Summary
Pelvic inflammatory disease (PID) is caused by a bacterial infection that spreads beyond the cervix to infect the upper female reproductive tract, i.e., the uterus (endometritis), fallopian tubes (salpingitis), and/or ovaries (oophoritis). It can also spread to surrounding pelvic structures (parametritis) and/or pelvic peritoneum (peritonitis). The most common pathogens that cause PID are Chlamydia trachomatis and Neisseria gonorrhoeae. Patients may be asymptomatic, have mild pelvic pain with vaginal discharge, or present with signs of systemic inflammation, including fever and severe abdominal pain. PID is a clinical diagnosis; asymptomatic patients might only be diagnosed retrospectively during a workup for complications such as infertility. Initial diagnostic studies include evaluation for STIs and pregnancy. Atypical or severe presentations and/or suspected complications may be confirmed with imaging and, in rare cases, laparoscopy. Empiric antibiotic therapy that covers both Chlamydia trachomatis and Neisseria gonorrhoeae is indicated when the minimum criteria for PID are met, even if no specific infectious cause is identified. PID can cause scarring that may lead to long-term complications, including infertility, ectopic pregnancy, and chronic pelvic pain.
Definitions
- A bacterial infection that spreads beyond the cervix to infect the upper female reproductive tract, i.e., the:
- Endometrium (endometritis; see also “Postpartum endometritis”)
- Fallopian tubes (salpingitis, pyosalpinx, tubo-ovarian abscess)
- Ovaries (oophoritis, tubo-ovarian abscess)
- Surrounding pelvic structures (parametritis)
- Pelvic peritoneum (peritonitis)
Epidemiology
- Lifetime prevalence: ∼ 4.5% in women of reproductive age (18–44 years) [1]
- > 1 million women experience an episode of PID/year. [2]
- PID is one of the most common causes of infertility. [1]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Pathogens [3][4]
- Most common: Chlamydia trachomatis, Neisseria gonorrhoeae
- Less common (consider coinfections): E. coli, Ureaplasma, Mycoplasma, and other anaerobes
-
Risk factors [4]
- Multiple sexual partners, unprotected sex
- History of prior STIs and/or adnexitis
- Intrauterine devices [3]
- Vaginal dysbiosis [5]
The risk of PID is lower during pregnancy; when it does develop, it usually occurs within the first trimester and increases the risk of maternal morbidity and preterm births. [6]
Clinical features
- Lower abdominal pain (generally bilateral), which may progress to acute abdomen [7]
- Nausea, vomiting
- Fever
- Dysuria, urinary urgency
- Menorrhagia, metrorrhagia
- Dyspareunia
- Abnormal vaginal discharge (yellow/green color)


Purulent discharge can be seen on this patient's vulva on external genital examination.
Source: “SOA-gonorroe-female” by SOA-AIDS Amsterdam, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
Subtypes and variants
Pelvic cellulitis (parametritis) [8]
- Definition: acute or chronic inflammation of the parametrium
-
Clinical features
- Fever
- Dull abdominal pain or the sensation of pelvic fullness
- Absence of gastrointestinal and/or urinary signs, masses, or peritoneal signs
-
Diagnosis
- Medical history: recent gynecological surgery or procedure, infections (e.g., cervicitis, endometritis)
- Ultrasound: hyperemic, edematous tissue surrounding the uterus
- Treatment: antibiotics (See “Treatment of PID.”)
Tubo-ovarian abscess [9][10][11]
- Definition: an infectious inflammatory mass of the fallopian tubes and/or ovary that may spread to adjacent organs (e.g., bladder, bowel)
-
Clinical features include the following (see “Clinical features of PID”):
- Fever
- Lower abdominal pain
- Vaginal discharge
- Leukocytosis
-
Diagnostics
- See “Diagnostics for PID.”
- Imaging (most commonly ultrasound) is required to confirm the diagnosis.
-
Treatment
- See “Treatment of PID.”
- Admit patient for at least 24 hours for IV empiric antibiotic therapy for PID.
-
Transition clinically improved patients to oral empiric antibiotic therapy for PID with:
- Doxycycline
- PLUS either metronidazole OR clindamycin
- Obtain consultation for drainage (surgical or image-guided percutaneous drainage) for any of the following indications:
- Abscess is > 3 cm [12]
- Patient is postmenopausal [11]
- There is lack of improvement after 24–48 hours of antibiotics [10]
Diagnosis
Approach [9][13]
PID is a clinical diagnosis.
- Determine if diagnostic criteria are met with an initial evaluation for PID that includes:
- Speculum examination
- Bimanual pelvic examination
- STI testing
- Pregnancy testing
- Pursue additional evaluation for PID (e.g., imaging, invasive diagnostics) only if:
- The diagnosis remains unclear
- OR symptoms persist after treatment
Maintain a low threshold for assessing for PID in young, sexually active women with lower abdominal pain.
PID may be overlooked in asymptomatic or mild infections and is therefore sometimes diagnosed retrospectively (e.g., during an evaluation for tubal infertility).

Diagnostic criteria [9]
| Diagnostic criteria for PID [9] | |
|---|---|
| Findings | |
| Minimum criteria for PID |
|
| Supportive criteria for PID |
|
Consider alternative diagnoses in patients with no mucopurulent cervical discharge and no leukorrhea. [9]
")
Initial evaluation for PID [9][13]
Gynecological exam
-
Speculum examination to evaluate for:
- Mucopurulent cervical discharge
- Cervical friability
-
Bimanual pelvic examination ; to evaluate for:
- Cervical motion tenderness, uterine or adnexal tenderness
- Tubo-ovarian abscess or mass
Laboratory studies
-
Vaginal and/or cervical swab testing
- NAAT and/or culture for N. gonorrhoeae and C. trachomatis (see “Diagnostics of gonorrhea” and “Chlamydia infections”)
-
Wet mount preparation to evaluate for:
- WBCs (leukorrhea)
- Trichomoniasis
- Bacterial vaginosis
- Pregnancy test: to rule out intrauterine and ectopic pregnancy
-
Blood tests
- HIV testing, RPR for syphilis
- Infection markers (nonspecific for PID) [14]
- Leukocytosis on CBC
- Elevated ESR and/or CRP
PID is unlikely if WBCs are not detected on microscopic examination of cervical discharge. [9]
A Giemsa stain of discharge typically shows cytoplasmic inclusions in C. trachomatis infection, but not in N. gonorrhoeae infection.

Additional evaluation for PID [9][13][14]
Indications
- Unclear diagnosis or concern for alternative diagnosis (e.g., ectopic pregnancy, tubo-ovarian abscess, ovarian torsion) [14]
- Severe illness, e.g., nausea, vomiting, fever > 38.5°C (> 101.3°F)
- Lack of improvement within 72 hours of treatment for PID
Imaging
-
Modalities [15]
- Transvaginal ultrasound: preferred initial study if tubo-ovarian pathology or pregnancy is suspected
- CT or MRI abdomen/pelvis
-
Findings suggestive of PID
- Free pelvic fluid
- Thickened fluid-filled fallopian tubes, due to salpingitis [9][16]
-
Complications of salpingitis, e.g.:
- Pyosalpinx: the accumulation of pus in the fallopian tubes [17]
- Tubo-ovarian abscess
- Perihepatitis
Imaging is not routinely indicated but can help confirm the diagnosis of PID, especially in ambiguous cases. [9]
Invasive diagnostics
These methods can definitively confirm a diagnosis of PID, but are rarely used.
-
Diagnostic laparoscopy
- May show signs of moderate to severe salpingitis (tubal edema, erythema, and purulent exudate) , oophoritis, perihepatitis, or tubo-ovarian abscess
- Cannot be used to diagnose endometritis
-
Endometrial biopsy
- May be performed transcervically as an isolated procedure or as part of a laparoscopy [1][9]
- Used to diagnose endometritis
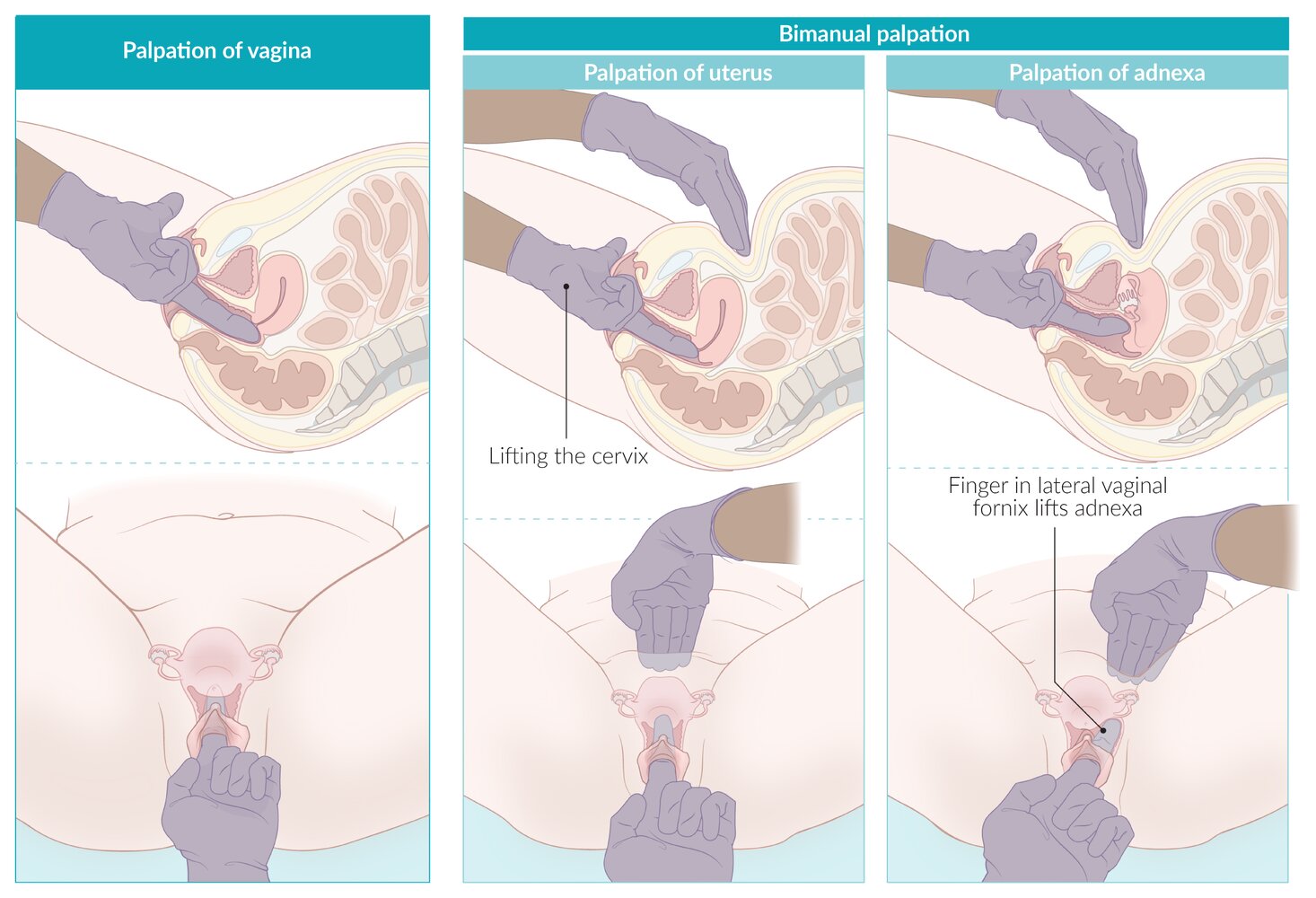
– Lubricate the index and middle fingers (or the index finger only if more size-appropriate) of one hand and slowly insert them into the vaginal canal. Place the other hand on the patient's abdomen for external pelvic palpation.
– With the inserted fingers, palpate the vaginal walls for any irregularities or masses (asking the patient to strain can make a uterine prolapse, cystocele, or rectocele more pronounced) and assess position, consistency and any tenderness of the cervix.
– Palpate the uterus bimanually, using the inserted fingers on the cervix to lift the uterus toward the abdominal examining hand. Assess uterine position, size, consistency, mobility, and any tenderness.
– Palpate the adnexa bimanually, placing the inserted fingers into each lateral vaginal fornix in turn and lifting upwards toward the abdominal examining hand, assessing for masses or tenderness. Note that the normal adnexa are frequently impalpable.
© AMBOSS
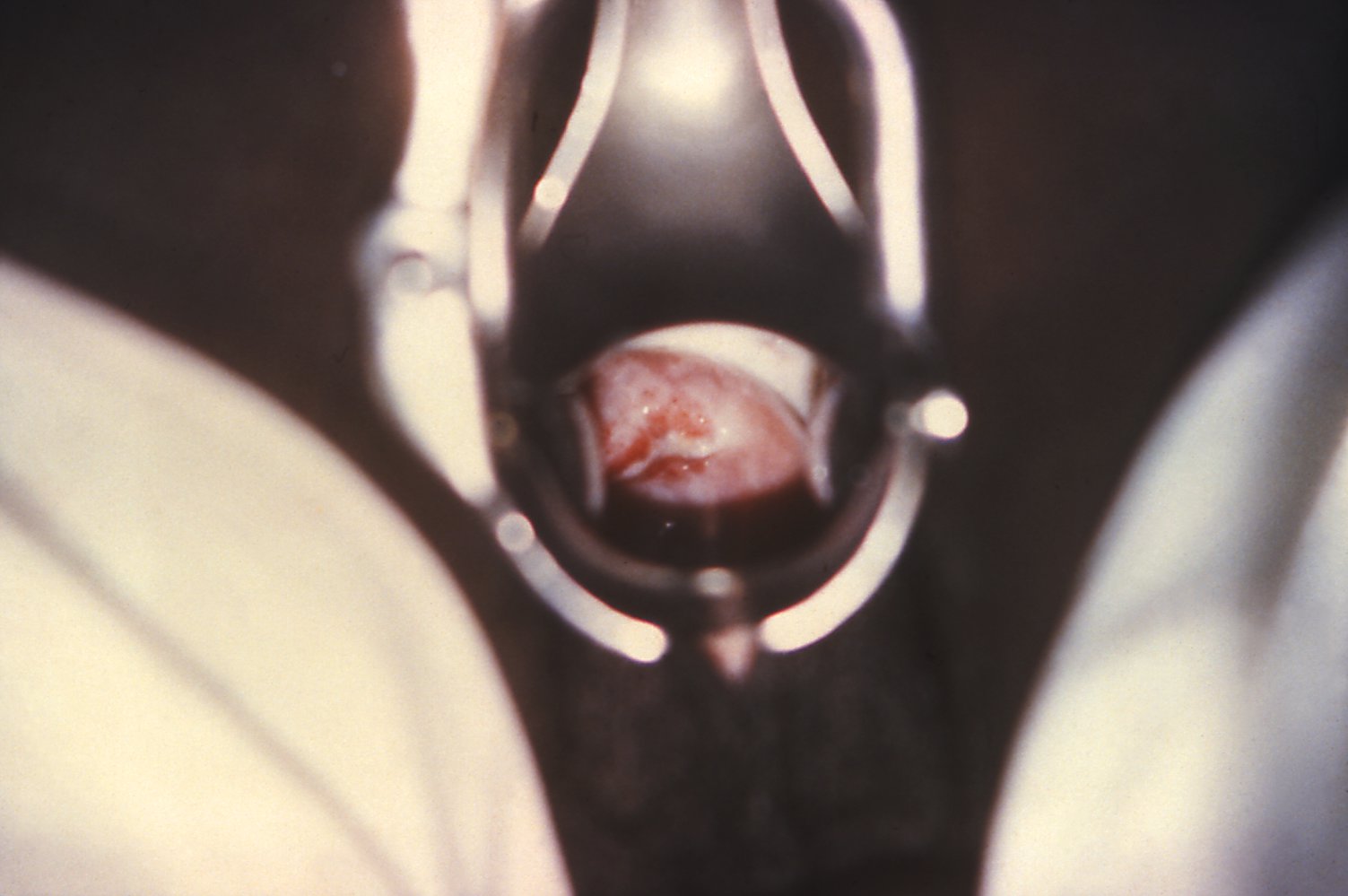
The surface of the cervix is covered with yellowish-white, purulent discharge. The external os of the uterus is inflamed and red.
These findings are consistent with gonorrhea.
Source: "ID#: 4087", CDC, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
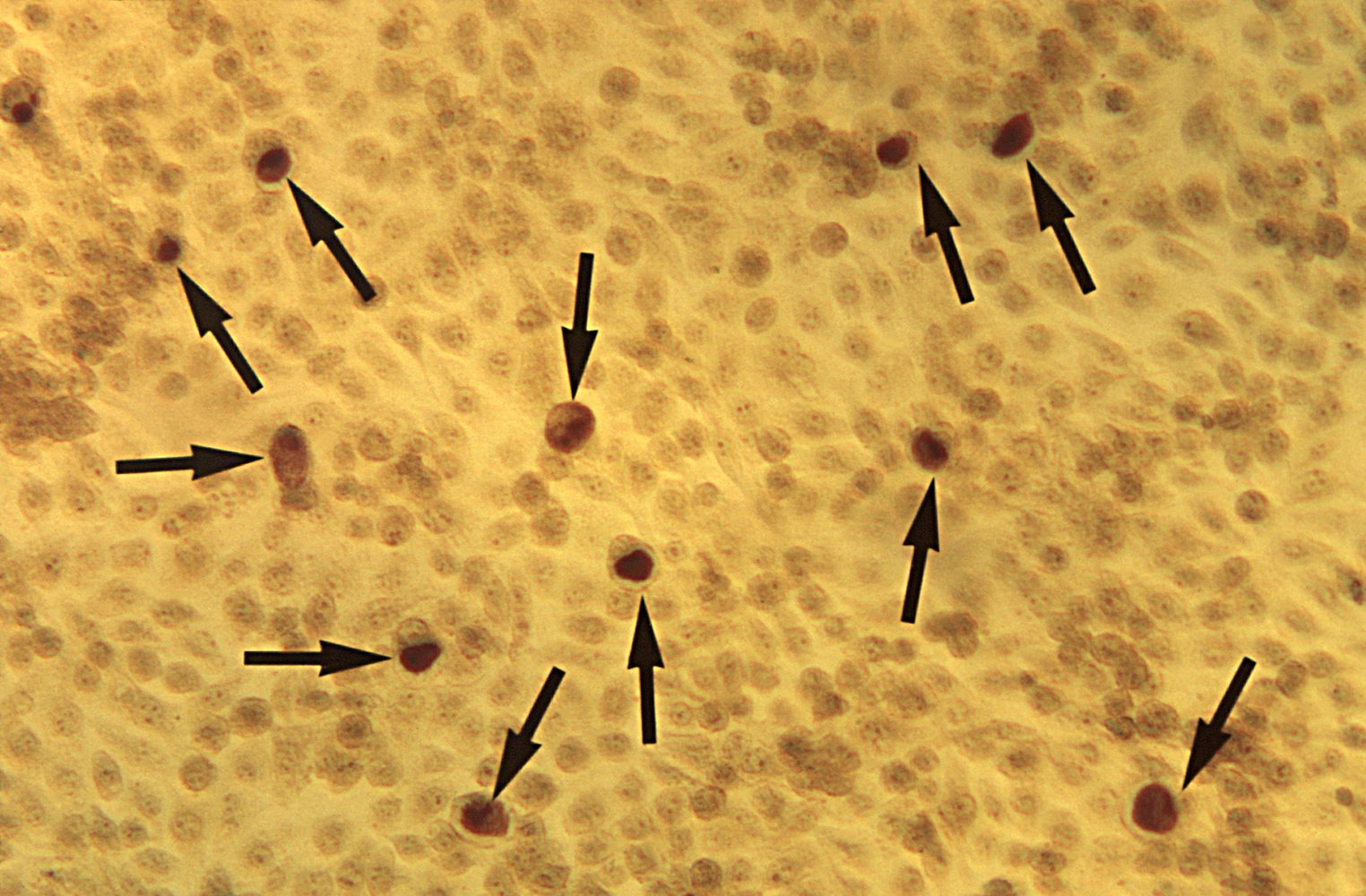
Photomicrograph of cells in McCoy cell culture (unknown magnification)
Cells infected with Chlamydia trachomatis (black arrows) show inclusion bodies (reticulate bodies, here in brown) under the microscope.
Chlamydiae are obligate intracellular bacteria that require cell culture, rather than growth medium, to grow. This characteristic is especially important for determining the best antibiotic for treatment.
Source: "ID#: 6428", CDC/ Dr. E. Arum, Dr. N. Jacobs, Centers for Disease Control and Prevention (CDC) licensed under Public Domain
Differential diagnoses
- Ectopic pregnancy
- Ovarian cyst rupture
- Ovarian torsion
- Dysmenorrhea
- Mittelschmerz
- Urinary tract infection
- Appendicitis
- Renal colic
- See also: “Causes of pelvic pain”
The differential diagnoses listed here are not exhaustive.
Treatment
Approach [9][13]
- Screen for signs of sepsis; if present, initiate immediate management of sepsis.
- Admit for inpatient management if any of the following indications are present:
- Concern for surgical emergency (e.g., differential diagnosis of acute abdomen)
- Tubo-ovarian abscess
- Severe illness with nausea, vomiting, fever > 38.5°C (101°F), and/or an unwell appearance
- Pregnancy
- Unable to tolerate or adhere to an oral regimen
- Initiate prompt empiric antibiotic therapy for PID.
- Reassess treatment response in 48–72 hours.
- Improvement : Complete a full treatment course.
- Inadequate improvement:
- Admit (if not already admitted) for IV antibiotics.
- Consider alternative diagnoses.
- Obtain additional evaluation for PID, including imaging and consideration of invasive diagnostics.
- Consider removal of IUD, if present.
- Obtain specialist consults in specific cases.
- PID in pregnancy: Consult infectious diseases.
- Tubo-ovarian abscesses with certain indications (see “Subtypes and variants”): Consult surgery and/or interventional radiology.
- Provide further management of PID, including partner screening and expedited partner therapy.
Start antibiotic therapy as soon as the diagnosis is suspected and complete treatment even if infectious testing comes back negative. Undertreating or missing PID can result in long-term infertility. [9]
IUDs only substantially increase the risk of PID in the first 3 weeks after placement. Do not remove an IUD in a patient diagnosed with PID unless there is inadequate improvement after 48–72 hours. [9]
Empiric antibiotic therapy for PID
Inpatient management [9][13]
-
Initiate prompt empiric parenteral antibiotics.
- Preferred: cephalosporin (cefotetan or cefoxitin) plus doxycycline
- Add metronidazole if a cephalosporin other than cefotetan or cefoxitin is used.
- After 24–48 hours of improvement, switch to an appropriate oral antibiotic regimen prior to discharge (e.g., doxycycline plus metronidazole).
- Arrange prompt follow-up.
| Inpatient antibiotic therapy for pelvic inflammatory disease [9] | ||
|---|---|---|
| Initial antibiotics | Transition to oral antibiotics | |
| Preferred |
|
|
| Alternatives (e.g., for patients allergic to penicillin and/or cephalosporin) [13] |
|
|
|
|
|
Outpatient management [9]
- If there are no indications for inpatient management, most patients can receive outpatient treatment with the following:
-
A single dose of either of the following:
- IM ceftriaxone
- IM cefoxitin PLUS oral probenecid
- Followed by 14 days of oral doxycycline PLUS metronidazole
-
A single dose of either of the following:
- Patients with cephalosporin allergy: Consult gynecology or infectious disease.
Quinolones are no longer recommended for first-line treatment of PID because of the emergence of quinolone-resistant gonorrhea strains. [9]
Further management of PID [9][13]
- Sexual partners of the patient within the 60 days prior to the onset of symptoms: Test and presumptively treat for chlamydia and gonorrhea.
- Instruct the patient not to engage in sexual intercourse until the patient and all sexual partners have completed treatment.
- Complete STI screening if not already performed.
- If positive for C. trachomatis or N. gonorrhoeae, repeat testing in 3 months.
- Provide patient education.
- Counseling on safe sex practices
- Counseling on contraceptive options
- Encourage regular STI screening.
Complications
Short-term complications
- Sepsis
-
Fitz-Hugh-Curtis syndrome (perihepatitis)
- Inflammation of the liver capsule
- Characterized by violin-string-like adhesions extending from the peritoneum to the liver
")
Long-term complications [14]
-
Pathophysiology: inflammation (e.g., salpingitis) →
- Tubal scarring
- Adhesions of the fallopian tubes and ovaries
- Hydrosalpinx: the accumulation of fluid in the fallopian tubes [17]
-
Manifestations
- Tubal infertility (related to loss of tubal ciliary function)
- Ectopic pregnancy
- Chronic pelvic pain
We list the most important complications. The selection is not exhaustive.
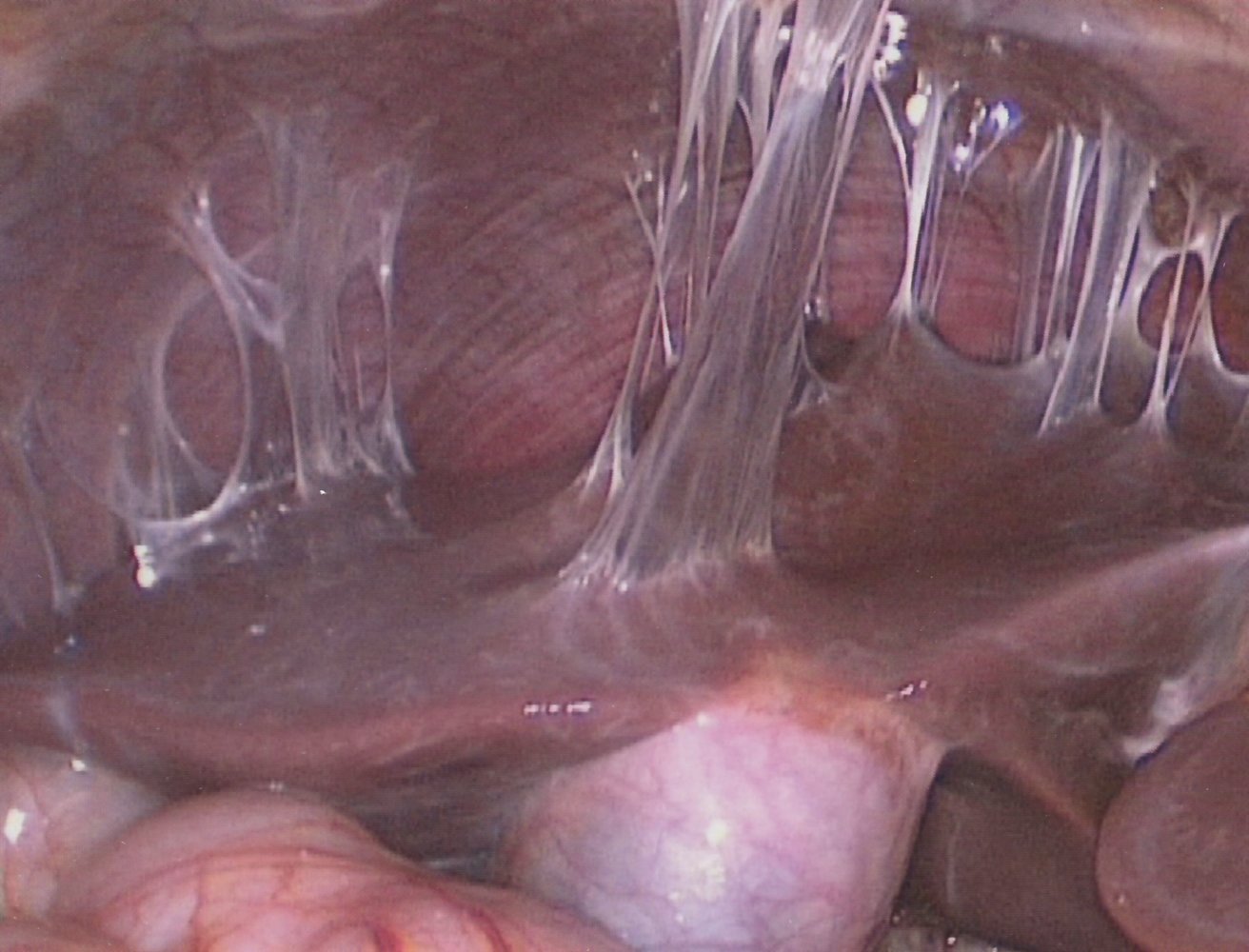
Photograph of the caudal view of the upper right peritoneum during a laparoscopy
Fibrous adhesions (green overlay) are visible between the peritoneal surface (P) and the liver (L); no other pathological findings are seen.
These adhesions are a characteristic complication of the liver capsule inflammation that occurs in Fitz-Hugh-Curtis syndrome.
Source: © IMPP
Special patient groups
Pelvic inflammatory disease in pregnancy [9][18]
- PID in pregnancy is rare; onset is typically during the first trimester. [18]
- Associated with an elevated risk of maternal morbidity, fetal loss, and preterm birth
- Begin treatment for PID with the following modifications:
- Admit all patients for inpatient management.
- Consult infectious diseases for guidance on antimicrobial choice as doxycycline is typically avoided in pregnancy. [19]
- Regimens including cephalosporins, azithromycin, and/or metronidazole may be recommended. [20]
- Pregnant individuals who test positive for chlamydia should have a test of cure for chlamydia 4 weeks after completing treatment. [9]
Avoid doxycycline when treating PID in pregnancy. Consult infectious diseases to guide antibiotic selection. [13]
Pelvic inflammatory disease in HIV [9]
- In patients with HIV, the clinical course of PID is similar to patients without HIV; tubo-ovarian abscess, however, is slightly more common.
- No modifications to regular antibiotic therapy are suggested.
Pelvic inflammatory disease in children [9][21]
-
Preadolescents
- Evaluate for child sexual abuse in all preadolescents presenting with PID.
- Refer to a child abuse specialist for diagnostic confirmation and treatment.
- See also:
- Gonorrhea in children
- Chlamydia in children
- Adolescents: Management of PID in children is the same as in adults.
PID is less common in preadolescents than in adults. [9]
External Resources
References
- "2015 Sexually Transmitted Diseases Treatment Guidelines - Pelvic Inflammatory Disease (PID)". https://web.archive.org/web/20170718205642/https://www.cdc.gov/std/tg2015/pid.htm. [2015-06-04]
- Sweet RL, Gibbs RS. "Infectious Diseases of the Female Genital Tract". Lippincott Williams & Wilkins. (2012). ISBN: 9781451148572
- Van de Wijgert JHHM, Jespers V. "The global health impact of vaginal dysbiosis". Res Microbiol. 168(9-10). :859-864. (2017)
- Gradison M. "Pelvic inflammatory disease.". Am Fam Physician. 85(8). :791-6. (2012)
- "Pelvic Inflammatory Disease (PID)". http://www.merckmanuals.com/professional/gynecology-and-obstetrics/vaginitis,-cervicitis,-and-pelvic-inflammatory-disease-pid/pelvic-inflammatory-disease-pid. [2015-01-01]
- Workowski KA, Bachmann LH, Chan PA, et al. "CDC Sexually Transmitted Infections Treatment Guidelines 2021". MMWR Recomm Rep. 70(4). :1-187. (2021)
- Curry A, Williams T, Penny ML. "Pelvic Inflammatory Disease: Diagnosis, Management, and Prevention.". Am Fam Physician. 100(6). :357-364. (2019)
- Mitchell C, Prabhu M. "Pelvic inflammatory disease: current concepts in pathogenesis, diagnosis and treatment.". Infect Dis Clin North Am. 27(4). :793-809. (2013)
- "ACR Appropriateness Criteria ®: Acute Pelvic Pain in the Reproductive Age Group (Revised 2023)". https://web.archive.org/web/20240130125832/https://acsearch.acr.org/docs/69503/Narrative. [2023-09-29]
- Revzin MV, Moshiri M, Katz DS, et al. "Imaging Evaluation of Fallopian Tubes and Related Disease: A Primer for Radiologists". Radiographics. 40(5). :1473-1501. (2020)
- Revzin MV, Mathur M, Dave HB, Macer ML, Spektor M. "Pelvic Inflammatory Disease: Multimodality Imaging Approach with Clinical-Pathologic Correlation". Radiographics. 36(5). :1579-1596. (2016)
- "Pelvic Inflammatory Disease (PID) Statistics". https://web.archive.org/web/20170506145751/https://www.cdc.gov/std/pid/stats.htm. [2017-01-27]
- "Pelvic Inflammatory Disease (PID)". https://www.acog.org/patient-resources/faqs/gynecologic-problems/pelvic-inflammatory-disease
- Bridwell RE, Carius BM, Long B, Oliver JJ, Schmitz G. "Sepsis in Pregnancy: Recognition and Resuscitation.". West J Emerg Med. 20(5). :822-832. (2019)
- Cross R, Ling C, Day NP, McGready R, Paris DH. "Revisiting doxycycline in pregnancy and early childhood--time to rebuild its reputation?". Expert Opin Drug Saf. 15(3). :367-82. (2016)
- Ortiz LN, Wyncott D, Battjes E. "What is the best treatment for PID in a pregnant woman?". Evidence-Based Practice. 17(10). :E1-E2. (2014)
- Committee on Infectious Disease, American Academy of Pediatrics. "Red Book: 2024-2027 Report of the Committee on Infectious Diseases, 33rd Edition". American Academy of Pediatrics. (2024). ISBN: 9781610027373
- Lachiewicz MP, Moulton LJ, Jaiyeoba O. "Pelvic surgical site infections in gynecologic surgery.". Infect Dis Obstet Gynecol. 2015. :614950. (2015)
- Munro K, Gharaibeh A, Nagabushanam S, Martin C. "Diagnosis and management of tubo-ovarian abscesses". The Obstetrician & Gynaecologist. 20(1). :11-19. (2018)
- R Eskander, M Berman, L Keder. "Practice Bulletin No. 174: Evaluation and Management of Adnexal Masses (reaffirmed 2021)". Obstet Gynecol. 128(5). :e210-e226. (2016)
- Weiss CR, Bailey CR, Hohenwalter EJ, et al. "ACR Appropriateness Criteria® Radiologic Management of Infected Fluid Collections". J Am Coll Radiol. 17(5). :S265-S280. (2020)