Summary
Postpartum hemorrhage (PPH) is an obstetric emergency and is defined as a blood loss ≥ 1000 mL or blood loss presenting with signs or symptoms of hypovolemia within 24 hours of delivery. It is the number one cause of maternal morbidity and mortality worldwide. PPH is generally associated with symptoms of hypovolemia. The onset may be within 24 hours (primary PPH) to 12 weeks postpartum (secondary PPH). The most significant causes of postpartum hemorrhage are uterine atony, maternal birth trauma, abnormal placental separation, velamentous cord insertion, and coagulation disorders. Clinical findings are related to the amount of blood loss and can include anemia (e.g., lightheadedness, pallor) or hypovolemic shock (e.g., hypotension, tachycardia). Diagnosis is done through early recognition of clinical findings, systematic evaluation of the most common causes, and, in some cases, confirmed with ultrasound. Treatment depends on the underlying condition and may include general measures to control blood loss and maintain adequate perfusion to vital organs, suturing of bleeding lacerations, active management of the third stage of labor like manual maneuvers to aid in placental separation, and use of uterotonic agents for uterine atony. A hysterectomy is often considered as a last resort in uncontrolled postpartum hemorrhage.
Overview
Definitions [1]
Blood loss ≥ 1000 mL or blood loss manifesting with features of hypovolemia within 24 hours of delivery.
- Primary PPH: blood loss ≤ 24 hours postpartum (more common)
- Secondary PPH: blood loss from 24 hours to 12 weeks postpartum
Epidemiology [1][2]
- Leading cause of maternal mortality worldwide
- Approx. 5% of obstetric patients experience PPH.
- PPH causes 12% of maternal deaths in the US.
Etiology [1]
| Overview of common causes of postpartum hemorrhage | |||||
|---|---|---|---|---|---|
| Risk factors/Etiology | Clinical features | Diagnostics | Treatment | ||
| Primary PPH | |||||
| Uterine atony |
|
|
|
|
|
| Uterine inversion |
|
|
|
|
|
| Abnormal placental separation | Retained placenta |
|
|
|
|
| Abnormal placentation |
|
|
|
|
|
| Birth trauma |
|
|
|
|
|
| Velamentous cord insertion |
|
|
|
|
|
| Secondary PPH | |||||
| Retained products of conception |
|
|
|
|
|
| Subinvolution of the placental site |
|
|
|
|
|
| Coagulation disorder | Acquired |
|
|
|
|
| Inherited [5] |
|
||||
| Postpartum endometritis |
|
|
|
|
|
The causes of postpartum hemorrhage are the 4 T's: Tone (uterine atony), Trauma (e.g., laceration, uterine inversion), Tissue (retained placenta), Thrombin (bleeding diathesis).
Clinical features
- Rapid, heavy vaginal bleeding
- Possible signs of hypovolemia/blood loss: decreased blood pressure, increased heart rate, dizziness
Diagnosis
- Laboratory measures: e.g., hematocrit, hemoglobin to estimate blood loss
- Physical examination findings: e.g., lacerations, hematoma, any other visible cause of bleeding, boggy uterus
-
Speculum examination:
- Uterine inversion
- Retained placental tissue or membranes
- Puerperal hematoma
-
Ultrasound
- Used to determine the correlation between the placenta and the cervical os
- Helpful to diagnose the following:
- Uterine atony: showing, e.g., an echogenic endometrial stripe
- Abnormal placental attachment: showing, e.g., thinning of uterine myometrial wall
- Color Doppler ultrasound: to confirm abnormal placental attachment (showing, e.g., turbulent blood flow)
Management of PPH
-
General measures: to control blood loss and ensure perfusion of vital organs
- Monitoring of vital signs and urine output
- Oxygenation
- Two large-bore IV access (≥ 16 gauge) and ice pack
- Fluid therapy (with intravenous crystalloid solutions)
- Blood transfusions; (whole blood or red blood cell concentrates) and/or platelet transfusions, if necessary
-
Surgical procedures: in cases of uncontrolled bleeding
-
Ligation of uterine or internal iliac arteries, or uterine artery embolization
- Decreases bleeding by reducing myometrial perfusion
- Fertility remains intact because of collateral blood supply by the ovarian arteries.
- Uterine suturing (e.g., B-Lynch suture)
- Hysterectomy: generally as last resort, except in placenta accreta spectrum
-
Ligation of uterine or internal iliac arteries, or uterine artery embolization
Prevention [1][6]
-
Antenatal assessment of risk factors, including:
- Identification of anemia and coagulopathies
- Sonography to identify placenta accreta in women with a history of cesarean deliveries
-
Active management of the third stage of labor: delivery of the placenta which involves the following components
- Uterotonic agents (; IV/IM oxytocin)
-
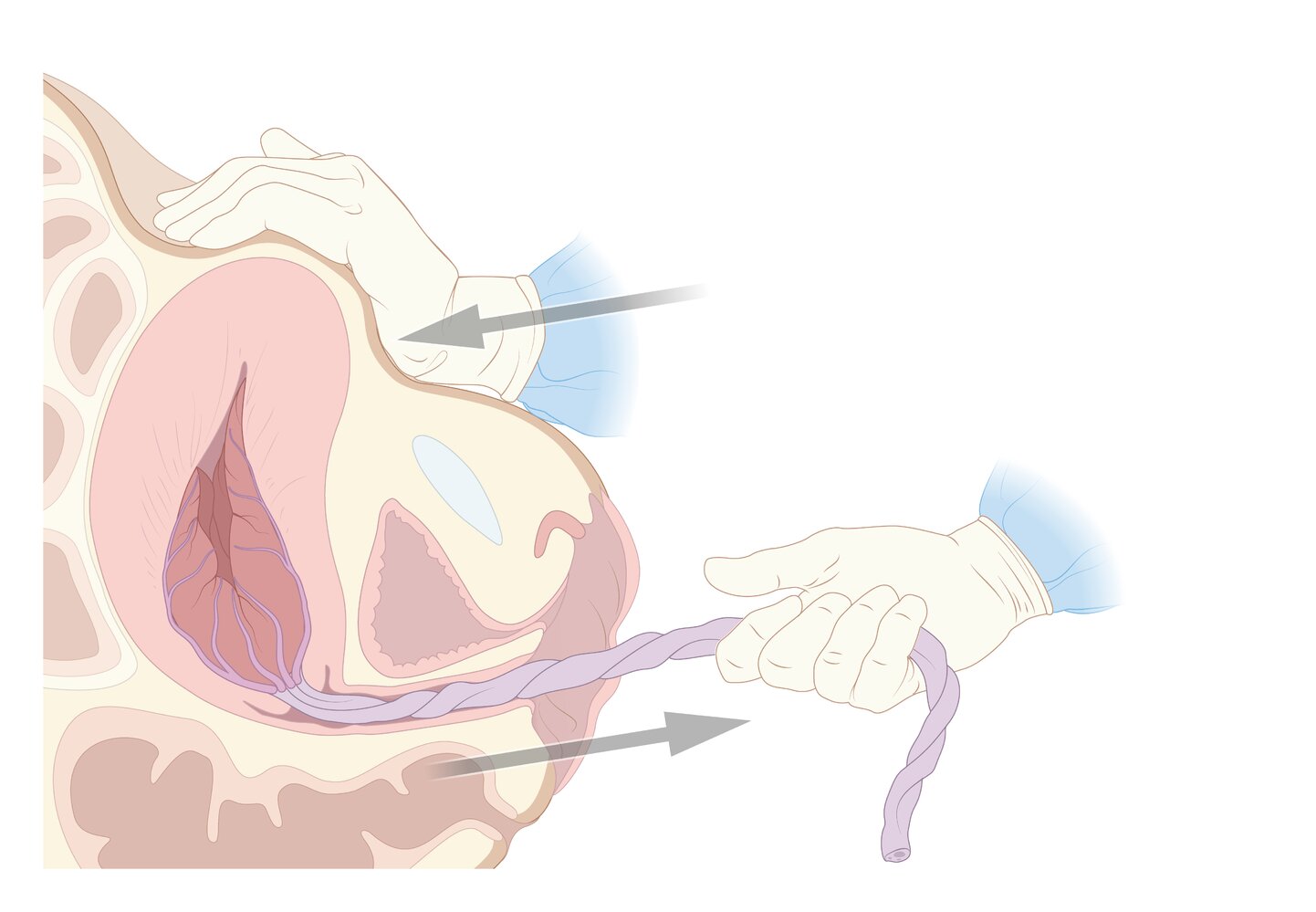
Controlled umbilical cord traction (Brandt-Andrews maneuver)
- One hand is placed on the abdomen, securing the uterine fundus and preventing uterine inversion.
- The other hand applies steady downward traction on the umbilical cord.
-
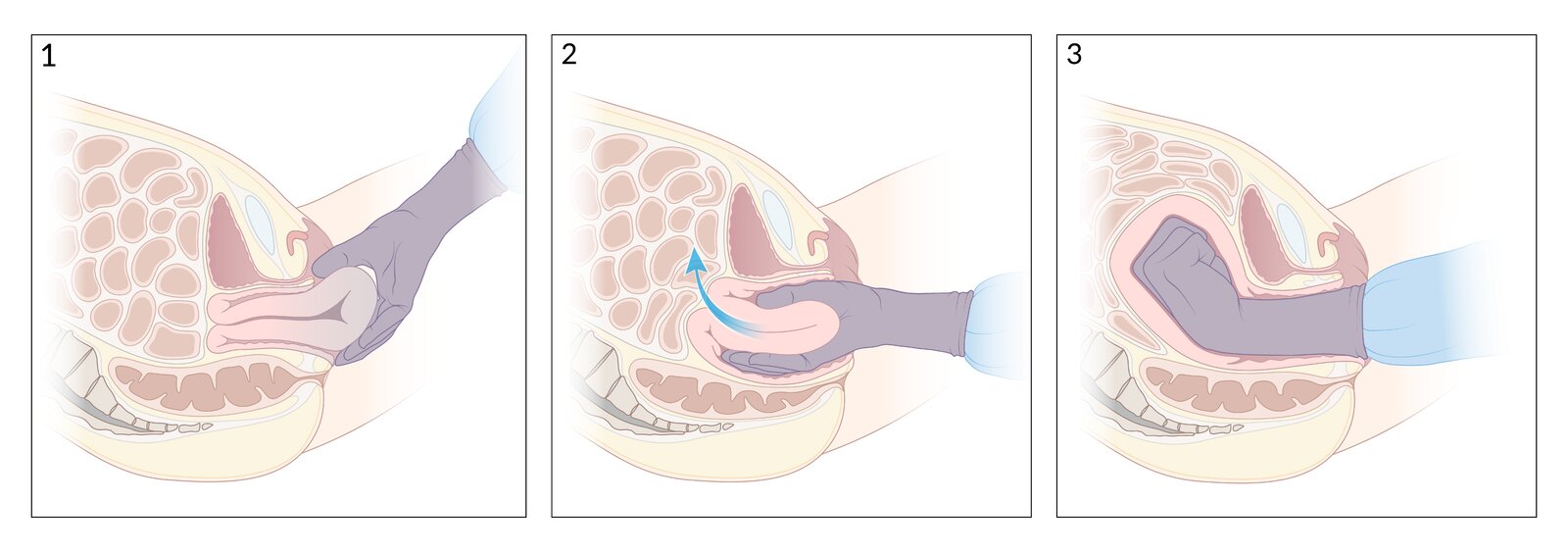
External compression of the uterus and bimanual uterine massage: a manual technique to promote uterine contractions and to tamponade the vascular sinuses in the uterus
- A clenched fist is inserted into the anterior vaginal fornix and exerts pressure on the anterior wall of the uterus.
- The other hand is positioned externally and the uterus is massaged between the two hands.
-
Fritsch maneuver
- One hand grasps the labia majora and presses it firmly into the vulva.
- Simultaneously, the second hand is positioned at the posterior side of the uterus (as in Credé maneuver) and is pushed distally against the other hand.
- The placenta is manually removed.
- Fundal massage
-
Credé maneuver
- The cranial part of the uterus is held with four fingers positioned at the posterior side of the uterus and the thumb at the anterior surface.
- The pressure compresses the uterine vessels and aids in the expulsion of the placenta.
- Avoidance of unnecessary episiotomy and assisted vaginal delivery



Complications [2]
- Anemia
- Hypovolemic shock
- Thromboembolism
- Sheehan syndrome
- Infection
- Maternal death
- Disseminated intravascular coagulation
- Fetal death (due to velamentous cord insertion)
- Abdominal compartment syndrome
© AMBOSS
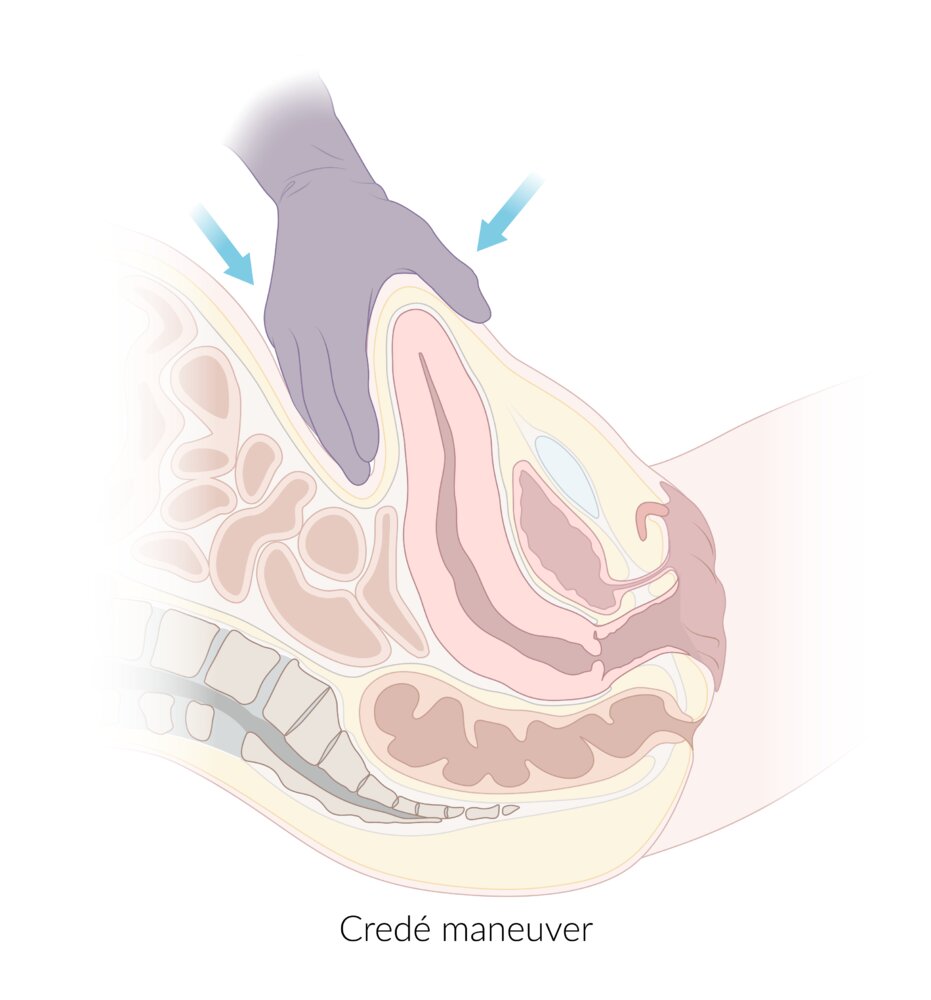
To reduce bleeding and aid the expulsion of the placenta after childbirth, the cranial part of the uterus is squeezed between the thumb (on the anterior surface) and the other four fingers (on the posterior surface).
© AMBOSS
1. One hand is carefully inserted into the anterior vaginal fornix.
2. The inside hand is clenched into a fist while the other hand is placed on the patient's lower abdomen over the uterine fundus.
3. The uterus is compressed and massaged between the two hands until it contracts.
© AMBOSS
Uterine atony
Definition
- Failure of the uterus to effectively contract after complete or incomplete delivery of the placenta, which can lead to severe postpartum bleeding from the myometrial vessels
Epidemiology
- Most common cause of PPH cases (approx. 80%) [1]
Pathophysiology
- Normally, the myometrium contracts and compresses the spiral arteries, which stops bleeding after delivery.
- Failure of the myometrium to effectively contract can lead to rapid and severe hemorrhage.
Risk factors [7]
-
Overdistention of the uterus
- Large for gestational age newborn (> 4000 g)
- Multiple pregnancies
- Polyhydramnios
-
Exhausted myometrium
- Multiparity
- Postterm pregnancy
- Prolonged delivery
- Prolonged oxytocin use
-
Anatomical abnormalities
- Fetal, uterine, abnormal placental implantation
- Uterine leiomyomas
- Infection: e.g., chorioamnionitis
-
Other
- Medications lowering contractions (e.g., anesthetics, MgSO4)
- Preterm delivery
- Maternal BMI > 40 kg/m2
AEIOU are risk factors for uterine atony: Anatomic Abnormalities, Exhausted myometrium, Infections, Overdistended Uterus
Clinical features [1][8]
- Profuse vaginal bleeding
- Soft, enlarged (increased fundal height), boggy ascending uterus
Diagnosis
- Bimanual pelvic exam after emptying the bladder
- Speculum examination of the vagina and cervix to evaluate possible sources of extrauterine bleeding (e.g., vaginal injury caused during birth)
Treatment [1][2][7][8]
- Active management of the third stage of labor: See “Prevention” in “Overview” section above.
-
Hemorrhage control
-
Uterotonic agents
- IV oxytocin (diluted in saline)
- IM carboprost tromethamine: if the patient does not suffer from asthma
-
IM methylergonovine: if no hypertension or arterial disease is present
- Ergot alkaloid agent
- Increases frequency and amplitude of uterine contractions, which shortens labor and reduces blood loss
- Contraindications include pre-existing hypertension and preeclampsia
- Prostaglandins such as misoprostol: useful when injectable uterotonic agents are unavailable or contraindicated (can also be given intracavitary)
-
Tranexamic acid
- Given concomitantly with uterotonic agents
- Should be administered as soon as possible after bleeding onset to stop fibrinolysis and reduce the likelihood of mortality
- Early clamping and cutting of the umbilical cord
-
Uterotonic agents
-
Exclude coagulation disorders: e.g., disseminated intravascular coagulation, hyperfibrinolysis
- Blood coagulation should be tested (alternatively a thrombelastogram should be performed).
- Treatment is based on the results of the coagulation panel.
- Substitution of deficient coagulation factors such as FFP or prothrombin complex concentrate
- Administration of tranexamic acid in hyperfibrinolysis
-
Surgical procedures
- Uterine balloon tamponade or packing: if severe bleeding persists, regardless of adequate general measures
- Compression sutures (e.g., B-Lynch suture)
- Surgical ligation of uterine or internal iliac arteries
- Last resort: hysterectomy
Complications
- Anemia
- Hypovolemic shock
- Sheehan syndrome
Uterine inversion
Definition
- An obstetric emergency in which the uterine fundus collapses into the endometrial cavity, resulting in a complete or partial inversion of the uterus, usually following vaginal delivery
Epidemiology
- Uncommon complication of vaginal birth
- Morbidity and mortality may occur in ∼ 41% of cases [9]
Classification [10]
Degree of inversion
- Partial uterine inversion: uterine fundus collapses into the endometrial cavity, without surpassing the cervix
- Complete uterine inversion: uterine fundus collapses into the endometrial cavity and descends through the cervix, but remains within the vaginal introitus
- Uterine prolapse: uterine fundus descends through the vaginal introitus

Time of onset
- Acute uterine inversion: uterine inversion occurring immediately after or within 24 hours of delivery
- Chronic uterine inversion: uterine inversion that has gone unnoticed or uncorrected, usually seen weeks or months after delivery
Etiology
- Puerperal inversion: uterine inversion following vaginal delivery (most common)
-
Nonpuerperal inversion
- Due to a submucous myomatous polyp arising from the fundus creating a traction effect
- Due to senile inversion of the uterus following high amputation of the cervix
Risk factors [1][6][11]
- Uncontrolled cord traction and/or excessive fundal pressure (Credé maneuver) during the third stage of labor
- Fetal macrosomia
- Previous uterine inversion
- Use of uterine muscle relaxants during the antepartum period (e.g., MgSO4)
- Difficult removal of the placenta
- Nulliparity
- Uterine anomalies (e.g., relaxed lower uterine segment and cervix)
- Uterine leiomyoma
- Placenta accreta
- Retained placental tissue
- Prolonged delivery
Pathophysiology
- Partial uterine wall relaxation → prolapse of the uterine wall through the cervical orifice, and if simultaneous downward traction of the uterus is performed → inversion of the uterus
Clinical features
-
Acute uterine inversion
- Brisk postpartum hemorrhage
- Lower abdominal pain
- Round mass (inverted uterus) protruding from the cervix or vagina
- Absent fundus (top of the uterus) at the periumbilical position during transabdominal palpation
- Urinary retention
-
Chronic uterine inversion
- History of postpartum hemorrhage
- Irregular bleeding
- Asymptomatic, round vaginal mass
- Vaginal discharge
- Chronic pelvic pain
Diagnosis
- See “Clinical features” above.
-
Ultrasound
- Confirms the diagnosis in uncertain cases
- Hyperechoic mass in the vagina with central hypoechoic cavity
Treatment
- General measures and immediate manual uterine repositioning should be performed. [10]
- In case of chronic uterine inversion, surgical intervention is usually necessary.
General measures
- See “Management” in the “Overview” section above.
- Stop all uterotonic agents (e.g., oxytocin) in order to relax the uterus.
- If the placenta is still in situ, remove it only after successful repositioning of the uterus.
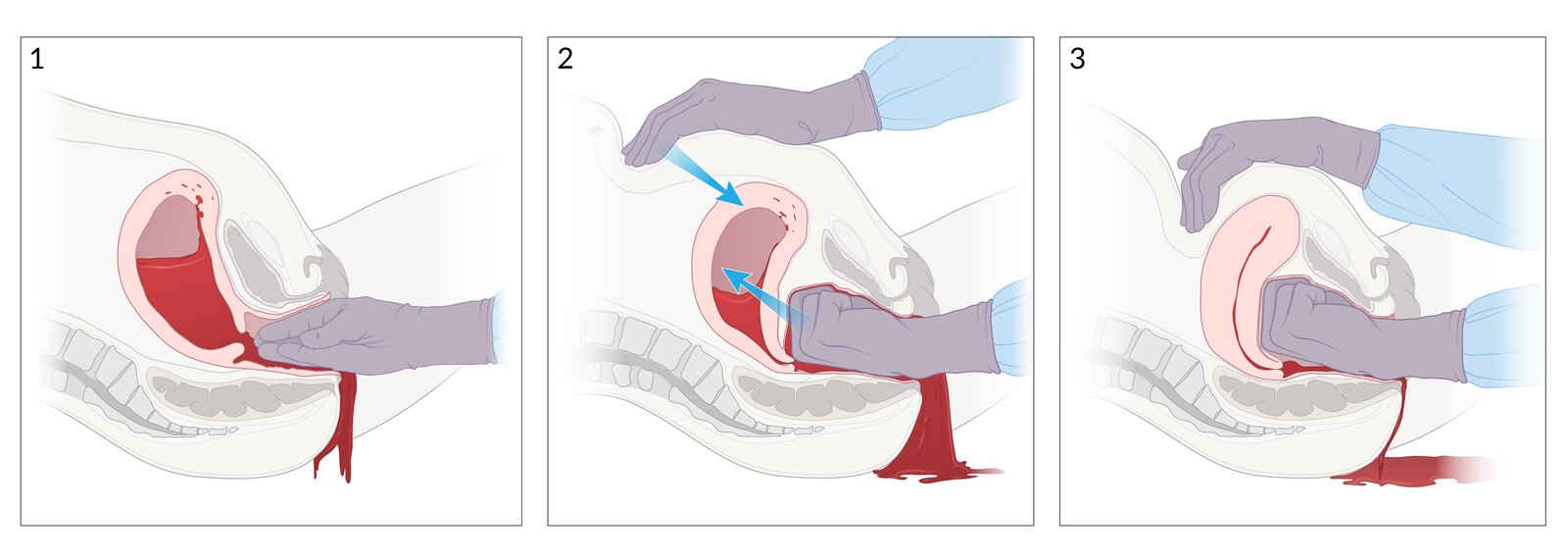
Manual uterine repositioning
-
Technique [1][6]
- Grasp the protruding uterus at the fundus with the thumb on the anterior surface and the four other fingers on the posterior surface.
- Carefully push the uterus back towards the posterior fornix through the pelvic cavity until it is in the correct position.
-
If repositioning is unsuccessful
- Hemodynamically stable patients
- Administer a uterine relaxant (e.g., MgSO4, nitroglycerin, or terbutaline) and reattempt manual repositioning.
- If ineffective: surgical repair
- Hemodynamically unstable patients: surgical repair
- Hemodynamically stable patients
- Following successful repositioning: oxytocin to induce placental extraction and prevent atony and reinversion
")
Complications
- Hypovolemic shock
- Neurogenic shock
- Maternal death

37-year-old woman, gravida 4 para 4, who presented in the ER right after the birth of her child. She was in pain but did not have active bleeding. The uterus is inverted and prolapsed completely through the vagina and vulva. The insertion site of the placenta (which is not attached anymore) can still be seen as a round, darker part compared to the lighter myometrium.
Source: “Completely inverted uterus” by Lawrence Mbuagbaw, Patrick Mbah Okwen, The Pan African Medical Journal, licensed under CC BY 4.0.
1. Grasp the protruding portion of the uterus.
2. Direct fingers towards the posterior fornix.
3. Lift the uterus into the abdominal cavity.
© AMBOSS
Abnormal placental separation
Retained placenta [12]
Definition
- Retention of the placental tissue inside the uterine cavity following the first 30 min postpartum.
Epidemiology
- Approx. 3% of vaginal deliveries [12]
Etiology
- Atonic uterus: See “Uterine atony” section above.
- Placenta accreta spectrum: See “Abnormal placentation” below.
- Premature closure of the cervix obstructing placental expulsion
Classification
- Adherent placenta: a placenta that is not detached because of insufficient uterine contractions (e.g., uterine atony)
- Trapped placenta: a detached placenta that cannot be delivered spontaneously or with light cord traction because of cervical closure
Risk factors
- Prior history of retained placenta (most common)
- Placenta previa
- Placenta accreta spectrum
- Prior cesarean delivery
- Uterine fibroids
- Prolonged use of uterotonic medication (e.g., oxytocin)
- Preterm labor
- Assisted reproduction procedures (e.g., in vitro fertilization)
Clinical features
- Main feature: severe bleeding before placental delivery
-
Physical examination
- Inability to completely separate the placenta during the third stage of labor
- Speculum inspection: visualization of placental fragments or fetal membranes within the uterus
Diagnosis
- Postpartum manual palpation and speculum inspection of the placenta and fetal membranes
- Ultrasound: showing a focal endometrial mass
Treatment
- General measures: See “Management” in “Overview” section above.
- Active management of the third stage of labor: See “Prevention” in “Overview” section above.
-
Manual removal of placenta
- Consider administering nitroglycerin.
- Perform under adequate regional or general anesthesia.
- Administer prophylactic antibiotics.
- Technique
- Keep fingers tightly together and use the edge of the hand to make a space between the placenta and the uterine wall to detach the placenta completely.
- After placenta is detached, withdraw the hand from the uterus, bringing the placenta with it.
- With the other hand, perform countertraction to the fundus by pushing it in the opposite direction of the hand that is removing the placenta.
-
Surgical management
- Indicated in cases where manual extraction fails
- Preferred method: suction curettage (associated with a risk of uterine perforation)
- Uterine balloon tamponade or packing: if severe bleeding persists
Abnormal placentation [13][14]
Definition
- Defective decidual layer of the placenta leading to abnormal attachment and separation during postpartum period
Epidemiology
- Placental detachment abnormalities due to anatomical causes occur in up to 1% of all pregnancies.
Classification
Depending on the depth of implantation of the trophoblast in the uterine wall [15]
- Placenta accreta: chorionic villi attach to the myometrium (but do not invade or penetrate the myometrium): rather than the decidua basalis (up to 75% of cases)
- Placenta increta: chorionic villi invade or penetrate into the myometrium (approx. 20% of cases)
- Placenta percreta: chorionic villi penetrate the myometrium, penetrate the serosa, and in some cases, adjacent organs/structures (approx. 5% of cases)
Pathophysiology [16]
- The exact pathogenesis is unknown
- Two main theories include
- Defective decidua: complete or partial lack of decidua in an area of previous scarring within the endometrial-myometrial interface
- Excessive trophoblastic invasion: abnormal growth → uncontrolled invasion of villi through the myometrium, including its vascular system
Risk factors [16]
Any prior damage to the endometrium
- History of uterine surgery (e.g., endometrial ablation, hysteroscopic removal of intrauterine adhesions, dilatation, curettage)
- Prior births by cesarean delivery
- Placenta previa
- Multiparity
- Advanced maternal age
- Assisted reproduction procedures
- Asherman syndrome
The types of abnormal placental attachment: Placenta Accreta “Attaches” to the myometrium, placenta Increta “Invades” the myometrium, and placenta Percreta “Perforates” the myometrium.


Clinical features
-
Most common manifestations
- Abnormal uterine bleeding
- Postpartum hemorrhage at the time of attempted manual separation of the placenta
-
Other manifestations
- Fever
- Rarely, hematuria in placenta percreta [17]
Diagnosis [18][19]
- Clinical diagnosis: See “Clinical features” above.
-
Ultrasound
- Thinning of uterine myometrial wall
- Placental lacunae (particularly irregularly shaped), giving the placenta a moth-eaten appearance
- Disruption of the junction between the bladder wall and uterine serosa
- Loss of clear space behind the placenta
- Specific to placenta increta/percreta
- Increased number of placental vessels extend beyond the myometrium into another serosa
- Focal mass of placental tissue extending through the uterine serosa into adjacent organs
-
Doppler ultrasonography: confirmatory imaging
- Shows turbulent blood flow
- Increased myometrial vascularity
- MRI: performed if ultrasound studies are inconclusive


Treatment [1]
-
Prevention of predelivery
- Scheduled delivery
- Avoid pelvic exams
- Avoid sexual intercourse
- Preoperative planning for PPH
- Active management of the third stage of labor: See “Prevention” in “Overview” section above.
- General measures: See “Management” in “Overview” section above.
-
Surgical procedures
- Dilation and curettage (D&C) or vacuum removal of RPOC under anesthesia/regional anesthesia
-
Cesarean hysterectomy
- Generally, the mode of delivery and treatment for placenta accreta spectrum
- The placenta is left in place after delivery and complete hysterectomy is performed.
Uterine-preserving measures are relatively contraindicated in placenta accreta spectrum due to high maternal mortality!
Prognosis [13]
- Morbidity is approx. 27%
- Placenta percreta has the highest complication rate.
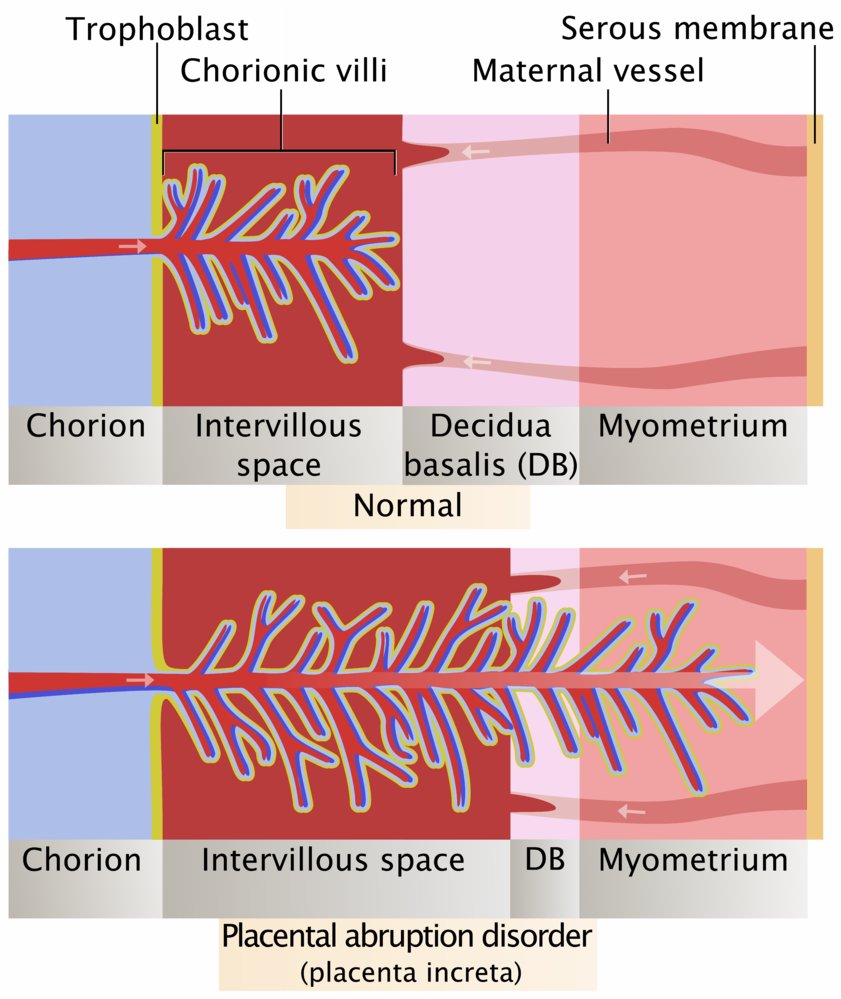
Normal: Chorionic villi with fetal blood reach into the intervillous space filled with maternal blood, which is located in between the chorion and the decidua basalis.
Placental abruption disorder: The decidual layer of the placenta is defective; the chorionic villi may attach to the myometrium (placenta accreta), penetrate or invade the myometrium (placenta increta, shown here), or even penetrate the serosa, and in some cases, adjacent organs (placenta percreta).
© AMBOSS
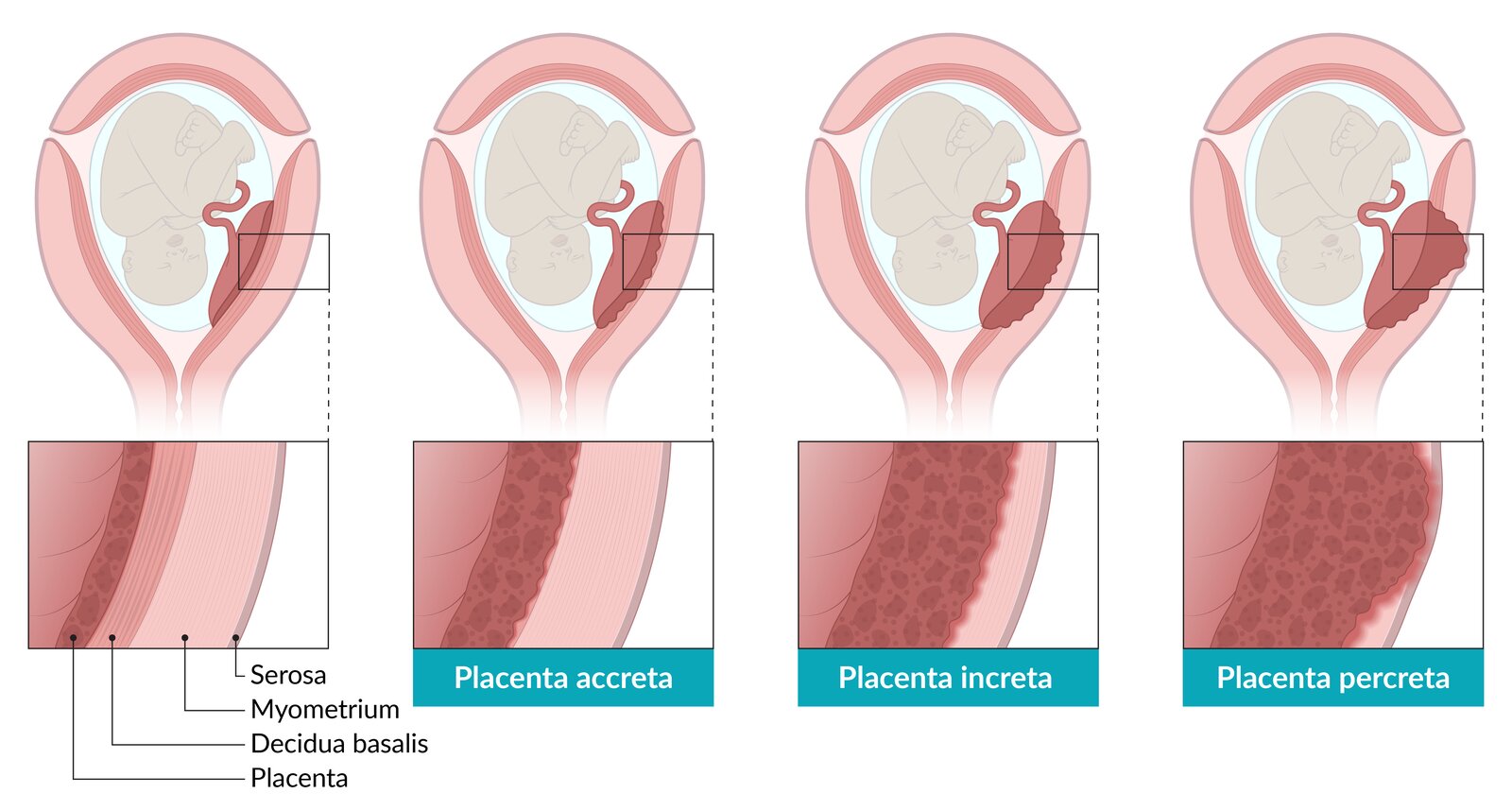
Placental attachment disorders are classified according to the depth of implantation of the trophoblast in the uterine wall:
– Left: Normal placentation
– Placenta accreta: chorionic villi attach to the myometrium rather than the decidua basalis (but do not invade or penetrate the myometrium)
– Placenta increta: chorionic villi invade or penetrate into the myometrium
– Placenta percreta: chorionic villi penetrate the myometrium, penetrate the serosa, and, in some cases, adjacent organs/structures
© AMBOSS

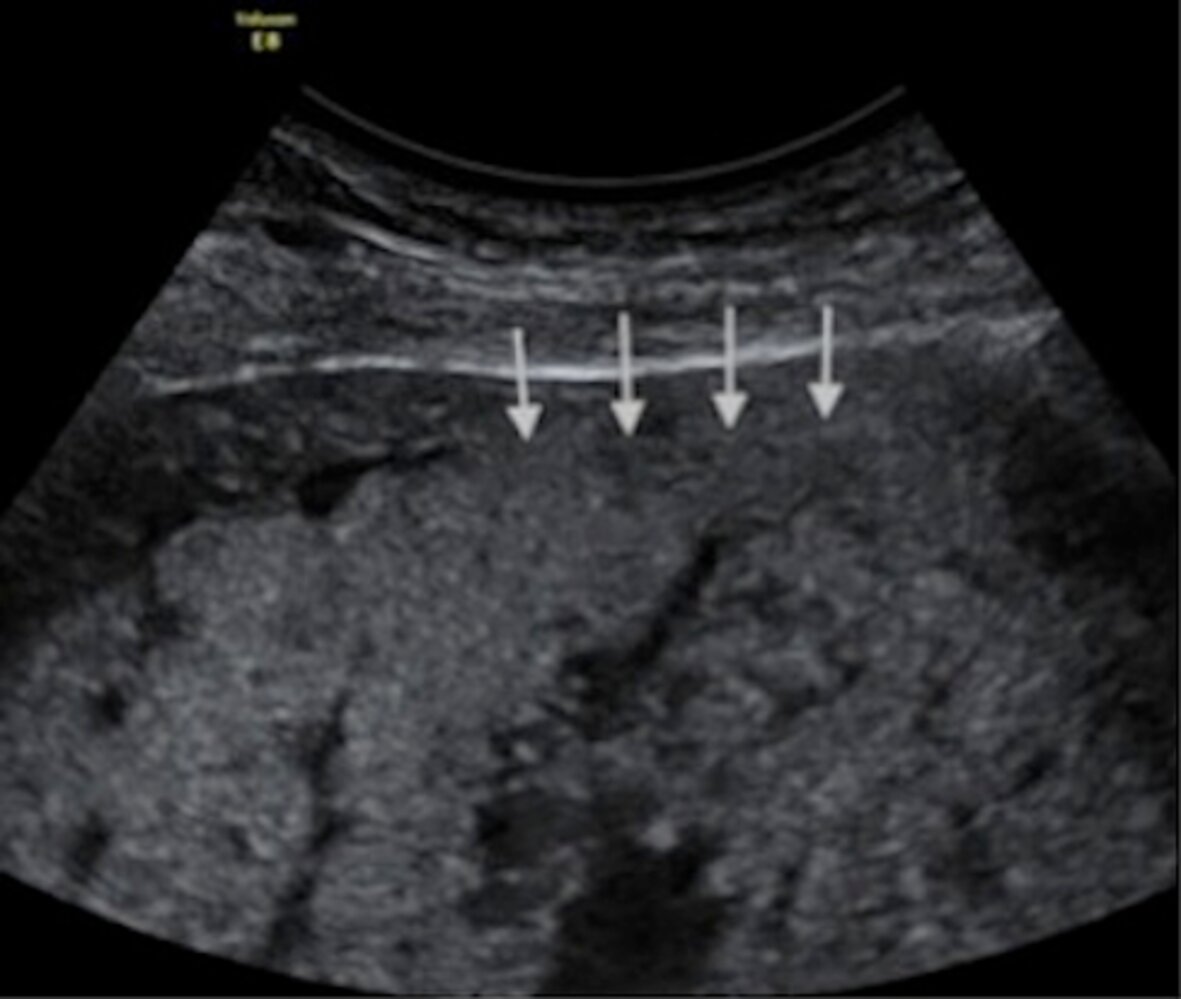
Ultrasound pelvis (placenta) of a patient with placenta accreta
Thinning of the myometrial wall has occurred, with loss of the retroplacental clear zone, focal disruption (arrows) of the normally hyperechoic uterine serosa-bladder wall interface (red overlay), and bulging of the uterus toward the bladder. Intraplacental lacunae (examples indicated by green overlay) are also visible.
Sonographic features that should prompt concern for placenta accreta include myometrial thinning or disruption of the serosa-bladder wall interface, loss of a normal retroplacental clear zone, and the presence of intraplacental lacunae.
B: bladder; P: placenta
Source: “Figure 2, in: Accuracy of Ultrasonography and Magnetic Resonance Imaging in the Diagnosis of Placenta Accreta” by Riteau A-S, Tassin M, Chambon G, Le Vaillant C, de Laveaucoupet J, Quéré M-P, et al., PLoS ONE, licensed under CC BY 4.0. Modifications: cropped white rim. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Ultrasound pelvis (placenta) of a patient with placenta accreta
There is obliteration (arrows) of part of the retroplacental (subplacental) clear zone, a normally hypoechoic region composed of decidua basalis and myometrium.
Deficiency of the clear zone can signify invasion of trophoblastic tissue and should prompt evaluation for additional markers of placenta accreta. Loss of the zone has also been reported in normal pregnancies.
P: placenta
Source: “Figure 1, in: Accuracy of Ultrasonography and Magnetic Resonance Imaging in the Diagnosis of Placenta Accreta” by Riteau A-S, Tassin M, Chambon G, Le Vaillant C, de Laveaucoupet J, Quéré M-P, et al., PLoS ONE, licensed under CC BY 4.0. Modifications: cropped white rim. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Birth trauma
Birth trauma can result in bleeding lacerations, puerperal hematomas, and/or uterine rupture.
Definition
Puerperal hematoma is an accumulation of blood in the vulva, vagina, or retroperitoneum, most commonly caused by iatrogenic injury during childbirth. Subtypes include:
- Vulvar hematoma: accumulation of blood in the vulvar soft tissue
- Vaginal hematoma: accumulation of blood in the vaginal soft tissue
- Retroperitoneal hematoma: accumulation of blood in the retroperitoneal space
Epidemiology
- Second most common cause (20% of individuals with postpartum hemorrhage) [2]
- Estimated incidence of puerperal hematoma ranges from 1:300 to 1:1500 deliveries.
Etiology
-
Iatrogenic injury: e.g., during assisted vaginal delivery, cesarean delivery
- Cervical laceration (most commonly caused by forceps delivery)
- Lower vaginal trauma (most commonly caused by episiotomy)
- Uterine rupture due to prior cesarean delivery
- Puerperal hematoma: most commonly caused by uncontrolled delivery or assisted vaginal delivery
-
Other
- Fetal macrosomia
- Malpresentation of the fetus
- Uncontrolled delivery
- Prolonged second stage of labor
- Primiparity
- Coagulopathy
- Hypertensive disease of pregnancy
Clinical features
-
Features of hematoma or bleeding laceration of the female genital tract
- Severe pain in the labia, pelvis and/or perineum ≤ 24 hours after delivery
- Severe bleeding, hypovolemic shock
- Vaginal hematoma: protruding, tender, palpable vaginal mass
-
Features of retroperitoneal hematoma
- Pelvic pain
- Signs and symptoms of hypovolemia (e.g., tachycardia, hypotension, diaphoresis, pale skin, dizziness)
- Features of uterine rupture
Treatment [2]
-
Following vaginal delivery
- Supportive measures (e.g., fundal massage, fluid therapy, uterotonic agents)
- Immediate repair of visible bleeding lacerations
- Hemodynamically stable patient: arterial embolization
-
Hemodynamically unstable patient
- Incision and drainage of hematoma
- If the cause of bleeding is not identified: immediate laparotomy
-
Following cesarean delivery
- Supportive measures
- Uterine artery ligation
- If the above techniques fail: uterine compression suture technique (e.g., B-Lynch suture)
- Hysterectomy: if there are life-threatening complications or other treatments have failed
Velamentous cord insertion
Definition
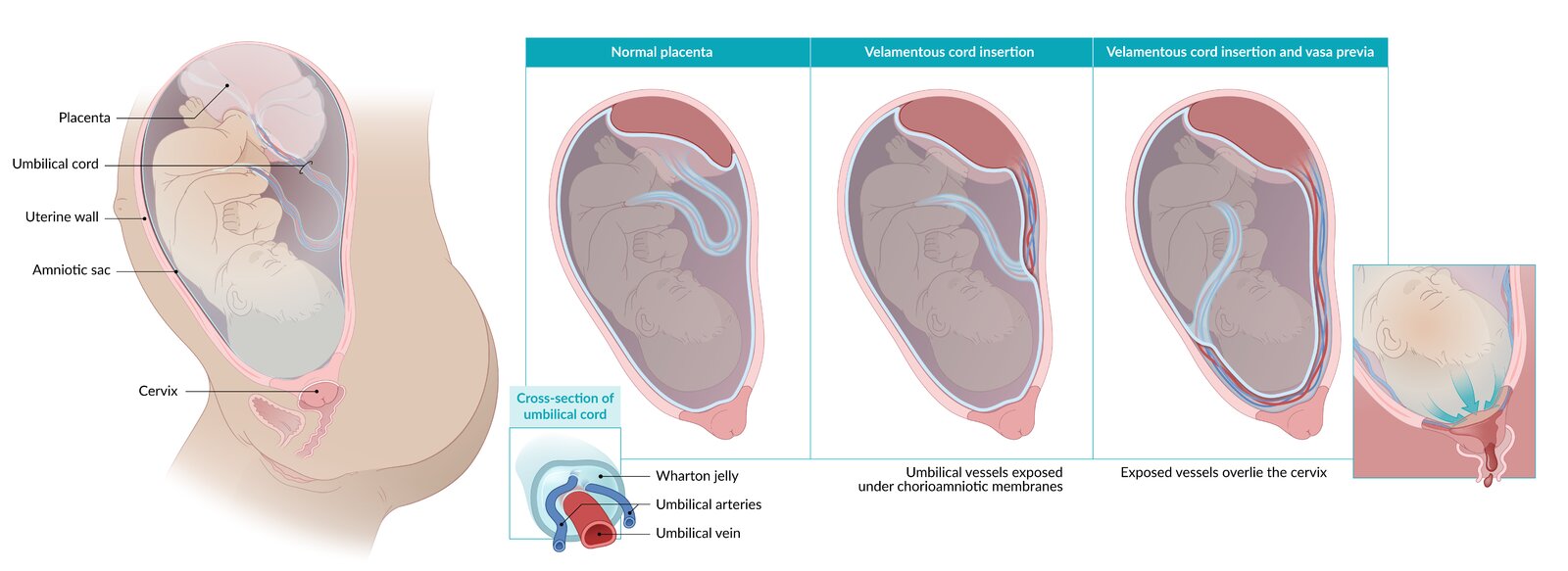
- Abnormal cord insertion into chorioamniotic membranes, resulting in exposed vessels only surrounded by thin fetal membranes, in the absence of protective Wharton jelly [20]

Epidemiology [21]
- Occurs in 1% of single pregnancies
- Up to 15% in twin pregnancies
- Associated with increased risk of hemorrhage during the third stage of labor
Risk factors
- Placenta previa
- Low-lying placenta
- Multiple pregnancies
- Assisted reproduction procedures (e.g., in vitro fertilization)
- Succenturiate placenta
Pathogenesis
The following two mechanisms have been described [22]
- Trophotropism theory: gradual placental migration towards a well-vascularized uterine section, displacing the cord towards the periphery of the placenta
- Polarity theory: oblique implantation of the blastocyst leading to an abnormal cord insertion
Clinical features
- Increased risk of hemorrhage during the third stage of labor
- Possible painless vaginal bleeding, typically in the third trimester: Blood loss occurs only in the fetus.
- Features of fetal hypoxia, especially following rupture of membranes (ROM)
Diagnosis
-
Prenatal period
-
Transabdominal ultrasound: helps to determine the correlation between the placenta and the cervical os
- Vessels pass over the internal cervical os
- Membranous umbilical vessels located at the placental cord insertion site and the umbilical cord sheath ends before the placenta
- Umbilical cord membranes are continuous with the chorionic plate
- Transvaginal color doppler ultrasound: indicated to rule out vasa previa [23]
-
Transabdominal ultrasound: helps to determine the correlation between the placenta and the cervical os
- Intrapartum clinical examination: See “Clinical features” above.
Management
-
If diagnosed prenatally
- Regular fetal assessment (e.g., fetal growth, fetal heart rate tracing)
- Deliver ≤ 40 weeks gestation
-
If diagnosed intrapartum
- Vaginal delivery if there are no signs of fetal distress
-
Emergency cesarean delivery if
- Signs of fetal distress
- PPH
- Vasa previa
Complications
- Vasa previa
- Fetal death
- Premature infant
- Fetal growth restriction
- Fetal malformation [24]
© AMBOSS

Placenta with amniotic sac and umbilical cord
The umbilical cord can be seen inserting into the membranes of the amniotic sac instead of the center of the placenta, where it normally inserts, and joining the placenta at the lateral border. Several vessels with large lumens run freely on the amniotic membrane between the placenta and the umbilical cord.
This phenomenon is called “velamentous insertion,” and it comes with a risk of injury to the umbilical vessels and potentially life-threatening fetal hemorrhage upon rupture of the membranes.
Source: "Insertio_velamentosa", Schokohäubchen, Wikimedia Commons licensed under Public Domain
{kind=link}
Subinvolution of placental implantation site
Definition
- A condition in which the uterus remains abnormally large following delivery because of the persistence of dilated uteroplacental vessels
Epidemiology
- Occurs most commonly in the second week postpartum
- Second most common cause of secondary postpartum hemorrhage (13% of affected individuals) [25]
Risk factors [3]
- Multiparity
- Cesarean delivery
- Uterine atony
- Endometritis
- Coagulopathy
- Retained products of conception
Clinical features
- Abnormal, severe uterine bleeding, most commonly during second week postpartum [4]
- Fever, chills
- Lower abdominal pain
- Signs of hypovolemia
Diagnostics [4]
- Ultrasound: hypoechoic tortuous vessels in the myometrium
- Pulsed wave Doppler: ↑ peak systemic velocity
- Histopathological examination (confirmatory test): large, dilated myometrial arteries with thickened walls and intravascular thrombosis
Treatment [26][27]
- Uterotonic agents (e.g., IV oxytocin)
- Surgical procedures (i.e., dilation and curettage or suction curettage)
- Severe bleeding: Uterine artery embolization, hysterectomy for patients with severe bleeding
References
- Committee on Practice Bulletins-Obstetrics. "Practice Bulletin No. 183: Postpartum Hemorrhage". Obstetrics & Gynecology. 130(4). :e168-e186. (2017)
- Marx J, Walls R, Hockberger R. "Rosen's Emergency Medicine - Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2013). ISBN: 9781455749874
- Gill P, Patel A, Van Hook MD JW. "Uterine Atony". StatPearls. (2020)
- Anderson JM, Etches D. "Prevention and Management of Postpartum Hemorrhage". Am Fam Physician. 75(6). :875-882. (2007)
- Perlman NC, Carusi DA. "Retained placenta after vaginal delivery: risk factors and management". International Journal of Women's Health. Volume 11. :527-534. (2019)
- American College of Obstetricians and Gynecologists. "Placenta Accreta Spectrum: Obstetric Care Consensus Number 7". American Journal of Obstetrics and Gynecology.. 132(December 2018). :259–75. (2018)
- Kainer F, Hasbargen U. "Emergencies associated with pregnancy and delivery: Peripartum hemorrhage". Dtsch Arztebl Int. 105(37). :629–638. (2008)
- Goh WA, Zalud I. "Placenta accreta: diagnosis, management and the molecular biology of the morbidly adherent placenta". The Journal of Maternal-Fetal & Neonatal Medicine. :1-6. (2015)
- Jauniaux E, Collins S, Burton GJ. "Placenta accreta spectrum: pathophysiology and evidence-based anatomy for prenatal ultrasound imaging". Am J Obstet Gynecol. 218(1). :75-87. (2018)
- Konijeti R, Rajfer J, Askari A. "Placenta percreta and the urologist.". Rev Urol. 11(3). :173-6
- Kumar S, Satija B, Wadhwa L, et al. "Utility of ultrasound and magnetic resonance imaging in prenatal diagnosis of placenta accreta: A prospective study". Indian Journal of Radiology and Imaging. 25(4). :464. (2015)
- Doubilet PM, Benson CB. "Atlas of Ultrasound in Obstetrics and Gynecology". Lippincott Williams & Wilkins. :201-203. (2012). ISBN: 9781608317783
- Lockwood CJ, Russo-Stieglitz K. "Velamentous umbilical cord insertion and vasa previa". UpToDate. UpToDate. https://www.uptodate.com/contents/velamentous-umbilical-cord-insertion-and-vasa-previa. [2016-11-22]
- Bohîlțea RE, Cîrstoiu MM, Ciuvica AI, et al. "Velamentous insertion of umbilical cord with vasa praevia: case series and literature review.". Journal of medicine and life. 9(2). :126-9
- Hasegawa J, Iwasaki S, Matsuoka R, et al. "Velamentous cord insertion caused by oblique implantation after in vitro fertilization and embryo transfer". J Obstet Gynaecol Res. 37(11). :1698-1701. (2011)
- Sinkey RG, Odibo AO, Dashe JS. "#37: Diagnosis and management of vasa previa". Am J Obstet Gynecol. 213(5). :615-619. (2015)
- Weeks A. "Retained placenta after vaginal birth". UpToDate. UpToDate. http://www.uptodate.com/contents/retained-placenta-after-vaginal-birth. [2016-10-05]
- Sellmyer MA, Desser TS, Maturen KE, Jeffrey RB, Kamaya A. "Physiologic, Histologic, and Imaging Features of Retained Products of Conception". RadioGraphics. 33(3). :781-796. (2013)
- Triantafyllidou O, Kastora S, Messini I, Kalampokis D. "Subinvolution of the placental site as the cause of hysterectomy in young woman". BMJ Case Reports. 14(2). :e238945. (2021)
- VanderMeulen H, Petrucci J, Floros G, et al. "The experience of postpartum bleeding in women with inherited bleeding disorders". Research and Practice in Thrombosis and Haemostasis. 3(4). :733-740. (2019)
- Evensen A, Anderson JM, Fontaine P. "Postpartum Hemorrhage: Prevention and Treatment.". Am Fam Physician. 95(7). :442-449. (2017)
- Wendel MP, Shnaekel KL, Magann EF. "Uterine Inversion: A Review of a Life-Threatening Obstetrical Emergency.". Obstet Gynecol Surv. 73(7). :411-417. (2018)
- Bhalla R, Wuntakal R, Odejinmi F, Khan RU. "Acute inversion of the uterus". The Obstetrician & Gynaecologist. 11(1). :13-18. (2009)
- Thakur M, Thakur A. "Uterine Inversion". StatPearls. (2020)
- Dossou M, Debost-Legrand A, Déchelotte P, Lémery D, Vendittelli F. "Severe Secondary Postpartum Hemorrhage: A Historical Cohort". Birth. 42(2). :149-155. (2015)
- Petrovitch I, Jeffrey RB, Heerema-McKenney A. "Subinvolution of the Placental Site". Journal of Ultrasound in Medicine. 28(8). :1115-1119. (2009)
- Ramkumar S, Kharshiing T. "Vessel Subinvolution of the Placental Implantation Site: A Case Report and Review of Supportive Literature". Cureus. (2021)
- American College of Obstetricians and Gynecologists. "Postpartum Hemorrhage". Obstetrics & Gynecology. 130(4). :923-925. (2017)
- Weeks AD. "The retained placenta.". Best Pract Res Clin Obstet Gynaecol. 22(6). :1103-17. (2008)