Summary
Plantar fasciitis is a common condition that affects the deep plantar fascia, resulting in foot and heel pain. Although it is traditionally thought to be an inflammatory-driven process, histological analysis in affected patients typically shows degenerative changes. Peak incidence is between 40–60 years of age, but an earlier onset is possible, especially in people engaged in repetitive activities such as running and dancing. Other risk factors include foot deformities, prolonged weight bearing, elevated BMI, and limited ankle dorsiflexion. Plantar fasciitis is characterized by foot and/or heel pain that is typically worse first thing in the morning, then improves throughout the day before returning in the evening. Pain is usually unilateral but may be bilateral in up to a third of cases. On examination, there is tenderness to palpation at the medioplantar surface. Diagnosis is usually clinical, but imaging may be helpful in patients with atypical, severe, or persistent symptoms, or to exclude differential diagnoses (e.g., calcaneal stress fracture). Treatment is usually conservative and includes NSAIDS and activity modification. Surgery may be considered for patients with refractory pain.
Epidemiology
- One of the most common causes of foot pain [1]
- Peak incidence: 40–60 years of age [1]
- ♀ > ♂ [1]
Plantar fasciitis is one of the most common causes of foot pain in adults. [1]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Not well studied but is thought to be an overuse condition resulting in degenerative changes [1]
Risk factors [1]
-
Modifiable risk factors
- Repetitive, high-impact activities
- High BMI (> 27 kg/m2)
- Prolonged weight-bearing
- Sedentary lifestyle
- Intrinsic foot and/or calf muscle tightness
-
Structural risk factors
- Limited ankle dorsiflexion
-
Foot deformities
- Pes planus
- Pes cavus
- Leg length discrepancy
Clinical features
-
Stabbing, nonradiating pain that affects the heel and sole of the foot (medioplantar surface) [1]
- Worse first thing in the morning or after inactivity
- Improves throughout the day
- Worsens again towards the end of the day because of prolonged weight-bearing activity
- Usually gradual onset
- May be unilateral or bilateral [2]
- On examination, there is tenderness at the calcaneal insertion of the plantar aponeurosis. [1]
Commonly, pain starts after a recent increase in activity. [1]



In patients with plantar fasciitis, tenderness can be elicited by applying pressure over the calcaneal insertion of the plantar aponeurosis (dotted circle).
© AMBOSS
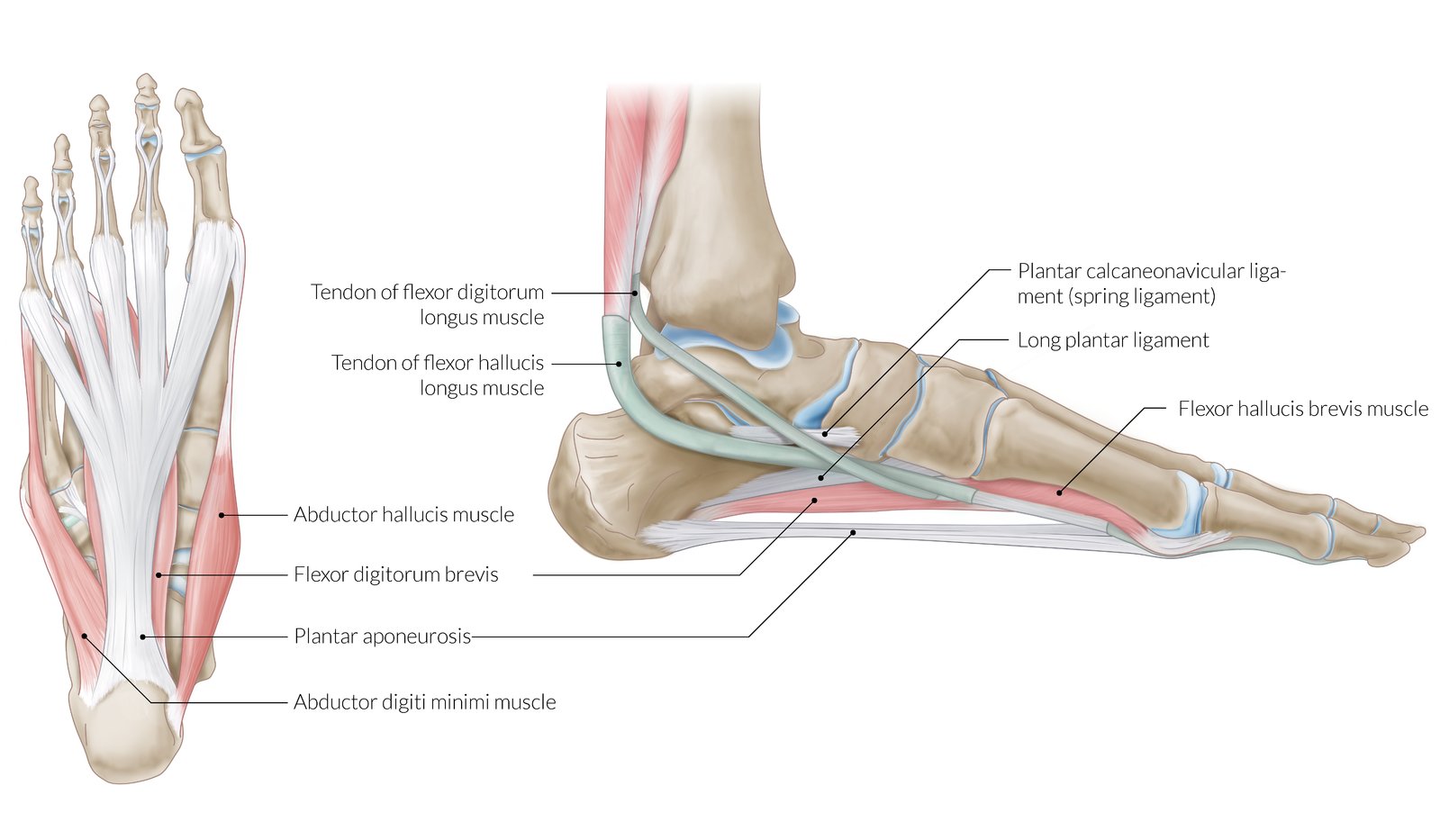
Left: plantar view; right: medial view
The plantar aponeurosis is the thickened deep fascia of the sole of the foot. It arises from the calcaneum and splits into 5 slips that are attached to the plantar aspect of the proximal phalanges of the toes. The plantar aponeurosis provides attachment to some of the intrinsic muscles of the foot, protects the deep plantar vessels from compression, and helps maintain the longitudinal arches of the foot.
The medial longitudinal arch of the foot is formed by the calcaneus, talus, navicular, 3 cuneiforms, and medial 3 metatarsals, and supported by the flexor digitorum longus, flexor hallucis longus, and intrinsic muscles of the foot, as well as the fibularis longus and the tibialis anterior and posterior (not shown here). The arches of the foot help distribute body weight and act as shock absorbers when running or walking.
© AMBOSS
Diagnosis
General principles [1][3]
- Diagnosis is usually clinical.
- Provocative tests such as the windlass test may be helpful in the diagnosis.
- Consider imaging in diagnostic uncertainty or refractory pain.
Fever, polyarthralgia, inability to bear weight, paresthesia, and/or numbness suggest differential diagnoses of plantar fasciitis and usually require further evaluation with laboratory studies and/or imaging. [1]
Provocative tests
- Performing the windlass test can aid in the diagnosis of plantar fasciitis. [4]
- The patient is asked to stand on a step stool with the toes overhanging the edge.
- The great toe is then passively dorsiflexed.
- The result is positive if pain is reproduced over the calcaneal insertion of the plantar aponeurosis.
- High specificity (100%) but low sensitivity (32%) for plantar fasciitis. [1]

Imaging [3][5]
-
Indications
- To rule out differential diagnoses of plantar fasciitis
- Worsening or atypical symptoms
- Persistent symptoms after 3–6 months of conservative management [1]
-
Modalities
- First-line: x-ray foot (weight-bearing) [5]
- Further studies: ultrasound, MRI
-
Findings are usually nonspecific; e.g:
- Bone spurs
- Plantar fascia thickening
- Edema at the insertion of the calcaneus
X-ray is the preferred imaging modality for the initial evaluation of patients with chronic foot pain. If symptoms persist and etiology is unclear, obtain an ultrasound or MRI. [5]



The patient is asked to stand on a step with the toes overhanging (to allow free movement). The great toe is then passively dorsiflexed. Pain that is reproduced over the calcaneal insertion of the plantar aponeurosis (red area) is consistent with plantar fasciitis.
© AMBOSS

X-ray (lateral view)
A bony outgrowth (green overlay) projects from the calcaneal tuberosity at the origin of the plantar fascia.
C: calcaneus
Source: © IMPP

X-ray calcaneus (lateral view)
A large enthesophyte (red overlay) is seen at the insertion of the Achilles tendon along the posterosuperior calcaneus, and another is present (blue overlay) in the region of the origin of the plantar fascia.
Source: “Achilles insertional calcific tendinosis” by Mikael Häggström, Wikimedia Commons, licensed under CC0 1.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
Differential diagnoses
-
Skeletal [1][6]
- Calcaneal stress fracture
- Acute calcaneal fracture
-
Neurologic [1][6]
- Tarsal tunnel syndrome
- Entrapment of the calcaneal nerve (medial or inferior)
- Entrapment of the plantar nerve (medial or lateral)
-
Soft tissue [1][6]
- Achilles tendinopathy
- Heel pad syndrome
- Tenosynovitis
- Plantar fascia rupture
- Retrocalcaneal bursitis
-
Others [1][6]
- Reactive arthritis
- Ankylosing spondylitis
- Gout
- Osteomyelitis
- Malignancy
The differential diagnoses listed here are not exhaustive.
Treatment
Initial management, which should be offered to all patients, improves symptoms in ∼ 80% of patients by 12 months. [1]
Initial management [1][3]
- Reduction of biomechanical stress
- Rest and activity modification
- Avoidance of nonsupportive shoes [3]
- Consideration of external support (e.g., foot taping, orthotic insoles) [1][3]
- Patients with high BMI: obesity management [3]
- Stretching and strengthening exercises specific for the plantar fascia [3]
-
Pain management, which may include:
- NSAIDS
- Corticosteroid injections [1][3]
- Botulin toxin injections [1][7]
Refractory plantar fasciitis [1][3]
Plantar fasciitis may become subacute (lasting 6–12 weeks) or chronic (lasting > 12 weeks) despite initial management; extracorporeal shockwave therapy or surgery may be required. [3]
Extracorporeal shockwave therapy
- Indications: refractory subacute or chronic plantar fasciitis [1][3]
- Techniques [3]
- 3–5 sessions of low-energy treatment (anesthesia not required)
- 1 session of high-energy treatment (sedation required)
Surgery [3]
- Indications: appropriate if no clinical improvement after 6–12 months of nonsurgical management
- Techniques
- Plantar fasciotomy (open or endoscopic)
- If equinus deformity is also present: gastrocnemius release
Treatment should be individualized to the patient's symptoms, lifestyle, and activity levels. [1][3]
There is no evidence for or against acupuncture or injection of autologous blood products (whole blood or platelet-rich plasma) in the treatment of plantar fasciitis; routine use is not currently recommended. [1][3]
External Resources
References
- Trojian T, et al. "Plantar Fasciitis". Am Fam Physician. 99(12). :744-750. (2019)
- Buchbinder R. "Clinical practice. Plantar fasciitis.". N Engl J Med. 350(21). :2159-66. (2004)
- Schneider HP, Baca JM, et al. "American College of Foot and Ankle Surgeons Clinical Consensus Statement: Diagnosis and Treatment of Adult Acquired Infracalcaneal Heel Pain". J Foot Ankle Surg. 57(2). :370-381. (2018)
- De Garceau D, Dean D, Requejo SM, Thordarson DB. "The Association between Diagnosis of Plantar Fasciitis and Windlass Test Results". Foot Ankle Int. 24(3). :251-255. (2003)
- Tafur M, Bencardino JT, Roberts CC, et al. "ACR Appropriateness Criteria® Chronic Foot Pain". J Am Coll Radiol. 17(11S). :S391-S402. (2020)
- Acosta-Olivo C, Simental-Mendía LE, Vilchez-Cavazos F, et al. "Clinical Efficacy of Botulinum Toxin in the Treatment of Plantar Fasciitis: A Systematic Review and Meta-analysis of Randomized Controlled Trials". Arch Phys Med Rehabil. 103(2). :364-371.e2. (2022)
- Tu P. "Heel Pain: Diagnosis and Management". Am Fam Physician. 97(2). :86-93. (2018)