Summary
Pituitary adenomas (also known as pituitary neuroendocrine tumors) are benign tumors that arise sporadically from the anterior pituitary gland. They are classified as either microadenomas or macroadenomas according to their size, and as either secretory (functional) or nonsecretory (nonfunctioning) according to their ability to secrete hormones. Secretory adenomas produce the pituitary hormone of the cell type from which they arise, which results in a state of hyperpituitarism. Nonsecretory macroadenomas can destroy the surrounding normal pituitary tissue, which results in hypopituitarism. Additionally, large macroadenomas compress the optic chiasm; therefore, patients may present with signs of mass effect such as bitemporal hemianopsia. MRI sella with IV contrast is the gold standard imaging method for the pituitary and should reveal any intrasellar masses. Pituitary hormone assays are used to evaluate patients for endocrine abnormalities, and perimetry is used to identify visual field defects. Transsphenoidal hypophysectomy is the first-line therapy for most patients with symptomatic pituitary adenomas; patients with nonsecretory microadenomas generally only require follow-up (until they become symptomatic), and prolactin-producing pituitary adenomas (prolactinomas) should be initially treated with dopamine agonists (e.g., cabergoline, bromocriptine). Pituitary irradiation is indicated in recurrent pituitary adenomas and/or if surgical therapy is contraindicated.
Epidemiology
-
Prevalence [1]
- Approx. 80 cases per 100,000 individuals
- Pituitary adenomas account for ∼ 15% of primary intracranial tumors. [1]
- Peak incidence: : 35–60 years [2]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Most cases occur sporadically.
- Some cases (∼ 5%) have a genetic/familial association: [3]
- Multiple endocrine neoplasia type 1
-
Carney complex
- Caused by a loss of function mutation in the PRKAR1A gene, which encodes the regulatory subunit (R1α) of protein kinase A, resulting in increased cAMP activity
- Patients present with cardiac myxoma, spotty skin pigmentation, and adrenal gland, testicular, and pituitary adenomas.
-
Familial isolated pituitary adenoma syndrome [4]
- Caused by mutations in the AIP gene
- Patients present with pituitary adenomas without other associated abnormalities.
- The most common familial cause of acromegaly/gigantism
Pathophysiology
- Pituitary adenomas are well-circumscribed, intrasellar tumors with monomorphic, polygonal cells arranged in sheets or cords without any connective tissue and/or reticulin.
-
Tumor classification according to size
- Pituitary microadenoma: ≤ 10 mm
- Pituitary macroadenoma: > 10 mm
-
Tumor classification according to ability to secrete hormones
- Nonsecretory pituitary adenomas [5]
- Nonfunctioning tumors account for 15–45% of all pituitary adenomas.
- Gonadotroph adenomas
- Null cell adenomas
- Plurihormonal adenomas
- Silent somatotroph and corticotroph adenomas
-
Secretory pituitary adenomas: hormone secretion → hyperpituitarism
- Most exclusively proliferate in only one type of endocrine cell and therefore secrete only one pituitary hormone.
- The presence of multiple pituitary hormones should also raise suspicions for atypical pituitary adenomas or pituitary carcinomas.
- Nonsecretory pituitary adenomas [5]
| Secretory pituitary adenomas | ||
|---|---|---|
| Origin | Relative frequency (as a percentage of all pituitary adenomas) | Pathophysiology |
| Lactotroph adenoma (prolactinoma) [6] |
|
|
| Somatroph adenoma |
|
|
| Corticotroph adenoma(Cushing disease) |
|
|
| Thyrotroph adenoma |
|
|
| Gonadotroph adenoma |
|
|
Prolactinomas are the most common pituitary adenomas.
Clinical features
| Type | Secretory adenomas | Nonsecretory adenomas [5] |
|---|---|---|
| Microadenomas |
|
|
| Macroadenomas |
|
|
The symptoms associated with pituitary adenomas depend on the size of the tumor and whether the tumor produces hormones.
Diagnosis
Approach
The diagnostic approach varies according to clinical presentation.
| Diagnostic approach for a suspected pituitary adenoma [7][8][9][10] | ||
|---|---|---|
| Presentation | Initial evaluation | Further evaluation |
| Symptoms of mass effect to the pituitary |
|
|
| Symptoms of hypopituitarism or hyperpituitarism |
|
|
| Pituitary incidentaloma [8] |
|
|
In patients with endocrine dysfunction, order hormone assays before imaging to prevent overdiagnosis of pituitary incidentalomas. [10]
Hormone assays [7][8][9]
Indications for testing
- First-line tests for all patients with symptomatic endocrine dysfunction
- Pituitary mass detected on imaging
- Prior to planned pituitary surgery
Initial studies
-
Choice of studies
- Symptomatic patients: Studies are chosen according to clinical presentation.
- Asymptomatic patients: general screening
-
Interpretation
- ↓ Hormone levels suggest hypopituitarism; see also “Diagnostics” in “Hypopituitarism.”
- ↑ Hormone levels suggest hyperpituitarism (secondary to a secretory adenoma); the hormones that are elevated will depend on the cellular origin of the adenoma (see “Pathophysiology”).
| Initial hormone studies for suspected pituitary endocrine dysfunction | |
|---|---|
| Symptoms | Initial studies |
| Asymptomatic patients [9] |
|
| Hyperprolactinemia |
|
| Hypogonadism or absent lactation |
|
| Hyperthyroidism or hypothyroidism |
|
| Hypercortisolism |
|
| Adrenal insufficiency |
|
| Acromegaly or gigantism |
|
Patients with pituitary incidentalomas should be evaluated for hypopituitarism and hormonal hypersecretion syndromes. [8]
About a third of patients with pituitary adenomas have associated hypopituitarism; consider screening for hormone deficiencies in all patients with a pituitary mass. [9]
Imaging studies [12][13]
-
MRI sella with IV contrast (gold standard)
- Indications
- First-line diagnostic modality for suspected secretory or nonsecretory pituitary adenomas
- Postsurgical surveillance after resection of a pituitary mass
- Characteristic finding: intrasellar mass
- Potential additional findings [7]
- Compression of adjacent structures (e.g., impingement on the optic chiasm)
- Hemorrhage and necrosis in pituitary apoplexy [10][14]
- Cavernous sinus invasion
- Indications
-
CT sella with IV contrast
- Indications
- Second-line diagnostic modality [13]
- Can be used to plan transsphenoidal hypophysectomy
- Supportive findings: similar to MRI
- Indications




Additional investigations
-
Visual field testing (e.g., perimetry) [7][9]
- Indicated for patients with visual symptoms or with pituitary adenomas affecting the optic chiasm on imaging [15]
- The characteristic finding is bitemporal hemianopsia; visual alterations correlate with tumor size.
- Histopathology: Order markers of proliferation (e.g., p53) and pituitary hormones for resected pituitary adenomas, particularly if the adenoma is aggressive or recurrent. [16]
- Genetic testing: Genetic testing is not routinely recommended; consider in patients with a family history suggestive of potential genetic syndromes (see “Etiology”). [7]
Visual defects may be present even in asymptomatic patients with a pituitary adenoma; consider early referral for visual field testing even in the absence of visual symptoms. [9]

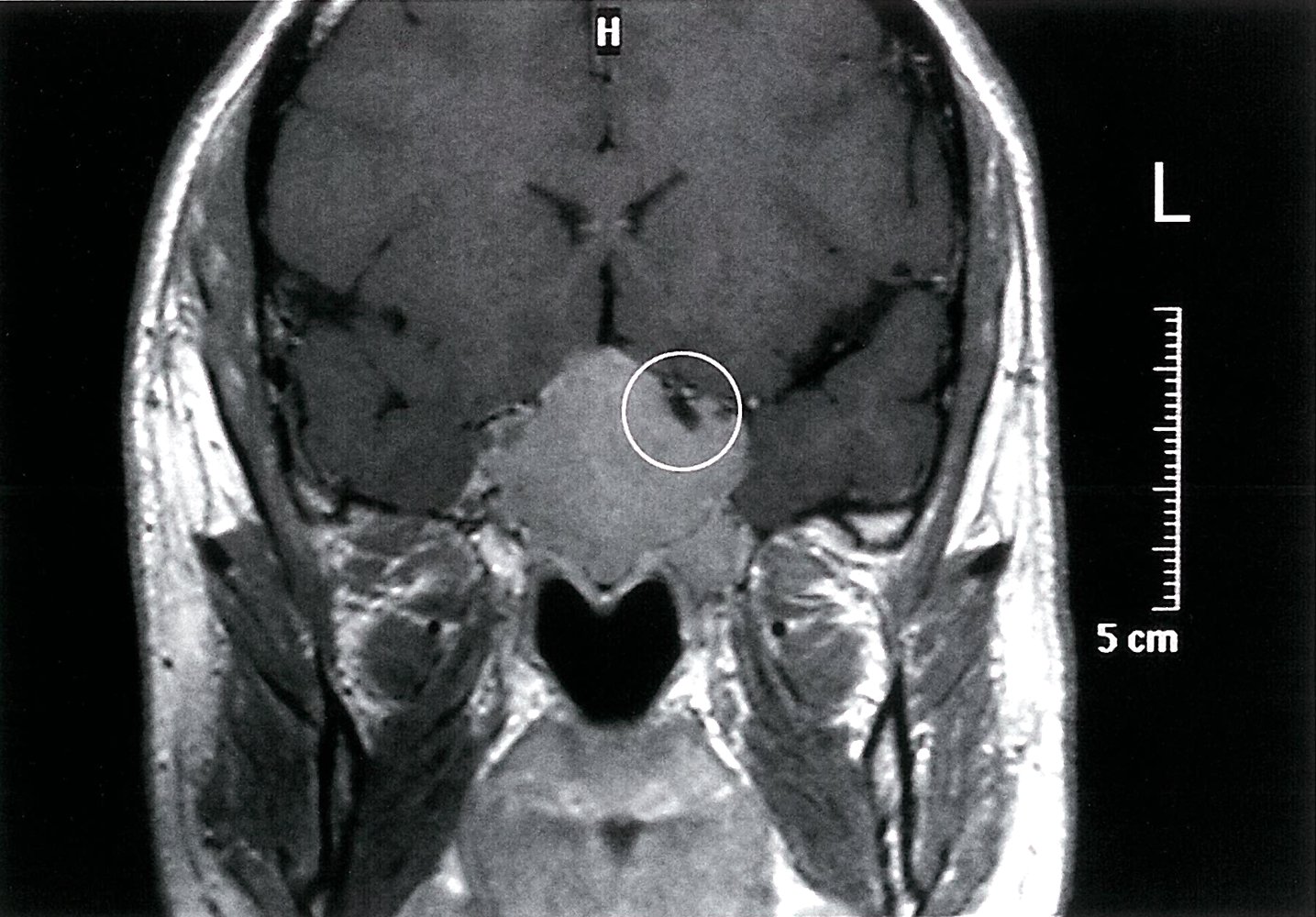
MRI head (T1-weighted; with contrast; coronal plane) of a patient with headache, retroorbital pressure, fatigue, and elevated serum prolactin
A large enhancing mass (indicated by arrows in overlay) is seen in the midline in the area of the sella turcica. The normal left internal carotid artery (encircled) is shown as a hypointense structure because of flow-related signal loss.
In light of the patient's history, a prolactin-secreting macroadenoma (prolactinoma) of the pituitary gland is the most likely diagnosis.
Source: © IMPP
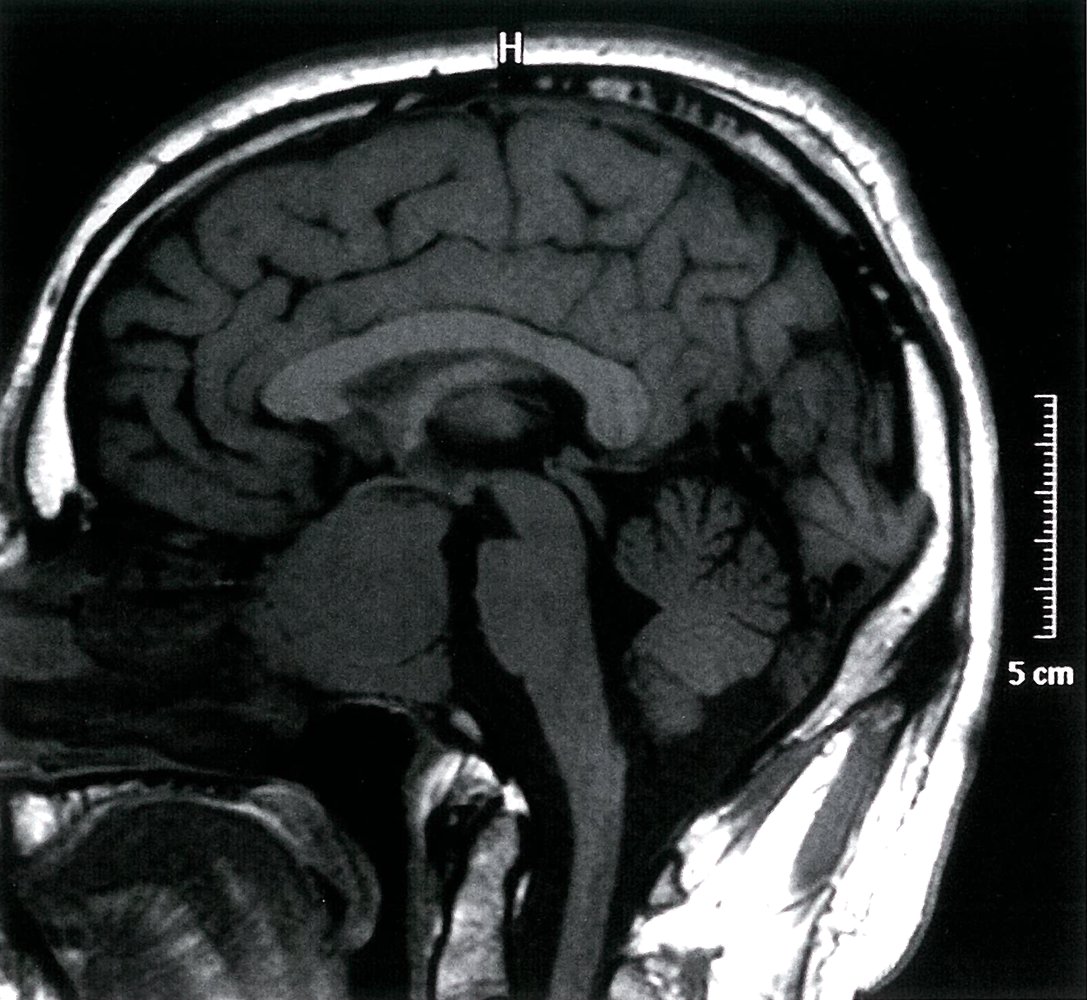
MRI head (T1-weighted; without contrast; sagittal plane) of a male patient with headache, retroorbital pressure, fatigue, and elevated serum prolactin
A large mass, which is isointense to gray matter, is seen in the area of the sella turcica (indicated by arrows).
Considering the patient's history, a prolactin-secreting macroadenoma (prolactinoma) of the pituitary gland is the most likely diagnosis.
Source: © IMPP
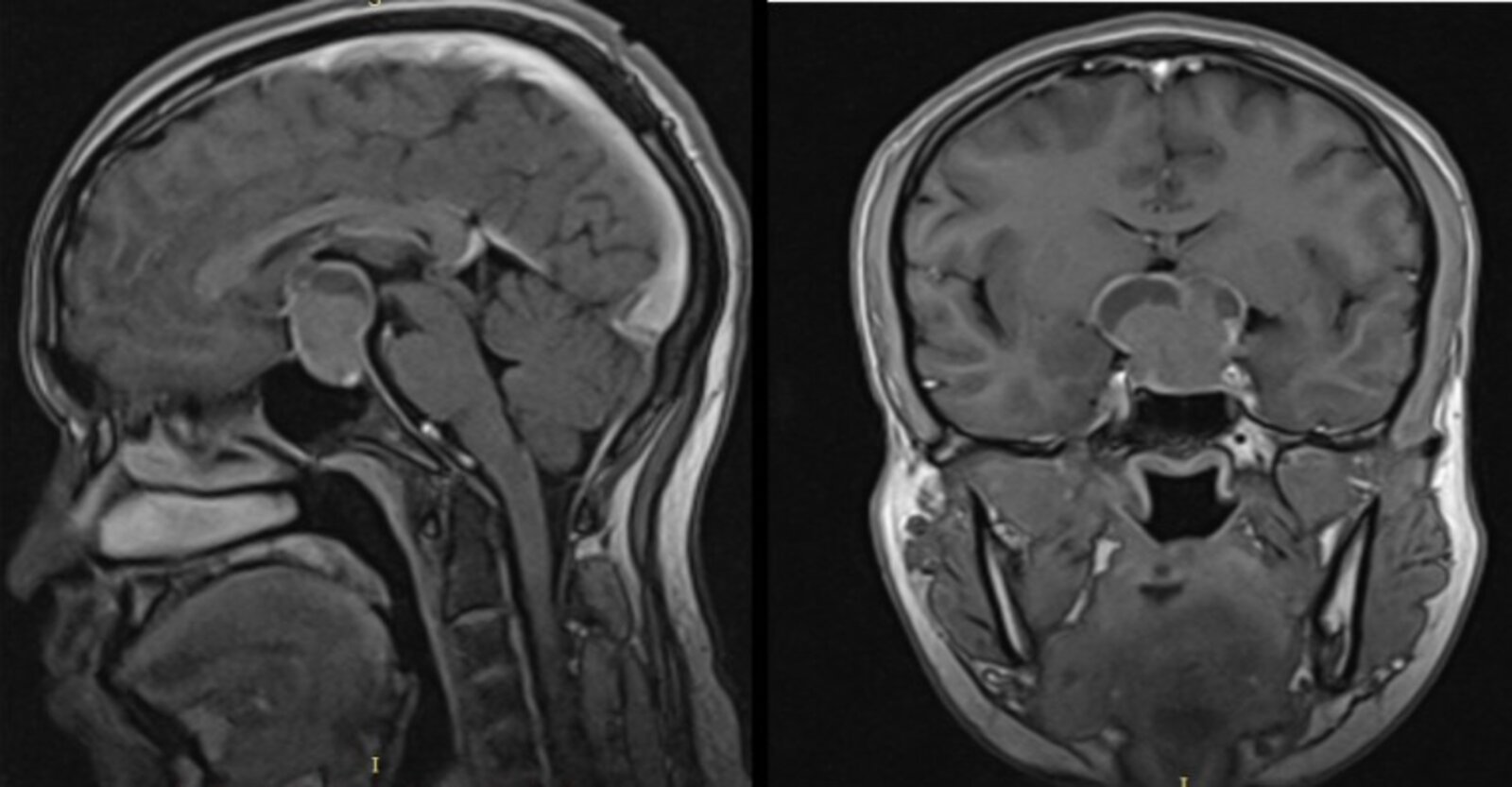
MRI head (T1-weighted; left: sagittal plane; right: coronal plane) of a 21-year-old, male patient with a pituitary macroadenoma
A large, lobulated mass (green overlay) with heterogeneous contrast enhancement extends from the sella turcica into the suprasellar space.
Blue overlay: compressed third ventricle
Source: “Figure 1, in: Giant Pituitary Adenoma Presenting with Foster-Kennedy Syndrome in a 21-Year Old Ethiopian Patient: A Rarely Reported Phenomenon: A Case Report” by B. Ayele, A. Mengesha, A. Wotiye et al., Ethiopian-Journal of Health Sciences, licensed under CC BY 4.0. Modifications: Image cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
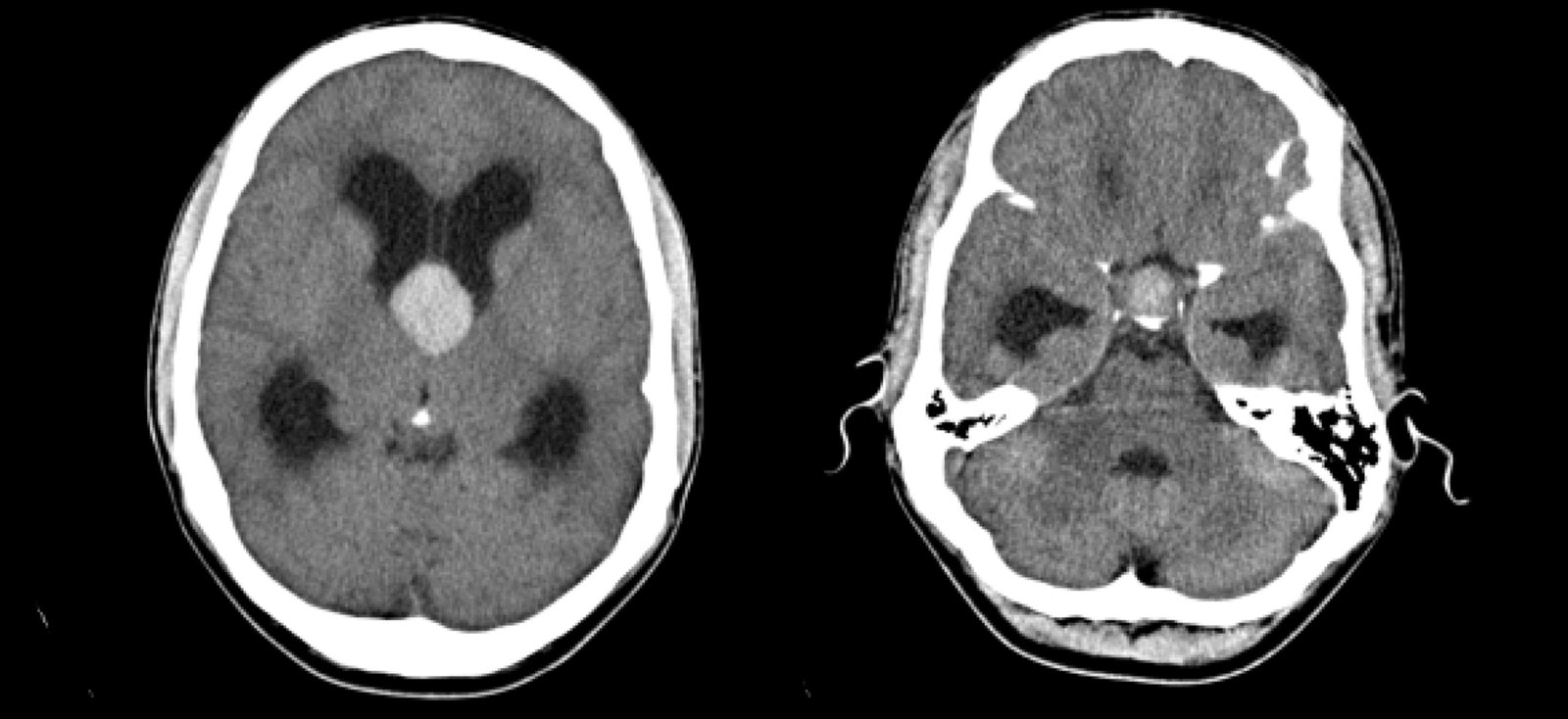
CT head (without contrast; axial plane)
A midline high-attenuation mass (green overlay) extends superiorly from the pituitary fossa into the suprasellar space. There is associated obstructive hydrocephalus, with dilatation of the lateral ventricles (dashed lines).
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.
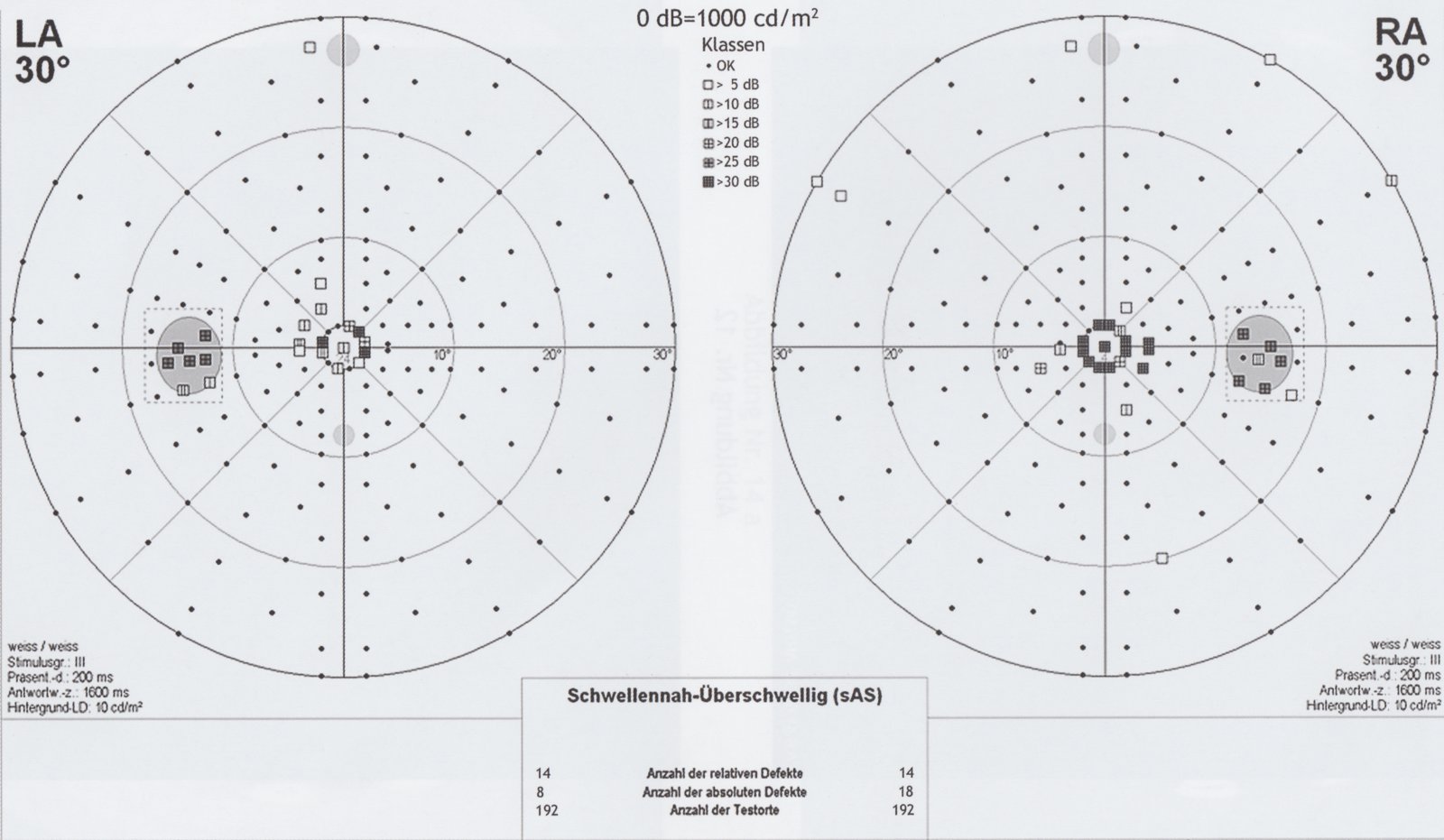
Automatic static perimetry images of a patient's left (LA) and right (RA) visual fields
Light stimuli of varying brightness are given at fixed measuring points and the patient is asked to press a button when they can perceive the light. The results are compared with an age-specific average and any visual defects are mapped (incrementally darker squares indicating severity). The result displays the visual field from the patient's point of view.
This perimetry finding indicates a central scotoma of both eyes (right > left). The blind spot (physiological scotoma) is also shown bilaterally (gray dashed box, temporal of the central fixation).
Source: © IMPP
Treatment
Approach [7][8][9]
- Assess patients for life-threatening and sight-threatening complications.
- Stabilize patients with acute hormonal imbalances.
- Refer patients with severe vision loss or altered mental state to neurosurgery urgently.
- Refer all patients to endocrinology.
- Treatment is based on the tumor type, tumor size, and presence of symptoms.
- Initial treatment options include surgery, pharmacotherapy, and observation.
- Refractory tumors : consider (repeat) transsphenoidal hypophysectomy, medical management, and/or pituitary irradiation. [7][17][18]
| Initial treatment of pituitary adenomas [7][8][9] | |
|---|---|
| Tumor type | First-line treatment |
| Prolactinomas (symptomatic or macroadenomas) | Pharmacotherapy |
| Secretory adenomas (except prolactinomas) | Surgery |
| Symptomatic nonsecretory adenomas | |
| Asymptomatic microprolactinomas | Observation |
| Asymptomatic nonsecretory adenomas | |
The management of patients with pituitary incidentalomas is the same as for those with any other pituitary adenoma. [7][8]
Treat patients with secretory incidentalomas according to tumor type, and treat patients with nonsecretory incidentalomas if symptoms of mass effect are present. [7][8]
Pituitary adenomas may bleed spontaneously, causing pituitary apoplexy (i.e., pituitary tumor apoplexy); this manifests with severe headaches, visual symptoms, cardiovascular collapse, and/or acute secondary adrenal insufficiency. [10]
Initial stabilization
Patients may be acutely unwell secondary to hormonal alterations; treat aggressively before starting definitive management.
-
Acute hypopituitarism, i.e., myxedema coma, or secondary adrenal insufficiency (may be secondary to pituitary apoplexy)
- Rapid administration of hydrocortisone can be lifesaving.
- For details and dosage information, see “Adrenal crisis” and “Myxedema coma.”
- Acute hyperpituitarism, i.e., thyroid storm: For details, see “Treatment of thyroid storm.”
Do not delay hydrocortisone treatment in patients with adrenal crisis or myxedema coma.
Surgical management [7][8][9][10]
-
Indications
-
First-line treatment for:
- Secretory adenomas (excluding prolactinomas)
- Symptomatic nonsecretory adenomas
- Pituitary apoplexy with visual symptoms [10]
- Second-line treatment if medical management fails in prolactinomas
-
First-line treatment for:
-
Presurgical stabilization
- Give patients with the following a steroid stress dose of hydrocortisone on the day of surgery: [19][20]
- Confirmed or suspected ACTH deficiency
- A pituitary adenoma that is likely to require total hypophysectomy
- In patients with hyperthyroidism, antithyroid drugs are recommended before surgery to achieve a euthyroid state (e.g., methimazole, propylthiouracil, beta blockers).
- Ensure that all patients who are referred to neurosurgery also receive an endocrinology consult.
- Give patients with the following a steroid stress dose of hydrocortisone on the day of surgery: [19][20]
-
Procedure: transsphenoidal hypophysectomy [21]
- Removal of pituitary tissue; performed under microscopic or endoscopic guidance via the sphenoidal sinus
- May be partial (hemihypophysectomy) or complete (total hypophysectomy)
-
Follow-up
- Monitor for early postoperative complications during hospitalization (consider ICU admission).
- Regular follow-ups are necessary to detect new or recurrent hormone imbalances early.
Transsphenoidal hypophysectomy can alter ADH secretion, causing transient or permanent central DI and/or SIADH. In some patients, these alterations can occur sequentially in a biphasic pattern (i.e., DI followed by SIADH), or less frequently, in a triphasic pattern (i.e., DI followed by SIADH followed by DI). [22]
Following transsphenoidal resection and/or pituitary irradiation, patients may develop hypopituitarism and potentially require lifelong hormone replacement therapy.
Pharmacotherapy [7]
-
Indications
- Prolactinomas: first-line treatment for symptomatic patients and those with macroadenoma
- Secretory adenomas: patients who are unsuitable for, or have symptoms refractory to, surgery
-
Treatment options
-
Prolactinomas: Dopamine agonists (cause the adenoma to shrink)
- First line: cabergoline [8]
- Second line: bromocriptine
-
ACTH-secreting tumor (see “Cushing disease” for details)
- Somatostatin analogs (e.g., pasireotide)
- Enzyme inhibitors (e.g., ketoconazole, metyrapone)
- Glucocorticoid antagonists (mifepristone)
-
GH-secreting tumor (see “Acromegaly” for details)
- Somatostatin analogs (e.g., octreotide, lanreotide) ± cabergoline
- GH-antagonists (pegvisomant)
- TSH-secreting tumor: somatostatin analogs (e.g., octreotide, lanreotide)
-
Prolactinomas: Dopamine agonists (cause the adenoma to shrink)
Observation
-
Indications
- Asymptomatic microprolactinomas
- Asymptomatic nonsecretory adenomas
| Observation strategies for asymptomatic nonsecretory pituitary adenomas [7][8] | ||
|---|---|---|
| Study | Follow-up intervals | |
| Nonsecretory incidentalomas | Asymptomatic prolactinoma | |
| Imaging studies (MRI) |
|
|
| Hormone assays |
|
|
| Visual field testing |
|
|
| ||
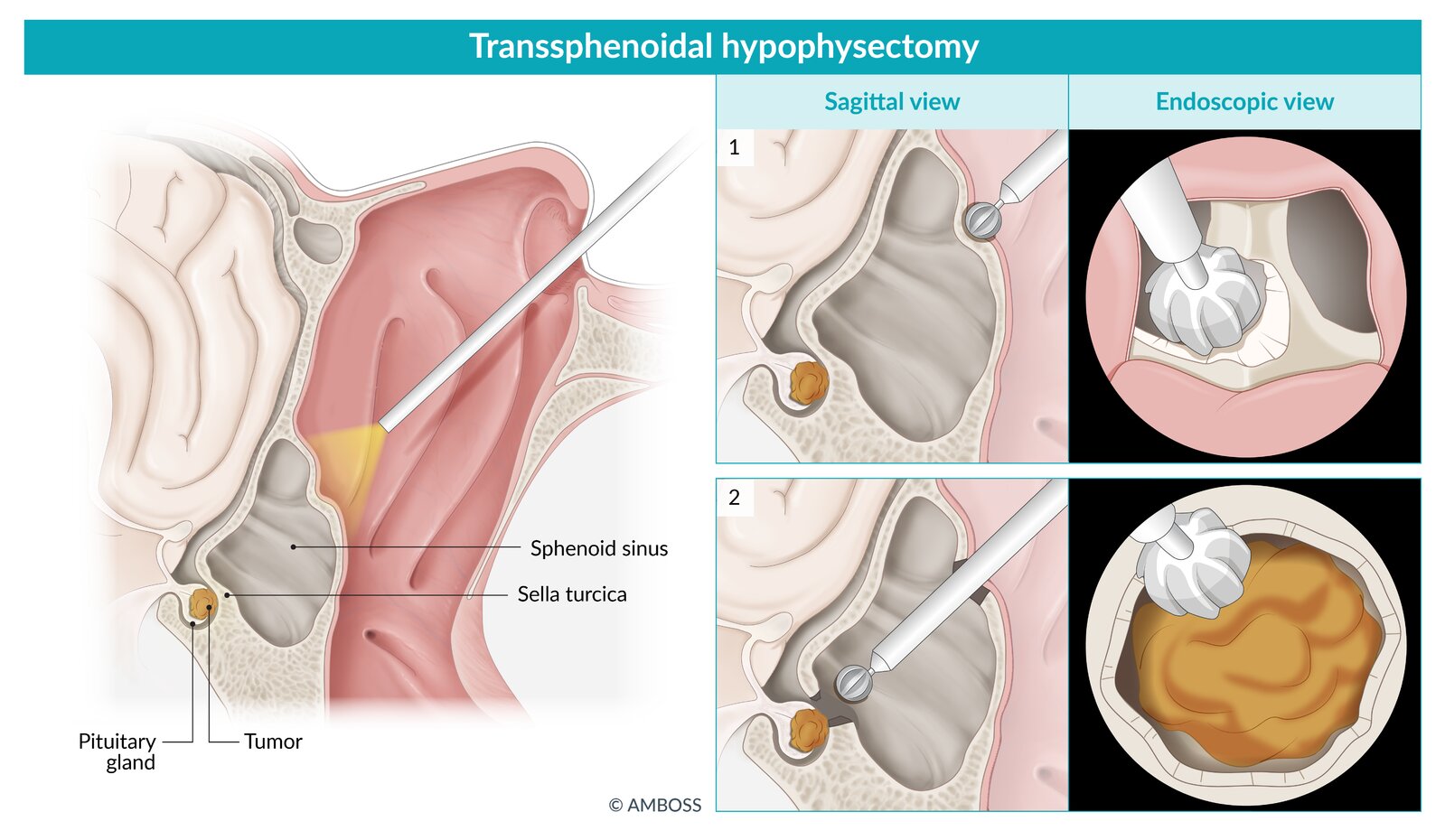
Schematic depiction of transsphenoidal hypophysectomy.
Left: Overview of the surgical approach to the sella turcica. An endoscope is inserted through the nasal cavity and advanced toward the anterior wall of the sphenoid sinus.
1: Partial resection of the anterior wall of the sphenoid sinus.
2: Subsequent resection of the posterior wall of the sphenoid sinus, providing access to the sella turcica and the pituitary gland for tumor resection.
© AMBOSS
Differential diagnoses
-
Intracranial neoplasms [10]
- Rathke cleft cyst (most common sellar mass after adenomas)
- Craniopharyngioma (suprasellar mass): most commonly in children
- Meningioma (parasellar mass)
- Neurofibroma
- Ectopic germinoma
- Granulomatous disorders invading the sellar region or hypothalamus
- Sarcoidosis
- Tuberculomas
- Carotid artery aneurysm
- Lymphocytic hypophysitis
The differential diagnoses listed here are not exhaustive.
Special patient groups
Prolactinoma in pregnancy [6][23][24]
In pregnancy, there is a significant risk of tumor growth in individuals with macroadenomas who have not previously undergone treatment with surgery or radiation therapy.
-
Preconception
- Weigh the risk of prolactinoma expansion and apoplexy against the risk of toxic effects of pharmacological treatment on the fetus.
- Consider debulking surgery before pregnancy for individuals with expansive or invasive macroadenomas and/or resistance to dopamine agonist therapy.
-
Microadenomas (< 10 mm)
- Discontinue dopamine agonist; microadenomas are less likely to enlarge during pregnancy than macroadenomas.
- Clinical review every 3 months
-
Macroadenomas (≥ 10 mm)
- Continue dopamine agonist; some clinicians prefer bromocriptine in pregnancy.
- Monthly clinical review for mass effect
- Visual field assessment every 3 months
- Visual field changes or worsening headaches: prompt noncontrast pituitary MRI
External Resources
References
- Scheithauer BW, Gaffey TA, Lloyd RV, et al. "Pathobiology of Pituitary Adenomas and Carcinomas". Neurosurgery. 59(2). :341-353. (2006)
- Aflorei ED, Korbonits M. "Epidemiology and etiopathogenesis of pituitary adenomas". J Neurooncol. 117(3). :379-394. (2014)
- Daly AF, Tichomirowa MA, Beckers A. "The epidemiology and genetics of pituitary adenomas". Best Practice & Research Clinical Endocrinology & Metabolism. 23(5). :543-554. (2009)
- Beckers A, Aaltonen LA, Daly AF, Karhu A. "Familial Isolated Pituitary Adenomas (FIPA) and the Pituitary Adenoma Predisposition due to Mutations in the Aryl Hydrocarbon Receptor Interacting Protein (AIP) Gene". Endocr Rev. 34(2). :239-277. (2013)
- Ntali G, Wass JA. "Epidemiology, clinical presentation and diagnosis of non-functioning pituitary adenomas". Pituitary. 21(2). :111-118. (2018)
- Molitch ME. "Diagnosis and Treatment of Pituitary Adenomas". JAMA. 317(5). :516. (2017)
- Freda PU, Beckers AM, Katznelson L, et al. "Pituitary Incidentaloma: An Endocrine Society Clinical Practice Guideline". J Clin Endocrinol Metab. 96(4). :894-904. (2011)
- Lake MG, Krook LS, Cruz SV. "Pituitary adenomas: an overview". Am Fam Physician. 88(5). :319-27. (2013)
- Melmed S, Polonsky KS, Larsen PR, Kronenberg HM. "Williams Textbook of Endocrinology". Elsevier. (2016). ISBN: 9780323297387
- Iglesias P, Diez JJ. "Macroprolactinoma: a diagnostic and therapeutic update". QJM. 106(6). :495-504. (2013)
- Chen CC, Carter BS, Wang R, et al. "Congress of Neurological Surgeons Systematic Review and Evidence-Based Guideline on Preoperative Imaging Assessment of Patients With Suspected Nonfunctioning Pituitary Adenomas". Neurosurgery. 79(4). :E524-E526. (2016)
- Burns J, Policeni B, Bykowski J, et al. "ACR Appropriateness Criteria® Neuroendocrine Imaging". J Am Coll Radiol. 16(5). :S161-S173. (2019)
- Boellis A, di Napoli A, Romano A, Bozzao A. "Pituitary apoplexy: an update on clinical and imaging features". Insights into Imaging. 5(6). :753-762. (2014)
- Newman SA, Turbin RE, Bodach ME, et al. "Congress of Neurological Surgeons Systematic Review and Evidence-Based Guideline on Pretreatment Ophthalmology Evaluation in Patients With Suspected Nonfunctioning Pituitary Adenomas". Neurosurgery. 79(4). :E530-E532. (2016)
- Raverot G, Burman P, McCormack A, et al. "European Society of Endocrinology Clinical Practice Guidelines for the management of aggressive pituitary tumours and carcinomas". Eur. J. Endocrinol. 178(1). :G1-G24. (2018)
- Sheehan J, Lee C-C, Bodach ME, et al. "Congress of Neurological Surgeons Systematic Review and Evidence-Based Guideline for the Management of Patients With Residual or Recurrent Nonfunctioning Pituitary Adenomas". Neurosurgery. 79(4). :E539-E540. (2016)
- Varlamov EV, McCartney S, Fleseriu M. "Functioning Pituitary Adenomas – Current Treatment Options and Emerging Medical Therapies". Eur Endocrinol. 15(1). :30. (2019)
- Inder WJ, Hunt PJ. "Glucocorticoid replacement in pituitary surgery: guidelines for perioperative assessment and management.". J Clin Endocrinol Metab. 87(6). :2745-50. (2002)
- Ausiello JC, Bruce JN, Freda PU. "Postoperative assessment of the patient after transsphenoidal pituitary surgery". Pituitary. 11(4). :391-401. (2008)
- Kuo JS, Barkhoudarian G, Farrell CJ, et al. "Congress of Neurological Surgeons Systematic Review and Evidence-Based Guideline on Surgical Techniques and Technologies for the Management of Patients With Nonfunctioning Pituitary Adenomas". Neurosurgery. 79(4). :E536-E538. (2016)
- Lamas C, del Pozo C, Villabona C. "Clinical guidelines for management of diabetes insipidus and syndrome of inappropriate antidiuretic hormone secretion after pituitary surgery". Endocrinol Nutr. 61(4). :e15-e24. (2014)
- Melmed S, Casanueva FF, Hoffman AR, et al. "Diagnosis and Treatment of Hyperprolactinemia: An Endocrine Society Clinical Practice Guideline". The Journal of Clinical Endocrinology & Metabolism. 96(2). :273-288. (2011)
- Petersenn S, Fleseriu M, Casanueva FF, et al. "Diagnosis and management of prolactin-secreting pituitary adenomas: a Pituitary Society international Consensus Statement". Nat Rev Endocrinol. 19(12). :722-740. (2023)
- Glezer A, Bronstein MD. "Prolactinomas in pregnancy: considerations before conception and during pregnancy". Pituitary. 23(1). :65-69. (2019)