Quick guide
Diagnostic approach
- ABCDE survey
- Targeted clinical evaluation
- PCR of nasopharyngeal swab
Red flag features
- Pneumonia
- Signs of respiratory failure
- Cyanosis
- Apnea
- Seizures
- Difficulty feeding
Management checklist
- Droplet precautions
- Antibiotic therapy for pertussis, e.g., azithromycin (off-label)
- Respiratory support
- Dehydration management
- Nutritional support
- Assess admission criteria for pertussis.
Summary
Pertussis, or whooping cough, is a highly infectious disease of the respiratory tract caused by the gram-negative bacterium Bordetella pertussis. This disease spreads via droplet transmission (and to a lesser extent via fomites) and most commonly occurs in children. Typically, pertussis manifests in three stages, with the second and third stages characterized by intense paroxysmal coughing that is followed by a distinctive whooping sound on inhalation and, in some cases, vomiting. Young infants may not develop the typical cough, and often present with apnea and cyanosis instead. Patients who meet the suspected case definition for pertussis should be started on antibiotic therapy for pertussis, and confirmatory laboratory studies (usually PCR or culture) should be conducted. Postexposure prophylaxis for pertussis is recommended for all close contacts and high-risk individuals (e.g., infants) regardless of immunization status. Pertussis immunization is part of the routine immunization schedule; while immunization reduces the severity of illness, it does not provide full immunity.
Epidemiology
- Pertussis is typically a childhood disease (particularly children aged < 1 year); however, older patients are increasingly affected. [1][2]
- High rate of infections in newborns: The Tdap vaccine is recommended for pregnant individuals between 27 and 36 weeks' gestation. [1][3]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Pathogen: Bordetella pertussis is a gram‑negative, obligate aerobic coccobacillus.
- Transmission: droplet transmission, fomite transmission [4][5]
-
Infectivity
- Without antibiotic treatment: 4–6 weeks
- With treatment: ∼ 5 days
- Highly virulent
- Incubation period: on average 7–10 days (range 4–21 days)

References:[1][6]
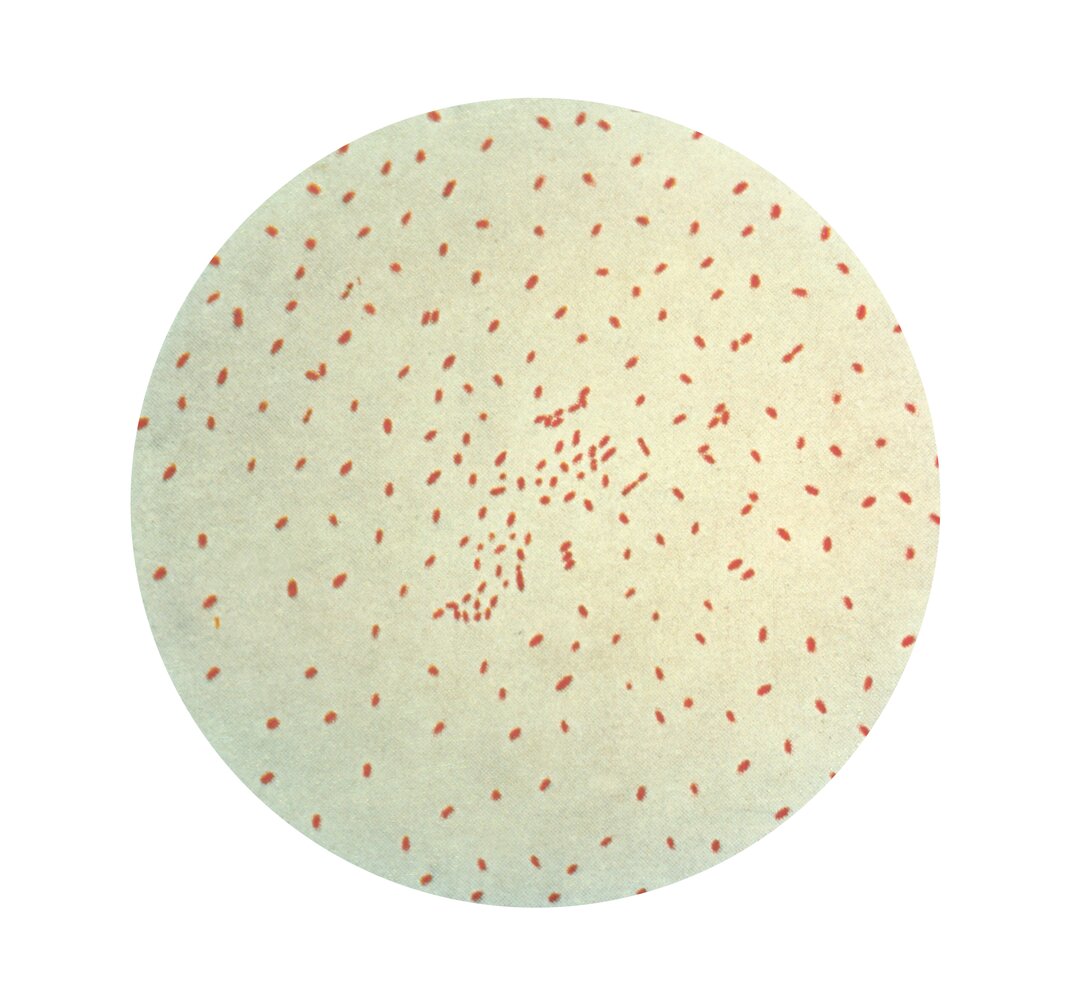
Photomicrograph (Gram-stain; high magnification) of a culture specimen of Bordetella pertussis.
Numerous Gram-negative coccobacilli are visible.
Source: "ID#: 2121", CDC, Centers for Disease Control and Prevention licensed under Public Domain
Pathophysiology
- Proliferation of Bordetella pertussis on ciliated epithelial cells of the respiratory mucosa → production of virulence factors (e.g., tracheal cytotoxin) → paralysis of respiratory epithelium cilia and inflammation → secretion of inflammatory exudate into respiratory tract → compromise of small airways → cough, pneumonia, cyanosis [7]
- Bordetella pertussis produces pertussis toxin → ADP-ribosylation of the α subunit of Gi protein → inhibition of Gi protein → adenylate cyclase disinhibition → cAMP accumulation → impaired cell signaling pathways [8]
- Pertussis toxin is responsible for most of the systemic manifestations associated with whooping cough (e.g., hypoglycemia, lymphocytosis, modulation of host immune response).
- Neither vaccination nor actual infection confers complete or lifelong immunity.
Clinical features
Pertussis classically has three stages: catarrhal, paroxysmal, and convalescent. Symptoms may vary, however, based on age and immunization status; vaccinated individuals tending to have a milder illness without characteristic whooping. [1][9]
Catarrhal stage (1–2 weeks) [9]
-
Nonspecific symptoms similar to an upper respiratory infection, e.g.:
- Mild cough
- Watery nasal discharge
- Rarely low-grade fever
- Possibly conjunctivitis
- Patients are highly infectious.
Paroxysmal stage (2–6 weeks) [9]
-
Intense paroxysmal coughing (often occurring at night)
- Followed by a deep and loud inhalation or high-pitched whooping sound
- Accompanied by struggling for breath, gagging, and tongue protrusion
- Possibly accompanied by cyanosis
- Increases in frequency and severity throughout the stage
- Followed by the expulsion of phlegm or posttussive vomiting (risk of dehydration)
- Potential bleeding of the conjunctiva, petechiae, and venous congestion
-
Infants (< 6 months) may present with: [1][6]
- Apneic episodes
- Paroxysmal coughing but no characteristic whoop [1]
Convalescent stage (weeks to months) [9]
- Progressive reduction of symptoms
- Coughing attacks may persist over several weeks before resolving.
- Patients have an increased susceptibility to respiratory infections.
The typical pattern of paroxysmal cough with whooping manifests mainly in unvaccinated children. Infants < 6 months of age, vaccinated individuals, and adults may not whoop and may not follow the classic stages of pertussis. [1][9]
Catarrhal stage manifests with Coryza, while the Paroxysmal stage manifests with Posttussive vomiting and whooPing cough.


Diagnosis
Approach [1][10]
- Perform confirmatory studies for any patient that meets the suspected case definition for pertussis. [9]
- The choice of diagnostic test depends on duration since symptom onset. [9][11][12]
- First 1–4 weeks: Obtain PCR ± culture.
- Between 4—12 weeks: Consider a serum sample for serology. [9][12]
-
For infants < 3 months, consider a CBC.
- Lymphocyte-predominant leukocytosis is common in infants and young children. [6]
- An absolute lymphocyte count of > 20,000/μL is a classic diagnostic finding and suggests a poor prognosis. [1][9]
Suspected case definition for pertussis [11][12][13]
Cough is present for any duration (with a low threshold for suspicion in infants), with ≥ 1 of the following: [9][13]
- Paroxysmal coughing
- Whooping on inspiration
- Posttussive vomiting
- Apnea [11][12]
- Known contact with confirmed case
- Living in an area with a pertussis outbreak
The presence of fever suggests an alternative diagnosis (see “Differential diagnoses of pertussis”). [9][13]
Confirmatory studies
PCR and/or cultures should be used for patients who present ≤ 4 weeks since cough onset. Serology should be used for patients who present > 4 weeks after developing symptoms.
PCR [1][6][11]
-
Preferred test [9]
- High sensitivity
- Rapid results
- Unaffected by antibiotic therapy or previous vaccination [1]
-
Specimen collection
- Preferred: nasopharyngeal swab
- Alternative: saline nasopharyngeal aspirate
Bacterial culture [1][6][11]
-
Gold standard [9]
- 100% specificity
- Use is limited by:
- Long growth time (7–10 days)
- Low sensitivity, especially in patients who are taking antibiotics or have been immunized [1]
- Indications [9][14]
- Alternative when PCR is not available
- In addition to PCR for strain identification
-
Specimen collection method
- Preferred: nasopharyngeal swab
- Alternative: saline nasopharyngeal aspirate
Pertussis serology [6][9][11]
- Used for patients who meet all the following criteria:
- 4–12 weeks since cough onset [1][6]
- Age ≥ 6 months [9]
- ≥ 1 year since the last vaccination dose
- Findings: ↑ IgG antibodies to pertussis toxin
The CDC only accepts positive culture or PCR for disease reporting; serology is, however, suggested for use in outbreak settings. [6][12]
Direct fluorescent antibody testing and blood cultures are not recommended because of low specificity and sensitivity. [6][11][15]
Differential diagnoses
- Bordetella parapertussis infection
- Respiratory syncytial virus bronchiolitis
- Pneumonia, particularly due to Chlamydia trachomatis or Mycoplasma pneumoniae
- Croup (laryngotracheobronchitis)
- Foreign body aspiration
The differential diagnoses listed here are not exhaustive.
Treatment
Approach [6]
- Start antibiotic therapy in suspected pertussis without waiting for diagnostic confirmation. [6][9][10]
- Assess patients for admission criteria for pertussis and admit if present.
- Consider the need for ICU/PICU consult.
- Infants with pertussis should be admitted to a facility able to escalate care. [6][16]
- Provide supportive care, e.g.: [17]
- Respiratory support [16]
- Frequent suctioning
- Management of dehydration and hypovolemia
- Nutritional support
- Initiate measures to prevent onward transmission of pertussis.
- After treatment, offer the acellular pertussis vaccine to stable unvaccinated patients. [1]
Symptomatic treatment of cough (e.g., with corticosteroids, antihistamines, albuterol) is not recommended, as there is no evidence symptomatic treatments reduce cough or duration of hospitalization. [9][18]
Pertussis is a nationally notifiable disease. [9]
Admission criteria for pertussis
- Admit patients with features of severe disease, e.g.: [6][17]
- Patients of any age with:
- Pneumonia
- Signs of respiratory failure (i.e., cyanosis, apnea)
- CNS complications (e.g., seizure)
- In infants with:
- Apnea
- Difficulty feeding
- Patients of any age with:
- Consider admission for patients with risk factors for severe pertussis, e.g.: [6][19][20]
- Individuals of any age with a history of:
- Immunocompromise
- Pulmonary disease (e.g., COPD, asthma)
- Neurologic disorders
- Genetic disease
-
Infants with any of the following characteristics:
- Age < 4 months
- Prematurity
- Low birth weight
- Mother who did not receive a pertussis vaccine during pregnancy
- Individuals of any age with a history of:
Infants < 6 months are at the highest risk for morbidity and mortality, especially those with a history of preterm delivery or inadequate maternal immunization. [6][20]
Antibiotic therapy for pertussis [1][6][9]
-
First-line: macrolides
- Preferred: azithromycin (off-label) [6][9]
- Alternative
- Erythromycin [6]
- Clarithromycin [6]
- Allergy/intolerance to macrolides: Consider trimethoprim/sulfamethoxazole: (off-label). [6]
Antibiotic therapy within 3 weeks of symptom onset decreases transmission of pertussis but may not improve the duration or severity of symptoms, especially if started at a later clinical stage. [1][7][11]
Monitor infants < 6 weeks of age who are being treated with azithromycin or erythromycin for hypertrophic pyloric stenosis. [6]
Complications
- Infection: otitis media
- Respiratory
- Bordetella pertussis pneumonia
- Hemoptysis, atelectasis, pneumothorax
- Cardiac: pulmonary hypertension [6]
- Neurologic: seizures, encephalopathy with possible permanent damage
- Sudden infant death [6]
References:[21][22][23]
We list the most important complications. The selection is not exhaustive.
Prognosis
- In children > 6 months: usually good; lengthy convalescence, but full recovery
- In children < 6 months: increased risk of complications; mortality highest in children < 2 months [1][6]
Prevention
Primary prevention of pertussis [24][25][26]
- Vaccine: the acellular pertussis vaccine is available as a combination vaccine that also contains the diphtheria vaccine and tetanus vaccine.
-
Choice of vaccine depends on age: [1]
- Children < 7 years of age: DTaP vaccine
- Children ≥ 7 years of age and adults: Tdap vaccine [1]
-
Primary course
- Recommended at 2, 4, 6, and 15–18 months and at 4–6 years
- Adults who were not vaccinated as children should receive a one-time dose of Tdap.
- See “ACIP immunization schedule” for details on routine and catch-up schedules.
-
Booster
- All individuals aged 11–12 years [6]
- During each pregnancy: one-time dose, preferably at 27–36 weeks of gestation
- Adults who receive a routine tetanus booster with Tdap will also be boosted against pertussis. [9][26]
-
Contraindications [24][26]
- Absolute contraindications: anaphylactic reaction to or encephalopathy from previous pertussis vaccination
-
Relative contraindications include:
- Moderate to severe acute illness
- Uncontrolled or evolving neurological disorders (e.g., Guillain-Barré syndrome or seizures)
- Arthus reaction
Pertussis vaccination helps reduce severity, but infection can still occur because the immunity from vaccination (as well as infection) is short-lived and there has been a rise in vaccine antigen-deficient strains. [9]
Ensure all close contacts (e.g., family members, caregivers) of infants have received all the recommended age-appropriate pertussis vaccines (DTaP, Tdap). [1][6][9]
Prevention of onward transmission of pertussis
Approach [6][11]
- Use droplet precautions when evaluating patients.
- Advise isolation precautions for pertussis for suspected or confirmed cases.
- The duration of isolation precautions varies based on treatment status: [1]
- Treated patients: until 5 days of antibiotic therapy have been completed
- Untreated patients: > 3 weeks since cough onset
- For patients in the community: [6]
- Advise avoiding contact with high-risk individuals (i.e., pregnant women, infants, and children).
- Children who attend daycare/school and staff in childcare and healthcare settings should remain at home.
- For hospitalized patients: Place the patient in a side room with droplet precautions. [11]
- The duration of isolation precautions varies based on treatment status: [1]
- Perform contact tracing to determine who should be offered postexposure prophylaxis for pertussis.
- Pertussis is a notifiable disease; ensure the state health department has been contacted.
Postexposure prophylaxis for pertussis [6][10]
-
Indications [11]
- All close contacts of an individual with pertussis, regardless of age and vaccination status [1]
-
High-risk individuals with possible exposure, e.g.:
- Infants
- Pregnant women (third trimester)
- Any individual who cares for infants and/or pregnant women (e.g., health care or daycare workers)
- Immunocompromised individuals [9]
- Individuals with chronic comorbidities (e.g., respiratory conditions) [9]
-
Prophylactic measures
- Administer antibiotic therapy for pertussis within 21 days of contact exposure. [9]
- Advise isolation precautions for pertussis until 5 days of antibiotic therapy has been completed. [27]
- Ensure all asymptomatic individuals are up-to-date with acellular pertussis vaccine according to the ACIP immunization schedule. [1][11]
External Resources
References
- Hall E, Wodi AP, Hamborsky J, et al. "Epidemiology and Prevention of Vaccine-Preventable Diseases 14th ed". Public Health Foundation. (2021). ISBN: 9780578969695
- Gabutti G, Rota MC. "Pertussis: a review of disease epidemiology worldwide and in Italy". Int J Environ Res Public Health. 9(12). :4626–4638. (2012)
- Clark TA. "Changing pertussis epidemiology: everything old is new again". J Infect Dis. 209(7). :978-91. (2014)
- "CDC Yellow Book 2024: Pertussis / Whooping Cough". https://web.archive.org/web/20231126044407/https://wwwnc.cdc.gov/travel/yellowbook/2024/infections-diseases/pertussis-whooping-cough. [2023-05-01]
- "Epidemiology and Control of Selected Infections Transmitted Among Healthcare Personnel and Patients (2022) – Section Pertussis". https://web.archive.org/web/20230925042250/https://www.cdc.gov/infectioncontrol/guidelines/healthcare-personnel/selected-infections/pertussis.html. [2022-11-02]
- AAP Committee on Infectious Diseases. "Red Book: 2021–2024 Report of the Committee on Infectious Diseases". American Academy of Pediatrics. (2021). ISBN: 9781610025218
- "Pertussis (Whooping Cough) - Disease Specifics". https://web.archive.org/web/20170526030534/https://www.cdc.gov/pertussis/clinical/disease-specifics.html. [2015-09-08]
- Carbonetti NH. "Pertussis toxin and adenylate cyclase toxin: key virulence factors ofBordetella pertussisand cell biology tools". Future Microbiol. 5(3). :455-469. (2010)
- Nemhauser JB. "CDC Yellow Book 2024". Oxford University Press. (2023). ISBN: 9780197570944
- Kline JM, Smith EA, Zavala A. "Pertussis: Common Questions and Answers". Am Fam Physician. 104(2). :186-192. (2021)
- "Pertussis: Vaccine Preventable Diseases Surveillance Standards". https://www.who.int/publications/m/item/vaccine-preventable-diseases-surveillance-standards-pertussis. [2018-09-04]
- "Pertussis (Whooping Cough) (Bordetella pertussis) 2020 Case Definition". https://ndc.services.cdc.gov/case-definitions/pertussis-2020/. [2021-04-16]
- Moore A, Harnden A, Grant CC, et al. "Clinically Diagnosing Pertussis-associated Cough in Adults and Children". Chest. 155(1). :147-154. (2019)
- "Pertussis (Whooping Cough) Specimen Collection and Diagnostic Testing". https://www.cdc.gov/pertussis/clinical/diagnostic-testing/specimen-collection-diagnosis.html. [2022-08-04]
- Janda WM, Santos E, Stevens J, et al. "Unexpected isolation of Bordetella pertussis from a blood culture". J Clin Microbiol. 32(11). :2851-3. (1994)
- Surridge J, Segedin ER, Grant CC. "Pertussis requiring intensive care". Arch Dis Child. 92(11). :970-975. (2007)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Wang K, Bettiol S, Thompson MJ, et al. "Symptomatic treatment of the cough in whooping cough". Cochrane Database Syst Rev. 2014(9). :CD003257. (2014)
- Cherry JD. "Pertussis in Young Infants Throughout the World". Clin Infect Dis. 63(suppl 4). :S119-S122. (2016)
- Mbayei SA, Faulkner A, Miner C, et al. "Severe Pertussis Infections in the United States, 2011-2015". Clin Infect Dis. 69(2). :218-226. (2019)
- Brooks D, Clover R. "Pertussis infection in the United States: role for vaccination of adolescents and adults". J Am Board Fam Med. 19(6). :603-11. (2006)
- Monaco F, Barone M, Manfredi VG et al. "Pneumomediastinum as a complication of critical pertussis". Clin Respir J. 10(6). :772-776. (2016)
- Long SS, Prober CG, Fischer M. "Principles and Practice of Pediatric Infectious Diseases E-Book". Elsevier Health Sciences. (2017). ISBN: 9780323461320
- "Child and Adolescent Immunization Schedule. Recommendations for Ages 18 Years or Younger, United States, 2023". https://web.archive.org/web/20230324163634/https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html. [2023-02-10]
- "Catch-up Immunization Schedule for Children and Adolescents Who Start Late or Who Are More than 1 Month Behind Recommendations for Ages 18 Years or Younger, United States, 2023". https://web.archive.org/web/20230324164753/https://www.cdc.gov/vaccines/schedules/hcp/imz/catchup.html. [2023-02-10]
- "Adult Immunization Schedule by Age Recommendations for Ages 19 Years or Older, United States, 2023". https://web.archive.org/web/20230324184103/https://www.cdc.gov/vaccines/schedules/hcp/imz/adult.html. [2023-02-10]
- "Infection Control in Healthcare Personnel: Epidemiology and Control of Selected Infections Transmitted Among Healthcare Personnel and Patients". https://www.cdc.gov/infectioncontrol/pdf/guidelines/IC-Guidelines-HCP-H.pdf. [2022-01-01]