Summary
Pleural effusion is the abnormal accumulation of fluid in the pleural cavity between the lining of the lungs and the thoracic cavity (i.e., the visceral and parietal pleurae). Normally, a small amount of pleural fluid is present, which helps lubricate the pleural cavity and facilitates lung movement within the thoracic space. An imbalance between the oncotic and hydrostatic forces that govern pleural fluid formation and lymphatic drainage can result in excessive fluid accumulation. Fluid that permeates into the pleural cavity through intact pulmonary vessels, e.g., in congestive heart failure (CHF), is called a transudate. Conversely, fluid that escapes into the pleural cavity through lesions in blood and lymph vessels, e.g., due to inflammation or tumors, is called an exudate. Pleural effusion is often diagnosed using chest x-ray and ultrasound, but chest CT may be used for very small effusions. Thoracentesis serves as both a diagnostic and therapeutic procedure: pleural fluid analysis can help identify the underlying cause and excess pleural fluid evacuation can provide symptomatic relief. Treatment of pleural effusion often focuses on treating the underlying condition.
Overview
| Transudative vs exudative pleural effusion [1][2][3] | |||
|---|---|---|---|
| Transudative pleural effusion | Exudative pleural effusion | ||
| Pathophysiology |
|
|
|
| Common causes (See “Etiology of pleural effusion” for details.) |
|
|
|
| Light Criteria | Pleural fluid protein/serum protein ratio |
|
|
| Pleural fluid LDH/serum LDH ratio |
|
|
|
| Pleural fluid LDH |
|
|
|

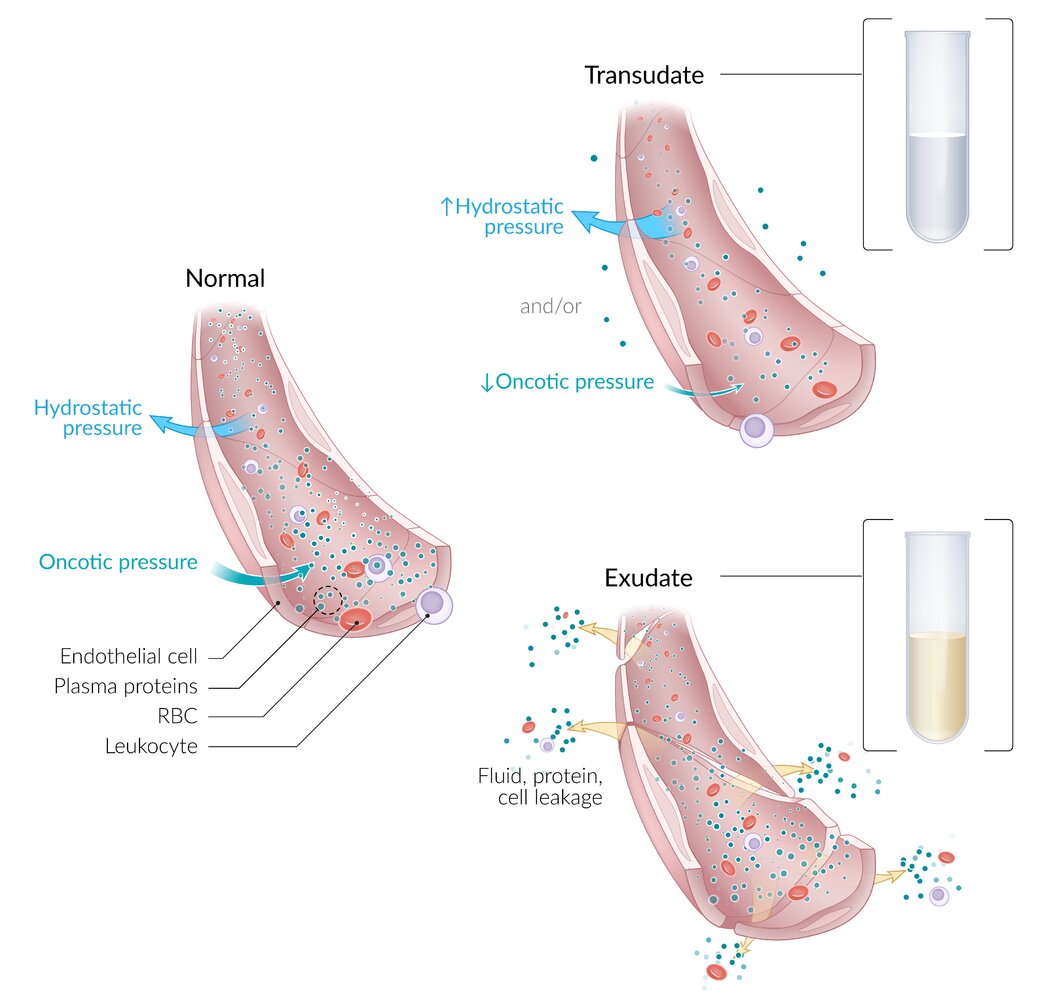
Normal: Capillary hydrostatic pressure (driving fluid out of capillaries) and capillary oncotic pressure (keeping fluid within capillaries) are roughly balanced.
Transudate is extravascular fluid caused by increased capillary hydrostatic pressure (e.g., in congestive heart failure) or decreased capillary oncotic pressure (e.g., in hypoalbuminemia). Transudate has a low protein and cell content and, therefore, tends to be clear.
Exudate is extravascular fluid caused by increased capillary permeability (e.g., secondary to inflammation or malignancy). Exudate has a high protein and cell content and, therefore, tends to be yellow or cloudy.
© AMBOSS
Definitions
An excessive amount of fluid between pleural layers that impairs the expansion of the lungs
Etiology
Transudative effusions [2][3]
- Congestive heart failure
- Hepatic cirrhosis
- Nephrotic syndrome
- Protein-losing enteropathy
- Chronic kidney disease (Na+ retention)
- Rare causes
- Superior vena cava obstruction
- Myxedema
Exudative effusions [2][3]
-
Infection
- Pneumonia (parapneumonic effusion)
- Tuberculosis
- Pleural empyema
- Parasitic illness (e.g., amebiasis, echinococcal disease)
-
Malignancies
- Lung cancer
- Metastatic breast cancer
- Lymphoma
- Mesothelioma
- Ovarian cancer
- Pulmonary embolism (PE)
-
Autoimmune disease (especially collagen vascular diseases)
- Vasculitis
- SLE
- Rheumatoid arthritis
- Sarcoidosis
- Trauma (high vascular permeability)
- Pancreatitis
- Hemothorax
- Chylothorax
- Pseudochylothorax
- Rare causes
- Postcardiac surgery
- Esophageal perforation
- Gynecological causes
- Endometriosis
- Ruptured ectopic pregnancy
- Meigs syndrome
Clinical features
Symptoms [3]
- Patients with a small pleural effusion (< 300 mL) are often asymptomatic.
- Characteristic symptoms
- Dyspnea
- Symptoms of hypoxia
- Pleuritic chest pain (sharp retrosternal pain)
- Dry, nonproductive cough
- Symptoms of the underlying disease (e.g., fever in empyema, cachexia in cases of malignancy, symptoms of left-sided heart failure)
Physical exam findings
- Inspection and palpation
- Asymmetric expansion and unilateral lagging on the affected side
- Reduced tactile fremitus due to fluid in the pleural space
-
Auscultation
- Faint or absent breath sounds over the area of effusion
- Pleural friction rub (squeaking sound of inflamed pleural layers rubbing together during inspiration and expiration)
- Percussion: dullness over the area of effusion




Findings in pneumonia (left) and pleural effusion (right)
Place hands on each side of the thorax, ask the patient to say “toy boat” repeatedly (“ninety-nine” is also commonly used), and feel for vibrations transmitted throughout the chest wall. Vibrations are typically decreased over fluid-filled areas (blue area) and increased over areas of dense consolidation (yellow area).
© AMBOSS
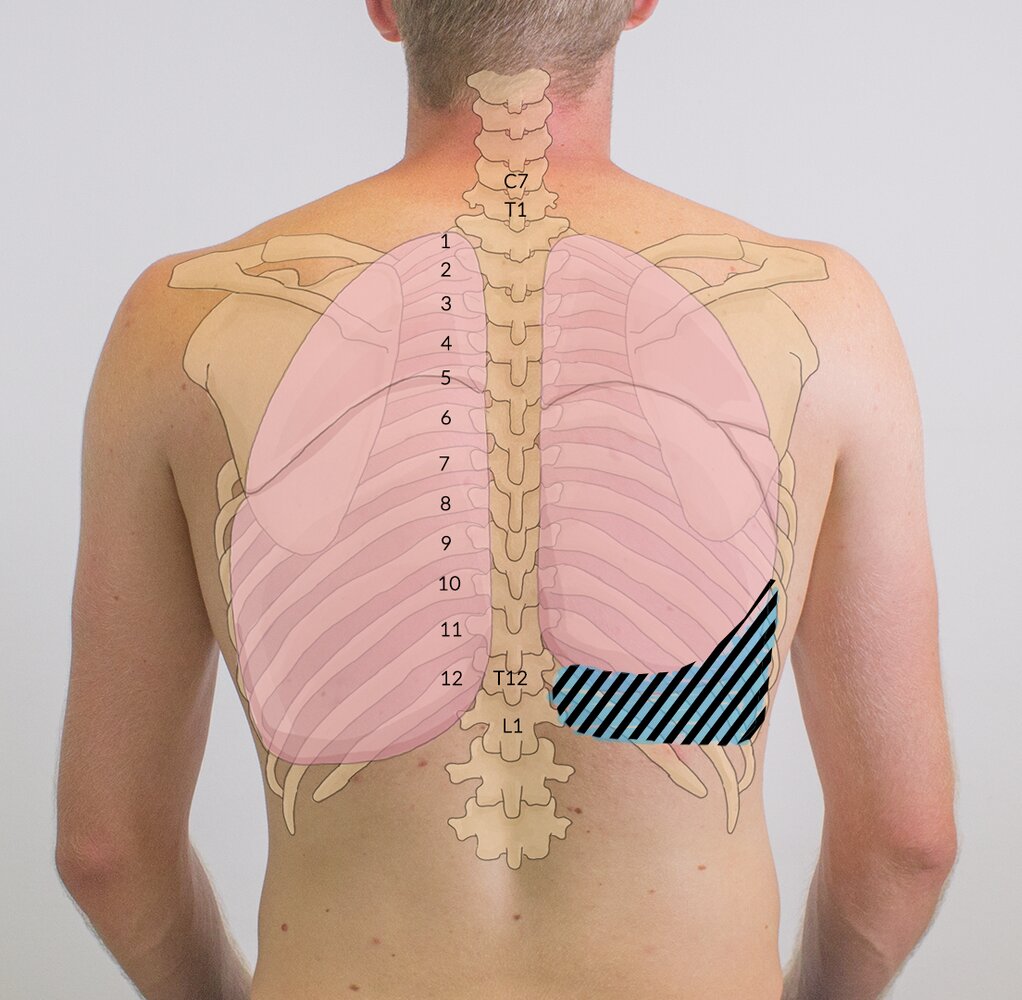
The blue striped area represents pleural effusion in the right lung. On examination, the percussion note would be dull and the breath sounds muffled compared to the other side.
© AMBOSS

© AMBOSS
Diagnosis
Approach
- Imaging is necessary to confirm the diagnosis.
- Consider diagnostic thoracentesis if the diagnosis is uncertain or management requires additional information (e.g., culture, cytology).
- Consider additional diagnostic procedures (e.g., bronchoscopy, VATS) if the diagnosis remains unclear.
Chest x-ray for pleural effusion [4][5]
-
Indications
- Standard initial imaging modality for detecting pleural effusion.
- Lateral decubitus view (most sensitive): allows for detection of fluid collections as small as 5 mL [6]
-
Supportive findings
- Typically unilateral blunting of the costophrenic angle
- Homogeneous density with a meniscus-shaped margin (meniscus sign)
-
Large effusion
- Complete opacification of the lung
- Mediastinal shift
- Tracheal deviation away from the effusion (space-occupying lesion)
- Disease-specific signs: See “Pleural empyema”, “Lung cancer”, “Active primary tuberculosis”, "Pneumonia diagnostics”, and “Pneumothorax.”
Supine CXR has poor sensitivity for pleural effusions, and effusions < 200 mL may not be visible on frontal upright CXR. Include lateral upright and lateral decubitus views whenever possible when obtaining radiographs. [3][4][6]
False positives for pleural effusions on CXR include elevated hemidiaphragm, atelectasis, consolidation, mass lesions.

")
")


Thoracic ultrasound for pleural effusion [4][7]
-
Indications
- Quick bedside assessment
- Thoracentesis planning
- Procedure: See; “Lung POCUS” and “eFAST.”
-
Ultrasound findings suggestive of pleural effusion: hypoechoic or anechoic collection in the lower margins of the pleural cavity (costodiaphragmatic recess)
- Very sensitive: can detect fluid amounts as low as 20 mL
- Hemothorax and empyema may appear heterogeneous.
- Pleural fluid septations may be present.
- Allows for detection of pleural thickening and pleural nodules
Thoracic ultrasound is more sensitive than chest x-ray for diagnosing effusions and estimating effusion size. [8]
False positives on ultrasound can result if the following are mistaken for pleural fluid: subdiaphragmatic fluid (e.g., ascites), pericardial fluid, contained fluid (e.g., hypoechoic masses, abscesses), or pleural thickening. False negatives may result if clotted blood or empyema fluid is mistaken for normal lung or liver tissue. [9]




Chest CT [4][7]
-
Indications: gold standard ; for small effusions but use is limited because of radiation and contrast exposure
- Guiding placement of indwelling pleural catheters
- Directed thoracentesis of a loculated effusion
- Suspected parenchymal or pleural pathology
- Better quantification of the amount of fluid (compared to CXR) is desired
-
Procedure: chest CT without IV contrast is usually sufficient
- With IV contrast: allows for the detection of underlying malignancy (e.g., metastases and/or primary tumor)
- CT angiogram: helps to identify vascular pathology (e.g., dissection or AVM)
-
Supportive findings
- Can detect > 3–5 mL of fluid
- Fluid density measurement can help differentiate pleural effusion from empyema and hemothorax [10]
- Disease-specific signs: See “Pleural empyema.”




Diagnostic thoracentesis [3][11]
Can be combined with therapeutic thoracentesis if both are indicated. See “Thoracentesis” for detailed indications, contraindications, procedural steps, and complications.
- Goal: obtain samples for pleural fluid analysis, e.g., to differentiate transudates from exudates, and identify the underlying cause of pleural effusion
- Indications: include new unilateral pleural effusions and bilateral effusions with atypical features (e.g., fever, chest pain, variable size).
-
Routine pleural fluid studies
- Biochemistry: protein, LDH, pH, and glucose
- Gram stain and culture
- Cytology
- Serum studies (for comparison): serum protein, LDH, pH, and glucose
-
Advanced pleural fluid studies (case by case)
- Cell count
- Lipids: cholesterol, triglycerides
- Amylase, lipase
- TB testing: adenosine deaminase, AFB smear microscopy
- Parasitology
- Tumor markers
- Rheumatological markers
- NT-proBNP
Additional studies [6]
-
Laboratory studies: may be indicated further workup of transudative effusions.
- Elevated serum NT-proBNP: suggests heart failure
- ↑ Liver transaminases, ↓ serum albumin, and abnormal coagulation studies: suggests cirrhosis
- Proteinuria: suggests nephrotic syndrome
- ↑ Serum TSH: suggests hypothyroidism
-
Invasive tests: Consider for patients with inconclusive pleural fluid analysis to rule out malignancy or intracellular infection.
- Bronchoscopy
- Percutaneous needle biopsy
- VATS
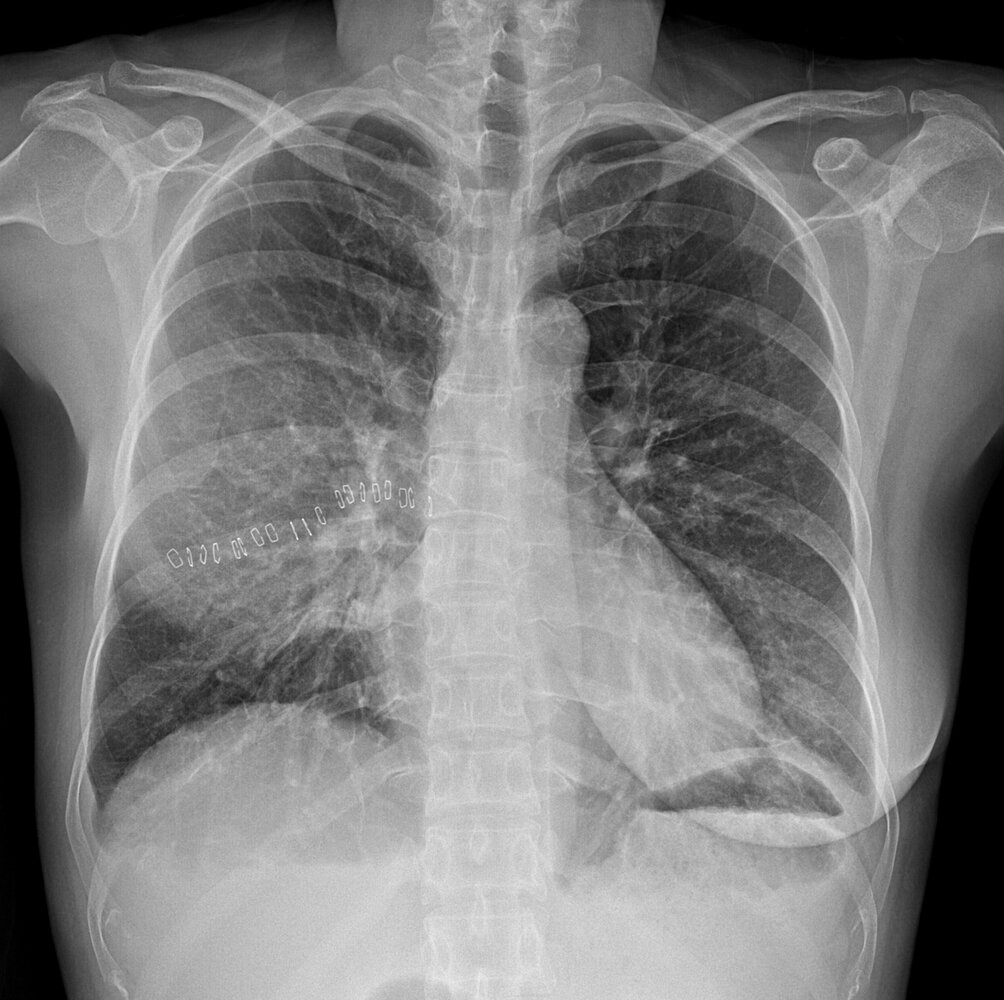
X-ray chest (PA view) of a patient with tamoxifen-induced acute eosinophilic pneumonia
Peribronchial thickening (examples circled in yellow) and linear parenchymal opacities (examples indicated by white lines) are evidence of interstitial lung disease. A small pleural effusion (red line) projects through the right hemidiaphragm and blunts the right lateral costophrenic sulcus. A normal costophrenic sulcus is typically seen as an acutely angled junction between the costal and diaphragmatic pleural reflections (white dashed line).
Right chest wall staples (examples indicated by black overlays) and breast asymmetry (green outline) are the result of a recent mastectomy and reconstruction.
Source: “Fig. 1, In: Tamoxifen-induced acute eosinophilic pneumonia in a breast cancer patient” by Eiyoung Kwon, Mijin Kim, Eunhye Choi, Youngsam Park, Cheolseung Kim, International Journal of Surgery Case Reports, licensed under CC BY 4.0. Modifications: image cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
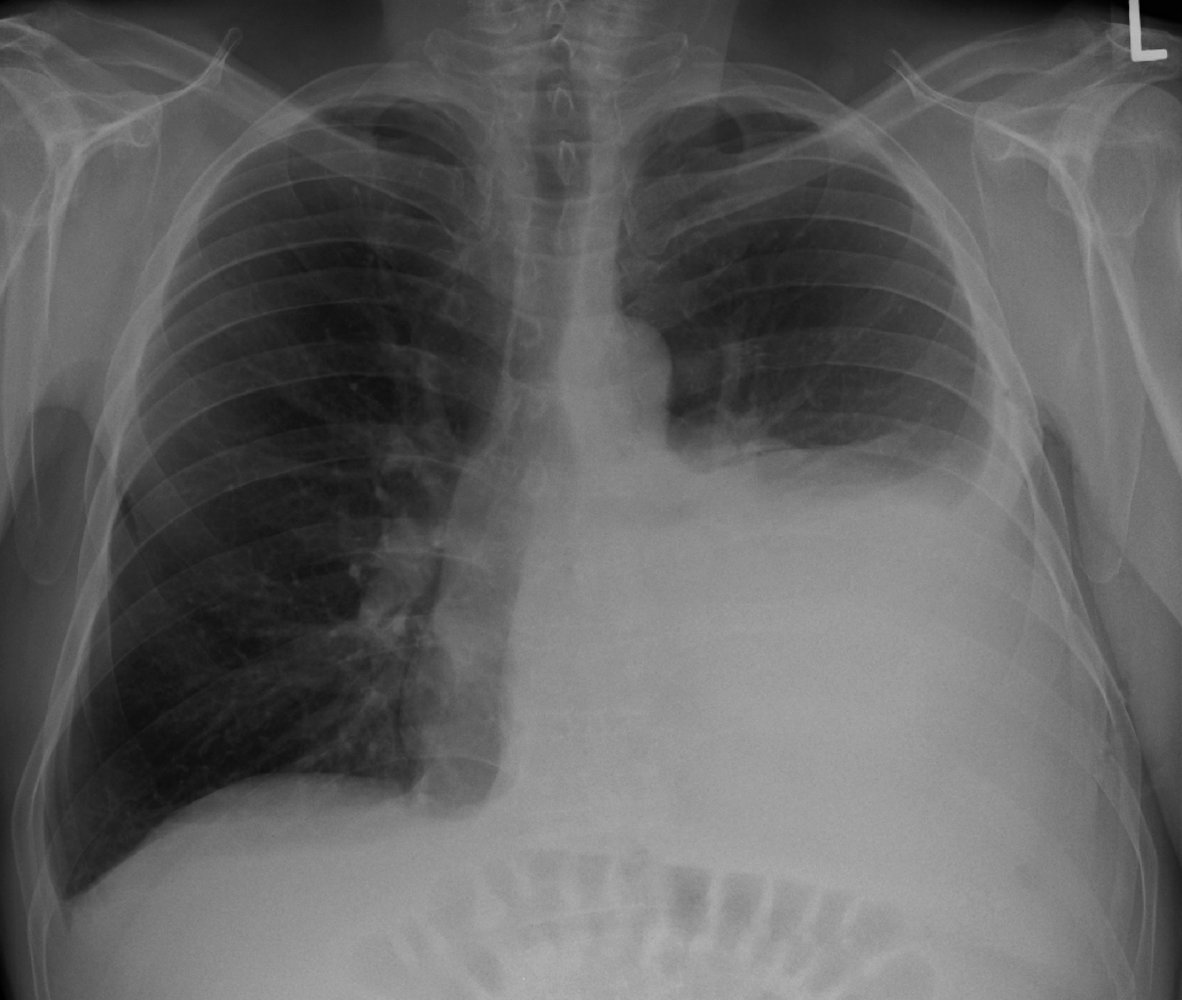
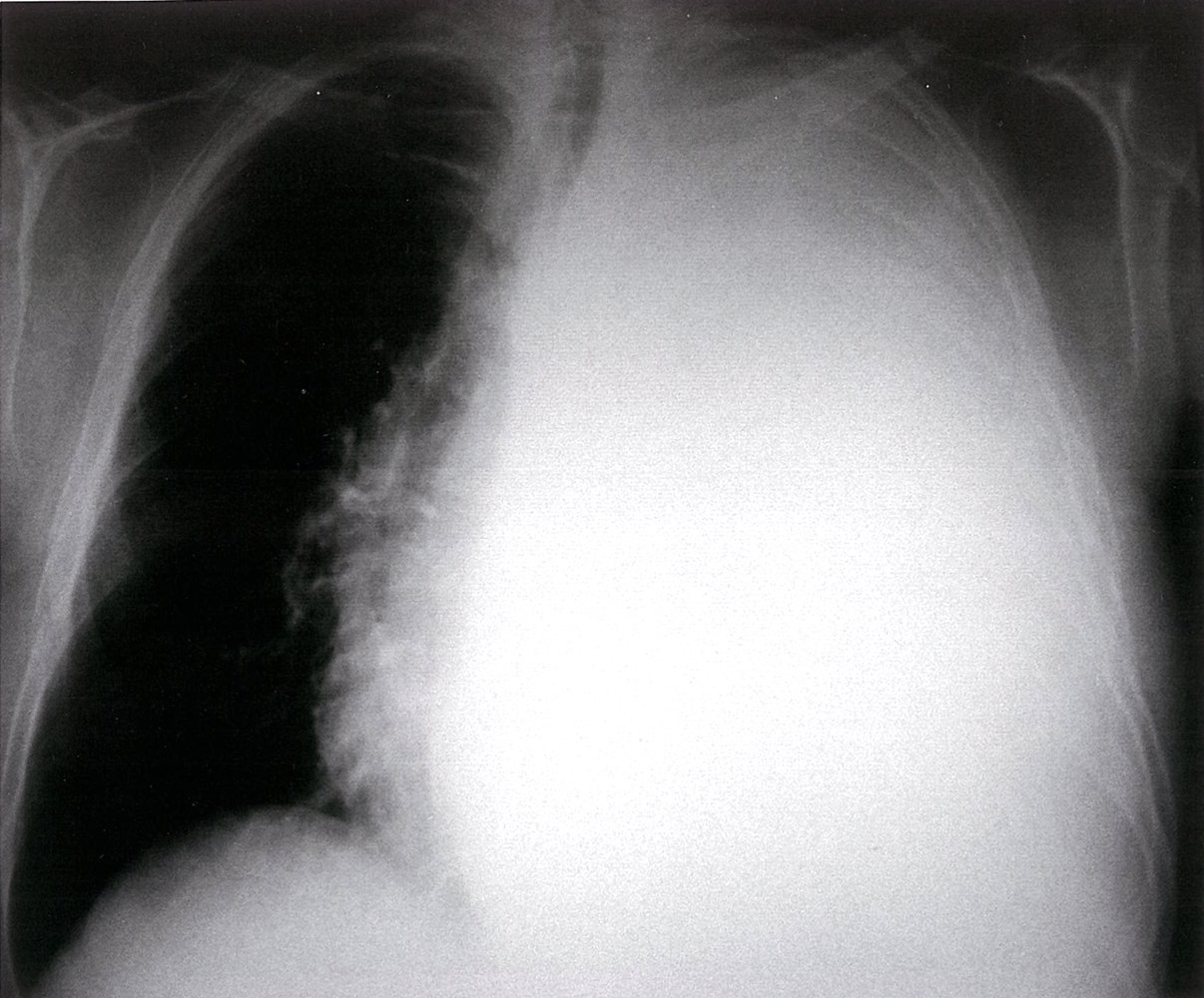
X-ray chest (PA view)
There is marked opacification (green overlay) of the middle and lower left hemithorax from pleural effusion and passive atelectasis of the adjacent lung. No gastric air bubble is seen projecting over the lower left hemithorax to suggest marked elevation of the left hemidiaphragm from a large amount of atelectasis, but concave upper lateral borders, or menisci (white dashed lines), help confirm the presence of effusion extending to the mid thorax.
The margins of the cardiac silhouette and left hemidiaphragm are obscured. Additionally, the cardiac silhouette is shifted slightly to the right (indicated by blue line and arrow) and the left bronchial tree is slightly elevated (indicated by black lines and arrow).
In the right hemithorax, a small meniscus from effusion is seen laterally (indicated by red line). Additionally, increased opacification projects through the right hemidiaphragm indicating effusion in the posterior sulcus (red overlay).
Source: “Effusionhalf” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: removed circle. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
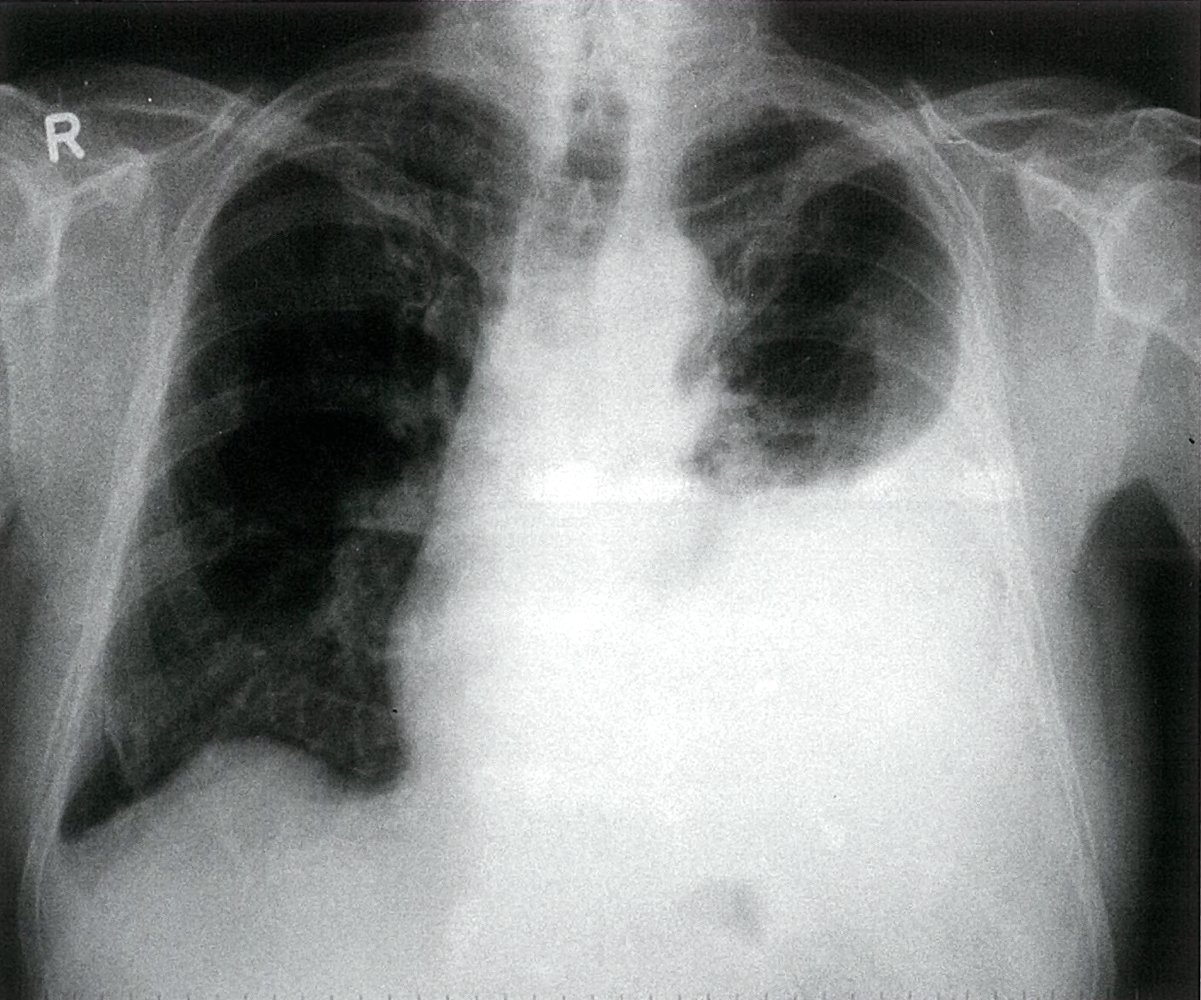
X-ray chest (PA view) of a malignant pleural effusion in a patient with lung cancer
Complete opacification of the left hemithorax (green overlay) is accompanied by mediastinal shift to the contralateral right side (indicated by blue and red lines and arrows). This shift confirms that a space-occupying process, rather than volume loss, is the primary cause of the opacification.
The absence of air in the distal left main bronchus reflects bronchial obstruction and correlates with the patient's clinical history of bronchogenic carcinoma.
T: trachea; Green outline: trachea and main bronchi
Source: © IMPP
X-ray chest (PA view) of a patient with malignant mesothelioma
Marked opacification of the middle and lower left hemithorax (green overlay) is accompanied by menisci that indicate the presence of a pleural effusion. There is no appreciable ipsilateral or contralateral mediastinal shift. Non-dependent pleural thickening at the left apex (red overlay) is more conspicuous on the lateral radiograph.
A meniscus from a small right pleural effusion (yellow overlay) is also visible.
Source: © IMPP

X-ray chest (lateral view) of a patient with malignant mesothelioma
Opacification of the middle and lower left hemithorax is accompanied by a meniscus that indicates the presence of a pleural effusion (green overlay). Also visible is pleural thickening (red overlay) encompassing the upper left hemithorax.
Source: © IMPP
Short video of an ultrasound examination of the lower left hemithorax (a marker indicates the probe position) showing pleural effusion
An anechoic pleural effusion (blue overlay) is visible in the costodiaphragmatic recess (costophrenic sulcus) near the middle of the video. On the left side of the video, aerated lung is visible. Since ultrasound waves are not transmitted through normal aerated lung, the lung is recognized by to and fro movement of the hyperechoic pleural line (green overlay) during respiration and the presence of horizontal lines (A-lines; reverberation artifact; yellow overlay) deep to the pleural line.
A pleural effusion (collection of fluid in the pleural space between the lungs and the chest wall) is a pathological finding.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
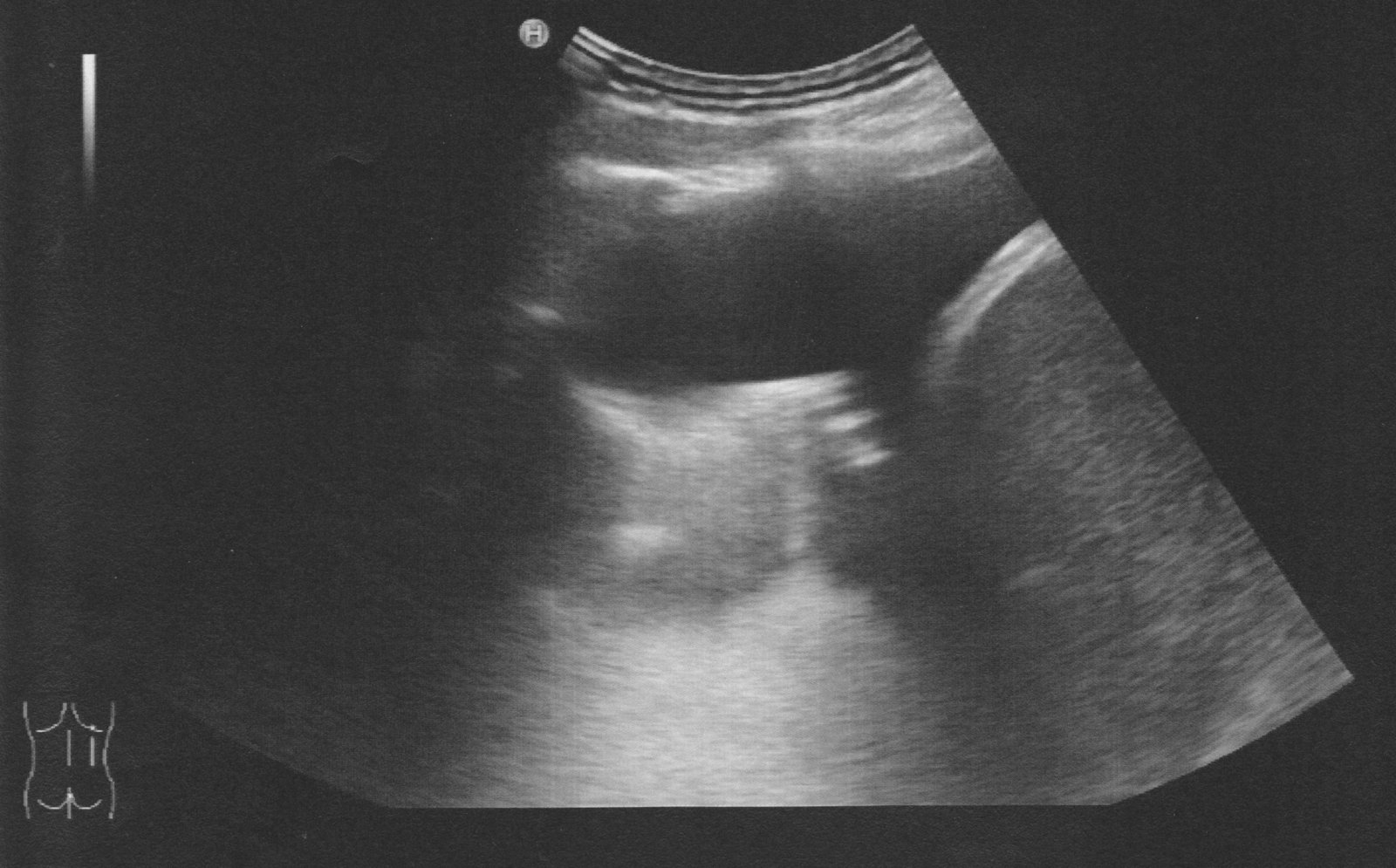
Ultrasound chest (posterior right hemithorax)
Anechoic fluid (green overlay; F) is visible in the costodiaphragmatic recess between the right hemidiaphragm (D) and atelectatic lung (Lu).
Li: liver
© AMBOSS
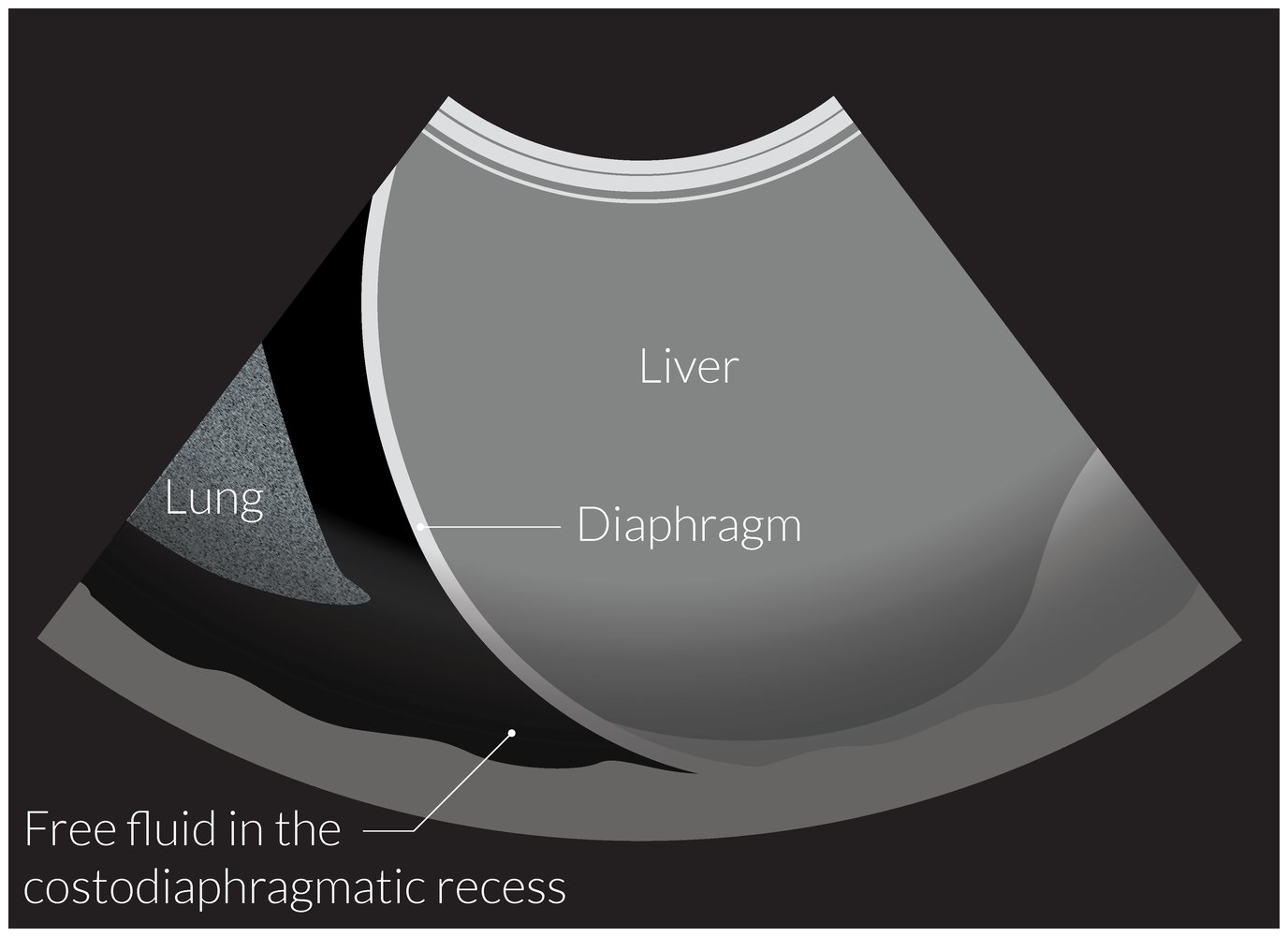
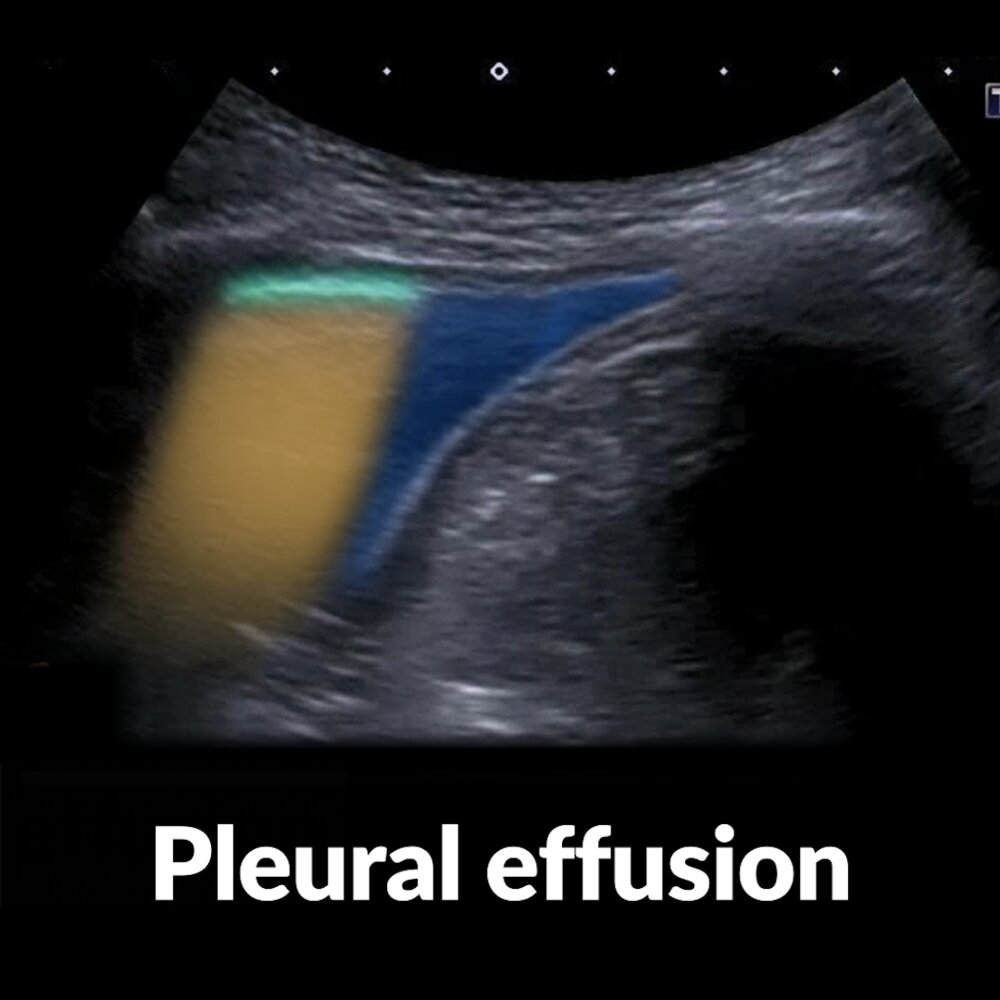
Illustration of an ultrasound of the right costodiaphragmatic recess
In the upright position, the costodiaphragmatic recess is the lowest dependent site of the pleural cavity. Therefore, it is the earliest site of fluid accumulation in the case of a pleural effusion or hemothorax, which both appear as an anechoic or hypoechoic space between the lung and the diaphragm on ultrasound, as depicted here.
© AMBOSS

Illustration of an ultrasound of the left costodiaphragmatic recess
In the upright position, the costodiaphragmatic recess is the lowest dependent site of the pleural cavity. Therefore, it is the earliest site of fluid accumulation in patients with pleural effusion or hemothorax, which both appear as an anechoic or hypoechoic space between the lung and the diaphragm on ultrasound, as depicted here.
© AMBOSS
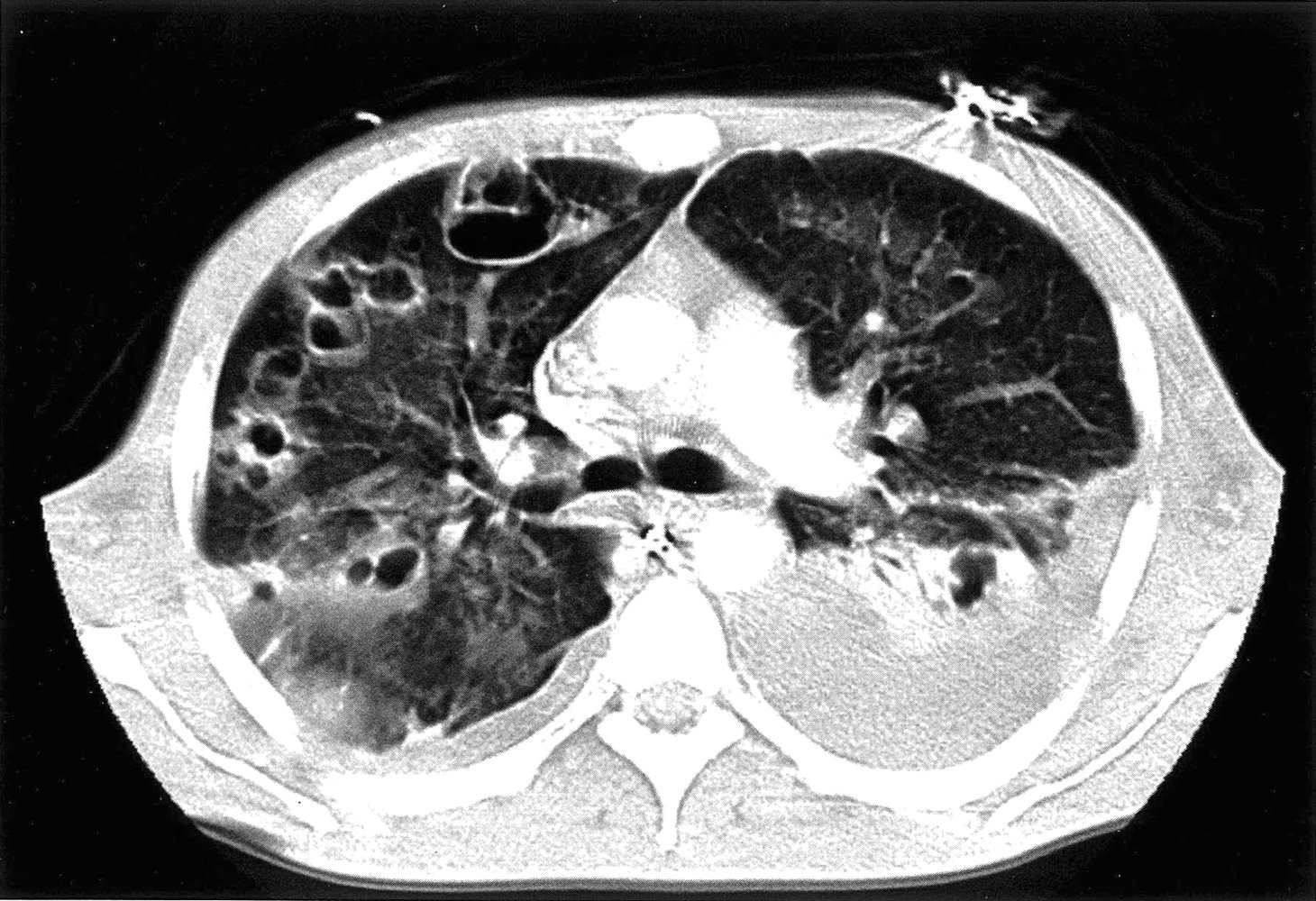
CT chest (with contrast; axial plane; lung window)
Multiple cavitary lesions (examples indicated by green overlay) are present in the lungs. Bilateral pleural effusions (red overlay) are present, and passive atelectasis (yellow overlay) in the left lower lobe is visible adjacent to the left effusion.
The differential for multiple cavitary lesions is broad and includes various infectious (septic emboli and mycobacterial, fungal, and parasitic organisms), malignant, and autoimmune conditions.
Source: © IMPP
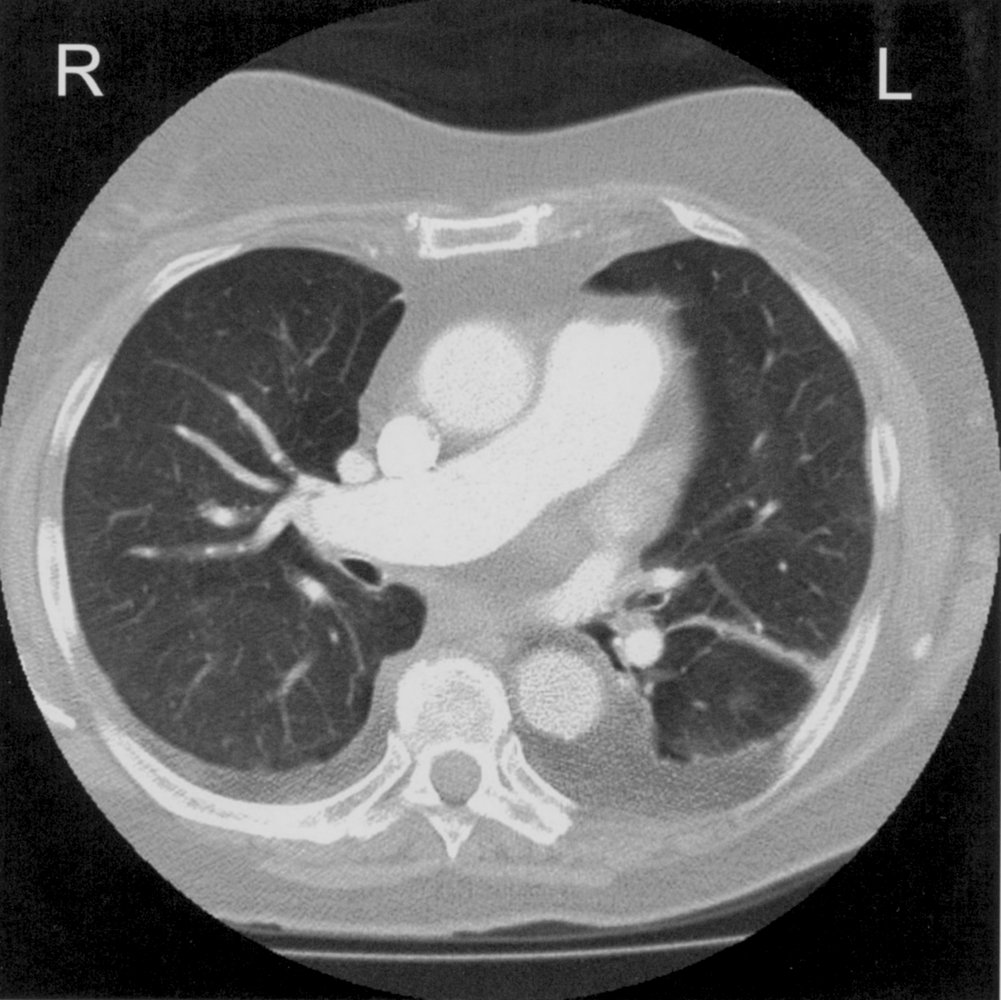
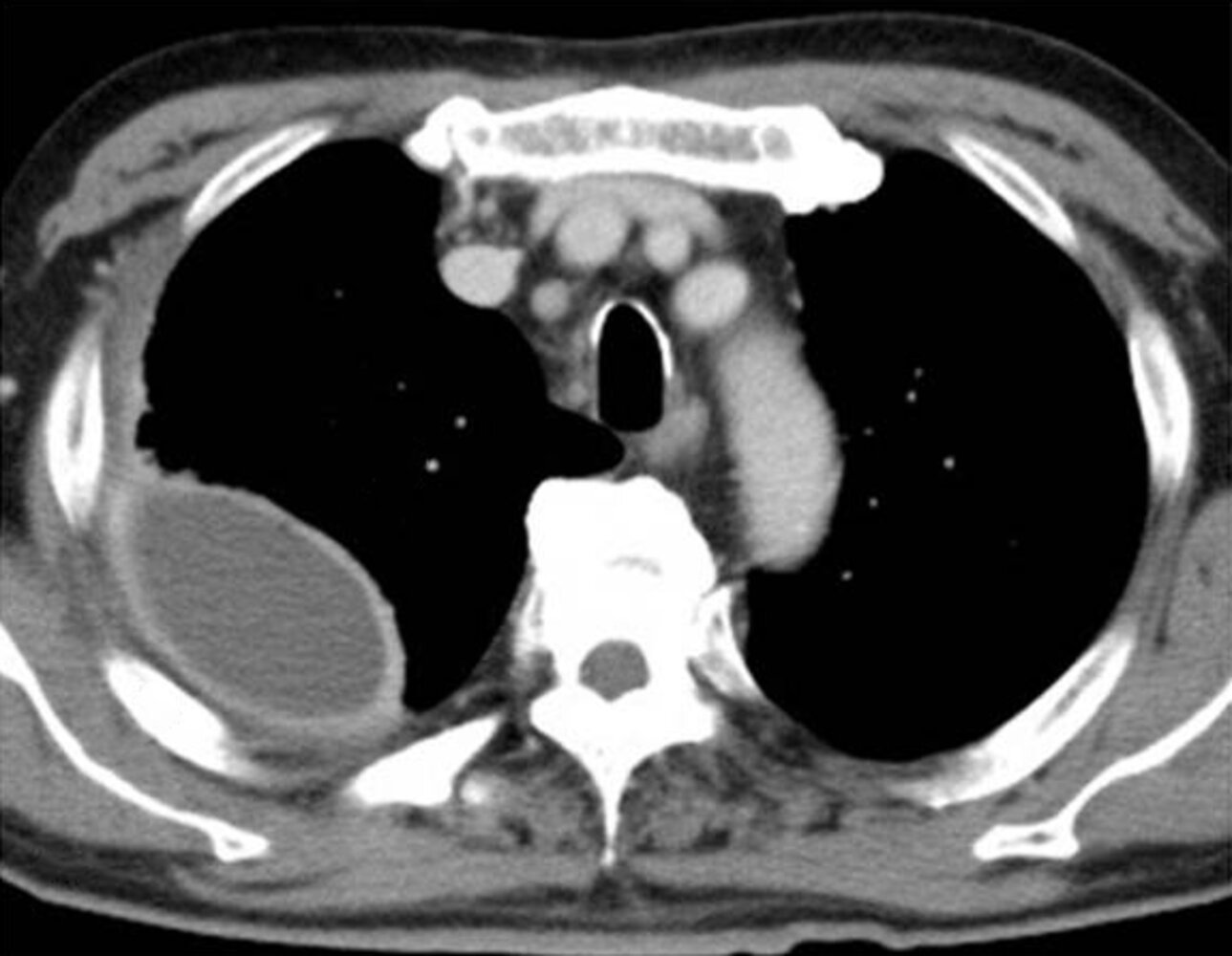
Chest CT with contrast (axial view; approx. at the level of T5)
Bilateral crescent-shaped attenuated areas (green overlay) are visible.
These findings are typical of pleural effusion.
AA = ascending aorta; DA = descending aorta; PT = pulmonary trunk, Vc = superior vena cava; PA = right pulmonary artery, V = vertebra
Source: © IMPP
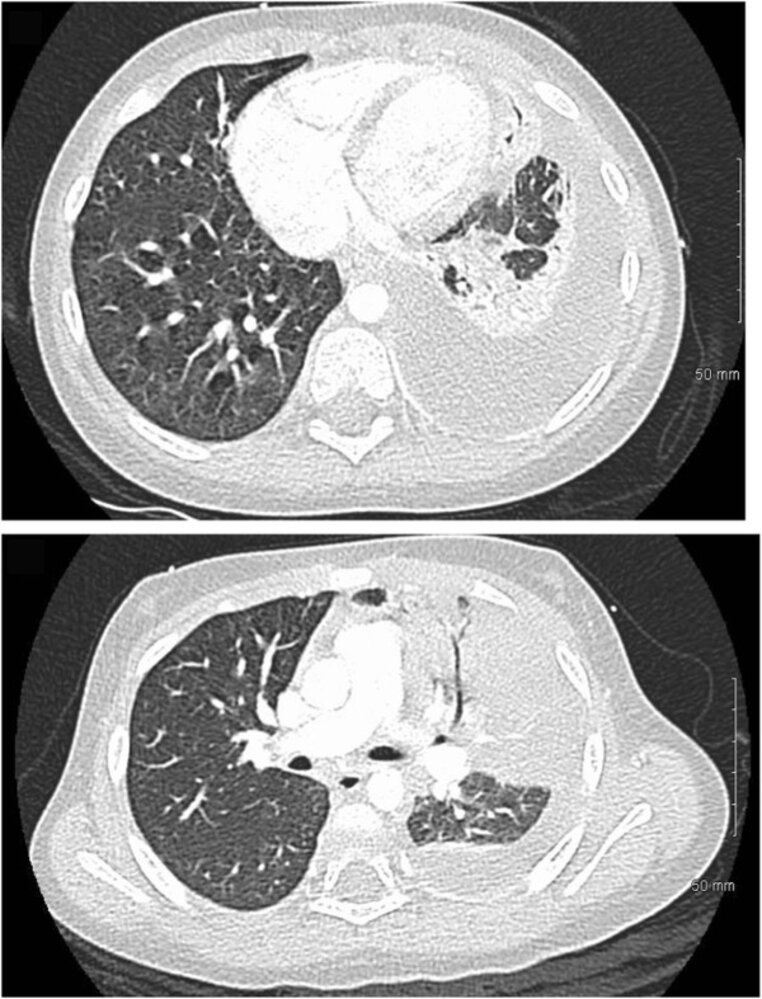
CT chest (with contrast; axial plane; lung window) of a patient with pneumonia
Air bronchograms (example indicated by arrow) are present within dense consolidation (green overlay) involving the left upper lobe. Passive left lower lobe atelectasis (A) is present adjacent to the accompanying pleural effusion (red overlay).
H: heart; PA: pulmonary artery
Source: “Images of CT scan of chest obtained from 2 year old child with empyema” by Elsa L Vazquez Melendez, John J Farrell, Andrea M Hujer et al., BMC Anesthesiology, licensed under CC BY 4.0. Modifications: Deleted A and B from original image. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
CT chest (with contrast; axial plane; mediastinal window)
CT scan shows right-sided pleural fluid collection (PC). The collection has a lenticular (biconvex) shape and is accompanied by thickening of the adjacent parietal (red line) and visceral pleurae (green line).
The split-pleura sign refers to thickening and contrast enhancement of the parietal and visceral pleurae separated by empyema or exudative effusion. The sign is the result of a fibrin pleural coat with capillary ingrowth and is considered reliable in distinguishing empyema from lung abscess. Lung abscesses, furthermore, tend to be round in contrast to the lenticular shape typical of empyemas.
T: trachea
Source: “Fig 2C, In: A Simple Method for Differentiating Complicated Parapneumonic Effusion/Empyema from Parapneumonic Effusion Using the Split Pleura Sign and the Amount of Pleural Effusion on Thoracic CT” by Tsujimoto N, Saraya T, Light RW et al., PLOS ONE, licensed under CC BY 4.0. Modifications: - original edit - letter removed - arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Pleural fluid analysis
Differentiating transudates from exudates [3][6][7][12][13]
| Primary pleural fluid analysis | |||
|---|---|---|---|
| Laboratory parameters | Transudative effusion | Exudative effusion | |
| Light criteria | Pleural fluid protein/serum protein ratio |
|
|
| Pleural fluid LDH/serum LDH ratio |
|
|
|
| Pleural fluid LDH |
|
|
|
| Pleural fluid cholesterol |
|
|
|
| Pleural fluid LDH |
|
|
|
| Pleural fluid cholesterol:serum cholesterol ratio |
|
|
|
Light criteria are useful for ruling out an exudate if all criteria are assessed as the sensitivity is high. They are less reliable for ruling in an exudate as the specificity is poor and can misclassify ∼ 25% of transudates as exudates. Interpret results taking the full clinical picture into account. [6][14]
| Adjunctive pleural fluid analysis [3][7][13] | |||
|---|---|---|---|
| Pleural fluid parameter | Suggests transudative effusion | Suggests exudative effusion | |
| Physical appearance |
|
|
|
| Specific gravity |
|
|
|
| pH Normal pH ∼ 7.6 |
|
|
|
| Glucose |
|
|
|
| Total protein gradient (i.e., the difference between pleural fluid and serum total protein) |
|
|
|
| Albumin gradient |
|
|
|
Narrowing the differential diagnosis of exudative effusions [3][7][13]
| Differential diagnosis of exudative effusions | ||
|---|---|---|
| Pleural fluid parameter | Associated conditions [2][11][15] | |
| Cell count and differential | WBC count > 10,000/mm3 |
|
| Neutrophils > 50% of total leukocytes |
|
|
| Lymphocytes > 50% of total leukocytes |
|
|
| RBC count > 5,000/mm3 |
|
|
| Hematocrit > 0.5 × peripheral hematocrit |
|
|
| pH < 7.2 [15] |
|
|
| Glucose < 60 mg/dL |
|
|
| Positive Gram stain or culture |
|
|
| Adenosine deaminase > 50 IU/L Positive AFB smear microscopy |
|
|
| Abnormal cytology |
|
|
| Amylase > 200 IU/L |
|
|
| Positive rheumatoid factor, ANA |
|
|
| Lipids | Triglycerides > 110 mg/dL |
|
| Total cholesterol > 200 mg/dL Total cholesterol:triglyceride ratio > 1 Cholesterol crystals |
|
|
| Total cholesterol 55–200 mg/dL Chylomicrons and fat-soluble vitamins |
|
|
| Appearance | Cloudy, milky |
|
| Purulent |
|
|
| Bloody |
|
|
Transudate is usually clear, has a decreased cell count, and has low levels of protein, albumin, and LDH. Exudate typically appears cloudy, has an increased cell count, and has high levels of protein, albumin, and LDH.
MEAT has low glucose: Malignancy, Empyema, Arthritis (rheumatoid pleurisy), and Tuberculosis are causes of pulmonary effusion associated with low glucose levels.
Pleural fluid with a bloody appearance suggests a malignant etiology or hemothorax!



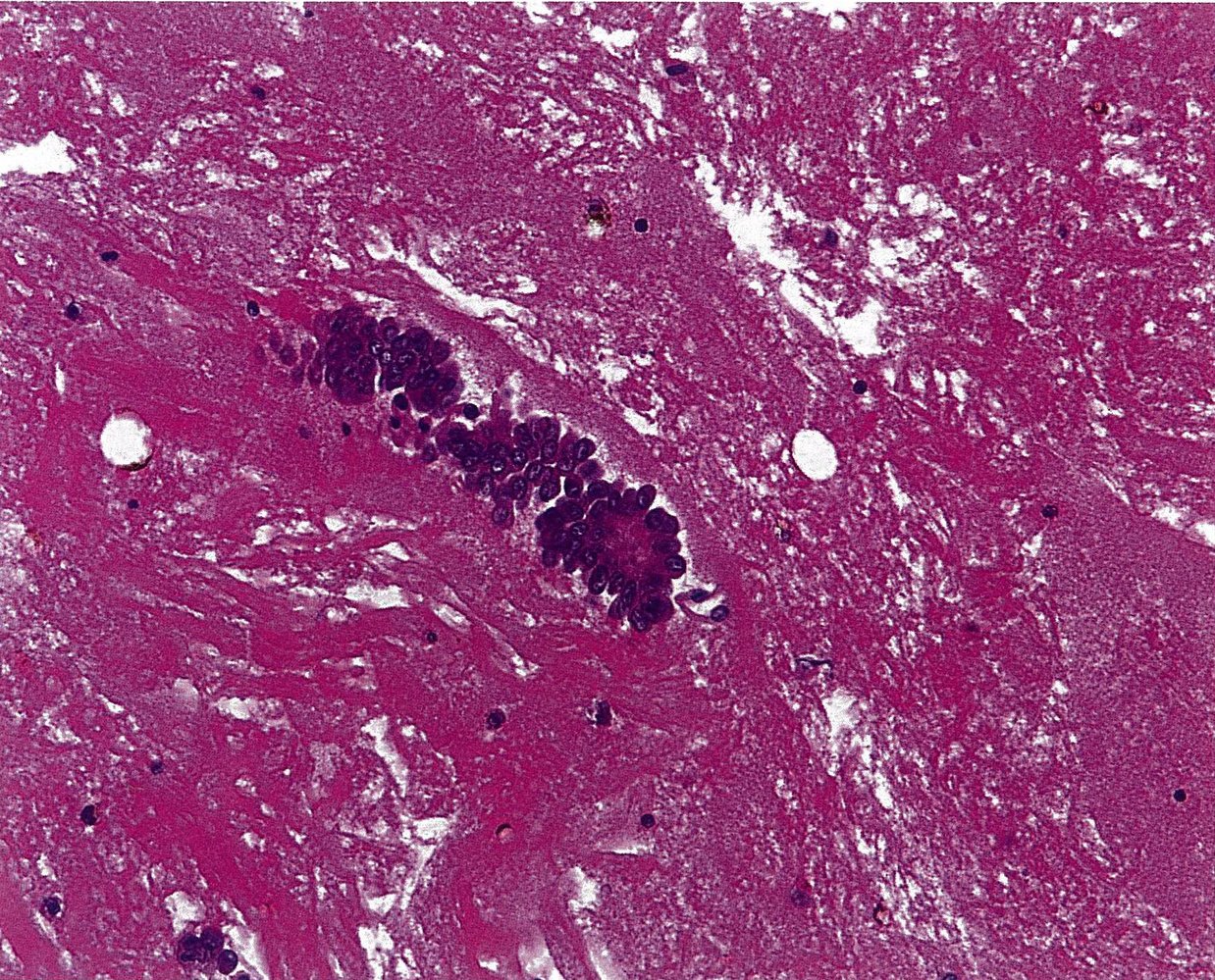
Photomicrograph of pleural fluid cytology specimen (H&E stain; unknown magnification)
Cells are clustered in dense groups and show marked pleomorphism (variability). Some cells show a pronounced shift in the nuclear-cytoplasm ratio and prominent nucleoli.
These findings are typical of malignant pleural effusion.
Source: © IMPP
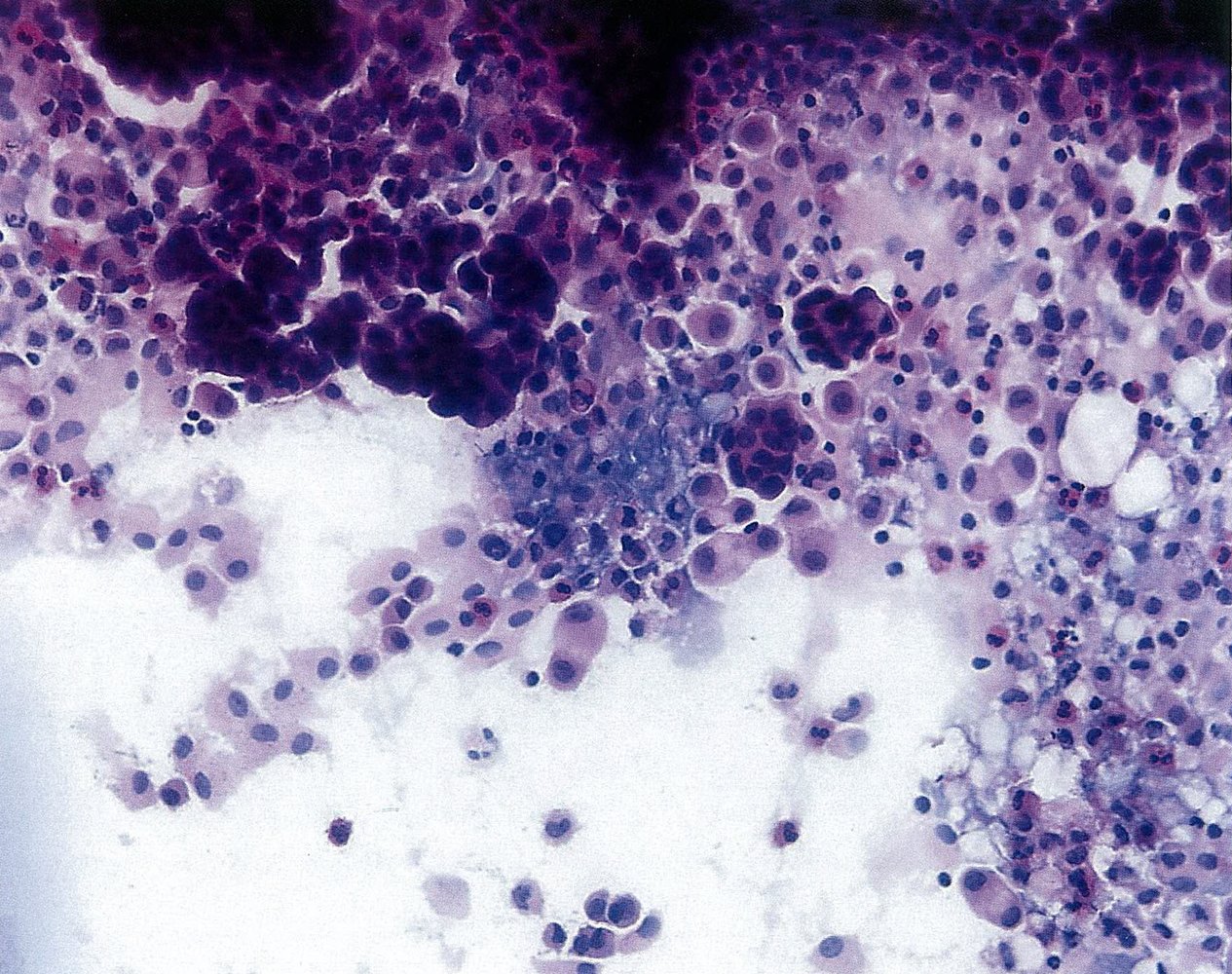
Photomicrograph of a pleural fluid cytology specimen (H&E stain; unknown magnification)
Cells are clustered in dense groups and show marked pleomorphism (variability). Some cells show a pronounced shift in the nuclear-cytoplasm ratio and prominent nucleoli.
These findings are typical of malignant pleural effusion.
Source: © IMPP
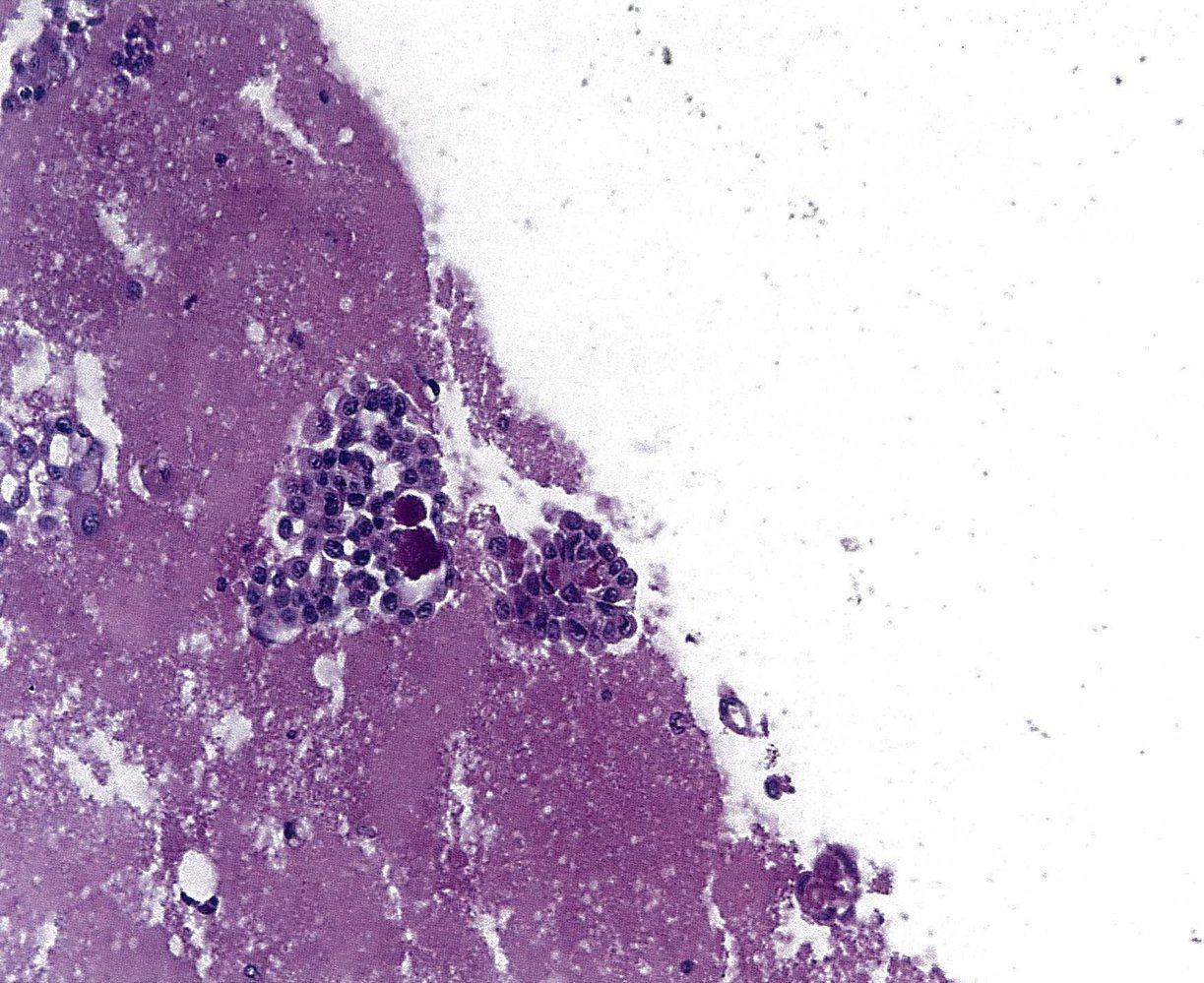
Photomicrograph of pleural fluid cytology specimen (H&E stain; unknown magnification)
Cells are clustered in dense groups and show marked pleomorphism (variability). Some cells show a pronounced shift in the nuclear-cytoplasm ratio and prominent nucleoli.
These findings are typical of malignant pleural effusion.
Source: © IMPP
Differential diagnoses
-
Lung densities on imaging
- Lung mass, e.g., bronchial carcinoma, lung metastasis
- Pneumonia
- Interstitial lung disease
- Atelectasis
-
Pleural densities on imaging
- Metastatic disease
- Pleural fibrosis or scarring
- Pleural mesothelioma
-
Other mimics
- Subphrenic abscess
- Pneumothorax
- Diaphragmatic hernia [16]
The differential diagnoses listed here are not exhaustive.
Management
Approach [6][11][15]
-
Unstable patients: e.g., respiratory distress, respiratory failure, or hemodynamic instability.
- Begin respiratory support.
- Perform urgent therapeutic thoracentesis.
-
All patients
- Identify and treat the underlying condition (see “Treatment of pleural effusion”).
- Consider elective therapeutic thoracentesis based on individual risk-benefit ratios.
- Consider specialized procedures and/or surgical therapy after specialty consultation.
Identify and treat life-threatening causes of pleural effusion, e.g., pulmonary embolism, esophageal rupture, and hemothorax.
Stabilization
-
ABCDE survey
- Oxygen therapy, mechanical ventilation, and immediate hemodynamic support as needed
- Emergency blood transfusion for massive hemothorax [17]
- Portable upright CXR or lung ultrasound to evaluate effusion size
-
Urgent therapeutic thoracentesis indications
- Respiratory distress signs
- Hemodynamic compromise secondary to the effusion
-
Management of life-threatening conditions
- Esophageal rupture: Consult surgery and start empiric antibiotics.
- Sepsis: Begin sepsis management.
- Acute heart failure: Begin AHF management.
Next steps
-
Clinical improvement (life-threatening causes ruled out)
- Continue detailed clinical evaluation.
- Obtain additional diagnostics for pleural effusion (e.g., CT chest, diagnostic thoracentesis).
-
Clinical deterioration
- Optimize oxygenation in mechanically ventilated patients
- Consult a specialist for admission (e.g., critical care) and complicated pleural fluid drainage (e.g., pulmonology, interventional radiology, and/or thoracic surgery)
Disposition [4][18]
Unstable patients
- ICU admission
- Consider immediate OR transfer for massive hemothorax.
Stable patients
- Consider admission for: [19][20]
- Parapneumonic effusion or empyema
- Underlying disease requiring inpatient treatment
- Large effusion of unknown etiology
- Consider observation and discharge after successful therapeutic thoracentesis in patients with a known and stable underlying condition and no complications.
- If thoracentesis is not indicated, consider discharge if all of the following are present:
- Known and self-limited etiology of pleural effusion (e.g., recent abdominal surgery)
- No signs of respiratory distress
- Ability to adhere to discharge instructions and follow-up
Acute management checklist
- Provide supplemental oxygen as needed.
- If respiratory distress, respiratory failure, or hemodynamic instability is present, perform urgent therapeutic thoracentesis and consult ICU.
- Consider continuous cardiac monitoring and pulse oximetry.
- Obtain confirmatory imaging: e.g., CXR (upright PA and lateral, or lateral decubitus), lung ultrasound, CT chest.
- Obtain CBC, coagulation panel, serum protein, and LDH. .
- Correct coagulopathy if present.
- Perform diagnostic thoracentesis and pleural fluid analysis if new effusion or etiology is uncertain.
- Routine studies: glucose, LDH, protein, cholesterol, and pH.
- Consider additional studies depending on patient history and the suspected etiology: AFB smear microscopy, adenosine deaminase, amylase/lipase, rheumatoid factor, ANA, cytology, immunohistochemistry, Gram stain plus culture
- Repeat CXR after thoracentesis.
- Identify and treat the underlying cause (see “Pleural fluid analysis” and “Common causes of pleural effusion”).
- If empyema is suspected, administer empiric IV antimicrobial therapy for pleural infection.
- Consider elective therapeutic thoracentesis for large symptomatic effusions and complicated parapneumonic effusions.
- Monitor for re-expansion pulmonary edema if therapeutic thoracentesis is performed.
- Consider other types of pleural fluid drainage on an individual basis depending on etiology and recurrence risk after specialty constulation, e.g., indwelling pleural catheter, tube thoracostomy, or surgery.
- Consult thoracic surgery for chest tube insertion and/or surgery for suspected empyema and/or hemothorax.
Treatment
Treatment of the underlying cause [6]
- Acute congestive heart failure: loop diuretics (see “Treatment of heart failure”)
- Collagen vascular diseases: steroids (see “Systemic lupus erythematosus” and “Rheumatoid arthritis”)
- Pancreatitis: See “Treatment of acute pancreatitis.”
- Pancreaticopleural fistula: Endoscopic or surgical intervention is recommended. [21][22][23]
- Meigs syndrome: Removal of the ovarian tumor is recommended.
- Other malignancy: targeted cancer immunotherapy, chemotherapy, radiotherapy, or surgical resection
Consider pulmonary embolism as a potential cause of unexplained effusion; anticoagulation therapy may be initiated even in the presence of blood-tinged pleural effusion. [24]
Therapeutic thoracentesis [11]
See “Thoracentesis” for detailed indications, contraindications, procedural steps, and complications.
- Goals: removal of pleural fluid that compromises cardiac and/or respiratory function and/or carries a risk of infection
- Indications include large symptomatic effusion (e.g., causing hemodynamic instability or respiratory failure), and complicated parapneumonic effusions.
- Complications include re-expansion pulmonary edema, infection, and injury.
Complicated parapneumonic effusions should be drained due to a high risk of progression to empyema.
Re-expansion pulmonary edema [25][26]
- Definition: Self-limiting noncardiogenic pulmonary edema that develops within 24 hours following rapid re-expansion of lung tissue that has collapsed as a result of air, pleural fluid, or mucus plugging; most commonly occurs as a complication of therapeutic thoracentesis.
-
Risk factors
- Age 20–40 years
- Diabetes
- Collapsed lung for > 3–7 days
- > 1.5 L of fluid removed
- Large associated pneumothorax
-
Clinical features
- Dyspnea, increased work of breathing
- Cough, frothy sputum
- Tachycardia, tachypnea, hypoxemia
- Diagnosis: confirmed by CXR or bedside ultrasound
-
Treatment
- Supplemental oxygen
- Severe cases: NIPPV or invasive mechanical ventilation
-
Prevention [4][27]
- Limit pleural fluid removal to < 1.2–1.5 L at a time.
- Avoid pleural pressures < -20 cm H2O.
Stop therapeutic thoracentesis if patients develop chest discomfort, cough, or hypoxia, as this could represent re-expansion pulmonary edema
Indwelling pleural catheter [28][29][30][31]
- Goal: recurrent pleural fluid removal without repeated puncture
- Indication: rapidly reaccumulating pleural effusions (e.g., malignant effusions ) [30][31]
- Contraindications: See “Contraindications to thoracentesis.”
-
Procedure [32]
- A pleural catheter is inserted under the guidance of interventional radiology.
- Similar to thoracentesis, except that the catheter is tunneled into the skin and can remain in situ for months.
-
Complications [32][33]
- Pain
- Mechanical: dislodgement, blockage, leak, tube fracture
- Infection: cellulitis, tunnel infection, empyema
- Fibrosis and loculation within the pleural cavity
- Catheter tract metastasis (i.e., deposition of malignant tissue at insertion site)
Mild cases of superficial cellulitis can often be treated with antibiotics without the need for catheter removal. [34]
Surgical procedures [6]
Consultation with a thoracic surgeon and/or chest physician is recommended.
Tube thoracostomy
-
Indications
- Pleural effusion in combination with significant cardiac and/or respiratory decompensation [35]
- For recurrent pleural effusion or urgent drainage of infected and/or loculated effusions [36][37]
- Drainage of high-viscosity fluid that is likely to clog [38][39]
- Empyema
- Hemothorax
- Procedure: See “Chest tube placement.”
Video-assisted thoracoscopic surgery (VATS)
- Definition: a minimally invasive surgical method used for diagnosis and treatment of various thoracic pathologies
-
Indications
- Collection of histological samples in malignant effusions
- Pleural biopsy
- Drainage of parapneumonic effusions that cannot be sufficiently controlled by tube thoracostomy
- Drainage of pleural empyema and debridement of fibrin deposits, adhesions, and scar tissue
Pleurodesis [29][30]
- Definition: chemical or surgical obliteration of the pleural space
-
Indication
- Recurrent malignant effusions [31]
- Effusions that do not respond to drugs (e.g., diuretics, antibiotics)
-
Contraindications [28]
- Predicted survival < 3 months
- Trapped lung
-
Procedure
- After draining the pleural effusion, a substance (e.g., talc) is introduced into the pleural cavity.
- This induces an inflammatory reaction that causes the pleural layers to bind together.
- Alternatively, thoracoscopic pleurodesis with partial resection of the pleural layers may be performed.
- Complication: fibrothorax
A chest x-ray should be performed after each of these procedures to rule out iatrogenic pneumothorax
Subtypes and variants
Pleural fluid analysis is necessary in almost all cases to distinguish between the various subtypes of pleural effusion. Treatment depends on the underlying cause. Subtypes of pleural effusion include the following:
- Parapneumonic effusion
- Pleural empyema
- Nontraumatic hemothorax
- Malignant pleural effusion
- Chylothorax
- Pseudochylothorax
Parapneumonic effusion
Definition [3][40]
-
Accumulation of exudative fluid in the pleural cavity in response to pneumonia
- Uncomplicated: without direct bacterial invasion
- Complicated: extension of bacterial infection into the pleural space
Distinguishing features [4][11][15][40]
-
Clinical features
- Fever, chills
- Cough
- Chest discomfort
-
Diagnostics
- Imaging: associated pneumonia
-
Pleural fluid analysis
- Exudative effusion
- Cloudy or purulent appearance
- WBC count > 10,000/mm3
- Positive Gram stain/culture for complicated parapneumonic effusion
-
Pleural fluid criteria for complicated parapneumonic effusion
- pH < 7.2
- ↑ LDH
- Glucose < 60 mg/dL
Treatment [11][37][41][42][43]
-
All patients: systemic antibiotic treatment
- Early antibiotic treatment can prevent progression to complicated effusion and empyema.
- See “Pneumonia treatment” for empiric antibiotic regimens.
- Patients with complicated parapneumonic effusions: therapeutic thoracentesis
- Complicated parapneumonic effusions at high risk of progression to pleural empyema: Consult surgery for surgical drainage. [20]
Pleural empyema
Definition [40]
- Accumulation of pus in the pleural cavity
Etiology [15][40]
- Most common: pneumonia
- Less common
- Infected hemothorax
- Ruptured lung abscess
- Esophageal tear
- Thoracic trauma
Classification [44][45]
- Stage I (exudative): accumulation of fluid and pus
- Stage II (fibrinopurulent): aggregation of fibrin deposits that form septations and pockets
- Stage III (organizing): formation of thick fibrous peel on pleural surface that restricts lung movement
Distinguishing features [40]
-
Clinical features
- Fever, chills
- Cough
- Chest discomfort
-
Diagnostics
-
CXR: will typically show opacity with one or more of the following characteristics [46]
- Meniscus sign
- Lenticular shape
- Diffuse consolidation of adjacent lung
- Ultrasound: heterogeneous fluid collection
-
Chest CT ; [10]
- Distinctive appearance of empyema fluid
- Split pleura sign: thickening of visceral and parietal pleura caused by fibrin that adheres to the surfaces, resulting in vascular proliferation
- Septations
- Displacement and compression of the adjacent lung
-
Pleural fluid analysis
- Exudative effusion
- Grossly purulent appearance
- Positive Gram stain and bacterial culture
- pH < 7.2
- Low glucose (< 30–60 mg/dL)
-
CXR: will typically show opacity with one or more of the following characteristics [46]
")
")

Treatment of pleural empyema
Empiric antibiotic therapy for pleural infection [37][41][42][43]
All patients should receive empiric antibiotics adjusted to their needs, local resistance patterns, and institutional guidelines.
-
Community-acquired pleural empyema [44]
- Combination therapy with a parenteral second- or third-generation cephalosporin (e.g., ceftriaxone ) PLUS one of the following for anaerobic coverage:
- Metronidazole
- Clindamycin
- Or single-agent therapy with a parenteral aminopenicillin and β-lactamase inhibitor (e.g., ampicillin-sulbactam )
- Combination therapy with a parenteral second- or third-generation cephalosporin (e.g., ceftriaxone ) PLUS one of the following for anaerobic coverage:
-
Hospital-acquired pleural empyema: Add MRSA and pseudomonal coverage to the above. [44]
-
Vancomycin PLUS one of the following:
- Cefepime and metronidazole
- Piperacillin-tazobactam
- Meropenem (if extended-spectrum β-lactamase-producing organisms are suspected)
-
Vancomycin PLUS one of the following:
-
Additional considerations [44]
- Aminoglycoside antibiotics are not recommended because of poor pleural bioavailability.
- Use empyema fluid culture to guide therapy.
- Intrapleural antibiotics are not recommended.
- Drainage should be arranged as quickly as possible for source control.
- Duration of therapy depends on the identified organism, source control, and clinical response.
- See tuberculosis therapy for the treatment of suspected tuberculous effusion.
Definitive treatment [44]
-
Stage I
- Chest tube (thoracostomy) to remove empyema fluid
- Consider intrapleural administration of fibrinolytic agents.
-
Stage II or mixed stage II/III
- First-line: chest tube drainage
- Second-line: VATS debridement if chest-tube drainage is ineffective
-
Stage III
- VATS debridement
- Pleurectomy and lung decortication via open thoracotomy
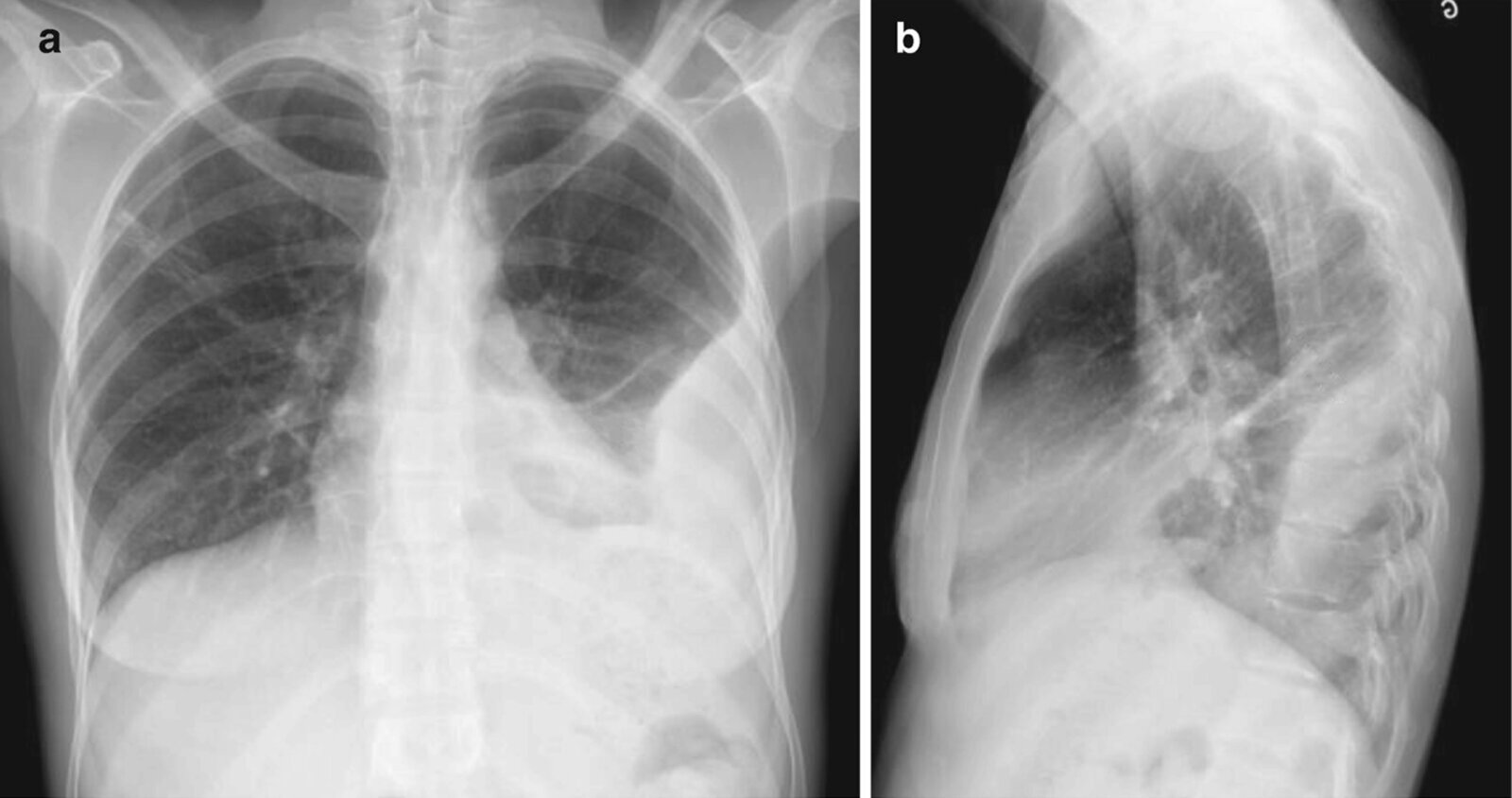
X-ray chest (a: PA view: b: lateral view) of a patient with a history of intravenous drug use and empyema
A loculated collection (red overlay) in the posterolateral lower left hemithorax has a biconvex shape compatible with a location within the pleural space. A meniscus and thickened major fissure from pleural fluid (blue lines) are also seen (blue lines), as are areas of lung consolidation (green overlay) and atelectasis (red lines).
Source: “A Systematic Approach to Chest Radiographic Analysis” by Jeffrey S. Klein, Melissa L. Rosado-de-Christenson, SpringerOpen, licensed under CC BY 4.0. Modifications: image cropped, arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
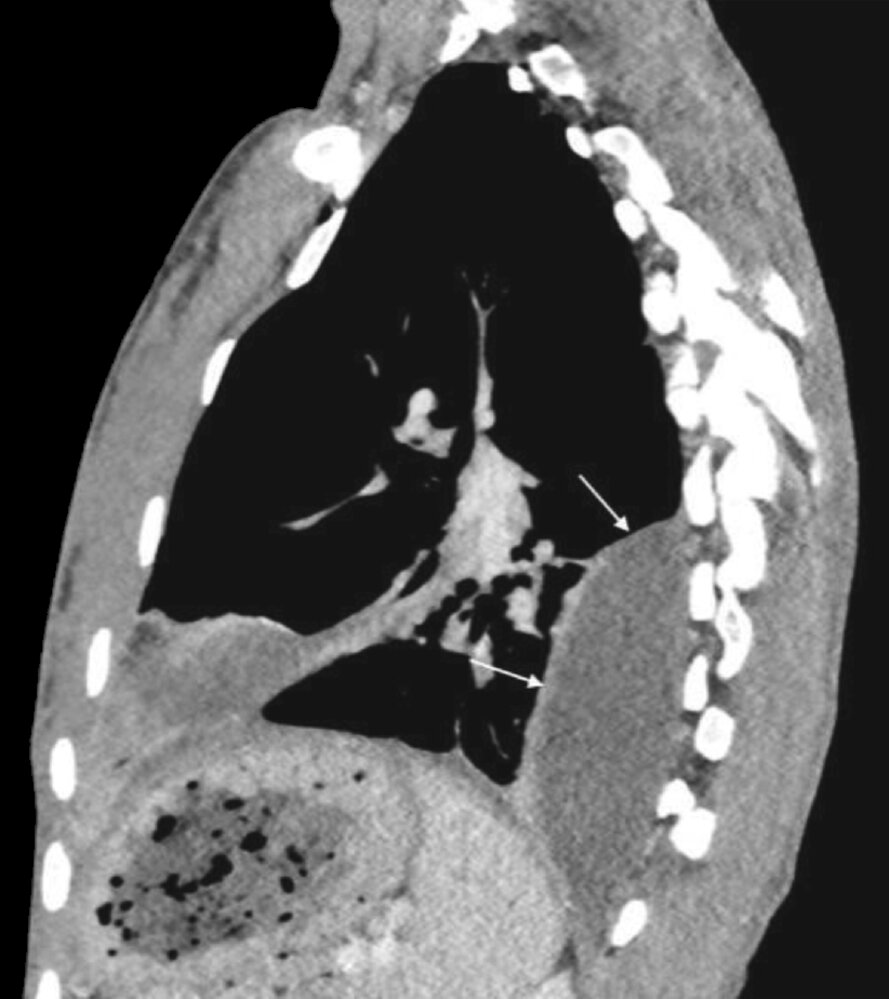
CT chest (with contrast; sagittal plane) of a patient with a history of intravenous drug use and empyema.
The loculated pleural collection (arrows) in the posterior left hemithorax has an enhancing wall and biconvex (lenticular) configuration. No gas is seen within the collection at this time. In addition, parenchymal consolidation and pleural effusion (dashed outline) are present anteriorly.
Source: “A Systematic Approach to Chest Radiographic Analysis” by Jeffrey S. Klein, Melissa L. Rosado-de-Christenson, SpringerOpen, licensed under CC BY 4.0. Modifications: image cropped, letter removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

Ultrasound left lateral thorax (intercostal oblique plane)
A complex pleural collection with loculations and thick septations is present in the right hemithorax (overlay).
Although there is overlap in the ultrasound appearances of exudative and transudative pleural collections, the presence of septations or homogeneous echoes often indicates an exudative collection. The appearance of an empyema depends on its composition, although empyemas are frequently septated.
L: liver
Our great thanks to Albertinen Krankenhaus, Hamburg, Germany, for kindly providing this case.
CT chest (with contrast; axial plane; lung window) of a patient with pneumonia
Air bronchograms (example indicated by arrow) are present within dense consolidation (green overlay) involving the left upper lobe. Passive left lower lobe atelectasis (A) is present adjacent to the accompanying pleural effusion (red overlay).
H: heart; PA: pulmonary artery
Source: “Images of CT scan of chest obtained from 2 year old child with empyema” by Elsa L Vazquez Melendez, John J Farrell, Andrea M Hujer et al., BMC Anesthesiology, licensed under CC BY 4.0. Modifications: Deleted A and B from original image. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
CT chest (with contrast; axial plane; mediastinal window)
CT scan shows right-sided pleural fluid collection (PC). The collection has a lenticular (biconvex) shape and is accompanied by thickening of the adjacent parietal (red line) and visceral pleurae (green line).
The split-pleura sign refers to thickening and contrast enhancement of the parietal and visceral pleurae separated by empyema or exudative effusion. The sign is the result of a fibrin pleural coat with capillary ingrowth and is considered reliable in distinguishing empyema from lung abscess. Lung abscesses, furthermore, tend to be round in contrast to the lenticular shape typical of empyemas.
T: trachea
Source: “Fig 2C, In: A Simple Method for Differentiating Complicated Parapneumonic Effusion/Empyema from Parapneumonic Effusion Using the Split Pleura Sign and the Amount of Pleural Effusion on Thoracic CT” by Tsujimoto N, Saraya T, Light RW et al., PLOS ONE, licensed under CC BY 4.0. Modifications: - original edit - letter removed - arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Parapneumonic effusion vs. empyema
| Overview of parapneumonic effusion and empyema | ||||
|---|---|---|---|---|
| Uncomplicated parapneumonic effusion | Complicated parapneumonic effusion | Pleural empyema | ||
| Definition |
|
|
||
| Etiology |
|
|
||
| Characteristics |
|
|
|
|
| Clinical features |
|
|||
| Diagnostics | Imaging |
|
|
|
| Pleural fluid analysis |
|
|
|
|
| Gram stain and blood culture [43][44] |
|
|
||
| Treatment |
|
|
|
|
X-ray chest (PA view) of a patient with tamoxifen-induced acute eosinophilic pneumonia
Peribronchial thickening (examples circled in yellow) and linear parenchymal opacities (examples indicated by white lines) are evidence of interstitial lung disease. A small pleural effusion (red line) projects through the right hemidiaphragm and blunts the right lateral costophrenic sulcus. A normal costophrenic sulcus is typically seen as an acutely angled junction between the costal and diaphragmatic pleural reflections (white dashed line).
Right chest wall staples (examples indicated by black overlays) and breast asymmetry (green outline) are the result of a recent mastectomy and reconstruction.
Source: “Fig. 1, In: Tamoxifen-induced acute eosinophilic pneumonia in a breast cancer patient” by Eiyoung Kwon, Mijin Kim, Eunhye Choi, Youngsam Park, Cheolseung Kim, International Journal of Surgery Case Reports, licensed under CC BY 4.0. Modifications: image cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
X-ray chest (a: PA view: b: lateral view) of a patient with a history of intravenous drug use and empyema
A loculated collection (red overlay) in the posterolateral lower left hemithorax has a biconvex shape compatible with a location within the pleural space. A meniscus and thickened major fissure from pleural fluid (blue lines) are also seen (blue lines), as are areas of lung consolidation (green overlay) and atelectasis (red lines).
Source: “A Systematic Approach to Chest Radiographic Analysis” by Jeffrey S. Klein, Melissa L. Rosado-de-Christenson, SpringerOpen, licensed under CC BY 4.0. Modifications: image cropped, arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
CT chest (with contrast; axial plane; lung window) of a patient with pneumonia
Air bronchograms (example indicated by arrow) are present within dense consolidation (green overlay) involving the left upper lobe. Passive left lower lobe atelectasis (A) is present adjacent to the accompanying pleural effusion (red overlay).
H: heart; PA: pulmonary artery
Source: “Images of CT scan of chest obtained from 2 year old child with empyema” by Elsa L Vazquez Melendez, John J Farrell, Andrea M Hujer et al., BMC Anesthesiology, licensed under CC BY 4.0. Modifications: Deleted A and B from original image. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
CT chest (with contrast; axial plane; mediastinal window)
CT scan shows right-sided pleural fluid collection (PC). The collection has a lenticular (biconvex) shape and is accompanied by thickening of the adjacent parietal (red line) and visceral pleurae (green line).
The split-pleura sign refers to thickening and contrast enhancement of the parietal and visceral pleurae separated by empyema or exudative effusion. The sign is the result of a fibrin pleural coat with capillary ingrowth and is considered reliable in distinguishing empyema from lung abscess. Lung abscesses, furthermore, tend to be round in contrast to the lenticular shape typical of empyemas.
T: trachea
Source: “Fig 2C, In: A Simple Method for Differentiating Complicated Parapneumonic Effusion/Empyema from Parapneumonic Effusion Using the Split Pleura Sign and the Amount of Pleural Effusion on Thoracic CT” by Tsujimoto N, Saraya T, Light RW et al., PLOS ONE, licensed under CC BY 4.0. Modifications: - original edit - letter removed - arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Nontraumatic hemothorax
Definition [47][48]
- Spontaneous or nontraumatic accumulation of blood in the pleural cavity
Etiology [48]
- Most common: spontaneous pneumothorax
- Less common
- Vascular disease
- Malignancy
- Coagulation disorders
- Necrotizing pneumonia [49]
- Endometriosis
- Bony exostoses
- See ”Penetrating trauma” for traumatic causes.
Distinguishing features
-
Clinical
- Symptoms of an underlying disorder
- If there is significant blood loss: hypotension, tachycardia
-
Diagnostics
- CXR: can show associated pneumothorax or malignancy
- Ultrasound: heterogeneous fluid collection
- Chest CT: hyperattenuating fluid collection; can reveal an underlying malignancy
- Chest CTA: allows for the identification of the source of hemorrhage (e.g., vascular abnormalities)
-
Pleural fluid analysis
- Bloody appearance
- RBC count > 5,000/mm3
- Hematocrit > 0.5 × peripheral hematocrit
- Laboratory studies: ↓ hemoglobin
Treatment of nontraumatic hemothorax [47][48]
- Stabilize the patient.
- Fluid resuscitation and blood transfusions as needed (see “Massive transfusion protocol”)
- Anticoagulant reversal (if applicable)
- Chest tube insertion indicated for most patients
- Urgent thoracotomy indicated for massive hemothorax (rare)
- Identify and treat the underlying cause.
- Consult surgery or interventional radiology for bleeding from tumors or vascular pathology.
A hemothorax, however small, must always be drained because blood in the pleural cavity will clot if not evacuated, resulting in a trapped lung or an empyema.
Use caution when inserting a chest tube if clinical and radiological signs suggest hemothorax secondary to aortic dissection or injury, as this may accelerate blood loss. [17]
Malignant pleural effusion
Description [50]
- Definition: accumulation of exudative fluid and malignant cells in the pleural cavity
- Pathophysiology: cancer-related barrier dysfunction of the capillary walls → increased permeation of plasma protein, blood cells, and tumor cells
Etiology [50]
- Caused by either direct invasion of the pleural space or distant metastases
- Most common: lung cancer, breast cancer
- Less common: mesothelioma, lymphoma, and pleural metastases
Distinguishing features [50]
- Clinical: symptoms of underlying malignancy (e.g., constitutional symptoms, cachexia, hemoptysis)
-
Diagnostics
- Imaging: associated underlying malignancy
-
Pleural fluid analysis
- Cell-rich exudative effusion
- Cloudy or straw-colored appearance
-
Abnormal cytology
- Pronounced nucleoli
- Cells with multiple nuclei
- Numerous figures of mitosis
- pH < 7.2
- Glucose < 60 mg/dL
- Amylase > 200 IU/L
- LDH usually high (> 0.45 x normal serum LDH)
- If hemorrhagic: bloody appearance, RBC count > 5,000/mm3
- Laboratory studies: positive tumor markers
Treatment [51]
- Asymptomatic: supportive care
-
Symptomatic
- Therapeutic thoracentesis
- Indwelling pleural catheter
- Chemical pleurodesis
- Treatment of underlying malignancy as needed
Photomicrograph of pleural fluid cytology specimen (H&E stain; unknown magnification)
Cells are clustered in dense groups and show marked pleomorphism (variability). Some cells show a pronounced shift in the nuclear-cytoplasm ratio and prominent nucleoli.
These findings are typical of malignant pleural effusion.
Source: © IMPP
Photomicrograph of a pleural fluid cytology specimen (H&E stain; unknown magnification)
Cells are clustered in dense groups and show marked pleomorphism (variability). Some cells show a pronounced shift in the nuclear-cytoplasm ratio and prominent nucleoli.
These findings are typical of malignant pleural effusion.
Source: © IMPP
Photomicrograph of pleural fluid cytology specimen (H&E stain; unknown magnification)
Cells are clustered in dense groups and show marked pleomorphism (variability). Some cells show a pronounced shift in the nuclear-cytoplasm ratio and prominent nucleoli.
These findings are typical of malignant pleural effusion.
Source: © IMPP
Chylothorax
Definition [7]
- Accumulation of lymphatic fluid from the thoracic duct (chyle) in the pleural cavity
Etiology [7]
- Trauma (including iatrogenic)
- Malignancy (e.g., lymphoma, bronchogenic carcinoma)
- Congenital lymphatic anomalies (e.g., lymphangiectasis)
Distinguishing features [7]
- Clinical: Chest pain is rare.
-
Diagnostics [2]
- Chest CT: underlying malignancy or thoracic injury
- Lymphangiography: source of chyle leak or obstruction
-
Pleural fluid analysis
- Cloudy, milky fluid with high concentrations of lipids (triglycerides, cholesterol, chylomicrons, and fat-soluble vitamins)
- Exudative effusion
- Total cholesterol usually < 200 mg/dL
- Triglyceride concentration > 110 mg/dL
- LDH usually low
- Glucose level similar to the plasma glucose level
- Lymphocyte predominance
Treatment of chylothorax [52]
-
First-line conservative treatment of chylothorax
- Total parenteral nutrition and special diet
- Adjunctive medication: somatostatin and octreotide
- Therapeutic thoracentesis as needed based on symptoms and the patient's functional needs
- Treatment of underlying disorder
-
Surgical treatment: via thoracotomy, thoracoscopy, or VATS
- Indications
- Unsuccessful conservative treatment
- Clinical deterioration (e.g., nutritional or metabolic)
-
Chyle drainage
- > 1000–1500 mL/day
- Up to 1000 mL/day for ≥ 5 days
- Unchanged over 1–2 weeks
- Persistent chyle leak: > 100 mL/day for > 2 weeks
- Procedures
- Thoracic duct: leak repair or ligation
- Pleura: defect repair, pleurodesis, or pleurectomy
- Diversion of chyle into a vein, the peritoneum, or externally
- Indications
-
Interventional radiology
- Indications: an alternative for patients who cannot tolerate operative procedures and for whom the treatment is anatomically feasible
- Procedures
- TIPS procedure (for hepatic chylothorax)
- Embolization or disruption of the lymph ducts
- Percutaneous repair of the thoracic ducts
Pseudochylothorax
Definition [7][53]
- Accumulation of cholesterol-rich fluid due to chronic inflammation in the pleural cavity
Etiology [7][53]
- Chronic pleural inflammation (e.g., due to underlying rheumatoid arthritis, pulmonary tuberculosis)
Distinguishing features [7][53]
-
Clinical
- Chronic symptoms of underlying disorder
- Dyspnea and chest pain in ∼ 75% of patients [53]
-
Diagnostics
- Imaging: signs of underlying disorder
-
Pleural fluid analysis
- Cloudy, milky appearance
- Exudative effusion
- Total cholesterol usually > 200 mg/dL
- Triglyceride concentration < 110 mg/dL
- Presence of cholesterol crystals
In contrast to chylothorax, a pseudochylothorax is characterized by high cholesterol and low triglyceride levels in the pleural fluid. The presence of cholesterol crystals may also help to differentiate a pseudochylothorax from a chylothorax.
Treatment
- Identical to first-line conservative treatment of chylothorax [53]
Pleurisy
Definition [54]
Pleurisy is an inflammatory condition that affects the pleura, the membranes lining the lungs and chest cavity, typically manifesting as sharp chest pain that worsens with deep breathing, coughing, or sneezing.
Etiology [55][56]
-
Viral infections
- Most common cause
- Adenovirus, coxsackieviruses, CMV, EBV, influenza virus, parainfluenza virus, RSV
-
Bacterial infections
- Pneumonia (parapneumonic pleuritis)
- Tuberculosis (TB pleuritis)
-
Inflammatory conditions
- Systemic lupus erythematosus
- Rheumatoid arthritis
- Sjogren syndrome
-
Pulmonary conditions
- Pneumothorax
- Asbestosis
- Malignancy e.g., mesothelioma
- Pulmonary embolism
-
Cardiac conditions
- Myocardial infarction
- Aortic dissection
- Cardiac surgery
-
Drugs
- Amiodarone, bleomycin, methotrexate
- Isoniazid, procainamide, hydralazine
Clinical features
- Pleuritic chest pain
- Pleural friction rub
- Further symptoms depend on the underlying disease, e.g.:
- Dry cough
- Dyspnea
- Constitutional symptoms
Diagnosis [54]
- History and physical examination
- Chest x-ray: signs of underlying pulmonary pathology e.g., pneumonia, pleural effusion
- Further investigation to rule out differential diagnoses; e.g., ECG to assess for signs of MI or pericarditis
Rule out life-threatening causes of pleuritic chest pain such as pulmonary embolism, myocardial infarction, and pneumothorax before making a clinical diagnosis of pleurisy.
Differential diagnosis of pleuritic chest pain [54]
- Myocardial infarction
- Pulmonary embolism
- Pneumothorax
- Pericarditis
- Bornholm disease
Treatment [55]
- Analgesia: NSAIDs (first line) can be used for relief of symptoms
- Treat underlying cause accordingly.
External Resources
- 2018 ATS Management of Malignant Pleural Effusions: An Official ATS/STS/STR Clinical Practice Guideline Implementation Tools
- 2011 ESTS, AATS Consensus Definitions to Promote an Evidence-based Approach to Management of the Pleural Space. A Collaborative Proposal by ESTS, AATS, STS, and GTSC
- 2010 BTS Pleural Disease Guideline 2010
- 2017 AATS consensus guidelines for the management of empyema
References
- McGrath EE, Blades Z, Anderson PB. "Chylothorax: Aetiology, diagnosis and therapeutic options". Respir Med. 104(1). :1-8. (2010)
- Saguil A, Wyrick K, Hallgren J. "Diagnostic approach to pleural effusion.". Am Fam Physician. 90(2). :99-104. (2014)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Rahman, NM, Chapman SJ, Davies RJO. "Pleural effusion: a structured approach to care†". Br Med Bull. 72(1). :31-47. (2004)
- Karkhanis V, Joshi J. "Pleural effusion: diagnosis, treatment, and management". Open Access Emergency Medicine. :31. (2012)
- Hooper et al. "Investigation of a unilateral pleural effusion in adults: British Thoracic Society pleural disease guideline 2010". Thorax. 65. :ii4-ii17
- Soni NJ, Franco R, Velez MI, et al. "Ultrasound in the diagnosis and management of pleural effusions". J Hosp Med. 10(12). :811-816. (2015)
- Socransky S, Wiss R, Hall G, et al. "Point-of-Care Ultrasound for Emergency Physicians". The EDE 2 Course Inc.. (2013). ISBN: 9780988012318
- Kraus GJ. "The Split Pleura Sign". Radiology. 243(1). :297-298. (2007)
- Roberts JR. "Roberts and Hedges' Clinical Procedures in Emergency Medicine and Acute Care". Elsevier. (2018). ISBN: 9780323354783
- Shin HB, Jeong YJ. "Late presenting congenital diaphragmatic hernia misdiagnosed as a pleural effusion". Medicine. 99(24). :e20684. (2020)
- Machado NO. "Pancreaticopleural Fistula: Revisited". Diagnostic and Therapeutic Endoscopy. 2012. :1-5. (2012)
- Yashant Aswani, Priya Hira. "Pancreaticopleural Fistula: A Review". JOP. Journal of the Pancreas. Vol 16. :No 1 (2015): January-p. 1. (2015)
- Schweigert M, Solymosi N, Dubecz A, Ofner D, Stein HJ. "Length of nonoperative treatment and risk of pleural empyema in the management of pancreatitis-induced pancreaticopleural fistula.". Am Surg. 79(6). :614-9. (2013)
- Findik S. "Pleural effusion in pulmonary embolism". Curr Opin Pulm Med. 18(4). :347-354. (2012)
- Kasmani R, Irani F, Okoli K, Mahajan V. "Re-expansion pulmonary edema following thoracentesis". Can Med Assoc J. 182(18). :2000-2002. (2010)
- Meeker JW, Jaeger AL, Tillis WP. "An uncommon complication of a common clinical scenario: exploring reexpansion pulmonary edema with a case report and literature review". Journal of Community Hospital Internal Medicine Perspectives. 6(3). :32257. (2016)
- Verhagen M, van Buijtenen JM, Geeraedts LMG. "Reexpansion pulmonary edema after chest drainage for pneumothorax: A case report and literature overview". Respiratory Medicine Case Reports. 14. :10-12. (2015)
- Zarogoulidis K, Zarogoulidis P, Darwiche K, et al. "Malignant pleural effusion and algorithm management.". Journal of thoracic disease. 5 Suppl 4. :S413-9. (2013)
- Detterbeck FC, Lewis SZ, Diekemper R, Addrizzo-Harris D, Alberts WM. "Diagnosis and Management of Lung Cancer, 3rd ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines". Chest. 143(5). :7S-37S. (2013)
- Simoff MJ, Lally B, Slade MG, et al. "Symptom Management in Patients With Lung Cancer". Chest. 143(5). :e455S-e497S. (2013)
- Puri V, Pyrdeck TL, Crabtree TD, et al. "Treatment of Malignant Pleural Effusion: A Cost-Effectiveness Analysis". Ann Thorac Surg. 94(2). :374-380. (2012)
- Lui MMS, Thomas R, Lee YCG. "Complications of indwelling pleural catheter use and their management". BMJ Open Respiratory Research. 3(1). :e000123. (2016)
- Chalhoub M, Saqib A, Castellano M. "Indwelling pleural catheters: complications and management strategies". Journal of Thoracic Disease. 10(7). :4659-4666. (2018)
- Mahmood K, Bower C. "Treatment of Infection Associated With Tunneled Pleural Catheters". J Bronchol Intervent Pulmonol. 17(1). :69-72. (2010)
- Saguil A, Wyrick K, Hallgren J. "Diagnostic approach to pleural effusion". Am Fam Physician. 90(2). :99-104. (2014)
- Cafarotti S, Dall’Armi V, Cusumano G, et al. "Small-bore wire-guided chest drains: Safety, tolerability, and effectiveness in pneumothorax, malignant effusions, and pleural empyema". J Thorac Cardiovasc Surg. 141(3). :683-687. (2011)
- Davies HE, Davies RJO, Davies CWH. "Management of pleural infection in adults: British Thoracic Society pleural disease guideline 2010". Thorax. 65(Suppl 2). :ii41-ii53. (2010)
- Porcel JM. "Chest Tube Drainage of the Pleural Space: A Concise Review for Pulmonologists". Tuberc Respir Dis (Seoul). 81(2). :106. (2018)
- Cooke DT, David EA. "Large-Bore and Small-Bore Chest Tubes". Thorac Surg Clin. 23(1). :17-24. (2013)
- Kasper DL, Fauci AS, Hauser S, et al. "Harrisons Principles of Internal Medicine ". McGraw-Hill Medical Publishing Division. 19. (2016). ISBN: 9780071802154
- Goldman L, Schafer AI. "Goldman-Cecil Medicine, 2-Volume Set". Elsevier. (2019). ISBN: 9780323532662
- Shen KR, Bribriesco A, Crabtree T, et al. "The American Association for Thoracic Surgery consensus guidelines for the management of empyema". J Thorac Cardiovasc Surg. 153(6). :e129-e146. (2017)
- Kwon YS. "Pleural Infection and Empyema". Tuberculosis and Respiratory Diseases. 76(4). :160. (2014)
- Hallifax RJ, Talwar A, Wrightson JM, Edey A, Gleeson FV. "State-of-the-art: Radiological investigation of pleural disease". Respir Med. 124. :88-99. (2017)
- Mandell LA, Wunderink RG, Anzueto A, et al. "Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults". Clinical Infectious Diseases. 44(Supplement_2). :S27-S72. (2007)
- Metlay JP, Waterer GW, Long AC, et al. "Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America". Am J Respir Crit Care Med. 200(7). :e45-e67. (2019)
- Sahn SA. "Diagnosis and Management of Parapneumonic Effusions and Empyema". Clinical Infectious Diseases. 45(11). :1480-1486. (2007)
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161
- Casali C, Susanna Storelli E, Di Prima E, Morandi U. "Long-term functional results after surgical treatment of parapneumonic thoracic empyema". Interact Cardiovasc Thorac Surg. 9(1). :74-78. (2009)
- Boersma et al. "Treatment of haemothorax". Respiratory Medicine. (2010)
- Patrini D, Panagiotopoulos N, Pararajasingham J, et al. "Etiology and management of spontaneous haemothorax.". J Thorac Dis. 7(3). :520-6. (2015)
- Morgan CK, Bashoura L, Balachandran D, Faiz SA. "Spontaneous Hemothorax". Annals of the American Thoracic Society. 12(10). :1578-1582. (2015)
- Chiumello D, Coppola S. "Management of pleural effusion and haemothorax". Oxford University Press. (2016). ISBN: 0198792654
- Psallidas et al. "Malignant pleural effusion: from bench to bedside". European Respiratory Review. 25(140). :189-198. (2016)
- Feller-Kopman et al. "Management of Malignant Pleural Effusions. An Official ATS/STS/STR Clinical Practice Guideline". American Journal of Respiratory and Critical Care Medicine. 197(7). (2018)
- Hans H. Schild, Christian P. Strassburg, Armin Welz, Jörg Kalff. "Treatment Options in Patients With Chylothorax". Deutsches Aerzteblatt Online. 110(48). :819–826. (2013)
- Lama et al. "Characteristics of patients with pseudochylothorax—a systematic review". Journal of Thoracic Disease. 8(8). :2093-2101. (2016)
- Tintinalli JE, Stapczynski JS, Ma OJ, et al. "Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9th edition". McGraw Hill Professional. (2019). ISBN: 9781260019940
- Dean NC, Griffith PP, Sorensen JS, et al. "Pleural Effusions at First ED Encounter Predict Worse Clinical Outcomes in Patients With Pneumonia". Chest. 149(6). :1509-1515. (2016)
- Reamy BV, Williams PM, Odom MR. "Pleuritic Chest Pain: Sorting Through the Differential Diagnosis.". Am Fam Physician. 96(5). :306-312. (2017)
- Kass SM, Williams PM, Reamy BV. "Pleurisy.". Am Fam Physician. 75(9). :1357-64. (2007)
- Hunter MP, Regunath H. "Pleurisy". StatPearls. (2020)
- Wilcox ME, Chong CAKY, Stanbrook MB, et al. "Does This Patient Have an Exudative Pleural Effusion?". JAMA. 311(23). :2422. (2014)
- Chubb SP, Williams RA. "Biochemical Analysis of Pleural Fluid and Ascites.". The Clinical biochemist. Reviews. 39(2). :39-50. (2018)
- Romero-Candeira S, Fernández C, Martı́n C, Sánchez-Paya J, Hernández L. "Influence of diuretics on the concentration of proteins and other components of pleural transudates in patients with heart failure". Am J Med. 110(9). :681-686. (2001)
- Rubins J. "Pleural Effusion". WebMD. http://emedicine.medscape.com/article/299959-workup. [2016-06-30]
- Ward MA. "Empyema and Abscess". WebMD. http://emedicine.medscape.com/article/807499-clinical#showall. [2015-03-18]
- Strange C. "Parapneumonic effusion and empyema in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/parapneumonic-effusion-and-empyema-in-adults?source=search_result&search=pleural%20empyema&selectedTitle=1~150. [2016-12-20]
- "Pleural effusion". https://radiopaedia.org/articles/pleural-effusion. [2017-02-19]
- "Radiology of the Chest: Chapter Four: Diagnostic Radiographic Signs"
- Bien MY, Wu MP, Chen WL, Chung CL. "VEGF correlates with inflammation and fibrosis in tuberculous pleural effusion". ScientificWorldJournal. 2015. (2015)
- "Pleural Disease". http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/pulmonary/pleural-disease/. [2010-08-01]
- Heffner JE. "Diagnostic Thoracentesis". UpToDate. UpToDate. https://www.uptodate.com/contents/diagnostic-thoracentesis. [2017-03-16]
- "Pleural Effusion". https://www.dynamed.com/topics/dmp~AN~T474331/Pleural-effusion. [2017-08-24]
- "Empyema vs pulmonary abscess". https://radiopaedia.org/articles/empyema-vs-pulmonary-abscess-2
- Tao Le, Vikas Bhushan, Deol M, Reyes G. "First Aid for the USMLE Step 2 CK, Tenth Edition". McGraw-Hill Education. (2018). ISBN: 9781260440294
- Heffner J; Broaddus V. "Diagnostic evaluation of a pleural effusion in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/diagnostic-evaluation-of-a-pleural-effusion-in-adults-initial-testing?search=pleural%20effusion&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1#H14. [2018-04-02]
- King, Thompson. "Radiological perspectives in empyema: Childhood respiratory infections". British Medical Bulletin. 61(1). :203–214. (2002)
- "Thoracic empyema". https://radiopaedia.org/articles/thoracic-empyema-1