopamine agonists). Deep brain stimulation surgery may be beneficial in specific cases.

© AMBOSS
Epidemiology
- Prevalence: second most common neurodegenerative disorder following Alzheimer disease [1]
- Age of onset: ∼ 60 years in sporadic cases [2]
-
Risk factors
- Genetic factors: 10–15% of all cases are familial. [3]
- Environmental factors (e.g., exposure to manganese and other substances)
- Diet/metabolism (e.g., low levels of vitamin D, high iron intake, obesity)
- History of traumatic brain injury
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Parkinson disease
- Idiopathic
- Contributing genetic factors include:
- α-Synuclein (SNCA)
- Glucocerebrosidase (GBA): A mutation in the GBA gene (the same gene associated with Gaucher disease) is the most common genetic risk factor for PD. GBA mutations are associated with altered autophagy and lysosomal function, potentially resulting in impairment of α-synuclein clearance.
- Dardarin (LRRK2): A mutation in LRRK2 gene is the most common cause of dominantly inherited PD.
- Parkin (PARK2): A mutation in PARK2 gene is the most common cause of recessively inherited PD.
Secondary parkinsonism
-
Medication (drug-induced parkinsonism or pseudoparkinsonism)
- Most frequent cause of secondary parkinsonism [3]
- Frequent use of drugs with considerable antidopaminergic effects: typical antipsychotics (e.g., haloperidol), some antiemetics (e.g., metoclopramide), some calcium channel blockers (e.g., flunarizine), amiodarone, valproate, and lithium [3][4]
- MPTP: an illegal drug that metabolizes to MPP+, damaging the substantia nigra
- Metabolic disorders: e.g., Wilson disease, hemochromatosis, Niemann-Pick disease
- Toxins: e.g., manganese, carbon monoxide, carbon disulfide
- Cerebrovascular disease (vascular parkinsonism): subcortical arteriosclerotic encephalopathy
-
CNS infections
- Viruses: e.g., herpes simplex virus, human immunodeficiency virus
- Bacteria: e.g., Treponema pallidum, Mycobacterium tuberculosis
- Protozoa: e.g., Toxoplasma gondii, Plasmodium spp.
- Prion agents: Creutzfeldt-Jakob disease
- Atypical parkinsonism: depends on the underlying disease (e.g., genetic abnormalities in Huntington disease)
Pathophysiology
- Progressive dopaminergic neuron degeneration in the substantia nigra (part of the basal ganglia) and the locus coeruleus → dopamine deficiency at the respective receptors of the striatum with interrupted transmission to the thalamus and motor cortex → motor symptoms of PD [5]
- Indirect pathway of the basal ganglia is affected (see “Basal ganglia” in “The cerebral cortex, meninges, basal ganglia, and ventricular system”)
- Serotonin and noradrenaline depletion (in the raphe nuclei): likely cause of depressive symptoms
- Acetylcholine surplus (in the nucleus basalis of Meynert): likely cause of dyskinesia
References:[3][5]
Clinical features
Overview
- Signs of PD gradually progress over time: The course is usually > 10 years.
- Motor signs are unilateral at onset but may progress to the contralateral side.
- Motor signs are asymmetrical (i.e., more pronounced on one side than on another).
- Preclinical (prodromal) stage with nonmotor signs may precede the onset of motor signs (clinical phase).
Preclinical stage [6]
- Constipation
- Anosmia
-
Sleep disturbances
- REM sleep behavior disorder (RBD)
- Restless leg syndrome
- Excessive daytime sleepiness
- Mood disorders (most commonly depression, apathy, and/or anxiety)
Clinical stage
Motor signs [7]
-
Parkinsonism: a syndrome comprising bradykinesia and either resting tremor or rigidity (or both) and that is consistent with impairment of the extrapyramidal system
- A core feature of PD
- Can be also seen in a variety of other disorders, e.g., multiple system atrophy, corticobasal degeneration (see “Atypical parkinsonism”)
- Bradykinesia: slowed movements in combination with decreased amplitude/speed when moving
-
Resting tremor (4–6 Hz)
- Oftentimes the presenting symptom
- Pill-rolling tremor that subsides with voluntary movements but increases with stress
- Most common in the hands but may involve the legs, jaw, lips, and tongue
-
Rigidity: increased and persistent resistance to passive joint movement that is independent of speed
- Froment maneuver: patient is asked to perform repetitive movements in the contralateral extremity (e.g., opening and closing of the left fist if the right side is examined) → subclinical rigidity becomes more pronounced and may be detected
-
Cogwheel rigidity
- A phenomenon caused by the overlay of increased muscle tonus and resting tremor in patients with PD
- May manifest before tremor becomes clinically apparent
- Muscles in an extremity (most commonly the arms) are passively stretched, eliciting a jerking-like motion.
- Muscle tone should be tested with at least two joints.
-
Postural instability
- Imbalance and tendency to fall
- Evaluated with the pull test
-
Gait abnormalities
- Parkinsonian gait: shuffling gait with quickened and shortened steps
- Freezing: sudden inability to start or continue movements
- Festination: gait pattern characterized by small, increasingly quick steps
- Propulsion: forward-leaning gait with a risk of a patient falling forward
- Decreased arm swing
-
Other motor findings
- Unhabituated glabellar reflex
- Signs of dystonia
- Stooped posture
- Abnormal flexor posturing of hands and feet (i.e., striatal deformities)
- Micrographia: size of handwriting is reduced
- Hypomimia: low degree of facial expression
Parkinsonism is required for the diagnosis of Parkinson disease. Unilateral onset is characteristic of Parkinson disease.
Parkinsonism TRAPs the patient: Tremor, Rigidity, Akinesia, and Postural instability.
Nonmotor signs
-
Autonomic symptoms
- Orthostatic hypotension
- Oily skin
- Urinary urgency
- Impaired sexual function
- Neuropsychiatric symptoms
- Depression
- Cognitive problems, e.g., decreased attention and concentration, executive dysfunction, impaired memory (Parkinson dementia): develop in advanced disease [5]
- Apathy
- Behavioral changes (e.g., irritability, impulsivity)
- Disordered sleep (sleep fragmentation; , vivid dreams)
- Fatigue
- Hyposmia, anosmia
Diagnosis
Approach [8][9][10]
- Consider PD in patients with parkinsonism.
- Perform a thorough clinical evaluation.
- Consider diagnostic testing to:
- Provide diagnostic certainty if a diagnosis cannot be made based on clinical features alone
- Help rule out alternative diagnoses of parkinsonism
- Refer to a neurologist or movement disorder specialist for diagnostic confirmation.
Parkinson disease is a clinical diagnosis. A definitive diagnosis requires postmortem confirmation of Lewy bodies.
Clinical evaluation [10][11]
- Evaluate for typical clinical features of PD based on:
- Detailed patient history
- Thorough physical examination, including complete neurological examination
- Assess for:
- Supportive features of PD
- Atypical features for PD suggesting other causes of parkinsonism
- A diagnosis can be made by a specialist using diagnostic criteria (see “Tips and Links”).
Supportive features [11]
- A diagnosis of PD requires the presence of parkinsonism (i.e., bradykinesia and either resting tremor, rigidity, or both).
- Supportive features include:
- Clear benefit from dopaminergic medication [12]
- Resting tremor
- Levodopa-induced dyskinesia (typically occurs during later stages of PD)
- Olfactory loss
Atypical features
Consider other causes of parkinsonism if any of the following are present :
-
Features
- Vertical gaze palsy
- Cortical signs
- Cerebellar signs
- Pyramidal tract signs
- Absence of typical nonmotor signs
-
Disease trajectory
- Rapid progression (e.g., early dementia, progressive aphasia, falls, gait impairment, severe autonomic or bulbar dysfunction)
- No progression of typical motor signs
- No benefit from dopaminergic medication
-
Distribution of symptoms
- Bilateral symmetric parkinsonism
- Limited to legs
-
History suggestive of alternative causes
- Use of dopaminergic blockers within 6–12 months
- Traumatic brain injury
- Encephalitis
If patients have atypical features for PD, evaluate for secondary parkinsonism or atypical parkinsonian syndromes.
Diagnostic testing
Imaging [13] [14]
Imaging is not routinely required for diagnosis but can be considered under specialist guidance if the diagnosis is unclear.
- MRI brain: usually no specific changes, nonspecific atrophy of the putamen may be seen in patients with PD
-
DaTSCAN: SPECT with visualization of striatal dopamine transporters using 123I-ioflupane
- Syndromes with nigrostriatal degeneration (e.g., PD, MSA): reduced dopamine transporter activity
- Essential tremor: normal
-
Iodobenzamide single-photon emission computed tomography (IBZM-SPECT): measures D2-receptor density in the striatum [15]
- PD: normal or increased D2-receptor density
- Atypical parkinsonism: decreased D2-receptor density
-
Other modalities (rarely used)
- PET
- Transcranial sonography
Ancillary tests
Ancillary tests are not routinely used but can support the diagnosis.
-
Levodopa challenge test: performed to support the diagnosis of PD or as part of the evaluation prior to implantation of a deep brain stimulator
- Motor symptoms are evaluated before, during, and after administration of oral levodopa and a decarboxylase inhibitor.
- The result is positive if administration of levodopa relieves symptoms.
- Olfactory testing: to test for hyposmia [8][9][16][17]
- MIBG myocardial scintigraphy: to test for cardiac sympathetic denervation
Pathology
-
Lewy bodies
- Aggregates of misfolded α-synuclein and other proteins, such as ubiquitin and neurofilament protein within the neural cell bodies
- Appear histologically as intracellular hyaline eosinophilic globules
- May be found in brainstem, substantia nigra, and cortex [6]
- Also seen in dementia with Lewy bodies
- Loss of dopaminergic neurons in substantia nigra pars compacta, causing depigmentation of substantia nigra on gross and microscopic examination
- Reactive gliosis is found within the areas of neural degeneration. [5]


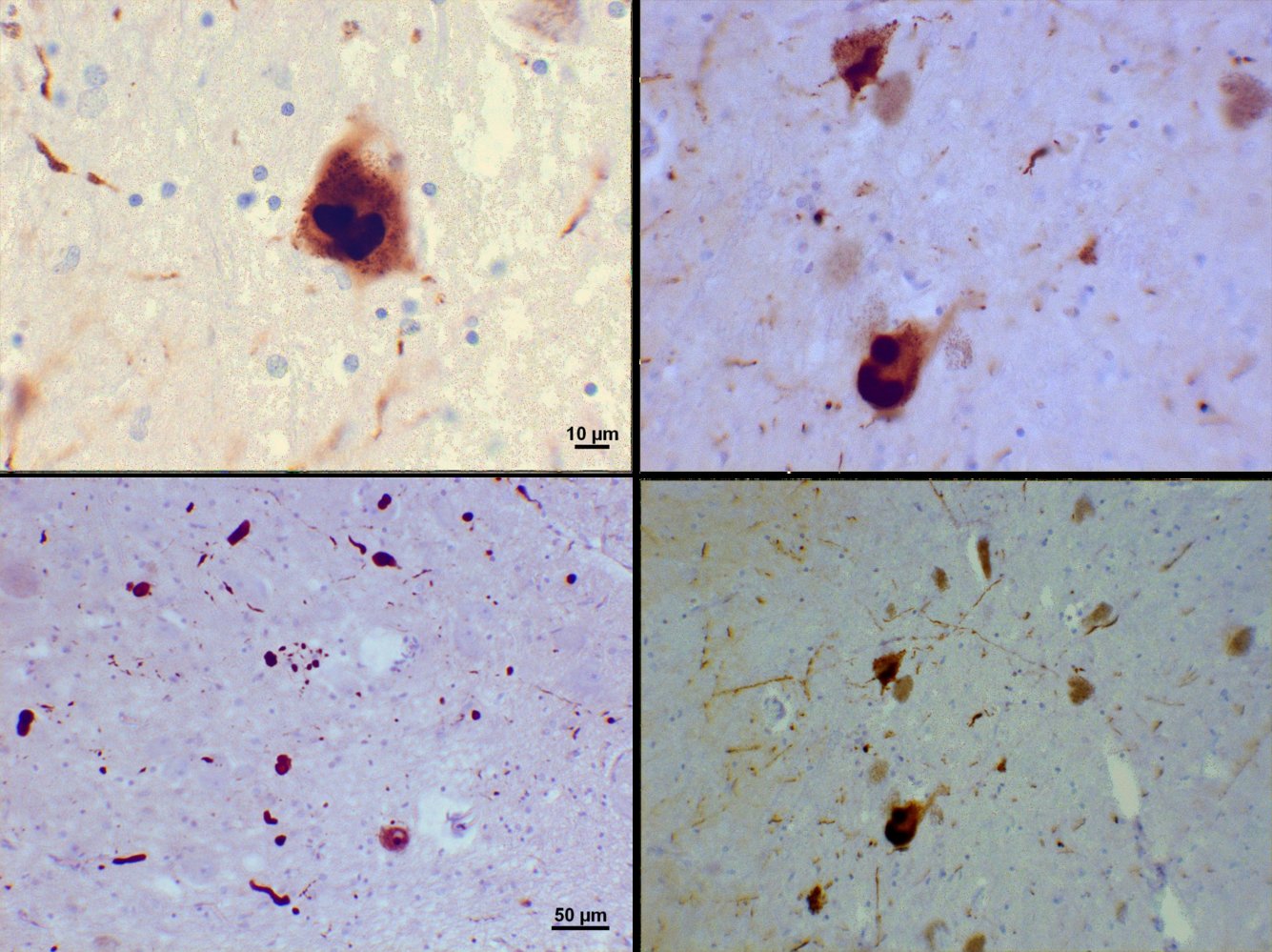
Microscopy of the substantia nigra of a patient with Parkinson disease (upper row: 60x magnification, lower row: 20x magnification; staining with antibodies against alpha-synuclein, counterstaining with Mayer hematoxylin)
Both Lewy bodies (spherical intracytoplasmic aggregates of alpha-synuclein; green overlay) and the strand-like Lewy neurites (neurites containing alpha-synuclein aggregates; white arrows) are visible.
Source: “Lewy bodies (alpha synuclein inclusions)” by Suraj Rajan, Wikimedia Foundation, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
.svg){kind=link}
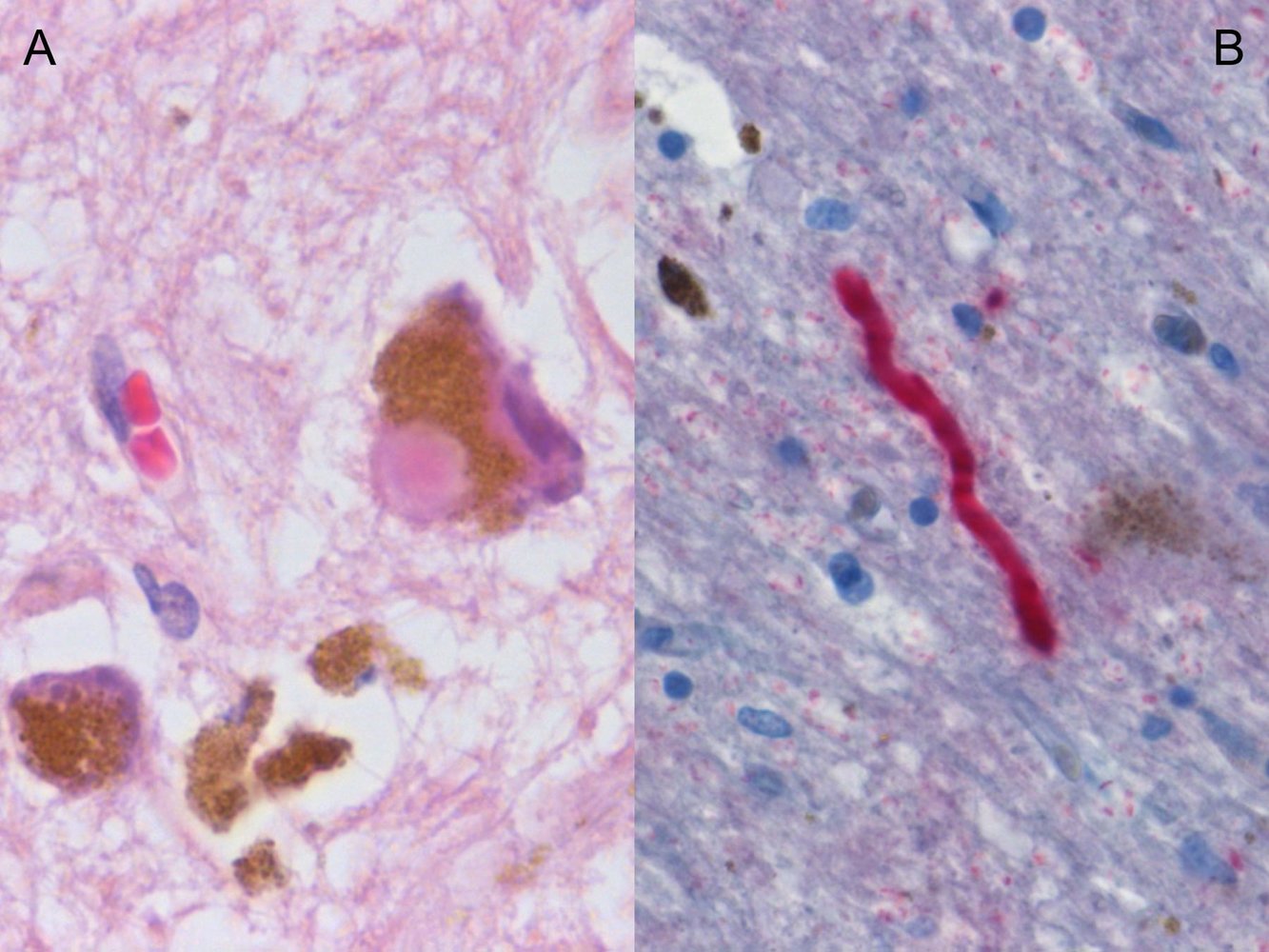
Photomicrographs of a substantia nigra tissue sample (A: H&E stain, 500x magnification; B: immunochemical α-synuclein stain, 400x magnification)
Image A: An eosinophilic cytoplasmic inclusion (Lewy body; blue overlay) is visible inside a neuron. There is a large accumulation of neuromelanin (brown granules; green overlay).
Image B: A neurite staining positive for α-synuclein is visible in the center of the image (Lewy neurite; yellow overlay).
Lewy bodies and neurites are seen in various neurodegenerative disorders, e.g., Parkinson's disease and dementia with Lewy bodies.
Source: “Figure 1, in: Proteome analysis of human substantia nigra in Parkinson's disease” by Cornelius Werner, Roland Heyny-von Haussen, Gerhard Mall, Sabine Wolf, Proteome Science Journal, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Differential diagnoses
| Differential diagnoses of Parkinson disease [5][11][18][19][20] | |||||
|---|---|---|---|---|---|
| Characteristics | Parkinson disease | Vascular parkinsonism | Multiple system atrophy | Progressive supranuclear palsy | Corticobasal degeneration |
| Usual onset age |
|
|
|
|
|
| Average survival |
|
|
|
|
|
| First symptoms |
|
|
|
|
|
| Parkinsonism | |||||
| Symmetricity |
|
|
|
|
|
| Tremor |
|
|
|
|
|
| Postural instability |
|
|
|
|
|
| Rigidity |
|
|
|
|
|
| Other clinical signs | |||||
| Eye movements |
|
|
|
|
|
| Bulbar dysfunction |
|
|
|
|
|
| Other specific features |
|
|
|
|
|
| Imaging |
|
|
|
|
|
The differential diagnoses listed here are not exhaustive.
Management
General principles [13][17][22]
- Offer supportive care to all patients.
- Initiate pharmacotherapy when symptoms start to cause functional impairment.
- Consult a neurologist or movement disorder specialist before initiating or changing treatment.
- Manage associated symptoms (e.g., major depressive disorder, dementia) as necessary.
Pharmacotherapy does not alter the disease trajectory in PD; initiate when symptoms interfere with quality of life.
Supportive care [10]
-
Rehabilitation
- Physical therapy and exercise
- Occupational therapy
- Speech therapy
-
Fall prevention [23]
- Assess for and eliminate or treat risk factors.
- See “Falls in older adults.”
-
Nutrition
- Encourage fiber intake and adequate hydration to reduce constipation.
- Ensure adequate calcium and vitamin D intake to optimize bone health.
- Consider referral to a dietitian for specialist advice.
- Sleep hygiene
-
Advance care planning
- Prognosis and end-of-life choices should be discussed early.
- Consider palliative care as needed.
Treatment [10][24][25]
Choose initial therapy based on individual patient factors (e.g., motor symptoms, age, comorbidities). To delay levodopa-based treatment for as long as possible, various age thresholds were previously recommended. [25]
- Commonly used options for initial monotherapy include levodopa, a dopamine agonist, or an MAO-B inhibitor.
-
Risk factors for levodopa-induced dyskinesia include: [24]
- Young age
- Low body weight
- Female sex
- Severe disease
- In patients with refractory symptoms or intolerable adverse effects that require dose reduction, consider:
- Switching monotherapy
- Combination therapy
- Avoid abrupt discontinuation or sudden changes in medication.
- Consider enteral infusion of levodopa or deep brain stimulation for patients with advanced disease and severe motor fluctuations.
- See “Medication for Parkinson disease” for additional information on mechanisms of action and adverse effects.
Levodopa is the most effective treatment for motor symptoms in PD but is associated with time- and dosage-dependent increase of dyskinesia.
Avoid abrupt discontinuation or sudden changes in medication. Consult a specialist if such changes are necessary.
Pharmacological treatment
| Pharmacological treatment for PD [10][22] | |||
|---|---|---|---|
| Agents | Indications | Important considerations | |
| Levodopa |
|
|
|
| Nonergot dopamine receptor agonists |
|
|
|
| MAO-B inhibitors |
|
|
|
| Anticholinergics |
|
|
|
| NMDA antagonist |
|
|
|
| COMT inhibitors |
|
|
|
Anticholinergics and levodopa/carbidopa can increase intraocular pressure; avoid in patients with glaucoma.
Ergot dopamine agonists (e.g., bromocriptine) have mostly been replaced by nonergot agonists because of significant side effects (e.g., pulmonary fibrosis).
Overstimulation of D2 receptors by levodopa or dopamine agonists may induce psychosis and hallucinations, especially in older patients with concurrent dementia or other psychiatric disorders.

Deep brain stimulation (DBS) [13][26]
-
Indications
- Severe motor symptoms or refractory tremor
- Decrease in dosage of medication because of adverse effects
-
Procedure
- Stereotactic implantation of stimulating electrode(s) targeting the subthalamic nucleus or internal globus pallidus
- Controlled remotely
-
Complications
- Infection
- Hemorrhage
- Breakage or displacement of electrodes or leads

Treatment of associated symptoms [13][22]
Under specialist guidance, carefully consider the risks and benefits of pharmacological treatment of nonmotor symptoms.
-
Major depressive disorder
- Options include cognitive behavioral therapy and/or treatment with an antidepressant, e.g., SSRI, SNRI, or tricyclic antidepressant.
- Do not combine these drug classes with MAO-B inhibitors.
- Dementia: Consider treatment with rivastigmine.
-
Psychosis
- Taper off antiparkinson medications as able.
- Consider pimavanserin, clozapine, or quetiapine (off-label). [13]
-
Autonomic dysfunction [10]
- Detrusor hyperactivity: Consider medications without significant CNS effects when available (e.g., trospium chloride).
- Neurogenic orthostatic hypotension: Consider droxidopa.
-
Constipation
- Encourage lifestyle changes for constipation.
- Consider polyethylene glycol or probiotic therapy.
- Erectile dysfunction: Consider sildenafil.
- Sialorrhea: Options include botulinum toxin injections, glycopyrrolate, or sublingual atropine.
-
Sleep disorders (e.g., RBD)
- Consider treatment with melatonin or clonazepam.
- Improve sleep hygiene.
While improvement of nonmotor symptoms is often crucial for quality of life, treatments often worsen other clinical features of PD.
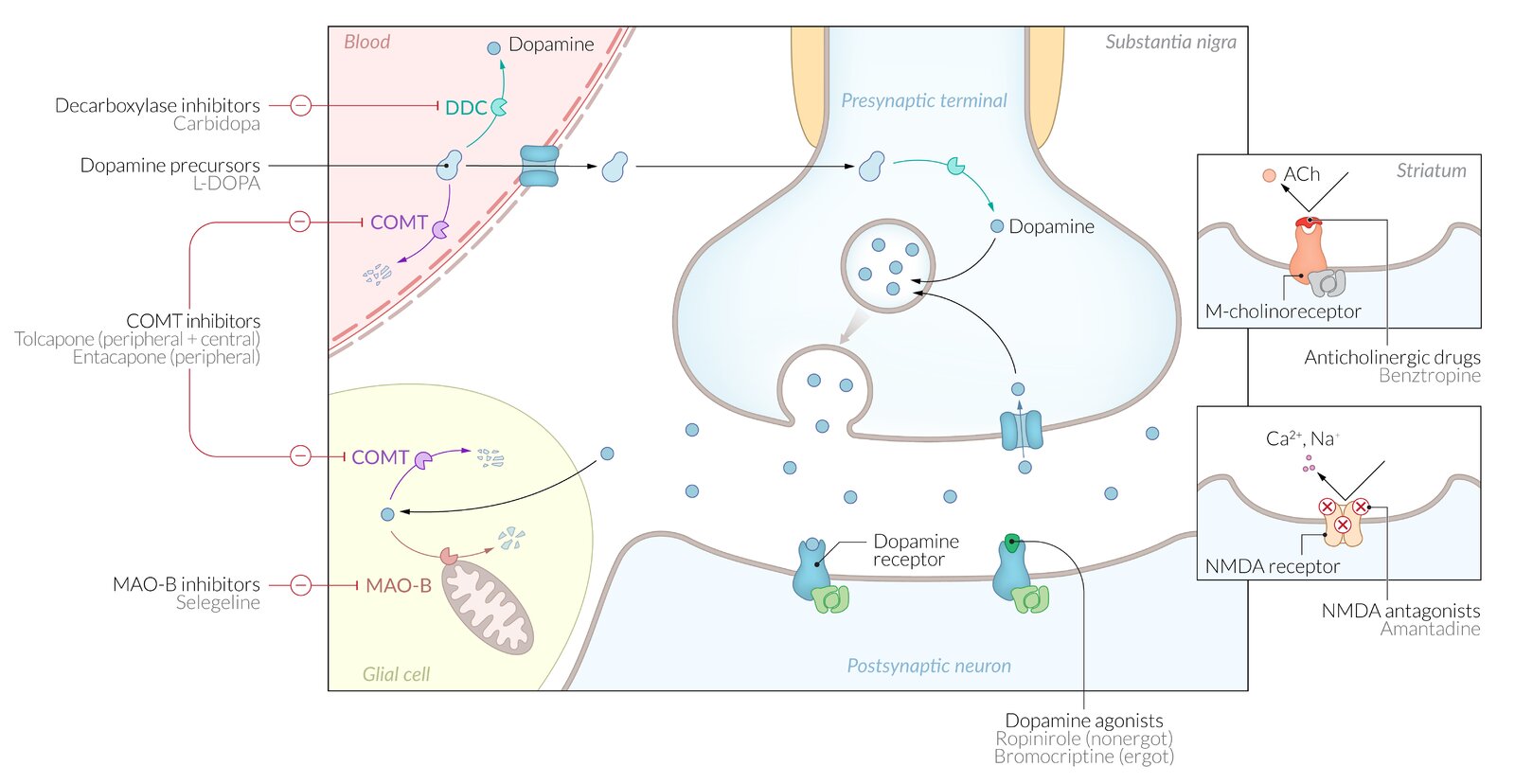
Dopamine agonists (e.g., ropinirole, bromocriptine) bind to the dopamine receptor, mimicking the action of dopamine.
DOPA-Decarboxylase (DDC) inhibitors (e.g., carbidopa) decrease the peripheral conversion of L-DOPA to dopamine, which results in reduced peripheral side-effects of L-DOPA. These drugs cannot cross the blood-brain barrier and therefore do not reduce dopamine production in the brain nor do they have central side-effects.
Dopamine precursors (e.g., L-DOPA) are converted by DOPA decarboxylase at the presynaptic neuron resulting in direct dopaminergic effects (especially in D2 receptors).
COMT inhibitors (e.g., entacapone, tolcapone) inhibits central (tolcapone) or peripheral (entacapone) catechol-O-methyl transferase (COMT) resulting in the reduced metabolization of dopamine, increase in dopamine effects, a decreased demand for L-DOPA, and a longer therapeutic effect with each dose.
MAO-B inhibitors (e.g., selegiline) reduce the metabolism of central dopamine by inhibiting the monoamine oxidase B enzyme, which normally breaks down dopamine (and catecholamines) in the brain. This results in a prolonged dopamine effect and reduced demand for L-DOPA.
Anticholinergic drugs (e.g., benztropine) inhibit excitatory cholinergic neurons, resulting in a proportionately lower concentration of acetylcholine compared to dopamine.
NMDA antagonists (e.g., amantadine) act as antagonists at the glutamate N-methyl-D-aspartate (NMDA) receptor, which results in a dopaminergic effect.
© AMBOSS

Cranial x-ray of a patient with Parkinson disease after bilateral insertion of electrodes for deep brain stimulation (coronal view)
The two lines of increased radiopacity represent electrodes placed in the basal ganglia with wires leading out through the skull and down the neck laterally. The wires are connected to a pulse generator that is usually placed in the chest.
Source: “Tiefe Hirnstimulation - Sonden RoeSchaedel ap” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
External Resources
References
- "The prevalence of Parkinson's disease: A systematic review and meta-analysis". http://onlinelibrary.wiley.com/doi/10.1002/mds.25945/abstract?systemMessage=Wiley+Online+Library+will+be+unavailable+on+Saturday+30th+July+2016+from+08:00-11:00+BST+/+03:00-06:00+EST+/+15:00-18:00+SGT+for+essential+maintenance.Apologies+for+the+inconvenience.. [2014-06-28]
- "A systematic review of the worldwide prevalence and incidence of Parkinson's disease". https://www.ncbi.nlm.nih.gov/pubmed/21696087. [2011-06-01]
- Kasper DL, Fauci AS, Hauser S, et al. "Harrisons Principles of Internal Medicine ". McGraw-Hill Medical Publishing Division. 19. (2016). ISBN: 9780071802154
- Shin HW, Chung SJ. "Drug-Induced Parkinsonism". J Clin Neurol. 8(1). :15-21. (2012)
- Daroff RB, et al. "Bradley's Neurology in Clinical Practice". Elsevier. ISBN: 9780323287838
- Lorraine V Kalia, Anthony E Lang. "Parkinson's disease". The Lancet. 386(9996). :896-912. (2015)
- Ropper A, Klein J, Samuels M. "Adams and Victor's Principles of Neurology 10th Edition". McGraw-Hill Education / Medical. (2014). ISBN: 9780071794794
- Halli-Tierney AD, Luker J, Carroll DG. "Parkinson Disease". Am Fam Physician. 102(11). :679-691. (2020)
- Homayoun H. "Parkinson Disease". Ann Intern Med. 169(5). :ITC33-ITC48. (2018)
- Armstrong MJ, Okun MS. "Diagnosis and Treatment of Parkinson Disease". JAMA. 323(6). :548. (2020)
- Postuma RB, Berg D, Stern M et al. "Clinical Diagnostic Criteria for Parkinson's Disease". Movement disorders. 30(12). :1591-1599. (2015)
- Saranza G, Lang AE. "Levodopa challenge test: indications, protocol, and guide". J Neurol. (2020)
- Poewe W, Seppi K, Tanner CM, et al. "Parkinson disease". Nat Rev Dis Primers. 3(1). (2017)
- Booth TC, Nathan M, Waldman AD, et al. "The Role of Functional Dopamine-Transporter SPECT Imaging in Parkinsonian Syndromes, Part 1". American Journal of Neuroradiology. 36(2). :229-235. (2015)
- Booth TC, Nathan M, Waldman AD, et al. "The Role of Functional Dopamine-Transporter SPECT Imaging in Parkinsonian Syndromes, Part 2". American Journal of Neuroradiology. 26(2). :236-244. (2015)
- Doty RL. "Olfactory dysfunction in Parkinson disease". Nature Reviews Neurology. 8(6). :329-339. (2012)
- Grimes D, Fitzpatrick M, Gordon J, et al. "Canadian guideline for Parkinson disease". Can Med Assoc J. 191(36). :E989-E1004. (2019)
- A. B. Deutschländer, O. A. Ross, D. W. Dickson, Z. K. Wszolek. "Atypical parkinsonian syndromes: a general neurologist's perspective". European Journal of Neurology. 25(1). :41-58. (2017)
- McFarland NR. "Diagnostic Approach to Atypical Parkinsonian Syndromes". CONTINUUM: Lifelong Learning in Neurology. 22(4). :1117-1142. (2016)
- Korczyn AD. "Vascular parkinsonism—characteristics, pathogenesis and treatment". Nature Reviews Neurology. 11(6). :319-326. (2015)
- Staszewski J, Piusińska-Macoch R, Brodacki B, et al. "Vascular parkinsonism and vascular dementia are associated with an increased risk of vascular events or death". Archives of Medical Science - Atherosclerotic Diseases. 2(2). :16-23. (2017)
- Connolly BS, Lang AE. "Pharmacological Treatment of Parkinson Disease". JAMA. 311(16). :1670. (2014)
- Allen NE, Schwarzel AK, Canning CG. "Recurrent Falls in Parkinson’s Disease: A Systematic Review". Parkinsons Dis. 2013. (2013)
- Pringsheim T, Day GS, Smith DB, et al. "Dopaminergic Therapy for Motor Symptoms in Early Parkinson Disease Practice Guideline Summary". Neurology. 97(20). :942-957. (2021)
- Susan H. Fox, Regina Katzenschlager, Shen-Yang Lim, et al. "International Parkinson and movement disorder society evidence-based medicine review: Update on treatments for the motor symptoms of Parkinson's disease". Movement Disorders. 33(8). :1248-1266. (2018)
- "Deep Brain Stimulation: A Paradigm Shifting Approach to Treat Parkinson's Disease". https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4848307/. [2016-04-28]
- Pahwa R, Factor SA, Lyons KE et al. "Practice Parameter: Treatment of Parkinson disease with motor fluctuations and dyskinesia (an evidence-based review)". Neurology. 66(7). :983-995. (2006)
- J. J. Ferreira et al. "Summary of the recommendations of the EFNS/MDS-ES review on therapeutic management of Parkinson's disease". European Journal of Neurology. 20(1). :5-15. (2012)