Summary
Pericardial effusion is the acute or chronic accumulation of fluid in the pericardial space (between the parietal and the visceral pericardium) and is often associated with a variety of underlying disorders. The fluid can be either bloody (e.g., following aortic dissection) or serous (usually idiopathic). As the pericardium is rather stiff, the capacity of the pericardial space is limited. In chronic effusion, the pericardium can stretch to a certain degree, accommodating slightly more fluid. In the acute setting, however, the added volume quickly exceeds the maximum capacity of the pericardial space. In both cases, the end result is often cardiac tamponade: compression of the heart that can lead to a life-threatening reduction in cardiac output. Pericardial effusion is initially asymptomatic, but cardiac tamponade has a distinct clinical presentation, including hypotension, tachycardia, jugular venous congestion, and pulsus paradoxus. Echocardiography is the most important diagnostic procedure and usually reveals an anechoic pericardial space. Treatment depends on hemodynamic stability: unstable patients require quick pericardial fluid drainage, through either pericardiocentesis or surgery, whereas in stable patients, treatment focuses on the underlying disease.
Definitions
- Pericardial effusion: an accumulation of fluid in the pericardial space between the parietal and visceral pericardium. May be acute or chronic.
- Cardiac tamponade: a pathophysiological process whereby elevated intrapericardial pressure from a pericardial effusion causes compression of the heart (especially the right ventricle) [1]
Etiology
-
Hemopericardium: accumulation of blood in pericardial space
- Cardiac wall rupture (e.g., complication of myocardial infarction)
- Chest trauma (traumatic cardiac tamponade)
- Aortic dissection
- Cardiac surgery (e.g., heart valve surgery, coronary bypass surgery)
-
Serous or serosanguinous pericardial effusion [2]
- Idiopathic
- Acute pericarditis (especially viral, but also fungal, tuberculous or bacterial)
- Malignancy
- Postpericardiotomy syndrome
- Uremia
- Autoimmune disorders
- Hypothyroidism
- Right heart failure
Pathophysiology
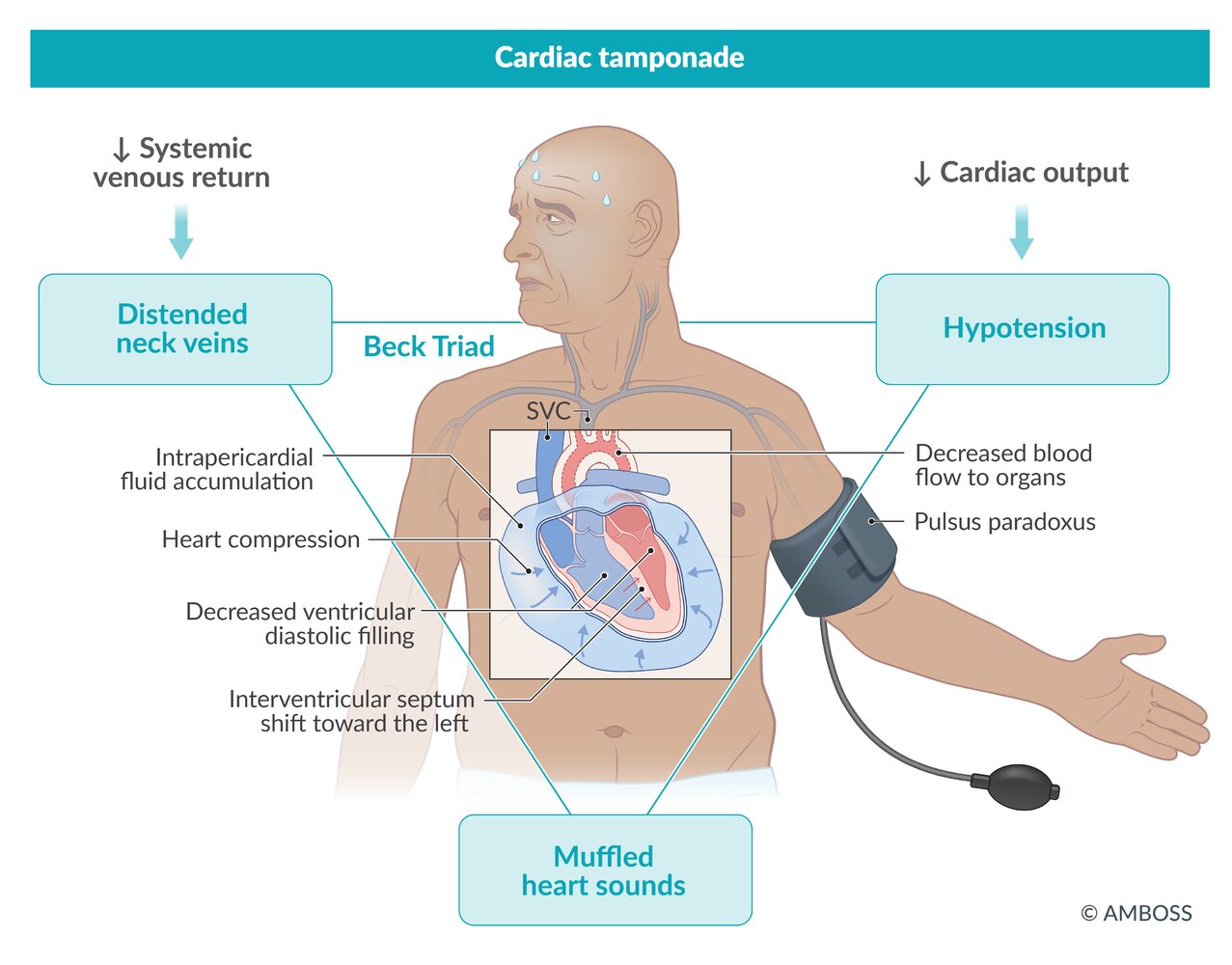
Cardiac tamponade: pericardial fluid collection (e.g., bloody or serous) → ↑ pressure in the pericardial space → compression of the heart (especially of the right ventricle due to its thinner wall) → interventricular septum shift toward the left ventricle chamber → ↓ systemic venous return (preload) → ↓ ventricular diastolic filling → ↓ stroke volume (and venous congestion) → ↓ cardiac output and equal end-diastolic pressures in all 4 chambers

© AMBOSS
Clinical features
Pericardial effusion [3]
- Initially asymptomatic in most cases
- Shortness of breath, especially when lying down (orthopnea)
- Retrosternal chest pain
- Can cause compressive symptoms
- Hoarseness
- Nausea
- Dysphagia
- Hiccups
- Apical impulse is difficult to locate or nonpalpable.
- Ewart sign: dullness to percussion at the base of the left lung with increased vocal fremitus and bronchial breathing due the compression of lung parenchyma by the pericardial effusion [4]
Tamponade [3]
-
Beck triad
- Hypotension
- Muffled heart sounds
- Distended neck veins
- Tachycardia, pulsus paradoxus
- Pallor, cold sweats
- Left ventricular failure
- Symptoms of right heart failure
- Obstructive shock, cardiac arrest (presenting as pulseless electrical activity) [1]
© AMBOSS
Diagnosis
Approach
- Unstable patients with suspected tamponade: Do not delay treatment for extensive diagnostic workup; proceed directly with management of cardiac tamponade.
- In all other patients, confirm the diagnosis with echocardiography (either TTE, FAST, or focused cardiac ultrasound).
- Laboratory studies and analysis of the pericardial fluid can be used in the investigation of the underlying etiology.
In unstable patients and those in cardiac arrest with suspected tamponade, pericardiocentesis should not be delayed for diagnostic confirmation.
Echocardiography
- Indication: diagnosis and monitoring of all patients with suspected pericardial effusion and/or tamponade [5]
- Procedure: : TTE (gold standard), FAST, or focused cardiac ultrasound (FoCUS)
-
Allows for the detection of: [6]
- Small effusions of 25–50 mL during ventricular systole
- Effusions of > 50 mL throughout the cardiac cycle
- Cardiac tamponade
-
Ultrasound findings supportive of pericardial effusion: Can be identified using POCUS (See “Subxiphoid view" of the “FAST scan.”)
-
Anechoic space between the pericardium and epicardium [7]
- < 10 mm: small effusion ∼ 300 mL
- 10–20 mm: moderate effusion ∼ 500 mL
- > 20 mm: large effusion > 700 mL
- Hemorrhagic or purulent effusions may be echogenic.
-
Anechoic space between the pericardium and epicardium [7]
-
Echocardiographic findings supportive of cardiac tamponade [7][8]
-
Chamber collapse
- Early signs: collapse of the right atrium during systole, collapse of the right ventricle during early diastole
- Later: collapse of the left atrium [7]
- Rare: collapse of the left ventricle
- Swinging motion of the heart
- Inspiration: decrease in LV filling
- Exhalation: increase in LV filling and decrease in RV filling
- Blood flow changes during inspiration
- Aortic valve and mitral valve: decrease
- Pulmonary valve and tricuspid valve: increase
- Hepatic vein and inferior vena cava plethora (See “IVC ultrasound.”)
-
Chamber collapse
Echocardiography is a quick and safe diagnostic tool for detecting pericardial effusions and pericardial tamponade.
Epicardial fat can be mistaken for pericardial fluid on echocardiography. However, unlike fluid, it tends to be brighter, moves along with the myocardium, and does not collect in dependent regions. [8]



ECG
-
Indication
- All patients with suspected pericardial effusion
- Used to rule out an ischemic cause
-
Findings in pericardial effusion
- Normal in smaller effusions
- Low voltage complexes and electrical alternans in larger effusions
-
Findings in cardiac tamponade [4]
- Sinus tachycardia
- Low voltage QRS complexes
- Electrical alternans: consecutive QRS complexes that alternate in height due to the swinging motion of the heart when surrounded by large amounts of pericardial fluid
- Pulseless electrical activity (PEA) in cardiac arrest [9]




Imaging
-
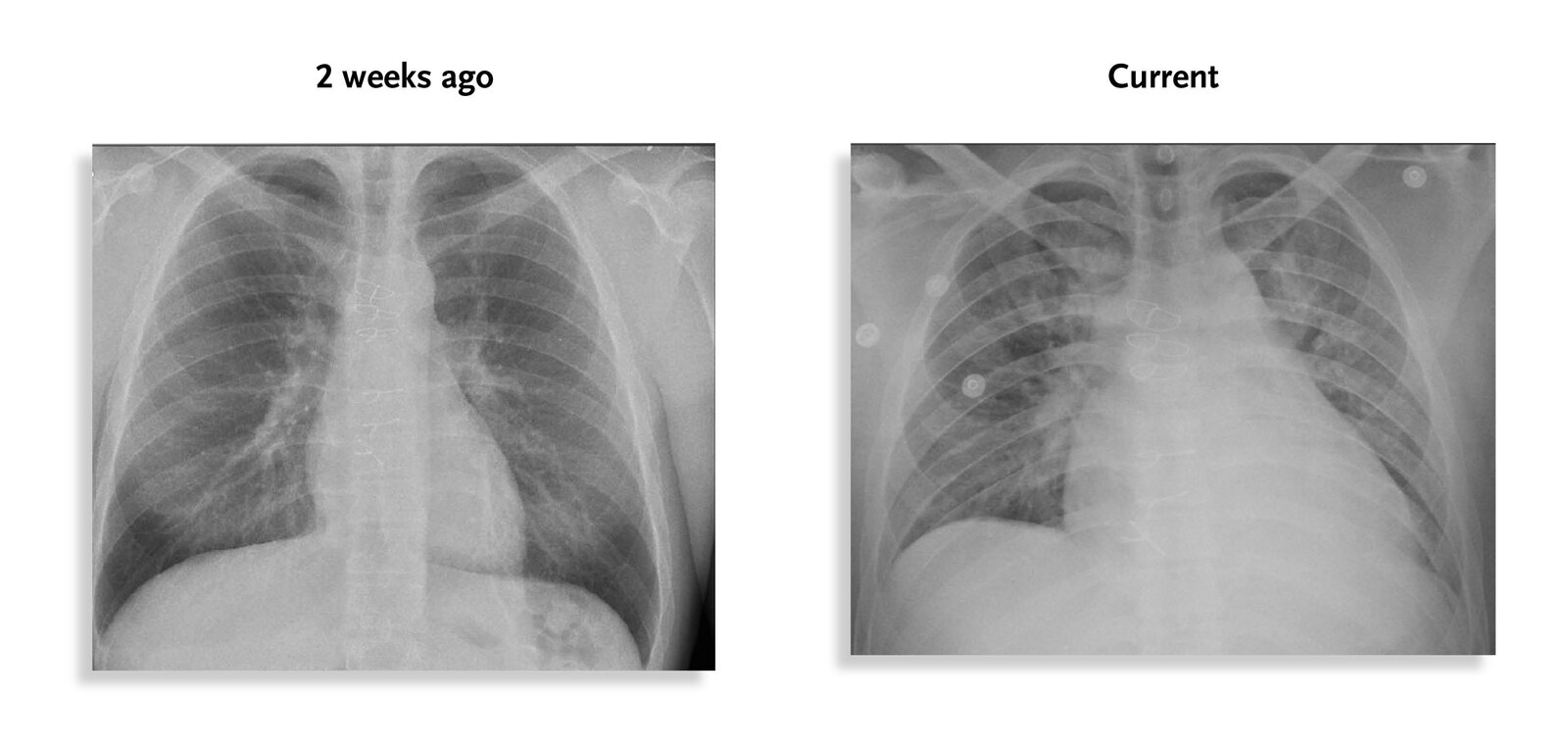
Chest x-ray: not required to diagnose pericardial effusion but often performed to exclude other causes of dyspnea [10][11]
- PA view findings
- Normal in small effusions [12]
- Enlarged cardiac silhouette and clear lungs may be seen in moderate effusions.
- Water bottle sign: the radiographic sign of a large pericardial effusion in which the cardiac silhouette resembles a bottle
-
Lateral view findings
- Posterior inferior bulge sign: a change in the silhouette of the heart due to a pericardial effusion that collects in the posterior-inferior pericardiac recess and expands the pericardium [13]
- Pericardiac fat pad sign: a > 2 mm soft-tissue stripe between the epicardiac fat and the anterior mediastinal fat that may be visible anterior to the heart [10]
- PA view findings
-
Further imaging [7]
- Indications: consider if small or loculated effusions are suspected or visualization via TTE is difficult
- Modalities include: TEE, CMR, CT
∼ 250 mL of pericardial fluid must be present before an effusion is visible on chest x-ray!







Investigation of the underlying etiology
Pericardial fluid analysis [14][15]
- Indication: pericardial effusion of unclear etiology [15]
- Procedure: Pericardial fluid is obtained via diagnostic pericardiocentesis.
-
Analysis [15]
- Cell count
- ↑ WBC in infection
- ↑ RBC in hemorrhagic effusions
- Gram stain and culture
- Cytology
- Acid-fast bacilli
- Glucose level: < 60–80 mg/dL suggestive of malignant, parapneumonic, or tuberculous effusions, or connective tissue disease.
- Protein level: > 6.0 g/dL is associated with purulent, parapneumonic, and tuberculous effusions.
- LDH: Isolated pericardial fluid LDH elevation of > 300 units/dL suggests malignant effusion.
- Cell count
-
Interpretation [14]
- There are no established biochemical thresholds for the classification of pericardial effusions.
- Light criteria can be used for interpretation.
| Interpretation of pericardial fluid samples | ||
|---|---|---|
| Fluid type | Appearance | Etiology [14] |
| Transudate |
|
|
| Exudate |
|
|
| Blood |
|
|
| Purulent [18] |
|
|
")
")
Laboratory studies and specific investigations [11]
- CBC: leukocytosis if infection or inflammation
- CRP, ESR: elevated in infection or inflammation
-
Troponin
- Can be slightly elevated in pericarditis
- Significantly elevated if there is associated myocarditis
- Creatinine kinase: elevated in myocarditis, rhabdomyolysis
- BMP: elevated BUN in uremic pericarditis
| Investigation of underlying etiology in pericardial effusion | |
|---|---|
| Suspected etiology | Additional investigations to consider |
| Acute pericarditis |
|
| Uremic pericardial effusion |
|
| Autoimmune disease |
|
| Malignancy |
|
| Hypothyroidism |
|
| Aortic dissection |
|
| Postpericardiotomy syndrome |
|
| Trauma |
|
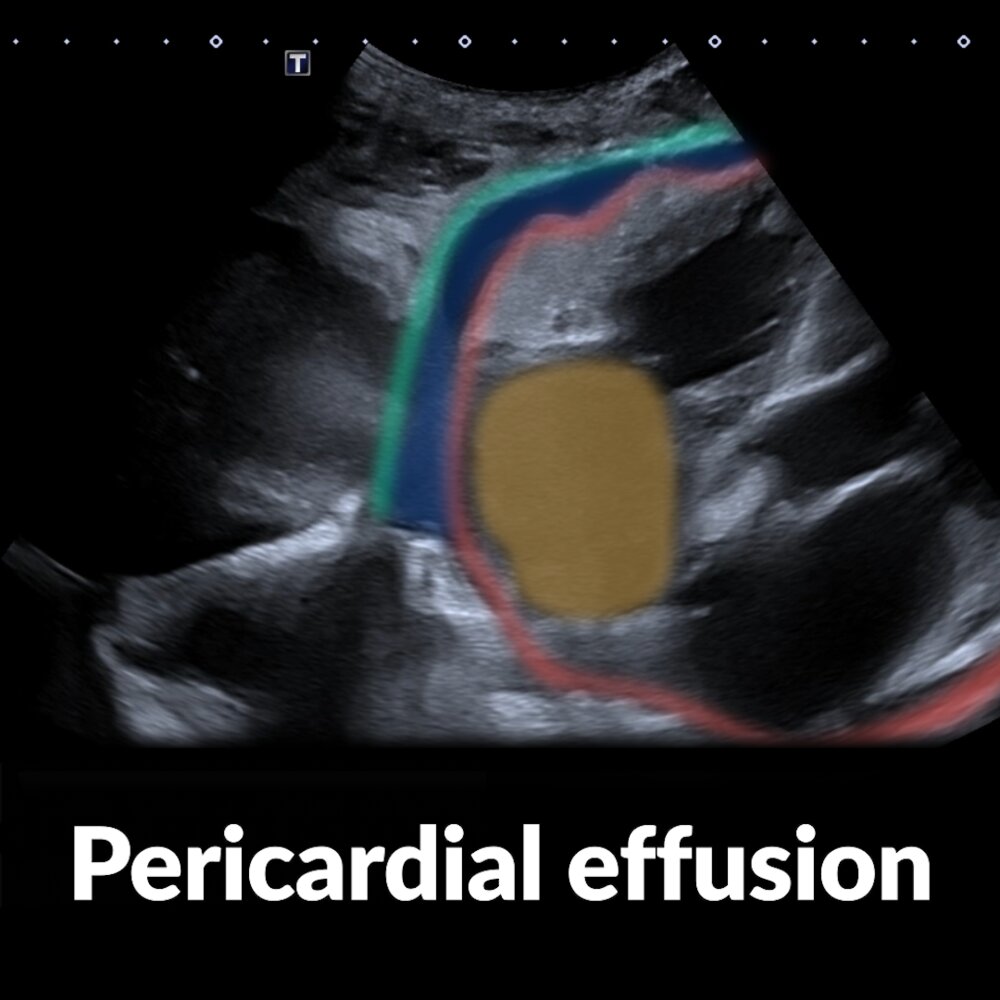
Short video of a subxiphoid ultrasound examination of the heart (a marker indicates the probe position) showing a pericardial effusion
The right atrium (yellow overlay) is seen in the center of the image. The visceral pericardium (epicardium; red line) is clearly separated from the parietal and fibrous pericardium (green line) by a hypoechoic area (blue overlay), which corresponds to a pericardial effusion.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.

Echocardiography (transthoracic; parasternal long axis)
The image was taken in ventricular diastole with the mitral valve (M) open. Anechoic pericardial effusion (green overlay) surrounds the heart.
LV: left ventricle; RV: right ventricle
Source: © IMPP
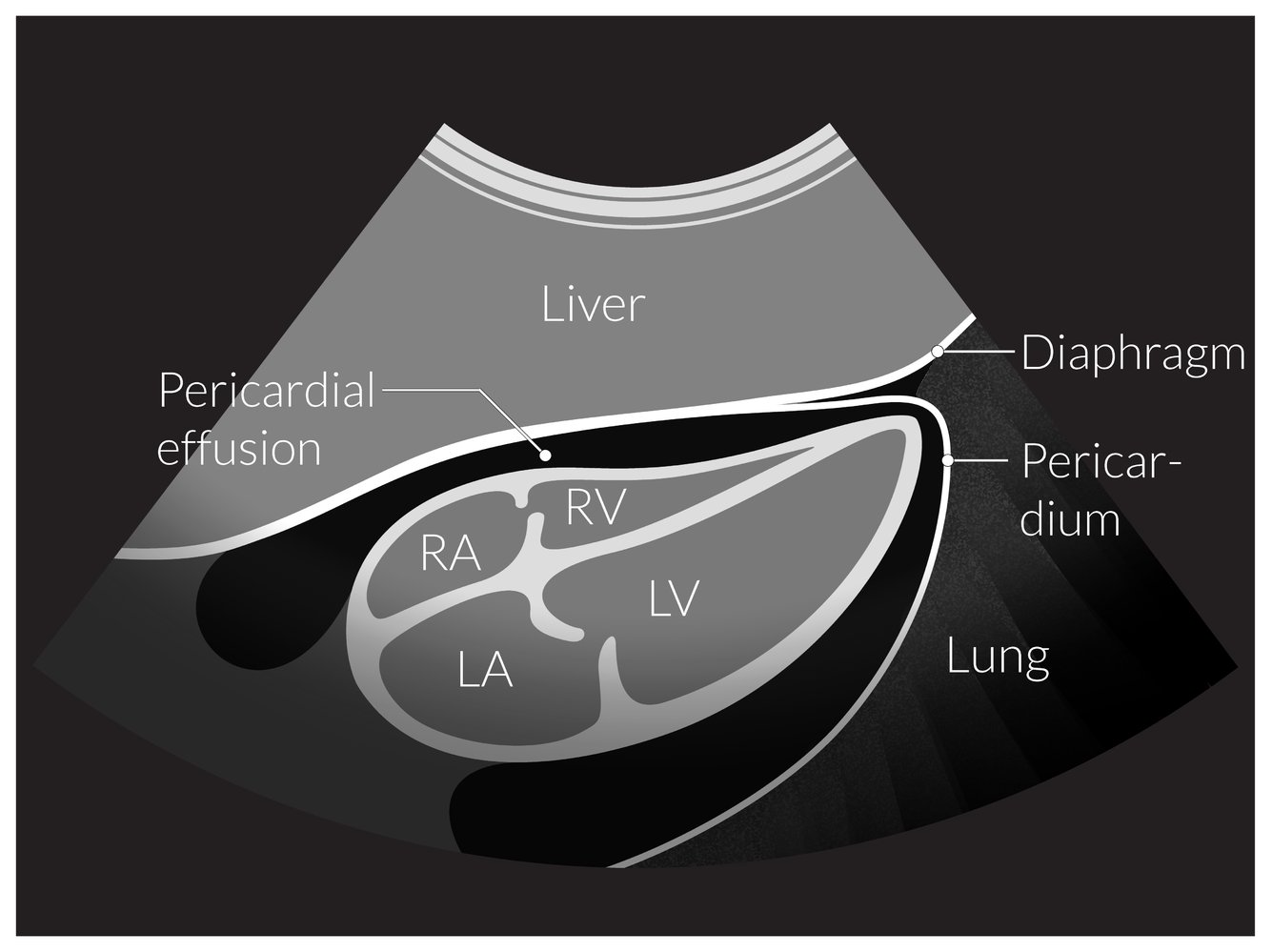
Echocardiography (schematic; subcostal view)
An anechoic (black) pericardial space indicates a pericardial effusion.
LA: left atrium; LV: left ventricle; RA: right atrium; RV: right ventricle
© AMBOSS
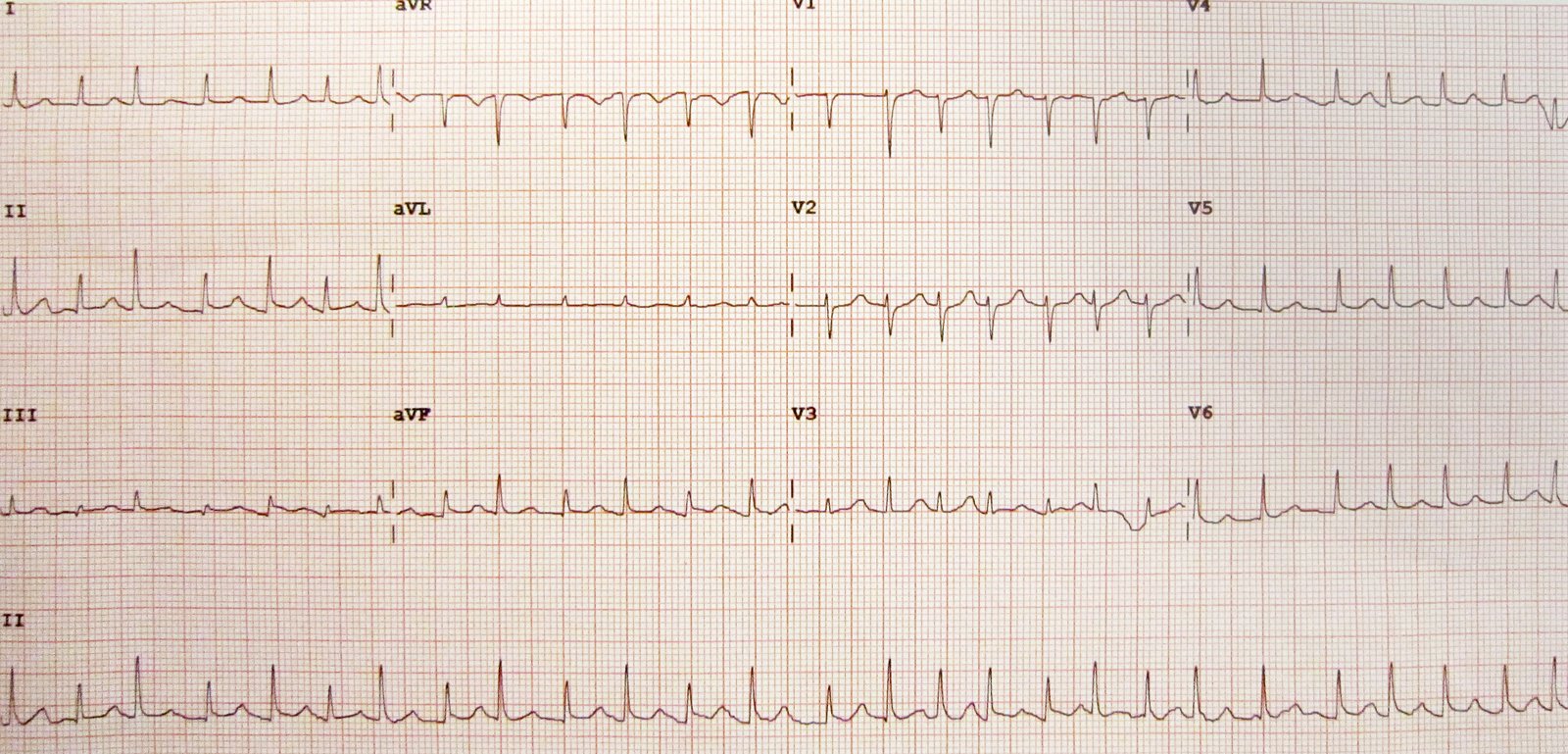
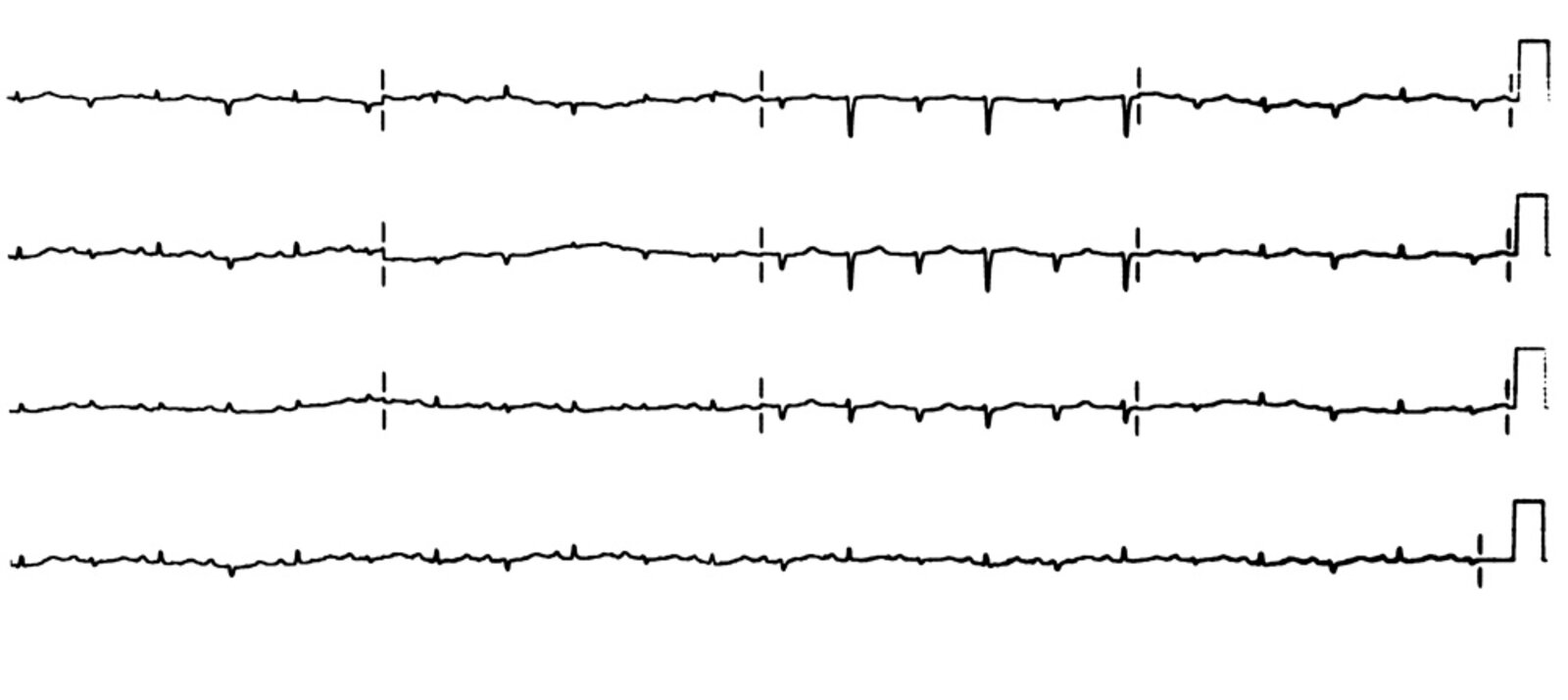
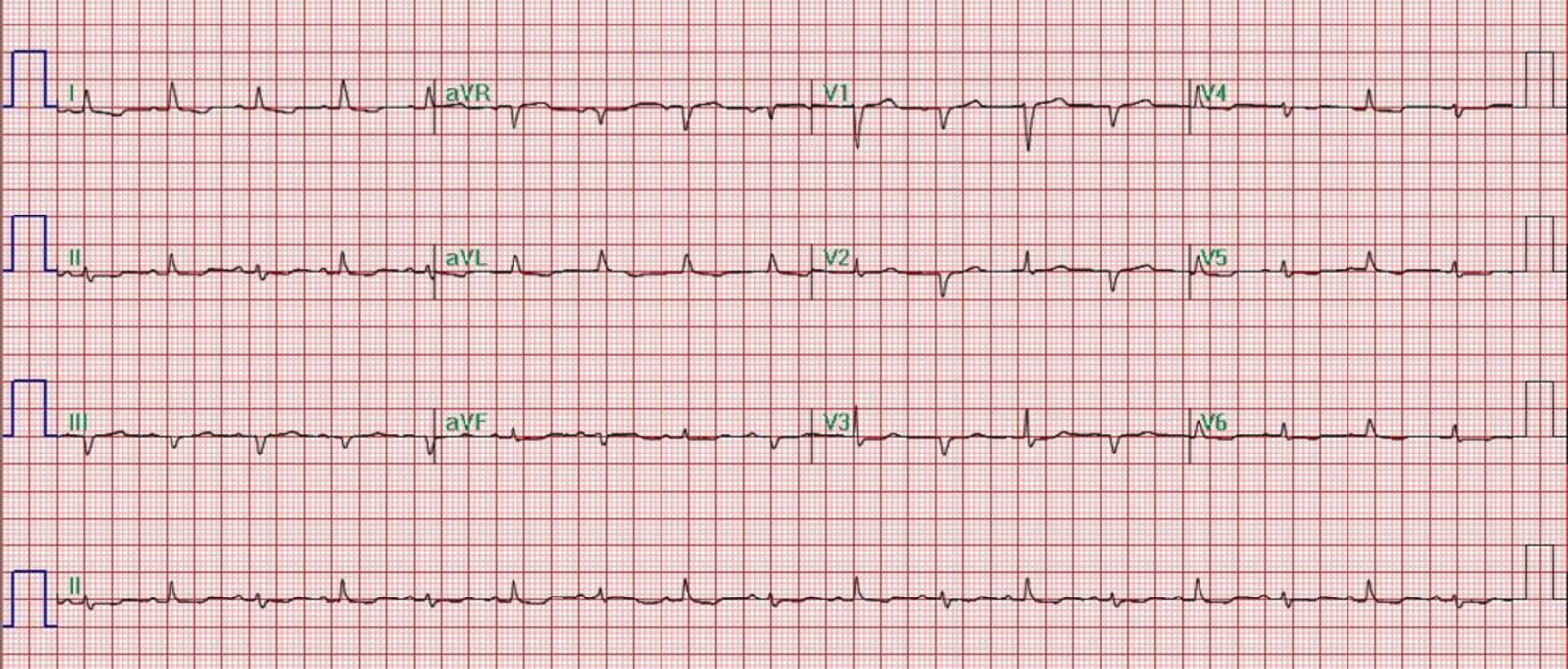
12-lead ECG (paper speed: 25 mm/s)
- Narrow-complex tachycardia with a ventricular rate of approx. 150/min
- Likely atrial fibrillation (irregular RR intervals, no definitive P waves)
- Normal cardiac axis (R > S in both I and aVF)
- QRS voltage is low, and consecutive R waves alternate in height (electrical alternans, red lines)
The combination of tachycardia, low QRS voltage, and electrical alternans is highly suggestive of a large pericardial effusion.
Source: “Electrical Alternans” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: brightened image. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
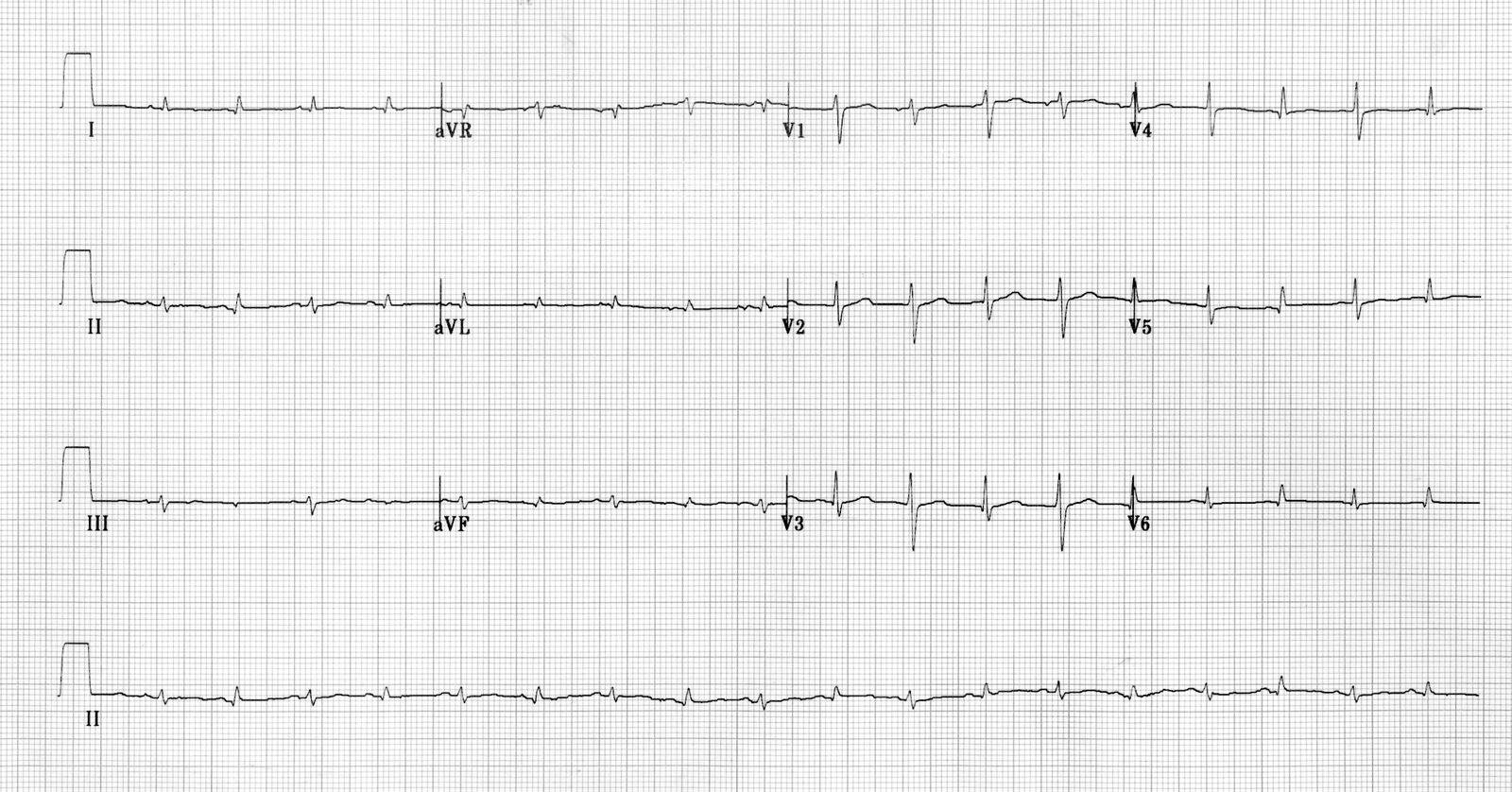
12-lead ECG (paper speed: 25 mm/s)
– Narrow-complex sinus tachycardia with a rate of ∼ 110/min
– Electrical alternans: consecutive QRS complexes alternate in height and axis (most clearly seen in V1–V3; examples indicated by red brackets)
– Low QRS voltage (most clearly seen in limb leads)
– T-wave flattening
These findings are consistent with a large pericardial effusion.
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
Electrical alternans c/w cardiac tamponade
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
Electrical alternans c/w cardiac tamponade
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
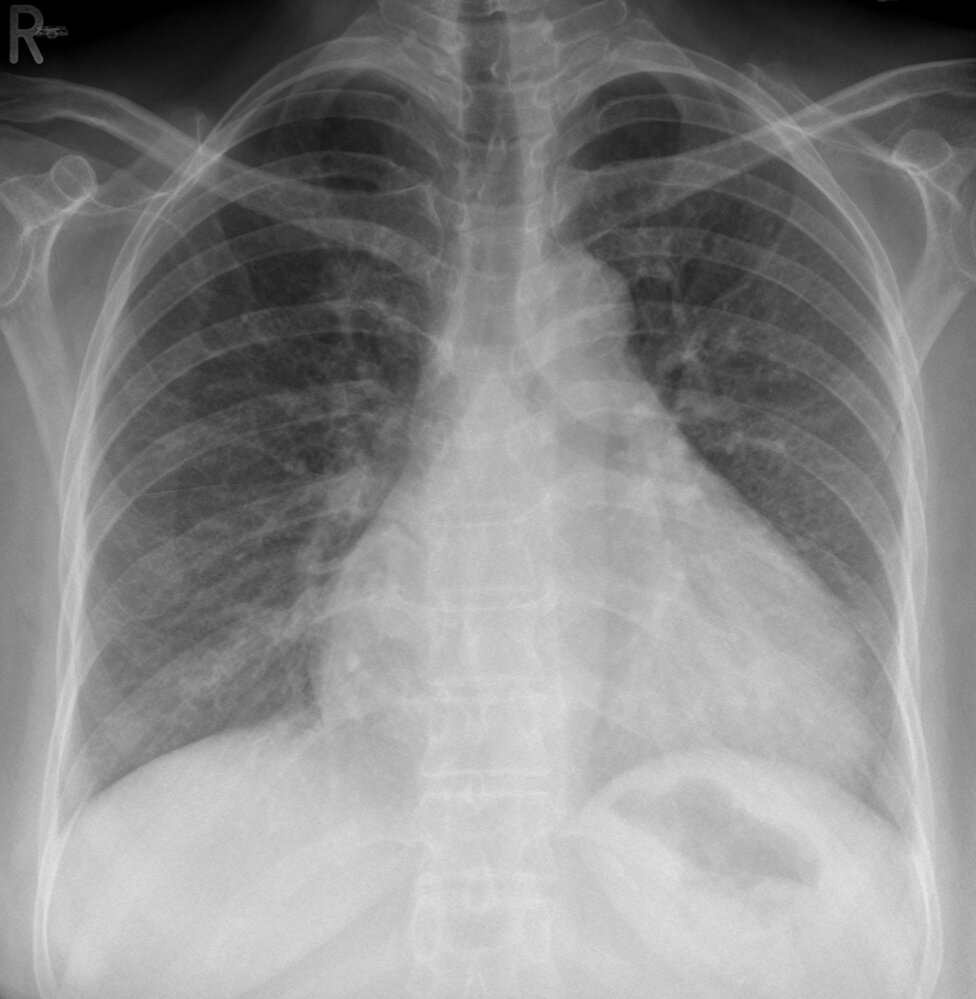
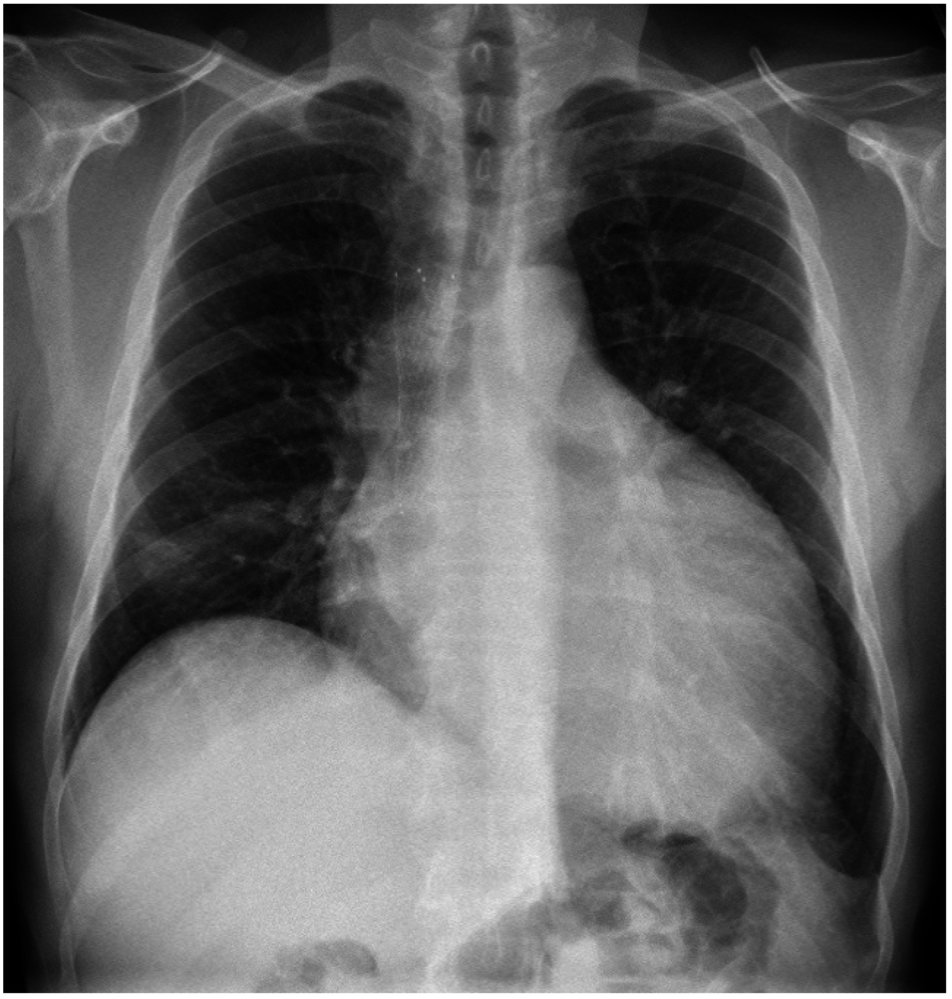
Chest X-ray (PA view) of a patient with a history of pericarditis and clinical findings of tamponade
The cardiac silhouette is enlarged (globular water bottle-shape; enlargement highlighted by green-hatched overlay) due to pericardial effusion.
Source: “28-01-Perikarderguss Perimyokarditis pa” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
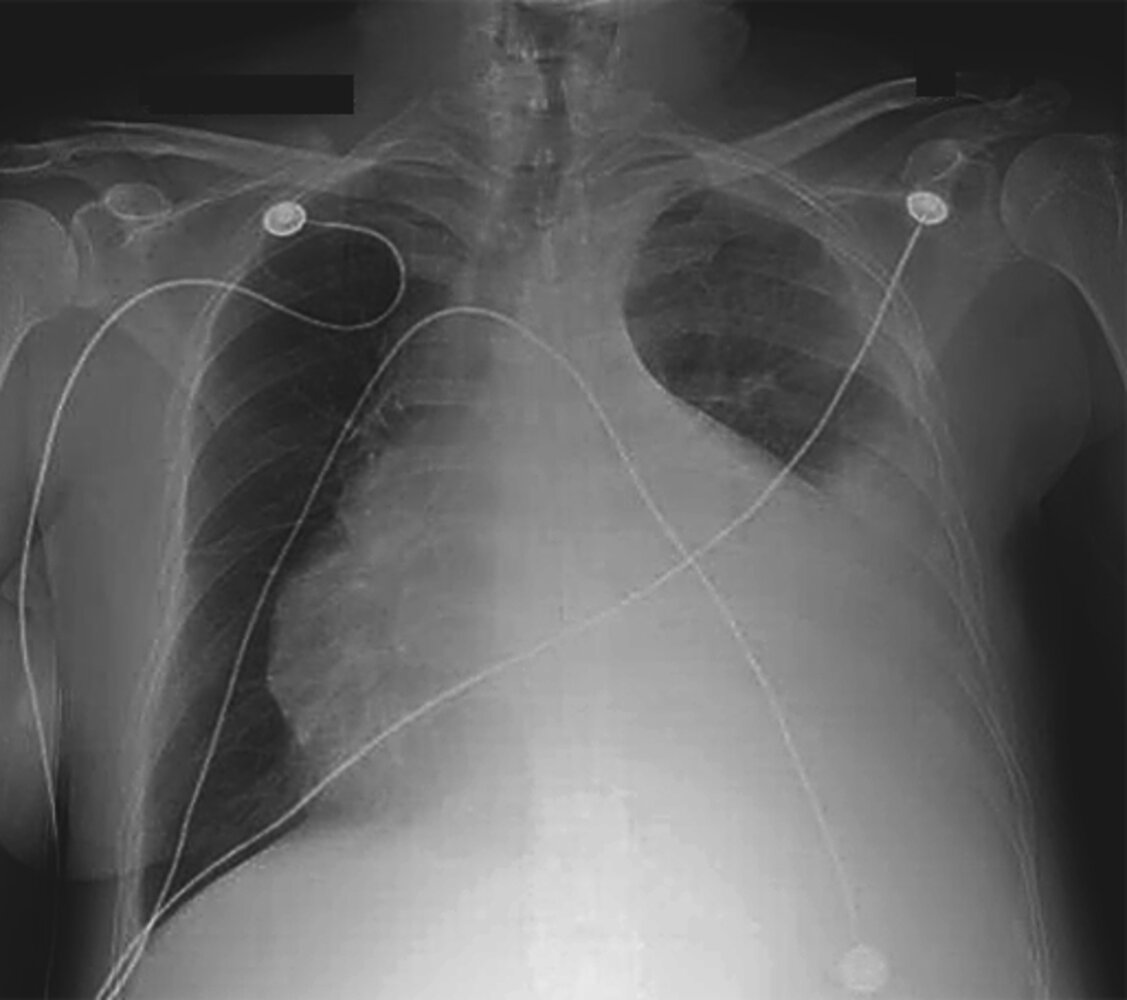
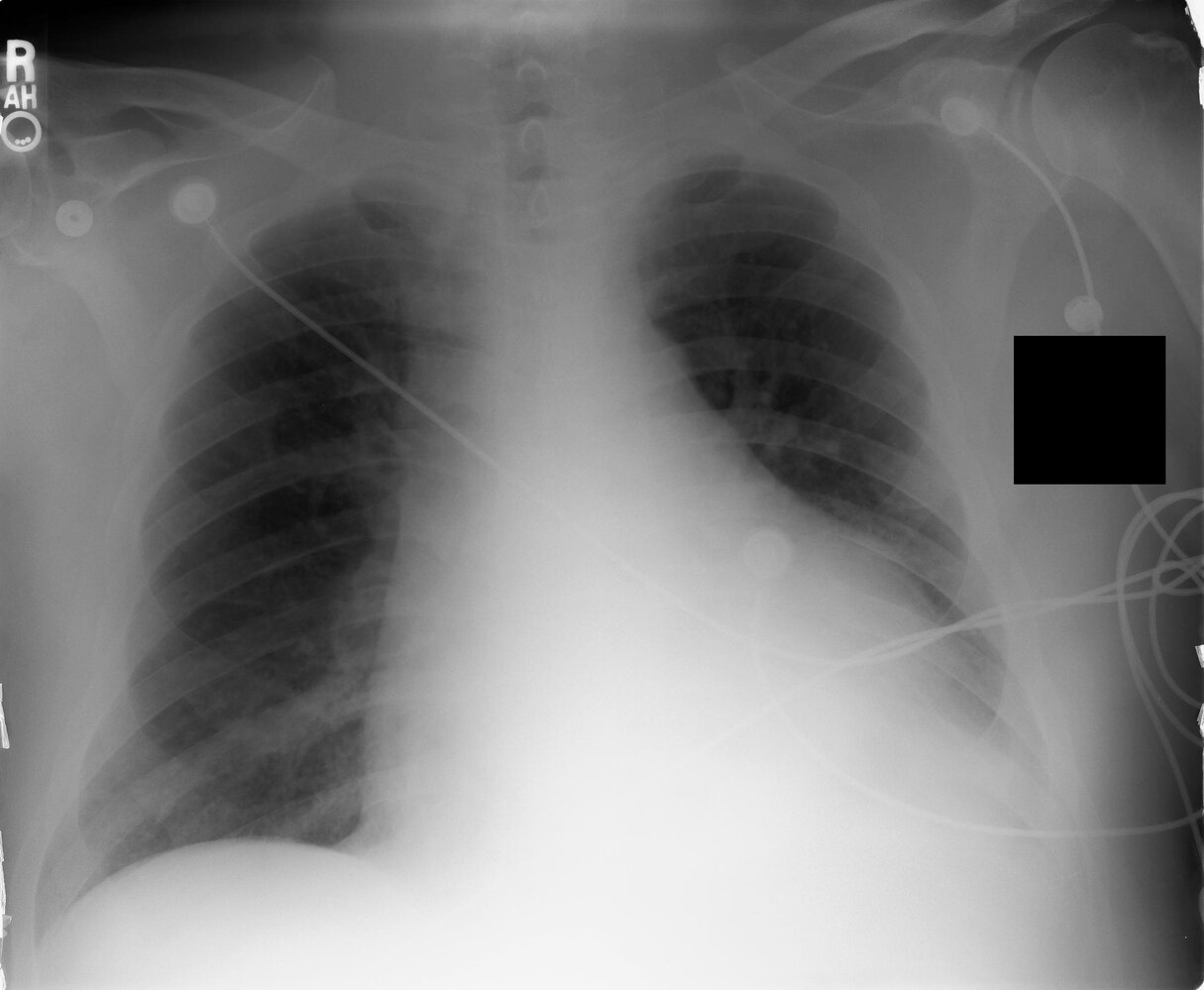
X-ray chest (PA)
There is marked enlargement of the cardiac silhouette (indicated by white arrows and white outline; normal heart shape indicated by white dashed outline). The convexity of the right mediastinum was produced by the edge of a mediastinal mass (indicated by red arrowheads), not the ascending aorta. The stent (green overlay) in the superior vena cava (SVC) was placed to relieve symptoms of extrinsic compression by the mass.
Enlargement of the cardiac silhouette was caused by malignant pericardial effusion.
Source: “Figure 3. in: Malignant Cardiac Tamponade from Non-Small Cell Lung Cancer: Case Series from the Era of Molecular Targeted Therapy” by Bob T. Li et al., Journal of Clinical Medicine, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
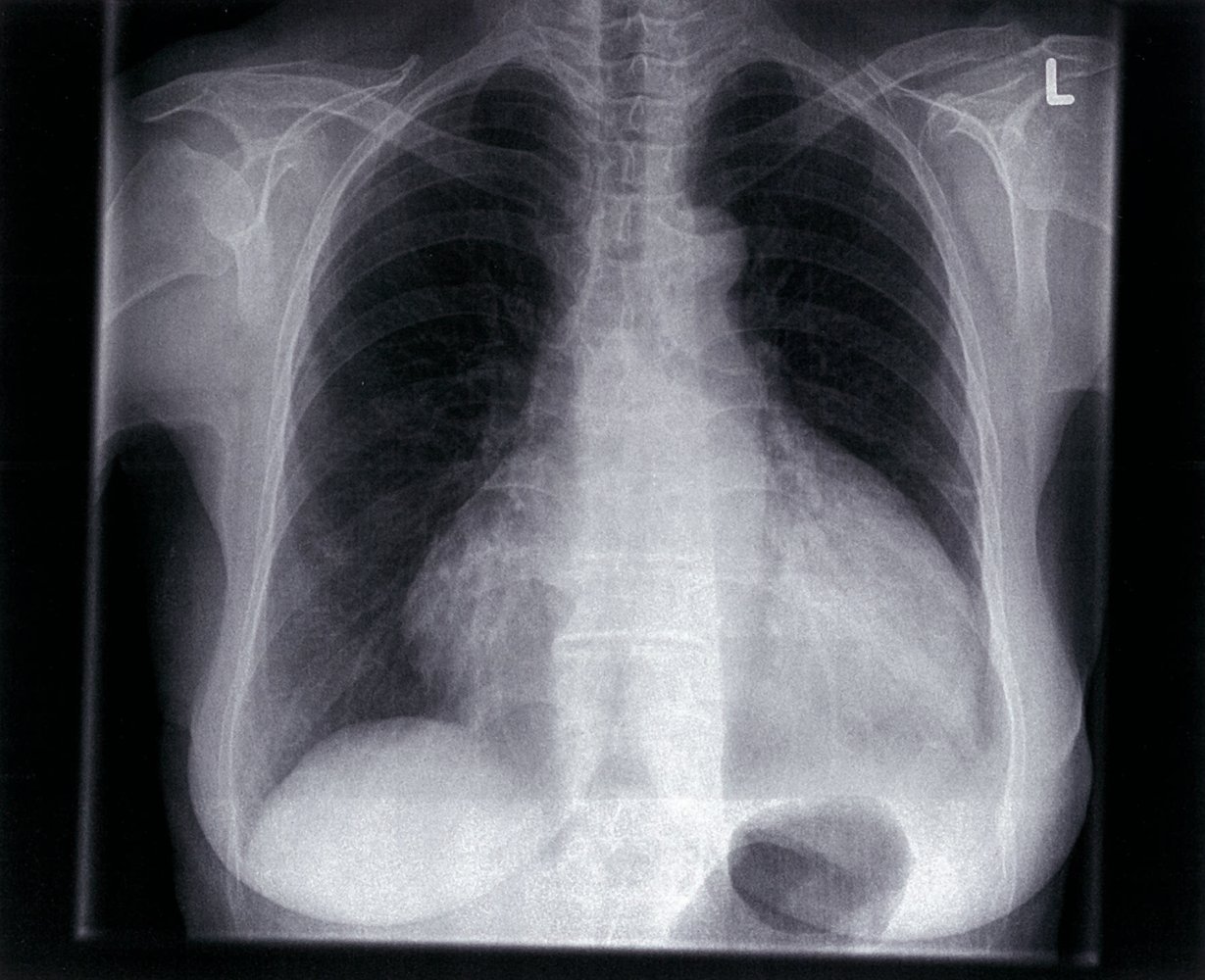
X-ray chest (PA view) of a patient with lupus pericarditis
The cardiac silhouette is enlarged and demonstrates a globular, or water bottle, configuration due to pericardial effusion (green hatched overlay).
Source: © IMPP
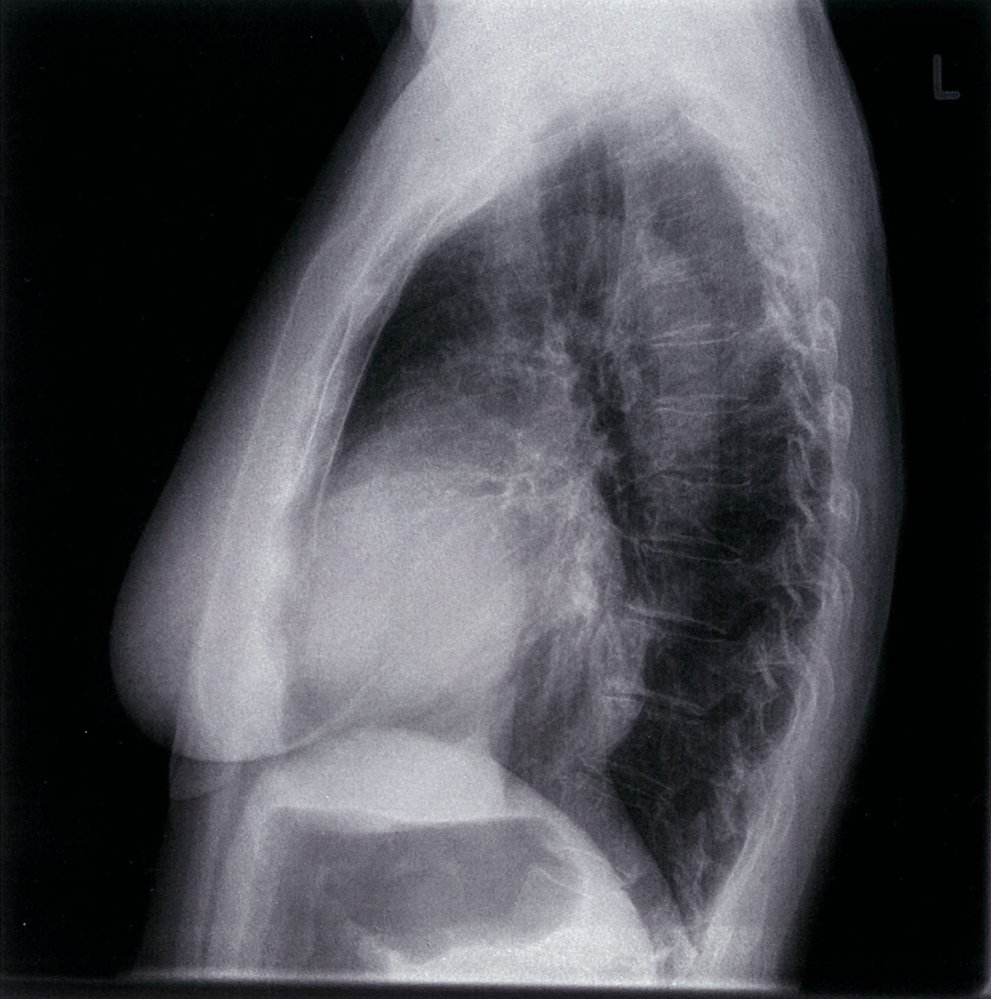
X-ray chest (lateral view)
The cardiac silhouette is enlarged due to a pericardial effusion.
Source: © IMPP
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
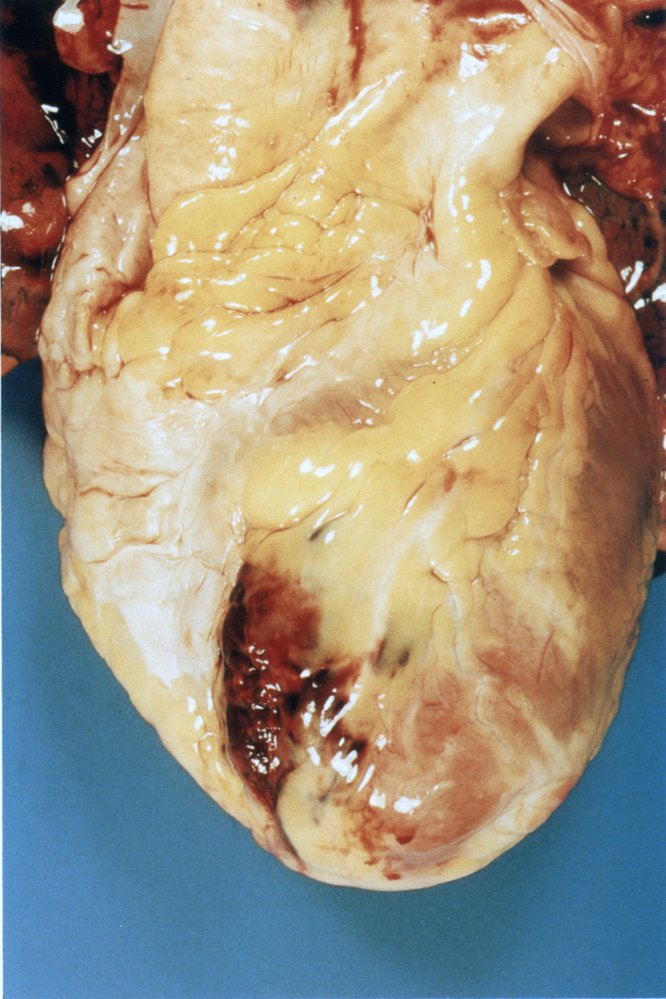
Photograph of a heart at autopsy
The red discoloration within the pericardial cavity is evidence of a hemorrhage.
Source: © IMPP
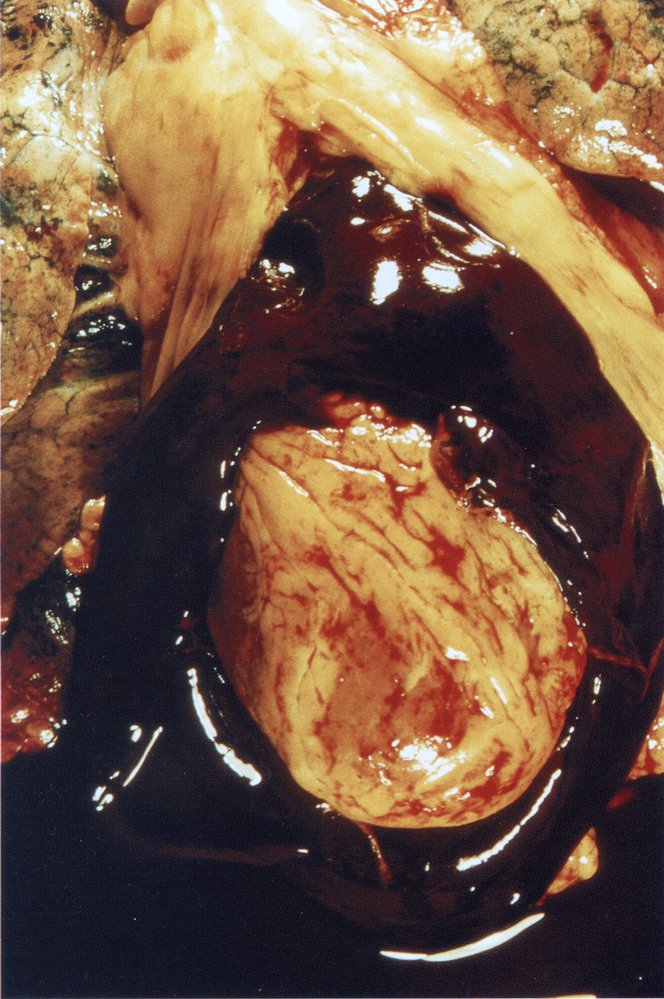
Photograph of a heart at autopsy (close-up of the left ventricle in longitudinal section)
There is coagulated, brown blood in the opened pericardium.
Coagulation indicates previous hemorrhage from the heart chambers into the pericardium. The coagulated blood compresses the heart (pericardial tamponade), leading to cardiac arrest.
Source: © IMPP
Treatment
Approach
- Unstable patients: Identify and treat cardiac tamponade urgently, if present.
-
Stable patients
- Small pericardial effusion: Conservative management focusing on treating the underlying cause is usually sufficient.
- Large pericardial effusion causing symptoms or of uncertain etiology: Consider pericardial fluid drainage.
-
All patients
- Treat the underlying cause, e.g., manage acute heart failure, treat pericarditis.
- Provide supportive care, e.g., pain management
-
Disposition
- Consult cardiology urgently if cardiac tamponade is suspected (See “Management of cardiac tamponade”).
- Consult cardiothoracic surgery if surgical pericardial fluid drainage is indicated.
- If pericardiocentesis is performed, admit patients to hospital ward or observation unit for postprocedure monitoring, serial examination, and pericardial fluid analysis.
Surgical pericardial fluid drainage (e.g., pericardiotomy and pericardiectomy) is commonly performed for patients with traumatic, purulent, loculated, rapidly reaccumulating, or malignant effusions. [11]
Pericardial fluid drainage [11][19]
-
Therapeutic pericardiocentesis
- Performed as a temporizing measure for hemodynamically unstable patients with cardiac tamponade
- Can relieve symptoms for large chronic or recurrent effusions
- Consider specialist referral for patients at high risk of reaccumulating pericardial fluid, e.g., for indwelling catheter or pericardiectomy
- See “Pericardiocentesis” for details.
-
Pericardiotomy: the creation of an opening in the pericardium to allow continuous drainage of pericardial fluid (externally or into the pleural space) [20]
-
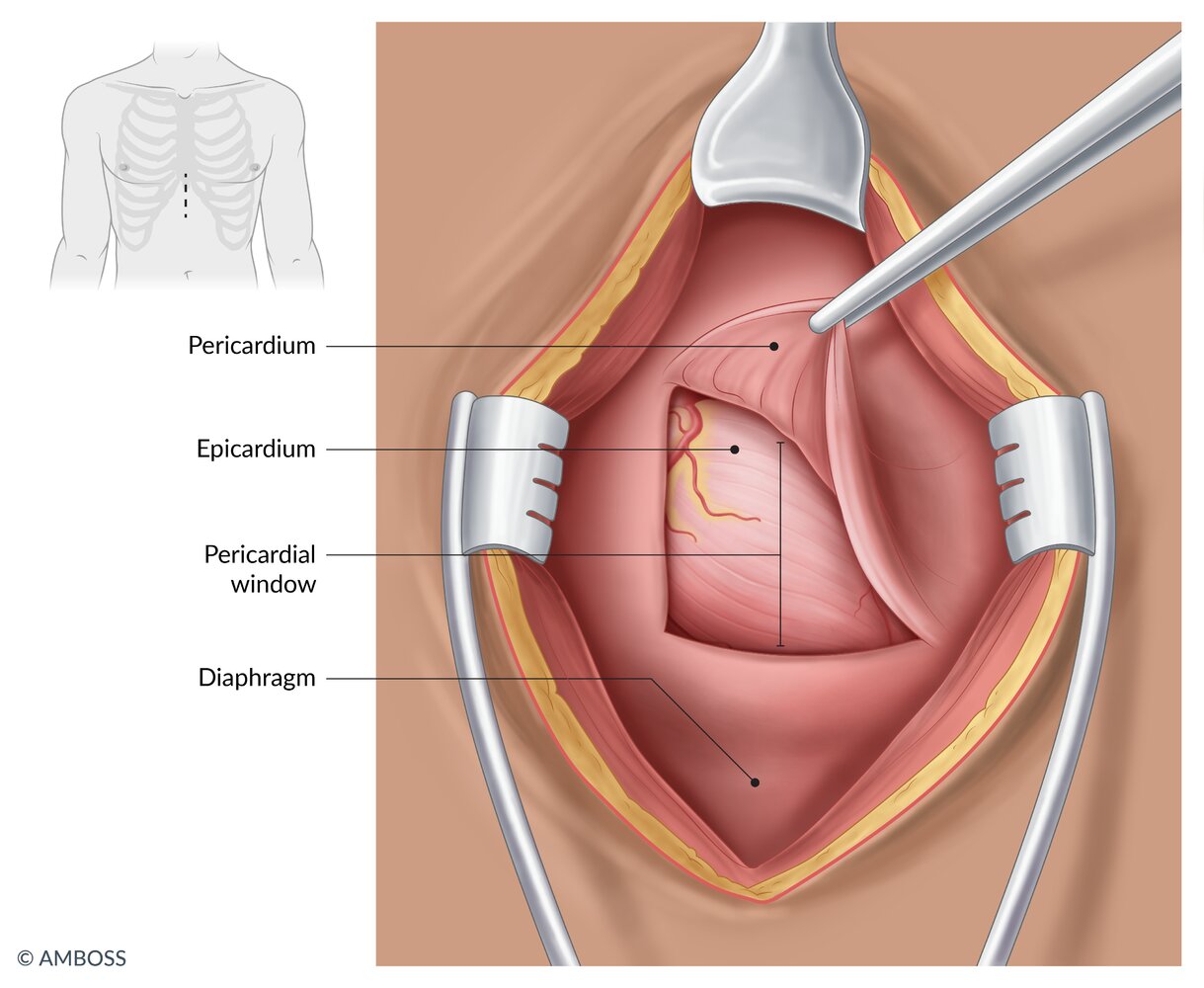
Surgical pericardiotomy (pericardial window): A surgical incision is made in the pericardium. [21]
- Subxiphoid approach: can be done under local anesthesia at the bedside (e.g., emergency department or ICU) and allows external fluid drainage
- Thoracotomy approach: needs to be done in the operating room and allows drainage into the pleural cavity
- Percutaneous balloon pericardiotomy: A transthoracic needle introduces a balloon-tipped catheter into the pericardial space which is progressively dilated to create an opening wide enough for continuous drainage.
- Complications: The mortality rate varies from 8–19%, depending on the underlying etiology. [22]
-
Surgical pericardiotomy (pericardial window): A surgical incision is made in the pericardium. [21]
- Pericardiectomy: performed as definitive management for refractory pericardial effusion, effusion due to constrictive pericarditis, or purulent pericarditis [12]
Treat hemopericardium due to penetrating chest injury surgically, e.g., with pericardial window, as soon as possible. Only consider pericardiocentesis as a temporizing measure if surgery is unavailable. [23]


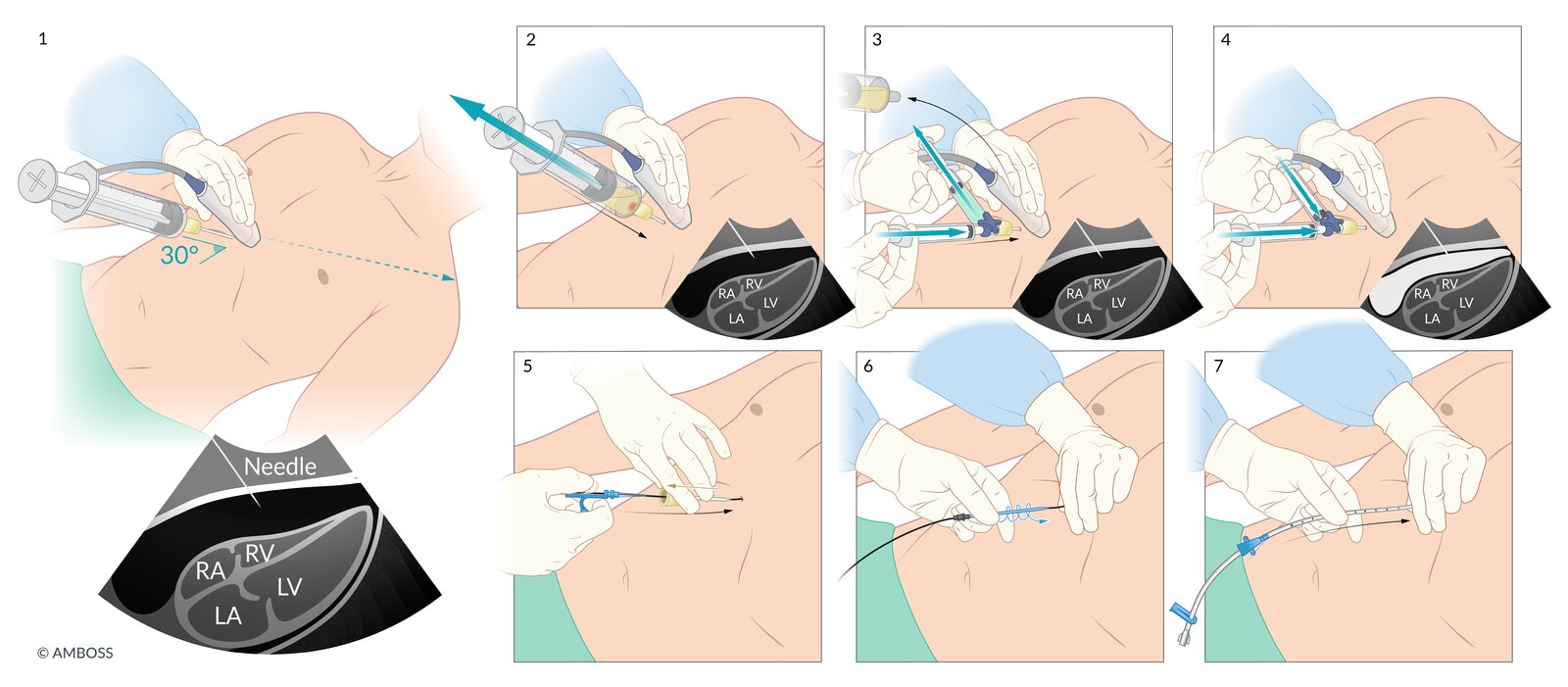
The subxiphoid approach to pericardiocentesis is shown.
1. The needle is inserted under ultrasound guidance at a 30° angle to the skin, approximately 1 cm inferior to the left xiphocostal angle.
2. Negative pressure is maintained on the syringe and the syringe is advanced until fluid returns.
3. The syringe is removed and the agitated saline apparatus is attached to confirm needle placement. With the stopcock shut to the needle, the saline is agitated by rapid injection and aspiration between the two syringes.
4. The stopcock is opened to the needle and agitated saline is injected into the pericardial sac, appearing as an echogenic stream on ultrasound.
5. If a pericardial drain is required, the Seldinger technique is used. First, a guidewire is advanced through the needle into the pericardial sac.
6. The needle is removed, a small incision is made at the insertion site, and a vascular dilator is advanced through the subcutaneous tissue using a spiral motion.
7. The dilator is removed and the catheter is advanced into the pericardial sac over the guidewire.
© AMBOSS. See related article for detailed procedural guidance.
© AMBOSS
Management of cardiac tamponade
Acute pericardial effusion with pericardial tamponade is a life-threatening condition that requires immediate pericardial decompression.
Rapid evaluation of unstable patients
Cardiac tamponade is a clinical diagnosis, however, clinical features are poorly sensitive and the diagnosis is often confirmed retrospectively. [24]
- Use POCUS to confirm the presence of a pericardial effusion (see “Focused cardiac ultrasound” or “FAST” for techniques).
- Suspect tamponade in patients with suggestive clinical features and/or bedside imaging findings.
-
≥ 70% of patients have ≥ 1 of the following: [24]
- Shortness of breath
- ↑ Heart rate
- ↑ JVP
- Pulsus paradoxus (> 10–12 mm Hg)
- Cardiac enlargement on CXR
- Beck's triad is poorly sensitive for tamponade and it is very rare for all elements to be present [25]
- < 50% of patients have low voltage QRS complexes on ECG. [24]
-
≥ 70% of patients have ≥ 1 of the following: [24]
- Obtain an urgent bedside echocardiogram to evaluate for echocardiographic findings supportive of cardiac tamponade.
- Evaluate the need for immediate pericardial fluid drainage.
- Consult a cardiologist and/or cardiothoracic surgeon and consider using a scoring system to help determine when urgent pericardiocentesis is advised and when it can safely be deferred. [26][27]
The most common underlying causes of cardiac tamponade are cardiac interventions (e.g., PCI, pacemaker implantation), malignancy, infectious or inflammatory pericarditis, mechanical complications of MI, and aortic dissection. [28]
Cardiac arrest due to suspected cardiac tamponade
See also “Cardiac arrest and cardiopulmonary resuscitation.”
-
Nontraumatic cardiac arrest [29]
- Consider POCUS in cardiac arrest to confirm pericardial effusion.
- Pause CPR to perform immediate pericardiocentesis as soon as possible if cardiac tamponade is the suspected etiology. [30][31]
- Blind pericardiocentesis can be performed using landmarks if no ultrasound guidance is available. . [23][32]
-
Traumatic cardiac arrest
- Assume pericardial fluid seen on FAST scan is traumatic hemopericardium.
- Perform emergency thoracotomy with vertical pericardiotomy. [23]
Urgent pericardial fluid drainage
- Perform pericardiocentesis under echocardiographic (or fluoroscopic) guidance without delay in unstable patients unless indications for immediate surgery are present. [11]
-
Do not delay immediate surgical management in patients with a low likelihood of successful pericardiocentesis due to immediate reaccumulation of pericardial fluid, for example in: [1][26][33]
- Type A aortic dissection
- Ventricular free wall rupture
- Severe blunt chest trauma or penetrating chest injury
- Iatrogenic hemopericardium refractory to percutaneous hemostatic control
- Refer for surgical management if pericardiocentesis is unsuccessful, e.g., due to difficult conditions [1][8][33]
Hemodynamic support
Manage as obstructive shock.
- Establish IV access with two large-bore IV lines (peripheral or central).
- Cautious fluid resuscitation (only in hypovolemic patients) [34]
- Inotropic support: dobutamine [33]
- Avoid anesthetic agents and positive pressure ventilation. [35]
- See “Hemodynamic compromise in mechanically ventilated patients” for the management approach if mechanical ventilation is unavoidable.
Positive pressure ventilation can lead to hemodynamic decompensation in patients with cardiac tamponade.
Subsequent management
- Identify and treat the underlying cause: See “Investigation of underlying etiology” in “Diagnostics.”
- Monitor for complications and reaccumulation.
- ICU admission recommended [12]
- Continuous telemetry
- Regular BP monitoring
- Serial pulsus paradoxus measurement
Acute management checklist
- Consult cardiology immediately.
- Confirm the diagnosis with FoCUS if the patient is stable (proceed directly to pericardiocentesis if not).
- Urgent pericardiocentesis in patients with cardiac tamponade
- Cardiac arrest or peri-arrest patient and no bedside imaging (e.g, POCUS) available: Consider blind technique.
- All other patients: Use POCUS guidance for unstable patients; consider CT or fluoroscopy guidance for stable patients.
- Continuous telemetry
- If the patient is hypotensive, consider cautious IV fluid use.
- Consult cardiothoracic surgery for surgical drainage if pericardiocentesis is unsuccessful or if hemopericardium or purulent effusion are suspected.
- Serial pulsus paradoxus measurement
- Transfer to ICU/CCU.
- Avoid anesthetic agents and positive pressure ventilation.
External Resources
References
- Maisch B, Seferović PM, Ristić AD, et al. "Guidelines on the diagnosis and management of pericardial diseases executive summary". European Heart Journal. 25(7). :587-610. (2004)
- Imazio M, Adler Y. "Management of pericardial effusion". Eur Heart J. 34(16). :1186-1197. (2012)
- Ariyarajah V, Spodick DH. "Cardiac tamponade revisited: a postmortem look at a cautionary case.". Tex Heart Inst J. 34(3). :347-51. (2007)
- Mekontso Dessap A, Chew MS. "Cardiac tamponade". Intensive Care Med. 44(6). :936-939. (2018)
- Doherty JU, Kort S, Mehran R, et al. "ACC/AATS/AHA/ASE/ASNC/HRS/SCAI/SCCT/SCMR/STS 2019 Appropriate Use Criteria for Multimodality Imaging in the Assessment of Cardiac Structure and Function in Nonvalvular Heart Disease". J Am Coll Cardiol. 73(4). :488-516. (2019)
- Jung H-O. "Pericardial Effusion and Pericardiocentesis: Role of Echocardiography". Korean Circ J. 42(11). :725. (2012)
- Ceriani E, Cogliati C. "Update on bedside ultrasound diagnosis of pericardial effusion". Intern Emerg Med. 11(3). :477-480. (2016)
- Chiabrando JG, Bonaventura A, Vecchié A, et al. "Management of Acute and Recurrent Pericarditis". J Am Coll Cardiol. 75(1). :76-92. (2020)
- Adams JG. "Emergency Medicine E-Book". Elsevier Health Sciences. (2012). ISBN: 9781455733941
- Balachandran G. "Interpretation of Chest X-Ray: An Illustrated Companion". JP Medical Ltd. (2014). ISBN: 9789351521723
- Adler Y, Charron P, Imazio M, et al. "2015 ESC Guidelines for the diagnosis and management of pericardial diseases". Eur Heart J. 36(42). :2921-2964. (2015)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Shabetai R. "The Pericardium". Springer Science & Business Media. (2012). ISBN: 9781441991379
- Milevoj Kopcinovic L, Culej J. "Pleural, peritoneal and pericardial effusions – a biochemical approach". Biochem Med (Zagreb). :123-137. (2014)
- Clinic C. "Current Clinical Medicine E-Book". Elsevier Health Sciences. (2010). ISBN: 9781437735710
- Atar S, Chiu J, Forrester JS, Siegel RJ. "Bloody Pericardial Effusion in Patients With Cardiac Tamponade". Chest. 116(6). :1564-1569. (1999)
- Maisch B. "Practical aspects of the management of pericardial disease". Heart. 89(9). :1096-1103. (2003)
- Petcu CP, Dilof R, Bătăiosu C, Petcu PD. "Purulent pericardial effusions with pericardial tamponade - diagnosis and treatment issues.". Curr Health Sci J. 39(1). :53-6. (2013)
- Roberts JR. "Roberts and Hedges' Clinical Procedures in Emergency Medicine and Acute Care". Elsevier. (2018). ISBN: 9780323354783
- Johns P. "Head injury". Elsevier. :105-114. (2014). ISBN: 9780443103216
- Labbé C, Tremblay L, Lacasse Y. "Pericardiocentesis versus Pericardiotomy for Malignant Pericardial Effusion: A Retrospective Comparison". Current Oncology. 22(6). :412-416. (2015)
- Eapen S, Firstenberg M. "Standardized approach to pericardial effusion management". Int J Acad Med. 4(2). :160. (2018)
- American College of Surgeons and the Committee on Trauma. "ATLS Advanced Trauma Life Support". American College of Surgeons. (2018). ISBN: 9780996826235
- Roy CL, Minor MA, Brookhart MA, Choudhry NK. "Does This Patient With a Pericardial Effusion Have Cardiac Tamponade?". JAMA. 297(16). :1810. (2007)
- Stolz L, Valenzuela J, Situ-LaCasse E, et al. "Clinical and historical features of emergency department patients with pericardial effusions". World Journal of Emergency Medicine. 8(1). :29. (2017)
- Risti AD, Imazio M, Adler Y, et al. "Triage strategy for urgent management of cardiac tamponade: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases". Eur Heart J. 35(34). :2279-2284. (2014)
- Duanmu Y, Choi DS, Tracy S, et al. "Development and validation of a novel prediction score for cardiac tamponade in emergency department patients with pericardial effusion". European Heart Journal. Acute Cardiovascular Care. 10(5). :542-549. (2020)
- Imazio M, De Ferrari GM. "Cardiac tamponade: an educational review". European Heart Journal. Acute Cardiovascular Care. 10(1). :102-109. (2020)
- Lavonas EJ, Drennan IR, Gabrielli A, et al. "Part 10: Special Circumstances of Resuscitation". Circulation. 132(18 suppl 2). :S501-S518. (2015)
- Link MS, Berkow LC, Kudenchuk PJ, et al. "Part 7: Adult Advanced Cardiovascular Life Support". Circulation. 132(18 suppl 2). :S444-S464. (2015)
- Vanden Hoek TL, Morrison LJ, Shuster M, et al. "Part 12: Cardiac Arrest in Special Situations: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care". Circulation. 122(18_suppl_3). :S829-S861. (2010)
- Petri N, Ertel B, Gassenmaier T, et al. "“Blind” pericardiocentesis: A comparison of different puncture directions". Catheter Cardiovasc Interv. 92(5). :E327-E332. (2018)
- Khanna S, Maheshwari K. "Hemopericardium and Acute Cardiac Tamponade". Anesthesiology. 128(5). :1006. (2018)
- Spodick DH. "Acute Cardiac Tamponade". N Engl J Med. 349(7). :684-690. (2003)
- Sharma A, Bansal R, Vyas V, et al. "Anesthetic challenges for pleuro-pericardial window". Saudi J Anaesth. 13(3). :272. (2019)
- Hoit BD. "Diagnosis and treatment of pericardial effusion". UpToDate. UpToDate. https://www.uptodate.com/contents/diagnosis-and-treatment-of-pericardial-effusion. [2015-11-25]
- Little WC, Freeman GL. "Pericardial Disease". Circulation. 113(12). :1622-1632. (2006)
- Foley J, Tong LP, Ramphul N. "Message in a bottle. The use of chest radiography for diagnosis of pericardial effusion". Afr J Emerg Med. 6(3). :148-150. (2016)
- Hines RL, Marschall KE. "Stoelting's Anesthesia and Co-existing Disease". Elsevier Health Sciences. (2008). ISBN: 9781416039983