Summary
Portal hypertension is the pathological elevation of portal venous pressure resulting from obstructions in portal blood flow, which can be prehepatic (e.g., portal vein thrombosis), hepatic (e.g., liver cirrhosis), or posthepatic (e.g., right-sided heart failure). The subsequent backflow of blood may lead to portosystemic anastomoses, splenomegaly, and/or ascites. A diagnosis of portal hypertension can be made based on clinical signs and knowledge of an underlying cause. In suspected cases, medical imaging and laboratory tests are used to support the diagnosis. Management involves treating the underlying condition and reducing portal pressure with nonselective beta blockers (NSBBs) and portosystemic shunts. Acute hemorrhage of esophageal varices is a potentially life-threatening complication of portal hypertension and is caused by increased blood flow via portosystemic anastomoses.
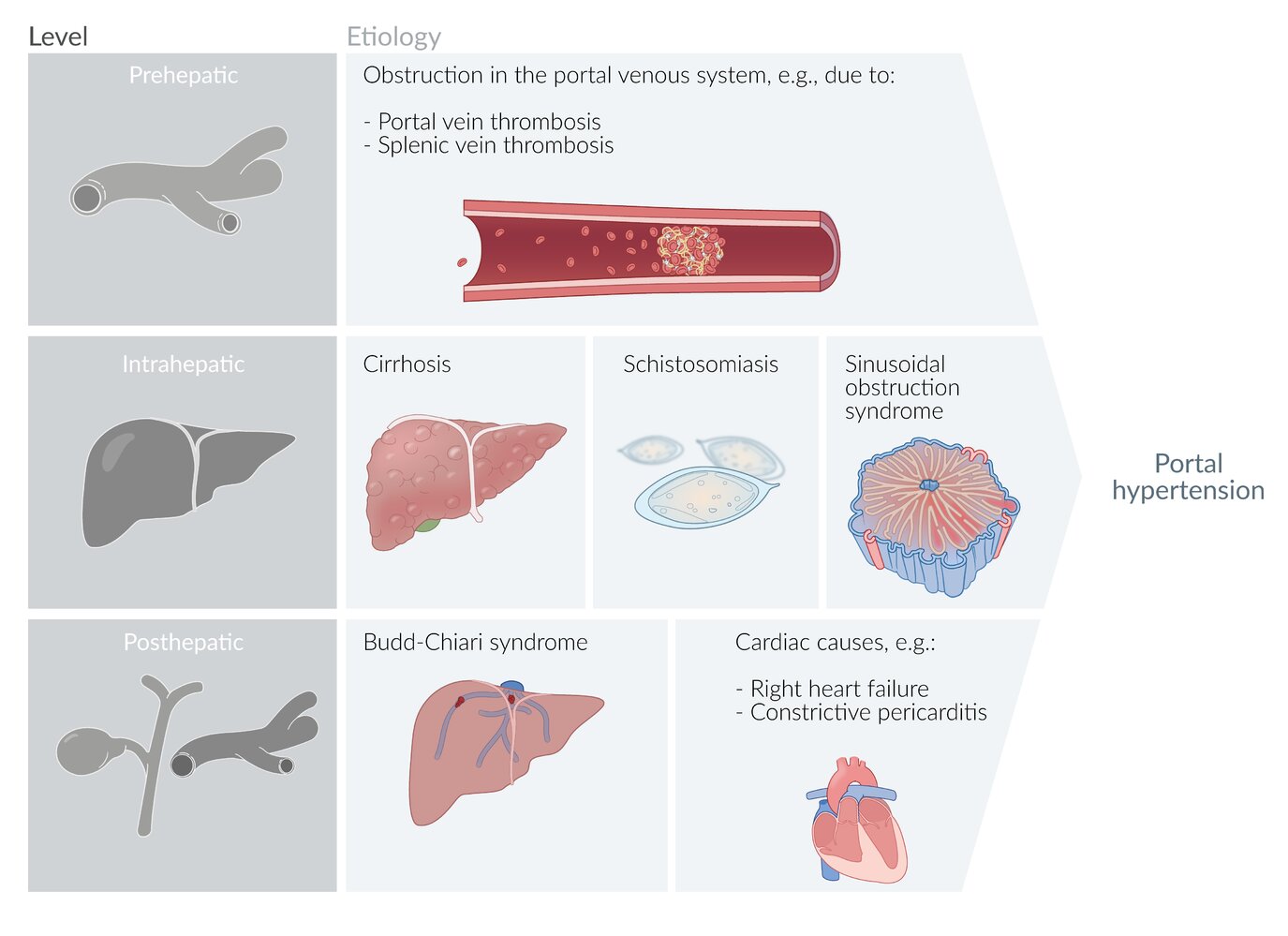
Etiology
Causes of portal hypertension are described based on the anatomical location of the lesion.

Prehepatic [1]
- Portal vein thrombosis
- Splenic vein thrombosis
- Mesenteric vein thrombosis [2]
- Congenital abnormalities of the portal vein system (e.g., portal vein agenesis)
- Compression of portal or splenic veins [3]
- Arteriovenous fistula
Hepatic [1][4]
Hepatic etiologies of portal hypertension are described anatomically in relation to the hepatic sinusoids.
-
Presinusoidal
- Hepatosplenic schistosomiasis (most common cause of noncirrhotic portal hypertension worldwide) [5]
- Granulomatous diseases (e.g., sarcoidosis, tuberculosis) [3]
- Malignancy (e.g., lymphoma) causing portal vein occlusion
- Biliary diseases (e.g., primary biliary cholangitis, primary sclerosing cholangitis)
- Developmental or genetic abnormalities (e.g., polycystic kidney disease, arteriovenous fistula)
-
Sinusoidal
- Cirrhosis (most common cause of portal hypertension in the US)
- Massive hepatic metastases
- Steatohepatitis
- Congenital hepatic fibrosis
- Amyloidosis
- Drug-induced liver injury (e.g., methotrexate-induced) or toxin-related liver injury (e.g., copper)
- Alcohol-associated liver disease
- Infiltrative diseases (e.g., Gaucher disease)
- Inflammatory and infectious conditions (e.g., viral hepatitis, chronic Q fever)
- Portosinusoidal vascular disorder
-
Postsinusoidal
- Sinusoidal obstruction syndrome
- Vascular malignancy (e.g., angiosarcoma)
- Granulomatous changes (due to, e.g., sarcoidosis or Mycobacterium avium)
- Sclerosis of the hepatic vein (due to, e.g., alcohol or hypervitaminosis A)
Posthepatic [1][3]
- Budd-Chiari syndrome
- Right-sided heart failure [6]
- Constrictive pericarditis
- Obstruction of IVC (e.g., IVC thrombosis)
© AMBOSS
Pathophysiology
Prehepatic [1][7]
Obstruction of portal vein or splenic vein → ↑ hydrostatic pressure in the tributaries of the obstructed vein
Hepatic [1][7]
- Presinusoidal: obstruction of outflow in portal vein at the porta hepatis or in the portal venules within liver → ↑ hydrostatic pressure in the portal vein and its tributaries
- Sinusoidal: ↑ resistance to blood flow in the hepatic sinusoids (e.g., due to hepatic fibrosis and ↓ intrahepatic nitric oxide production in cirrhosis) → ↑ hydrostatic pressure in the hepatic sinusoids → ↑ hydrostatic pressure in the portal vein and its tributaries
- Postsinusoidal: obstruction of outflow in the central vein and/or hepatic venules → ↑ hydrostatic pressure in the hepatic sinusoids → ↑ hydrostatic pressure in the portal vein and its tributaries
Posthepatic [1][7]
Hepatic vein congestion or obstruction of hepatic vein outflow → ↑ hydrostatic pressure in the hepatic sinusoids → ↑ hydrostatic pressure in the portal vein and its tributaries
Clinical features
The etiology determines whether portal hypertension manifests as acute or chronic.
-
Signs and symptoms of underlying disease, e.g.:
- Clinical features of cirrhosis
- Clinical features of right-sided heart failure
-
Signs and symptoms of complications: features of increased blood flow via portosystemic anastomoses
-
Gastrointestinal bleeding [9]
- Hematemesis and/or melena (e.g., due to esophageal varices or gastric varices)
- Hematochezia (e.g., due to hemorrhoidal or anorectal varices)
- Caput medusae
- Signs of hypersplenism due to congestive splenomegaly (e.g., thrombocytopenia)
- Abdominal distention due to ascites
- Hepatic encephalopathy
-
Gastrointestinal bleeding [9]
Patients usually present with signs of their underlying disease and/or symptoms related to the complications of portal hypertension.



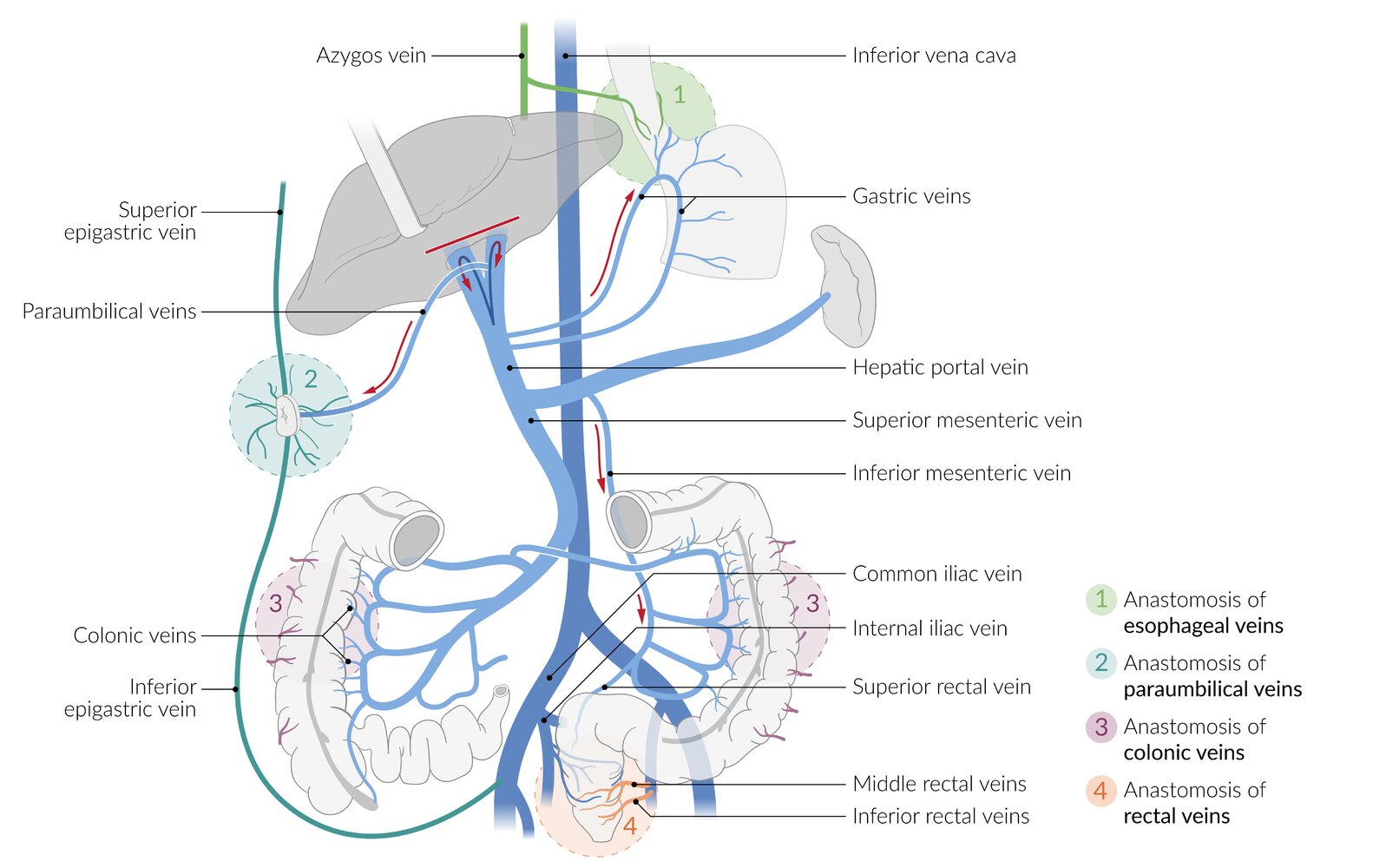
Portocaval anastomoses are anastomoses between veins of the portal venous system (veins that drain directly/indirectly into the portal vein) and veins of the caval venous system (veins that drain directly/indirectly into the superior or inferior vena cava). Physiologically, there is minimal/no blood flow through these anastomoses. In portal hypertension, increased portal venous pressure causes shunting of blood from the portal system into the caval system, which increases the pressure within the caval veins, causing variceal dilation of the caval veins at the sites of portocaval anastomoses.
(1) Distal esophagus: anastomosis between the left gastric vein (portal system) and the azygous vein (caval system), which manifests as esophageal varices in portal hypertension
(2) Paraumbilical region: anastomosis between the paraumbilical veins (portal system) and the superior and inferior epigastric veins (caval system), which manifests as caput medusae in portal hypertension
(3) Colon: anastomosis between the colonic veins (portal system) and the retroperitoneal veins (caval system), which manifests as colonic varices in portal hypertension
(4) Rectum and anal canal: anastomosis between the superior rectal vein (portal system) and the middle and inferior rectal veins (caval system), which manifests as anorectal varices in portal hypertension
© AMBOSS
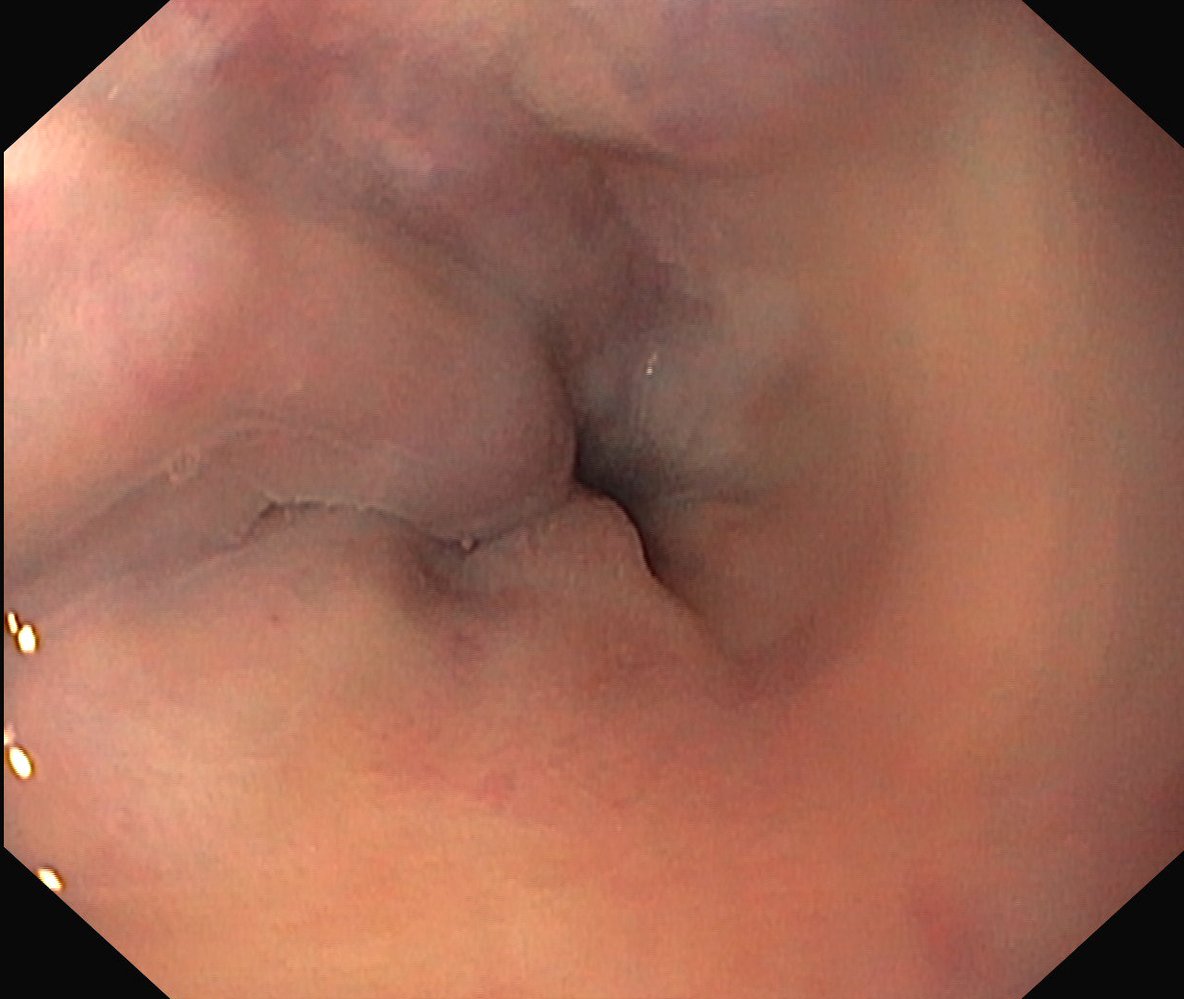
Endoscopic view of the distal esophagus
The esophageal lumen is narrowed by dilated submucosal veins (green overlay). Despite endoscopic insufflation, the varices still surpass the mucosal level by more than 5 mm but show no sign of recent or impending bleeding.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
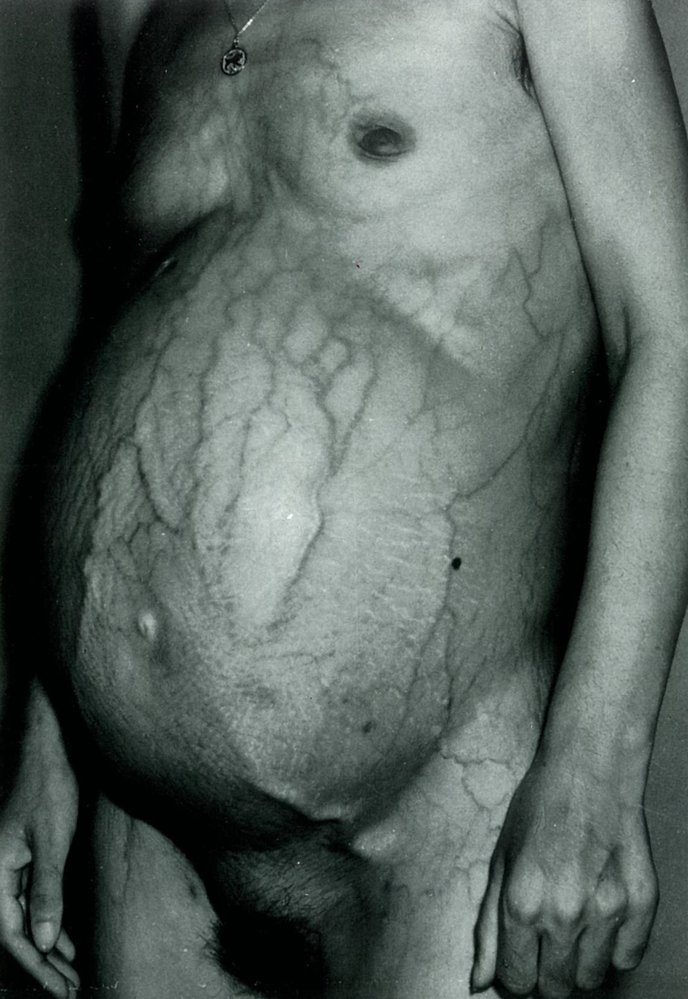
There is distention of the abdomen (ascites) and periumbilical dilatation of subcutaneous veins (caput medusae).
These findings are characteristics of decompensated liver disease.
Source: © IMPP
Diagnosis
General principles [10][11]
-
CSPH is confirmed in patients with either: [10]
- HVPG measurement ≥ 10 mm Hg
-
Surrogate markers of CSPH:
- Complications of portal hypertension: e.g., esophageal varices on EGD, portosystemic collaterals on abdominal imaging
- Abnormal noninvasive tests: transient elastography with PLT count [12]
- Once confirmed, identify the underlying causes of portal hypertension.
- Obtain a diagnostic workup for the most likely cause (e.g., diagnostics for cirrhosis).
- Consult hepatology if the diagnosis remains unclear.
The combination of elevated liver stiffness and thrombocytopenia provides the most reliable estimation of CSPH using noninvasive tests. [10]
Laboratory studies [6][10]
Findings are nonspecific but may further support the diagnosis and help to identify the underlying cause.
-
CBC
- Thrombocytopenia (most common laboratory finding in portal hypertension)
- Anemia related to an underlying condition
- Liver chemistries: transaminitis and/or hyperbilirubinemia suggest liver disease.
- Coagulation panel: coagulopathy is a sign of advanced liver disease
- Ascitic fluid analysis: high SAAG ≥ 1.1 g/dL [6]
Imaging studies [10][13]
Transient elastography [10][12]
- Indications: Obtain for all patients with nonconfirmed disease.
-
Findings: Correlate with PLT levels to increase diagnostic yield.
-
CSPH is confirmed with the following findings : [10]
- Liver stiffness > 25 kPa (regardless of PLT level)
- Liver stiffness 20–25 kPa (if PLT < 150,000/mm3)
- Liver stiffness 15–20 kPa (if PLT ≤ 110,000/mm3)
- CSPH is ruled out if liver stiffness < 15 kPa and platelets ≥ 150,000/mm3. [10]
-
CSPH is confirmed with the following findings : [10]
Transient elastography is the recommended noninvasive test for diagnostic confirmation in patients with suspected portal hypertension. [10]
Abdominal imaging [10]
Findings may help establish the diagnosis and identify the underlying cause.
-
Modalities
-
MR elastography
- For diagnostic uncertainty after transient elastography [12]
- Liver stiffness ≥ 5.1 kPa on MR elastography suggests CSPH. [12]
- Doppler ultrasound abdomen: Obtain to assess portal circulation.
- CT or MRI abdomen are usually reserved for:
- Concerns for extrahepatic obstruction
- Preprocedural planning
-
MR elastography
-
Specific findings of CSPH: sufficient to establish a diagnosis of portal hypertension [10][14]
- Portosystemic collateral circulation
- Blood flow reversal in the portal system
-
Nonspecific findings
- Portal and/or splenic vein dilation > 10 mm
- Decreased portal vein velocity on Doppler ultrasound
- Splenomegaly, ascites, and/or varices
- Findings that suggest the underlying cause, e.g.:
- Cirrhosis (e.g., nodular liver)
- Liver masses
- Portal vein thrombosis





Hepatic venous pressure gradient (HVPG) measurement [10][11][15]
- Indication: reserved for diagnostic confirmation in cases of uncertainty (gold standard test) [10]
- Method: Free and wedge occlusion pressures of the hepatic vein are measured via catheterization, using ultrasound or fluoroscopy. [11]
-
Interpretation of HVPG levels [10]
- > 5 mm Hg: mild portal hypertension
- ≥ 10 mm Hg: clinically significant portal hypertension (CSPH) [6]
- > 12 mm Hg: associated with complications (e.g., variceal bleeding) [6]
Esophagogastroduodenoscopy (EGD) [10][11]
-
Indications (all of the following)
- Diagnosis of cirrhosis or compensated advanced chronic liver disease
- Non-invasive methods to diagnose CSPH (e.g., transient elastography) are unavailable
- Interpretation: The presence of esophageal varices of any size confirms the diagnosis of CSPH. [10]


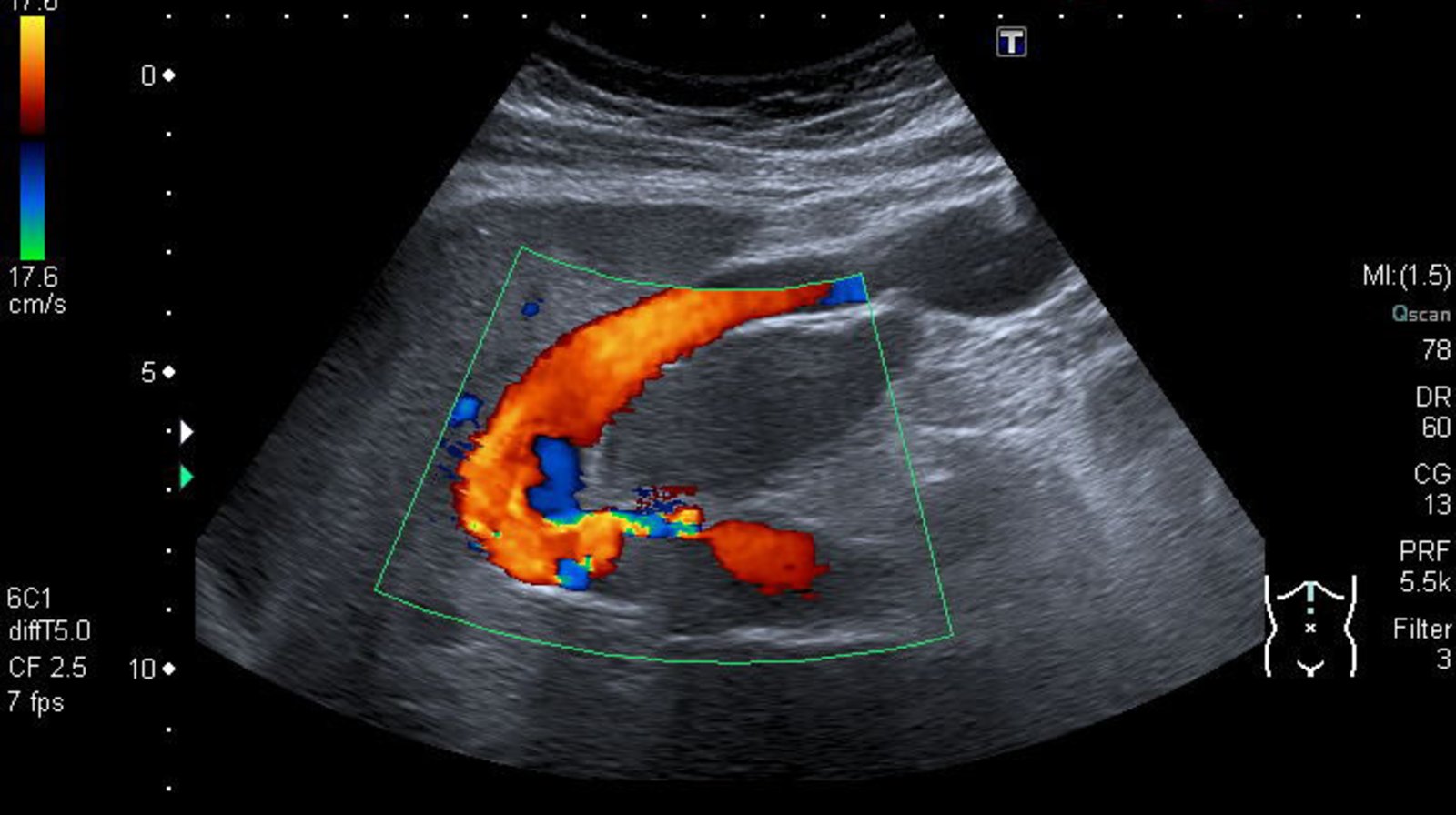
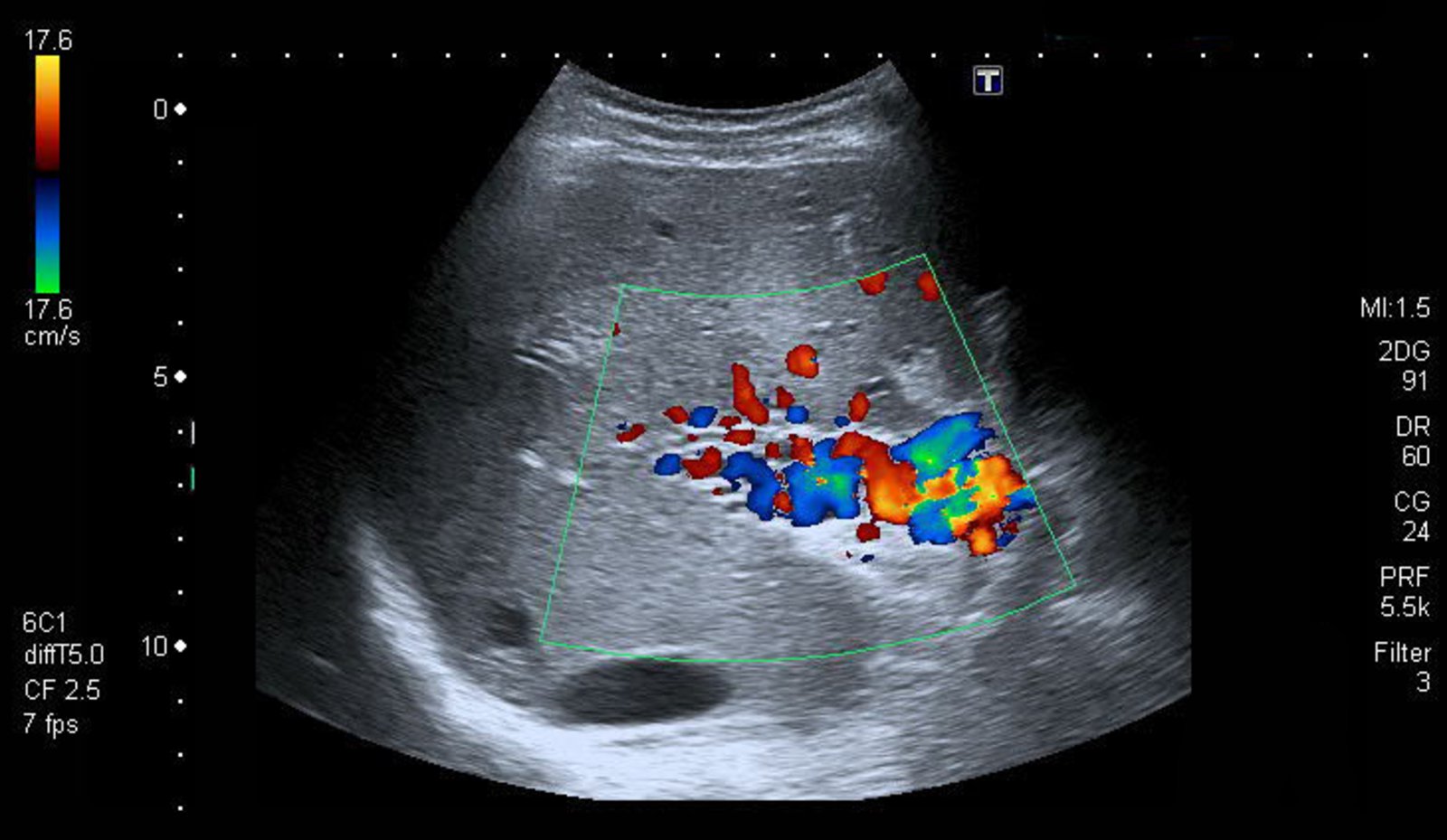
Ultrasound liver (color Doppler; longitudinal plane) of a patient with hepatic cirrhosis
The umbilical vein is dilated. The direction of blood flow (arrow) is primarily toward the transducer (red), from the liver (L) to the umbilicus.
The findings are consistent with recanalization of a paraumbilical vein, which occurs secondary to portal hypertension.
Arrow: flow direction
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
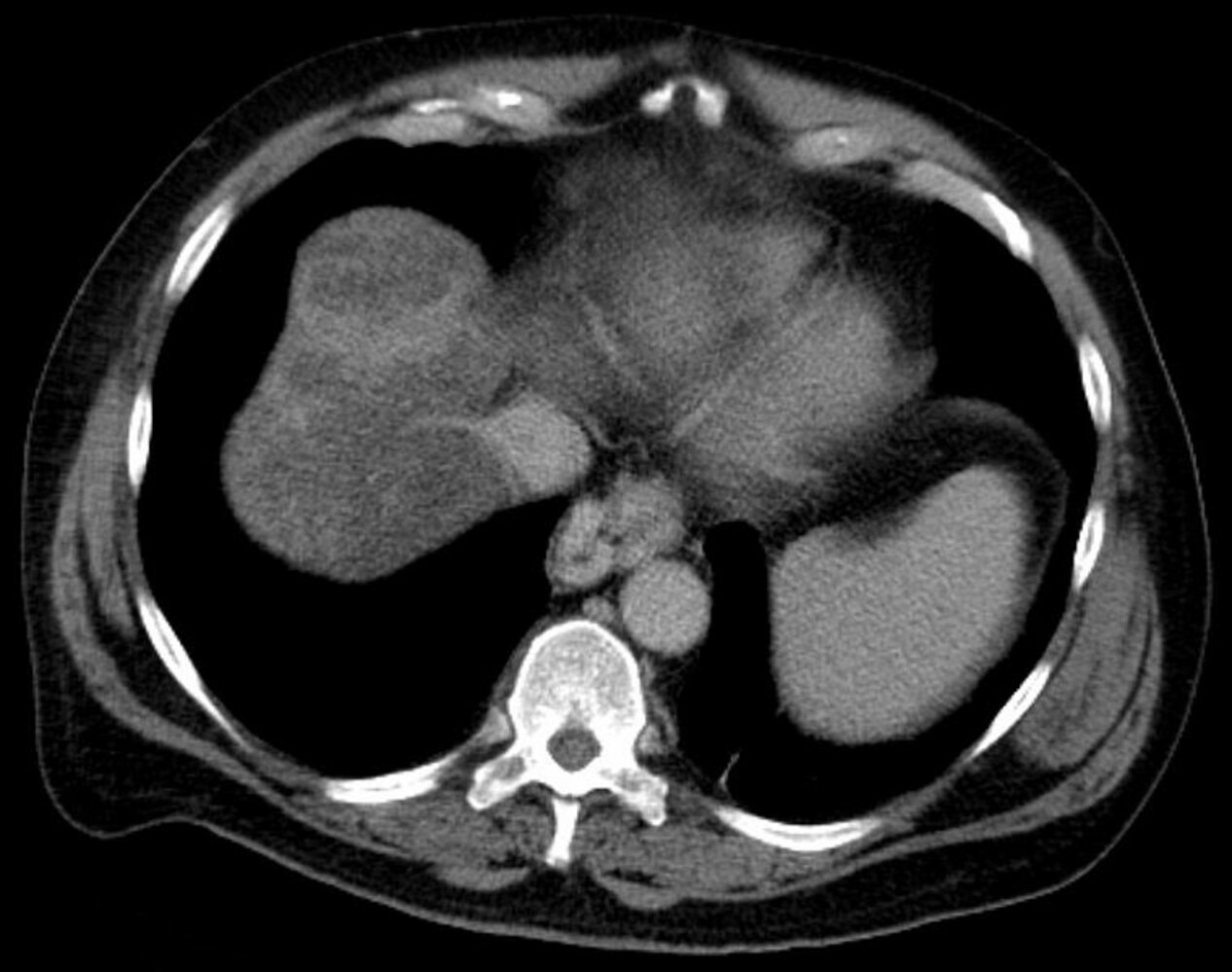
CT chest (oral and IV contrast-enhanced; axial section)
A bulbous, contrast-enhancing mass, not clearly separated from the esophageal wall, can be seen (green overlay). There is also a heterogeneous perfusion pattern (red overlay) seen in the liver, likely due to cirrhosis.
These findings are characteristic of portal hypertension with esophageal varices.
A: aorta; V: inferior vena cava
Source: “Oesophagusvarizen 01” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
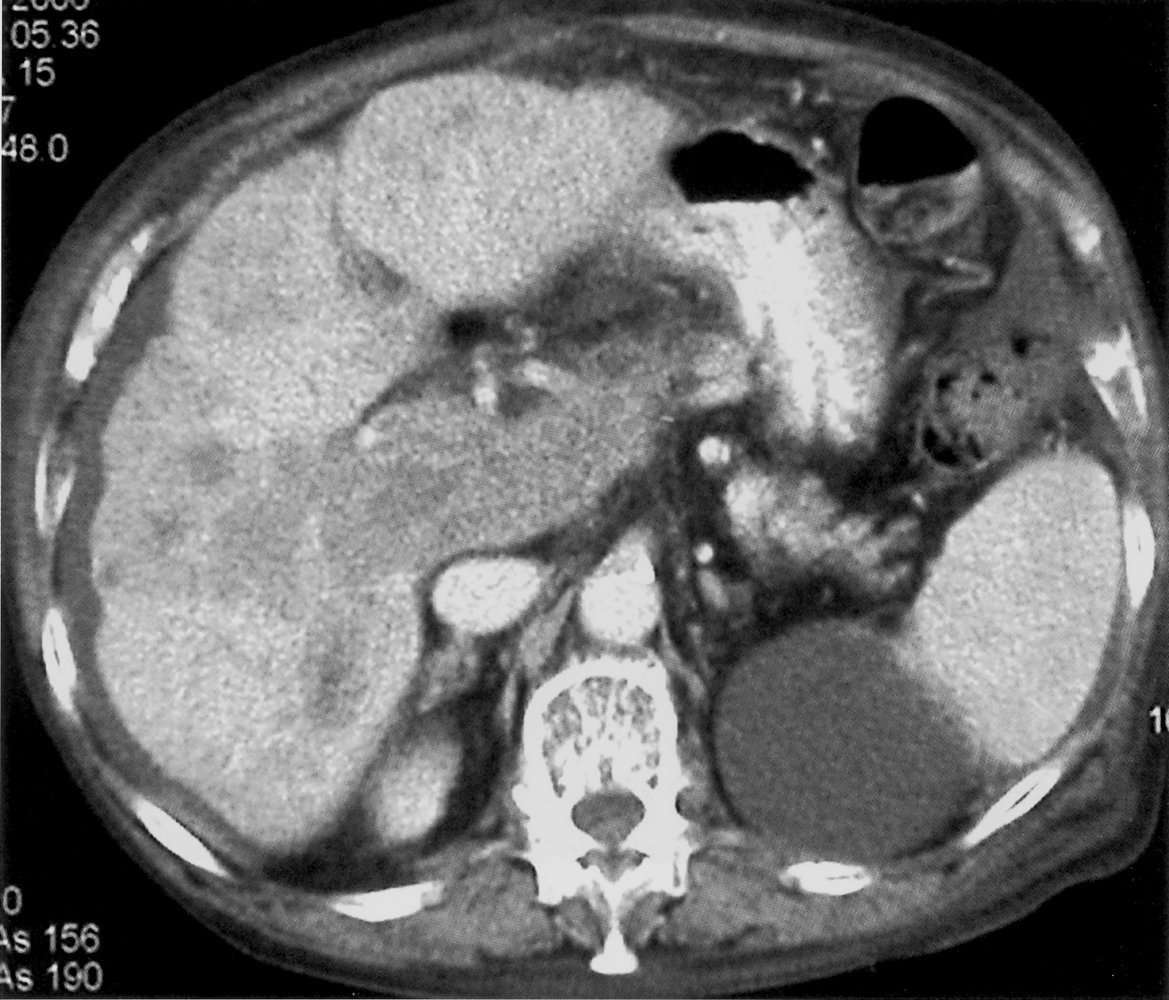
CT abdomen (axial plane) of a patient with hepatic cirrhosis
The liver (L) shows heterogeneous enhancement and a lobulated margin. The spleen is borderline prominent. Multiple serpiginous enhancing blood vessels medial to the stomach are varices (V) that have developed as a result of portal hypertension.
Ao: aorta; IVC: inferior vena cava; Sp: spleen; St: stomach
Source: “Fundusvarizen” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
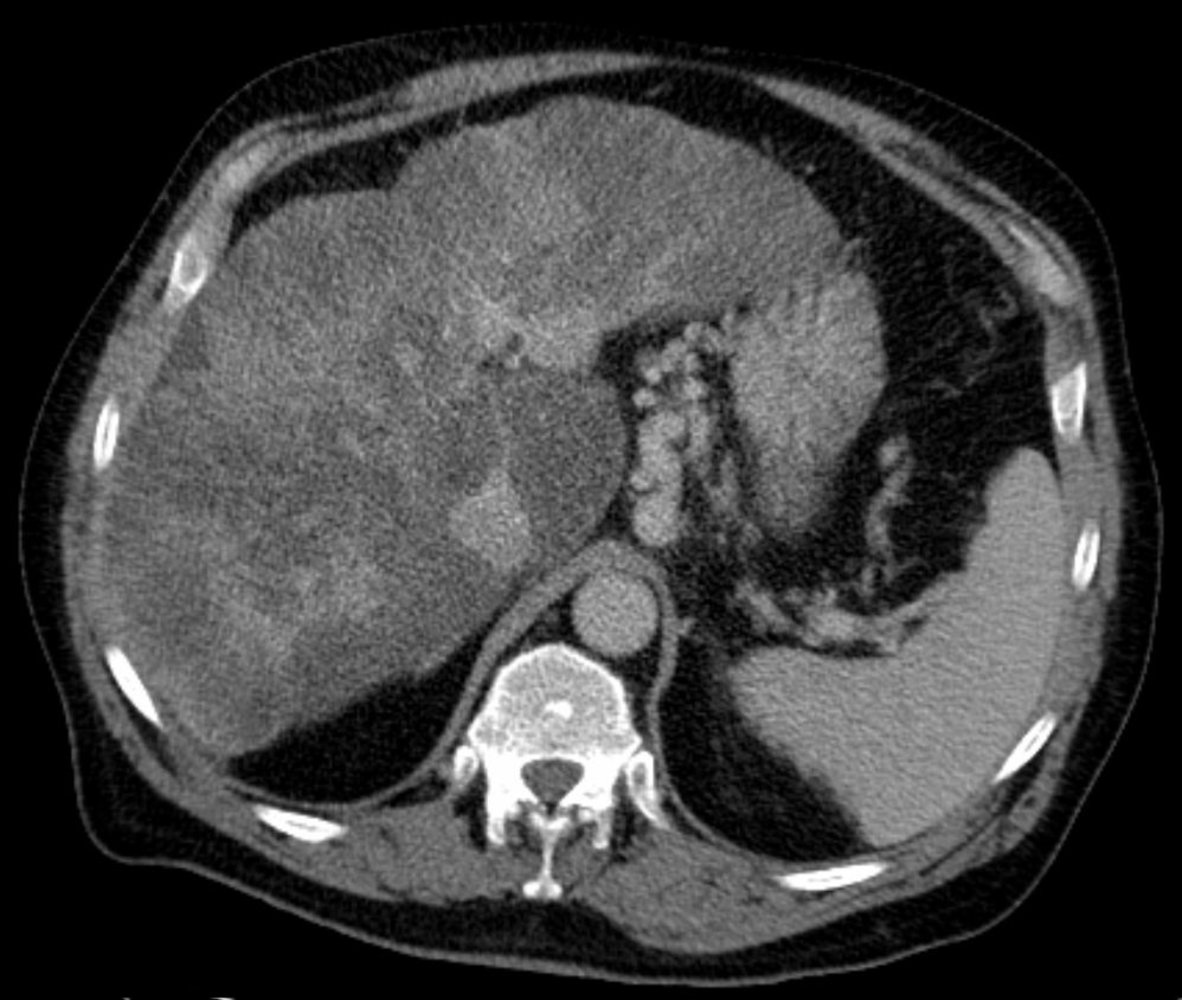
CT abdomen (with contrast, venous phase; axial plane) of a patient with cirrhosis
Multiple ill-defined hypoattenuating lesions (examples indicated by green overlay) are seen throughout the irregular cirrhotic liver. The portal vein (blue overlay) is enlarged and contains an enhancing tumor thrombus. A small amount of ascites (red overlay) is visible.
Several patterns of enhancement can be seen with hepatocellular carcinoma (HCC). HCC commonly shows vivid enhancement during the late arterial phase (~35 seconds). Rapid washout in the portal venous phase follows, with the lesions becoming iso- or hypodense compared to background liver parenchyma.
AA: abdominal aorta; C: renal cyst; IVC: inferior vena cava; S: spleen
Source: © IMPP
Ultrasound portal vein (color Doppler)
Numerous small collateral veins (red: flow toward transducer; blue: flow away from transducer) are seen in the portal vein bed. A normal main portal vein was not identified.
Cavernous transformation of the portal vein is a sequela of portal vein obstruction from thrombosis or tumor, resulting in portal hypertension and the development of venous collaterals. Collateral formation occurs over days to months.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
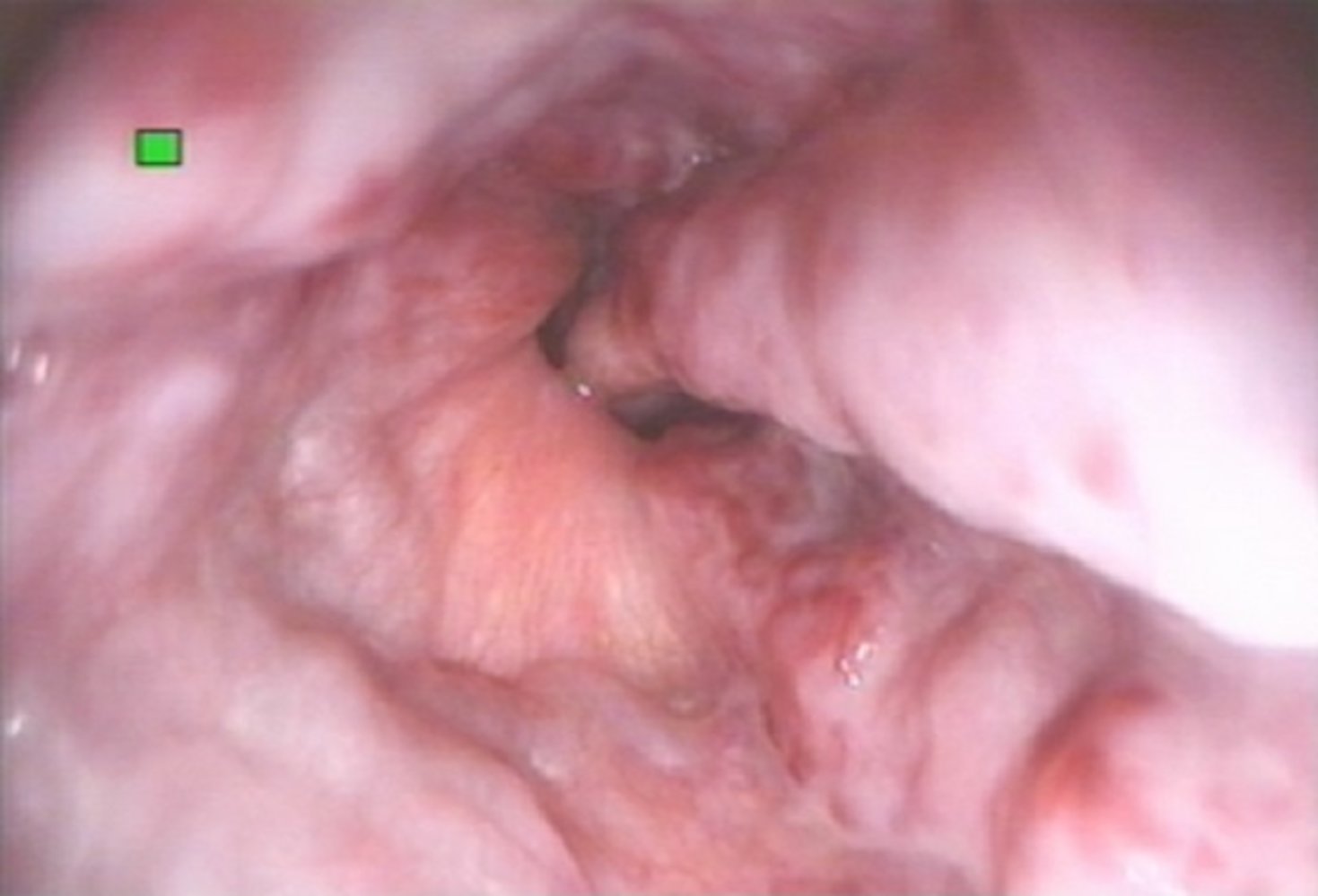
Endoscopic view of the distal esophagus
The esophageal lumen is narrowed by dilated submucosal veins (green overlay). Despite endoscopic insufflation, the varices still surpass the mucosal level by more than 5 mm but show no sign of recent or impending bleeding.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
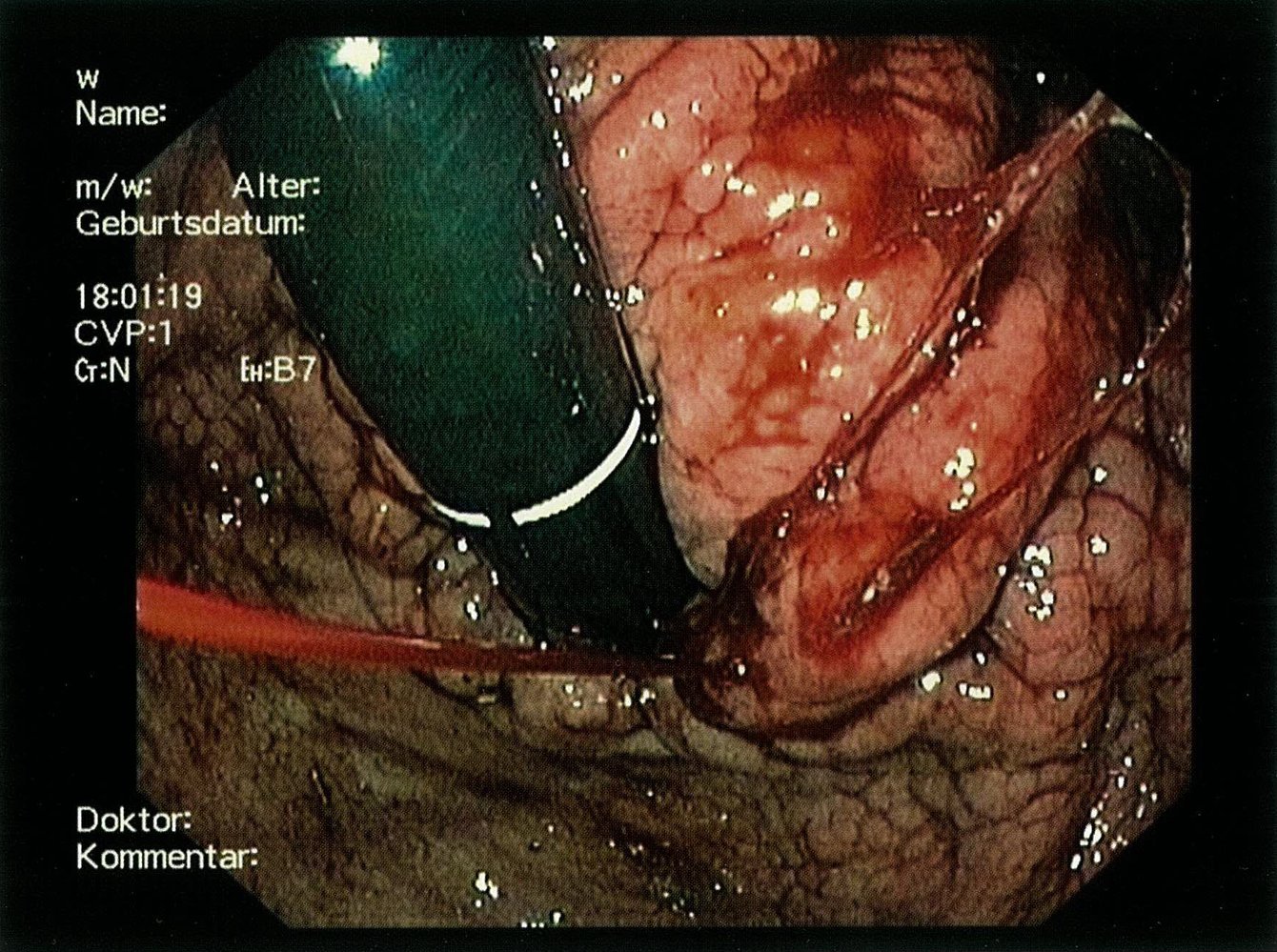
Endoscopic view of the distal esophagus
Dilated, submucosal veins are visible, most prominently at the 2, 4, 7, and 11 o'clock positions. Several cherry-red spots are visible on the varices, suggesting a recent or impending variceal bleed.
Source: “Figure 2 (b) in: Etiology and Management of Hemorrhagic Complications of Portal Hypertension in Children” by Alejandro Costaguta, Fernando Alvarez, International Journal of Hepathology, licensed under CC BY 3.0.
Endoscopic view of the stomach (retroflexion) in a patient with liver cirrhosis
The varix appears as a prominent mucosal fold (blue overlay). At the cardiac end of the varix a spurting hemorrhage is visible (arrow). The surrounding mucosa is partially covered by liquid and clotted blood.
Source: © IMPP
Treatment
General principles [10][11][13]
Consult hepatology for specialist-guided management that includes:
- Management of the underlying causes of portal hypertension (mainstay of treatment)
- Pharmacotherapy with NSBBs
- Portosystemic shunts for refractory disease
- Management of complications of portal hypertension, e.g., treatment of ascites, treatment of hepatic encephalopathy, treatment of esophageal varices
Pharmacotherapy (off-label) [10][11]
-
NSBBs: used to prevent hepatic decompensation (e.g., variceal bleeding)
- Indicated in patients with CSPH and cirrhosis (unless there are contraindications for beta blockers) [10]
- Preferred agent: carvedilol [10][11]
- Alternative agents: propranolol, nadolol
- Reduce dose or discontinue in patients with complications of advanced liver disease.
Transjugular intrahepatic portosystemic shunt (TIPS or TIPSS) [16][17]
- Definition: implantation of a stent between the hepatic vein and portal vein
-
Goals
- Ensure blood drainage from the portal to the systemic system bypasses the liver, thus lowering portal pressure
- Reduce the risk of variceal bleeding and reduce the formation of ascites
-
Indications
- Persistent, recurring, or treatment-resistant upper gastrointestinal bleeding resulting from portal hypertension, e.g., from esophageal varices
- Other complications of portal hypertension refractory to medical therapy, e.g.: [16]
- Ascites
- Hepatic hydrothorax
- Budd-Chiari syndrome
- Chronic complete portal vein thrombosis
-
Contraindications [16][17]
- Refractory overt hepatic encephalopathy
- Severe circulatory diseases, i.e.:
- Heart failure
- Severe pulmonary hypertension (mPAP > 45 mm Hg)
- Severe untreated valvular heart disease, e.g., tricuspid regurgitation
- Ongoing infection or sepsis
- Severe, uncorrectable coagulopathy (relative contraindication) [17]
- Anatomical barriers (relative contraindication) [17]
-
Procedure [10][18]
- Access site: internal jugular vein
- The hepatic vein is catheterized and an expandable stent is placed between the hepatic and portal veins.
-
Complications [17][19]
- Procedure-related, e.g., inadvertent carotid artery puncture, stent migration, stent occlusion
- Portosystemic shunt-related, e.g., hepatic encephalopathy, TIPS-induced hemolysis
- Prevention of complications: Periprocedural rifaximin may be used to reduce the risk of hepatic encephalopathy. [17]
Shunt implementation results in reduced hepatic elimination of ammonia and may lead to worsening of encephalopathy.
")
Surgical portosystemic shunts [20][21]
-
Indications [20][22]
- Recurrent variceal bleeding after TIPS
- Contraindications to TIPS
-
Techniques
- Total (nonselective) portosystemic shunts: The portal vein is completely shunted to the vena cava, reducing portal pressure. [21]
- Selective portosystemic shunts
- The portal vein is partially shunted to the vena cava, reducing portal pressure.
- The partial shunt prevents variceal bleeding while continuing to allow portal perfusion. [21]
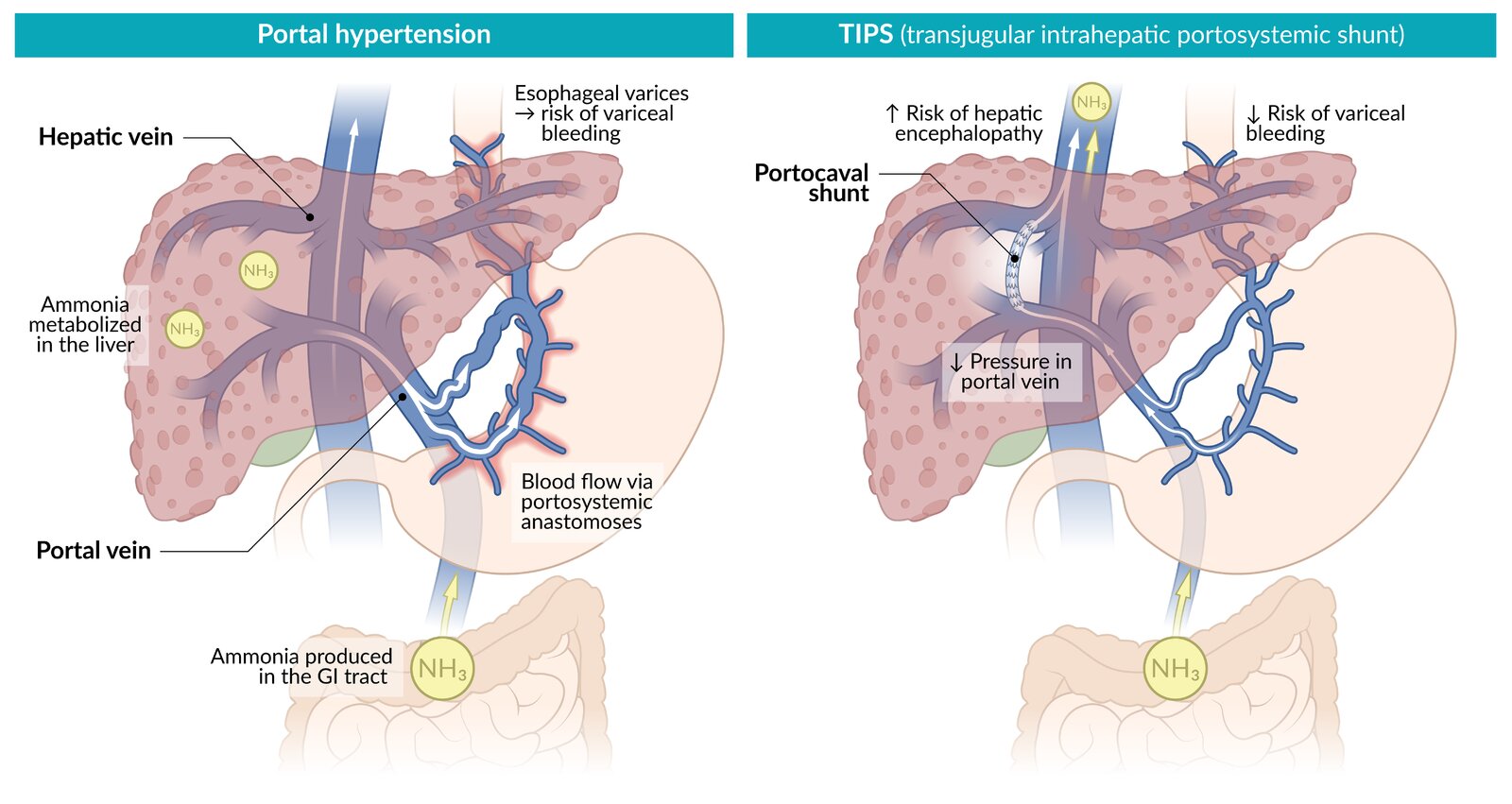
Portal hypertension (i.e., elevated portal venous pressure), can lead to the backflow of venous blood into portosystemic anastomoses (gastrointestinal varices) through the branches of the portal vein. Increased blood flow in esophageal varices can cause potentially life-threatening variceal hemorrhages.
In TIPS, a metallic stent is inserted through the jugular vein to connect a hepatic vein radicle with an intrahepatic branch of the portal vein. TIPS diverts the drainage of blood from the portal to the systemic circulation, bypassing the liver, thus lowering portal pressure and reducing the risk of variceal bleeding. TIPS increases the level of ammonia in the systemic circulation because blood bypasses the liver, increasing the risk of hepatic encephalopathy.
© AMBOSS
Complications
- Life-threatening esophageal variceal bleeding
- Portal hypertensive gastropathy
- Ascites
- Spontaneous bacterial peritonitis
- Hepatorenal syndrome
- Impaired liver function (see “Cirrhosis”)
- Hepatic encephalopathy
- Pulmonary complications of portal hypertension (e.g., hepatopulmonary syndrome, portopulmonary hypertension)
- Cirrhotic cardiomyopathy
- Gastric antral vascular ectasia
We list the most important complications. The selection is not exhaustive.
Portal hypertensive gastropathy
- Definition: gastric venous and capillary ectasia resulting from CSPH [10]
-
Epidemiology
- Prevalence among patients with compensated cirrhosis: approx. 50–80% [10]
- More common in patients with medium or large gastroesophageal varices than in those with no or small gastroesophageal varices
-
Clinical features
- Often asymptomatic
- Symptoms of iron-deficiency anemia from chronic blood loss
- Features of overt GI bleeding (rare) [10]
-
Diagnostics
-
EGD (first-line) [10]
- Proximal lesions [23]
- Mosaic pattern (“snakeskin” mucosa)
- Intramucosal hemorrhage (red or black-brown markings)
- Portal hypertension (PH) related polyps may be visible. [10]
- Other modalities: CT, MRI, capsule endoscopy [23]
-
EGD (first-line) [10]
-
Management [10]
- Acute GI bleeding from severe PHG
- Vasoactive therapy (e.g., octreotide) at doses used for variceal bleeding for 2–5 days
- See “Management of esophageal variceal hemorrhage.”
- Chronic management
- NSBBs to prevent decompensation or rebleeding
- Management of chronic blood loss [23]
- Iron supplementation
- Blood transfusions
- TIPS for patients who are transfusion-dependent despite NSBB therapy
- Argon plasma coagulation
- Acute GI bleeding from severe PHG
Rule out H. pylori infection (a common differential diagnosis) before initiating prophylactic therapy with NSBBs. [10]

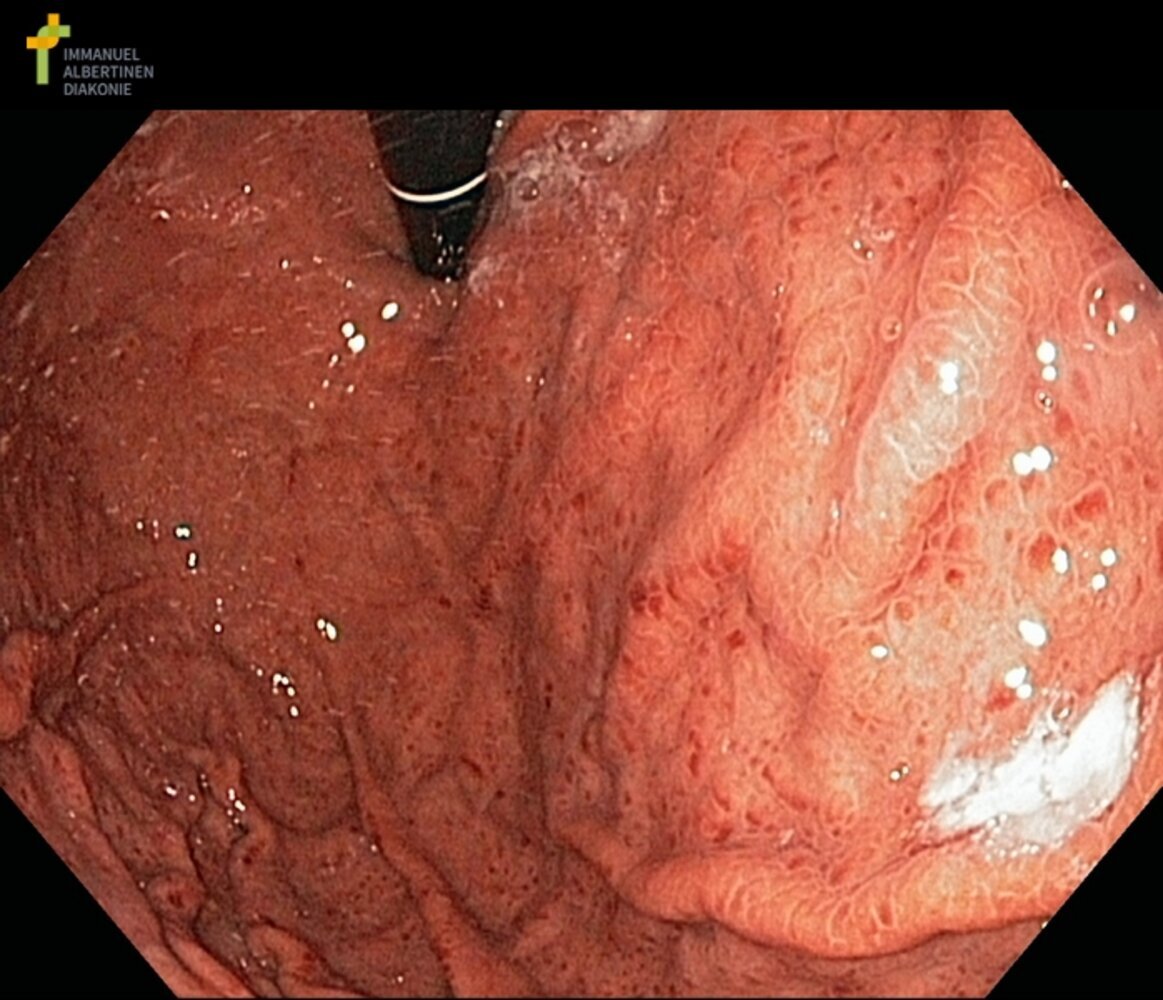
Endoscopic view of the stomach (retroflexion) in a patient with portal hypertension
The mucosa is edematous and erythematous with multiple areas of bleeding.
These findings are pathognomonic of portal hypertensive gastropathy.
Our great thanks to Albertinen Krankenhaus, Hamburg, Germany, for kindly providing this case.
Gastric antral vascular ectasia (GAVE)
- Definition: dilation of small mucosal and submucosal blood vessels in the gastric antrum
-
Associated conditions [23]
- Portal hypertension, cirrhosis
- Chronic kidney disease
- Connective tissue disorders (e.g., systemic sclerosis)
- Cardiovascular disease
- Bone marrow transplantation
-
Clinical features [24]
- Often asymptomatic
- Symptoms of iron-deficiency anemia from chronic blood loss
- Features of overt GI bleeding (rare)
-
Diagnostics: EGD [23]
- Distal linear erythematous streaks
- Classically described as “watermelon stomach”
- Biopsy in selected cases for diagnostic confirmation (e.g., when the diagnosis is uncertain) [23]
-
Management
- Endoscopic therapy, e.g., argon plasma coagulation, radiofrequency ablation, band ligation [24][25]
- Management of chronic blood loss, e.g., iron supplementation, transfusions
- Initial management of overt GI bleeding
While GAVE is associated with portal hypertension, it is not thought to be caused by portal hypertension, and medication to reduce CSPH is ineffective in the management of GAVE. [23]

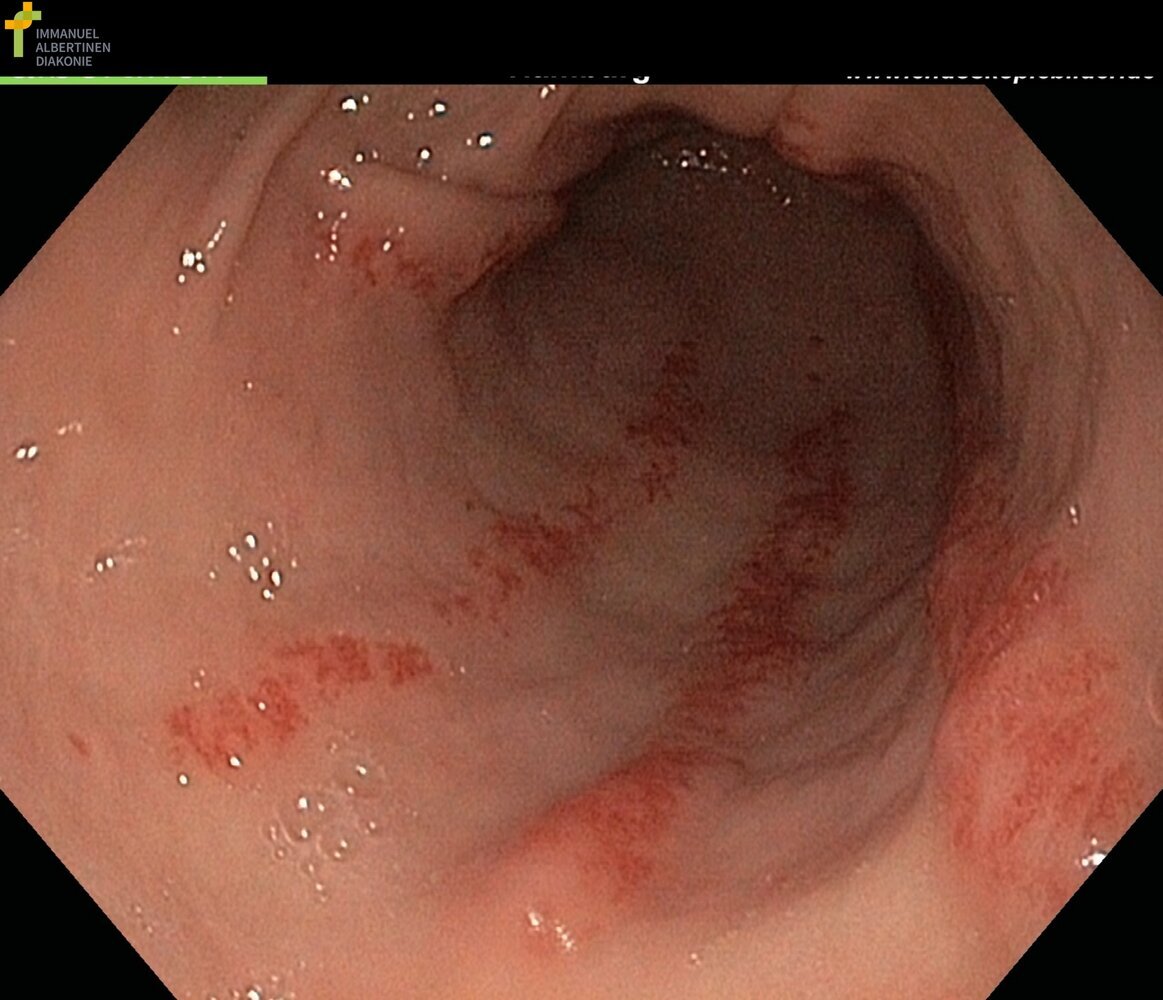
Endoscopic view of the stomach in a patient with portal hypertension
Fragile dilated blood vessels are visible as red stripes in the pyloric antrum.
These findings are pathognomonic of gastric antral vascular ectasia.
Our great thanks to Albertinen Krankenhaus, Hamburg, Germany, for kindly providing this case.
External Resources
- 2024 AASLD Practice Guideline on Noninvasive Liver Disease Assessment of Portal Hypertension
- 2024 AASLD Practice Guidance on Risk Stratification and Management of Portal Hypertension and Varices in Cirrhosis
- 2023 AASLD Practice Guidance on the use of TIPS, Variceal Embolization, and Retrograde Transvenous Obliteration in the Management of Variceal Hemorrhage
- 2022 North American Practice-Based Recommendations for Transjugular Intrahepatic Portosystemic Shunts in Portal Hypertension
- 2022 Baveno VII - Renewing Consensus in Portal Hypertension
References
- Nakhleh RE. "The pathological differential diagnosis of portal hypertension". Clin Liver Dis (Hoboken). 10(3). :57-62. (2017)
- Singal AK, Kamath PS, Tefferi A. "Mesenteric Venous Thrombosis". Mayo Clin Proc. 88(3). :285-294. (2013)
- Garcia-Tsao G. "Idiopathic Noncirrhotic Portal Hypertension: What Is It?". Clin Liver Dis (Hoboken). 5(5). :120-122. (2015)
- Schouten JNL, Garcia-Pagan JC, Valla DC, Janssen HLA. "Idiopathic noncirrhotic portal hypertension". Hepatology. 54(3). :1071-1081. (2011)
- Guimarães Cavalcanti M, Marcello de Araujo-Neto J, Mauro Peralta J. "Schistosomiasis: Clinical management of liver disease". Clin Liver Dis (Hoboken). 6(3). :59-62. (2015)
- Koh C, Heller T. "Approach to the diagnosis of portal hypertension". Clin Liver Dis (Hoboken). 1(5). :133-135. (2012)
- Iwakiri Y. "Pathophysiology of Portal Hypertension". Clin Liver Dis. 18(2). :281-291. (2014)
- Al-Busafi SA, McNabb-Baltar J, Farag A, Hilzenrat N. "Clinical Manifestations of Portal Hypertension". Int J Hepatol. 2012. :1-10. (2012)
- Biecker E. "Portal hypertension and gastrointestinal bleeding: Diagnosis, prevention and management". World J Gastroenterol. 19(31). :5035. (2013)
- Kaplan DE, Bosch J, Ripoll C, et al. "AASLD practice guidance on risk stratification and management of portal hypertension and varices in cirrhosis". Hepatology. (2023)
- de Franchis R, Bosch J, Garcia-Tsao G, et al. "Baveno VII – Renewing consensus in portal hypertension". J Hepatol. 76(4). :959-974. (2022)
- Sterling RK, Asrani SK, Levine D, et al. "AASLD Practice Guideline on noninvasive liver disease assessment of portal hypertension". Hepatology. (2024)
- Simonetto DA, Liu M, Kamath PS. "Portal Hypertension and Related Complications: Diagnosis and Management". Mayo Clin Proc. 94(4). :714-726. (2019)
- Garcia‐Tsao G, Abraldes JG, Berzigotti A, et al. "Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases". Hepatology. 65(1). :310-335. (2016)
- Bochnakova T. "Hepatic Venous Pressure Gradient". Clin Liver Dis (Hoboken). 17(3). :144-148. (2021)
- Boike JR, Thornburg BG, Asrani SK, et al. "North American Practice-Based Recommendations for Transjugular Intrahepatic Portosystemic Shunts in Portal Hypertension". Clin Gastroenterol Hepatol. 20(8). :1636-1662.e36. (2022)
- Lee EW, Eghtesad B, Garcia-Tsao G, et al. "AASLD Practice Guidance on the use of TIPS, variceal embolization, and retrograde transvenous obliteration in the management of variceal hemorrhage". Hepatology. (2023)
- Patidar KR, Sydnor M, Sanyal AJ. "Transjugular Intrahepatic Portosystemic Shunt". Clin Liver Dis. 18(4). :853-876. (2014)
- Bhogal HK, Sanyal AJ. "Transjugular intrahepatic portosystemic shunt: An overview". Clin Liver Dis (Hoboken). 1(5). :173-176. (2012)
- Taslakian B, Faraj W, Khalife M, et al. "Assessment of surgical portosystemic shunts and associated complications: The diagnostic and therapeutic role of radiologists". Eur J Radiol. 84(8). :1525-1539. (2015)
- Harmantas A. "Selective vs total portosystemic shunts in the treatment of variceal hemorrhage in cirrhotic patients: is there any advantage?". Hepatology Res. 14(2). :144-153. (1999)
- Boyer TD, Haskal ZJ. "The role of transjugular intrahepatic portosystemic shunt in the management of portal hypertension". Hepatology. 41(2). :386-400. (2005)
- Rockey DC. "Portal Hypertensive Gastropathy and Colopathy". Clin Liver Dis. 23(4). :643-658. (2019)
- McCarty TR, Hathorn KE, Chan WW, Jajoo K. "Endoscopic band ligation in the treatment of gastric antral vascular ectasia: a systematic review and meta-analysis". Endosc Int Open. 09(07). :E1145-E1157. (2021)
- Maida M, Camilleri S, Manganaro M, Garufi S, Scarpulla G. "Radiofrequency Ablation for Treatment of Refractory Gastric Antral Vascular Ectasia: A Systematic Review of the Literature". Gastroenterol Res Pract. 2017. :1-5. (2017)