Summary
Pelvic organ prolapse (POP) is the protrusion of the uterus, vaginal apex, or surrounding pelvic structures (e.g., bladder, rectum) into the vaginal vault due to decreased pelvic floor support. It most commonly occurs in older adults. Other risk factors include multiparity (particularly vaginal births), prior pelvic surgery, connective tissue disorders, and increased intra-abdominal pressure secondary to obesity or chronic constipation. Manifestations include a sensation of pressure in the vagina, discomfort, and/or pain. Diagnosis is made with visualization of the prolapse on examination; diagnostic studies may be indicated to assess for complications. All patients should be offered conservative management to prevent progression. Symptomatic patients may also benefit from a vaginal pessary. Surgery is indicated for patients with symptomatic prolapse who do not respond to or decline conservative management. Complications of POP include urinary or fecal retention or incontinence, abdominal and/or pelvic pain, and sexual dysfunction.
Overview
-
Definition: herniation into or descent of pelvic organs to or beyond the vaginal walls
- Partial/subtotal prolapse: The pelvic organs are only partially outside the vaginal opening.
- Total prolapse: The pelvic organs are everted and located outside of the vaginal opening.
-
Anatomical overview: The pelvic floor is supported by a continuous endopelvic fascia, which consists of:
- Uterosacral ligament complex (suspends the uterus and vaginal apex from the sacrum and lateral pelvis)
- Paravaginal attachments
- Perineal body, perineal membrane, and the perineal muscles
-
Specific sites
-
Vaginal wall prolapse
- Anterior vaginal wall prolapse: herniated anterior vaginal wall, which is often associated with a cystocele (descent of the bladder ; ) or urethrocele (descent of the urethra); can be due to weakness of the pubocervical fascia
- Posterior vaginal wall prolapse: herniated posterior vaginal wall, which is associated with a rectocele (descent of the rectum) or enterocele (herniated section of the intestines); can be due to weakness of the rectovaginal fascia
- Uterine prolapse: descent of the uterus
- Vaginal vault prolapse: descent of the apex of the vagina
- Apical compartment prolapse: herniated uterus, cervix, or vaginal vault
- Uterine procidentia: protrusion of all vaginal walls or cervix beyond the vaginal introitus
-
Vaginal wall prolapse



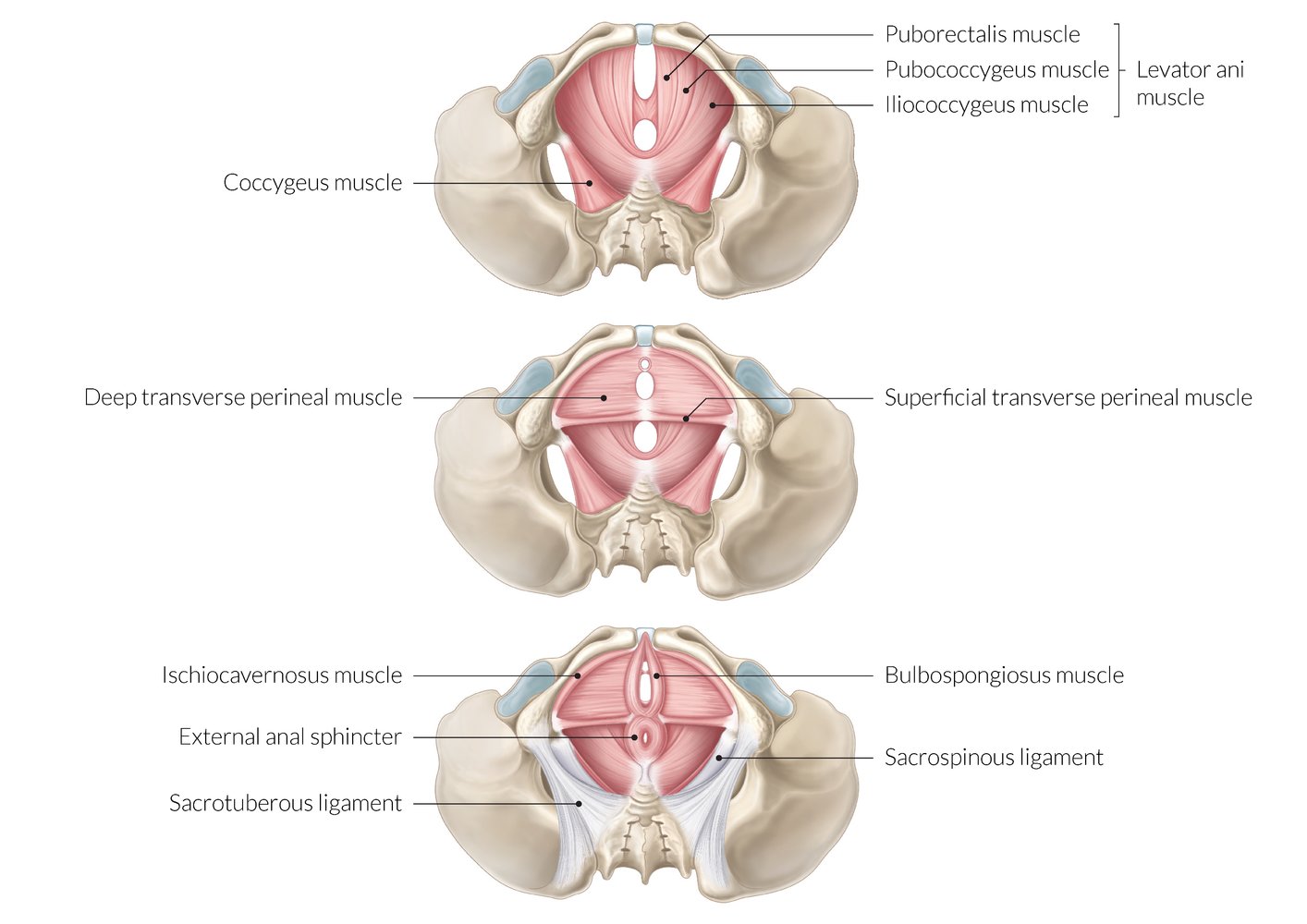
The pelvic floor is composed of three layers.
– Innermost (deep) layer: contains the pelvic diaphragm (levator ani and coccygeus)
– Middle layer: contains the urogenital diaphragm (the deep transverse perineal muscle)
– Outermost (superficial) layer: contains the external anal sphincter and the superficial transverse perineal, ischiocavernosus, and bulbospongiosus muscles
The pelvic floor has two openings: the anterior urogenital hiatus (through which the urethra and vagina pass) and the posterior rectal hiatus (through which the rectum passes).
© AMBOSS
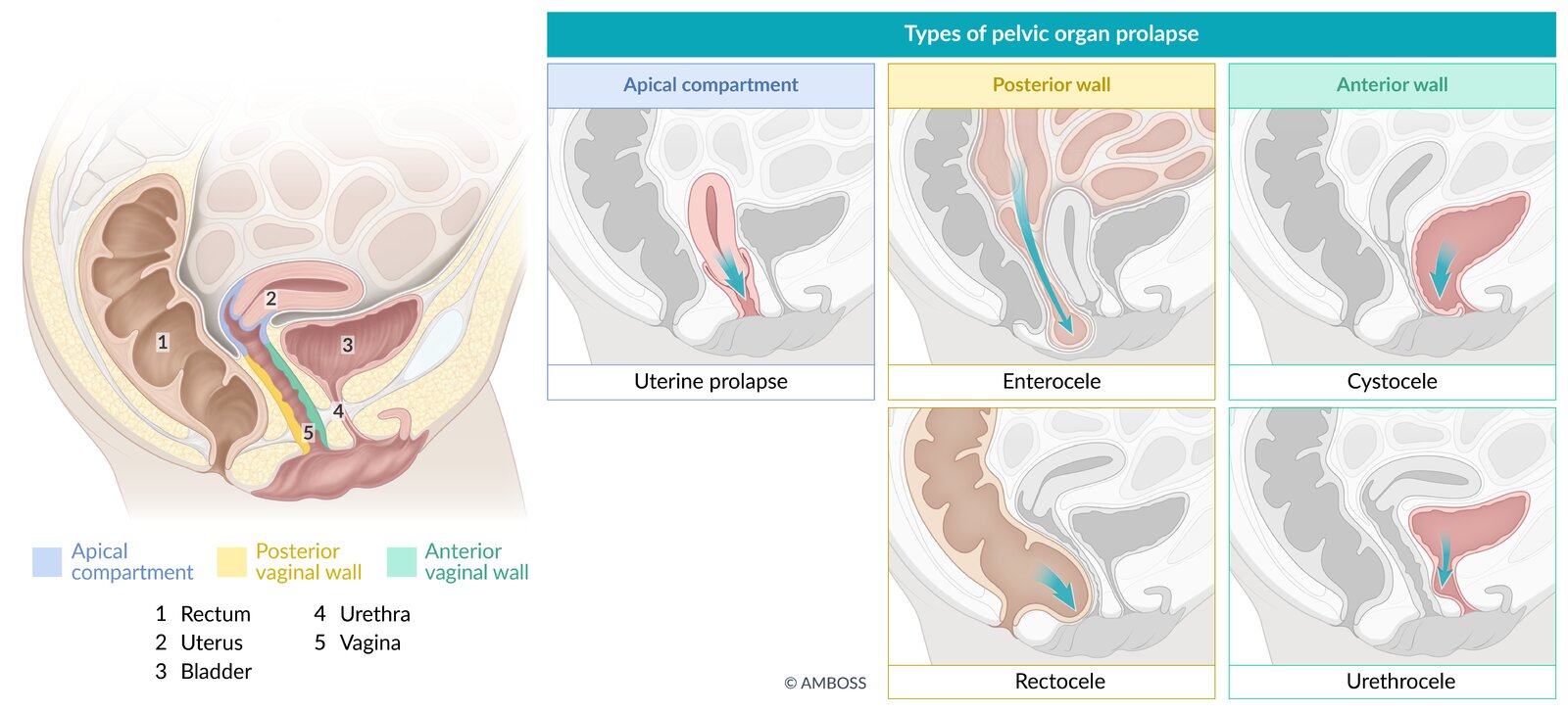
Apical compartment prolapse (uterine prolapse, vaginal vault prolapse): herniated vaginal apex (uterus and cervix, cervix alone, or vaginal vault) into the lower vagina, hymen, or beyond the vaginal introitus
Posterior compartment prolapse: herniated posterior vaginal segment, often associated with rectocele (descent of the rectum) or enterocele (herniated section of the intestines)
Anterior compartment prolapse: herniated anterior vaginal wall, which is often associated with a cystocele (descent of the bladder) or urethrocele (descent of the urethra)
© AMBOSS
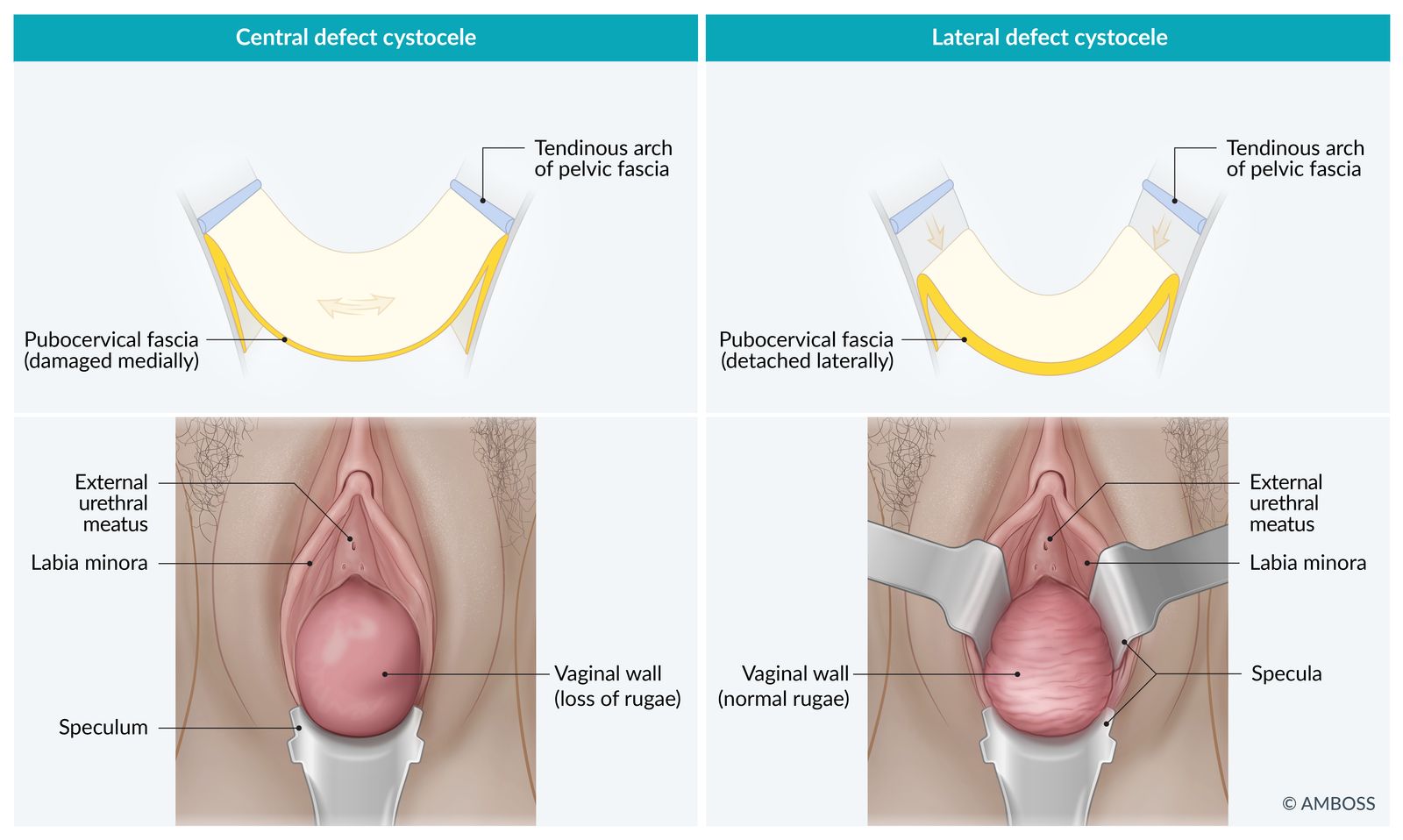
Schematic representation of the two forms of cystocele
Left: pulsation cystocele
Characterized by the bulging and thinning of the pubocervical fascia (median defect); the rugae (folds) are stretched and flattened
Right: traction cystocele
Involves a tear of the pubocervical fascia from the arcus tendineus fasciae pelvis (lateral defect); the rugae are preserved and remain intact
© AMBOSS
Epidemiology
- POP is a common disorder in older women. [1]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Etiology: : insufficiency of the pelvic floor muscles and the ligamentous supportive structure of the uterus and vagina (low-tone pelvic floor dysfunction)
-
Risk factors [2]
- Older age
- Multiple vaginal deliveries and/or traumatic births (greatest risk factor)
- Low estrogen levels (e.g., during menopause)
- Increased intra-abdominal pressure (due to, e.g., obesity; , cough related to chronic lung disease and/or smoking, ascites, pelvic tumors, constipation)
- Previous pelvic surgery (e.g., hysterectomy)
- Connective tissue disorders (e.g., Ehlers-Danlos syndrome)
- Diabetes mellitus
Clinical features
- Feeling of pressure on or discomfort around the perineum (“sensation of vaginal fullness”) [2]
- Lower back and pelvic pain (may become worse with prolonged standing or walking)
- Rectal fullness, constipation, incomplete rectal emptying
-
Prolapse of the anterior (most common) or the posterior vaginal wall
- Occurs at rest and with increased abdominal pressure
- Possibly with excessive vaginal discharge on inspection, bimanual examination, and speculum examination of the patient in lithotomy position
- Weakened pelvic floor muscle and anal sphincter tone
- Urinary symptoms (e.g., stress incontinence, overactive bladder, urinary retention) [2]
- Sexual dysfunction (e.g., dyspareunia) [3]
In addition to clinical features of POP, patients may also present with features associated with pelvic floor dysfunction (e.g., bowel or urinary symptoms, dyspareunia, pelvic pain).
Diagnosis
Pelvic organ prolapse is a clinical diagnosis.
Approach [2][4]
- Determine the location and severity of prolapse through clinical examination.
- Assess the impact of symptoms on daily life using a validated symptom questionnaire. [4]
- Evaluate associated symptoms if present.
- Refer patients with atypical or complex symptoms to a specialist for imaging. [5]
Pelvic examination for pelvic organ prolapse [2][3]
- Examine the external genitalia and perineum for skin irritation and/or breakdown.
- Assess for POP at rest and during the Valsalva maneuver.
- Perform a speculum examination to: [3]
- Individually examine the anterior and posterior vaginal walls for prolapse during the Valsalva maneuver.
- Measure vaginal length
- Perform a vaginal examination of the pelvic floor musculature. [6]
Staging of pelvic organ prolapse[3]
POP are staged with the patient maximally straining, using the Pelvic Organ Prolapse Quantification system.
- Stage 0: no prolapse
- Stage 1: The most distal portion of prolapse is > 1 cm above the level of the hymen.
- Stage 2: The most distal portion of prolapse is ≤ 1 cm proximal or distal to the hymenal plane.
- Stage 3: The most distal portion of prolapse is > 1 cm below the hymenal plane but no more than 2 cm less than the vaginal length.
- Stage 4: The vagina is completely everted or uterine procidentia has occurred.



Assessment of associated symptoms [4]
- Urinary symptoms: Studies are chosen based on clinical features.
- Postvoid residual volume: for patients with urinary retention
- Urinalysis: if there is concern for infection
- Urodynamic testing: for patients with incontinence
- See also “Initial evaluation for urinary incontinence.”
- Bowel symptoms
- Perform a digital rectal examination, including assessment of anal tone and sensation.
- Consider defecography (fluoroscopic or MR).
- See also “Diagnostics for fecal incontinence.”

The cervix can be seen visibly protruding out of the vaginal introitus of this older postmenopausal patient. Note that the labia are thin and atrophic, a normal postmenopausal change.
Source: "Uterine_prolapse", Mikael Häggström, Wikimedia Commons licensed under Public Domain
{kind=link}
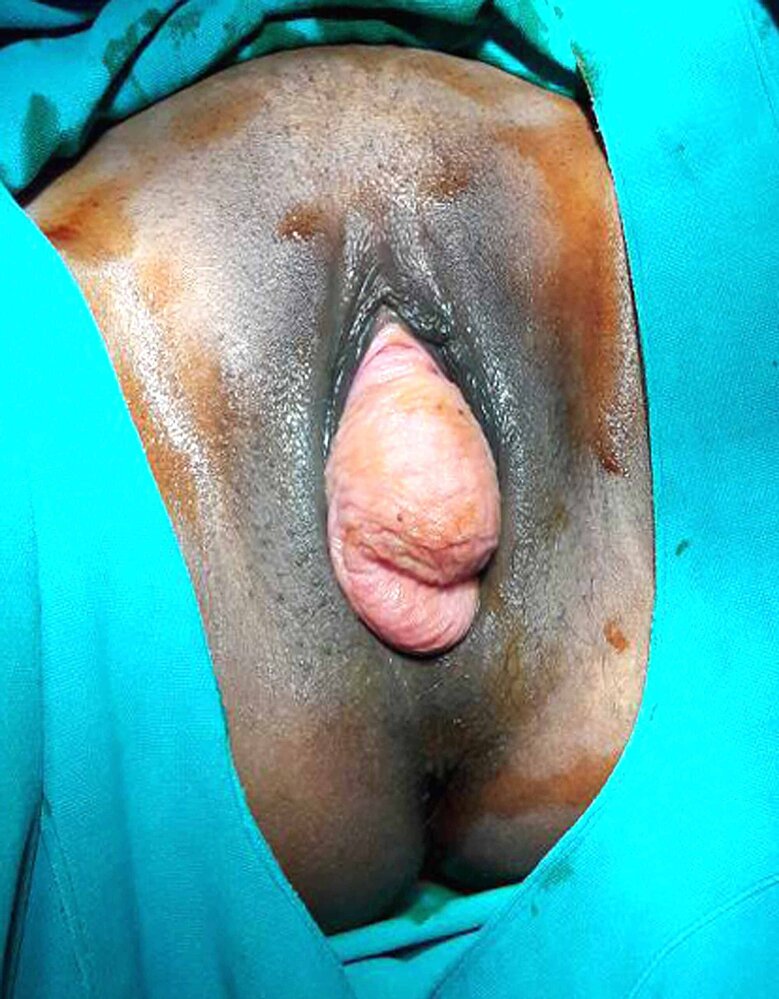
The cervix is protruding from the vaginal introitus.
Source: “Fig 1, In: Successful Pregnancy Outcome After Laparoscopic Sacrohysteropexy for Pelvic Organ Prolapse” by Samantray SR, Mohapatra I, Cureus, licensed under CC BY 4.0.

The vagina is everted and the uterus has completely prolapsed. The cervix is visible at the lower edge of the image.
Source: “Fig 1, In: Anatomical and functional outcomes after hysterectomy and bilateral sacrospinous ligament fixation for stage IV uterovaginal prolapse: a prospective case series” by Kavvadias T, Schoenfisch B, Brucker SY, Reisenauer C, BMC Urology, licensed under CC BY 4.0.
Differential diagnoses
Elongation of the cervix
- An elongated cervix can be mistaken for a prolapse.
- Evaluated during pelvic examination
Urethral diverticulum [7]
- Definition: a distinct outpouching of the urethral mucosa most often located posterolaterally in the mid and distal two-thirds of the urethra
-
Epidemiology
- Rare
- Most commonly occurs in women (20–60 years of age)
-
Etiology
-
Acquired (most common)
- Recurrent infection of the periurethral glands
- Pelvic trauma (particularly involving the vagina, bladder, or urethra)
- Gynecological surgery, periurethral procedures
- Vaginal delivery
- Congenital
-
Acquired (most common)
-
Clinical features
- Dysuria
- Dyspareunia
- Urinary incontinence (particularly, postvoid dribbling of urine)
- Tender anterior vaginal wall mass during pelvic examination
-
Diagnostics
- MRI
- Transvaginal ultrasound if MRI is not available/feasible
- Urinalysis to evaluate for other conditions (e.g., urinary tract infection or malignancy)
-
Differential diagnosis
-
Skene duct cyst
- A retention cyst that results from obstruction, accumulation of fluid, and cystic dilation of the ducts that drain the paraurethral glands.
- Manifests with dysuria, dyspareunia, and urinary overflow incontinence.
- Pelvic examination typically shows masses located just lateral to the external urethral meatus.
-
Skene duct cyst
-
Treatment
-
Conservative management
- Indicated for individuals with minor symptoms
- Manual compression of the suburethral mass after voiding
-
Surgery
- Indicated for individuals with persistent symptoms, urinary calculi in the diverticulum, or suspicion of malignancy
- Transvaginal diverticulectomy: is a preferred procedure
-
Conservative management
The differential diagnoses listed here are not exhaustive.
Management
Approach [2][3]
- Management of POP depends on the stage and patient preference.
- Offer conservative management to all patients to prevent progression and reduce symptoms.
- Asymptomatic patients: regular review to monitor progression
-
Symptomatic patients: Refer to a specialist for further management.
- Vaginal pessary (preferred)
- Surgery (alternative)
POP can cause urethral obstruction; advise patients that treatment may relieve the obstruction, unmasking stress urinary incontinence. [4]
Conservative management [2]
-
Lifestyle modifications to address risk factors and associated symptoms, e.g.:
- Smoking cessation
- Weight management, if indicated
- Treatment of constipation
- Avoidance of heavy lifting
- Pelvic floor muscle training (e.g., Kegel exercises) [2]
Vaginal pessary [2][3]
- A silicone or latex device that is inserted into the vagina to provide support for pelvic organs
- Available in many shapes and sizes, selected based on symptoms and stage of POP [2][3]
- Must be fitted by an appropriately trained clinician [8]
-
Requires regular cleaning to prevent complications (e.g., pressure ulcers and erosions into the bladder and/or rectum) [2][8]
- Patients able to clean the pessary: Follow up annually.
- Patients unable to clean the pessary: Follow up every 3 months.
Bacterial vaginosis occurs in one-third of patients who use a pessary. [2]
Pessaries may not be suitable for patients with dementia, chronic pelvic pain, or barriers to follow-up. [2]
Surgery [3]
- Indications for surgical referral include symptomatic prolapse in patients who do not respond to or do not want conservative management.
- Choice of surgical approach depends on factors such as:
- Location and severity of prolapse
- Associated symptoms
- Patient condition and preferences
Techniques
- Vaginal hysterectomy, with vaginal apex suspension and repair of anterior and posterior vaginal wall prolapse as necessary
- For patients wishing to avoid hysterectomy:
- Uterine suspension with hysteropexy
-
Colpocleisis
- Surgical narrowing or closure of the vagina
- Can be considered for individuals who no longer wish to have vaginal sexual intercourse
Repair with synthetic mesh and/or grafting is no longer recommended for most individuals with POP because of the high risk of complications. [3]
Urethropexy may be performed at the same time as POP surgery to prevent postoperative stress incontinence. [9]
Complications
Urinary disorders [10]
- Stress incontinence
- "Masked" urinary incontinence
- Obstructive uropathy
Defecation disorders
- Fecal incontinence
- Dyssynergic defecation
Other complications
- Pressure ulcers with hemorrhage
- Ascending infections (e.g., cystitis, pyelonephritis, vaginal and cervical infections, endometritis, salpingitis/adnexitis)
- Pelvic pain
- Sexual dysfunction
- Surgical complications (e.g., recurrence)
We list the most important complications. The selection is not exhaustive.
External Resources
- 2023 AUGS-SUNA Joint Clinical Consensus Statement: Vaginal Pessary Use and Management
- 2022 ACR Appropriateness Criteria®: Pelvic Floor Dysfunction in Females
- 2019(reaffirmed 2024) ACOG Practice Bulletin Nr. 214: Pelvic Organ Prolapse
- 2017 (reaffirmed 2020) AUGS Best Practice Statement: Evaluation and Counseling of Patients With Pelvic Organ Prolapse
References
- Dunivan GC, Anger JT, Alas A, et al. "Pelvic Organ Prolapse". Female Pelvic Med Reconstr Surg. 20(6). :322-327. (2014)
- Iglesia CB, Smithling KR. "Pelvic Organ Prolapse". Am Fam Physician. 96(3). :179-185. (2017)
- Committee on Practice Bulletins—Gynecology and the American Urogynecologic Society. "Pelvic Organ Prolapse". Obstetrics & Gynecology. 134(5). :e126-e142. (2019)
- American Urogynecologic Society. "AUGS Best Practice Statement: Evaluation and Counseling of Patients With Pelvic Organ Prolapse". Female Pelvic Med Reconstr Surg. 23(5). :281-287. (2017)
- Khatri G, Bhosale PR, Robbins JB, et al. "ACR Appropriateness Criteria® Pelvic Floor Dysfunction in Females". J Am Coll Radiol. 19(5). :S137-S155. (2022)
- Harm-Ernandes I, Boyle V, Hartmann D, et al. "Assessment of the Pelvic Floor and Associated Musculoskeletal System: Guide for Medical Practitioners". Female Pelvic Med Reconstr Surg. 27(12). :711-718. (2021)
- Vaidya RV, Olson K, Wolter C, Khan A. "Characterization of Urethral Diverticula in Women". Female Pelvic Med Reconstr Surg. 28(1). :54-56. (2021)
- Jundt K, Wagner S, von Bodungen V, Friese K, Peschers U. "Occult incontinence in women with pelvic organ prolapse - does it matter?". Eur J Med Res. 15(3). :112. (2010)
- American Urogynecologic Society. "AUGS-SUNA Joint Clinical Consensus Statement: Vaginal Pessary Use and Management for Pelvic Organ Prolapse". Urogynecology. 29(1). :5-20. (2023)
- American College of Obstetricians and Gynecologists. "Practice Bulletin No. 155: Urinary Incontinence in Women (Reaffirmed 2022)". Obstet Gynecol. 126(5). :e66-e81. (2015)