Summary
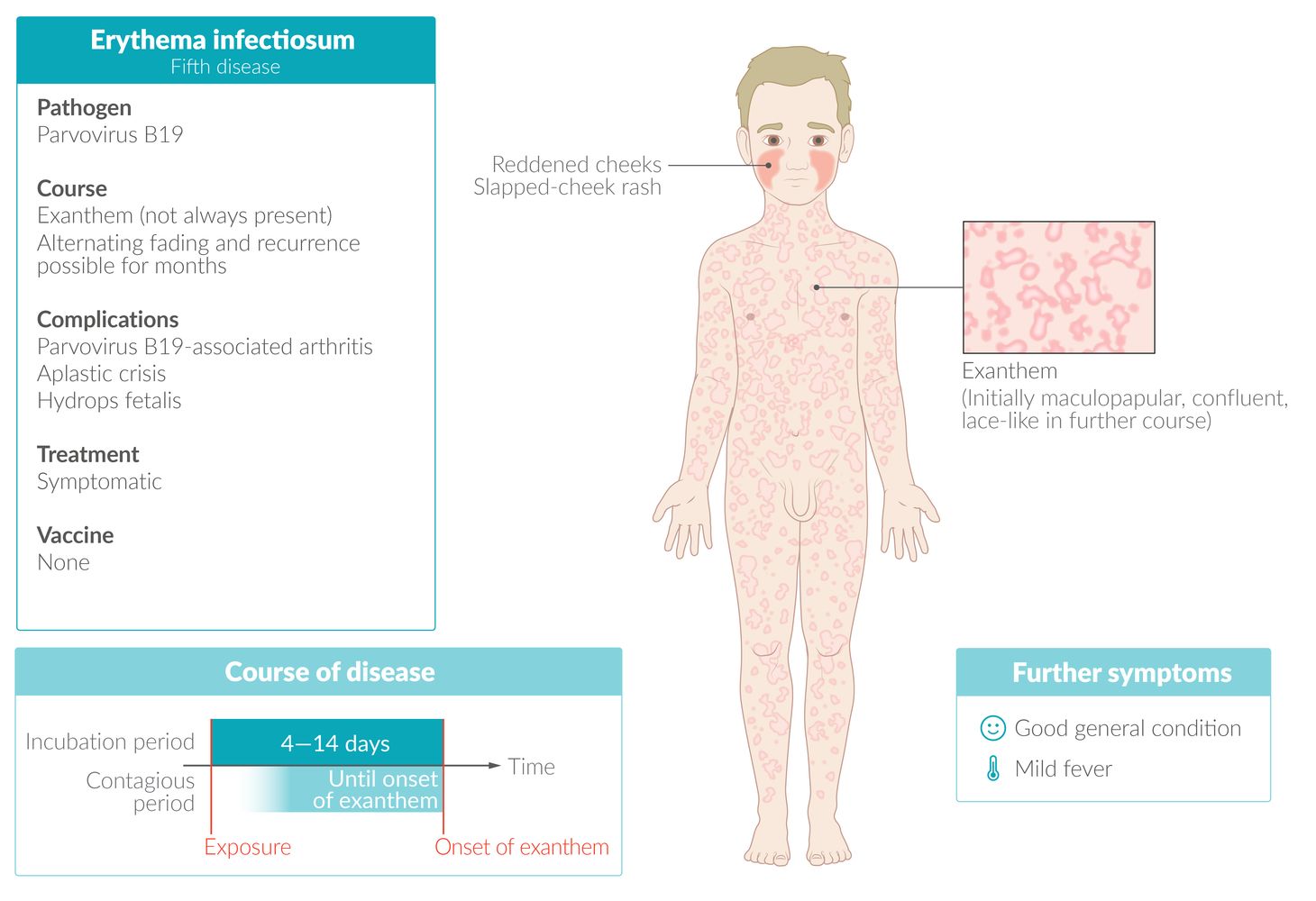
Parvovirus B19 is transmitted through respiratory droplets and has a wide range of clinical presentations. Infections occur most frequently in children, with peak incidence between 5 and 15 years of age (infection provides lifelong immunity). While most infections are asymptomatic, erythema infectiosum (fifth disease) is the most common clinical manifestation in symptomatic children. Erythema infectiosum begins with a mild febrile illness followed 7–10 days later by a rash with macules and papules that is especially noticeable on the cheeks (slapped‑cheek rash) and trunk and spreads to the extremities. The rash may be pruritic. Once the rash has appeared, the infection is no longer contagious and the patient usually feels well again, although the rash may persist for weeks, especially with heat and exposure to sunlight. In adults, the rash is typically absent and patients may develop acute-onset polyarthralgia (parvovirus B19-associated arthritis). Individuals who are immunocompromised and/or have preexisting hematological disease may develop severe anemia or pancytopenia because the virus affects the bone marrow. Diagnosis of erythema infectiosum is usually clinical; confirmatory studies are recommended for atypical presentations, pregnant patients (because of the risk of congenital TORCH infection), and immunocompromised individuals. Management is supportive.
 fact sheet")
© AMBOSS
Epidemiology
- Peak incidence: 5–15 years [1]
-
Prevalence of seropositivity
- ∼ 10% in preschool children
- ∼ 70% in adults
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Pathogen
-
Human parvovirus B19 (the smallest of the DNA viruses)
- Family: Parvoviridae
- Single‑stranded DNA virus (linear)
- Nonenveloped
- Humans are the only reservoir for parvovirus B19.
Route of transmission
- Main route: aerosol
-
Other routes
- Hematogenous transmission
- Transplacental transmission: In seronegative pregnant women, transmission to the unborn fetus may occur (in up to 30% of cases).
Incubation period [2]
- Average: 4–14 days
- May be up to 21 days
References:[3][4]
Pathophysiology
- Parvovirus B19 binds to the P antigen (globoside) on erythroid progenitor cells → cellular invasion → viral DNA enters the nucleus of erythroid cells → viral DNA replication → cytotoxicity → clinical manifestations + transient cessation of erythropoiesis [5][6]
- Parvovirus B19 can also bind to and infect endothelial cells via the P antigen, potentially causing cardiovascular complications. [7][8]
Clinical features
Individuals with parvovirus B19 infection may be asymptomatic or have any of the following presentations (see “Subtypes and variants” for additional details). [2][9]
- Mild respiratory symptoms
-
Rash
- Erythema infectiosum (fifth disease)
-
Papular-purpuric gloves-and-socks syndrome
- Painful, pruritic, papular, petechial, and/or purpuric rash affecting the hands and feet
- Fever and oral lesions may be present.
- Parvovirus B19-associated arthritis
- Severe anemia or transient aplastic crisis
-
Hydrops fetalis
- Parvovirus B19 is a TORCH infection that can cause fetal death and miscarriage.
- See also “Congenital parvovirus B19 infection.”
Children with parvovirus B19 infection often present with an exanthem, while adults are more likely to present with arthritis. [2][10]




Diffuse erythema with perioral sparing is visible on both cheeks (slapped cheek rash).
This rash is characteristic of erythema infectiosum (fifth disease).
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.

A confluent papular rash covers the palmar aspect of the hand, extending to the wrist.
This rash is consistent with papular-purpuric gloves-and-socks syndrome, a manifestation of parvovirus B19 infection.
Source: Courtesy of Dr. Gary M. White, MD

Left foot of an adult
There is a rash with macules and papules on the arch of the foot, extending upward toward the medial malleolus. Confluent erythema is seen over the rest of the visible foot.
Together with similar lesions in the hands, this is a typical finding of papular-purpuric gloves-and-socks syndrome, which is usually triggered by viral infections (most commonly parvovirus B19).
Source: Courtesy of Dr. Gary M. White, MD
Diagnosis
General principles [11][12]
- Erythema infectiosum and parvovirus B19-associated arthritis are diagnosed clinically.
-
Confirmatory studies for parvovirus B19 are recommended in:
- Diagnostic uncertainty
- Immunocompromised individuals
- Additional testing may be indicated for:
- Suspected anemia or aplastic crisis (e.g., in immunocompromised individuals)
- Exclusion of alternative diagnoses (e.g., rheumatologic disease in patients with arthritis)
- See “Subtypes and variants” for details.
Congenital infection with parvovirus B19 can cause severe complications; for more information on diagnosis during pregnancy, see “Parvovirus B19 infection during pregnancy.”
Confirmatory studies for parvovirus B19
-
Immunocompetent individuals: IgM and IgG antibodies [2]
- IgM: usually detectable when the rash appears; remains positive for 2–3 months
- IgG: positive after approx. 2 days; remains positive for life
- Immunocompromised individuals: NAAT [2]
Immunocompromised patients may have falsely negative serum IgM and IgG. [2]
Subtypes and variants
Erythema infectiosum (fifth disease) [2]
-
Clinical features
-
Prodromal stage: systemic symptoms occurring 7–10 days before rash [2]
- Fever (often mild)
- Myalgia and/or arthralgias
- Malaise
- Headache
-
Exanthem stage: characteristic rash
- Slapped-cheek appearance; diffuse redness of the face with perioral sparing
- Reticular rash originating on the trunk and spreading to the extremities; adopts a lace‑like, reticular appearance over time as it clears.
- Often pruritic
- May recur with environmental changes (e.g., sunlight, heat exposure) over several weeks or months
-
Prodromal stage: systemic symptoms occurring 7–10 days before rash [2]
- Diagnosis: clinical diagnosis
-
Differential diagnoses
- Other infectious rashes in childhood
- Drug hypersensitivity reaction
-
Management
- Management is supportive.
- See “Management of parvovirus B19 infection” for details.







Parvovirus B19-associated arthritis [2][10]
-
Clinical features
-
Adults [10]
- Acute-onset arthralgia with symmetrical, nondestructive polyarthritis, particularly in small joints (fingers, hands), ankles, and knees
- Affects ♀ > ♂ [2]
- Rash: absent or atypical
- May be accompanied by systemic symptoms (e.g., fever, malaise)
- Usually resolves within 2 weeks; may last months or years [10]
- Children (uncommon): most commonly affects the knees
-
Adults [10]
-
Diagnosis
- Clinical diagnosis
- In patients with diagnostic uncertainty:
- Obtain confirmatory studies for parvovirus B19.
- Consider additional studies to exclude alternative diagnoses (e.g., diagnostics for rheumatoid arthritis).
-
Differential diagnoses
- Rheumatoid arthritis
- Differential diagnoses of infection-associated arthritis
-
Management
- NSAIDs for pain management
- See “Management of parvovirus B19 infection” for details.
Parvovirus B19-associated anemia [2]
-
Clinical features
- Symptoms of pancytopenia (e.g., symptoms of anemia, symptoms of thrombocytopenia)
- May be preceded by fever, malaise, and myalgia
- Chronic pure red cell aplasia occurs in immunocompromised individuals.
- Transient aplastic crisis occurs in patients with chronic hemolytic diseases (e.g., sickle cell disease)
-
Diagnosis
- Perform confirmatory studies for parvovirus B19 in all patients. [2]
-
CBC and reticulocyte count [2]
- ↓ Reticulocytes
- ↓↓ Hemoglobin
- Thrombocytopenia and leukopenia in transient aplastic crisis
-
Management
- Refer patients with severe anemia or transient aplastic crisis to hematology.
- Blood transfusion and IVIG may be required.
- See also “Management of parvovirus B19 infection.”

There is diffuse redness of the face with perioral sparing (slapped‑cheek rash).
This rash is characteristic of erythema infectiosum (fifth disease).
© AMBOSS

There is diffuse redness of the face with perioral sparing (slapped‑cheek rash).
This rash is characteristic of erythema infectiosum (fifth disease).
© AMBOSS

The cheeks are bright red (slapped-cheek rash) and a diffuse, red, confluent rash with macules and papules is visible over the body of this infant.
This is the characteristic cutaneous appearance of erythema infectiosum (fifth disease), which is caused by infection with parvovirus B19.
This image is an adaptation. Source of original image: Wikimedia Commons. Original title: “Fifth disease”. Created by: Andrew Kerr. Licensed under Public Domain. Modifications to original image: Pixelated eyes.
{kind=link}

Multiple erythematous, partially confluent macules and papules extend over the upper arm in a reticular pattern.
This is the typical appearance of the exanthem associated with erythema infectiosum (fifth disease).
Image source of original image: www.paediatrie-in-bildern.de. Created by: Dr. Thomas Rautenstrauch.

A bilateral reticular macular exanthem is visible over the dorsal aspects of both hands.
This is the characteristic appearance of the exanthem of erythema infectiosum (fifth disease), which is caused by infection with parvovirus B19.
Source: "ID#: 4511", CDC, Centers for Disease Control and Prevention licensed under Public Domain
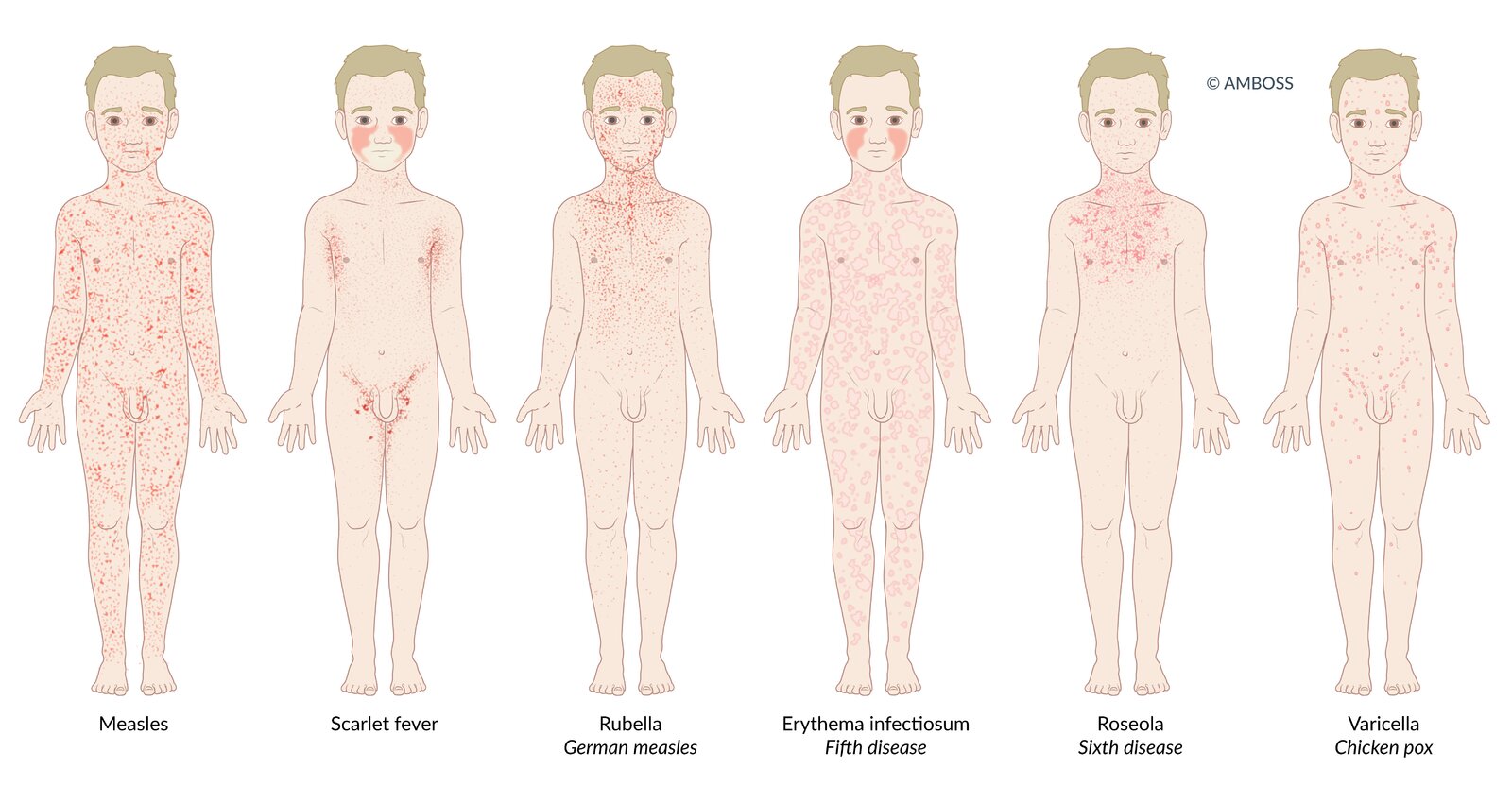
Many infectious diseases in children present with a rash (exanthem). The distribution and morphological characteristics of the exanthem allow the diseases to be differentiated from one another.
Measles: Patients present with a dark red, erythematous, maculopapular, partially confluent exanthem, which spreads from behind the ears to the rest of the body.
Scarlet fever: Patients present with a fine, light red rash with sandpaper-like texture. The exanthem begins on the neck or trunk and disseminates to the whole body. Cheeks may be flushed with perioral pallor. In flexural areas (e.g., axilla and groin), the rash may be more pronounced and linear petechiae (Pastia lines) may be present.
Rubella (German measles): Patients typically present with a nonconfluent, pink, maculopapular exanthem, which begins on the face and spreads to the trunk and extremities.
Erythema infectiosum (fifth disease): A confluent, maculopapular rash appears only in ¼ of patients. It may take on a lace-like, reticular appearance over time. Additionally, patients present with diffuse redness of the face with perioral sparing (slapped-cheek rash).
Roseola infantum (sixth disease): 3-7 days of high fever are followed by a sudden decrease in temperature and development of a patchy, blanching rose-pink maculopapular rash. The rash originates on the trunk, and may spread to the face and extremities.
Varicella (chickenpox): The exanthem affects the whole body, typically spreading to the scalp as well. Various stages of the rash occur simultaneously, which leads to the characteristic clinical finding known as “starry sky.”
© AMBOSS

© AMBOSS
Management
-
Offer symptomatic treatment. [13]
- Arthralgia: NSAIDs (for dosages, see “Oral analgesics” for adults and “Nonopioid oral analgesia in children”)
- Pruritus: Consider antihistamines.
- Fever (e.g., antipyretics, supportive care for pediatric fever)
- Provide specialist referral as indicated, e.g.:
- Obstetrics: all pregnant patients (and pregnant contacts); see also “Congenital parvovirus B19 infection.”
- Hematology: patients with severe anemia and aplastic crisis
- Educate on appropriate infection control measures. [2]
- Advise hand hygiene and respiratory hygiene for all patients and caregivers.
- Use droplet precautions for hospitalized patients with : [2][14]
- Aplastic crisis [2]
- PPGSS
- Immunosuppression and pure red cell aplasia
Children with the rash of erythema infectiosum are not contagious and do not require exclusion from school or daycare. [2]


© AMBOSS
Complications
- Hepatitis
- Myocarditis
- Aseptic meningitis and/or encephalitis
- Hemophagocytic lymphohistiocytosis
- Nephrotic syndrome
We list the most important complications. The selection is not exhaustive.
External Resources
References
- Heegaard ED, Brown KE. "Human Parvovirus B19". Clin Microbiol Rev. 15(3). :485-505. (2002)
- Committee on Infectious Disease, American Academy of Pediatrics. "Red Book: 2024-2027 Report of the Committee on Infectious Diseases, 33rd Edition". American Academy of Pediatrics. (2024). ISBN: 9781610027373
- Goodwin TM, Montoro MN, Muderspach L, Paulson R, Roy S. "Management of Common Problems in Obstetrics and Gynecology". John Wiley & Sons. (2010). ISBN: 9781444390346
- Lamont RF, Sobel JD, Vaisbuch E, et al. "Parvovirus B19 infection in human pregnancy". BJOG. 118(2). :175-186. (2010)
- Alfego D, Hernandez-Romieu AC, Briggs-Hagen M, et al. "Detection of Increased Activity of Human Parvovirus B19 Using Commercial Laboratory Testing of Clinical Samples and Source Plasma Donor Pools — United States, 2024". MMWR Morb Mortal Wkly Rep. 73(47). :1076-1081. (2024)
- Bennett JE, Dolin R, Blaser MJ. "Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases". Elsevier Health Sciences. (2014). ISBN: 9780323263733
- Landry ML. "Parvovirus B19". Microbiol Spectr. 4(3). (2016)
- Servey JT, Reamy BV, Hodge J. "Clinical Presentations of Parvovirus B19 Infection". Am Fam Physician. 75(3). :373-376. (2007)
- Allmon A, Deane K, Martin KL. "Common Skin Rashes in Children". Am Fam Physician. 92(3). :211-6. (2015)
- "Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings (2007)". https://web.archive.org/web/20250214115649/https://www.cdc.gov/infection-control/media/pdfs/Guideline-Isolation-H.pdf. [2007-01-01]
- Bua G, Manaresi E, Bonvicini F, Gallinella G. "Parvovirus B19 replication and expression in differentiating erythroid progenitor cells". PLoS ONE. 11(2). :e0148547. (2016)
- Brown KE, Anderson SM, Young NS. "Erythrocyte P antigen: cellular receptor for B19 parvovirus". Science. 262(5130). :114-7. (1993)
- Bachelier K, Biehl S, Schwarz V, et al. "Parvovirus B19-induced vascular damage in the heart is associated with elevated circulating endothelial microparticles". PLoS ONE. 12(5). :e0176311. (2017)
- Dyrsen ME, Iwenofu OH, Nuovo G, Magro CM. "Parvovirus B19-associated catastrophic endothelialitis with a Degos-like presentation". J Cutan Pathol. 35. :20-25. (2008)