Quick guide
Diagnostic approach
- ABCDE survey
- Assess for pelvic instability
- Evaluate for features of genitourinary trauma
- FAST
- Pelvic x-ray
- CBC
- CMP
- Coagulation studies
- Type and screen
- Urinalysis
- Pregnancy test
- CT abdomen and pelvis with IV contrast
Red flag features
- Hemodynamic instability
- Hemoperitoneum
- Pelvic instability
- Open fracture
- Genitourinary injury
- Neurovascular injury
Management checklist
- Two large-bore peripheral IVs
- Apply interventions for pelvic hemorrhage control (e.g., pelvic binder)
- Parenteral analgesia
- Antibiotic prophylaxis for open fractures
- Consult interventional radiology for angioembolization
- Consult surgery for intraperitoneal hemorrhage
- Consult urology for genitourinary injury
- Consult orthopedics for pelvic fracture
Summary
Pelvic fractures most often occur in patients with multiple trauma caused by impact injuries such as motor vehicle crashes or falls. Patients present with pelvic pain, reduced range of motion, and hematomas. Concomitant injuries such as urethral injury are common. The pelvic stability of every patient with multiple trauma must be checked, as shifted pelvic injuries can lead to extensive intraperitoneal and/or retroperitoneal bleeding, which can lead to hemorrhagic shock or death. The treatment for stable fractures is often conservative, with short-term bed rest and subsequent pain‑adapted mobilization. Unstable pelvic ring fractures with significant bleeding require surgery (e.g., external fixation) and/or angioembolization for hemorrhage control. This is followed by definitive fixation with plates or screws after the patient becomes hemodynamically stable. High-energy trauma may also lead to acetabular fractures. Patients present with hip pain and limited mobility. Management includes careful assessment, with nonoperative measures for stable fractures and surgical intervention for unstable cases. Alongside other possible complications, there is a significantly increased risk of thrombosis, and prophylaxis should be administered accordingly.
Epidemiology
- Peak incidence: 15–28 years
- 20% of multiple trauma patients have a pelvic injury.
- 60% of patients with pelvic injury have multiple trauma.
References:[1][2]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- High-speed motor vehicle crashes (MVCs)
- Falls, especially in older adults
Classification
Tile classification of pelvic fractures [3]
The Tile classification is based on fracture location and remaining stability of the pelvic ring.
-
Type A: stable or minimally displaced
- Type A1: fracture of the pelvic edge
- Type A2: fracture of the anterior pelvic ring
- Type A3: transverse fracture of the sacrum and/or coccyx
-
Type B: rotationally unstable and vertically stable
- Type B1: symphysis diastasis (external rotation, open book pelvic fracture)
- Type B2: lateral compression injury (internal rotation of one hemipelvis due to lateral force, e.g., sacral compression fracture)
- Type B3: bilateral fractures
-
Type C: rotationally and vertically unstable
- Type C1: unilateral fracture
- Type C2: bilateral fracture (one side type B, one side type C)
- Type C3: bilateral type C fractures


Young-Burgess classification [3][4]
The Young-Burgess classification is based on the mechanism of injury.
-
Lateral compression (internal rotation)
- Typical mechanism: side-impact MVC
- Impact on stability: varying degrees of rotational instability
- Associated injuries: bladder and urethral injuries caused by impingement of the lower genitourinary system [5]
-
Anteroposterior compression (external rotation, open book pelvic fracture)
- Typical mechanism: frontal-impact MVC (e.g., motorcycle crash)
- Impact on stability: symphysis diastasis, varying degrees of rotational and vertical instability
- Associated injuries: tears in the posterior venous plexus and branches of internal iliac arteries; hemorrhagic shock [5]
-
Vertical shear (vertical displacement of the hemipelvis)
- Typical mechanism: fall from height
- Impact on stability: complete rotational and vertical instability
- Associated injuries: disruption of sacrospinous and sacrotuberous ligaments; hemorrhagic shock [5][6]
-
Combined fracture mechanism
- More than one compression force (e.g., both lateral compression and vertical shear) applied
- Results in complex pelvic fractures
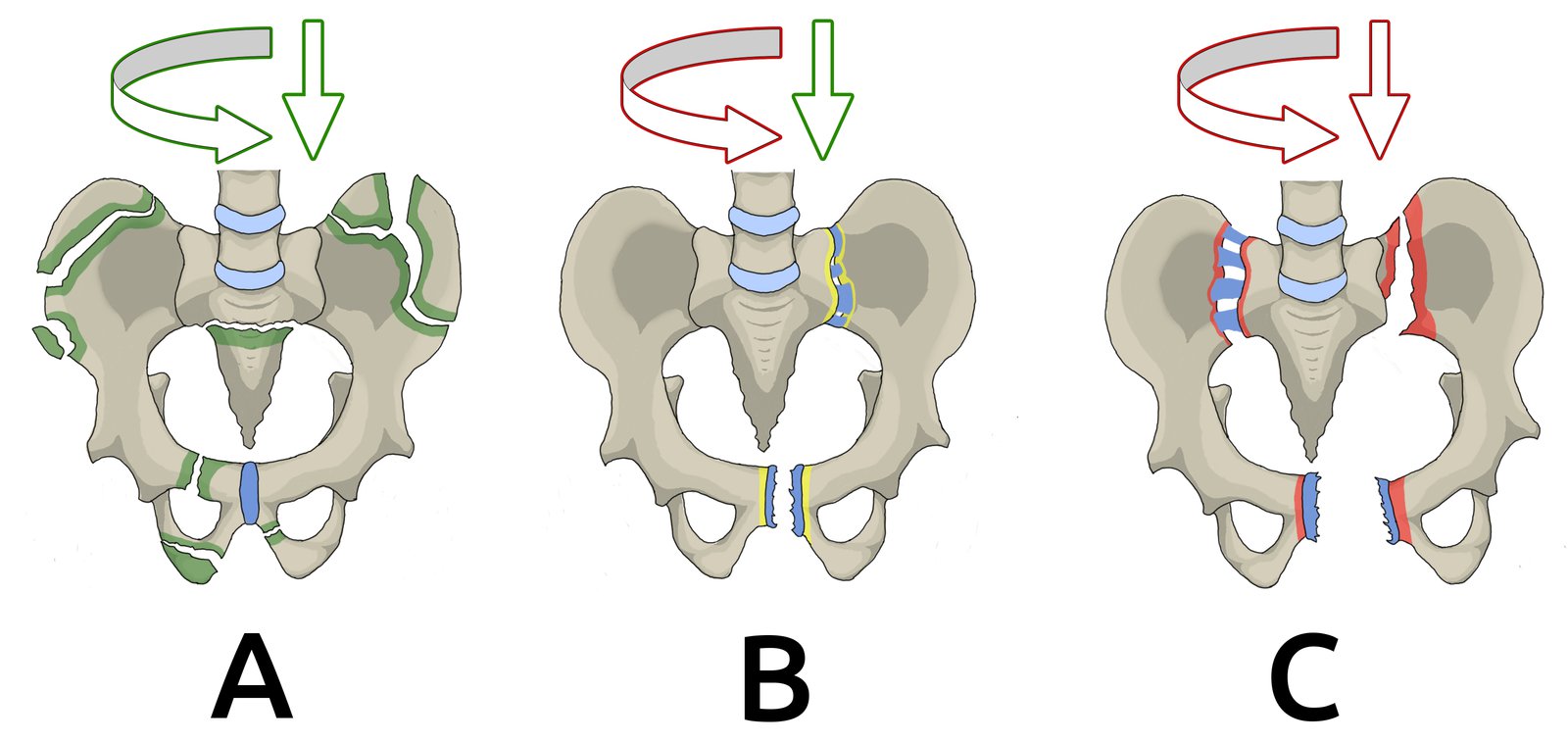
(A) stable or minimally displaced fracture (fracture of the pelvic edge, the anterior pelvic ring, or the sacrum/coccyx)
(B) rotationally unstable, vertically stable fracture (symphysis diastasis, diastasis of the sacroiliac joint)
(C) injury of the pelvic ring with rotational and vertical instability (anterior and posterior pelvic ring fracture with bilateral diastasis of the sacroiliac joint and symphysis diastasis)
The injuries are categorized according to severity (green = A, yellow = B, red = C). Green arrows indicate preserved vertical/rotational stability; red arrows indicate instability.
© AMBOSS
© AMBOSS
Clinical features
- Pelvic pain caused by movement, weight-bearing, and compression of the iliac crests
- Tilted pelvis and unequal leg length with reduced range of motion in the hip joint
-
Pelvic instability [4]
- Movement in any direction during pelvic stability assessment
- Rotational instability: Laxity of internal rotation or external rotation may be present.
- Vertical instability: Limb length discrepancy or asymmetry of the anterior superior iliac spines (ASIS) may be present.
- Labial, scrotal, flank, and inguinal hematomas
- Concomitant injuries may occur, e.g.:
- Urethral injury: blood at urethral meatus, high-riding or nonpalpable prostate, perineal swelling
- Bladder injury: frank hematuria
- Rectal, vaginal, perineal lacerations suggest an open fracture
- Acute abdomen in abdominal trauma (bowel perforation, spleen, liver rupture)
- Neurovascular injury : decreased rectal tone, perianal paresthesia, compromise of lower limbs
- Axial and long bone injuries
An isolated unilateral anterior fracture of the pelvic ring may exhibit fairly mild symptoms!
Avoid vigorous downward pressure on the ASIS when assessing pelvic stability, as pressure can loosen blood clots at the fracture site and worsen hemorrhage. [5]
Initial management
Approach [7][8][9]
In patients with pelvic fractures and hemodynamic instability, interventions for pelvic hemorrhage control take priority. Shock necessitates immediate aggressive management regardless of fracture pattern. See also “Approach to blunt abdominal trauma” for patients with associated abdominopelvic injuries.
-
Primary survey: Assess pelvic stability and identify life-threatening complications and associated injuries.
- Clinical features of shock
- Blunt abdominal trauma: e.g., abdominal bruising, peritoneal signs, positive FAST examination
- Features of genitourinary trauma
- Lower extremity neurovascular injuries
-
Patients with pelvic instability
- Obtain bedside AP pelvic x-ray.
- The following high-risk features prompt early interventions for pelvic hemorrhage control:
- High-energy fracture patterns (e.g., vertical shear, anterior-posterior compression with disruption of anterior and posterior pelvic ring)
- Open pelvic fractures
- Age > 64 years
-
Apply a pelvic binder to reduce the risk of hemorrhage and displacement.
- Slide the binder under the supine patient, centering it over the greater trochanters.
- Secure the bind and reassess pelvic stability. [7]
-
Hemodynamically unstable patients
- Signs of intraabdominal hemorrhage: Expedite emergency laparotomy and interventions for pelvic hemorrhage control simultaneously or in rapid sequence.
- No signs of intraabdominal hemorrhage: Initiate interventions for pelvic hemorrhage control.
-
Hemodynamically stable patients: Obtain CT abdomen and pelvis with contrast.
- Evidence of arterial bleeding on CT: Consult interventional radiology for angioembolization.
- Consult; orthopedic or trauma surgery for fracture stabilization.
-
Suspected genitourinary injury
- Obtain a retrograde urethrogram; and consult urology (see “Approach to genitourinary trauma”).
- Avoid transurethral catheterization; consider suprapubic catheterization instead.
Pelvic fractures with hemodynamic instability and intraabdominal hemorrhage require coordination among trauma surgery, orthopedic surgery, and/or interventional radiology, with priorities based on patient needs and available resources.
Perform DRE and vaginal examination carefully in trauma patients to avoid causing iatrogenic open pelvic fractures.
Interventions for pelvic hemorrhage control [7][9][10]
Temporizing methods
- External pelvic stabilization: e.g., pelvic binder, external fixation, pelvic C-clamp
- Preperitoneal packing: can be performed as part of damage control surgery or combined with surgeries for concomitant injuries
-
Resuscitative endovascular balloon occlusion of the aorta (REBOA)
- A minimally invasive, temporary endovascular occlusion of the aorta to prevent exsanguination [11]
- May be considered in select patients with:
- Hemodynamically unstable pelvic fractures with signs of shock when other temporizing measures are insufficient [7]
- Severe hemorrhage and/or multisystem trauma as a bridge to definitive treatment
- Limitations [7][12][13][14]
- Not for stabilization prior to transfer: requires facility with immediate resources for definitive surgical care (e.g., operating room, interventional radiology) [8]
- Guidance on indications and timing is mixed; consult with specialists and follow local protocol.
- Evidence regarding safety and efficacy is mixed.
- Adverse effects include ischemic injury and venous thromboembolism. [7][14]
Angioembolization [9][10]
- Goal: definitive hemostatic control
-
Indications
- Hemodynamic instability despite mechanical pelvic stabilization
- Evidence of active bleeding on CT
-
Timing: varies depending on patient requirements and available resources; requires multispecialty coordination [10]
- Usually performed after initial external pelvic stabilization
- May need to be performed before or after exploratory laparotomy for intraabdominal hemorrhage control
Pelvic injuries can cause heavy and potentially fatal blood loss!
Diagnosis
Imaging [7][15][16]
For patients with polytrauma, see “Urgent diagnostics for trauma patients.”
-
Pelvic x-ray: useful for bedside screening, especially in hemodynamically unstable patients ; [7][17][18]
- AP view: commonly obtained in patients with pelvic pain or tenderness after trauma
- Inlet and outlet views: can improve diagnostic sensitivity and specificity
- Findings: radiographic fracture signs
-
CT abdomen and pelvis with IV contrast
- Gold standard for hemodynamically stable patients [7]
- Potential findings
- Radiographic fracture signs
- Signs of arterial injury
- Hemoperitoneum or pneumoperitoneum
- MRI pelvis and affected hip without IV contrast: useful for detecting occult fractures [19][20]







Additional diagnostics [5][7]
- Urinalysis to screen for hematuria
- Retrograde urethrogram for suspected genitourinary trauma (see “Approach to genitourinary trauma”)
- Hemodynamic monitoring parameters and serial hemoglobin and hematocrit
- Other urgent diagnostics for trauma patients, e.g., coagulation panel, type and screen

X-ray pelvis (AP view)
The right hemipelvis is displaced superiorly, compatible with disruption of the sacroiliac joint (indicated by dashed lines and double-headed arrow). Bilateral pubic ramus fractures are also present (indicated by arrowheads).
Source: “Fig 1A, In: Robot-assisted treatment of unstable pelvic fractures with a percutaneous iliac lumbar double rod fixation combined with a percutaneous pelvic anterior ring INFIX fixation” by Du W, Sun T, Ding Y et al., SpringerLink, licensed under CC BY 4.0. Modifications: image cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
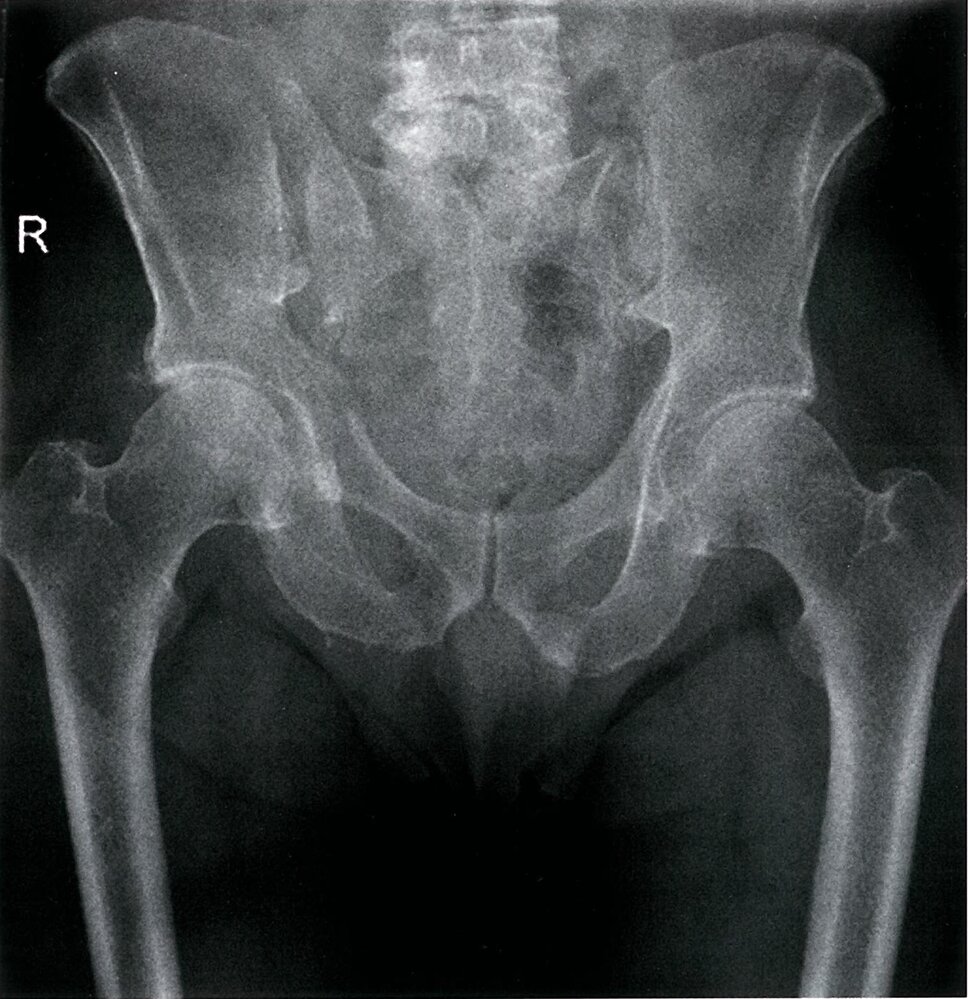
X-ray pelvis (AP view)
There is a step in the cortex at the right side of the pelvic inlet, representing a fracture of the right pubis (circle). The right sacroiliac joint is widened, indicating disruption (green overlay).
The extent of injuries visible on this radiograph indicates a need for a CT to help identify any further injuries. The CT of this patient also identified a fracture of the ilium.
Source: © IMPP

X-ray pelvis (AP view) of patient after high-energy trauma
Marked pubic symphysis diastasis is seen along with diastasis of the right sacroiliac joint. An intramedullary nail is present within the right femur.
Source: “Diastasis symphysis pubis 1300500” by Nevit Dilmen, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: Arrow removed.
{kind=link}
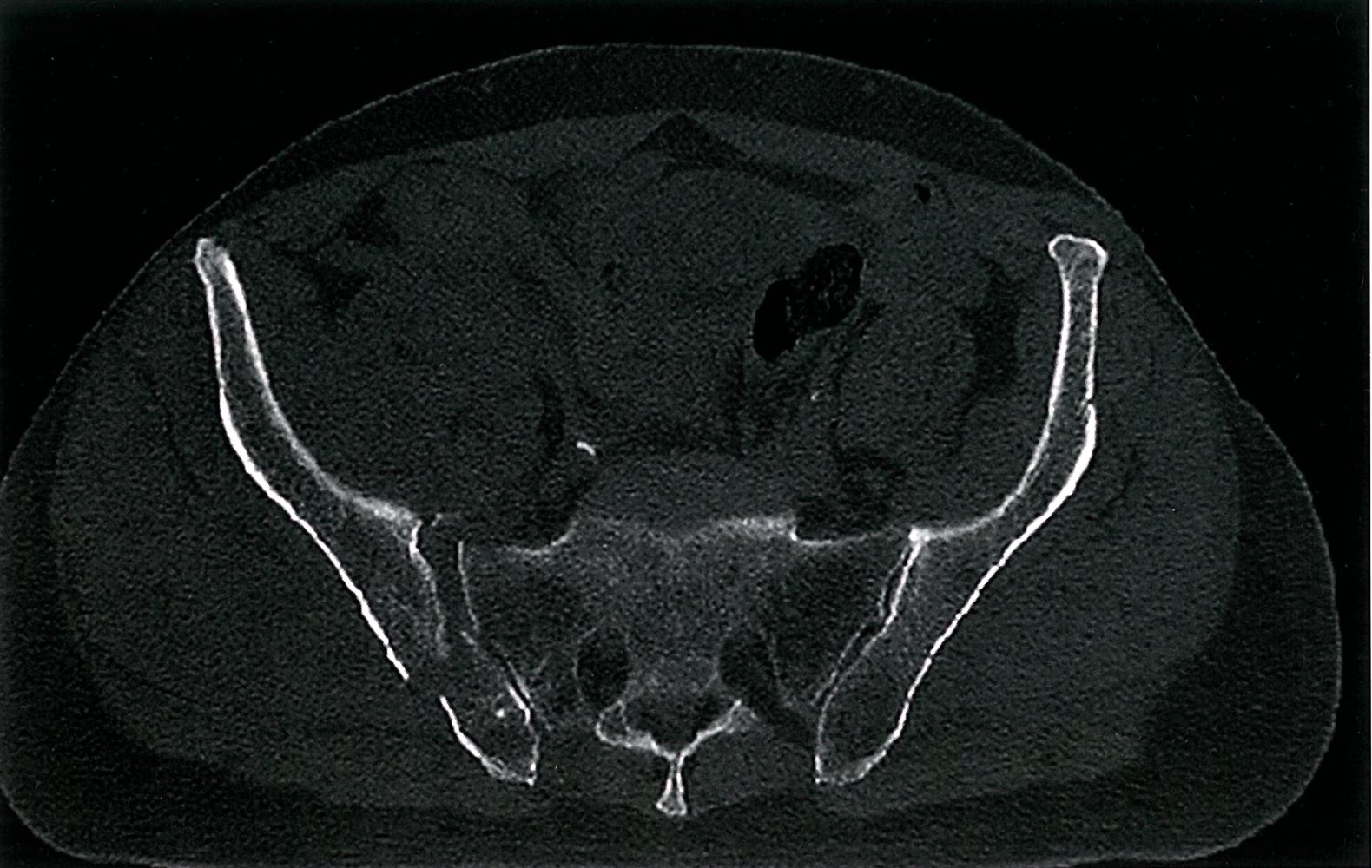
CT pelvis (bone window; axial view)
There is disruption of the right sacroiliac joint (red hatching) with a fracture through the right ilium (green circle).
Source: © IMPP
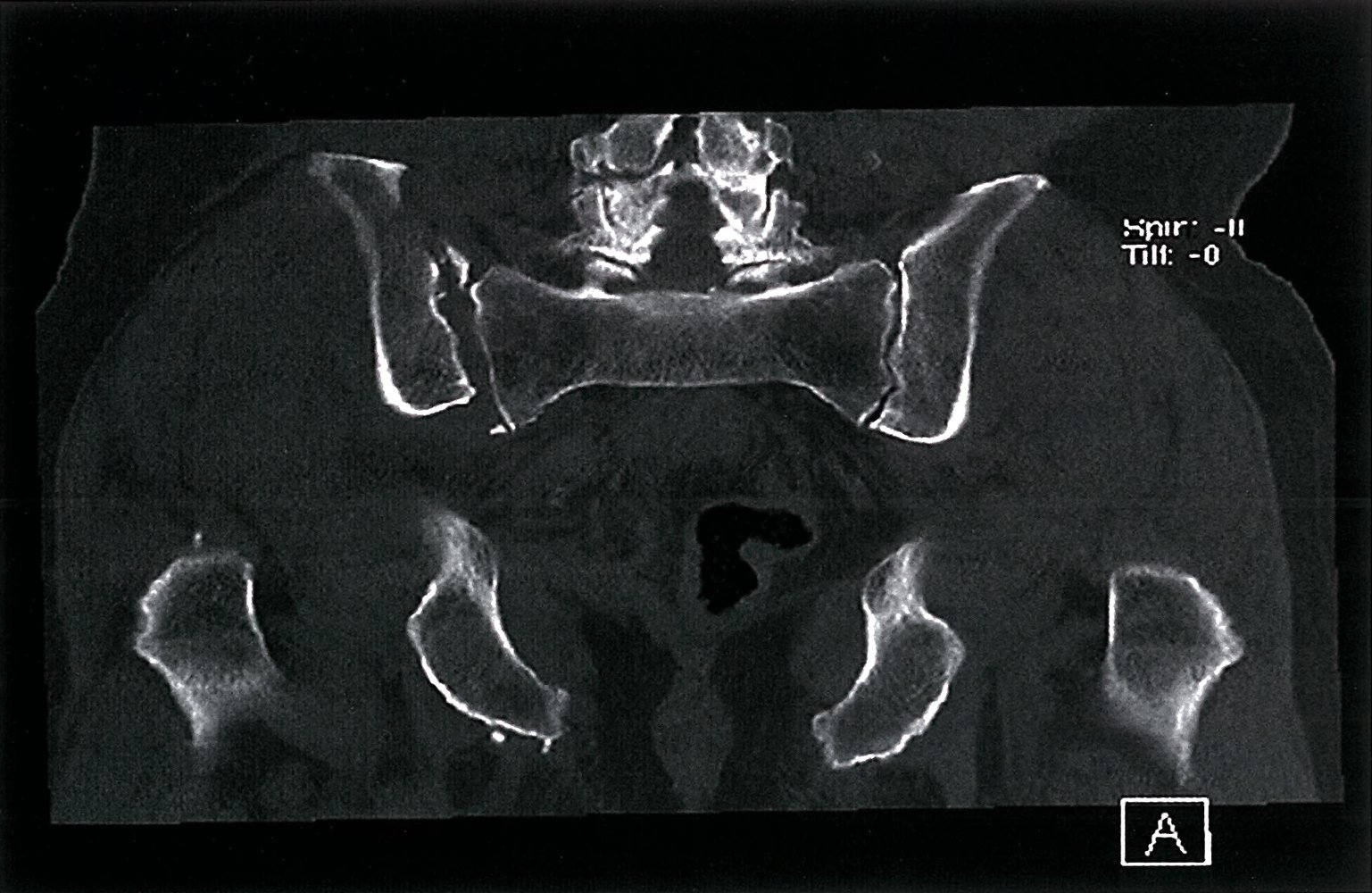
CT pelvis (bone window; coronal plane)
There is widening of the right sacroiliac joint with a small fracture fragment visible at the superior aspect of the joint (green circle).
Source: © IMPP
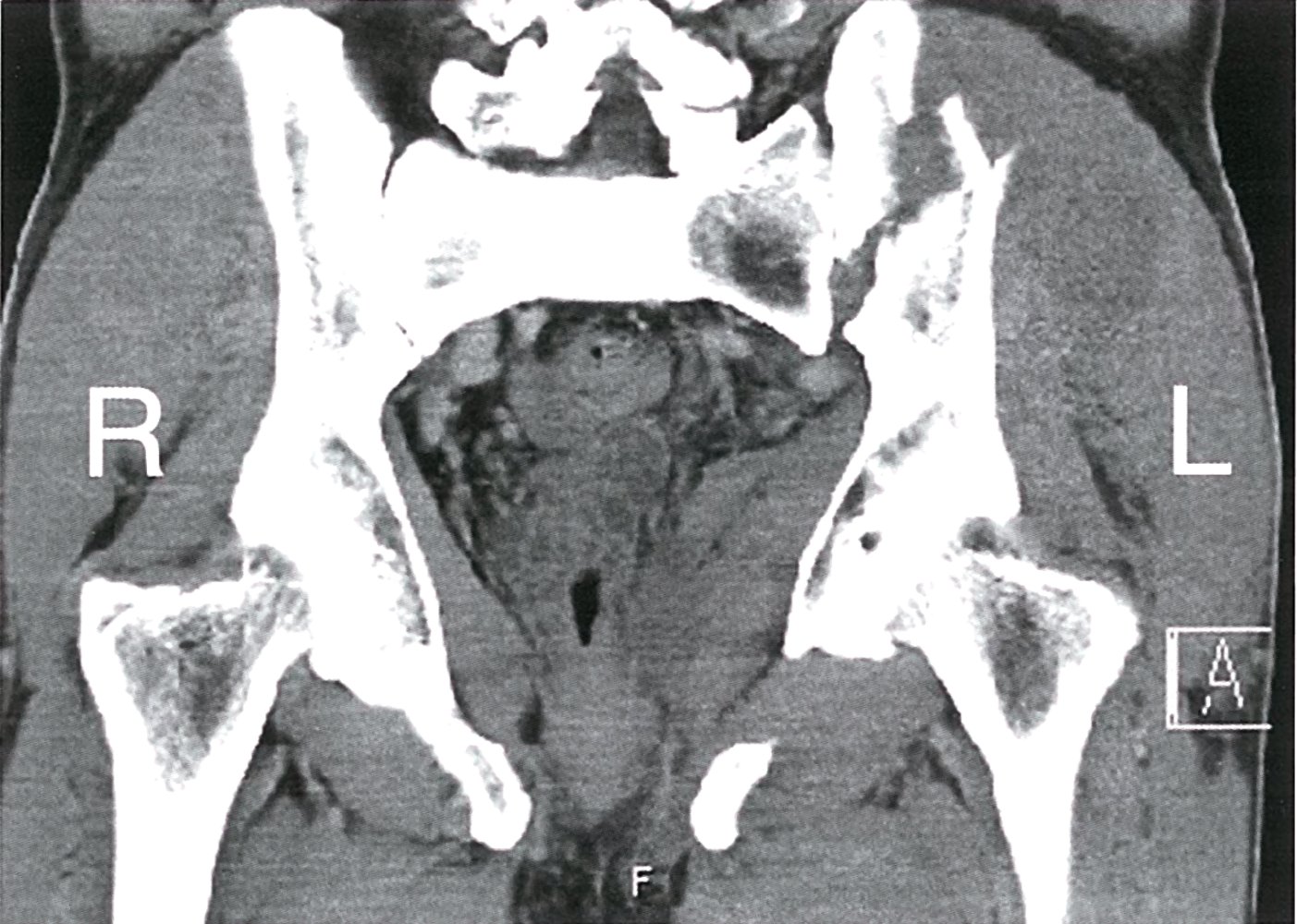
CT pelvis (soft tissue window; coronal section)
An obliquely oriented fracture, communicating with the left sacroiliac joint, is visible through the left iliac wing (green line).
Source: © IMPP

CT pelvis (3D reconstruction)
Fractures of the pubis and ischium are visible, as well as an obliquely oriented comminuted fracture through the left iliac wing to the left sacroiliac joint (green lines).
This is a type C pelvic ring fracture, according to the Tile classification, as there is disruption of both the posterior and the anterior pelvic ring.
Source: © IMPP
Treatment
See “Initial management of pelvic fractures” for the initial approach for patients with major trauma.
Nonoperative management [9]
- Indication: stable fracture patterns (e.g., Tile classification type A) [7]
-
Treatment
- Non-weight-bearing status
- Analgesia for fractures
- Physical therapy
-
VTE prophylaxis [9][21][22]
- Begin as soon as possible after hemostatic control is achieved
- Agent of choice: LMWH (See “Approach to VTE prophylaxis” for dosages.)
Surgical management [5][7]
-
Definitive surgical repair
- Indications: open, unstable, or complex fractures (e.g., open book pelvic fracture or vertical shear injury)
- Technique: depends on fracture pattern, e.g., ORIF of pelvic ring disruptions or iliac wing fractures
-
Additional surgical interventions
- Exploratory laparotomy for abdominopelvic organ injury, e.g., bowel injuries
- Repair of genitourinary injuries, e.g., bladder rupture, urethral injuries
Disposition [9]
- Admit patients with hemodynamic instability to the ICU.
- Hospital admission is typically necessary for patients with:
- Fractures requiring surgical repair
- Associated acetabular fracture
- Concomitant injuries (e.g., genitourinary, intraabdominal)
- Consider discharging patients with stable fractures and no evidence of other injuries.
Special patient groups
Pelvic fractures in children and older adults have distinct clinical features and management considerations. For pregnancy-specific trauma care, see "Management of pregnant patients with trauma".
Pelvic fractures in children [8]
- Children are less likely than adults to develop life-threatening intrapelvic hemorrhage due to a thick periosteum surrounding the pelvis.
-
Open book pelvic fractures and signs of shock
- Immediately apply a pelvic binder.
- Initiate fluid resuscitation.
- Transfer to a pediatric trauma center.
Pelvic fractures in older adults [8]
- Higher mortality
- Low-energy mechanisms (e.g., ground-level falls) can cause significant bleeding, often necessitating angioembolization.
Acetabular fracture
Etiology [9][23]
- High-impact trauma, e.g., MVC
- Direct blow to the hip
- Falls
Older individuals, especially those with osteoporosis, may sustain acetabular fractures from low-energy trauma such as falls from standing. [23]
Clinical features [9]
- Pain exacerbated by movement
- Bruising and swelling
- Inability to bear weight
- Restricted range of motion
Diagnostics [9][20][24]
- Initial imaging: Pelvic x-ray (AP and Judet views)
- Confirmatory imaging: CT pelvis and hip to assess fracture pattern, displacement, and/or involvement of surrounding structures, and for preoperative planning
- Occult fracture imaging: MRI pelvis and hip
Management
-
Nonoperative management [9][25]
- Indications: nondisplaced or minimally displaced fractures, not a surgical candidate
- Treatment includes restricted weight-bearing, analgesia, and physical therapy.
-
Surgical management [26][27][28]
- Indications: displaced fractures, comminuted fractures, and unstable fractures
- Techniques
- Open reduction and internal fixation
- Complex fractures may require total hip replacement.
Complications [29]
- Posttraumatic arthritis
- Avascular necrosis of the femoral head [30]
- Nerve injuries (e.g., sciatic nerve palsy)
- Chronic pain
Complications
- Intraperitoneal and retroperitoneal bleeding can cause hemorrhagic shock.
- Abdominal compartment syndrome
- Deep vein thrombosis
- Surgical site infection
- Neurological injury: bowel and bladder incontinence, sexual dysfunction
Pelvic fractures typically require VTE prophylaxis because of the high risk of venous thromboembolism. [22]
We list the most important complications. The selection is not exhaustive.
External Resources
- 2017 Pelvic trauma: WSES classification and guidelines
- 2016 updates: Western Trauma Association Critical Decisions in Trauma: Management of pelvic fracture with hemodynamic instability
- 2011 Eastern Association for the Surgery of Trauma Practice Management Guidelines for Hemorrhage in Pelvic Fracture - Update and Systematic Review
References
- Gänsslen A, Pohlemann T, Paul C, Lobenhoffer P, Tscherne H. "Epidemiology of pelvic ring injuries ". Injury. 27(Suppl 1). :S-A13-20. (1996)
- Asensio JA, Trunkey DD. "Current Therapy of Trauma and Surgical Critical Care". Elsevier. (2015). ISBN: 9780323169172
- Wong JML, Bucknill A. "Fractures of the pelvic ring". Injury. 48(4). :795-802. (2017)
- Halawi MJ. "Pelvic ring injuries: Emergency assessment and management". J Clin Orthop Trauma. 6(4). :252-258. (2015)
- American College of Surgeons and the Committee on Trauma. "ATLS Advanced Trauma Life Support". American College of Surgeons. (2018). ISBN: 9780996826235
- Halawi MJ. "Pelvic ring injuries: Surgical management and long-term outcomes". J Clin Orthop Trauma. 7(1). :1-6. (2016)
- "ACS TQP Best Practices Guidelines in Imaging". https://www.facs.org/media/oxdjw5zj/imaging_guidelines.pdf. [2018-10-01]
- Shyu JY, Khurana B, Soto JA, et al. "ACR Appropriateness Criteria® Major Blunt Trauma". J Am Coll Radiol. 17(5). :S160-S174. (2020)
- Coccolini F, Stahel PF, Montori G. "Pelvic trauma: WSES classification and guidelines". World J Emerg Surg. (2017)
- Obaid AK, Barleben A, Porral D, et al. "Utility of Plain Film Pelvic Radiographs in Blunt Trauma Patients in the Emergency Department". Am Surg. 72(10). :951-954. (2006)
- Kirby MW, Spritzer C. "Radiographic Detection of Hip and Pelvic Fractures in the Emergency Department". Am J Roentgenol. 194(4). :1054-1060. (2010)
- Sun EX, Mandell JC, Weaver MJ, et al. "Clinical utility of a focused hip MRI for assessing suspected hip fracture in the emergency department". Emerg Radiol. 28(2). :317-325. (2020)
- Ross AB, Lee KS, Chang EY, et al. "ACR Appropriateness Criteria® Acute Hip Pain-Suspected Fracture". J Am Coll Radiol. 16(5). :S18-S25. (2019)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Mahmoud SS, Esser M, Jain A. "Thromboembolic events in pelvic and acetabulum fractures: a systematic review of the current literature on incidence, screening, and thromboprophylaxis". Int Orthop. 46(8). :1707-1720. (2022)
- Aggarwal S, Patel S, Vashisht S, et al. "Guidelines for the prevention of venous thromboembolism in hospitalized patients with pelvi-acetabular trauma". J Clin Orthop Trauma. 11(6). :1002-1008. (2020)
- Firoozabadi R, Cross WW, Krieg JC, Routt MLC. "Acetabular Fractures in the Senior Population- Epidemiology, Mortality and Treatments". Arch Bone Jt Surg. 5(2). :96-102. (2017)
- Scheinfeld MH, Dym AA, Spektor M, et al. "Acetabular Fractures: What Radiologists Should Know and How 3D CT Can Aid Classification". Radiographics. 35(2). :555-577. (2015)
- Antell NB, Switzer JA, Schmidt AH. "Management of Acetabular Fractures in the Elderly". J Am Acad Orthop Surg. 25(8). :577-585. (2017)
- Kelly J, Ladurner A, Rickman M. "Surgical management of acetabular fractures – A contemporary literature review". Injury. 51(10). :2267-2277. (2020)
- Ebrahimi HDN, Wu CH, Karczewski D, et al. "Total hip arthroplasty in acute acetabulum fractures: a systematic review". Arch Orthop Trauma Surg. 143(11). :6665-6673. (2023)
- Giustra F, Cacciola G, Pirato F, et al. "Indications, complications, and clinical outcomes of fixation and acute total hip arthroplasty for the treatment of acetabular fractures: A systematic review". Eur J Orthop Surg Traumatol. (2023)
- Jindal K, Aggarwal S, Kumar P, et al. "Complications in patients of acetabular fractures and the factors affecting the quality of reduction in surgically treated cases". J Clin Orthop Trauma. 10(5). :884-889. (2019)
- Zanna L, Ceri L, Scalici G, et al. "Outcome of surgically treated acetabular fractures: risk factors for postoperative complications and for early conversion to total hip arthroplasty". Eur J Orthop Surg Traumatol. 33(6). :2419-2426. (2022)
- American College of Surgeons. "ATLS Advanced Trauma Life Support". American College of Surgeons. ISBN: 9781880696521
- Tran TLN, Brasel KJ, Karmy-Jones R, et al. "Western Trauma Association Critical Decisions in Trauma: Management of pelvic fracture with hemodynamic instability — 2016 updates". J Trauma Acute Care Surg. 81(6). :1171-1174. (2016)
- Bini JK, Hardman C, Morrison J, et al. "Survival benefit for pelvic trauma patients undergoing Resuscitative Endovascular Balloon Occlusion of the Aorta: Results of the AAST Aortic Occlusion for Resuscitation in Trauma Acute Care Surgery (AORTA) Registry". Injury. 53(6). :2126-2132. (2022)
- Jarvis S, Kelly M, Mains C, et al. "A descriptive survey on the use of resuscitative endovascular balloon occlusion of the aorta (REBOA) for pelvic fractures at US level I trauma centers". Patient Saf Surg. 13(1). (2019)
- Harfouche M, Inaba K, Cannon J, et al. "Patterns and outcomes of zone 3 REBOA use in the management of severe pelvic fractures: Results from the AAST Aortic Occlusion for Resuscitation in Trauma and Acute Care Surgery database". J Trauma Acute Care Surg. 90(4). :659-665. (2021)
- Chien CY, Lewis MR, Dilday J, et al. "Worse outcomes with resuscitative endovascular balloon occlusion of the aorta in severe pelvic fracture: A matched cohort study". Am J Surg. 225(2). :414-419. (2023)