Summary
Pneumonia is a respiratory infection characterized by inflammation of the alveolar space and/or the interstitial tissue of the lungs. In industrialized nations, it is the leading infectious cause of death. Pneumonia is most commonly transmitted via aspiration of airborne pathogens (primarily bacteria, but also viruses and fungi) but may also result from the aspiration of stomach contents. The most likely causal pathogens can be narrowed down based on patient age, immune status, and where the infection was acquired (community-acquired or hospital-acquired). Pneumonia is classified based on clinical features as either typical or atypical; each type has its own spectrum of commonly associated pathogens. Typical pneumonia manifests with sudden onset of malaise, fever, and a productive cough. On auscultation, crackles and bronchial breath sounds are audible. Atypical pneumonia manifests with gradual onset of unproductive cough, dyspnea, and extrapulmonary manifestations. Auscultation is usually unremarkable. Some patients may present with elements of both types. Diagnostics include blood tests for inflammatory parameters and pathogen detection in blood, urine, or sputum samples. Chest x-ray in cases of typical pneumonia shows opacity restricted to one lobe, while x-ray in atypical pneumonia may show diffuse, often subtle infiltrates. Together with the characteristic clinical features, newly developed pulmonary infiltrate on chest x-ray confirms the diagnosis. Management consists of empiric antibiotic treatment and supportive measures (e.g., oxygen administration, antipyretics).
For specific information on the diagnosis and management of pneumonia in pediatric patients, see “Pneumonia in children.”
Etiology
Pathogens
| Pneumonia pathogens according to the source of infection | |
|---|---|
| Type of pneumonia | Common pathogens |
| Community-acquired pneumonia |
|
| Hospital-acquired pneumonia |
|
For atypical pneumonia bacterial causes, remember the mnemonic: Atypically, Legions of Clams Mind their P's and Q's!
• Legionella pneumophila
• Chlamydia pneumoniae
• Mycoplasma pneumoniae
• Psittacosis (Chlamydia psittaci)
• Q fever (Coxiella burnetii)


| Pneumonia pathogens according to location | |
|---|---|
| Type of pneumonia | Common pathogens |
| Lobar pneumonia |
|
| Bronchopneumonia |
|
| Interstitial pneumonia |
|
| Cryptogenic organizing pneumonia |
|
| Pneumonia pathogens according to affected population | |
|---|---|
| Type of pneumonia | Common pathogens |
| Pneumonia in immunocompromised patients |
|
| Pneumonia in newborns |
|
| Pneumonia in children (4 weeks –18 years) |
|
| Pneumonia in young adults (18–40 years) |
|
| Pneumonia in adults (40–65 years) |
|
| Pneumonia in elderly individuals |
|
| Recurrent pneumonia |
|
“Track my respiration: chlassic strep formation”: C. trachomatis, Mycoplasma, Respiratory syncytial virus, Chlamydia pneumoniae, and Streptococcus pneumoniae are the most common causative agents of pneumonia in children.
Risk factors [7]
- Old age and immobility of any cause
-
Chronic diseases
- Preexisting cardiopulmonary conditions (e.g., bronchial asthma, COPD, heart failure)
- Acquired or congenital abnormalities of the airways (e.g., bronchiectasis, space-occupying lesions, cystic fibrosis)
-
Immunosuppression
- HIV infection
- Diabetes mellitus
- Cytostatic and immunosuppressive therapy
- Alcoholism
- Malnutrition
-
Impaired airway protection
- Alteration in consciousness (e.g., due to stroke, seizure, anesthesia, drugs, alcohol)
- Dysphagia
- Smoking
-
Environmental factors
- Crowded living conditions (e.g., prisons, homeless shelters)
- Toxins (e.g., solvents, gasoline)
- Endemic exposures (e.g., areas of high Coccidioides and Histoplasma endemicity)
- Contaminated water systems (e.g., in hotels, on cruise ships)
- Zoonotic exposures (e.g., birds, farm animals)
-
Cryptogenic organizing pneumonia
- Specific medications; (e.g., amiodarone, bleomycin) [8]
- Chronic inflammatory disorders (e.g., rheumatoid arthritis)
-
Surgical procedures
- Upper abdominal surgery
- Chest surgery
Bear in mind immune status and potential exposures when considering potential pathogens in patients with suspected pneumonia.
Consider aspiration pneumonia in patients with altered mental status or other risk factors for aspiration.

© AMBOSS
© AMBOSS
Classification
Pneumonia can be classified according to etiology, location acquired, clinical features, and the area of the lung affected by the pathology.
Etiology
- Primary pneumonia: no apparent preexisting conditions that may predispose to pneumonia
-
Secondary pneumonia
- Bronchial asthma, COPD, heart failure, cystic fibrosis
- Viral upper respiratory tract infections with bacterial superinfection
- Anatomical abnormalities such as tubercular caverns, bronchial tumors, or stenosis (postobstructive pneumonia) [9]
- Aspiration pneumonia
Location acquired
- Community-acquired pneumonia (CAP): pneumonia that is acquired outside of a healthcare establishment
-
Hospital-acquired pneumonia (HAP): pneumonia onset > 48 hours after a patient is admitted to a hospital without evidence of disease at the time of admission [10]
- Ventilator-associated pneumonia (VAP): pneumonia occurring in patients who are on mechanical ventilation breathing machines in hospitals (typically in the intensive care unit)
- Healthcare-associated pneumonia (HCAP): A historical term for pneumonia acquired in healthcare facilities; this terminology is no longer in use.
Clinical features
-
Typical pneumonia
- Pneumonia featuring classic symptoms (typical findings on auscultation and percussion)
- Manifests as lobar pneumonia or bronchopneumonia
-
Atypical pneumonia
- Pneumonia with less distinct classical symptoms and often unremarkable findings on auscultation and percussion
- Manifests as interstitial pneumonia
Area of lung affected by the pathology
-
Lobar pneumonia: pneumonia affecting one lobe of a lung
- Multilobar pneumonia refers to the involvement of multiple lobes in a single lung or both lungs.
- Panlobar pneumonia involves all the lobes of a single lung.
- Bronchial pneumonia: pneumonia affecting the tissue around the bronchi and/or bronchioles
- Interstitial pneumonia: pneumonia affecting the tissue between the alveoli
- Cryptogenic organizing pneumonia (formerly known as bronchiolitis obliterans organizing pneumonia): a noninfectious pneumonia of unknown etiology characterized by the involvement of the bronchioles, alveoli, and surrounding tissue
Pathophysiology
Routes of infection
- Most common: microaspiration (droplet infection) of airborne pathogens or oropharyngeal secretions
- Aspiration of gastric acid (aspiration pneumonitis) , food, or liquids
- Hematogenous dissemination (rare)
Pathogenesis
- Failure of protective pulmonary mechanisms; (e.g., cough reflex, mucociliary clearance , alveolar macrophages )
- Infiltration of the pulmonary parenchyma by the pathogen → interstitial and alveolar inflammation
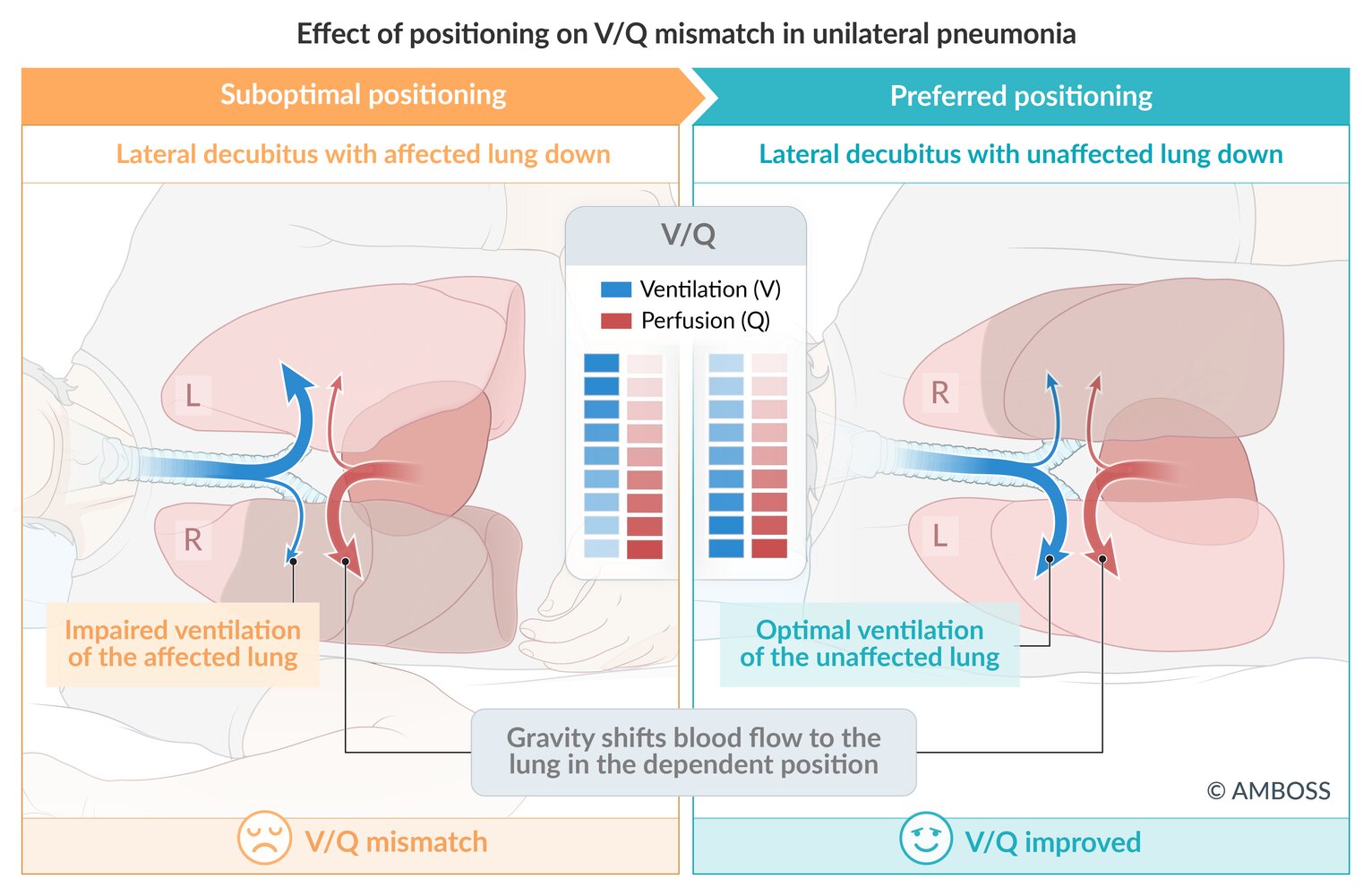
- Impaired alveolar ventilation → ventilation/perfusion (V/Q) mismatch with intrapulmonary shunting (right to left)
-
Hypoxia due to increased alveolar-arterial oxygen gradient
- Hypoxia is worsened when the affected lung is in the dependent position, as perfusion to the dependent lung is better compared to the nondependent lung.
- In the case of a large unilateral pulmonary abscess, it may be helpful to position the patient so that the affected lung is in the dependent position in order to prevent the pus from filling the unaffected lung.

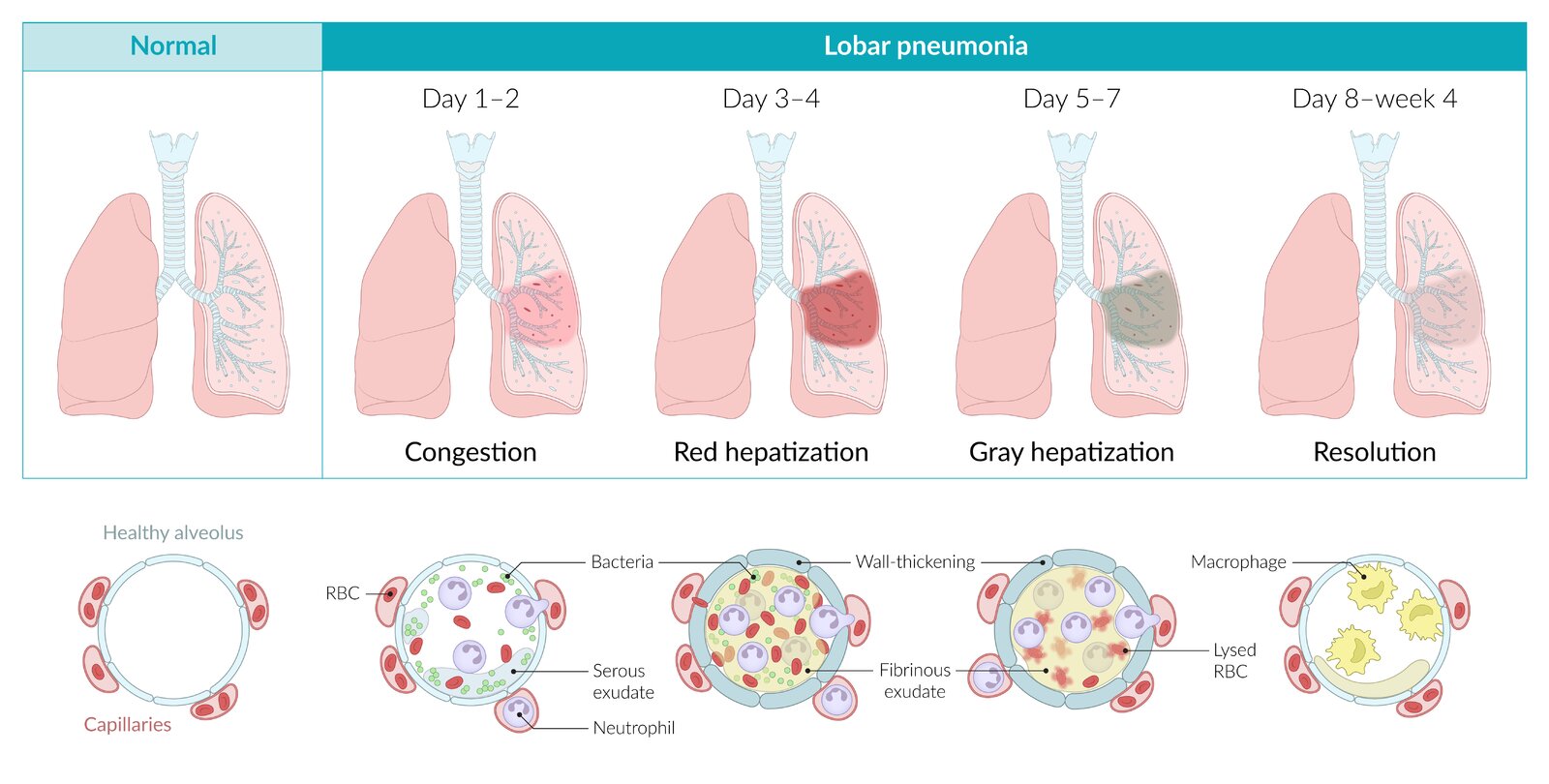
Pattern of involvement
-
Lobar pneumonia
- Classic (typical) pneumonia of an entire lobe; primarily caused by pneumococci
- Characterized by inflammatory intra-alveolar exudate, resulting in consolidation
- Can involve the entire lobe or the whole lung
| Stages of lobar pneumonia | ||
|---|---|---|
| Stages | Macroscopic findings | Microscopic findings |
| Congestion (day 1–2) |
|
|
| Red hepatization (day 3–4) |
|
|
| Gray hepatization (day 5–7) |
|
|
| Resolution (day 8 to week 4) |
|
|
-
Bronchopneumonia: most commonly a descending infection that affects the bronchioles and adjacent alveoli
- Primarily caused by pneumococci and/or other streptococci
- Characterized by acute inflammatory infiltrates that fill the bronchioles and the adjacent alveoli (patchy distribution)
- Usually involves the lower lobes or right middle lobe and affects ≥ 1 lobe
- Manifests as typical pneumonia
- Necrotizing bronchopneumonia and pneumatocele are caused by Staphylococcus aureus and are often preceded by an influenza infection. [11]
-
Interstitial pneumonia: interstitial inflammation, typically caused by Mycoplasma and viral infections
- Characterized by a diffuse patchy inflammation that mainly involves the alveolar interstitial cells
- Bilateral multifocal opacities are classically found on chest x-ray.
- Manifests as atypical pneumonia
- Often has an indolent course (walking pneumonia)
- Miliary pneumonia: multiple small infiltrations caused by hematogenous dissemination (e.g., of tuberculosis)
- Cryptogenic organizing pneumonia: characterized by inflammation of the bronchioles and surrounding structures




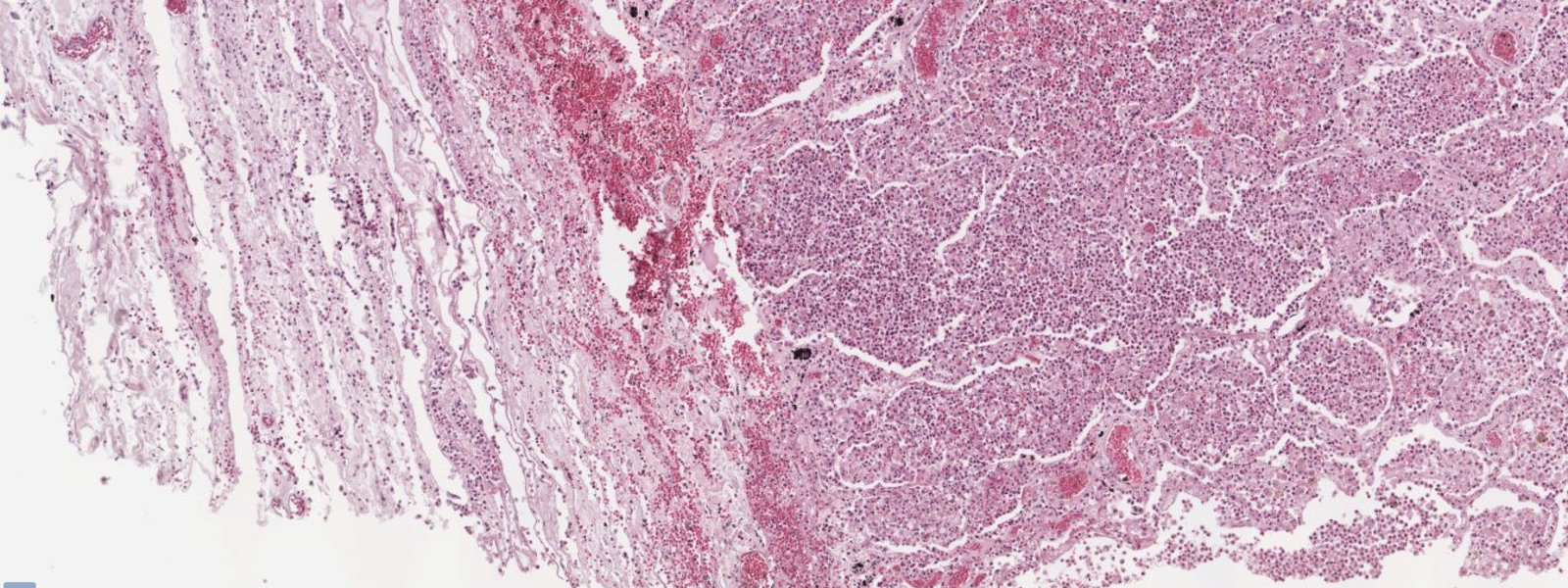
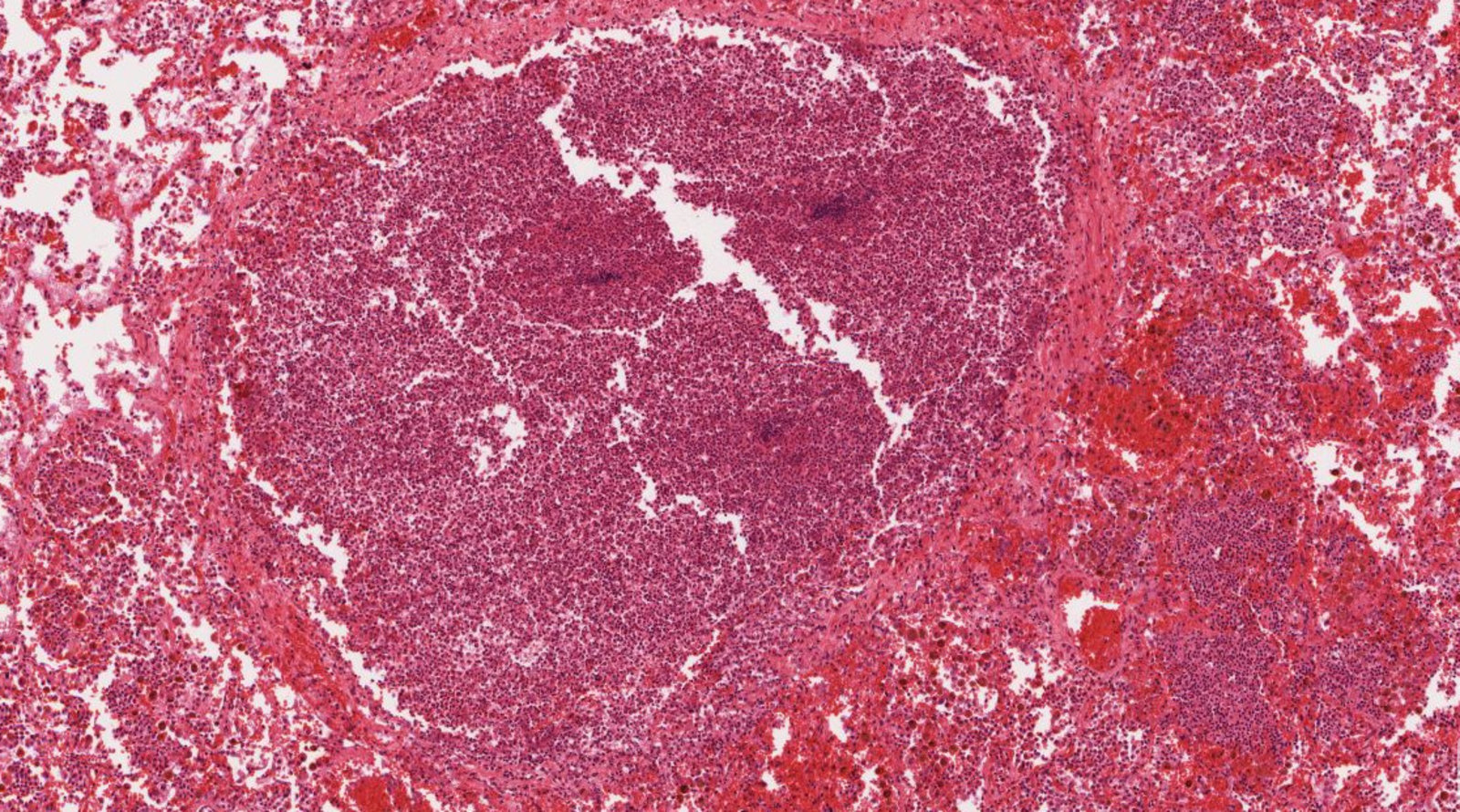
Photomicrograph of a lung tissue specimen (H&E stain; 250x magnification)
Neutrophilic pleuritis is seen at the bottom left of the sample (red overlay). There is also neutrophil invasion with fibrinopurulent exudate seen in the alveoli (green overlay in black circles).
These are typical findings in lobar pneumonia.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
Photomicrograph of a lung tissue specimen (H&E stain; medium magnification)
Relatively normal lung tissue (green overlay) can be seen next to pathologic lung tissue (white overlay) with alveolar infiltrates of mainly neutrophils as well as exudation of erythrocytes. A cross-section of an airway (white outline) also shows purulent infiltrates (examples indicated by black arrows) consisting predominantly of neutrophils.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
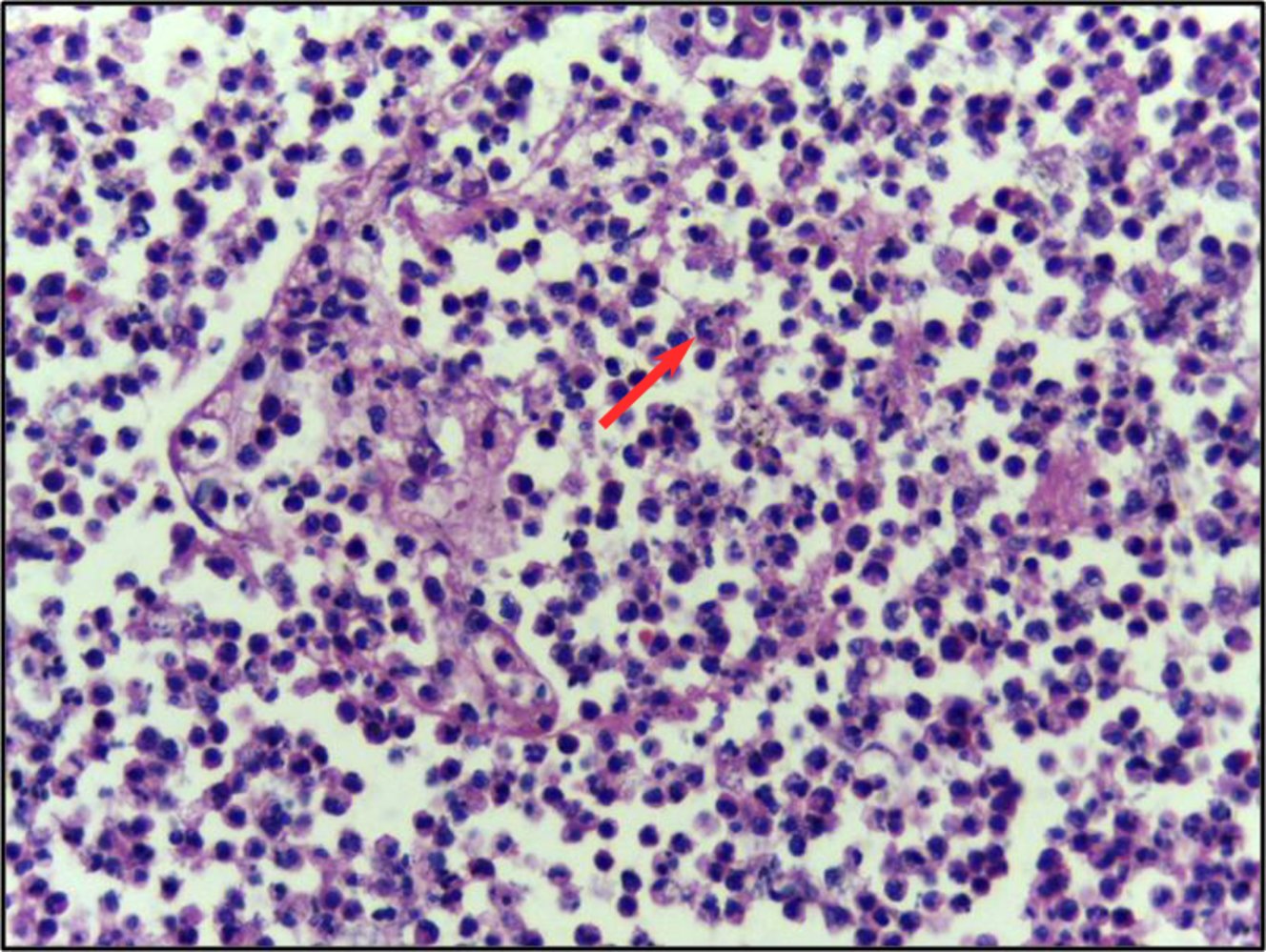
Photomicrograph of a section of lung tissue (H&E stain; 40x magnification)
The alveoli are filled with neutrophils (red arrow) and there is congestion of the alveolar wall.
These are characteristic histopathological findings of pneumonia.
Source: “Lung biopsy showing lobar pneumonia 40X” by Department of Pathology, Calicut Medical College, Wikimedia Commons, licensed under CC BY-SA 4.0. Modifications: added arrow.
{kind=link}
Clinical features
Typical pneumonia
Typical pneumonia is characterized by a sudden onset of symptoms caused by lobar infiltration.
- Severe malaise
- High fever and chills
-
Productive cough with purulent sputum (yellow-greenish)
- Crackles and bronchial breath sounds on auscultation
- Decreased breath sounds
- Enhanced bronchophony, egophony, and tactile fremitus
- Dullness on percussion
- Tachypnea and dyspnea (nasal flaring, thoracic retractions)
- Pleuritic chest pain when breathing, often accompanying pleural effusion
- Pain that radiates to the abdomen and epigastric region (particularly in children; see also “Pneumonia in children”)
Suspect bacterial pneumonia in immunocompromised patients with acute high fever and pleural effusion.
Atypical pneumonia
Atypical pneumonia typically has an indolent course (slow onset) and commonly manifests with extrapulmonary symptoms.
- Nonproductive, dry cough
- Dyspnea
- Auscultation often unremarkable
- Common extrapulmonary features include fatigue, headaches, sore throat, myalgias, and malaise.
This classification does not have a major impact on patient management because it is not always possible to clearly distinguish between typical and atypical pneumonia.


© AMBOSS
Diagnosis
General principles [12][13]
- Pneumonia diagnosis is based on new pulmonary infiltrates on chest imaging in patients with respiratory symptoms and systemic inflammatory response.
- The choice of microbiological studies is guided by a severity assessment for CAP or the presence of HAP or VAP.
- In ambulatory settings, normal vital signs and an unremarkable lung examination indicate a very low likelihood of CAP. [14][15]
Diagnosis of pneumonia can be challenging due to the lack of a gold-standard test and numerous mimics (e.g., COPD exacerbation, heart failure), especially when diagnostic testing is ambiguous. [13][16]
Diagnosis of CAP [12][13]
- New pulmonary infiltrate on chest imaging (e.g., CXR)
- AND ≥ 1 new or increased respiratory symptom: e.g., cough, sputum, dyspnea, or pleuritic pain
- AND ≥ 1 of the following:
- Fever or hypothermia
- Leukocytosis, bandemia, or leukopenia
- Hypoxemia
Consider chest CT or empiric treatment when clinical suspicion for CAP remains high despite a negative CXR, as false negatives are possible. [16][17]
Laboratory studies
Routine studies
- CBC: leukocytosis
- ↑ CRP, ↑ ESR
-
↑ Serum procalcitonin (PCT): an acute phase reactant that can help diagnose bacterial lower respiratory tract infections ; [12][18]
- Obtain for patients with IDSA/ATS criteria for severe CAP. [12][18]
- Consider for patients with nonsevere CAP alongside viral diagnostics. [12][18]
- PCT levels ≥ 0.25 mcg/L correlate with an increased probability of a bacterial infection.
-
Low PCT level after 2–3 days of antibiotic therapy can help facilitate the decision to discontinue antibiotics. [19][20]
- Decrease of PCT to ≤ 80% of peak level
- Decrease of PCT to < 0.25 mcg/L
- ABG: ↓ PaO2 [21]
- BMP
- LFTs
Do not rely solely on inflammatory markers (e.g., CRP, procalcitonin) to guide decisions on antibiotic therapy. [16][22]
Microbiological studies [10][12][13][18]
-
Severe CAP [12][13]
- Obtain the following in all patients:
- Blood cultures (2 sets)
- Sputum culture and Gram stain
- Influenza and COVID-19 testing
- Pneumococcal urinary antigen
- Legionella pneumophila urinary antigen
- Obtain a MRSA nasal swab for patients with:
- Current empiric coverage for MRSA
- History of parenteral antibiotics in a hospital setting within the past 90 days
- History of MRSA colonization or infection in the past year
- If available:
- Obtain a bacterial molecular panel.
- Consider obtaining an expanded viral molecular panel (e.g., RSV, rhinovirus, enterovirus) when it would alter management.
- Obtain the following in all patients:
-
Nonsevere CAP
- Obtain the following during periods of community transmission or recent potential exposure (e.g., recent travel to areas with high transmission):
- Influenza and COVID-19 testing
- Legionella pneumophila urinary antigen
-
Obtain sputum culture and Gram stain for patients with:
- History of parenteral antibiotics in a hospital setting within the past 90 days
- Current empiric coverage for MRSA or P. aeruginosa
- Structural lung disease
- Obtain a MRSA nasal swab for patients with:
- Current empirical coverage for MRSA
- History of parenteral antibiotics in a hospital setting within the past 90 days
- If available, consider the following when it would alter management:
- Expanded viral molecular panel (e.g., RSV, rhinovirus, enterovirus)
- Bacterial molecular panel
- Obtain the following during periods of community transmission or recent potential exposure (e.g., recent travel to areas with high transmission):
-
HAP or VAP [10]
- Obtain respiratory culture and Gram stain (noninvasive methods are preferred). [10]
- Consider additional testing based on individual patient factors and severity.
Test for COVID-19 and influenza in all patients with possible CAP during periods of community transmission or if they are at high risk of exposure (e.g., recent travel to areas with high transmission). [12]
Avoid routine blood cultures and sputum Gram stain in patients with CAP, except when severe or there is concern for MRSA or Pseudomonas infection. [18]
Imaging
Chest x-ray (posteroanterior and lateral)
- Indications: all patients suspected of having pneumonia
-
X-ray findings in pneumonia
-
Lobar pneumonia
- Opacity of one or more pulmonary lobes
- Presence of air bronchograms: appearance of translucent bronchi inside opaque areas of alveolar consolidation
-
Bronchopneumonia
- Poorly defined patchy infiltrates scattered throughout the lungs
- Presence of air bronchograms
-
Atypical or interstitial pneumonia
- Diffuse reticular opacity
- Absent (or minimal) consolidation
- Parapneumonic effusion
-
Lobar pneumonia
A new pulmonary infiltrate on chest x-ray in a patient with classic signs and symptoms of pneumonia confirms the diagnosis. [16]
Typical pneumonia usually appears as lobar pneumonia on x-ray, while atypical pneumonia tends to appear as interstitial pneumonia. However, the underlying pathogen cannot be conclusively identified based on imaging results alone.




")
")



")
")
")

")




Chest CT (usually without contrast)
-
Indications
- Inconclusive chest x-ray
- Recurrent pneumonia
- Poor response to treatment
- Advantages: more reliable evaluation of circumscribed opacities, pleural empyema, or sites of consolidation
-
Findings: [23]
- Localized areas of consolidation (hyperdense)
- Air bronchograms
- Ground-glass opacities
-
Pleural effusion/empyema
- Hyperdense fluid collection
- Split pleura sign
-
Nodules
- Large (e.g., in tuberculosis or fungal pneumonia)
- Peribronchial (e.g., bronchopneumonia)
- Disseminated (e.g., septic emboli or varicella-zoster pneumonia)
CT is more sensitive and specific than CXR for the diagnosis of pneumonia. [16]





Lung ultrasound in pneumonia [16]
Point-of-care ultrasound of the lungs (lung POCUS) has high sensitivity and specificity for the diagnosis of pneumonia. [24][25]
-
Indications
- Evaluation of suspected pneumonia
- Assessment of undifferentiated dyspnea [26]
-
Characteristic findings [27][28]
-
Ultrasound findings of lung consolidation [29]
- Tissue-like sign
- Shred sign
- Sonographic air bronchograms
- Unilateral B-lines
- Sonographic findings of pleural effusion
-
Ultrasound findings of lung consolidation [29]
In the emergency department, consider POCUS to quickly confirm pneumonia and assess for other causes of dyspnea.
Advanced diagnostics for pneumonia
Bronchoscopy
-
Indications
- Suspected mass (e.g., recurrent pneumonia)
- Need for pathohistological diagnosis (e.g., biopsy of a central mass discovered on CT)
- Inconclusive results on CT
- Poor response to treatment
Thoracentesis
- Indications: See “Indications for thoracentesis.”
- Findings: See “Pleural fluid analysis.”
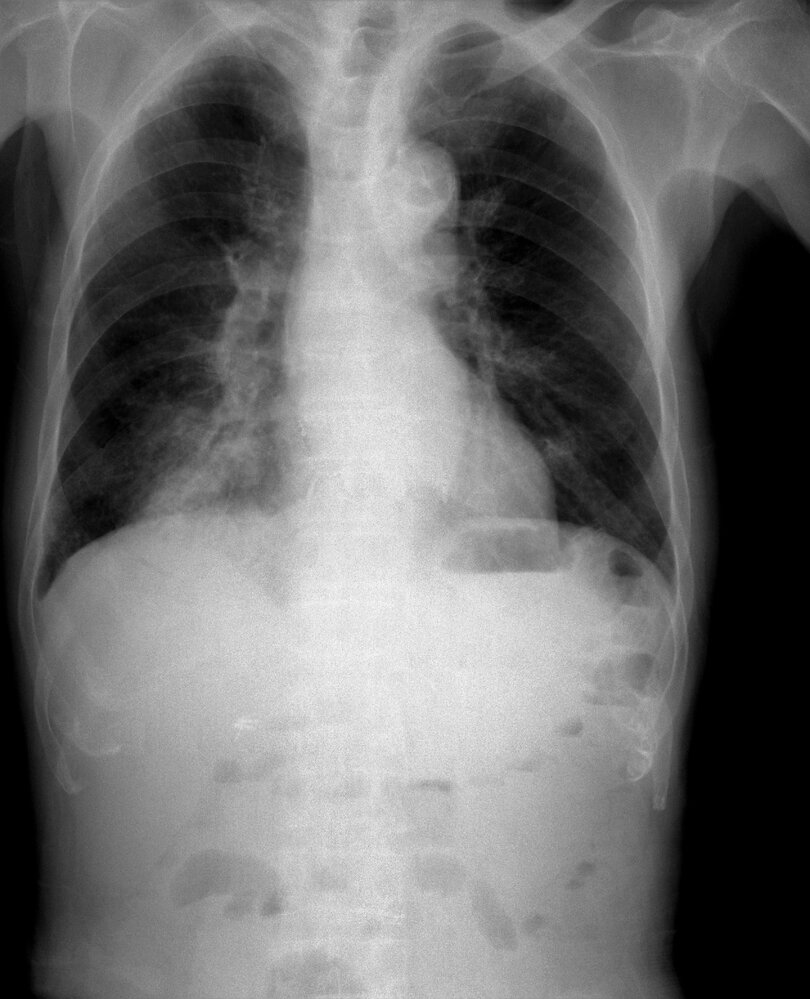
X-ray chest (PA view) of a patient with a history of Legionella pneumonia
An abnormal area of airspace opacification (green overlay) is seen medially in the left lung projecting over the hilum. The sharp edge along its inferolateral aspect (red line) may be a portion of a major fissure displaced by accompanying volume loss.
Source: © IMPP
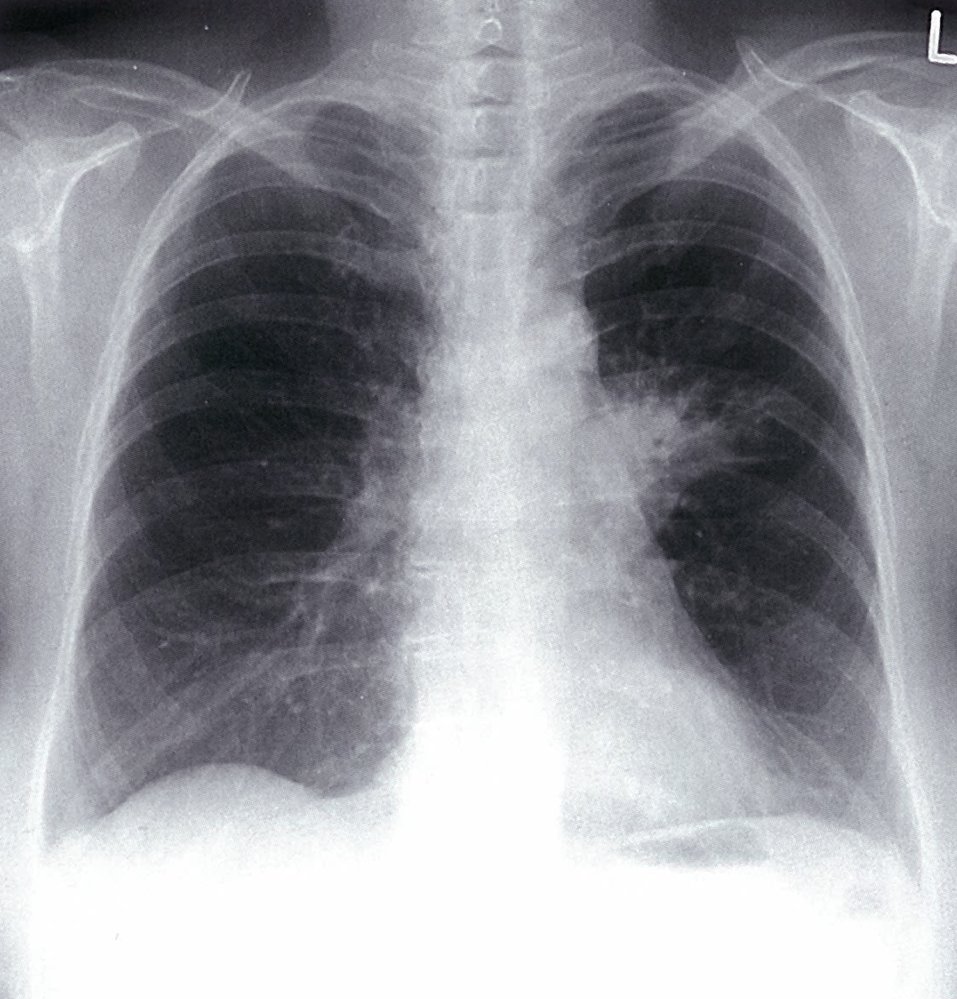
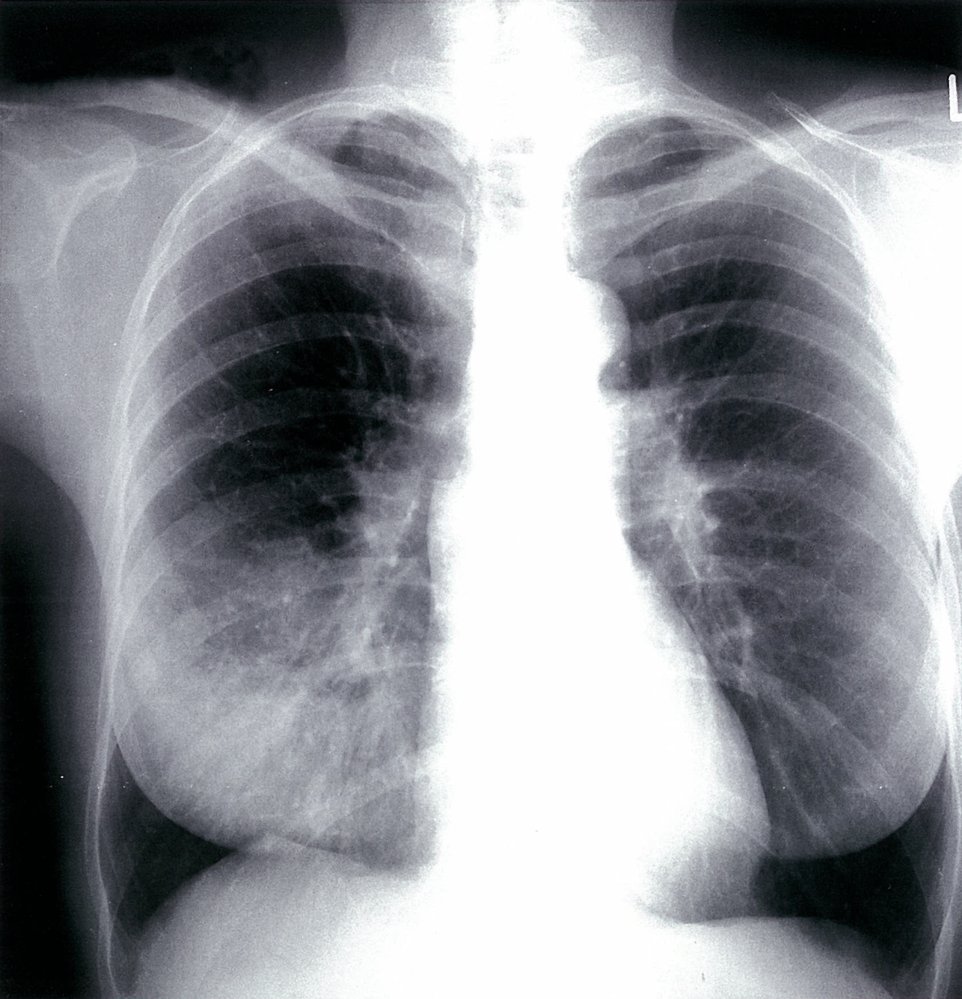
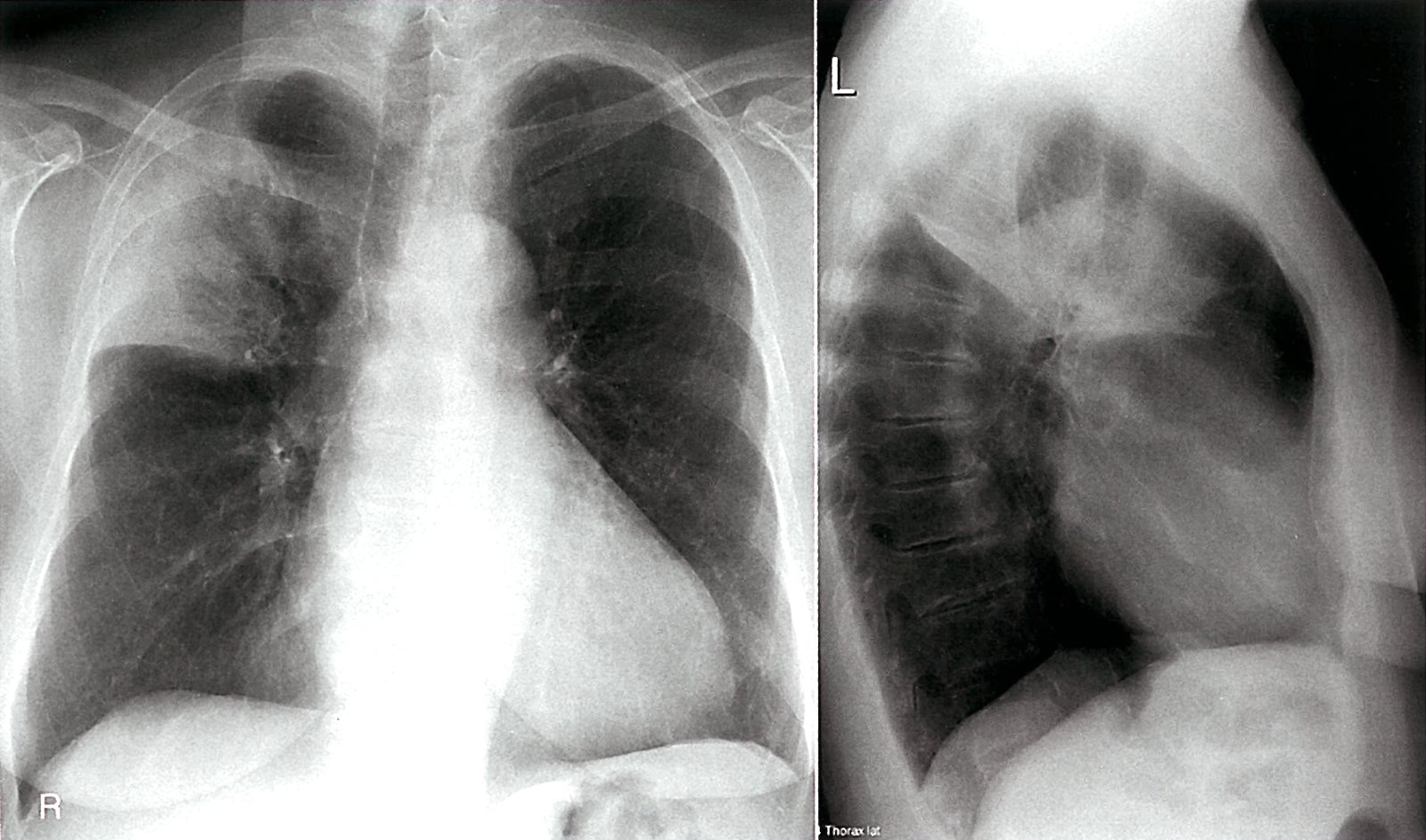
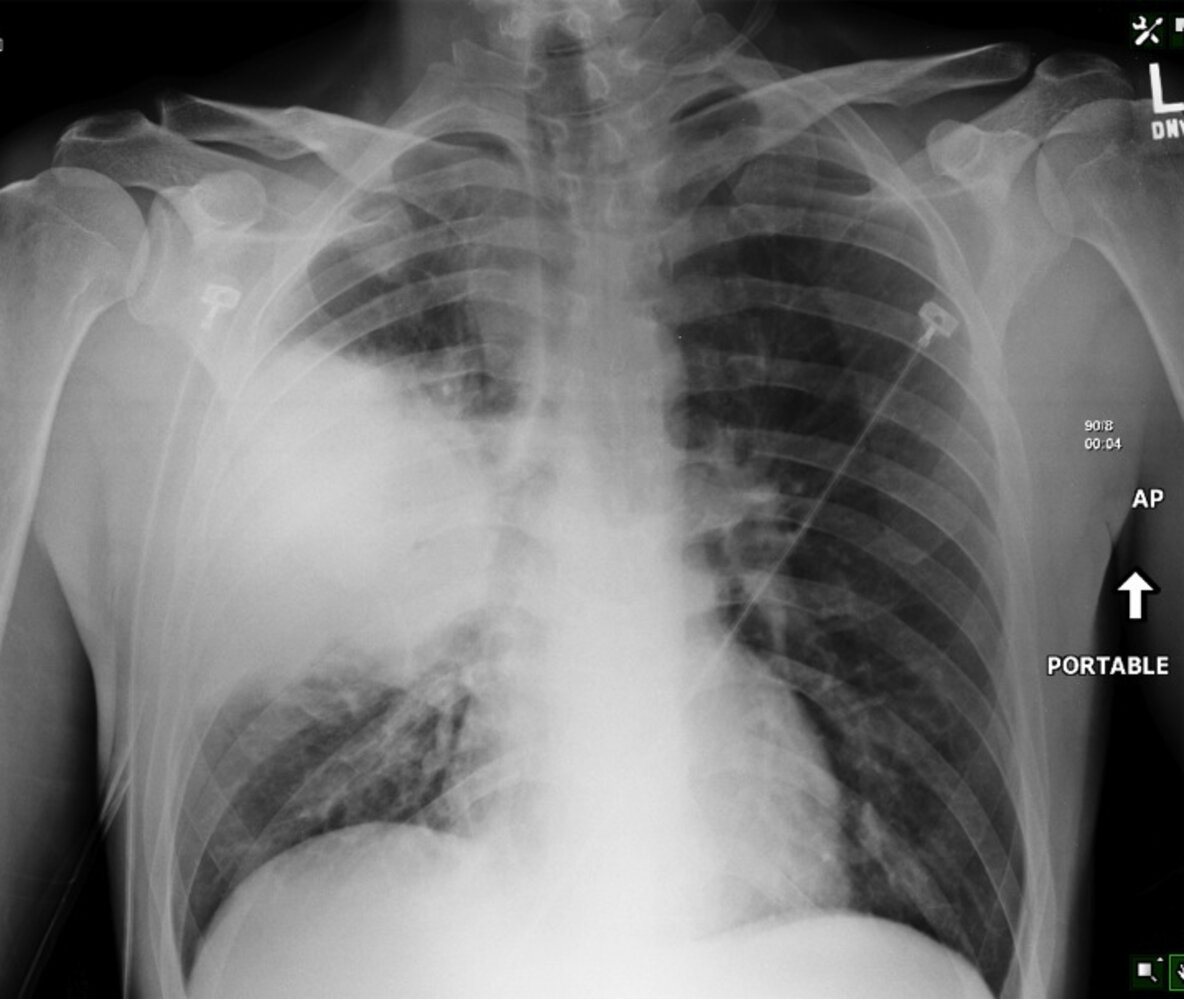
X-ray chest (PA view)
A large area of opacification (green overlay) in the left lung obscures pulmonary vessels, the left heart border, and the left hilum. Air bronchograms are visible (indicated by red lines), consistent with the presence of air space disease. Non-visualization of the hilum limits the ability to assess for a central mass.
Source: © IMPP
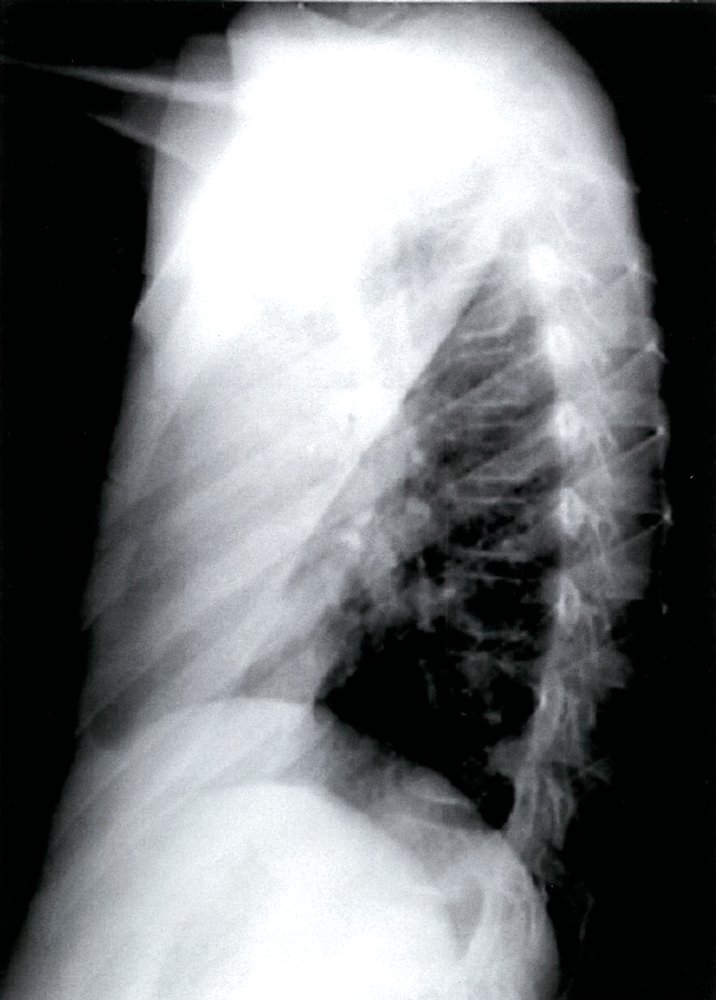
X-ray chest (lateral view)
Marked opacification of the left upper lobe (UL) is accompanied by volume loss; the major fissure (red line) is located anterior to its normal position (indicated by dashed line) and the left lower lobe (LL) is hyperinflated.
Source: © IMPP
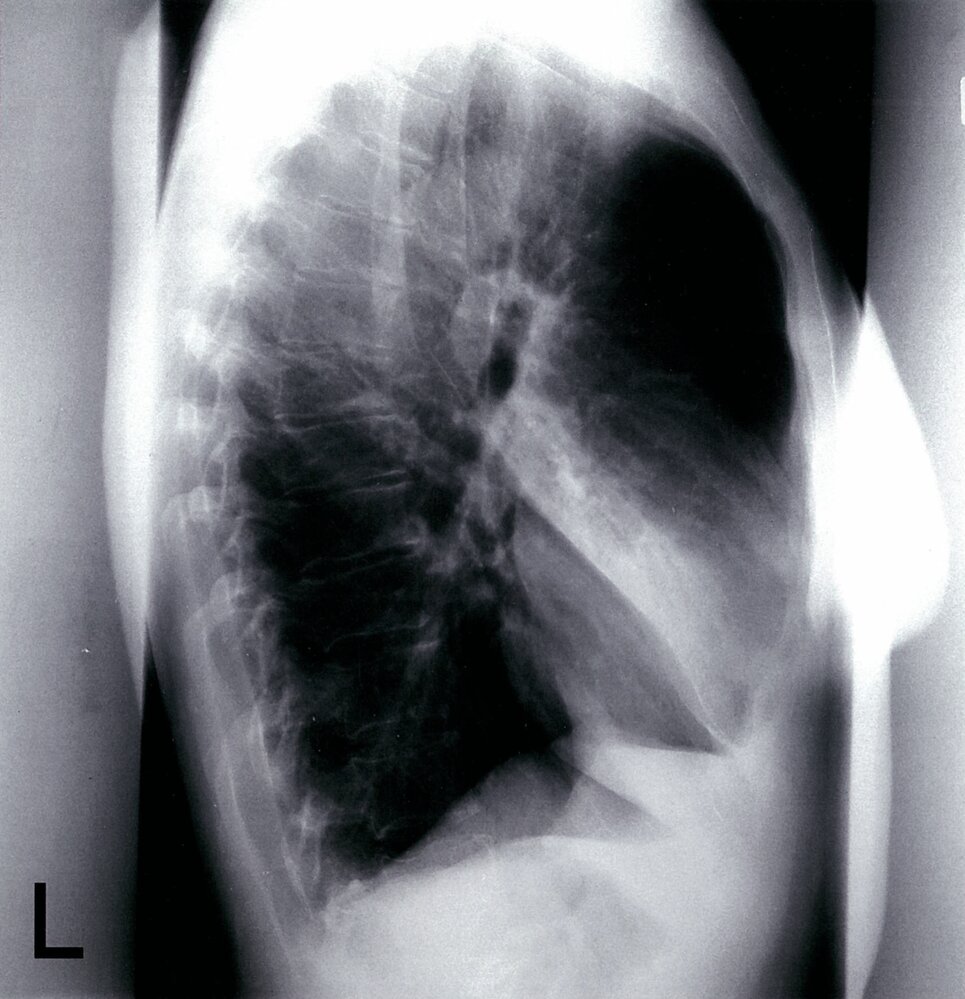
X-ray chest (lateral view) of a patient with a history of Legionella pneumonia
Subtle opacification (green overlay) is seen in the anterior upper thorax superior to a partially visible major fissure (red dashed line). The PA view showed air-space disease medially in the left lung, which correlates with this abnormality. When viewed together, the radiographs show that the abnormality is in the left upper lobe.
LL: lower lobe; T: trachea
Source: © IMPP
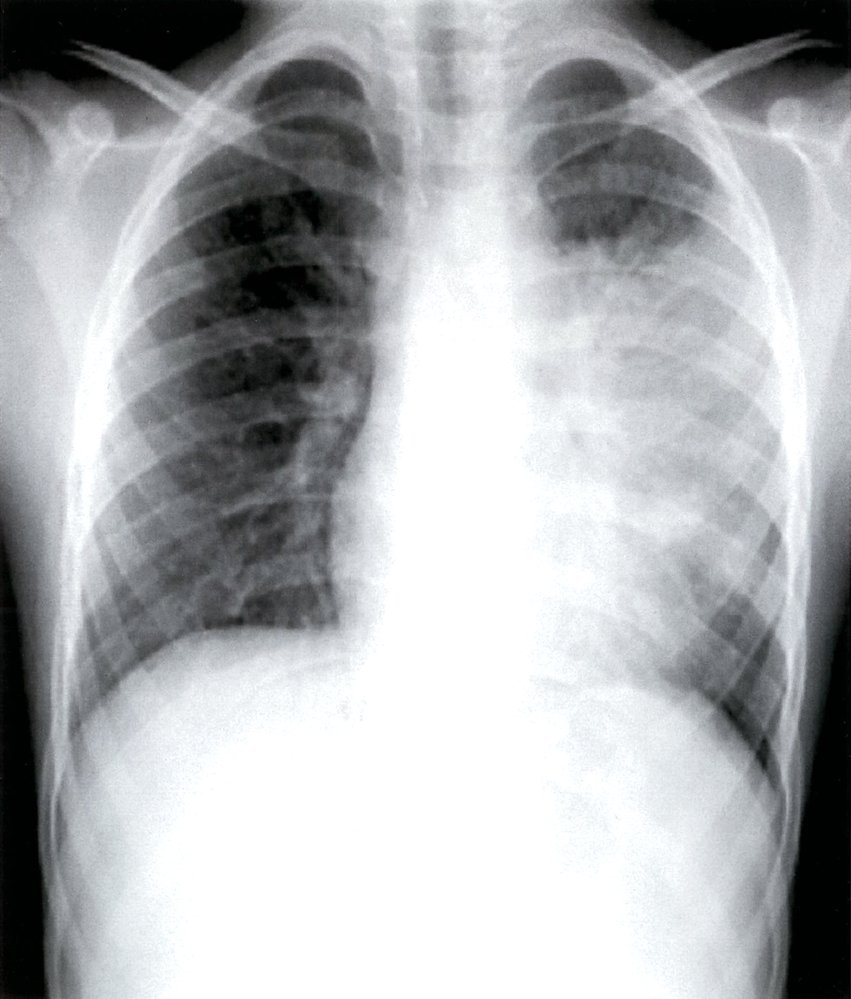
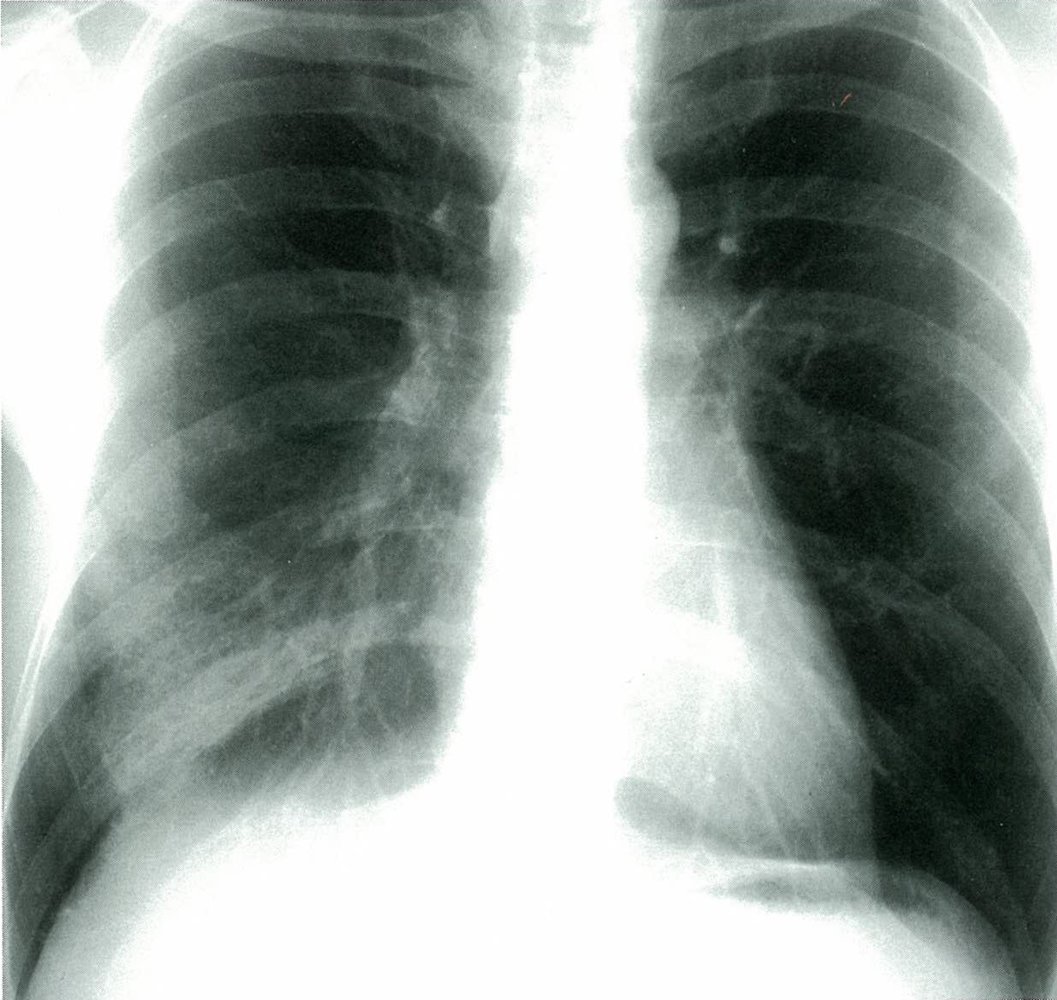
X-ray chest (PA view) of a febrile patient with a severe cough and right-sided chest pain
Heterogeneous opacification (green overlay) from consolidation in the middle and lower right lung projects through the right breast shadow. In the absence of comparison studies, the radiograph cannot distinguish whether the cause is acute or chronic.
Source: © IMPP
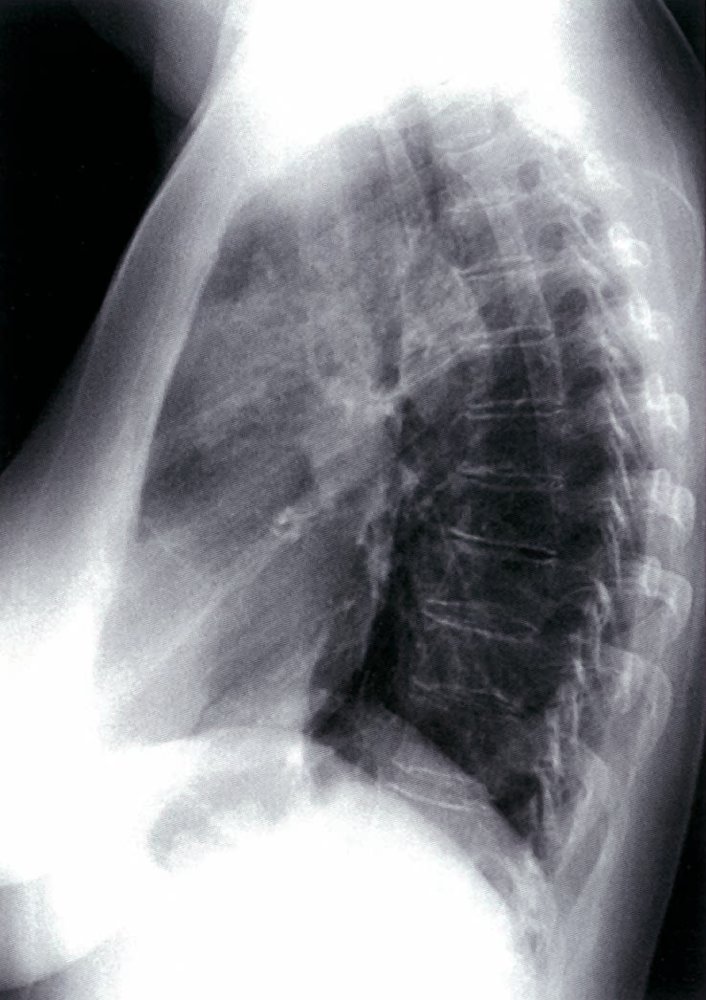
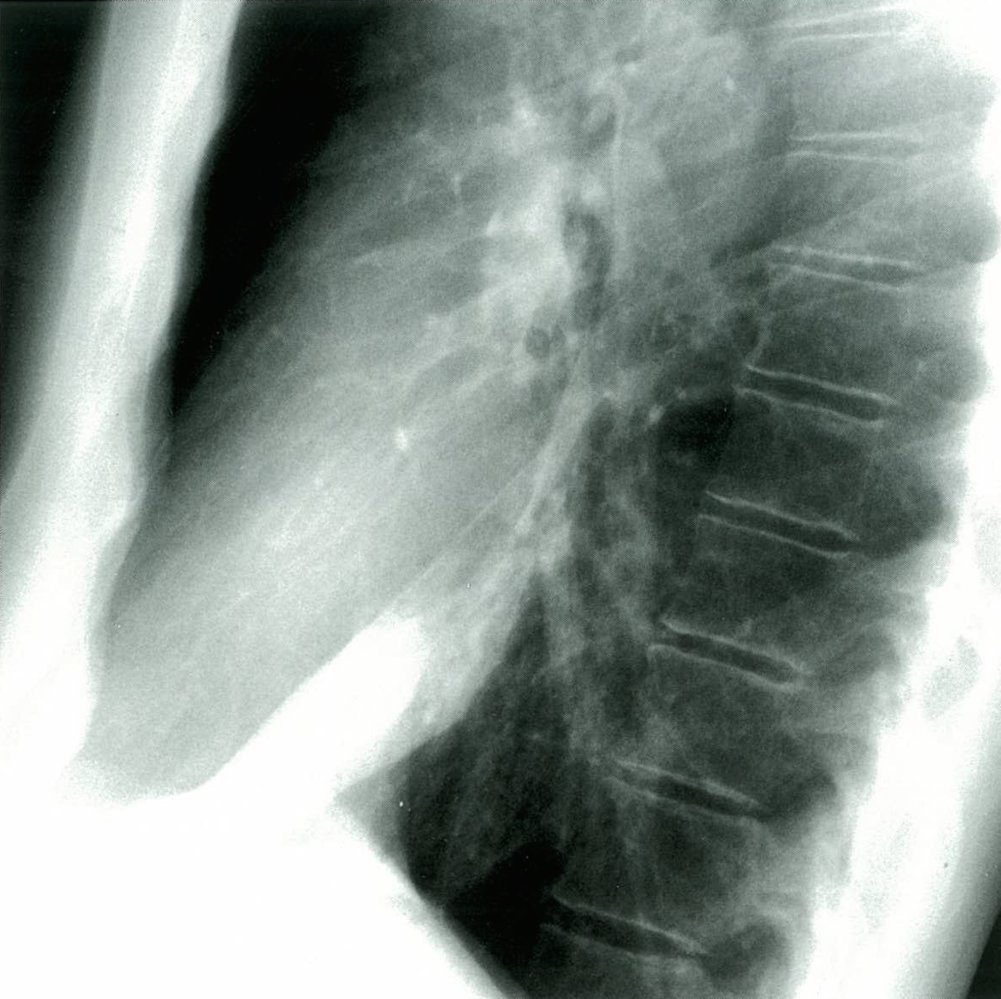
X-ray chest (lateral view)
Opacification (green overlay) projecting over the cardiac silhouette abuts the major fissure (black dashed line), which is slightly displaced superiorly consistent with a small component of volume loss. A PA view showed the abnormality to be located on the right side. The opacification is compatible with air space consolidation in the right middle lobe (ML). In the absence of comparison studies, the radiograph cannot distinguish whether the cause is acute or chronic.
LL: lower lobe; UL: upper lobe; white dashed line: minor fissure
Source: © IMPP

X-ray chest (left: PA view; right: lateral view) of a patient with history of pneumonia
Extensive heterogeneous air space consolidation (green overlay) in the left upper lobe abuts part of the major fissure (dashed line). A small pleural effusion is present.
Examples of causes of pulmonary consolidation that can mimic the appearance of infectious pneumonia include organizing pneumonia, malignancy (adenocarcinoma, lymphoma), and pulmonary hemorrhage.
Red: meniscus of pleural effusion
Source: “Lobaerpneumonie” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: Arrows removed and lateral picture flipped (left to right).. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
X-ray chest (PA and lateral views) of a patient with pneumonia
There is heterogeneous right upper lobe consolidation (green overlay) with air bronchograms (examples of bronchial walls indicated by white lines). The major (white dashed line) and minor fissures (red dashed lines) are elevated from normal position as a result of accompanying atelectasis. No hilar enlargement or pleural effusion is seen.
The differential diagnosis for airspace consolidation considers the radiographic appearance, associated findings (e.g., lymphadenopathy, pleural effusion), and patient history and symptoms. Pneumonia, hemorrhage, edema, tumor, and protein can all present as consolidation on a chest radiograph.
Green line: aortic arch margin; LL: lower lobe; ML: middle lobe; UL: upper lobe
Source: © IMPP
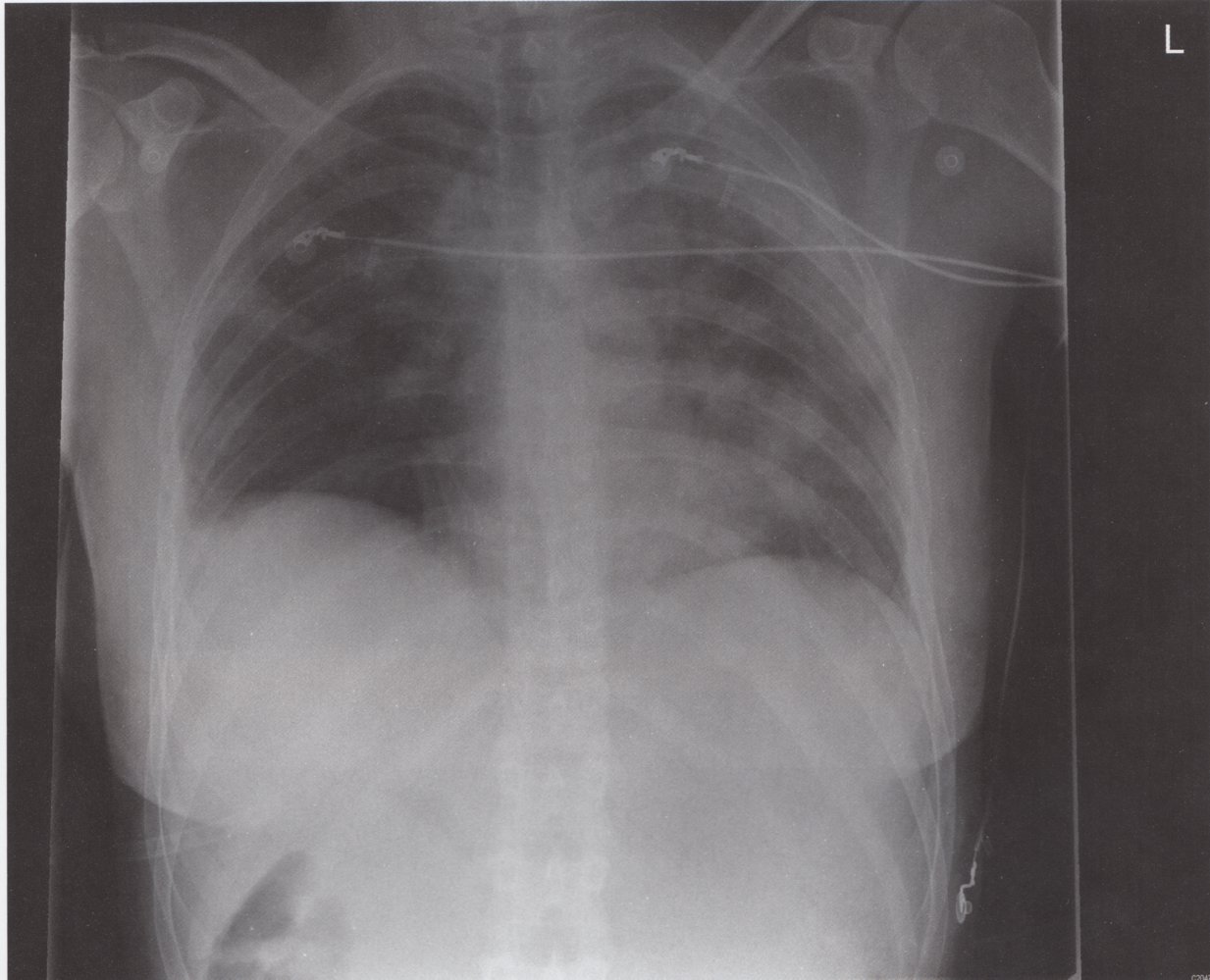
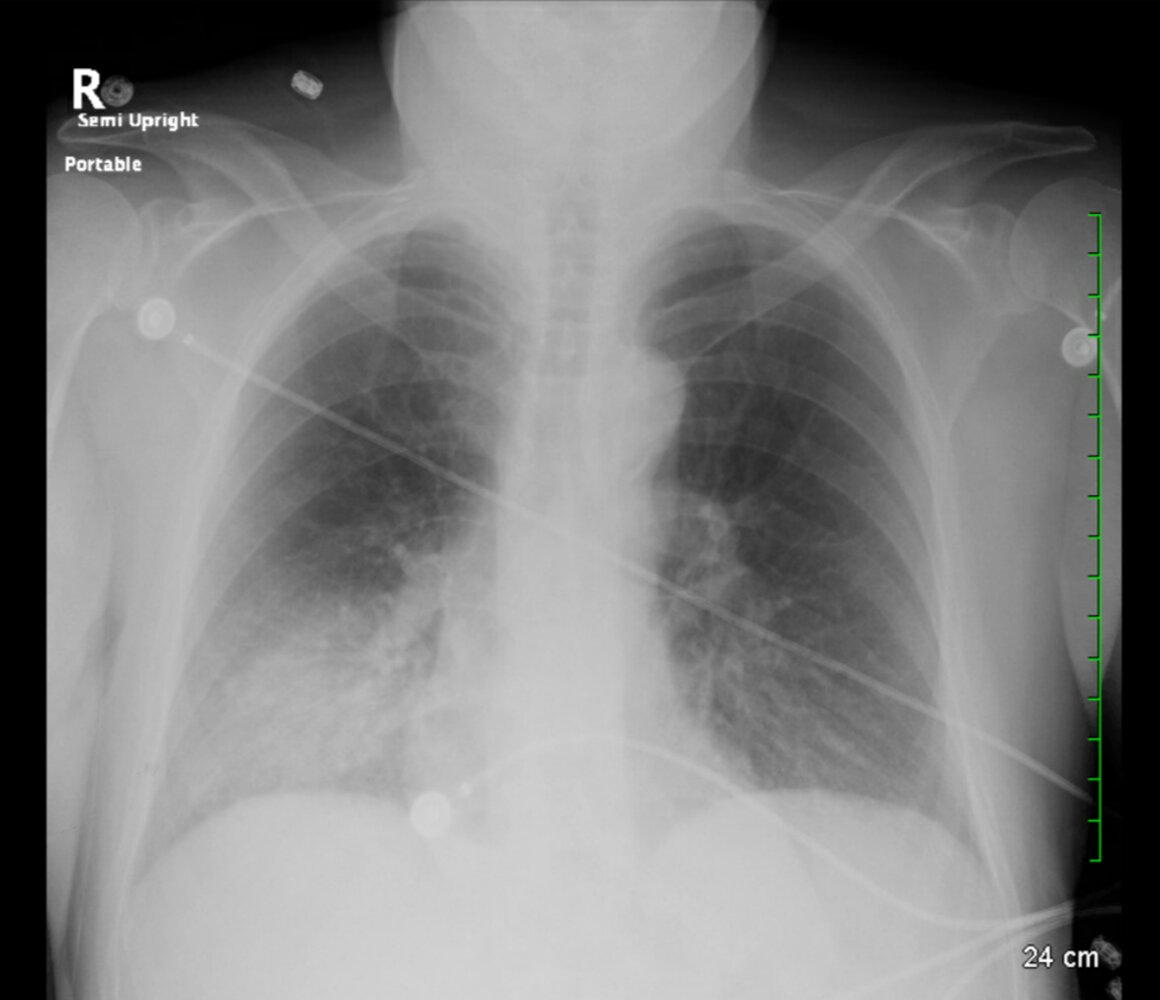
X-ray chest (AP view) of a patient with symptoms of pulmonary infection
Numerous ill-defined opacities (examples indicated by green overlay) are present in both lungs. ECG electrodes and lead wires are also seen.
Bronchopneumonia is characterized by multifocal opacities that may involve one or more lobes of the lung. The infection is airway-centered and progresses to involve the lung parenchyma. Opacities sometimes coalece and mimic lobar pneumonia.
Bronchopneumonia is commonly caused by bacterial infections, such as S. aureus, K. pneumoniae, E. coli, H. influenzae, and P. aeruginosa. It may also be caused by viral and fungal infections. Certain neoplasms, granulomatous diseases, and inflammatory conditions can produce a similar appearance of multifocal opacities.
Source: © IMPP
X-ray chest (PA view) of a patient with a history of pneumonia
An ill-defined area of opacification in the lower right lung (green overlay) extends inferiorly to obscure part of the margin of the right hemidiaphragm.
Source: © IMPP
X-ray chest (lateral view) of a patient with a history of pneumonia
A homogeneous area of opacification (green overlay) abuts the major fissure (red dashed line) anteriorly and extends inferiorly to obscure part of the margin of the adjacent hemidiaphragm (black dashed line).
Source: © IMPP
X-ray chest (PA view)
Diffuse, bilateral, interstitial opacification (blue overlay) can be seen extending from the hila to the periphery of the lungs.
This appearance is characteristic of PCP infection.
Source: "PCP CAP CXR", Samir, Wikimedia Commons licensed under Public Domain
{kind=link}
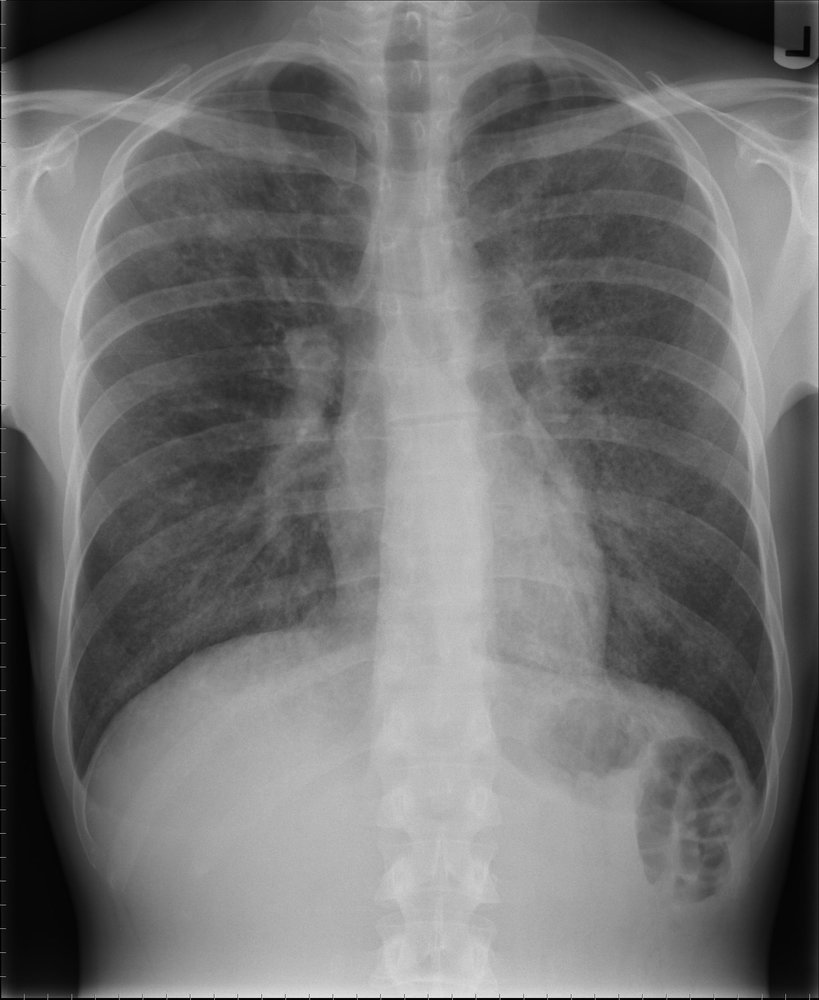
X-ray chest (AP view; semierect) of a patient with clinical presentation of pneumonia
Ill-defined air space opacification is seen in the lower right lung (arrows). Small portions of the right hemidiaphragm are obscured, which suggests that the right lower lobe is involved. Close proximity to the right heart border also raises the question of right middle lobe (medial segment) involvement. PA and lateral views could help distinguish lower and middle lobe involvement.
The radiographic findings favor aspiration as the cause of pneumonia. The lower lobe of the right lung is the most common site of aspiration pneumonia in an erect patient due to the vertical orientation of the right main bronchus and its larger caliber compared to the left main bronchus.
Source: “Figure 1, in: A Rare Case of Coexisting Psychogenic Polydipsia and Nephrogenic Diabetes Insipidus With Lithium Therapy” by Antala D, Sharma A, Adhikari A, et al., Cureus, licensed under CC BY 4.0. Modifications: removed black arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
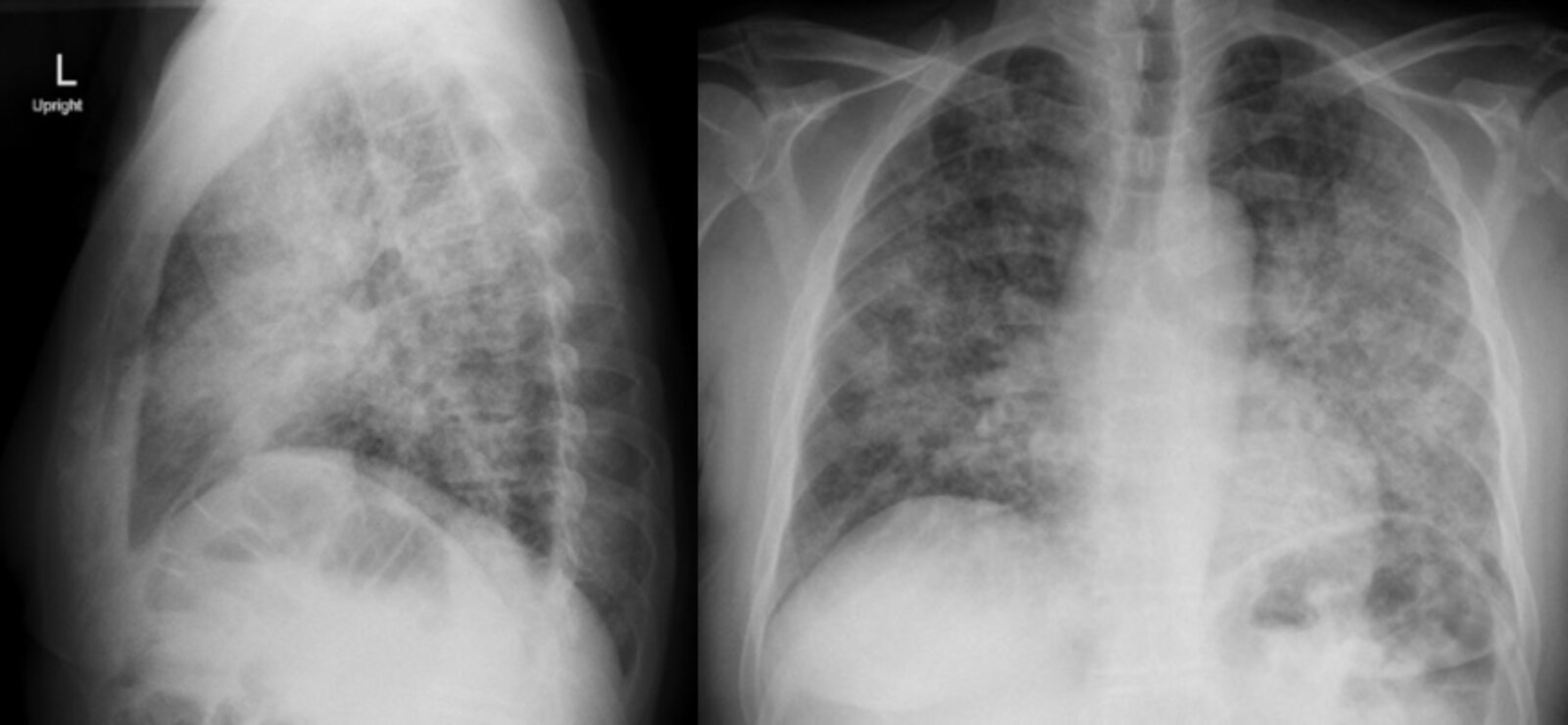
X-ray chest (left: lateral view; right: AP view) of a patient with a medical history of untreated HIV
Chest x-ray reveals diffuse, patchy interstitial, and alveolar infiltrates bilaterally. The (left-sided) perihilar lung shadowing (also known as “bat wing” or “butterfly opacities”) in AP view is concerning for Pneumocystis jirovecii infection.
Source: “Fig. 1, in: Pneumocystis jirovecii (carinii) Pneumonia” by Brian Knight; Jonathan Patane; Robert Katzer, JETem, licensed under CC BY 4.0. Modifications: - image is product of two separate images.
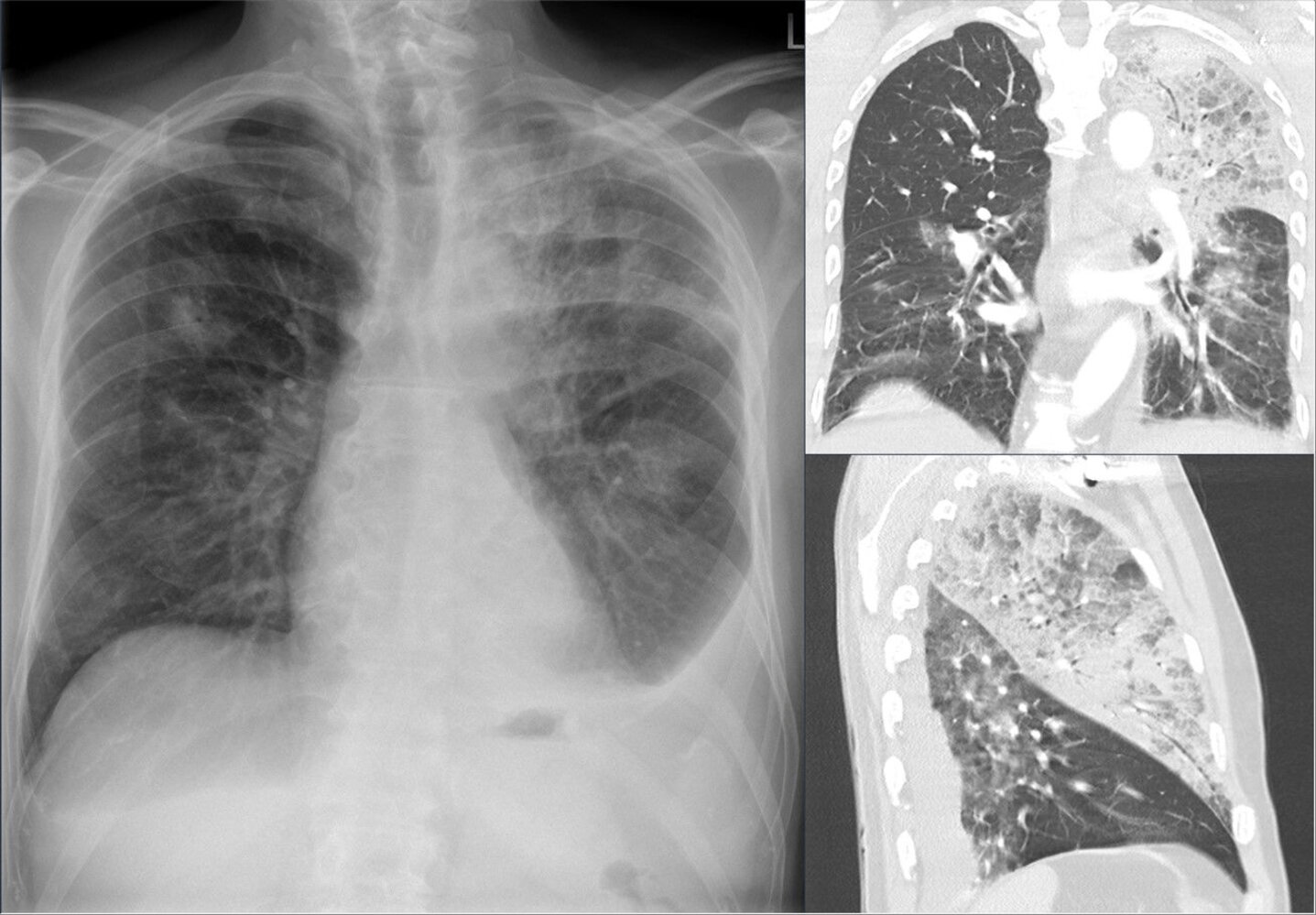
X-ray chest (left; PA view) and CT chest (right; lung window; top: coronal plane; bottom: sagittal plane) of a patient with Legionella pneumonia
Scattered ill-defined opacities are seen in both lungs, and extensive air space consolidation is present in the left upper lobe (green overlay). The latter is accompanied by slight elevation of the major fissure (arrowheads), indicating volume loss. Bilateral pleural effusions (red overlay), left greater than right, are present .
The imaging features of Legionella pneumonia are variable. Consolidation can manifest in a single lobe or as bilateral and multifocal opacities. Pleural effusions are common. Radiographic findings may lag behind clinical improvement.
Source: “Legionellenpneumonie vor allem im linken Oberlappen 65M - CR pa und CT koronar und sagittal - 001” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}

© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.

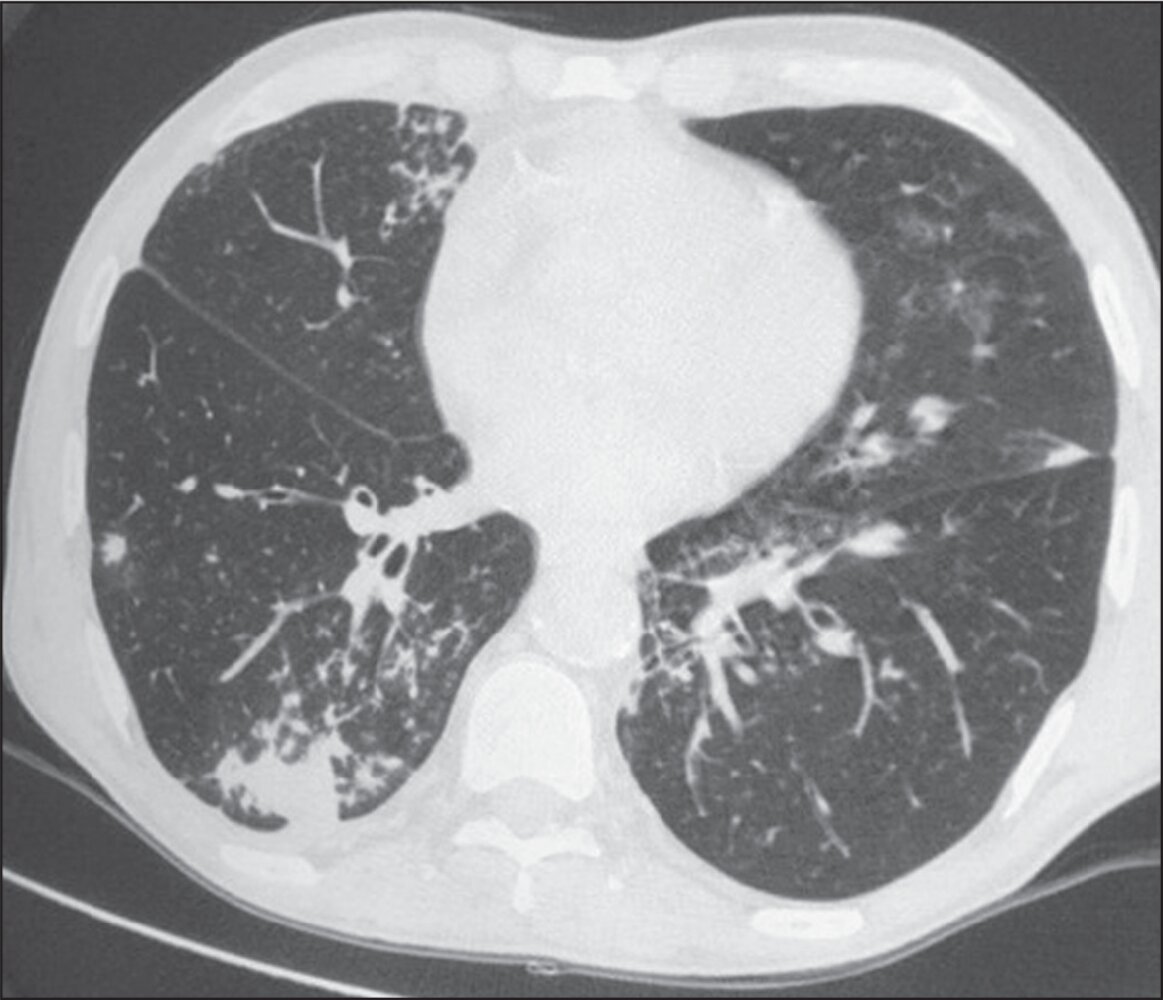
CT chest (with contrast; axial plane; lung window) of a patient with a 2-week history of productive cough 10 months after kidney transplantation
Multiple foci of centrilobular nodularity are seen bilaterally (examples indicated by red overlay). Some nodular areas show coalescence into air space consolidation. The largest of these is in the right lower lobe (green overlay). Airway disease is also seen, with thickening of bronchial walls in multiple locations (examples indicated by blue overlay).
The history and bronchopneumonia pattern prompted bronchoalveolar lavage, which revealed M. tuberculosis.
Source: “Fig 2, In: Padrões tomográficos de agentes etiológicos da pneumonia durante o primeiro ano após transplante renal” by Damázio LOA, Lins EM, Ferraz AAB et al., SciELO, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
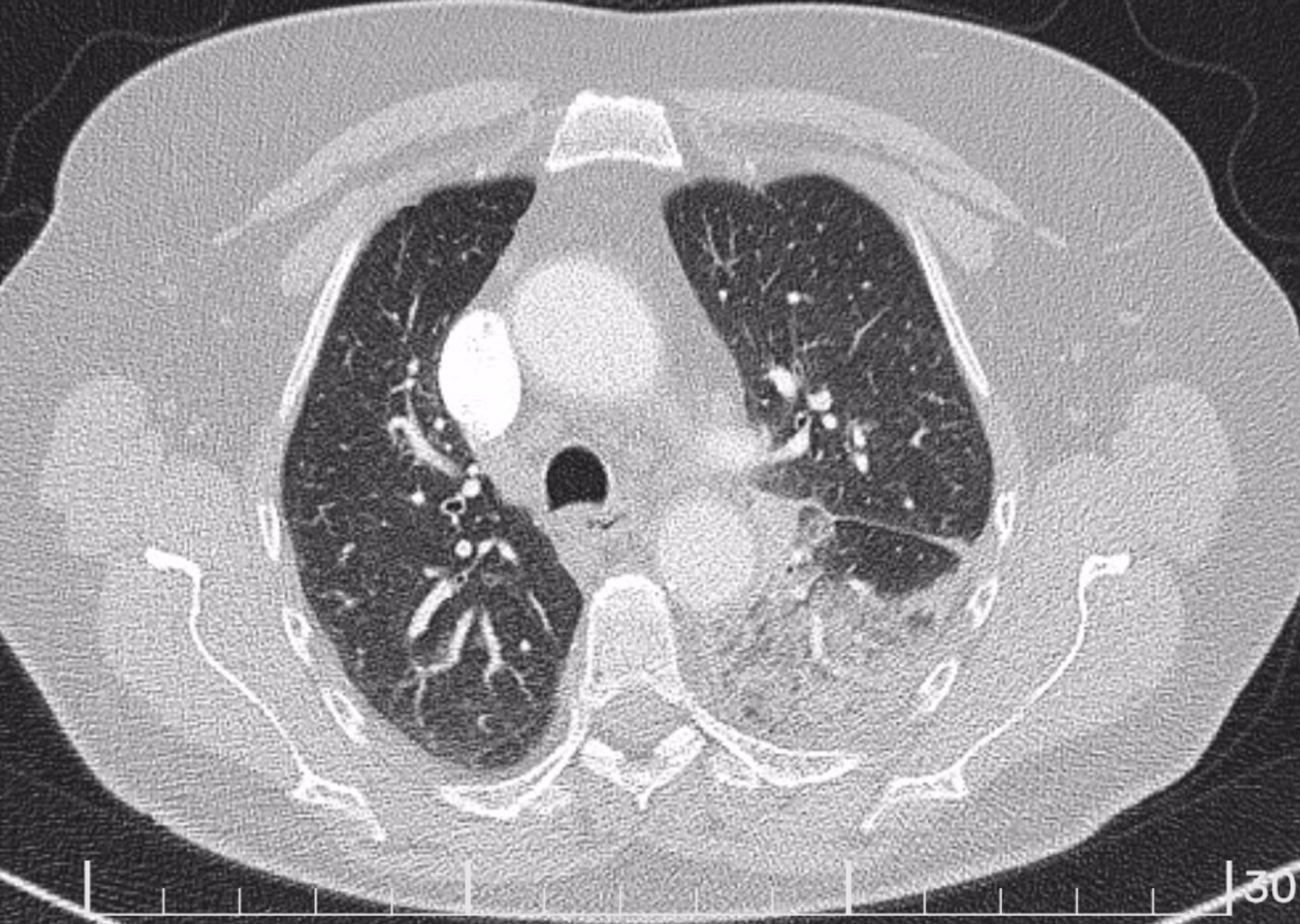
CT chest (with contrast; axial plane, mediastinal window; axial plane, lung window) of a patient with symptoms of pneumonia
Dense consolidation nearly completely opacifies the left lower lobe. Some areas of relative sparing are seen, especially within the superior segment. Reactive lymph nodes are present along the left superior mediastinum and central pulmonary vessels. There is a very small left pleural effusion .
Our great thanks to Nandor Faluhelyi M.D., Ph.D. (University of Pécs, Medical School) for kindly providing this image.

CT chest (axial plane; lung window) of a patient with a history of bacterial pneumonia
Opacification of much of the right lower lobe parenchyma is the result of air space consolidation. Pulmonary vessels are obscured and patent airways (air bronchograms, white dashed line) are seen. Consolidation extends to the major fissure (green overlay).
Parenchymal opacification can be caused by fluid or solid material. Major causes in the acute setting include pneumonia, aspiration, edema, and hemorrhage. In the chronic setting, the main causes include invasive adenocarcinoma and alveolar proteinosis.
Source: © IMPP
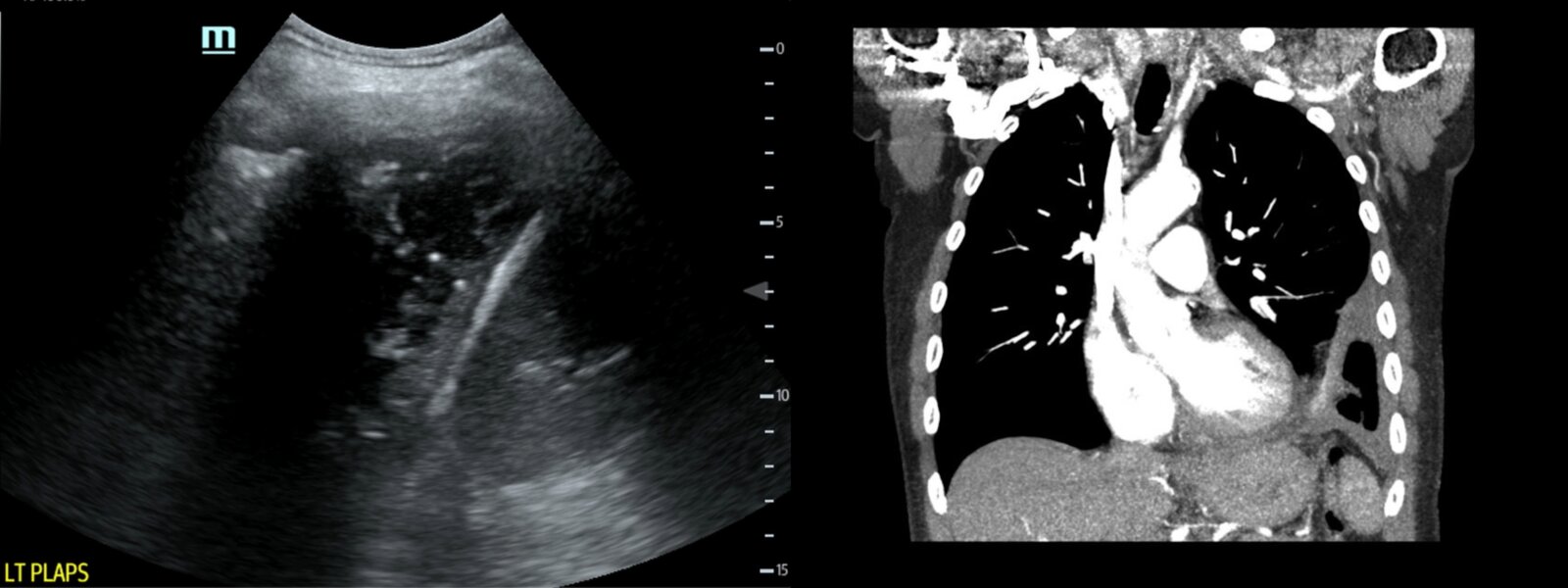
Ultrasound (left mid-axillary line) and CT chest (coronal plane) of a patient with hypoxia and productive cough with yellow sputum
Ultrasound demonstrates a loculated left-sided pleural effusion of moderate size (green overlay) in the lower lobe. Its inferior margin is outlined by the diaphragm (red overlay). On the left side of the image, rib shadowing (white overlay) hides the full extent of effusion. CT confirms the diagnosis of left-sided loculated pleural effusion (green overlay).
The clinical findings and imaging are suspicious for empyema.
Source: “Fig. 2 and 3, in: Case Report of an Empyema Identified on Lung Ultrasound” by Michelle Brown; Carly Heffernan; Alisa Wray, JETem, licensed under CC BY 4.0. Modifications: - image is product of two separate images. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
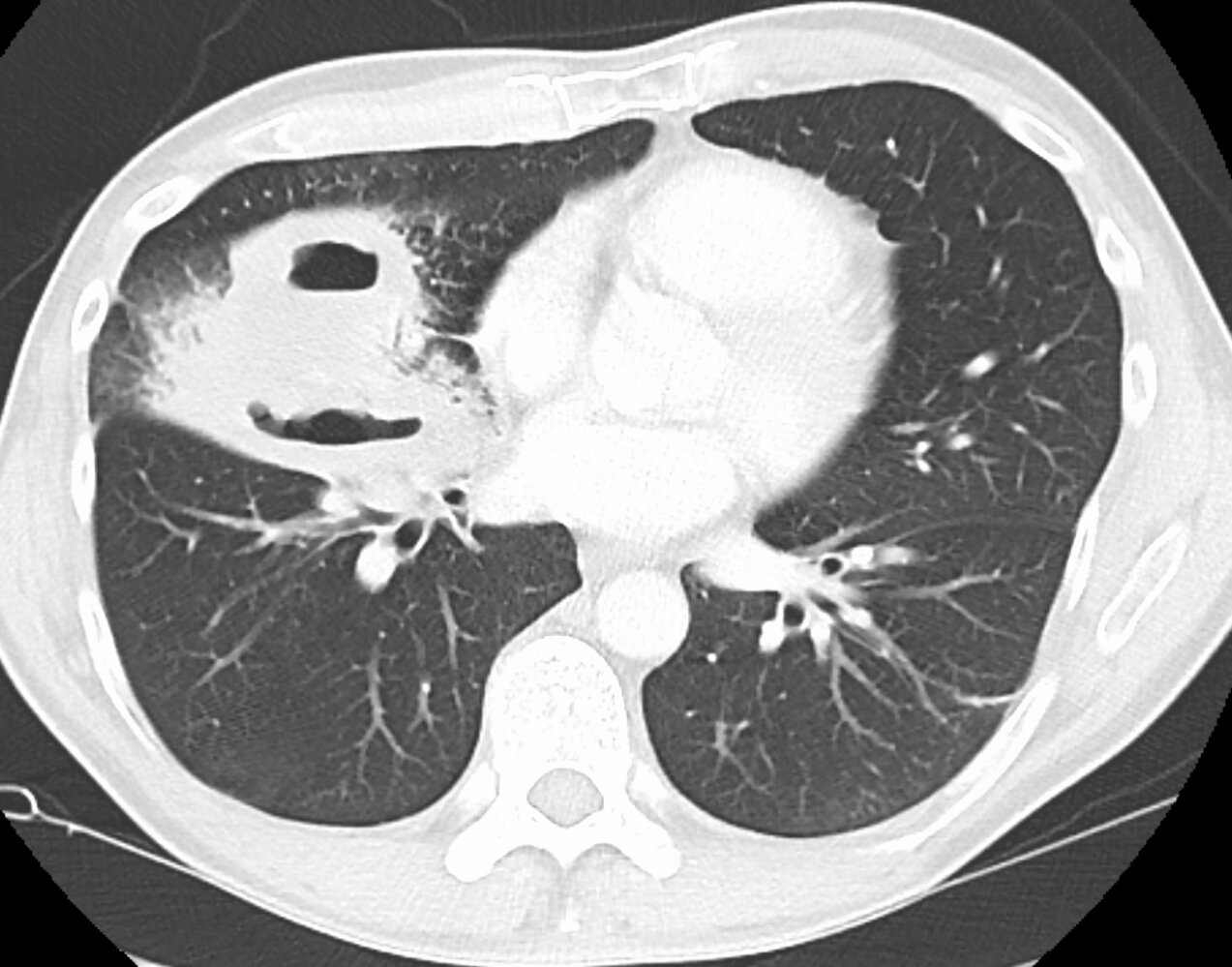
CT chest (axial plane; lung window) of a patient with pneumonia and lung abscesses
Two thick-walled cavitary lesions (green overlay) are seen in the right middle lobe. A sharp air-fluid level is visible within the anterior cavity. Air bronchograms (examples indicated by red overlays) are present within the surrounding consolidation.
Source: “PulmonaryabsNo” by Doc James, Wikimedia commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
Disposition
Criteria for hospitalization [18][22]
Every patient should be assessed individually; clinical judgment is the most important factor. The pneumonia severity index (PSI) and the CURB-65 score are tools that can help to determine whether to admit a patient.
-
Pneumonia severity index (PSI/PORT score) [18][30]
- Patients are assigned to one of five risk classes based on a more complex point system than in CURB-65.
- Points are distributed based on patient age, comorbidities, and lab results.
-
CURB-65 score ; [31]
- Confusion (disorientation, impaired consciousness)
- Serum Urea/BUN > 7 mmol/L
- Respiratory rate ≥ 30/min
- Blood pressure: systolic BP ≤ 90 mm Hg or diastolic BP ≤ 60 mm Hg
- Age ≥ 65 years
-
Interpretation
- Each finding is assigned 1 point.
- CURB-65 score 0 or 1: The patient may be treated as an outpatient.
- CURB-65 score ≥ 2: Hospitalization is indicated.
- CURB-65 score ≥ 3: Consider ICU level of care.
-
CRB-65 score (if serum urea is not known or unavailable)
- CRB-65 score of 0: The patient may be treated as an outpatient.
- CRB-65 score of ≥ 1: Hospitalization is recommended.

The CURB-65 score and PSI are tools for evaluating the risk of mortality. They have not been validated for determining the necessity for ICU admission.
Criteria for ICU admission (severe CAP) [18][22]
- The IDSA/ATS criteria for severe CAP can be used to triage patients with CAP and guide diagnostic testing and empiric antibiotic therapy decisions. [18]
- The decision of whether to admit a patient to the ICU should be based on clinical judgment.
| IDSA/ATS criteria for severe CAP [18] | |
|---|---|
| Major criteria |
|
| Minor criteria |
|
Interpretation
| |
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Treatment
Approach
- Evaluate all patients for hypoxemia and sepsis and manage as indicated.
- Determine the appropriate level of care using clinical judgment and prediction tools (e.g., PSI score and IDSA/ATS criteria for severe CAP).
- Begin empiric antibiotic therapy based on severity and patient risk factors (e.g., VAP vs. CAP).
- Consider antiviral therapy for influenza and COVID-19 as indicated.
-
Glucocorticoids
- Consider initiating hydrocortisone within 24 hours of diagnosis in patients being treated for severe CAP in the ICU. [16][32]
- Not recommended for nonsevere CAP [16][20]
- Reevaluate therapy within 48 hours.
Consider deferral of antibiotic therapy in outpatients with a viral diagnosis and no comorbidities. [16]

Initial stabilization [20][33][34]
- Identification and management of sepsis
- Fluid resuscitation and management of septic shock as needed
-
Respiratory support as needed
- Supplemental oxygen for hypoxia
- HFNC oxygen therapy, NIPPV, or intubation for respiratory failure
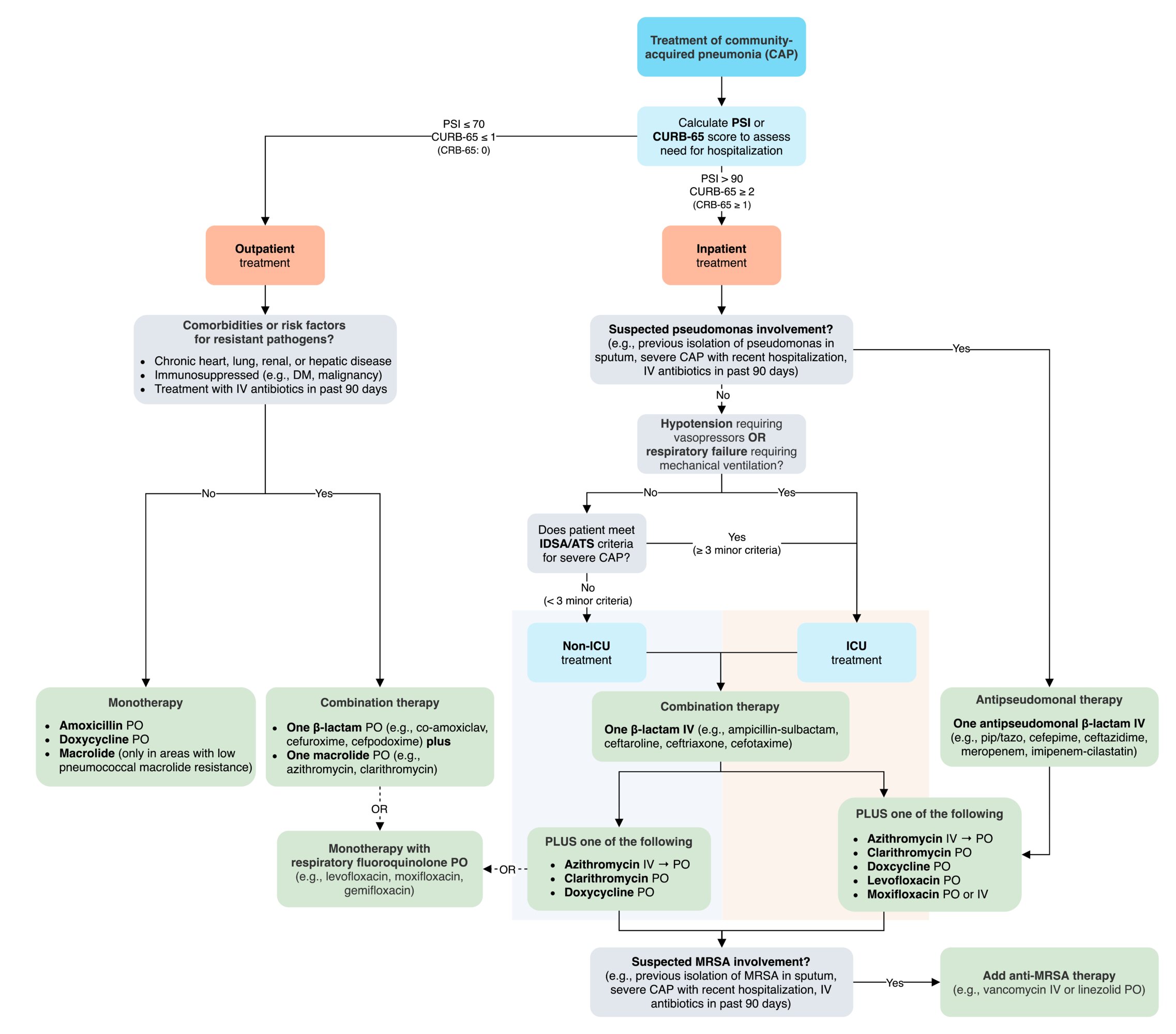
Empiric antibiotic therapy for community-acquired pneumonia [12][13][18]
Outpatient
| Empiric antibiotic therapy for community-acquired pneumonia in an outpatient setting | |
|---|---|
| Patient profile | Recommended empiric antibiotic regimen [13][18] |
| Previously healthy patients without comorbidities or risk factors for resistant pathogens |
|
| Patients with comorbidities or risk factors for resistant pathogens |
|
-
Duration of treatment
- 3 to 4 days of therapy is usually sufficient for CAP that is treated in the outpatient setting. [16]
- Any patient being treated in a primary care setting should be re-examined after 48–72 hours to evaluate the efficacy of the prescribed antibiotic.
- Additional considerations: Knowing local resistance patterns of S. pneumoniae to macrolides is critical when deciding on an empiric antibiotic regimen.
Inpatient
| Empiric antibiotic therapy for community-acquired pneumonia in an inpatient setting | |
|---|---|
| Patient profile | Recommended empiric antibiotic regimen [12][13][18] |
| Nonsevere CAP/non-ICU treatment |
|
| Severe CAP/ICU treatment |
|
| Risk factors for Pseudomonas aeruginosa |
|
| Risk factors for MRSA (or positive nasal swab) |
|
-
Duration of treatment
- The following courses are recommended for inpatients who reach clinical stability: [16]
- Nonsevere CAP: 3–4 days [16]
- Severe CAP: ≥ 5 days [16]
- Consider longer courses for any of the following:
- Not responding to treatment [16]
- Concern for MRSA or P. aeruginosa infection [16]
- Concurrent meningitis
- Unusual pathogens (e.g., Burkholderia pseudomallei, fungal infection)
- The following courses are recommended for inpatients who reach clinical stability: [16]
-
Additional considerations
- If aztreonam is used instead of a β-lactam antibiotic (e.g., for penicillin allergy), the addition of MSSA coverage (e.g., a fluoroquinolone) is necessary.
- Anaerobic coverage is not routinely recommended for suspected aspiration pneumonia (unless lung abscess or empyema is suspected). [18]
If aztreonam is used as an alternative to other β-lactam antibiotics, additional coverage for MSSA must be included (e.g., a fluoroquinolone).
Empiric antibiotic therapy for hospital-acquired pneumonia [10]
| Empiric antibiotic therapy for hospital-acquired pneumonia | |
|---|---|
| Patient profile | Recommended empiric antibiotic regimen [10] |
| Patients not at high risk for mortality and without risk factors for MRSA infection |
|
| Patients not at high risk for mortality but with risk factors for MRSA infection |
|
| Patients at high risk for mortality Patients with structural lung disease (e.g., cystic fibrosis, bronchiectasis) |
|
-
Duration of treatment
- Empiric antibiotic therapy should be narrowed and/or de-escalated as soon as feasible.
- Seven days of therapy are usually sufficient. [10]
- Additional considerations: Resistance patterns can vary widely; local antibiograms should be considered when starting empiric treatment.
Patients with structural lung disease and/or at high risk for mortality should receive double antipseudomonal coverage!
Empiric antibiotic therapy for ventilator-associated pneumonia [10]
-
Recommended combination therapy
-
An antipneumococcal, antipseudomonal β-lactam
- Aztreonam
- Imipenem
- Meropenem
- Ceftazidime
- Cefepime
- Piperacillin-tazobactam
-
PLUS one of the following antibiotics with MRSA activity:
- Vancomycin
- Linezolid
-
PLUS one of the following:
-
A fluoroquinolone
- Levofloxacin
- Ciprofloxacin
-
An aminoglycoside
- Amikacin
- Gentamicin
- Tobramycin
-
A polymyxin
- Colistin
- Polymyxin B
-
A fluoroquinolone
-
An antipneumococcal, antipseudomonal β-lactam
- Duration of treatment: Seven days of therapy are usually sufficient. [10]
-
Additional considerations:
- Risk factors for multi-drug resistant organisms (e.g., presence of structural lung disease, recent IV antibiotic therapy, local resistance patterns) should be considered when deciding on an empiric regimen
- Empiric antibiotic therapy for ventilator-associated tracheobronchitis is not routinely recommended. [10]
Supportive therapy for pneumonia
- Sufficient rest (not absolute bed rest) and physical therapy
- Hydration with PO or IV fluids, supplemental oxygen as needed
- Incentive spirometer
- Antipyretics, analgesics as needed (e.g., acetaminophen )
- Expectorants and mucolytics [35]
- Antitussives (e.g., codeine )
© AMBOSS
Dot phrase
Community-acquired pneumonia (severe)
Assessment: This is a @AGE@-year-old @SEX@ presenting with [**fever, productive cough, tachypnea, tachycardia] found to have severe CAP requiring ICU admission based on [**respiratory failure (hypoxemia (PaO2/FiO2 < 250), need for mechanical ventilation), sepsis/shock (persistent hypotension requiring vasopressors despite fluids), radiological findings (multilobar infiltrates on chest x-ray/CT), clinical features fever, productive cough, tachypnea, tachycardia), labs (leukocytosis/leukopenia, elevated CRP/procalcitonin, lactic acidosis)].
Differential diagnoses: viral pneumonia (e.g., due to influenza, SARS-CoV-2), aspiration pneumonia, acute exacerbation of COPD, acute heart failure
Plan: Admit to ICU.
Diagnostics (if not already done)
–Cultures: blood, sputum, and pleural fluid if effusion present
–Labs: CBC, CMP, lactate, CRP, procalcitonin, ABG
–Imaging: Repeat chest x-ray/CT PRN.
–Pathogen-specific tests: influenza, SARS-CoV-2, Legionella urine antigen, pneumococcal urine antigen
Stabilization and monitoring
–Continuous SpO2, telemetry, hourly vitals
Respiratory support
–High-flow oxygen or noninvasive ventilation
–Intubation and mechanical ventilation [if PaO2< 60 mm Hg or significant distress]
Hemodynamic support
–IV fluids: 500–1,000 mL LR over 10–30 minutes; repeat PRN.
–[Vasopressors (e.g., norepinephrine) if shock]
Empiric antibiotics (started within 1 hour of diagnosis)
–[Ceftriaxone 1–2 g IV once daily] OR [Ampicillin/sulbactam 3 g IV every 6 hours]
OR if pseudomonas risk factors: [piperacillin/tazobactam 4.5 g IV every 6 hours] OR [cefepime 2 g IV every 8 hours]
–PLUS [Azithromycin 500 mg IV daily] OR [Doxycycline 100 mg IV every 12 hours] OR [Moxifloxacin 400 mg PO/IV once daily] OR [Levofloxacin 750 mg PO once daily]
–PLUS if risk factors for MRSA: [vancomycin 15 mg/kg IV every 12 hours; adjust based on serum trough levels] OR [linezolid 600 mg IV/PO every 12 hours]
Supportive care
–Fever: acetaminophen
–DVT prophylaxis: LMWH
–Glycemic control: Maintain blood glucose at 140–180 mg/dL.
–Nutrition: enteral feeding if unable to eat
Community-acquired pneumonia (nonsevere, inpatient management)
Assessment: This is a @AGE@-year-old @SEX@ presenting with CAP based on symptoms [**fever, productive cough, dyspnea, pleuritic chest pain], radiological findings [**consolidation/infiltrates on chest x-ray], and laboratory findings [**leukocytosis, elevated CRP/procalcitonin].
Differential diagnoses: viral pneumonia (e.g., influenza, SARS-CoV-2), aspiration pneumonia, acute exacerbation of COPD or CHF
Severity assessment: nonsevere CAP as patient does not meet criteria for ICU admission (e.g., no respiratory failure, hemodynamic instability, or severe sepsis); [**PSI/CURB-65] score: [**]
Plan
–Disposition: Admit to medicine.
–Monitor vitals, SpO2, and clinical status.
–Labs: CBC, CMP, CRP or procalcitonin
–Pathogen-specific tests: influenza, SARS-CoV-2, Legionella urine antigen, pneumococcal urine antigen (if indicated)
–Repeat chest x-ray if no improvement after 48–72 hours or clinical deterioration.
Oral or IV antibiotics based on severity and ability to tolerate oral intake
–Preferred: ceftriaxone 1–2 g IV once daily PLUS azithromycin 500 mg PO once daily
–Alternative: amoxicillin 1 g PO three times daily PLUS azithromycin 500 mg PO once daily
–If contraindication to macrolides: doxycycline 100 mg PO twice daily
Adjust therapy based on culture results or pathogen-specific testing.
Supportive care
–Supplemental O2: Titrate to SpO2 ≥ 92%.
–Acetaminophen or ibuprofen for fever or pleuritic pain
–Encourage oral intake or provide IV fluids if dehydrated.
–DVT prophylaxis: LMWH if immobile
Monitoring and disposition
–Reassess clinical response daily: resolution of fever, improvement in respiratory symptoms, normalization of vitals
–Discharge criteria: clinically stable (afebrile, normalizing respiratory status) and able to tolerate oral intake
–Outpatient follow-up: PCP visit in 1–2 weeks after discharge
Community-acquired pneumonia (outpatient management)
Assessment: This is a @AGE@-year-old @SEX@ presenting with CAP based on symptoms [**fever, productive cough, dyspnea, and pleuritic chest pain], radiological findings [**consolidation/infiltrates on chest x-ray], laboratory findings (if available) [**leukocytosis, elevated CRP/procalcitonin].
Differential includes viral pneumonia (e.g., influenza, SARS-CoV-2), acute bronchitis, and aspiration pneumonia.
Severity assessment: Patient meets criteria for outpatient management of CAP based on stability of vitals, absence of respiratory failure, and ability to tolerate oral intake; [**PSI/CURB-65] score: [**]
Plan
–Amoxicillin 1 g PO three times daily for 5 days
–OR Doxycycline 100 mg PO twice daily for 5 days
–OR (if comorbidities or recent antibiotic use) Amoxicillin/clavulanate 875/125 mg PO twice daily plus azithromycin 500 mg PO daily for 5 days
–SARS-CoV-2 and influenza testing if clinically indicated
–Acetaminophen or ibuprofen for fever or pleuritic pain
–Adequate hydration and rest
Patient education
–Seek immediate care for worsening symptoms (e.g., high fever, increasing dyspnea, or confusion).
–Complete the prescribed antibiotic course.
–Smoking cessation [if applicable]
Follow-up
–48–72 hours via phone or clinic to assess symptom improvement
–Follow-up visit with PCP within 1–2 weeks after symptom resolution to ensure recovery and assess for any residual issues.
Acute management checklist
- Calculate the PSI score to identify patients who would benefit from admission.
- Assess severity of CAP with the IDSA/ATS criteria for severe CAP.
- Order microbiological workup as indicated by patient severity and risk factors.
- Community-acquired pneumonia: Start empiric antibiotics for CAP.
- Consider hydrocortisone for patients being treated for severe CAP in the ICU.
- Hospital-acquired pneumonia: Start empiric antibiotics for HAP.
- Ventilator-associated pneumonia: Start empiric antibiotics for VAP.
- Evaluate and treat sepsis if present.
- Administer supplemental O2 if patient is hypoxemic.
- Consider advanced diagnostic evaluation.
- Provide supportive care for pneumonia (e.g., antipyretics, IV fluids).
- Continuous pulse oximetry
- Trend inflammatory markers, procalcitonin.
- Narrow antibiotic therapy as soon as feasible.
Pathogen-specific pneumonia
Mycoplasma pneumonia [36]
-
Epidemiology
- One of the most common causes of atypical pneumonia
- More common in school-aged children and adolescents
- Outbreaks most commonly occur in schools, colleges, prisons, and military facilities.
-
Clinical features
- Generalized papular rash
- Erythema multiforme
- See “Atypical pneumonia”.
-
Diagnostics
- Subclinical hemolytic anemia: associated with elevated cold agglutinin titers (IgM)
- Interstitial pneumonia; , often with a reticulonodular pattern on chest x-ray
- Chest x-ray can show extensive pulmonary involvement in patients with mild pneumonia.
-
Treatment
- A macrolide, doxycycline, or fluoroquinolones
- Beta-lactam antibiotics are not effective
- See “Empiric antibiotics for CAP” for dosages and duration of treatment.

Other types of pathogen-specific pneumonia
- Legionnaire disease
- Pneumocystis pneumonia
- Pseudomonas aeruginosa: causes VAP
- Tuberculosis
- Primary influenza pneumonia
- Various viral infections (e.g., respiratory syncytial virus, hantavirus, adenovirus, CMV, SARS-CoV, SARS-CoV-2)
- Ornithosis

Trunk and right arm of an infant
Multiple erythematous macules are visible, arranged in concentric rings with a pale center and an outer erythematous margin. The macules are partly confluent and of different sizes.
These lesions are suggestive of erythema multiforme, a hypersensitivity reaction that can be caused by various infections (most commonly herpes simplex virus infections), certain drugs, or immune dysregulation.
Source: “Erythema multiforme EM 02” by Grook Da Oger, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
Aspiration pneumonia
Definitions
-
Aspiration
- The inhalation of foreign material into the respiratory tract
- Most commonly occurs after instrumentation of the upper airways or esophagus (e.g., upper GI endoscopy) or secondary to vomiting and regurgitation of gastric contents
- Aspiration pneumonia: a type of pneumonia that occurs as a result of oropharyngeal secretions and/or gastric contents aspiration
-
Aspiration pneumonitis
- Aspiration of gastric acid that initially causes tracheobronchitis, with rapid progression to chemical pneumonitis
- May cause ARDS in extreme cases
Patients may develop aspiration pneumonitis without pneumonia, aspiration pneumonia without pneumonitis, or aspiration pneumonitis complicated by pneumonia. [37]
The risk of developing aspiration pneumonia and the severity of lung injury are directly related to the volume of aspirated material. [38][39]
Etiology
-
Pathogens [18][37]
- Gram-positive and gram-negative aerobic bacteria predominate in community-acquired infections (e.g., S. pneumonia, S. aureus, H. influenza, Enterobacteriaceae).
- Gram-negative bacilli predominate in hospital-acquired infections (e.g., P. aeruginosa, Klebsiella spp.).
- Mixed infections with anaerobic organisms; may occur (e.g., Fusobacterium, Peptostreptococcus, Bacteroides).
-
Risk factors for aspiration (predispose individuals to reduced epiglottic gag reflex and dysphagia)
- Altered consciousness: alcohol, sedation, general anesthesia, stroke
- Apoplexy and neurodegenerative conditions
- Gastroesophageal reflux disease, esophageal motility disorders
- Congenital defects (e.g., tracheoesophageal fistula)
- Use of a nasogastric feeding tube
Aspiration pneumonitis and pneumonia are unusual following aspiration of tube feeds or blood, which are typically high-pH and sterile. [37]
Clinical features [37][40]
-
Aspiration pneumonitis
- Immediate symptoms: bronchospasms , dyspnea, wheezing and/or crackles, hypoxemia
- Late symptoms: fever, shortness of breath, cough
-
Aspiration pneumonia
- Immediate symptoms: often none
- Late symptoms: fever, shortness of breath, cough with foul-smelling sputum
Diagnostics of pulmonary aspiration
Clinical diagnosis supported by characteristic laboratory and imaging findings
- Laboratory and microbiological studies: same as for the diagnosis of pneumonia.
- ABG: e.g., ↓ PaO2
-
Imaging: The lung region in which the infiltrates are seen depends on the patient's position on aspiration. [41][42]
- Supine position: superior segment of the right lower lobe and posterior segment of the right upper lobe (most common sites of aspiration)
- Standing/sitting: posterior basal segment of the right lower lobe
- Right lateral decubitus position: posterior segment of the right upper lobe and right middle lobe
- Left lateral decubitus: posterior segment of the left upper lobe and lingula
The initial CXR may be negative in early aspiration pneumonia. [37]


Treatment of pulmonary aspiration [37]
-
Acute aspiration: airway management and respiratory support
- Immediate oropharyngeal suctioning
- Intubation if there is ongoing risk of aspiration (e.g., post-extubation, ↓ LOC)
- O2 therapy and inhaled bronchodilators as needed
-
Aspiration pneumonitis: typically requires supportive care only
- Antibiotics are usually not required [18]
- Consider empiric antibiotics for patients with any of the following :
- Respiratory failure or suspected septic shock
- Acid suppression medications
- Small bowel obstruction
-
Aspiration pneumonia: antibiotic therapy following standard pneumonia treatment regimens
- Choose agents based on site of acquisition, illness severity, and risk factors for resistant organisms (see “Empiric antibiotics for CAP“ and “Empiric antibiotics for HAP”).
- Consider coverage for anaerobic bacteria (e.g., with ampicillin-sulbactam, moxifloxacin) in patients with severe periodontal disease, lung abscess, or empyema. [18][37][43]
- All patients: supportive care for pneumonia, monitoring, consider serial imaging.
Aspiration pneumonia requires antibiotic therapy while aspiration pneumonitis typically self-resolves within 24–48 hours with supportive care alone. [18][44]
Avoid routine anaerobic coverage for aspiration pneumonia without lung abscess, empyema, or severe periodontal disease. [43]
Complications
- Acute respiratory failure, acute respiratory distress syndrome (ARDS)
- Abscess
Prevention [37]
- Treatment of underlying causes to reduce the risk of aspiration
- NPO status prior to elective procedures with general anesthesia
- Formal swallowing evaluation when clinically appropriate
-
Aspiration precautions for patients with risk factors for aspiration
- Regular oral care
- Elevation of the head of the bed
- Dysphagia-modified diet
- One-on-one observation with meals
- Suctioning equipment at bedside
X-ray chest (PA view) of a patient with a history of aspiration pneumonia
Heterogeneous consolidation is present in the lower lobe of the right lung (green circle). There is also fullness overlying the inferior aspect of the right hilum, which is suspicious for lymphadenopathy (red circle).
In an erect patient, aspiration is likely to involve basal lung segments as well as the middle lobe and lingula. The upper lobe posterior segments and lower lobe superior segments are more likely to be involved in a recumbent patient.
Source: “Aspiration pneumonia201711-3264” by melvil, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
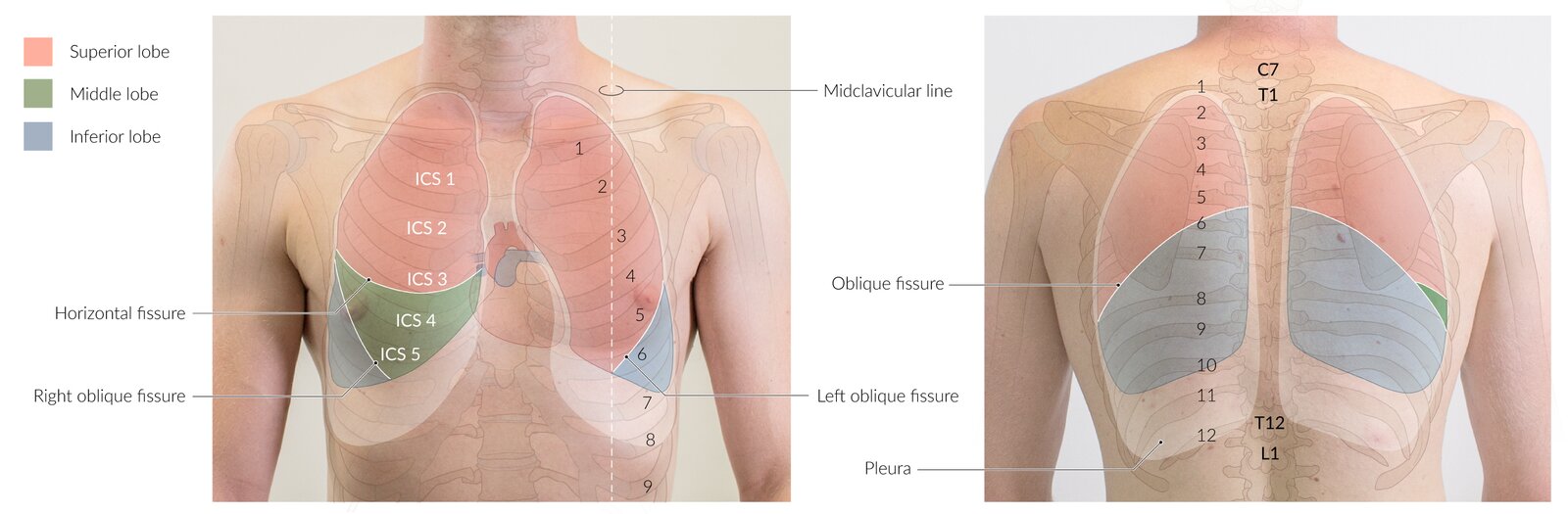
ICS: intercostal space
© AMBOSS
Community-acquired pneumonia in pregnancy
-
Overview
- CAP is responsible for approx. 5% of antepartum admissions for nonobstetric complications. [45]
- Physiological changes during pregnancy (e.g., decreased functional residual capacity) may increase the risk for a severe disease course.
- Diagnostics: Pregnancy should not rule out chest x-ray, if indicated.
-
Management
- Outpatient management: only in patients with mild disease and no comorbidities, if optimal follow-up is feasible
- Low threshold for hospital admission: The presence of comorbidities (e.g., asthma, immunologic disorders, renal disease) warrants inpatient management.
-
The approach to antibiotic therapy during pregnancy is the same as that for the general adult population, excluding potentially teratogenic medications, e.g.,:
- Clarithromycin
- Fluoroquinolones
- Tetracyclines
Complications
-
Parapneumonic pleuritis
- Fibrinous pleuritis: inflammation → increased vessel permeability → fibrin-rich exudate deposited on the serosal surface of the pleura → pleuritic chest pain and friction rub
- Analgesics can be used for the relief of symptoms.
- Parapneumonic pleural effusion (common)
- Pleural empyema
- Lung abscess
- ARDS
- Respiratory failure
- Sepsis
We list the most important complications. The selection is not exhaustive.
Prognosis
- Mortality increases with age.
- The mortality risk can be evaluated with the CURB-65 score. [46]
- Score 0: ∼ 1%
- Score 1–2: ∼ 10%
- Score 3: ∼ 14%
- Score 4: ∼ 40%
- HAP is associated with a mortality rate of > 20%.
Prevention
-
Immunization (see “ACIP immunization schedule” for information on doses and intervals)
- Pneumococcal vaccination
- Influenza vaccination
- COVID-19 vaccination
- Smoking cessation
- Prevention of ventilator-associated infections
Related One-Minute Telegram
- One-Minute Telegram 108-2024-3/3: Confronting diagnostic discordance in pneumonia
- One-Minute Telegram 87-2023-2/3: Breathe easier: a breakthrough in preventing ventilator-associated pneumonia
- One-Minute Telegram 72-2023-1/3: An infusion of hope for pneumonia survival
- One-Minute Telegram 36-2021-1/3: Can probiotics prevent pneumonia in mechanically ventilated patients?
- One-Minute Telegram 36-2021-2/3: Can point-of-care testing safely reduce the use of antibiotics?
- One-Minute Telegram 14-2020-2/3: Admit patient to home: virtual hospitals for patients with COVID-19
- One-Minute Telegram 13-2020-1/3: Robots vs. residents: who can interpret chest x-rays better?
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- One-Minute Telegram
- 2023 IDSA Community-Acquired Pneumonia (CAP) Clinical Pathway Overview Presentation
- 2023 ERS/ESICM/ESCMID/ALAT Guidelines for the Management of Severe Community-Acquired Pneumonia
- 2019 IDSA/ATS Clinical Practice Guideline: Diagnosis and Treatment of Adults with Community-acquired Pneumonia
- 2016 IDSA/ATS Clinical Practice Guideline: Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia
References
- Olubamwo OO, Onyeka IN, Aregbesola A, et al. "Determinants of hospitalizations for pneumonia among Finnish drug users". SAGE Open Medicine. 6. :205031211878431. (2018)
- Mishra K, Bhardwaj P, Mishra A, Kaushik A. "Acute Chlamydia trachomatis respiratory infection in Infants". Journal of Global Infectious Diseases. 3(3). :216. (2011)
- Hammerschlag MR. "Chlamydia trachomatis and Chlamydia pneumoniae Infections in Children and Adolescents". Pediatrics in Review. 25(2). :43-51. (2004)
- "Chlamydia pneumoniae Infection". https://web.archive.org/web/20210210052018/https://www.cdc.gov/pneumonia/atypical/cpneumoniae/about/causes.html. [2019-01-10]
- Simonetti AF, Viasus D, Garcia-Vidal C, Carratalà J. "Management of community-acquired pneumonia in older adults". Therapeutic Advances in Infectious Disease. 2(1). :3-16. (2014)
- Stupka JE, Mortensen EM, Anzueto A, Restrepo MI. "Community-acquired pneumonia in elderly patients". Aging Health. 5(6). :763-774. (2009)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Cordier J-F. "Cryptogenic organising pneumonia". European Respiratory Journal. 28(2). :422-446. (2006)
- Abers MS, Sandvall BP, Sampath R et al. "Postobstructive Pneumonia: An Underdescribed Syndrome". Clin Infect Dis. 62(8). :957-961. (2016)
- Kalil AC, Metersky ML, Klompas M, et al. "Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society". Clin Infect Dis. 63(5). :e61-e111. (2016)
- Löffler B, Niemann S, Ehrhardt C et al. "Pathogenesis of Staphylococcus aureus Necrotizing Pneumonia". Expert Rev Anti Infect Ther. 11(10). :1041-1051. (2014)
- "CAP clinical pathway". https://www.idsociety.org/globalassets/idsa/practice-guidelines/community-acquired-pneumonia-in-adults/cap-clinical-pathway-overview.pdf. [2023-10-31]
- Vaughn VM, Dickson RP, Horowitz JK, et al. "Community-Acquired Pneumonia: A Review". JAMA. (2024)
- Ebell MH, Chupp H, Cai X, Bentivegna M, Kearney M. "Accuracy of Signs and Symptoms for the Diagnosis of Community‐acquired Pneumonia: A Meta‐analysis". Acad Emerg Med.. 27(7). :541-553. (2020)
- Marchello CS, Ebell MH, Dale AP, et al. "Signs and Symptoms That Rule out Community-Acquired Pneumonia in Outpatient Adults: A Systematic Review and Meta-Analysis". J Am Board Fam Med.. 32(2). :234-247. (2019)
- Jones BE, Ramirez JA, Oren E, et al. "Diagnosis and Management of Community-acquired Pneumonia. An Official American Thoracic Society Clinical Practice Guideline". Am J Respir Crit Care Med. (2025)
- Loubet P, Tubiana S, Claessens YE, et al. "Community-acquired pneumonia in the emergency department: an algorithm to facilitate diagnosis and guide chest CT scan indication". Clin Microbiol Infect.. 26(3). :382.e1-382.e7. (2020)
- Metlay JP, Waterer GW, Long AC, et al. "Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America". Am J Respir Crit Care Med. 200(7). :e45-e67. (2019)
- Rhee C. "Using Procalcitonin to Guide Antibiotic Therapy". Open Forum Infectious Diseases. :ofw249. (2016)
- Martin-Loeches I, Torres A, Nagavci B, et al. "ERS/ESICM/ESCMID/ALAT guidelines for the management of severe community-acquired pneumonia". Eur Respir J. 61(4). :2200735. (2023)
- Lim WS, Baudouin SV, George RC, et al. "BTS guidelines for the management of community acquired pneumonia in adults: update 2009". Thorax. 64(Suppl 3). :iii1-iii55. (2009)
- Smith MD, Fee C, Mace SE, et al. "Clinical Policy: Critical Issues in the Management of Adult Patients Presenting to the Emergency Department With Community-Acquired Pneumonia". Ann Emerg Med. 77(1). :e1-e57. (2021)
- Nambu A. "Imaging of community-acquired pneumonia: Roles of imaging examinations, imaging diagnosis of specific pathogens and discrimination from noninfectious diseases". World Journal of Radiology. 6(10). :779. (2014)
- Llamas-Álvarez AM, Tenza-Lozano EM, Latour-Pérez J. "Accuracy of Lung Ultrasonography in the Diagnosis of Pneumonia in Adults". Chest. 151(2). :374-382. (2017)
- Orso D, Guglielmo N, Copetti R. "Lung ultrasound in diagnosing pneumonia in the emergency department". Eur J Emerg Med.. 25(5). :312-321. (2018)
- Qaseem A, Etxeandia-Ikobaltzeta I, Mustafa RA, et al. "Appropriate Use of Point-of-Care Ultrasonography in Patients With Acute Dyspnea in Emergency Department or Inpatient Settings: A Clinical Guideline From the American College of Physicians". Ann Intern Med. 174(7). :985-993. (2021)
- Volpicelli G, Elbarbary M, et al. "International evidence-based recommendations for point-of-care lung ultrasound". Intensive Care Med. 38(4). :577-591. (2012)
- Blaivas M. "Lung Ultrasound in Evaluation of Pneumonia". J Ultrasound Med.. 31(6). :823-826. (2012)
- "Choosing Wisely Recommendations: Avoid the use of combination topical steroid antifungals for tinea corporis, Candida skin infections, and diaper dermatitis". https://web.archive.org/web/20250609213858/https://www.aafp.org/pubs/afp/collections/choosing-wisely/471.html
- Dequin PF, Meziani F, Quenot JP, et al. "Hydrocortisone in Severe Community-Acquired Pneumonia". N Engl J Med. (2023)
- Phua J, Dean NC, Guo Q, et al. "Severe community-acquired pneumonia: timely management measures in the first 24 hours". Crit Care. 20(1). (2016)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Siempos II, Vardakas KZ, Kopterides P, Falagas ME. "Adjunctive therapies for community-acquired pneumonia: a systematic review". J Antimicrob Chemother. 62(4). :661-668. (2008)
- File TM Jr. "Treatment of Hospital-acquired and Ventilator-associated Pneumonia in Adults". UpToDate. UpToDate. https://www.uptodate.com/contents/treatment-of-hospital-acquired-and-ventilator-associated-pneumonia-in-adults. [2017-06-26]
- Mandell LA, Niederman MS. "Aspiration Pneumonia". N Engl J Med. 380(7). :651-663. (2019)
- Košutová P, Mikolka P. "Aspiration syndromes and associated lung injury: incidence, pathophysiology and management". Physiological Research. :S567-S583. (2021)
- DeLegge MH. "Aspiration Pneumonia: Incidence, Mortality, and At‐Risk Populations". Journal of Parenteral and Enteral Nutrition. 26(6S). (2002)
- Neill S, Dean N. "Aspiration pneumonia and pneumonitis". Curr Opin Infect Dis. 32(2). :152-157. (2019)
- Son YG, Shin J, Ryu HG. "Pneumonitis and pneumonia after aspiration.". Journal of dental anesthesia and pain medicine. 17(1). :1-12. (2017)
- Sun JC, V. Joffe H. "The Most Common Inpatient Problems in Internal Medicine". Saunders. (2007). ISBN: 9781416032038
- Vedamurthy A, Rajendran I, Manian F. "Things We Do for No Reason™: Routine Coverage of Anaerobes in Aspiration Pneumonia". J Hosp Med. 15(12). :754-756. (2020)
- Dragan V, Wei Y, Elligsen M, et al. "Prophylactic Antimicrobial Therapy for Acute Aspiration Pneumonitis". Clin Infect Dis. 67(4). :513-518. (2018)
- "Mycoplasma pneumoniae Infections". https://web.archive.org/web/20211205055914/https://www.cdc.gov/pneumonia/atypical/mycoplasma/about/. [2020-06-05]
- Sheffield JS, Cunningham FG. "Community-Acquired Pneumonia in Pregnancy". Obstet Gynecol.. 114(4). :915-922. (2009)
- Fine MJ, Auble TE, Yealy DM, et al. "A Prediction Rule to Identify Low-Risk Patients with Community-Acquired Pneumonia". N Engl J Med. 336(4). :243-250. (1997)
- Lim WS. "Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study". Thorax. 58(5). :377-382. (2003)