CME information and disclosures
To see contributor disclosures related to this article, click on this reference: [1]
Physicians can earn CME/MOC credit by using this article to address a clinical question and completing a brief evaluation about how they applied the information in their practice.
AMBOSS designates this internet point-of-care activity for a maximum of 0.5 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
For answers to questions about AMBOSS CME, including how to redeem CME/MOC credit, see “Tips and links” at the bottom of this article.
Summary
Postpartum complications include infectious, vascular, genitourinary, musculoskeletal, and behavioral conditions. Infectious complications include postpartum endometritis, postpartum sepsis, mastitis, and wound infections. Vascular complications include postpartum hemorrhage, venous thromboembolism, amniotic fluid embolism, and thrombophlebitis. Genitourinary complications include uterine injuries and dysfunction, bladder dysfunction, urinary tract infections, and vaginal or perineal trauma. Musculoskeletal complications include diastasis recti, pelvic or back pain, and nerve injuries. Behavioral complications include postpartum depression, psychosis, and sexual dysfunction. Early recognition and treatment are crucial for maternal recovery and well-being.
See also “Complications of normal labor and delivery,” “Abnormal labor and delivery,” and "Sepsis in pregnancy and postpartum."
Infectious
Peripartum pelvic infections [2][3]
Maternal peripartum infection [4][5]
- An infection of the genital tract and adjacent tissue occurring within 6 weeks of childbirth, miscarriage, or induced abortion
- Sites include:
- Postpartum endometritis
- Surgical site infection (e.g., from cesarean delivery or episiotomy)
- Wound infection or SSTI from vaginal injuries or perineal lacerations
- Pelvic intraabdominal abscess
- Peritonitis
- Presence of ≥ 2 of the following is necessary for diagnosis: [4]
- Fever
- Pelvic pain
- Abnormal vaginal discharge
- Delay in uterine involution
- Complications: postpartum sepsis
Maternal peripartum infection is the most common cause of postpartum sepsis. [3]
Postpartum endometritis [6][7]
Background
- Definition: inflammation of the endometrium; may include the myometrium (postpartum endomyometritis), parametrium (postpartum parametritis), and/or surgical site
-
Risk factors
- Cesarean delivery [6]
- Prolonged labor
- Prolonged rupture of membranes
- Multiple cervical examinations
- RPOC
- Meconium in amniotic fluid [8]
- Low socioeconomic status
- Etiology: mostly polymicrobial (2–3 ascending organisms, e.g., Gardnerella vaginalis, Staphylococcus epidermidis, Group B Streptococcus, Escherichia coli, and/or Ureaplasma urealyticum, all of which are usually found in the normal vaginal flora) [9]
- Pathophysiology: retention of lochia → ideal breeding ground for infection → postpartum endometritis/postpartum endomyometritis → postpartum sepsis
Clinical features of postpartum endometritis
- Fever
- Lower abdominal pain, uterine tenderness
- Chills, malaise
- Foul-smelling lochia
Diagnostics
Primarily clinical diagnosis; studies help guide management
- Pelvic examination: Check for RPOC and surgical site infection.
- Vaginal cultures: Obtain if vaginal discharge is purulent; otherwise utility is limited due to contamination.
- Blood cultures: Obtain if signs of sepsis are present.
- STI screening: Consider if not performed during routine prenatal care.
-
Imaging (ultrasound and/or CT) [6]
- Useful for ruling out complications (e.g., abscess) and differential diagnoses (e.g., appendicitis)
- Consider for patients with:
- Signs of sepsis or peritoneal signs
- Endometritis after cesarean delivery
Treatment [10]
-
All patients: empiric IV antibiotics
- First line: clindamycin PLUS gentamicin (off-label) [6]
- Second line
- Cefoxitin OR cefotaxime [6]
- PLUS vancomycin (off-label) [6]
- Patients with RPOC: curettage to prevent puerperal sepsis
Treat puerperal sepsis, if present.
Disposition
- Consult obstetrics.
- Hospital admission is usually required. [6]
Complications
- Peritonitis
- Intraabdominal abscess
Other peripartum infections
- Mastitis
- Urinary tract infections
- Surgical site infections
- Other skin and soft tissue infections
- Aspiration pneumonia
Vascular
Bleeding
- Postpartum hemorrhage
- Postpartum retroperitoneal hematoma
Thromboembolic complications
- Deep vein thrombosis
- Pulmonary embolism
- Cerebral venous thrombosis
- Nonthrombotic embolism: amniotic fluid embolism
Septic pelvic thrombophlebitis [11][12][13]
- Definition: : a rare condition characterized by inflammation and thrombosis of the pelvic veins that most commonly occurs in the postpartum period
-
Risk factors
- Cesarean deliveries
- Pelvic infections (e.g., endometritis, chorioamnionitis)
- Abortion
-
Etiology
- Pregnancy-induced hypercoagulability
- Postpartum pelvic venous stasis
- Endothelial damage due to an infection (e.g., endometritis) or bacteremia
-
Clinical features: Onset is usually within one week of delivery.
- Patients are acutely unwell with fever and abdominal pain and tenderness on the side of the affected vein; a palpable cord may be present.
- Approx. 90% of cases involve the right ovarian vein.
-
Diagnostics
-
Contrast CT or MRI
- Visualization of dilation and thrombosis of the affected vein confirms the diagnosis.
- Most commonly ovarian vein thrombosis
- Blood culture: most commonly streptococci, Enterobacteriaceae, and anaerobes
-
Contrast CT or MRI
- Treatment: antibiotics (e.g., clindamycin, gentamicin) and anticoagulation (e.g., LMWH or UFH)
- Complications: Pulmonary emboli are rare.
Genitourinary
Uterine
-
Subinvolution of the uterus
- Impaired retraction of the uterine muscles
- Can cause severe bleeding
- Retained placenta
- Uterine rupture
- Uterine inversion
- Uterine prolapse
Urinary
- Urinary insufficiency: See “Urinary incontinence in pregnancy”
- Bladder dysfunction: e.g., overactive bladder
- Urethral injury
Postpartum urinary retention (PUR) [14][15]
-
Definition: inability to void after delivery
- Overt PUR: inability to void 6 hours after vaginal delivery or, in case of cesarean section, 6 hours after removal of urinary catheter
- Covert PUR: post-void residual bladder volume ≥ 150 mL following micturition (assessed by ultrasound or catheterization)
-
Risk factors [16]
- Prolonged labor
- Perineal lacerations
- Macrosomia
-
Clinical features
- Potentially asymptomatic
- Bladder pain/discomfort
- Bladder distention
- Small void volumes
- Straining to void
- Slow stream
- Urinary frequency
-
Treatment
- Intermittent catheterization in symptomatic patients
- Prognosis: typically self-limited (resolves within 1 week)
Vaginal and perineal
- Vaginal injury
- Perineal laceration
- Rectovaginal fistula
- Dyspareunia
Musculoskeletal
Diastasis recti
- Definition: a > 2 cm separation of the right and left rectus abdominis muscles resulting in protrusion of abdominal organs on straining
-
Risk factors
- Conditions that increase intraabdominal pressure (e.g., pregnancy, abdominal surgery)
- Aneurysmal disease
-
Clinical features
- Some patients may be asymptomatic.
- Abdominal pain and discomfort
- Pelvic instability and lumbar pain
- Urinary and/or fecal incontinence
-
Diagnostics
- Physical examination: distortion or extension of the linea alba
- Ultrasound: confirms the diagnosis
-
Treatment
- Postpartum exercise: Initiating an exercise program 6–8 weeks postpartum can help strengthen the abdominal rectus muscles and reduce the abnormal extension of the linea alba.
- Weight loss: may be appropriate in patients who develop diastasis recti due to obesity.
- Surgical repair (e.g., abdominoplasty)
- Patients with severe, recurring, and symptomatic diastasis recti
- If conservative treatment fails after > 6 months
- Complications: pelvic organ prolapse

Pubic symphysis diastasis [17]
- Definition: a rare complication of the peripartum period characterized by a widening of the pubic symphysis beyond the physiological width (≤ 10 mm).
-
Risk factors include:
- Macrosomia
- Cephalopelvic disproportion
- Prolonged second stage of labor
- Previous pelvic trauma
- Forceps delivery
-
Clinical features
- Potentially asymptomatic
-
Pain and tenderness of the pubic symphysis
- Worsens with walking, climbing stairs, lifting heavy objects, and standing on one leg
- May radiate to the sacroiliac area and anterior and/or lateral part of the thigh
- Destot sign: labia majora hematoma
-
Diagnostics
- Ultrasound and MRI are preferred during pregnancy.
- Pelvic x-ray and CT scan may be used after childbirth.
-
Treatment
- Conservative: analgesia, pelvic belt, and physiotherapy
- Surgery should be considered if conservative therapy fails: open reduction with internal fixation
Other MSK complications
- Back pain
- Pelvic pain
- Obstetric nerve injuries
- Coccydynia
- Pelvic floor dysfunction
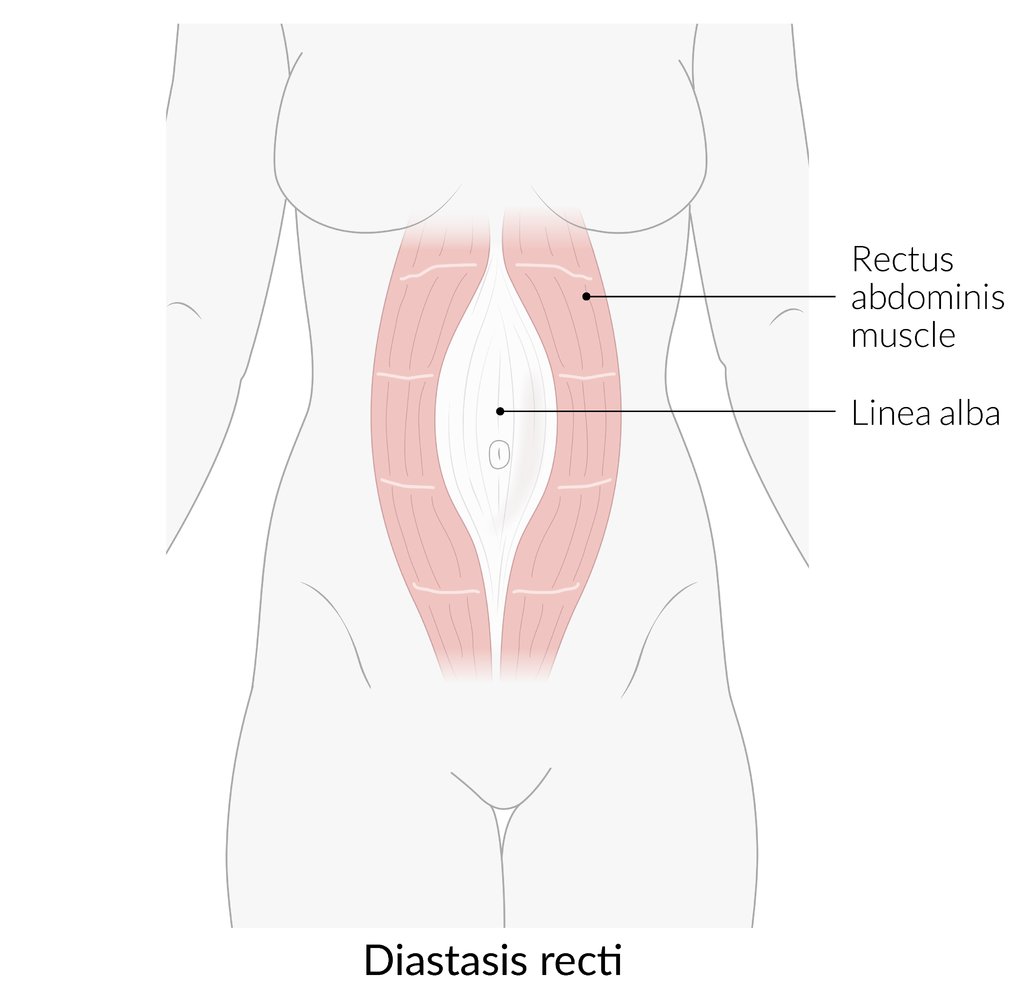
There is an abnormally large separation (>2 cm) between the two rectus abdominis muscles. This results in protrusion of intra-abdominal contents through the linea alba on straining (e.g., coughing, sitting up from a reclined posture), causing a midline bulge. The abdominal fascias (not shown here) remain intact.
© AMBOSS
Behavioral
Postpartum sexual dysfunction
- Definition: the decline of sexual function after delivery that may not return to its baseline levels during the postpartum period
-
Risk factors
- Prepregnancy dyspareunia
- Delivery mode (e.g., vacuum-assisted vaginal delivery, emergency cesarean delivery)
- Perineal trauma (e.g., second and third-degree perineal tears)
- Episiotomy
- Breastfeeding (associated with decreasing vaginal lubrication, causing vaginal atrophy and loss of interest in sexual activity)
- Postpartum physiological and psychological changes (e.g., postpartum mood changes, postpartum depression, fatigue)
- Childbirth complications (e.g., postpartum genital infections, postpartum hemorrhage, obstructed labor)
Psychiatric
- Postpartum depression
- Postpartum psychosis
External Resources
References
- Plante LA, Pacheco LD, Louis JM. "SMFM Consult Series #47: Sepsis during pregnancy and the puerperium". Am J Obstet Gynecol. 220(4). :B2-B10. (2019)
- Shields A, de Assis V, Halscott T. "Top 10 Pearls for the Recognition, Evaluation, and Management of Maternal Sepsis". Obstet Gynecol. 138(2). :289-304. (2021)
- World Health Organization. "WHO Recommendations for Prevention and Treatment of Maternal Peripartum Infections". World Health Organization. (2015). ISBN: 9789241549363
- Adorno M. "Sepsis in the Obstetric Client". Crit Care Nurs Clin North Am. 30(3). :415-422. (2018)
- Wheaton N, Al-Abdullah A, Haertlein T. "Postdelivery Emergencies". Emerg Med Clin North Am. 37(2). :287-300. (2019)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Pakniat H, Mohammadi F, Ranjkesh F. "Meconium Amniotic Fluid is Associated with Endomyometritis". J Obstet Gynecol India. 66(S1). :136-140. (2016)
- Mehta S, Grover A. "Infections and Pregnancy". Springer Singapore. (2022). ISBN: 9789811678646
- Mackeen AD, Packard RE, Ota E, Speer L. "Antibiotic regimens for postpartum endometritis". Cochrane Database Syst Rev. 2015(12). (2015)
- Chellman-Jeffers MR. "Ovarian Vein Thrombosis". WebMD. https://emedicine.medscape.com/article/404364. [2016-01-09]
- Chen KT. "Septic Pelvic Thrombophlebitis". UpToDate. UpToDate. https://www.uptodate.com/contents/septic-pelvic-thrombophlebitis. [2016-02-24]
- "Septic thrombophlebitis". http://www.dynamed.com/topics/dmp~AN~T922454/Septic-thrombophlebitis. [2018-09-05]
- Yip SK, Sahota D, Pang MW, Chang A. "Postpartum urinary retention.". Acta obstetricia et gynecologica Scandinavica. 83(10). :881-91. (2004)
- Yip SK, Brieger G, Hin LY, Chung T. "Urinary retention in the post-partum period. The relationship between obstetric factors and the post-partum post-void residual bladder volume.". Acta obstetricia et gynecologica Scandinavica. 76(7). :667-72. (1997)
- Cavkaytar S, Kokanalı MK, Baylas A, et al. "Postpartum urinary retention after vaginal delivery: Assessment of risk factors in a case-control study.". Journal of the Turkish German Gynecological Association. 15(3). :140-3. (2014)
- Stolarczyk A, Stępiński P, Sasinowski Ł, et al. "Peripartum Pubic Symphysis Diastasis-Practical Guidelines.". Journal of clinical medicine. 10(11). (2021)
- "Contributor Disclosures - Postpartum complications. None of the individuals in control of the content for this article reported relevant financial relationships with ineligible companies. For details, please review our full conflict of interest (COI) policy"